
Submitted:
15 March 2024
Posted:
18 March 2024
You are already at the latest version
Abstract
Background/Objectives: Patients with rheumatoid arthritis (RA) have an increased risk of infections. The risk of presenting herpes zoster (HZ) is 1.5-2 times higher than in immunocompetent individuals and disseminated presentation is more frequent. Our aim was to analyze the prevalence and general features of HZ in RA patients. Methods: Prospective study of 392 RA patients included in the vaccination program of our hospital between 2011 and 2016, and followed-up until December 2020. Diagnosis of HZ was made according to clinical manifestations: skin rash, blisters, paresthesia and local pain in one or more dermatomes. Results: We studied 392(309women/83men), mean age 59±13years. Every patient was followed-up during a mean period of 137±110 months (range: 42months- 42years). HZ infection was observed in 30 of 392 (25women/5men) patients; age (mean±SD) 64.7±11.8years. Prevalence was 7.65% in this period and incidence rate was 13.22/1000patients/year. Three patients had facial involvement, one with optic involvement and one patient presented a disseminated HZ. Seven patients presented postherpetic neuralgia treated with gabapentinoids. The main features of RA of these 30 patients were: positive RF(n=17; 56.6%), positive anti-CCP(13; 43.3%) and erosive disease(10; 33.3%). At HZ infection they were in treatment with glucocorticoids (19; 63.3%), conventional DMARDs (15; 50%), biological DMARDs (15; 50%), tofacitinib (2; 6.6%) and upadacitinib (1; 3.3%). Conclusions: HZ is a relative frequent viral complication of RA patients. In our series, one patient presented a disseminated HZ and nearly 25% of patients had post-herpetic neuralgia. Include HZ vaccine in our vaccination program in RA patients may be beneficial.
Keywords:
Rheumatoid arthritis
; Herpes zoster
; Infection
; Biological therapy
1. Introduction
Rheumatoid arthritis (RA) carries an increased risk of infections [1,2]. This increased risk of infections is associated with the immune dysregulation due to the disease itself and the immunomodulation drugs used to treat the disease. Furthermore, there are other risk factors such as age, comorbidity and concomitant treatments [3,4,5,6].
Varicella zoster virus (VZV) may produce two different diseases. The primary infection that usually appears in childhood is varicella or chickenpox, and it is characterized by skin rash and small pruriginous blisters in chest, back and face which subsequently extend [7,8,9] Second, herpes zoster (HZ) or shingles, which is caused by the reactivation of latent infection from the virus. In fact, anyone that had suffered from varicella could develop HZ [10]. After the first infection, viral particles of VZV settle in cranial and dorsal root ganglia and cell-mediated immunity is created by specific antibodies and CD4+ T cells [11]
HZ presents with dysesthesia in the sensory region for the affected ganglia, followed by skin rash and blisters. In 2-3 days, blisters ulcerate and form scabs that may last for months. After the acute phase, neuropathic pain may remain for weeks and months causing post-herpetic neuralgia (PHN) in 20%-30% of patients that represents an important morbidity requiring pharmacological treatment in most cases [12,13]
Diagnosis of HZ is usually clinical but can be confirmed by the demonstration of VZV-DNA by PCR in a sample of the blisters contents [14]. HZ infection have been associated with many triggers. Between them, we find intercurrent acute illnesses, malignancy, emotional stress and use of some type of medication such as immunosuppressive agents, particularly glucocorticoids (GC) and methotrexate (MTX) [15,16,17,18].
In general population, the incidence of VZV reactivation is 3-5/1000 patients-year, being a similar incidence in US, Europe and Asia [19]. This risk is increased in aged people (6-8/1000/year in people over 60 years and 8-12/1000/years in individuals older than 80 years), mainly due to decline of the cell mediated-immunity related to age [20,21]
After 85 years, the risk of developing HZ is near to 50% and sequelae are much more common. The same occurs in immunocompromised patients as those ones with bone narrow or solid organ transplantation, lymphoproliferative diseases, leukemia and human immunodeficiency virus (HIV) infection. In the same group of risk are patients with rheumatic or systemic autoimmune diseases [19,22]. In fact, RA patients have 1.5 to 2 times higher risk of presenting HZ than immunocompetent individuals. Furthermore, disseminated forms and post-herpetic sequelae are much more likely in these patients [23]
Taking into account all these considerations, the aim of this study was to assess the incidence and clinical characteristics of HZ in a group of RA patients followed in a single University hospital and to established the risk factors to develop this virus reactivation, and then, to establish the need to include the HZ vaccine in the vaccination programs of our health system.
2. Materials and Methods
Design and Enrollment Criteria
We performed a prospective study of patients diagnosed with RA from a single hospital (Marqués de Valdecilla University Hospital, Santander, Spain) that were consecutively included in the vaccination program of our hospital over a 5-year-period (from October 2011 to October 2016). These patients were later followed-up until December 2020. RA was diagnosed according to EULAR/ACR 2010 criteria [24]. Patients diagnosed before 2010 were reevaluated and the diagnosis was confirmed with these criteria.
HZ was diagnosed according to cutaneous manifestations of skin rash and blisters, and the occurrence of neuropathic pain in one (localized) or several (disseminated) dermatomes was recorded. The presence of cutaneous manifestations was evaluated with an exhaustive physical exploration performed by a rheumatologist or a general physician. In all doubtful cases, they were also assessed by a dermatologist. Sequelae were also checked out in all these patients [14,25]
Outcome Variables
Outcome variables were recorded at baseline and at the moment of HZ infection. General variables included age, sex, time of evolution of RA and administered therapies
The main outcome variables of RA were related to the severity of the disease. Clinical manifestations were: presence of erosions and extra-articular manifestations such as rheumatoid nodules, associated interstitial lung disease, Sjögren´s syndrome and rheumatoid vasculitis. Laboratory findings included positivity for rheumatoid factor (RF) and anti-citrullinated cyclic peptide antibodies (anti-CCP)
Treatment with prednisone, conventional synthetic(cs) disease-modifying antirheumatic drugs (DMARDs), biological DMARDs and JAK inhibitors (JAKinh) prior and at the moment of the shingles occurrence was recorded and later analyzed
Associated comorbidities in these patients were also collected and analyzed to find risk factors. These comorbidities included hypertension, hypercholesterolemia, diabetes mellitus and active smoking. Many triggers have been reported in patients with HZ. The most commonly referred are emotional stress, use of medications (immunosuppressive drugs), intercurrentacute or chronic illnesses and presence of malignancy [15]. All of them were searched in our patients.
Localization of HZ was described by the rheumatologist, general physician or dermatologist in every case. Adequate response to antiviral treatment was evaluated in the two weeks following the diagnosis of HZ. Presence of sequelae, such as PHN or visual alterations in case of facial involvement, and the need of neuropathic pain killers were recorded in this period and followed-up until symptoms disappeared.
