
Submitted:
13 March 2024
Posted:
15 March 2024
You are already at the latest version
Abstract
Despite the importance of influenza vaccination for healthcare workers (HCWs), their uptake remains challenging. This study aimed to measure influenza vaccine hesitancy among HCWs in Nakhon Phanom province, Thailand. A representative cross-sectional survey was conducted at six hospitals during August – September 2020 using a self-administered questionnaire. HCWs delaying getting influenza vaccines, accepting but unsure, or refusing with doubts were categorized as hesitant. Those accepting without any doubts were classified as non-hesitant. Vaccine hesitancy determinants were identified by multivariable logistic regression analysis. A total of 338 participants (97%) completed the questionnaires; most were female nurses working at district hospitals without pre-existing chronic medical conditions. Nearly 60% of participants (197/338) exhibited influenza vaccine hesitancy, and significant factors included age above 50 years adjusted odds ratio [aOR] 3.2, 95% CI 1.3-8.5), fair knowledge of influenza/vaccination (aOR 0.4, 95% CI 0.2-0.8), and negative influence of other HCW (High level– aOR 2.3, 95% CI 1.1-4.8; Moderate level- aOR 2.1, 95% CI 1.1-4.4). Imparting updated information to the HCW combined with positive guidance from influential peers may help reduce this hesitancy.
Keywords:
influenza vaccine
; healthcare workers
; vaccine hesitancy
; Thailand
1. Introduction
Healthcare workers (HCWs) are recommended for seasonal influenza vaccines as they are at a higher risk of contracting influenza and inadvertently transmitting the virus to high-risk and vulnerable patients who may develop severe complications [1,2,3,4,5]. However, despite several recommendations, influenza vaccine uptake among HCWs has remained a challenge globally [6,7,8]. Many studies indicate that despite vaccine availability, some HCWs may be hesitant about vaccines, especially influenza vaccines, including when considering the vaccines for their children or their patients [9,10,11].
While the anti-vaccination movement is not a recent development [12], more people are becoming skeptical of vaccines, such that vaccine hesitancy is now considered a major threat to global health [13]. As HCW recommendations are highly influential for patients [14,15], acceptance of vaccination by HCWs themselves is, therefore, also an important determinant of influenza vaccine uptake in the populations that they serve. Addressing the concerns of HCWs may be strategically beneficial in reducing vaccine hesitancy among the general public as well [16].
Defined as “a delay in acceptance or refusal of vaccines despite availability of vaccination services” by the World Health Organization (WHO)’s Strategic Advisory Group of Experts (SAGE), vaccine hesitancy is a behavioral phenomenon that broadens the scope of study of vaccination decision-making [17]. Vaccine-hesitant people are seen in a spectrum between those who accept vaccination without any doubts and those who reject vaccination at all costs. In their “3C” model, SAGE identified “complacency”, “inconvenience in accessing vaccines”, and “lack of confidence” as three key reasons for this hesitancy [17]. However, this phenomenon is dependent on the context and specific to vaccines. For example, the hesitancy to influenza vaccine may be different than to other vaccines. Therefore, SAGE supplemented the “3C” model with a vaccine hesitancy determinant matrix that included contextual, individual and group, and vaccine/vaccination-specific influences [17]. Although Paterson et al. adapted this matrix for HCW and added a few more determinants [18], it has been informed largely by research from high-income countries. Evidence from middle-income countries like Thailand has remained minimal.
In Thailand, HCWs were the first group to be recommended for yearly influenza vaccination by the Ministry of Public Health (MOPH) since 2004 [19]. Vaccination rates among Thai HCWs were self-reported to be as high as 89% in 2009 [20]. However, in 2018, regional reports showed that HCW influenza vaccine coverage had plummeted to below 30% in some regions (Department of Medical Services [DMS], MOPH). Although little is known about Thai HCW’s attitudes towards influenza vaccines, there are some disconcerting pieces of evidence. A study revealed that only 60% of Thai HCWs were willing to receive the pandemic influenza A(H1N1) vaccine [21]. In 2013, more than one-third of the Thai physicians working in ante-natal care clinics were found to have doubts about influenza vaccine’s safety and effectiveness, and only 25% of them routinely recommended influenza vaccines to pregnant women [22]. Another study reported that the seasonal influenza vaccine acceptance rate among medical professionals at a tertiary hospital in Bangkok was 65.4% [23]. Being the most informed group of people about the benefits of vaccines and having more access to vaccine than others, moderate acceptance and lower recommendations of influenza vaccines by Thai HCW may indicate deeper-lying cultural or personal concerns that might relate to vaccine hesitancy.
Despite being the study site of many influenza vaccine-related research in Thailand in the recent past that have actively partnered with local HCWs [24,25,26], the HCW uptake rate in Nakhon Phanom province was only 28% in 2018 (DMS, MOPH). Low uptake of influenza vaccines among HCWs is particularly remarkable in this border northeastern province as it is considered a “model” province for influenza vaccine research in Thailand, where vaccination rates are supposed to be higher. As Thailand’s influenza vaccination policies were largely shaped by the active surveillance data from this province [27,28,29], we found it important to evaluate if the HCWs in the province were themselves hesitant to influenza vaccines. Therefore, the objectives of this cross-sectional survey were to identify and measure influenza vaccine hesitancy among HCWs in Nakhon Phanom province.
2. Materials and Methods
2.1. Study Design and Setting
This cross-sectional survey was part of a mixed-methods study on influenza vaccine hesitancy among healthcare workers in Nakhon Phanom province, which is located in the plateau region of northeastern Thailand, approximately 735 km from Bangkok. The province borders Lao PDR and has a total area of 5,528.88 sq. km. The province consists of 12 districts, with Muang district as the capital, along with 97 sub-districts and 1,123 villages [27]. There are 14 public hospitals in the province: one provincial general hospital, 11 community hospitals, a psychiatric hospital, and a military hospital. From 2003 to 2015, there was active surveillance of respiratory illnesses in the public hospitals of this province [27,28,29].
2.2. Study Population
Thai HCWs of Nakhon Phanom province were the targeted population of the study. Although the WHO defines HCW as “all people engaged in actions whose primary intent is to enhance health” [30], we limited HCW's definition to those who were currently working in public hospital settings in Nakhon Phanom for operational feasibility. As per a report of DMS, 1,863 registered HCWs were working in the province in 2018 (DMS, MOPH). The HCWs were broadly categorized into two groups according to the amount of patients’ contact/exposure and as grouped by WHO [31]: a) Health service providers who delivered health services and came in direct contact with patients and substances such as patients’ blood and other specimens, and b) Health management and support staff who assisted in the functioning of the health system without directly providing health services and as such may or may not have had direct contact with the patients. According to the nature of their work, health service providers were further sub-categorized into six groups - medical doctors, dentists, nurses, pharmacists, public health officers, and other service providers [31].
2.3. Participant Selection Criteria
Thai HCWs of both sexes (male and female) aged above 18 years, having a good command of the written and spoken Thai language, and currently working at a public hospital in Nakhon Phanom province were included in the study. HCWs who were not present in the hospital at the time of data collection and who were not willing to participate in the study voluntarily were excluded.
2.4. Sample Size and Sampling Technique
As there was no prior estimate of influenza vaccine hesitancy among Thai HCWs, a conservative proportion of 50% was taken to calculate the sample size for the survey. A sample size of 350 was calculated using the single proportion formula and a finite population correction factor in OpenEpi (www.openepi.com), assuming a Type I error of 5%, absolute precision of 7.5 percentage points, and a design effect of 2 given the cluster sampling used for the population size of 1,863 HCW in Nakhon Phanom after inflating 10% for refusal and absences.
HCWs were recruited in the survey using a two-stage cluster sampling. In the first stage, hospitals were selected as clusters to recruit 50 HCWs in each cluster (i.e., seven clusters in total). The hospitals were chosen by a systematic random sampling using probability proportional to size (PPS) of the number of HCWs. As Nakhon Phanom Provincial hospital was a large hospital, it got selected twice. Therefore, 100 HCWs were recruited from that particular hospital, and 50 HCWs were selected from five other hospitals. In the second stage, HCWs were chosen using stratified random sampling according to their professional categories and proportional distribution in each hospital. Microsoft Excel sheets were used to generate the random numbers for the sampling in both stages, as described above.
