
Submitted:
17 March 2024
Posted:
18 March 2024
You are already at the latest version
Abstract
Background: The management of erectile dysfunction (ED) shows several grey zones and new treatments for reduce the percentage of patients who discontinued the treatment are required. Here, we aim to evaluate the role of a natural mixture of named Icarifil (L-Citrulline, L-Carnitine, Eruca vesicaria, Panax ginseng, Tribulus terrestris, Turnera diffusa, Taurine, Vitamin E, Zinc) in the management of patients with ED. Methods: From September 2022 to March 2023, all patients attending 3 urological institutions due to ED were randomized to receive: Icarifil 1 sachet every 24 h (Group 1) or Icarifil 1 sachet + tadalafil 5 mg 1 tablet every 24 h (Group 2) or tadalafil 5 mg 1 tablet daily (Group 3), for 3 months. All patients underwent urologic visit and dedicated questionnaires (IIEF-5, SEP-2, SEP-3) at the enrollment and at the follow-up evaluation (3 months). Patient Reported Outcomes (PROs) at the follow-up evaluation were used. Primary endpoint was the difference in the questionnaires at the follow-up visit when compared with enrollment among the study groups. Results: In the per-protocol analysis, 52 patients in the Group 1, 55 in the Group 2 and 57 in Group 3 have been analyzed. At the follow-up evaluation, IIEF-5 have been improved in all the 3 Groups between enrollment and follow-up evaluation, but a statistically significant difference has been reported between Group 2 (+7.4) versus Group 1 (+4.1) or 3 (+5.1), (p<0.001; p<0.001). Moreover, 47 patients (94.0%) in the Group 2 showed an improvement in the SEP questionnaires, when compared with the baseline, while 29 in the Group 1 (56.9%) and 42 in the Group 3 (82.3%) with a statistically significant difference (p=0.004; p=0.003) among the Groups. The PROs analysis reported a better efficacy and patients’ satisfaction in Group 2 when compared with Group 1 or 3. Conclusions: In conclusion, Icarifil is able to improve penile erectile function in mild–moderate ED and it is able to significantly improve the clinical efficacy of tadalafil 5 mg daily use. Icarifil could be represent an interesting alternative treatment in patients experiencing adverse effects or with contraindications for chronic treatment with PDE5-is.
Keywords:
nutraceuticals
; erectile dysfunction
; Eruca vesicaria
; Panax ginseng
; Tribulus terrestris
; L-arginine
; L-citrulline
; PDE5i.
1. Introduction
Erectile dysfunction (ED) is a common pathological condition with severe impact on patients and patient’s partner quality of life [1]. Epidemiological studies showed that ED increases with age and is therefore much higher in elderly than in young men, but still relatively frequent during middle age [2,3]. The prevalence rates ranging from 1 to 15% and from 6 to 40% in men aged 30–50 and 50–80 years [4]. In the last years, however, the use of phosphodiesterase-5 inhibitors is increased, especially in the young-middle age males, demonstrating that the prevalence of ED is rising [5]. Oral phosphodiesterase-5 inhibitors (PDE-5is) represent the first line pharmacological approach to patient with ED, due to its great efficacy and generally favorable safety profile [6]. However, the percentage of patients who discontinued the treatment is still high. On the other hand, several nutraceuticals compounds, supplemented as single agents and/or in different combinations, have been reported to offer benefits in the treatment of ED, without adverse effects. Several compounds, such has carnitine, ginseng, Tribulus terrestris or damiana, have been reported interesting results in terms of clinical efficacy in patients with vasculogenic erectile dysfunction [7,8,9]. Considering the concept that nutraceuticals or phytotherapeutic compounds are considered safer and are generally efficacious for the treatment of mild-moderate ED, some components might represent a valid therapeutic alternative in the treatment of ED alone or in association with PDE-5is. Recently, a mixture of phytotherapeutic compounds named Icarifil®, containing L-Citrulline, L-Carnitine, Eruca vesicaria, Panax ginseng, Tribulus terrestris, Turnera diffusa, Taurine, Vitamin E, Zinc has been introduced in the pharmaceutical market for the management of moderate ED. Recently, Amante C. et al demonstrated, in an in vitro model, that Icarifil® showed efficacy in inhibiting PDE-5is levels higher than 65% compared to the control and is able to increase the capability of tadalafil to inhibit PDE-5is, showing a promising possibility of reducing the daily dosage of the drug and consequently its adverse effects [10]. Basing on these concerns, we aim to evaluate the role of Icarifil® in the management of patients with ED, by using a randomized and controlled study.