We also calculated the prevalence and incidence rate of HZ in our cohort.
Data Collection
Data of patients were collected from the clinical records of our hospital and from the informatics programs of General Practitioners. These data included clinical and laboratory data, diagnosis and pharmacological agents used in the management of RA. Manifestations of HZ, localization, antiviral treatment used and sequelae were also registered. Data were reviewed to confirm the diagnosis and then stored in a computerized data file.
Statistical Analysis
Results are expressed as mean ± standard deviation (SD) for variables with normal distribution, or as median and interquartile range [IQR] [25th, 75th] for those not normally distributed. To compare continuous variables, the Wilcoxon signed-rank test was used. For the analysis of dichotomous variables, the chi-square test or the Fisher exact test were used. To check for risk factors of HZ, a Cox regression analysis was performed. Statistical analysis was performed using the SPSS software (IBM, NY,USA). A p-value <0.05 was considered as statistically significant.
3. Results
We studied 392 RA patients that were included consecutively in the vaccination program of the Preventive Medicine department of our hospital since October 2011 to October 2016. The mean follow-up was 11 years. None of included patients had previously received the vaccination for HZ.
Demographic and Clinical Features of the Participants
Demographic and disease-related characteristics of the participants are shown in Table 1. The mean age was 59±13years and 79% were female. Current smoking, hypertension, dyslipidemia and diabetes mellitus were present in 40%, 42%, 38% and 14% of patients, respectively. Positivity for RF and anti-CCP was 57% and 53%, respectively. 145 patients (37%) presented an erosive disease. The most important extra-articular manifestations were subcutaneous nodules (6%), interstitial lung disease (5%), Sjögren´s syndrome (5%) and rheumatoid vasculitis (6%).
Thirty patients (25 women/5 men) developed HZ during follow-up. Mean age of patients at the moment of HZ was 64.7±11.8years. The mean follow-up was 45 months, with a minimum period of 4 months and a maximum of 7 years. Main demographic and clinical data and treatment of these 30 patients at the moment of HZ infection are shown in Table 2.
In the group with HZ, most of the patients presented important comorbidities such as high blood pressure (60%), dyslipidemia (47%) and diabetes mellitus (20%). Eleven patients were active smokers.
Half of HZ patients were found to be positive for RF (57%) or anti-CCP (43%), and almost the half had an erosive RA (33%). Regarding to extra-articular manifestations, three patients presented interstitial lung disease (10%), one patient associated with Sjögren´s syndrome (3%) and two patients with rheumatoid vasculitis (7%). One patient presented rheumatoid nodules (3%).
Comparison between the main clinical characteristics and RA treatments of both groups, non-HZ and HZ patients, at baseline visit, are shown in Table 1.
There were not differences neither in age, time of evolution of RA or sex, nor in active smoking, dyslipidemia and diabetes mellitus. Hypertension was statistically more common in patients with HZ in our RA cohort (p=0.039). RA-related features (RF, anti-CCP, presence of erosions, associated lung disease, Sjögren´s syndrome, rheumatoid nodules and rheumatoid vasculitis) had not shown differences at baseline.
Therapies Administered at Baseline
A comparison of RA treatment was also made. More than half of the patients of our cohort were receiving treatment with GC at baseline with a mean prednisone-equivalent dose of 3.75 (0-7.5)mg/day in the group of HZ versus 5 (0-5) in the other group, with no significant differences. Conventional synthetic DMARDs were the drugs more frequently used in both groups, preferably MTX, leflunomide, sulfasalazine and azathioprine, with no statistical differences between both groups. Likewise, there were no differences in baseline treatment with bDAMRDs in both groups. In contrast, the number of TNF inhibitors used in HZ group was higher than in the non-HZ group (p=0.014), specially with etanercept (p=0.033), and the time of exposition to rituximab was also higher (p<0.05).
Herpes Zoster Infection Characteristic
HZ infection characteristics are collected in Table 3. The main locations for HZ were in the trunk [intercostal (n=6), dorsal (n=4), lumbar (n=3), abdominal (n=3), intermammary fold (n=1) and submmamary fold (n=1)], followed by head and neck [cervical (n=1), ophthalmic (n=1), facial (n=1), and trigeminal (n=1)], and extremities [left upper extremity (n=1) and gluteus (n=1)]. One patient presented a disseminated form of HZ involving 3 different zones of the body. We did not identify the location of HZ in 5 patients. PHN, as the principal sequelae, was found in seven patients. Neuropathic pain killers and gabapentinoids such as pregabalin or gabapentin were needed during several months in these patients. One of them also presented cutaneous sequelae as we can see in Figure 1.
The patient with ophtalmic involvement suffered from visual loss for a week with a later complete resolution after that time.
HZ was treated only with topical treatment in 2 patients and 5 were not treated due to a late diagnose. Two patients received both, topical and systemic antiviral agents and twenty one patients received only systemic treatment. The main antiviral drugs used were brivudine and famciclovir, both of them in 7 patients. The other treatments were acyclovir (n=6) and valaciclovir (n=3).
Interestingly, we have not identified any trigger for the HZ development in our patients and, remarkably, no patient reported a primary infection for VZV.
RA Treatment in HZ Infection
Concerning to RA treatment, more than the half of patients (63.3%) were taking GCat the time of VZV reactivation and the mean dose was 7.5 (5-10)mg/day.
Almost every patient was under treatment with conventional synthetic(n=9), biological (n=10) DMARDs or JAK inhibitors either in monotherapy (n=2) or in combination (n=7). One patient was receiving only GC and another was not receiving any treatment for RA at that moment.
The csDMARDs used were: MTX (n=11), leflunomide (n=3), sulfasalazine (n=1) and azathioprine (n=1). One patient was taken leflunomide and MTX in combination.
Eight patients were receiving TNF-α antagonists, 4 in combination with a csDMARDs. Etanercept (ETN) (n=4) was the most common drug used, being given at the standard dose. Adalimumab (ADA) (n=1) was used at the standard dose too. Golimumab (GLM) (n=2) was used at the standard dose in one patient and optimized in the other patient (50 mg subcutaneously every45 days). Certolizumab pegol was used in a single patient at the standard dose.
In the remaining patients under bDMARDs, the non-TNFα drugs used were: tocilizumab (n=3), abatacept (n=3), sarilumab (n=1), and JAK inhibitors in 3 patients (tofacitinib in 2 cases and upadacitinib in other one). Every one of these drugs were administrated at the standard dose.
Multivariate Analysis
Cox regression revealed that hypertension was the only comorbidity associated with VZV reactivation [Hazard Ratio (HR) 2.25; 95%CI: 1.09-4.68; p=0.029]. Regarding to RA treatment, only exposition to etanercept showed a relation with HZ infection in our patients (HR 2.04, 95%CI:0.99-4.18; p=0.05).