2.5. Survey Instrument and Data Collection
The survey questions were modified from the sample questions of SAGE’s vaccine hesitancy determinant matrix for the Thai context to measure influenza vaccine hesitancy and its three broad determinants: contextual or sociocultural, individual/group, and influenza vaccine-specific influences [18,32]. The participants were asked to indicate their level of agreement or disagreement with the items of the constructs on a 5-point Likert scale, with ‘1’ meaning strongly disagree and ‘5’ strongly agree. The questionnaire took around 30-35 minutes to complete and was validated for use in the Thai context by another research project in which face validity, content validity, acceptability, and internal consistency were assessed by pilot testing among 30 HCWs in a randomly selected hospital in Bangkok.
In this survey, the questionnaire was self-administered to the HCWs who were approached through designated focal points at the six hospitals in the province, identified by the sampling technique, from August to September 2020. A total of 350 questionnaires were distributed to the participants.
2.6. Variables and Measurement
The dependent variable of the study, influenza vaccine hesitancy, was defined as either delaying getting influenza vaccines, accepting the vaccines but being unsure, or refusing the vaccine despite seeing its value. It was measured as a binary variable (yes/no).
“Yes” meant those HCWs who displayed some form of hesitancy, and “No” meant HCWs who accepted the influenza vaccine without any doubts.
The independent variables included demographic and work characteristics. Participant’s age and years of experience as HCW were first measured as continuous variables and then converted to appropriate categories. Categorical variables were sex (binary - male/female), religion, level of the hospital (Provincial/District), HCW type (Health service providers/Health management and support staff), daily exposure to patients (<1 meter/≥1 meter/no contact), education level, and self-reported presence of any pre-existing medical conditions (yes/no). Participants’ knowledge of influenza and vaccination was assessed using seven items and then grouped into three categories using a modification of Bloom’s original cut-off points, such that six or more correct answers (i.e. ≥80%) represented “good knowledge”, four to five correct answers (i.e. 60-79%) meant “fair knowledge” and three or less correct answers (i.e. <60%) were considered as “needed improvement”.
The determinants of vaccine hesitancy were measured as constructs (i.e., composite variables). Contextual factors included the negative influence of media/social media (2 items), politics/policies (2 items), pharmaceutical industry influences (2 items), and the level of trust in the health system (2 items). Individual/group influences contained constructs of experience with past vaccination (3 items), beliefs and attitudes about influenza and vaccination (3 items), vaccination as a social norm (3 items), and influence of other healthcare professionals (2 items). Influenza vaccine/vaccination-specific issues included constructs of risk/benefit (perceived, heuristic) (4 items), risk of adverse events due to vaccination (3 items), fear of painful injections (2 items), and access to vaccines in the hospital (4 items) (Table A1). Both positively and negatively worded statements were used, and the direction of negatively worded questions was reversed for data analysis. Items under each construct were averaged to create aggregated mean scores for the construct. The average scores were case-ranked and then used to divide the construct into three categories – high, moderate, and low.
2.7. Data Analysis
Descriptive statistics were first employed to provide a summary of the selected variables and study samples. The mean scores of vaccine hesitancy determinants were compared between hesitant and non-hesitant HCWs using independent t-tests. The associated factors of influenza vaccine hesitancy were identified by a series of binary logistic regression models. As the dependent variable (influenza vaccine hesitancy) was categorical, the logistic regression analysis was performed using non-hesitant HCW as the reference category. All variables showing at least some evidence of association (Type III p values <0.1 in the binary logistic regression models) were entered into a multivariable logistic regression model, adjusting hospital locations to account for clustering. Variables with significant adjusted odds ratio (aOR) in the final model were recognized as associated factors (p-value <0.05). All data analysis was conducted using SPSS version 20 (IBM Corp., Armonk, NY).
2.8. Ethical Considerations
Written informed consent was obtained from each participant before data collection. The study protocols and all related study documents were reviewed and approved by the Mahidol University - Central Institutional Review Board (MU-CIRB) (Protocol number MU-CIRB 2020/138.1606). Permission for data collection was also received from the Provincial Chief Medical Officer, Nakhon Phanom Provincial Public Health Office (ref no. 78.02/ 06115).
3. Results
3.1. Response Rate
3.2. Participant Characteristics
Of those 338 participants, the mean age was 37.2±9.7 years, with a minimum of 20 years and a maximum of 60 years. Almost all participants were Buddhists (333; 98.5%). A majority of the participants were female (280; 82.8%), nurses (136; 40.2%), from district hospitals (238; 70.7%), with bachelor’s degrees (223; 65.9%), and without any pre-existing chronic medical conditions (264; 78.1%) (Table 1). The participants had a mean work experience of 13.8±9.8 years as HCW, and around half of them reported having high daily exposure with patients in the proximity of less than 1 meter (172; 50.9%).
3.3. Knowledge about Influenza and Vaccination
A high majority of HCWs were aware of the MOPH recommendation of influenza vaccination for them (302; 89.3%). However, most participants were misinformed about the influenza vaccines as only 52% correctly identified that the influenza vaccine may not work if it contained the wrong virus strains than the circulating ones, and only 30% firmly believed that the influenza vaccine does not itself cause some people to get influenza (Table 2). Overall, only a quarter of the participants had a good knowledge regarding influenza and vaccination (85; 25.1%) (Table 2).
3.4. Influenza Vaccine Hesitancy among the Participants
A majority of the participants reported some degree of hesitancy towards influenza vaccines (197; 58.3%), and 7 HCWs (2.1%) were outright refusers of influenza vaccines who were not hesitant in their refusal (Figure 1). On closer inspection, most of the hesitant HCWs were “hesitant compliers” who had doubts about the influenza vaccines but still accepted them (172; 87.3%). Only 3 (1.5%) refused the vaccine while being considerate of its benefits, and 22 (11.2%) delayed receiving the vaccine for themselves (Figure 2). More than 60% of the health management staff, other medical professionals (paramedics), and nurses reported vaccine hesitancy, while other HCW types had less hesitancy than the sample prevalence of 58.3%; the least hesitancy was seen among pharmacists (31.6%) (Figure 3).
3.5. Vaccine Hesitancy Determinants
Removing the seven HCWs who refused influenza vaccines left with an analytical sample of 331 HCWs. The aggregated mean scores and standard deviations of the vaccine hesitancy determinants are presented in Table 3. The mean scores are on a scale of 1-5, where higher scores signify higher hesitancy or more negative sentiment towards the construct. Overall, the participants reported the highest negative perceptions towards pharmaceutical industry influences (mean score 2.8, SD 1.0) and influence of media/ social media (mean score 2.7, SD 0.8) (Table 3). When the mean scores were compared, HCW with influenza vaccine hesitancy were more likely to have a higher lack of trust in the health system (2.7 vs 2.3; p-value 0.008), negative past experience of vaccination (2.4 vs 2.1; p-value 0.017), negative perception of vaccination as a social norm (2.3 vs 2.0; p-value 0.011), negative influence of other HCW (2.2 vs 1.9; p-value 0.006), higher perceived risk and lack of benefit of influenza vaccine (2.4 vs 2.1; p-value 0.001), risk of adverse events due to vaccination (2.7 vs 2.3; p-value 0.001), fear of painful injections (2.5 vs 2.2; p-value 0.007), and lack of access to vaccines (2.5 vs 2.2; p-value <0.001) (Table 3).
3.6. Factors Associated with Influenza Vaccine Hesitancy
In a series of univariable logistic regression analyses, different variables were found to be significantly associated with influenza vaccine hesitancy (Table 4). Compared to young HCWs (aged 30 years and below), HCWs aged above 50 years were nearly three times more likely to be vaccine-hesitant (OR 2.8; 95% CI 1.2-6.3). Similarly, HCWs with 20 years or more work experience were more than two times more likely to be vaccine-hesitant than HCWs with experience of 5 years or less (OR 2.2; 95% CI 1.2-4.2). In contrast, HCWs having fair knowledge of influenza and vaccines were less likely to be hesitant compared to HCWs with less knowledge (OR 0.5; 95% CI 0.3-0.8).