2. Materials and Methods
2.1. Study Design and Schedule
All consecutive patients attending 3 urological institutions due to mild-moderate ED from September 2022 to March 2023 were enrolled in randomized, controlled phase III study. At the enrolment all patients underwent urologic visit and dedicated questionnaires. Patients were assigned to treatment groups according to a 1:1 randomization. Enrolled patients were not blinded. No placebo run-in period was considered necessary. All patients who met the inclusion criteria were randomized by using a computer-generated sequence of allocation, as follows: Icarifil® 1 sachet every 24 h (Group 1) or Icarifil® 1 sachet + tadalafil 5 mg 1 tablet every 24 h (Group 2) or tadalafil 5 mg, alone, 1 tablet daily (Group 3). Patients in both groups underwent 3 months of treatment. All patients were contacted by telephone on day 30 of the therapy to ensure correct timing and dosing of treatment. At the end of the treatment (3 months), all patients underwent urologic visit and dedicated questionnaires. Patient Reported Outcomes (PROs) at the follow-up evaluation were used. The primary endpoint was the difference among the groups in terms of questionnaires scores between baseline and end of treatment. The Figure 1 shows the study schedule, according to the CONSORT statement [11].
2.2. Inclusion and Exclusion Criteria
We enrolled patients, aged higher that 18 years, affected by mild-moderate erectile dysfunction, according to the results of 5-question International Index of Erectile Function (IIEF-5) questionnaire [12]. Only patients scored from 12 to 16 at the IIEF-5 questionnaire have been included in the study, according to Tang et al. [13]. Patients with a history of ED on a hormonal basis, secondary to pelvic surgery or purely psychogenic or associated with penile deformity will be excluded.
All patients with major comorbidities have been excluded, too. In order to obtain a homogeneous group of patients to analyze, we excluded all patients who had undergone previous treatment with PDE-5is or alprostadil local or injections.
2.3. Composition and Characterization of the Extracts Used
Intervention schedule included a 3-months treatment with Icarifil® or tadalafil 5 mg or in combination. One oral sachet of Icarifil® (registration number 018623914) contain L-Citrulline 1500 mg, L-Carnitine 500 mg, Eruca vesicaria (Icariina 5%) 200 mg, Panax ginseng (Ginsenosids 80%) 150 mg, Tribulus terrestris 100 mg, Turnera diffusa (damiana) 100 mg, Taurine 50 mg, Vitamin E 50 mg and Zinc 15 mg, as described in the manufacturer's instructions (Anvest Health S.p.A, Milan - Italy).
2.4. Questionnaires
The validated Italian versions of the Index of Erectile Function (IIEF) [12] and the Sexual Encounter Profile (SEP) questionnaires [14] were filled in by each patient on the arrival to the urological outpatient clinics. The questionnaires were collected for each patient at the baseline and at the follow-up evaluation. The IIEF and SEP have been validated in previous clinical trials and have been shown to correlate well with the response to therapy in patients with ED [15,16]. The Erection hardness score (EHS) has been used too (3 measurements in 2 separate occasions). The partners of the enrolled patients will also be involved in the study by measuring the effectiveness of the therapy using the same questionnaires administered to the patients. Patient Reported Outcomes (PROs) were also considered in results analysis, as well as the patients’ partner PROS, according to Cai et al. [17].