In Table 4 are summarized the proposed predictive factors of HZ development in our cohort of patients with RA.
4. Discussion
In this study, we present 30 cases of HZ in a series of 392 patients with RA included in the vaccination program of our hospital in a 5-year period.
HZ or shingles is the result of the reactivation of VZV that rest latent in cranial and dorsal root ganglia after the primary infection normally in childhood [7,8,9,10,11,12,13,14,15,16,17,18,19]
HZ is a relatively frequent infection in general population, 3-5/1000patients/year, and the estimate incidence in immunocompromised people, as RA patients, is 1.5-2 times higher1, 2. The incidence rate for HZ in our RA cohort was 13.2 per 1000 patients-year, similar to other cohorts in classic publications and a little higher than most of them (Table 5).
Remarkably, not only the acute infection by HZ causes important morbidity, but also sequelae such as PHN, that is frequent in this type of patients. Disseminated variant of HZ affecting two or more dermatomes and internal organs is also more frequent in RA patients. Severe complications as skin rash bacterial super-infection or Ramsay-Hunt syndrome are more likely in immunocompromised patients and loss of vision, when ophthalmic involvement occurs, is alsopossible [17]. Recent reviews suggest that patients suffering from HZ could develop stroke in the weeks following the virus reactivation, especially in aged people [1,26]
As expected, the group of RA patients that developed HZ in our cohort was older (mean age 65 years) and the time of evolution of the RA was longer (mean duration 13 years).
Over the last few years, new treatments for RA and other immune-mediated inflammatory diseases, have increased the risk of reactivation of VZV as the population ages [2,4,20]
Several studies have demonstrated that high doses of GC are associated with increased risk of infections, especially opportunistic infections as reactivation of VZV [6,17,27]. In our series, more than half of the patients with HZ (63.3%) were under treatment with GC when shingles occurred, although the mean dose was relatively low [7.5 (5-10)mg/day].
The reason for the increased risk of HZ in patients treated with anti-TNF drugs is not clear. In 2007,Smitten et al founded a slightly elevated risk of HZ in patients treated with conventional and biological DMARDs, compared to RA patients with no therapy [2]. Two years later, one study in the US showed that the use of adalimumab or etanercept seemed to protect from the reactivation of VZV, and the risk with infliximab was significantly low [28]. Interestingly, in the RABBIT registry there were no consistent data. The incidence of HZ was similar in the monoclonal antibodies (adalimumab and infliximab), etanercept and non-biologic DMARD group but, in the multivariate analysis, the risk was significantly higher in patients treated with TNF-αantagonists [29]
In our HZ cohort, eight patients were under treatment with anti-TNFα at the moment of the virus reactivation, being etanercept the most frequently used (n=4), followed by golimumab (n=2), adalimumab (n=1) and certolizumab pegol (n=1). Furthermore, the number of anti-TNF drugs used in this group was significantly higher than in the other (p=0.014), specially etanercept (p=0.033).
For the other bDMARD agents, the risk of HZ has not been systematically evaluated. Results of several studies are not consistent, but the general results suggest that the use of other biological drugs may also increase the risk of shingles [30,31,32]. In fact, in our HZ cohort, three patients were taking tocilizumab, three abatacept and one sarilumab in the moment of the virus reactivation.
JAK inhibitors are the latest and promising treatments for RA, but the risk of HZ is also very high with them. Many reports and clinical trials have demonstrated an increased risk of VZV reactivation, especially with tofacitinib. This increased risk is due to the mechanism of action of these molecules. The inhibition of Janus kinases 1, 2 and 3 decreases the functionality of Th1 cells and block specific cytokines that protect from the infection or reactivation of herpes virus. Interestingly, the risk of viral infections is related to the dose in all these therapies [33,34,35,36,37,38,39]
In our group of patients with HZ, two patients were under treatment with tofacitinib and one with upadacitinib at the moment of shingles.
Currently, we know that vaccination is an essential point to prevent HZ infection. Nonetheless, until recently, vaccines to prevent the reactivation of this virus were normally norstandardized in patients with RA. In fact, in our cohort, none patient had been vaccinated for this virus at the moment of diagnosis.
Nowadays, there are two vaccines available for HZ infection. Zostavax® is a live attenuated vaccine, similar to one of the varicella vaccines administrated in the childhood but fourteen times more potent to be able to create immunity in elderly or suppressed immune system [40]
Shingrix® is the last approved HZ vaccine. It is a recombinant vaccine that contains the VZV glycoprotein E and the AS01B adjuvant system. The mechanism of action is similar to Zostavax, increasing the production of specific CD4+T-cells. The studies have demonstrated that the response persist for at least 3 years, even in immunocompromised patients [41]. The main advantage of this vaccine is the possibility of administration at any moment during the disease. Recent reports suggest that the recombinant vaccine is superior to live-attenuated in reducing the number of cases of HZ and its sequelae as PHN.
The last EULAR recommendations for vaccination (2019) state that HZ vaccination should be considered in adult patients with autoimmune inflammatory rheumatic diseases, but these recommendations are not homogeneousin most of hospitals yet42.In fact, in our country, this vaccine is currently approved only for patients older than 65 years or for patients under certain therapies such as JAK inhibitors.
5. Conclusions
Overall, we can conclude that risk of HZ is higher in immunocompromised patients such as RA patients, which are more likely to suffer from complications or sequelae like PHN. In our series, despite the fact that the number of patients under treatment with JAK inhibitors was low, the incidence rate was high. Thus, we think that new recombinant vaccine for HZ should be recommended in vaccination programs to all patients with RA
Funding
This research received no external funding.
Institutional Review Board Statement
approved by the Institutional Ethics Committee of COMITÉ DE ÉTICA DE LA INVESTIGACIÓN CON MEDICAMENTOS DE CANTABRIA Approval Code: 2018.266 / Approval Date: 08 de abril de 2020
Acknowledgments
To patients and all the members, physicians and nurses, of Rheumatology and Preventive Medicine departments of our hospital
Conflicts of Interest
Disclosures that might be interpreted as constituting of possible conflict(s) of interest for the study:
- -
- Lucía C. Domínguez-Casas has received research supports and participation in company-sponsored speaker’s bureau from Abbvie, Janssen, Lilly and Celgene.
- -
- S.Castañeda has received research supports from MSD and Pfizer and had consultation fees/participation in company-sponsored speaker’s bureau from BMS, Eli-Lilly, MSD, Roche and UCB.
- -
- R. Blanco received grants/research supports from Abbvie, MSD and Roche, and had consultation fees/participation in company sponsored speaker´s bureau from Abbvie, Pfizer, Roche, Bristol-Myers, Janssen and MSD.