Among the contextual factors, HCWs with negative perceptions of politics/policies and lack of trust in the health system had significant odds of being vaccine-hesitant compared to HCWs with positive perceptions (Table 4). Similarly, in the individual/group influences, significant determinants of hesitancy were negative past experience of vaccination (High - OR 2.1, 95% CI 1.2-3.7; Moderate – OR 1.7, 95% CI 1.0-2.9), moderate level of negative beliefs (OR 2.0, 95% CI 1.2-3.5), high negative perception of vaccination as a social norm (OR 2.2, 95% CI 1.3-3.9), and negative influence of other HCW (High – OR 3.3, 95% CI 1.9-5.7; Moderate - OR 2.7, 95% CI 1.5-4.9). Among the factors specific to influenza vaccines, low perceived risk (Low - OR 2.5, 95% CI 1.4-4.45; Moderate – OR 1.9, 95% CI 1.1-3.2), high risk of adverse events after vaccination (OR 2.8, 95% CI 1.5-5.3), fear of painful injections (High – OR 1.7, 95% CI 1.1-2.7; Moderate - OR 2.3, 95% CI 1.0-4.8), and reduced access to vaccines in the hospital (Low – OR 2.0, 95% CI 1.2-3.5; Moderate – OR 2.1, 95% CI 1.2-3.5) were significantly associated with the hesitancy.
However, in the multivariable model, only age (above 50 years – aOR 3.2, 95% CI 1.3-8.5), fair knowledge (aOR 0.4, 95% CI 0.2-0.8), and negative influence of other HCW (High – aOR 2.3, 95% CI 1.1-4.8; Moderate - aOR 2.1, 95% CI 1.1-4.4) remained significant factors of influenza vaccine hesitancy (Table 4). Work experience was not entered in the final model as it showed a high correlation with age.
4. Discussion
Influenza vaccine hesitancy was highly prevalent among the Thai HCWs in this study, as nearly 60% of the survey participants reported having some degree of hesitancy. Older age and the role of other HCWs were associated with increased hesitancy, while fair knowledge of influenza and vaccination was indicated to reduce hesitancy. The findings of this study can be used to improve local influenza vaccination policy in Thailand.
Since vaccine hesitancy studies are in their nascent stage in Thailand, there are no prior estimates of the prevalence of influenza vaccine hesitancy among the HCWs. Therefore, the proportion of 58.3% found in this study can function as a baseline figure of influenza vaccine hesitancy among Thai HCWs for future reference. Nevertheless, comparisons can be made with past Thai studies regarding the HCW doubts of the influenza vaccines. Nearly 50% of HCWs had some doubts about the influenza vaccine in this current study, which is higher than the 30% reported among Thai physicians in 2017 [22]. In a similar vein, the vaccine acceptance rate in this study was lower than the 65.4% reported among HCWs in a Bangkok hospital [23]. Although these comparisons are limited due to differences in study sites and the HCW definition, which was expanded to include all types of HCW working in the hospital in this study as opposed to only doctors or medical service providers in the past studies [22,23], they indicate that HCW in Nakhon Phanom may be more hesitant towards influenza vaccines than normally expected. Our result is also slightly higher compared to studies in countries such as Egypt, Hong Kong, and South Africa, where influenza vaccine hesitancy among HCWs was reported to be below 50% [33,34,35,36].
While the proportion of hesitant HCWs in this study is alarming, the proportion of HCWs who actively delayed and refused vaccination was only around 11%. Most of the hesitant HCWs were those who were skeptical of the influenza vaccine but still received the vaccination. A possible explanation for this phenomenon may be that although there isn’t a mandatory vaccination for HCWs and there is a notion of HCW’s choice, in reality, the HCWs often end up taking the influenza vaccines as an obligation, particularly as Nakhon Phanom is a “model” province for influenza vaccine research in Thailand where vaccination rates are supposed to be higher.
In this study, the role of other HCWs, such as the medical doctor, vaccinator nurses, or senior staff, was a significant predictor of influenza vaccine hesitancy. This is an important finding as it suggests that HCW vaccine hesitancy can be potentially reduced when HCWs, such as medical doctors and supervisors, provide positive feedback and peer support to their fellow HCWs. Medical doctors have a higher social class [37], and along with vaccinator nurses, senior HCWs have more social capital to be influential in social interactions with other HCWs in hospital settings [38]. As many studies indicate, the acceptance of influenza vaccination among this group is likely to be transferred to their HCW colleagues. For example, supervisor and physician encouragement has been found to be a key predictor of HCW vaccination [39]. The strategy of using influential HCWs and senior staff was found to improve HCW vaccination in research conducted in countries such as Spain and Canada [40,41]. Similarly, in Israel, a randomized controlled trial showed that an intervention comprising of a lecture from a family physician, in addition to e-mail reminders, and a personal approach from a key local staff (doctor or nurse), was able to increase the odds of influenza vaccination among HCW by 3.51 (95% CI 2.03-6.09) compared to the control group [42]. Our study also provides supportive evidence that increasing knowledge of influenza disease and vaccine may help to reduce hesitancy to a certain extent, particularly when combined with support from an influential senior HCW.
The social capital of senior HCWs (i.e., the capital derived from one’s social position and status) may explain why the vaccine-hesitant HCWs were more likely to be older than 50 years in our study. Using Bourdieu’s concept of social capital [43], it can be hypothesized that when this group of experienced and senior HCWs becomes influenza vaccine-hesitant, they can exert their power to either resist (i.e., refuse) or negotiate (i.e., delay) taking vaccines. Hesitant HCWs of this group may have more options instead of being confined to the government vaccines and thus have more power to choose. In previous research, vaccine hesitancy was viewed as a form of symbolic capital that helped to understand and elaborate on the social processes, uncertainties, and difficulties in various vaccine-related journeys [44]. While in this study, the older HCW’s accrued social capital with the virtue of their seniority and social networks built in the hospital for many years may have provided them with more power to resist the vaccination policy and the approaches of junior vaccinators. The higher social standing of the older HCWs may be the reason why they could overtly display their hesitancy, while the younger HCWs may have had to keep it hidden. This hypothesis, however, needs to be further explored and corroborated by other studies.
Overall, this study contributes to the growing literature on vaccine hesitancy and presents the situation of HCWs in a rural northeastern province in Thailand. This study has been reported here in accordance with the STROBE statement on cross-sectional studies (Table A3). Nevertheless, there are some limitations in the study. First, the research was conducted after Thailand's first wave of coronavirus disease 2019 (COVID-19). This presented different logistic hurdles and time delays in conducting the survey. More importantly, the emergence of COVID-19 might have affected some HCWs’ influenza vaccine decision-making, which was not captured in the survey data as the questionnaire was designed in the pre-COVID period. Second, there may have been a potential selection bias as the data was collected exclusively in the daytime, and the HCWs working night shifts were unable to be included. Although stratified random sampling was used in the survey, which accounted for all staff working in the hospital and gave the HCW working at night time an equal probability to get enrolled, cross-sectional data collection in the daytime may have limited their participation. Finally, a small number of samples in some HCW categories reduced the statistical power of the survey to draw valid comparisons between the HCW types. Nonetheless, the survey provided a representative sample of HCWs of the province selected by a multistage cluster sampling using probability proportional to HCW size in the hospitals.
In conclusion, a high proportion of HCWs had some form of hesitancy towards influenza vaccines. The findings of this study can be used as a baseline to monitor the changes in the level of vaccine hesitancy of Thai HCWs in future studies. Public health strategies and interventions informed by the study findings may be more effective in reducing influenza vaccine hesitancy among Thai HCW.