2.5. Statistical Analysis, Outcome Measures and Ethical Considerations
On the basis of literature data, it is estimated that therapy with Icarifil® can lead to an average improvement in erectile function of approximately 4 points in the IIEF-EF score. On the basis of these considerations, has been estimated that the study requires 45 patients per group (135 assessments), plus 10% due to the possible drop-out: 150 patients (50 per group). The Chi-square test was used for categorical parameters and changes from baseline to end of therapy and were analyzed by ranked one-way analysis of variance (ANOVA). The threshold of statistical significance was set at P<0.05. All reported P-values are two-sided. All statistical analyses were performed using SPSS 23.0 (IBM Corporation, Armonk, NY, USA). The primary outcome was to evaluate the change in erectile function domain score (IIEF-5 and SEP-2 and SEP-3) from baseline to the control visit among the groups. Moreover, PROs measure has been used. This study was approved by the local Ethic Committee (approval protocol number 258, 2019) and its was conducted in compliance with the Institutional Review Board/Human Subjects Research Committee requirements and with the Declaration of Helsinki and the Guidelines for Good Clinical Trial Practice criteria. Patients may decide to abandon the study at any time as specified by the informed consent. An enrolled patient may also be excluded if serious side effects related to the proposed treatment appear. Randomization was based on a single sequence of random assignments (simple randomization) and performed using a pseudo-random number generator software (Research Randomizer Version 4.0, Social Psychology Network, Wesleyan University, Middletown, CT, USA).
Results
3.1. Patients
From an initial cohort of 177 patients attending our centers in the study enrollment period, 161 met the inclusion criteria and were randomly allocated with 54 to the group 1, 55 to Group 2 and 52 to the group 3. Ten patients have been excluded from the final analysis due to missing data at the follow-up evaluation. In the per-protocol analysis, data from 51 patients in the Icarifil® alone group, 50 in the Icarifil® in association with tadalfil 5 mg and 51 in the tadalafil alone group. The Table 1 shows all demographic, anamnestic, clinical and laboratory data at enrollment.
3.2. Follow-Up Results
At the follow-up evaluation, 47 patients (94.0%) in the Group 2 showed an improvement in the SEP-2, when compared with the baseline, while 29 in the Group 1 (56.9%) and 42 in the Group 3 (82.3%) with a statistically significant difference (p=0.004; p=0.003) among the Groups. In all the three Groups, a statistically significant difference has been reported from baseline to the follow-up in terms of SEP-2 and 3 questionnaires (p=0.002; p=0.003; p=0.003). Moreover, IIEF-5 have been improved in all the 3 Groups between enrollment and follow-up evaluation, but a statistically significant difference has been reported between Group 2 (+7.4) versus Group 1 (+4.1) or 3 (+5.1), (p<0.001; p<0.001). The PROs analysis reported a better efficacy and patients’ satisfaction in Group 2 when compared with Group 1 or 3. The Table 2 shows the follow-up results according to the Groups.
3.3. Patients and Their Partners Reported Outcome (PROs)
All patients asked about the efficacy of the drugs comparing the pre- and post-treatment erectile function, as too their partners. All patients in the three groups reported a significant improvement in their erectile function. In the Icarifil® associated with tadalafil group, the reported efficacy seems better than in the other groups, by using a PROs evaluation. Their partners confirmed these findings. Moreover, also in the group treated with Icarifil® alone, the daily administration shows a more “natural” treatment strategy because avoid the on-demand administration, even if the IIEF-5 results are lower than the combination group. Moreover, in the all three Groups, patients reported an increasing of the frequency of spontaneous nocturnal penile tumescence: +47% in Group 1, +79% in Group 2 and +56% in Group 3.
3.4. Adverse Effects
Patients treated with Icarifil® alone reported a lower prevalence of adverse effects in comparison with Icarifil® in association with tadalafil or tadalafil alone. In the association group and tadalafil alone group 7 and 8 patients reported mild adverse effects, respectively. These adverse effects did not require the treatment discontinuation (lower back pain).
Discussion
4.1. Major Finding
Here, we demonstrated that Icarifil® seems an interesting therapeutic approach to patients affected by mild–moderate erectile dysfunction and in all patients in which an improvement of clinical efficacy of tadalafil 5 mg daily use is needed. Moreover, the use of Icarifil® seems also represent an interesting alternative treatment in patients experiencing adverse effects or with contraindications for chronic treatment with PDE5-is.