- -
- Iván Ferraz-Amaro and Carmen Lasa-Teja have not conflicts of interest for this study
References
- Winthrop, K.L.; Tanaka, Y.; Lee, E.B.; Wollenhaupt, J.; Al Enizi, A.; Azevedo, V.F.; Curtis, J.R. Prevention and management of herpes zoster in patients with rheumatoid arthritis and psoriatic arthritis: a clinical review. Clin. Exp. Rheumatol. 2022, 40, 162–172. [Google Scholar] [CrossRef]
- Allison L Smitten 1, Hyon K Choi, Marc C Hochberg, SamySuissa, Teresa A Simon, Marcia A Testa et al,; The risk of herpes zoster in patients with rheumatoid arthritis in the United States and the united kingdom. Arthritis& Rheumatism. 2007; Dec 15;57(8):1431–1438.
- Chen, S.-Y.; Suaya, J.A.; Li, Q.; Galindo, C.M.; Misurski, D.; Burstin, S.; Levin, M.J. Incidence of herpes zoster in patients with altered immune function. Infection 2013, 42, 325–334. [Google Scholar] [CrossRef]
- Winthrop, K.L.; Furst, D.E. Rheumatoid arthritis and herpes zoster: risk and prevention in those treated with anti-tumour necrosis factor therapy. Ann. Rheum. Dis. 2010, 69, 1735–1737. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Cho, S.; Lee, J.; Bae, S.; Sung, Y. Increased risk of opportunistic infection in early rheumatoid arthritis. Int. J. Rheum. Dis. 2019, 22, 1239–1246. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Rondaan, C.; Heijstek, M.; van Assen, S.; Bijl, M.; Agmon-Levin, N.; Breedveld, F.C.; D'Amelio, R.; Dougados, M.; Kapetanovic, M.C.; et al. Incidence and prevalence of vaccine preventable infections in adult patients with autoimmune inflammatory rheumatic diseases (AIIRD): a systemic literature review informing the 2019 update of the EULAR recommendations for vaccination in adult patients with AIIRD. RMD Open 2019, 5, e001041. [Google Scholar] [CrossRef]
- Pinchinat, S.; Cebrián-Cuenca, A.M.; Bricout, H.; Johnson, R.W. Similar herpes zoster incidence across Europe: results from a systematic literature review. BMC Infect. Dis. 2013, 13, 170–170. [Google Scholar] [CrossRef] [PubMed]
- Sauerbrei, A. , Diagnosis, antiviral therapy, and prophylaxis of varicella-zoster virus infections. European Journal of Clinical Microbiology and Infectious Diseases 2016 May;35(5):723-34.
- Amrita John, David H. Canaday, Herpes zoster in the older adult, Infectious Disease Clinics of North America. 2017 Dec; 31(4): 811–826.
- Schmader, K. , Herpes zoster. Annals of Internal Medicine. 2018 Aug 7;169(3):ITC19-ITC31.
- Arvin, A.M. Humoral and Cellular Immunity to Varicella-Zoster Virus: An Overview. J. Infect. Dis. 2008, 197, S58–S60. [Google Scholar] [CrossRef]
- ChristienRondaan, Aalzen de Haan, Gerda Horst, J. Cordelia Hempel, Coretta van Leer, Nicolaas A. Boset al., Altered cellular and humoral immunity to varicella-zoster virus in patients with autoimmune diseases, Arthritis& Rheumatology. 2014 Nov;66(11): 3122–3128.
- Lang, P.-O.; Aspinall, R. Vaccination for quality of life: herpes–zoster vaccines. Aging Clin. Exp. Res. 2019, 33, 1113–1122. [Google Scholar] [CrossRef]
- Dayan, R.R.; Peleg, R. Herpes zoster – typical and atypical presentations. Postgrad. Med. 2017, 129, 567–571. [Google Scholar] [CrossRef]
- Pragya A., Nair; Bhupendra, C. Patel, Herpes Zoster,In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. 2022. Sep 5.
- Yamaguchi, R.; Tanaka, E.; Nakajima, A.; Inoue, E.; Abe, M.; Sugano, E.; Sugitani, N.; Saka, K.; Ochiai, M.; Higuchi, Y.; et al. Risk of herpes zoster in patients with rheumatoid arthritis in the biologics era from 2011 to 2015 and its association with methotrexate, biologics, and corticosteroids. Mod. Rheumatol. 2021, 32, 522–527. [Google Scholar] [CrossRef]
- Pappas, D.A.; Hooper, M.M.; Kremer, J.M.; Reed, G.; Shan, Y.; Wenkert, D.; Greenberg, J.D.; Curtis, J.R. Herpes Zoster Reactivation in Patients With Rheumatoid Arthritis: Analysis of Disease Characteristics and Disease-Modifying Antirheumatic Drugs. Arthritis Care Res. 2015, 67, 1671–1678. [Google Scholar] [CrossRef]
- Riley, T.R.; George, M.D. Risk for infections with glucocorticoids and DMARDs in patients with rheumatoid arthritis. RMD Open 2021, 7, e001235. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.; Sfikakis, P.P.; Boumpas, D.; Boki, K.; Vassilopoulos, D. Study of the natural course and specific immunity after herpes zoster in patients with rheumatoid arthritis receiving biologic DMARDs. Mediterr. J. Rheumatol. 2017, 28, 164–168. [Google Scholar] [CrossRef]
- Kosuke Kawai, Barbara P. Yawn,Risk Factors for Herpes Zoster: A Systematic Review and Meta-analysis. Mayo Clinic Proceedings2017 Dec;92(12):1806-1821.
- Lecrenier, N.; Beukelaers, P.; Colindres, R.; Curran, D.; De Kesel, C.; De Saegher, J.-P.; Didierlaurent, A.M.; Ledent, E.Y.; Mols, J.F.; Mrkvan, T.; et al. Development of adjuvanted recombinant zoster vaccine and its implications for shingles prevention. Expert Rev. Vaccines 2018, 17, 619–634. [Google Scholar] [CrossRef] [PubMed]
- Theresa Mallick-Searle, Brett Snodgrass, Jeannine M Brant,Postherpetic neuralgia: epidemiology, pathophysiology, and pain management pharmacology. Journal of Multidisciplinary Healthcare. 2016;9:447–454.
- Hata, A.; Kuniyoshi, M.; Ohkusa, Y. Risk of Herpes zoster in patients with underlying diseases: a retrospective hospital-based cohort study. Infection 2011, 39, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann. Rheum. Dis. 2010, 69, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Robert, W. Johnson, Marie-José Alvarez-Pasquin, Marc Bijl, Elisabetta Franco, Jacques Gaillat, João G. Clara et al., Herpes zoster epidemiology, management, and disease and economic burden in Europe: : a multidisciplinary perspective Therapeutic Advances in Vaccines2015 Jul; 3(4): 109–120.