Author Contributions
Conceptualization: MS PPS SCP PP; Data curation: MS KP SC; Formal analysis: MS SCP KP; Investigation: MS PPS SCP PP; Methodology: MS PPS SCP PP; Project administration: MS KP SC; Resources: KP PP; Supervision: PPS SCP PP; Validation: PPS SCP; Visualization: MS SCP PP; Writing – original draft: MS; Writing – review & editing: MS PPS SCP KP SC PP. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Mahidol University - Central Institutional Review Board (MU-CIRB) (Protocol number MU-CIRB 2020/138.1606, 16th July 2020). Permission for data collection was also received from the Provincial Chief Medical Officer, Nakhon Phanom Provincial Public Health Office (ref no. 78.02/ 06115).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from each participant before data collection to publish this paper.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
Acknowledgments
We are grateful to the HCWs who participated in the study and the focal points at the six hospitals who helped in conducting the survey.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A

Table A1.
HCW Influenza Vaccine Hesitancy Determinant Items (5 point Likert scale):.
| Determinants | Items |
|---|---|
| a) Contextual factors: | |
|
|
|
|
|
|
|
|
| b) Individual/group influences: | |
|
|
|
|
|
|
|
|
| c) Influenza vaccination-specific issues | |
|
|
|
|
|
|
|
|
Table A2.
Response rates from each of the study hospitals.
| Location | Expected respondents (N) | Respondents (n) |
Response rate (%) |
|---|---|---|---|
| Nakhon Phanom Hospital | 100 | 100 | 100.0 |
| That Phanom Hospital | 50 | 50 | 100.0 |
| Phonsawan Hospital | 50 | 50 | 100.0 |
| Plapak Hospital | 50 | 49 | 98.0 |
| Na Kae Hospital | 50 | 49 | 98.0 |
| Wang Yang Hospital | 50 | 40 | 80.0 |
| Overall | 350 | 338 | 96.6 |
Table A3.
STROBE Statement—Checklist of items that should be included in reports of cross-sectional studies.
Table A3.
STROBE Statement—Checklist of items that should be included in reports of cross-sectional studies.
| Item No | Recommendation | Page No |
|
|---|---|---|---|
| Title and abstract | 1 | (a) Indicate the study’s design with a commonly used term in the title or the abstract | 1 |
| (b) Provide in the abstract an informative and balanced summary of what was done and what was found | 1 | ||
| Introduction | |||
| Background/rationale | 2 | Explain the scientific background and rationale for the investigation being reported | 1-2 |
| Objectives | 3 | State specific objectives, including any prespecified hypotheses | 2 |
| Methods | |||
| Study design | 4 | Present key elements of study design early in the paper | 2 |
| Setting | 5 | Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | 2-3 |
| Participants | 6 | (a) Give the eligibility criteria, and the sources and methods of selection of participants | 3 |
| Variables | 7 | Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if applicable | 4 |
| Data sources/ measurement | 8* | For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of assessment methods if there is more than one group | 4 |
| Bias | 9 | Describe any efforts to address potential sources of bias | |
| Study size | 10 | Explain how the study size was arrived at | 3 |
| Quantitative variables | 11 | Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why | 3-4 |
| Statistical methods | 12 | (a) Describe all statistical methods, including those used to control for confounding | 4 |
| (b) Describe any methods used to examine subgroups and interactions | N/A | ||
| (c) Explain how missing data were addressed | N/A | ||
| (d) If applicable, describe analytical methods taking account of sampling strategy | 4 | ||
| (e) Describe any sensitivity analyses | N/A | ||
| Results | |||
| Participants | 13* | (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed | 5 |
| (b) Give reasons for non-participation at each stage | 5,9 | ||
| (c) Consider use of a flow diagram | 5 | ||
| Descriptive data | 14* | (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential confounders | 5-7 |
| (b) Indicate number of participants with missing data for each variable of interest | N/A | ||
| Outcome data | 15* | Report numbers of outcome events or summary measures | 8 |
| Main results | 16 | (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval). Make clear which confounders were adjusted for and why they were included | 9-13 |
| (b) Report category boundaries when continuous variables were categorized | 9 | ||
| (c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | N/A | ||
| Other analyses | 17 | Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses | N/A |
| Discussion | |||
| Key results | 18 | Summarise key results with reference to study objectives | 13 |
| Limitations | 19 | Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | 14 |
| Interpretation | 20 | Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | 13-14 |
| Generalisability | 21 | Discuss the generalisability (external validity) of the study results | 13-14 |
| Other information | |||
| Funding | 22 | Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | 15 |
*N/A: not applicable.
References
- Wilson, K.E.; Wood, S.M.; Schaecher, K.E.; Cromwell, K.B.; Godich, J.; Knapp, M.H.; et al. Nosocomial outbreak of influenza A H3N2 in an inpatient oncology unit related to health care workers presenting to work while ill. American Journal of Infection Control 2019, 47, 683–687. [Google Scholar] [CrossRef]
- Wilson, P.; Zumla, A. Transmission and prevention of acute viral respiratory tract infections in hospitals. Curr Opin Pulm Med. 2019, 25, 220–224. [Google Scholar] [CrossRef]
- Huzly, D.; Kurz, S.; Ebner, W.; Dettenkofer, M.; Panning, M. Characterisation of nosocomial and community-acquired influenza in a large university hospital during two consecutive influenza seasons. Journal of Clinical Virology 2015, 73, 47–51. [Google Scholar] [CrossRef]
- Fiore, A.E.; Shay, D.K.; Broder, K.; Iskander, J.K.; Uyeki, T.M.; Mootrey, G.; et al. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2009. MMWR Recommendations and reports: Morbidity and mortality weekly report Recommendations and reports / Centers for Disease Control. 2009.
- World Health Organization. Vaccines against influenza WHO position paper—November 2012. Wkly Epidemiol Rec. 2012, 87, 461–476. [Google Scholar]
- Black, C.L.; Yue, X.; Ball, S.W.; Fink, R.V.; de Perio, M.A.; Laney, A.S.; et al. Influenza Vaccination Coverage Among Health Care Personnel - United States, 2017–2018 Influenza Season. MMWR Morb Mortal Wkly Rep. 2018, 67, 1050–1054. [Google Scholar] [CrossRef]
- Health Canada. Vaccine uptake in Canadian adults: Results from the 2014 adult National Immunization Coverage (aNIC) survey; Government of Canada, 2016. [Google Scholar]
- To, K.W.; Lai, A.; Lee, K.C.K.; Koh, D.; Lee, S.S. Increasing the coverage of influenza vaccination in healthcare workers: review of challenges and solutions. Journal of Hospital Infection 2016, 94, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; et al. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef] [PubMed]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: a critical review. Social Science & Medicine 2014, 112, 1–11. [Google Scholar]
- Verger, P.; Fressard, L.; Collange, F.; Gautier, A.; Jestin, C.; Launay, O.; et al. Vaccine hesitancy among general practitioners and its determinants during controversies: a national cross-sectional survey in France. EBioMedicine 2015, 2, 891–897. [Google Scholar] [CrossRef]
- Dubé, E.; Vivion, M.; MacDonald, N.E. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement: influence, impact and implications. Expert Review of Vaccines. 2015, 14, 99–117. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten threats to global health in 2019; WHO, 2019. [Google Scholar]
- Kwon, D.S.; Kim, K.; Park, S.M. Factors associated with influenza vaccination coverage among the elderly in South Korea: the Fourth Korean National Health and Nutrition Examination Survey (KNHANES IV). BMJ Open 2016, 6, e012618. [Google Scholar] [CrossRef]
- Offeddu, V.; Tam, C.C.; Yong, T.T.; Tan, L.K.; Thoon, K.C.; Lee, N.; et al. Coverage and determinants of influenza vaccine among pregnant women: a cross-sectional study. BMC Public Health. 2019, 19, 890. [Google Scholar] [CrossRef]
- MacDonald, N.E.; Dubé, E. Unpacking Vaccine Hesitancy Among Healthcare Providers. EBioMedicine 2015, 2, 792–793. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef]
- Owusu, J.T.; Prapasiri, P.; Ditsungnoen, D.; Leetongin, G.; Yoocharoen, P.; Rattanayot, J.; et al. Seasonal influenza vaccine coverage among high-risk populations in Thailand, 2010–2012. Vaccine 2015, 33, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Chotpitayasunondh, T.; Sawanpanyalert, N.; Bumrungsak, R.; Chunthitiwong, P.; Chainatraporn, P. Influenza vaccination among health care workers in Thailand. BMC proceedings: Springer; 2011. p. 84.