- Calabrese, L.H.; Xie, F.; Yun, H.; Winthrop, K.L.; Baddley, J.W.; Calabrese, C.; Curtis, J.R. Herpes Zoster and the Risk of Stroke in Patients With Autoimmune Diseases. Arthritis Rheumatol. 2016, 69, 439–446. [Google Scholar] [CrossRef]
- Youssef, J.; Novosad, S.A.; Winthrop, K.L. Infection Risk and Safety of Corticosteroid Use. Rheum. Dis. Clin. North Am. 2016, 42, 157–176. [Google Scholar] [CrossRef]
- McDonald, J.R.; Zeringue, A.L.; Caplan, L.; Ranganathan, P.; Xian, H.; Burroughs, T.E.; Fraser, V.J.; Cunningham, F.; Eisen, S.A. Herpes Zoster Risk Factors in a National Cohort of Veterans with Rheumatoid Arthritis. Clin. Infect. Dis. 2009, 48, 1364–1371. [Google Scholar] [CrossRef]
- Strangfeld, A.; Listing, J.; Herzer, P.; Liebhaber, A.; Rockwitz, K.; Richter, C.; Zink, A. Risk of Herpes Zoster in Patients With Rheumatoid Arthritis Treated With Anti–TNF-α Agents. JAMA 2009, 301, 737–44. [Google Scholar] [CrossRef]
- Pawar, A.; Desai, R.J.; Solomon, D.H.; Ortiz, A.J.S.; Gale, S.; Bao, M.; Sarsour, K.; Schneeweiss, S.; Kim, S.C. Risk of serious infections in tocilizumab versus other biologic drugs in patients with rheumatoid arthritis: a multidatabase cohort study. Ann. Rheum. Dis. 2019, 78, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Yun, H.; Xie, F.; Delzell, E.; Chen, L.; Levitan, E.B.; Lewis, J.D.; Saag, K.G.; Beukelman, T.; Winthrop, K.; Baddley, J.W.; et al. Risks of Herpes Zoster in Patients With Rheumatoid Arthritis According to Biologic Disease-Modifying Therapy. Arthritis Care Res. 2014, 67, 731–736. [Google Scholar] [CrossRef] [PubMed]
- Tran, C.T.; Ducancelle, A.; Masson, C.; Lunel-Fabiani, F. Herpes zoster: Risk and prevention during immunomodulating therapy. Jt. Bone Spine 2017, 84, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Flavia Sunzini, Iain McInnes, Stefan Siebert, Patient-reported outcomes from a randomised phase III study of baricitinib in patients with rheumatoid arthritis and an inadequate response to biological agents (RA-BEACON). Annalsof Rheumatic Diseases. 2017 Apr;76(4):694-700.
- Roy Fleischmann, Eduardo Mysler, Stephen Hall, Alan J Kivitz, Robert J Moots, Zhen Luo et al., Efficacy and safety of tofacitinib monotherapy, tofacitinib with methotrexate, and adalimumab with methotrexate in patients with rheumatoid arthritis (ORAL Strategy): a Phase IIIb/IV, double-blind, head-to-head, randomised controlled trial. Lancet. 2017 Jul 29;390 (10093): 457-468.
- Burmester, G.R.; Kremer, J.M.; Bosch, F.V.D.; Kivitz, A.; Bessette, L.; Li, Y.; Zhou, Y.; A Othman, A.; Pangan, A.L.; Camp, H.S. Safety and efficacy of upadacitinib in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying anti-rheumatic drugs (SELECT-NEXT): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2018, 391, 2503–2512. [Google Scholar] [CrossRef] [PubMed]
- Roy Fleischmann, Aileen L. Pangan, In-Ho Song, Eduardo Mysler, Louis Bessette, Charles Peterfyet al., Upadacitinib versus placebo or adalimumab in patients with rheumatoid arthritis and an inadequate response to methotrexate: results of a phase 3, double-blind, randomized controlled trial. Arthritis & Rheumatology 2019 Nov;71(11):1788-1800.
- Chen, Y.-J.; Huang, W.-N.; Chen, H.-H.; Liao, T.-L.; Chen, J.-P.; Hsieh, T.-Y.M.; Chen, Y.-H.; Chen, D.-Y. Herpes Zoster in rheumatoid arthritis patients receiving tofacitinib, a single center experience from Taiwan. Medicine 2020, 99, e22504. [Google Scholar] [CrossRef]
- Bechman, K.; Subesinghe, S.; Norton, S.; Atzeni, F.; Galli, M.; Cope, A.P.; Winthrop, K.L.; Galloway, J.B. A systematic review and meta-analysis of infection risk with small molecule JAK inhibitors in rheumatoid arthritis. Rheumatology 2019, 58, 1755–1766. [Google Scholar] [CrossRef]
- Sullivan, N.L.; Eberhardt, C.S.; Wieland, A.; A Vora, K.; Pulendran, B.; Ahmed, R. Understanding the immunology of the Zostavax shingles vaccine. Curr. Opin. Immunol. 2019, 59, 25–30. [Google Scholar] [CrossRef] [PubMed]
- A Shah, R.; Limmer, A.L.; E Nwannunu, C.; Patel, R.R.; Mui, U.N.; Tyring, S.K. Shingrix for Herpes Zoster: A Review. 2019, 24, 5–7.
- Furer, V.; Rondaan, C.; Heijstek, M.W.; Agmon-Levin, N.; Van Assen, S.; Bijl, M.; Breedveld, F.C.; D’Amelio, R.; Dougados, M.; Kapetanovic, M.C.; et al. 2019 update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann. Rheum. Dis. 2020, 79, 39–52. [Google Scholar] [CrossRef]
Figure 1.
Sequelae of dorsal herpes zoster in a patient with RA.
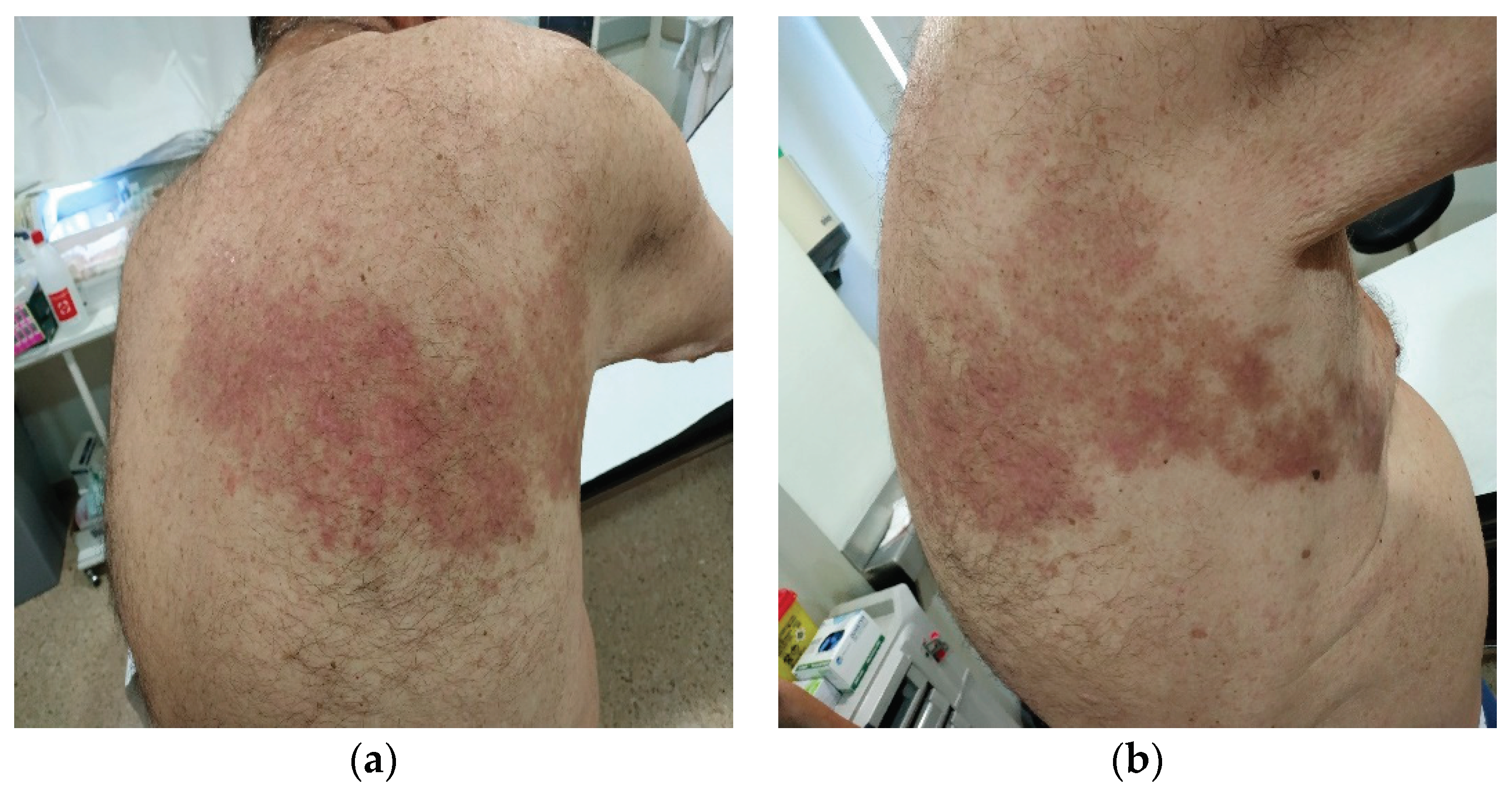

Table 1.
Demographics and disease-related data differences at baseline between patients developing herpes zoster infection or not.
Table 1.
Demographics and disease-related data differences at baseline between patients developing herpes zoster infection or not.
| RA patients (N=392) |
RA patients with HZ (N=30) |
RA patients without HZ (N=362) | P-value | |
|---|---|---|---|---|
| Age (years) (mean±SD) | 59±13 | 61±13 | 59±13 | 0.36 |
| Time of evolution of RA, (months)(mean±SD) | 136.9±109.8 | 158±118 | 135.3±109.2 | 0.33 |
| Women, n (%) | 309 (79) | 25 (83) | 284 (78) | 0.53 |
| Smokers, n (%) | 155 (40) | 11 (37) | 144 (40) | 0.74 |
| Hypertension, n (%) | 165 (42) | 18 (60) | 147 (41) | 0.039 |
| Diabetes mellitus, n (%) | 55 (14) | 6 (20) | 49 (14) | 0.33 |
| Dyslipidemia, n (%) | 148 (38) | 14 (47) | 134 (37) | 0.30 |
| Positive rheumatoid factor, n (%) | 223 (57) | 17 (57) | 206 (57) | 0.98 |
| Positive anti-citrullinated peptide antibodies, n (%) | 206 (53) | 13 (43) | 193 (53) | 0.29 |
| Erosive disease, n (%) | 145 (37) | 10 (33) | 135 (37) | 0.67 |
| Subcutaneous nodules, n (%) | 23 (6) | 1 (3) | 22 (6) | 0.57 |
| Interstitial lung disease, n (%) | 20 (5) | 3 (10) | 17 (5) | 0.21 |
| Sjögren´s syndrome, n (%) | 20 (5) | 1 (3) | 19 (5) | 0.65 |
| Vasculitis, n (%) | 23 (6) | 2 (7) | 21 (6) | 0.85 |
| Baseline use of therapies | ||||
| Prednisone | ||||
| N (%) | 228 (58) | 16 (55) | 212 (59) | 0.72 |
| Dose, mg/day | 5 (0-5) | 5 (0-5) | 3.75 (0-7.5) | 0.92 |
| Conventional synthetic DMARDs | ||||
| Methotrexate | 252 (64) | 20 (67) | 232 (64) | 0.78 |
| Leflunomide | 38 (10) | 2 (7) | 36 (10) | 0.56 |
| Sulfasalazine | 12 (3) | 1 (3) | 11 (3) | 0.61 |
| Azathioprine | 1 (0) | 0 (0) | 1 (0) | 0.99 |
| Biological DMARDs | ||||
| Any anti-TNFα | 92 (23) | 9 (30) | 83 (23) | 0.38 |
| Adalimumab | 35 (10) | 3 (10) | 32 (9) | 0.74 |
| Etanercept | 40 (10) | 5 (17) | 35 (10) | 0.23 |
| Infliximab | 7 (2) | 0 (0) | 7 (2) | 0.99 |
| Golimumab | 43 (11) | 4 (13) | 39 (11) | 0.56 |
| CertolizumabPegol | 1 (0) | 0 (0) | 1 (0) | 0.99 |
| Tocilizumab | 16 (4) | 1 (3) | 15 (4) | 0.99 |
| Rituximab | 11 (3) | 2 (7) | 9 (2) | 0.20 |
| Abatacept | 4 (1) | 0 (0) | 4 (1) | 0.99 |
| Cumulative treatment for RA | ||||
| Conventional DMARDs (not concomitant), n (%) | ||||
| Methotrexate | 351 (90) | 325 (90) | 26 (87) | 0.81 |
| Leflunomide | 126 (32) | 114 (31) | 12 (40) | 0.34 |
| Sulfasalazine | 90 (23) | 83 (23) | 7 (23) | 0.96 |
| Azathioprine | 22 (6) | 19 (5) | 3 (10) | 0.23 |
| Cyclosporine A | 11 (2) | 11 (3) | 0 (0) | 0.99 |
| Gold salts | 37 (9) | 34 (9) | 3 (10) | 0.75 |
| Penicillamine | 8 (2) | 7 (2) | 1 (3) | 0.47 |
| Biological DMARDs, n (%) | ||||
| Any anti-TNF | 260 (66) | 234 (65) | 26 (87) | 0.014 |
| Adalimumab | 145 (37) | 131 (36) | 14 (47) | 0.25 |
| Etanercept | 139 (35) | 123 (34) | 16 (53) | 0.033 |
| Infliximab | 40 (10) | 35 (10) | 5 (17) | 0.22 |
| Golimumab | 33 (8) | 30 (8) | 3 (10) | 0.73 |
| Certolizumab Pegol | 13 (3) | 12 (3) | 1 (3) | 0.99 |
| Tocilizumab | 134 (34) | 119 (33) | 15 (50) | 0.057 |
| Rituximab | 71 (18) | 62 (17) | 9 (30) | 0.079 |
| Abatacept | 53 (14) | 47 (13) | 6 (20) | 0.28 |
| Sarilimumab | 3 (1) | 2 (1) | 1 (1) | 0.093 |
| JAK inhibitors, n (%) | 42 (11) | 38 (11) | 4 (13) | 0.63 |
| Tofacitinib | 16 (4) | 14 (4) | 2 (1) | 0.46 |
| Baricitinib | 32 (8) | 30 (8) | 2 (7) | 0.99 |
| Upadacitinib | 4 (1) | 3 (1) | 1 (3) | 0.27 |
| Months of exposition to biological or targeted therapies, median (IQR) | ||||
| Any anti-TNF-α | 42 (12-82) | 43 (12-79) | 36 (13-101) | 0.69 |
| Adalimumab | 22 (9-56) | 23 (9-59) | 15 (9-31) | 0.43 |
| Etanercept | 26 (4-72) | 26 (4-64) | 25 (4-124) | 0.99 |
| Infliximab | 19 (7-40) | 19 (6-42) | 11 (9-38) | 0.82 |
| Golimumab | 22 (8-53) | 18 (6-53) | 34 (24-38) | 0.54 |
| Certolizumab | 21 (15-41) | 21 (12-40) | 58 (58-58) | 0.18 |