- Chotpitayasunondh, C.; Patrasuwan, S.; Prontri, M.; Poiynok, S. Acceptance of pandemic influenza A (H1N1) 2009 vaccine among health care workers, Thailand. BMC proceedings: Springer; 2011. p. P83.
- Praphasiri, P.; Ditsungneon, D.; Greenbaum, A.; Dawood, F.S.; Yoocharoen, P.; Stone, D.M.; et al. Do Thai Physicians Recommend Seasonal Influenza Vaccines to Pregnant Women? A Cross-Sectional Survey of Physicians’ Perspectives and Practices in Thailand. PLOS ONE 2017, 12, e0169221. [Google Scholar]
- Tanavikrankoon, M.; Suwannapong, N.; Thipayamongkolkul, M.; Howteerakul, N. Acceptance of seasonal influenza vaccination among medical personnel in a super tertiary care hospital, Bangkok. Vajira Nursing Journal 2015, 17, 15–29. [Google Scholar]
- Goyal, S.; Prasert, K.; Praphasiri, P.; Chittaganpitch, M.; Waicharoen, S.; Ditsungnoen, D.; et al. The acceptability and validity of self-collected nasal swabs for detection of influenza virus infection among older adults in Thailand. Influenza and Other Respiratory Viruses 2017, 11, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Chittaganpitch, M.; Puthavathana, P.; Praphasiri, P.; Waicharoen, S.; Shrestha, M.; Mott, J.A.; et al. Antibody responses against influenza B lineages among community-dwelling individuals 65 years of age or older having received trivalent inactivated influenza vaccine during two consecutive seasons in Thailand. SouthEast Asian Journal of Tropical Medicine and Public Health 2019, 50, 500–513. [Google Scholar]
- Prasert, K.; Patumanond, J.; Praphasiri, P.; Siriluk, S.; Ditsungnoen, D.; Chittaganpich, M.; et al. Effectiveness of trivalent inactivated influenza vaccine among community-dwelling older adults in Thailand: A two-year prospective cohort study. Vaccine 2019, 37, 783–791. [Google Scholar] [CrossRef]
- Prapasiri, P.; Jareinpituk, S.; Keawpan, A.; Chuxnum, T.; Baggett, H.C.; Thamathitiwat, S.; et al. Epidemiology of radiographically-confirmed and bacteremic pneumonia in rural Thailand. The Southeast Asian journal of tropical medicine and public health 2008, 39, 706–718. [Google Scholar]
- Baggett, H.C.; Peruski, L.F.; Olsen, S.J.; Thamthitiwat, S.; Rhodes, J.; Dejsirilert, S.; et al. Incidence of Pneumococcal Bacteremia Requiring Hospitalization in Rural Thailand. Clinical Infectious Diseases 2009, 48, S65–S74. [Google Scholar] [CrossRef] [PubMed]
- Jordan, H.T.; Prapasiri, P.; Areerat, P.; Anand, S.; Clague, B.; Sutthirattana, S.; et al. A comparison of population-based pneumonia surveillance and health-seeking behavior in two provinces in rural Thailand. International Journal of Infectious Diseases 2009, 13, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Dal Poz, M.R.; Kinfu, Y.; Dräger, S.; Kunjumen, T.; Diallo, K. Counting health workers: definitions, data, methods and global results; World Health Organization: Geneva, 2006. [Google Scholar]
- World Health Organization. Health workers: a global profile. Working together for health: the World health report 2006. 2006.
- Larson, H.J.; Jarrett, C.; Schulz, W.S.; Chaudhuri, M.; Zhou, Y.; Dube, E.; et al. Measuring vaccine hesitancy: the development of a survey tool. Vaccine 2015, 33, 4165–4175. [Google Scholar] [CrossRef] [PubMed]
- Hussein, Y.H.; Ibrahim, M.H.; Badran, S.G.; Eldeeb, S.M. Hesitancy for influenza vaccine among healthcare workers and mothers of preschool children: A cross-sectional study in Zagazig, Egypt. Journal of Family and Community Medicine 2022, 29, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. International journal of nursing studies 2021, 114, 103854. [Google Scholar] [CrossRef] [PubMed]
- Alobwede, S.M.; Kidzeru, E.B.; Katoto, P.D.M.C.; et al. Influenza Vaccination Uptake and Hesitancy among Healthcare Workers in Early 2021 at the Start of the COVID-19 Vaccine Rollout in Cape Town, South Africa. Vaccines (Basel) 2022, 10, 1176. [Google Scholar] [CrossRef] [PubMed]
- Sibanda, M.; Meyer, J.C.; Godman, B.; Burnett, R.J. Low influenza vaccine uptake by healthcare workers caring for the elderly in South African old age homes and primary healthcare facilities. BMC Public Health 2023, 23, 91. [Google Scholar] [CrossRef] [PubMed]
- Lipworth, W.; Little, M.; Markham, P.; Gordon, J.; Kerridge, I. Doctors on Status and Respect: A Qualitative Study. Journal of Bioethical Inquiry 2013, 10, 205–217. [Google Scholar] [CrossRef]
- Strömgren, M.; Eriksson, A.; Ahlstrom, L.; Bergman, D.K.; Dellve, L. Leadership quality: a factor important for social capital in healthcare organizations. Journal of Health Organization and Management 2017, 31, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Corace, K.; Prematunge, C.; McCarthy, A.; Nair, R.C.; Roth, V.; Hayes, T.; et al. Predicting influenza vaccination uptake among health care workers: what are the key motivators? Am J Infect Control 2013, 41, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Llupià, A.; García-Basteiro, A.L.; Olivé, V.; Costas, L.; Ríos, J.; Quesada, S.; et al. New interventions to increase influenza vaccination rates in health care workers. American Journal of Infection Control 2010, 38, 476–481. [Google Scholar] [CrossRef] [PubMed]
- Slaunwhite, J.M.; Smith, S.M.; Fleming, M.T.; Strang, R.; Lockhart, C. Increasing vaccination rates among health care workers using unit "champions" as a motivator. Can J Infect Control 2009, 24, 159–164. [Google Scholar]
- Abramson, Z.H.; Avni, O.; Levi, O.; Miskin, I.N. Randomized Trial of a Program to Increase Staff Influenza Vaccination in Primary Care Clinics. The Annals of Family Medicine 2010, 8, 293–298. [Google Scholar] [CrossRef]
- Bourdieu, P. Distinction: A Social Critique of the Judgement of Taste 1984.
- Attwell, K.; Meyer, S.B.; Ward, P.R. The Social Basis of Vaccine Questioning and Refusal: A Qualitative Study Employing Bourdieu's Concepts of 'Capitals' and 'Habitus'. International journal of environmental research and public health 2018, 15, 1044. [Google Scholar] [CrossRef]
Figure 1.
Study flow and influenza vaccine hesitancy among healthcare workers in Nakhon Phanom Province, Thailand.
Figure 1.
Study flow and influenza vaccine hesitancy among healthcare workers in Nakhon Phanom Province, Thailand.