| Tocilizumab | 27 (7-65) | 28 (7-65) | 19 (6-41) | 0.22 |
| Rituximab | 24 (4-63) | 26 (5-68) | 9 (2-26) | 0.055 |
| Abatacept | 12 (6-33) | 11 (5-31) | 16 (16-33) | 0.26 |
| Sarilimumab | 3 (1-14) | 8 (1-14) | 3 (3-3) | 0.99 |
| JAK inhibitors (all) | 11 (6-18) | 11 (6-18) | 11 (2-19) | 0.81 |
| - Tofacitinib | 11 (2-19) | - | 11 (2-19) | - |
| - Baritinib | 9 (5-14) | 9 (5-14) | - | - |
| - Upadacitinib | 9 (1-28) | 1 (1-16) | 39 (39-39) | 0.16 |
Abbreviations (in alphabetical order):DMARDs: disease-modifying anti-rheumatic drugs; HZ: herpes zoster; IQR: interquartile range; JAK: Janus kinase; N (n): number; RA: rheumatoid arthritis; TNF: tumor necrosis factor; SD: standard deviation.
Table 2.
Main demographic, clinical data and treatment of 30 patients with herpes zoster.
| Case | Sex | Age at HZ | HZ location | HZ treatment | HZ antiviral treatment | Postherpetic Neuralgia | Concomitant RA treatment |
|---|---|---|---|---|---|---|---|
| 1 | Female | 71 | Upper Extremity (left) | Unknown | - | No | Corticosteroids/MTX/TCZ |
| 2 | Female | 62 | Intercostal (right) | Systemic antiviral | Brivudine | No | Corticosteroids/GLM |
| 3 | Male | 70 | Intercostal (right) | Systemic antiviral | Famciclovir | Yes | GLM |
| 4 | Female | 84 | Unknown | Topic | - | No | Corticosteroids/MTX |
| 5 | Female | 68 | Dorsal (right) | None | - | Yes | Corticosteroids/ABA |
| 6 | Female | 78 | Lumbar (left) | Systemic antiviral | Brivudine | No | Corticosteroids/MTX |
| 7 | Male | 72 | Intercostal (left) | None | - | No | ETN |
| 8 | Female | 79 | Abdominal | Systemic antiviral | Brivudine | Yes | Corticosteroids/MTX |
| 9 | Female | 36 | Unknown | Systemic antiviral | Aciclovir | No | Corticosteroids/MTX |
| 10 | Female | 51 | Disseminated | Systemic antiviral | Famciclovir | Yes | Corticosteroids |
| 11 | Female | 66 | Dorsal (left) | None | - | No | Corticosteroids/MTX/ADA |
| 12 | Male | 82 | Ophthalmic(left) | Topic | - | No | Corticosteroids/ABA |
| 13 | Female | 45 | Abdominal | Systemic antiviral | Brivudine | No | SARI |
| 14 | Female | 52 | Unknown | Topic/Systemic antiviral | Aciclovir | No | Corticosteroids/TCZ |
| 15 | Female | 63 | Cervical | None | - | No | MTX |
| 16 | Female | 71 | Submammary fold (left) | Systemic antiviral | Famciclovir | No | Corticosteroids/MTX |
| 17 | Female | 68 | Intercostal (left) | Systemic antiviral | Brivudine | Yes | None |
| 18 | Female | 53 | Intermammary fold | Systemic antiviral | Brivudine | No | TOFA |
| 19 | Female | 75 | Lumbar | Systemic antiviral | Valaciclovir | No | Corticosteroids/MTX/UPA |
| 20 | Female | 58 | Unknown | Topic/Systemic antiviral | Famciclovir | No | Corticosteroids |
| 21 | Male | 73 | Intercostal (left) | Systemic antiviral | Aciclovir | Yes | Corticosteroids/ABA |
| 22 | Female | 40 | Dorsal (left) | Systemic antiviral | Famciclovir | No | Corticosteroids/AZA/CZP |
| 23 | Female | 58 | Abdominal | Systemic antiviral | Famciclovir | No | Corticosteroids/TCZ |
| 24 | Female | 73 | Lumbar (right) | Systemic antiviral | Aciclovir | No | Corticosteroids/LFN |
| 25 | Female | 66 | Unknown | Systemic antiviral | Aciclovir | Yes | TOFA |
| 26 | Male | 57 | Intercostal (left) | Systemic antiviral | Brivudine | No | Corticosteroids/SSZ/ETN |
| 27 | Female | 61 | Dorsal (left) | Systemic antiviral | Aciclovir | No | LFN/ETN |
| 28 | Female | 63 | Facial (right) | Systemic antiviral | Famciclovir | No | MTX |
| 29 | Female | 67 | Gluteus (left) | Systemic antiviral | Valaciclovir | No | Corticosteroids/MTX/LFN |
| 30 | Female | 79 | Trigeminal (left) | Systemic antiviral | Valaciclovir | No | ETN |
Abbreviations (in alphabetical order): ABA: abatacept; ADA: adalimumab; AZA: azathioprine; CZP: certolizumabpegol; ETN: etanercept; GLM: golimumab; HZ: herpes zoster; IFX: infliximab; LFN: leflunomide; MTX: methotrexate; RA: rheumatoid arthritis; SARI: sarilumab; SSZ: sulfasalazine; TCZ: tocilizumab; TOFA: tofacitinib; UPA: upadacitinib.
Table 3.
Herpes zoster infection characteristics and therapy for rheumatoid arthritis when infection appeared.
Table 3.
Herpes zoster infection characteristics and therapy for rheumatoid arthritis when infection appeared.
| Age at the moment of HZ,mean±SD (years) | 64.7±11.8 |
| Time of evolution of RA, mean±SD (months) | 158.4±115.7 |
| Location, n(%) | |
| Trunk | 18 (60) |
| Head and neck | 4 (13) |
| Extremities | 2 (7) |
| Disseminated | 1 (3) |
| Unknown | 5 (17) |
| Antiviral treatment, n (%) | 23 (77) |
| Brivudine | 7 (30) |
| Famciclovir | 7 (30) |
| Aciclovir | 6 (126) |
| Valaciclovir | 3 (13) |
| Sequelae | |
| Postherpetic neuralgia | 7 (87) |
| Temporary visual alteration | 1 (13) |
| Current treatment when zoster infection occurred | |
| Prednisone, n (%) | 19 (63) |
| Prednisone dose, mg/day | 7.5 (5-10) |
| DMARDs, n (%) | 15 (50) |
| Metothrexate | 10 (67) |
| Leflunomide | 2 (13) |
| Metothrexate + leflunomide | 1 (7) |
| Azathioprine | 1 (7) |
| Sulfasalazine | 1 (7) |
| Biological therapy, n (%) | 15 (50) |
| Etanercept | 4 (27) |
| Abatacept | 3 (20) |
| Tocilizumab | 3 (20) |
| Golimumab | 2 (13) |
| Adalimumab | 1 (7) |
| Certolizumab | 1 (7) |
| Sarilumab | 1 (7) |
| JAK inhibitors, n (%) | 3 (10) |
| Tofacitinib | 2 (13) |
| Upadacitinib | 1 (33) |
Abbreviations (in alphabetical order): DMARDs: disease-modifying anti-rheumatic drugs; HZ: herpes zoster; JAK: Janus kinase; N (n): number; RA: rheumatoid arthritis: SD: standard deviation.
Table 4.
Predictive factors of herpes zoster development in our cohort of patients with rheumatoid arthritis.
Table 4.
Predictive factors of herpes zoster development in our cohort of patients with rheumatoid arthritis.
| HR (95%CI) | p | |
|---|---|---|
| Age (years) (mean±SD) | 1.02 (0.99-1.05) | 0.21 |
| Time of evolution of RA (months) (mean±SD) | 1.002 (0.99-1.005) | 0.31 |
| Women, n (%) | 1.31 (0.50-3.42) | 0.58 |
| Active smokers, n (%) | 0.90 (0.43-1.90) | 0.79 |
| Hypertension, n (%) | 2.25 (1.09-4.68) | 0.029 |
| Diabetes Mellitus, n (%) | 1.70 (0.70-4.17) | 0.24 |
| Dyslipidemia, n (%) | 1.50 (0.73-3.08) | 0.27 |
| Positive RF, n (%) | 0.96 (0.46-1.97) | 0.91 |
| Positive anti-CCP, n (%) | 0.67 (0.33-1.38) | 0.28 |
| Erosions, n (%) | 0.86 (0.40-1.85) | 0.71 |
| Subcutaneous nodules, n (%) | 0.53 (0.07-3.92) | 0.54 |
| Interstitial lung disease, n (%) | 2.10 (0.64-6.94) | 0.22 |
| Sjögren´s syndrome, n (%) | 0.62 (0.08-4.52) | 0.63 |
| Number of conventional DMARDs (not concomitant) | ||
| Methotrexate | 0.77 (0.29-2.06) | 0.60 |
| Leflunomide | 1.33 (0.67-2.66) | 0.42 |
| Sulfasalazine | 1.08 (0.46-2.51) | 0.87 |
| Azathioprine | 1.93 (0.59-6.38) | 0.28 |
| Gold salts | 1.04 (0.32.3.44) | 0.95 |
| Penicillamine | 1.58 (0.21-11.60) | 0.65 |
| Biological DMARDs, n (%) | ||
| Any anti-TNF | 1.12 (0.51-2.47) | 0.78 |
| Adalimumab | 1.21 (0.59-2.50) | 0.60 |
| Etanercept | 2.04 (0.99-4.18) | 0.05 |
| Infliximab | 1.88 (0.72-4.90) | 0.20 |
| Golimumab | 1.05 (0.32-3.48) | 0.93 |
| CertolizumabPegol | 0.98 (0.13-7.18) | 0.98 |
| Tocilizumab | 1.55 (0.75-3.17) | 0.23 |
| Rituximab | 1.94 (0.88-4.22) | 0.99 |
| Abatacept | 1.46 (0.59-3.57) | 0.41 |
| Sarilumab | 3.90 (0.53-28.62) | 0.18 |
| JAK inhibitors | 1.46 (0.56-3.82) | 0.44 |
| Tofacitinib | 1.34 (0.32-5.64) | 0.69 |
| Baricitinib | 0.73 (0.17-3.07) | 0.67 |
| Upadacitinib | 4.14 (0.56-30.59) | 0.16 |
Abbreviations(in alphabetical order): anti-CCP: anti-citrullinated peptide antibodies; CI: confidence interval; DMARDs: disease-modifying anti-rheumatic drugs; HR: hazard ratio; JAK: Janus kinase; N (n): number; RF: rheumatoid factor; TNF: tumor necrosis factor; SD: standard deviation.
Table 5.
Comparative incidence rates in classic rheumatoid arthritis cohorts.
| Design | Underlying disease | Number of RA patients | IR* of HZ | |
|---|---|---|---|---|
| Wolfe et al (2006) | Observational | RA | 28852 | 7.70 |
| Smitten et al (2007) | Retrospective | RA RA |
122272 38621 |
9.83 3.71 |
| McDonald et al (2009) | Retrospective | RA and other MSK diseases | 20357 | 9.96 |
| Chen et al (2011) | Observational | Immune-mediated diseases | 11446 | 12.24 |
| Pappas et al (2015) | Observational | RA | 10614 | 13.20 |
| Harada et al (2017) | Prospective | RA | 1987 | 6.66 |
| Dominguez et al (2023) | Prospective | RA | 392 | 13.22 |
Abbreviations (in alphabetical order): HZ: herpes zoster; IR: incidence rate; MSK: musculoskeletal diseases; RA: rheumatoid arthritis.*Incidence rate expressed in 1000 patients-year.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