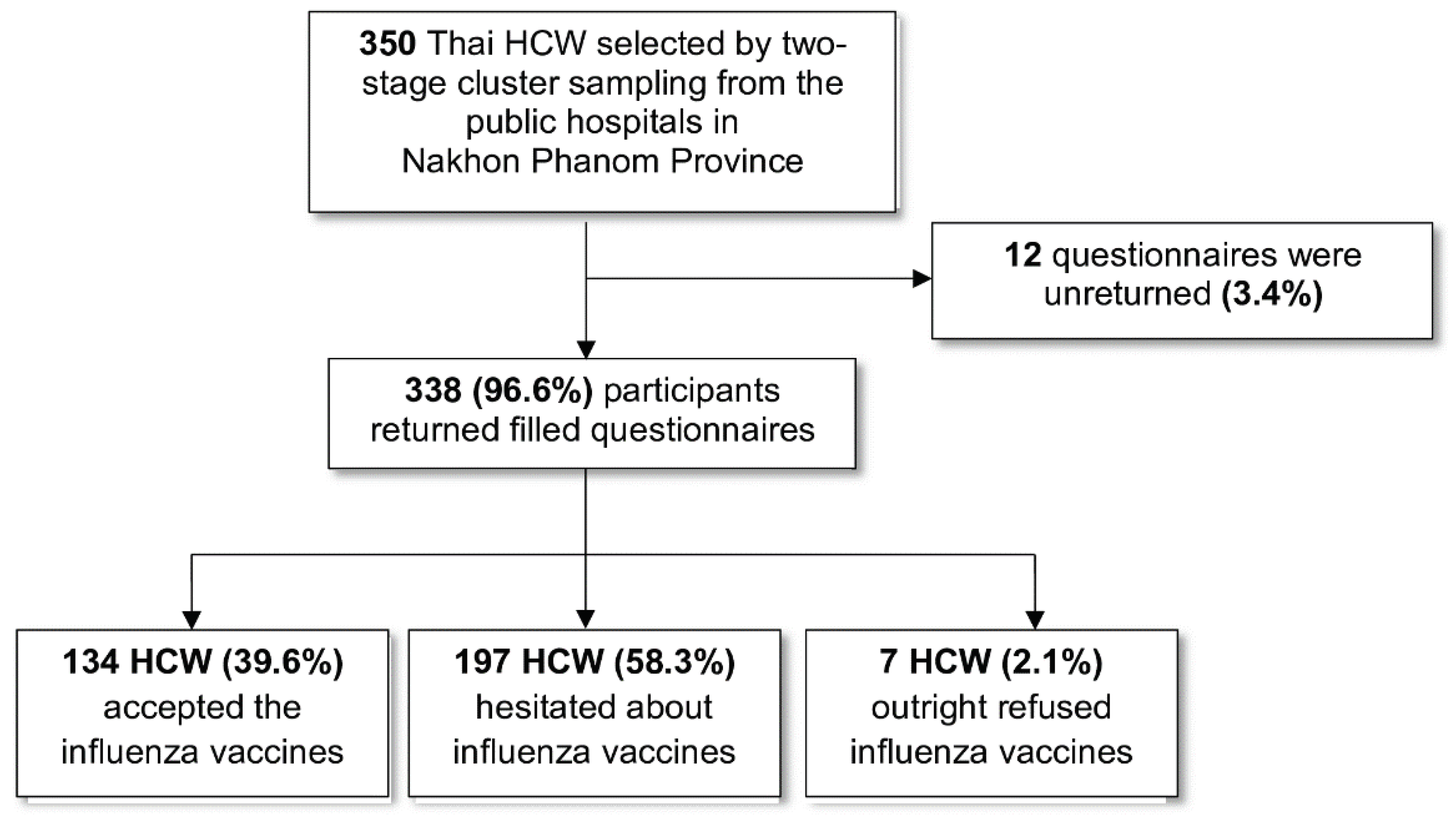
Figure 2.
Types of hesitant HCW among the participants.
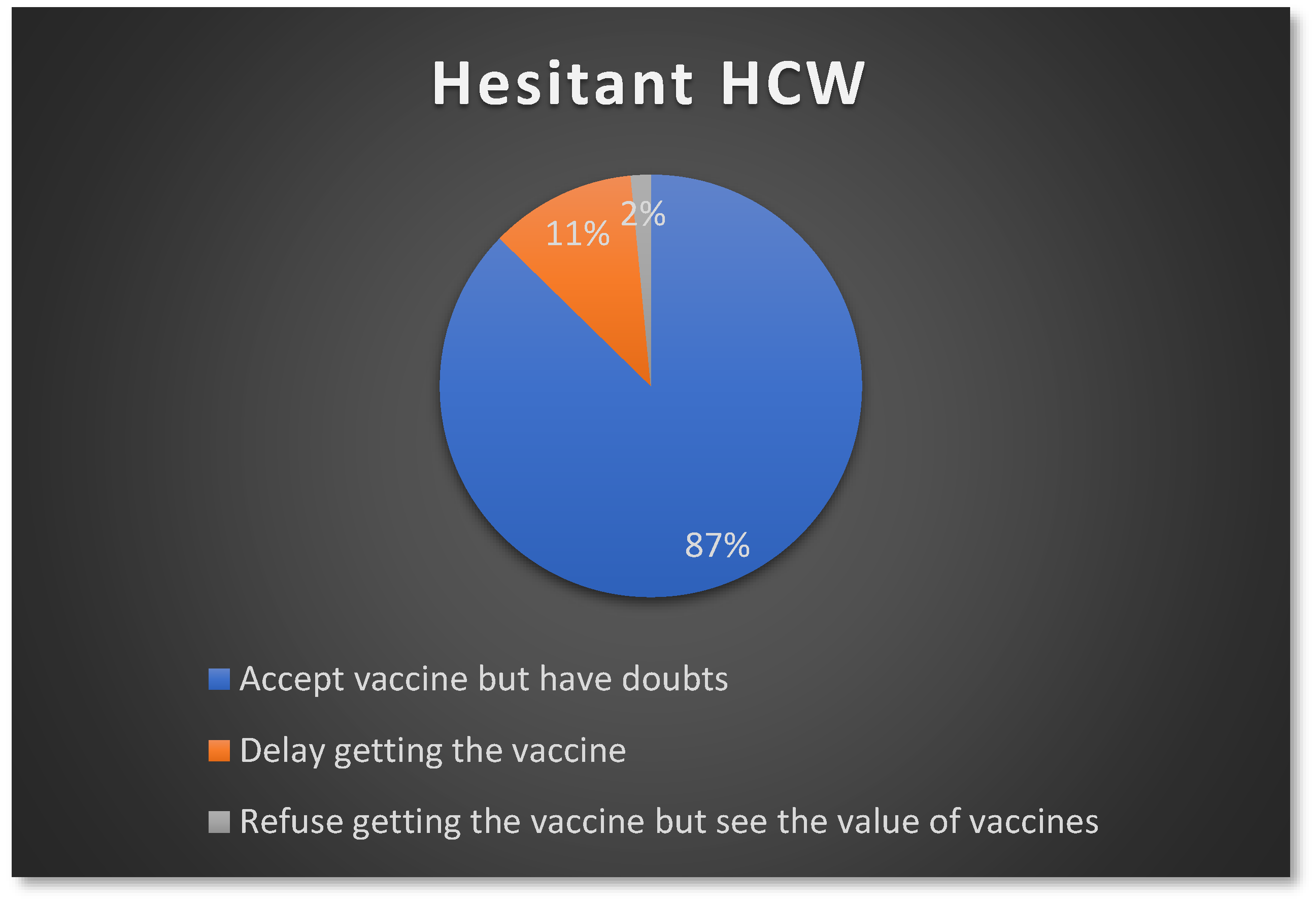
Figure 3.
Influenza vaccine hesitancy levels among different HCW types.
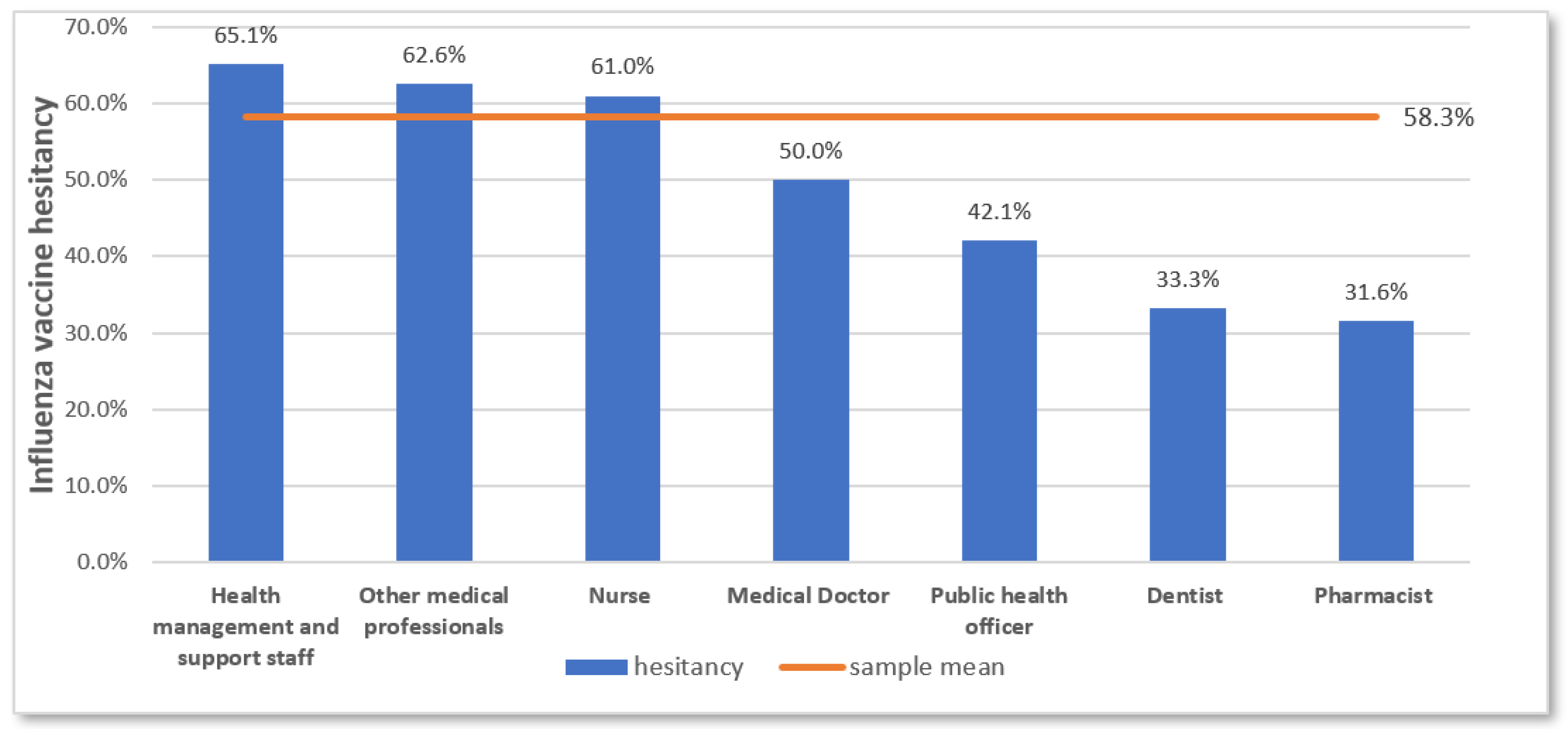
Table 1.
Participant characteristics (n=338).
| Characteristic | Number | Percentage |
|---|---|---|
| Age group | ||
| ≤30 years | 102 | 30.2 |
| 31-40 years | 121 | 35.8 |
| 41-50 years | 72 | 21.3 |
| >50 years | 43 | 12.7 |
| Mean (SD): 37.2 years (9.7); Min: 20, Max: 60 | ||
| Sex | ||
| Female | 280 | 82.8 |
| Male | 58 | 17.2 |
| Religion | ||
| Buddhism | 333 | 98.5 |
| Christianity | 5 | 1.5 |
| Level of hospital | ||
| Provincial | 100 | 29.6 |
| District | 238 | 70.4 |
| HCW type | ||
| Health service providers | 295 | 87.3 |
| Nurse | 136 | 40.2 |
| Pharmacist | 19 | 5.6 |
| Public health officer | 19 | 5.6 |
| Medical doctor | 16 | 4.7 |
| Dentist | 6 | 1.8 |
| Other medical personnel | 99 | 29.3 |
| Hospital assistant staff | 55 | 16.3 |
| Patient assistants | 27 | 8.0 |
| Emergency medical technicians (EMT)/paramedic | 7 | 2.1 |
| Laboratory staff | 7 | 2.1 |
| Nurse aids | 3 | 0.9 |
| Health management and support staff | 43 | 12.7 |
| Average daily exposure with patients | ||
| High (<1 meter) | 172 | 50.9 |
| Moderate (1 meter or more) | 106 | 31.4 |
| Low (no direct patient contact) | 60 | 17.8 |
| Work experience as HCW | ||
| ≤5 years | 74 | 21.9 |
| >5 years to <20 years | 166 | 49.1 |
| ≥20 years | 98 | 29.0 |
| Mean (SD): 13.8 years (9.8); Min:1, Max: 37 | ||
| Highest educational attainment | ||
| High school or below | 36 | 10.7 |
| Diploma or vocational college | 43 | 12.7 |
| Bachelor’s degree | 223 | 65.9 |
| Master’s degree or higher | 36 | 10.7 |
| Pre-existing chronic medical condition | ||
| Yes | 74 | 21.9 |
| No | 264 | 78.1 |
Abbreviations: SD, Standard deviation; Min, Minimum; Max, Maximum.
Table 2.
Participants’ correct responses to each item of knowledge on influenza and vaccination (n=338).
Table 2.
Participants’ correct responses to each item of knowledge on influenza and vaccination (n=338).
| Knowledge items | Correct response | Number | % |
|---|---|---|---|
|
True | 302 | 89.3 |
|
True | 273 | 80.8 |
|
True | 240 | 71.0 |
|
False | 219 | 64.8 |
|
True | 176 | 52.1 |
|
True | 140 | 41.4 |
|
False | 102 | 30.2 |
| Overall knowledge categories | |||
| Need improvement (Overall score <60%) | 0-3 | 104 | 30.8 |
| Fair (Overall score 60-79%) | 4-5 | 149 | 44.1 |
| Good (Overall score ≥80%) | 6-7 | 85 | 25.1 |
Table 3.
Influenza vaccine hesitancy determinants aggregated mean scores (n=331).
| Determinant | Total Mean (SD) |
Influenza vaccine hesitancy | p-value* | |||
|---|---|---|---|---|---|---|
| Yes (n=197) | No (n=134) | |||||
| Mean | SD | Mean | SD | |||
| Contextual factors | ||||||
| Negative influence of media/ social media | 2.7 (0.8) | 2.6 | 0.8 | 2.8 | 0.9 | 0.154 |
| Negative perception of politics/policies | 1.9 (0.9) | 1.9 | 0.8 | 1.8 | 0.9 | 0.057 |
| Negative perception of pharmaceutical industry | 2.8 (1.0) | 2.8 | 0.9 | 2.7 | 1.1 | 0.435 |
| Lack of trust in health system | 2.5 (1.0) | 2.7 | 0.7 | 2.3 | 1.1 | 0.008 |
| Individual/Group influences | ||||||
| Negative past experience of vaccination | 2.3 (1.1) | 2.4 | 1.1 | 2.1 | 1.0 | 0.017 |
| Negative beliefs, attitudes about influenza and vaccination | 2.2 (0.9) | 2.2 | 0.8 | 2.1 | 1.0 | 0.614 |
| Negative perception of vaccination as a social norm | 2.2 (0.9) | 2.3 | 0.8 | 2.0 | 0.9 | 0.011 |
| Negative influence of other HCW | 2.0 (1.0) | 2.2 | 0.9 | 1.9 | 1.0 | 0.006 |
| Influenza vaccine specific factors | ||||||
| Perceived risk of influenza infection and lack of benefit of vaccination | 2.2 (0.7) | 2.4 | 0.6 | 2.1 | 0.7 | 0.001 |
| Risk of adverse events due to vaccination | 2.5 (0.9) | 2.7 | 0.9 | 2.3 | 1.0 | 0.001 |
| Fear of painful injections | 2.4 (0.7) | 2.5 | 0.8 | 2.2 | 0.8 | 0.007 |
| Access to vaccines in the hospital | 2.4 (0.7) | 2.5 | 0.7 | 2.2 | 0.7 | <0.001 |
Abbreviations: SD, Standard deviation; Min, Minimum; Max, Maximum. *p-value obtained from independent t-test.
Table 4.
Factors associated with vaccine hesitancy among HCW (n=331).
| Factor | Influenza vaccine hesitancy | Crude OR | 95% CI | Adjusted ORa | 95% CI | |
|---|---|---|---|---|---|---|
| Yes (n=197) | No (n=134) | |||||
| n (%) | n (%) | |||||
| Age-groups (in years) | ||||||
| ≤30 | 55 (53.9) | 47 (46.1) | Ref | Ref | ||
| 31-40 | 65 (55.1) | 53 (44.9) | 1.0 | 0.6-1.8 | 1.1 | 0.6-2.1 |
| 41–50 | 44 (64.7) | 24 (35.3) | 1.6 | 0.8-2.9 | 1.9 | 0.9-4.1 |
| >50 | 33 (76.7) | 10 (23.3) | 2.8 | 1.2-6.3* | 3.2 | 1.3-8.5* |
| Sex | ||||||
| Male | 34 (59.6) | 23 (40.4) | Ref | |||
| Female | 163 (59.5) | 111 (40.5) | 0.9 | 0.6-1.8 | ||
| Level of hospital | ||||||
| Provincial | 54 (55.7) | 43 (44.3) | Ref | |||
| District | 143 (61.1) | 91 (38.9) | 1.2 | 0.8-2.0 | ||
| HCW type | ||||||
| Health service providers | 169 (58.3) | 121 (41.7) | 0.6 | 0.3-1.3 | ||
| Health management and support staff | 28 (68.3) | 13 (31.7) | Ref | |||
| Average daily patient exposure | ||||||
| High | 96 (56.8) | 73 (43.2) | 0.8 | 0.4-1.5 | ||
| Moderate | 65 (63.1) | 38 (36.9) | 1.1 | 0.6-2.1 | ||
| Low | 36 (61.0) | 23 (39.0) | Ref | |||
| Work experience | ||||||
| ≤5 years | 37 (50.0) | 37 (50.0) | Ref | |||
| >5 years to <20 years | 95 (58.3) | 68 (41.7) | 1.4 | 0.8-2.4 | ||
| ≥20 years | 65 (69.1) | 29 (30.9) | 2.2 | 1.2-4.2* | ||
| Highest educational attainment | ||||||
| High school or below | 25 (69.4) | 11 (30.6) | Ref | |||
| Diploma/ vocational college | 31 (72.1) | 12 (27.9) | 1.1 | 0.4-3.0 | ||
| Bachelor’s degree | 122 (56.2) | 95 (43.8) | 0.6 | 0.3-1.2 | ||
| Master’s degree or higher | 19 (54.3) | 16 (45.7) | 0.5 | 0.2-1.4 | ||
| Pre-existing chronic condition | ||||||
| Yes | 44 (60.3) | 29 (29.7) | 1.0 | 0.6-1.8 | ||
| No | 153 (59.3) | 105 (40.7) | Ref | |||
| Knowledge of influenza and vaccination | ||||||
| Need improvement | 71 (69.6) | 31 (30.4) | Ref | Ref | ||
| Fair | 74 (51.4) | 70 (48.6) | 0.5 | 0.3-0.8* | 0.4 | 0.2-0.8* |
| Good | 52 (61.2) | 33 (38.8) | 0.7 | 0.4-1.3 | 0.9 | 0.5-2.0 |
| Contextual factors | ||||||
| Negative influence of media/ social media | ||||||
| High | 41 (57.7) | 30 (42.3) | 0.7 | 0.4-1.4 | ||
| Moderate | 93 (57.1) | 70 (42.9) | 0.7 | 0.4-1.2 | ||
| Low | 63 (64.9) | 34 (35.1) | Ref | |||
| Negative perception of politics/policies | ||||||
| High | 76 (69.1) | 34 (30.9) | 2.6 | 1.5-4.7* | 1.8 | 0.8-4.0 |
| Moderate | 78 (61.4) | 49 (38.6) | 1.9 | 1.1-3.2* | 1.2 | 0.6-2.3 |
| Low | 43 (45.7) | 51 (54.3) | Ref | Ref | ||
| Negative perception of pharmaceutical industry | ||||||
| High | 58 (65.9) | 30 (34.1) | 1.6 | 0.9-2.9 | ||
| Moderate | 89 (58.6) | 63 (41.4) | 1.1 | 0.7-1.9 | ||
| Low | 50 (54.9) | 41 (45.1) | Ref | |||
| Lack of trust in health system | ||||||
| High | 52 (69.3) | 23 (30.7) | 2.6 | 1.3-4.9* | 1.3 | 0.5-3.5 |
| Moderate | 106 (61.3) | 67 (38.7) | 1.8 | 1.1-3.0* | 1.2 | 0.6-2.4 |
| Low | 39 (47.0) | 44 (53.0) | Ref | Ref | ||
| Individual/group factors | ||||||
| Negative past experience of vaccination | ||||||
| High | 65 (67.0) | 32 (33.0) | 2.1 | 1.2-3.7* | 1.4 | 0.6-3.2 |
| Moderate | 80 (62.5) | 48 (37.5) | 1.7 | 1.0-2.9* | 1.2 | 0.6-2.5 |
| Low | 52 (49.1) | 54 (50.9) | Ref | Ref | ||
| Negative beliefs, attitudes about influenza and vaccination | ||||||
| High | 62 (59.0) | 43 (41.0) | 1.4 | 0.8-2.5 | 0.7 | 0.3-1.5 |
| Moderate | 86 (67.2) | 42 (32.8) | 2.0 | 1.2-3.5* | 1.4 | 0.7-2.7 |
| Low | 49 (50.0) | 49 (50.0) | Ref | Ref | ||
| Negative perception of vaccination as a social norm | ||||||
| High | 78 (68.4) | 36 (31.6) | 2.2 | 1.3-3.9* | 0.9 | 0.4-2.3 |
| Moderate | 70 (59.3) | 48 (40.7) | 1.5 | 0.9-2.5 | 1.1 | 0.5-2.2 |
| Low | 49 (49.5) | 50 (50.5) | Ref | Ref | ||
| Negative influence of other HCW | ||||||
| High | 92 (70.2) | 39 (29.8) | 3.3 | 1.9-5.7* | 2.3 | 1.1-4.8* |
| Moderate | 60 (65.9) | 31 (34.1) | 2.7 | 1.5-4.9* | 2.1 | 1.1-4.4* |
| Low | 45 (41.3) | 64 (58.7) | Ref | Ref | ||
| Influenza vaccination specific factors | ||||||
| Perceived risk of influenza infection and lack of benefit of vaccination | ||||||
| Low | 73 (68.2) | 34 (31.8) | 2.5 | 1.4-4.5* | 1.0 | 0.4-2.5 |
| Moderate | 82 (61.7) | 51 (38.3) | 1.9 | 1.1-3.2* | 0.9 | 0.4-1.8 |
| High | 42 (46.2) | 49 (53.8) | Ref | Ref | ||
| Risk of adverse events due to vaccination | ||||||
| High | 55 (73.3) | 20 (26.7) | 2.8 | 1.5-5.3* | 1.6 | 0.6-4.1 |
| Moderate | 84 (60.9) | 54 (39.1) | 1.6 | 0.9-2.6 | 0.9 | 0.5-1.9 |
| Low | 58 (49.2) | 60 (50.8) | Ref | Ref | ||
| Fear of painful injections | ||||||
| High | 104 (63.8) | 59 (36.2) | 1.7 | 1.1-2.7* | 0.9 | 0.5-1.6 |
| Moderate | 28 (70.0) | 12 (30.0) | 2.3 | 1.0-4.8* | 1.8 | 0.7-4.5 |
| Low | 65 (50.8) | 63 (49.2) | Ref | Ref | ||
| Access to vaccines in the hospital | ||||||
| Low | 64 (66.0) | 33 (34.0) | 2.0 | 1.2-3.5* | 1.3 | 0.6-2.8 |
| Moderate | 71 (66.4) | 36 (33.6) | 2.1 | 1.2-3.5* | 1.4 | 0.7-2.8 |
| High | 62 (48.8) | 65 (51.2) | Ref | Ref | ||
Abbreviations: OR, Odds Ratio; CI, Confidence Interval. aAdjusted OR and 95% CI, and p-values calculated using multivariable logistic regression, controlling for hospital locations to account for clustering.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