4.2. Results in Comparison with Other Studies
Several phytotherapy compounds have been, recently, introduced in everyday clinical practice for managing patients affected by ED. The interest among reasearchers and clinicians for phytotherapy and nutraceuticals in the management of ED is increasing in the last years. It is due to the high cost of PDE5-is, the lack of responsiveness in patients with certain comorbidities, and related adverse events of PDE5-is [18]. In this scenario a new natural mixture, Icarifil®, has been introduced in the pharamacological market for modulating the to the nitric oxide/cyclic guanosine 3’5’-monophosphate (NO-cGMP) system and improve erectile function. Amante C. et al. demonstrated that this compound is able to inhibit PDE5 levels higher than 65% compared to the control and 35% compared to a control mixture of L-Citrulline and L-Carnitine [10]. The clinical efficacy of Icarifil® is due to the specific pharmacological properties of each singular component [10]. L-Citrulline is metabolized and conversed in Arginine, that represents a precursor of nitric oxide [18,20]. The choice to use L-Citrulline rather than Arginine is due to the fact that Arginine shows reduced bioavailability due to a significant intestinal pre-systemic metabolization by arginases [21]. On the other hand, L-Citrulline is not metabolized by arginases [21]. Through the same NO/cGMP pathway, Panax ginseng is able to induce vasodilatation of the corpus cavernosum and improve the erectile function [22]. Erectile dysfunction is associated to aging through the penile fibrosis and decreasing smooth muscle and endothelial integrity. The preservation of endothelial function is essential in order to reduce the risk of ED. Icariin and erucine, derivates from Eruca vesicaria, are able to preserve penile hemodynamics, smooth muscle, endothelial integrity, and neuronal expression of nitric oxide synthetases [23] and cause myorelaxation and vasodilatory activity of the smooth muscles [24]. Moreover, Icariin and erucine are able to preserve the inactivation of nitric oxide by oxidative stress, too [24]. Finally, protodioscin, extracted from Tribulus terrestris, is a steroidal saponin precursor of androgens that has been also involved in the nitric oxide synthase pathway determining relaxation of the corpus cavernosum [25]. It may be the reason of the increased frequency of spontaneous nocturnal penile tumescence in patients treated with Icarifil®. Has been previously described that the frequency of decreased nocturnal penile tumescence is one of the most common symptoms highly suggestive of hypogonadism [26]. In this sense, the recovery of spontaneous nocturnal penile tumescence during the treatment with Icarifil®, is an indirect demonstration of the role of Tribulus terrestris in the improving androgens level. The pre-clinical and clinical efficacy of Icarifil® is due to three different mechanisms of action: one through the androgen pathway, one through the nitric oxide synthase pathway and one through the anti-ROS and endothelial and smooth cells integrity preservation pathway.
Recently, Mirone V et al. reported the results of a clinical study evaluating the role of a nutritional combination of Panax ginseng (500 mg), Moringa oleifera (200 mg) and rutin (50 mg) in the management of patients affected by ED [27]. They compared tadalafil 5 mg once daily plus nutritional supplement once daily with Tadalafil 5 mg plus placebo with the same administration schedule for 3 months. By using a two phases study, the authors concluded that IIEF-5 significant increase in the combination group, highlighting the antioxi-dant effects of moringa oleifera, ginseng and rutin and this can enhance the endothelial NO and cGMP production [27]. As reported in our study, Mirone V. et al. highlighted that some nutraceuticals compounds are able to improve the efficacy of tadalafil through the increasing of nitric oxide synthase pathway and endothelial and smooth cells integrity preservation. In our study, the higher increasing in IIEF-5, SEP, EHS and PROs questionnaires is probably due to the role of Tribulus terrestris that is able to enhance the endothelial response to PDE5is through the androgens pathway.
4.3. Strengths and Limitations of the Present Study
This study shows important aspects that should be considered, such as the study design and the use of a single phytotherapy compound. This study has been planned as randomized and controlled study that should be considered a strength of the study. Moreover, we use a single phytotherapy compound that has been, previously, tested by using an in vitro study, with interesting findings. On the other hand, the present study had a few limitations that should be considered: the small number of enrolled patients, even if useful for the statistical analysis and the non-blinded nature of the study.
5. Conclusions
In conclusion, the use of combination of L-Citrulline, L-Carnitine, Eruca vesicaria, Panax ginseng, Tribulus terrestris, Turnera diffusa, Taurine, Vitamin E, Zinc, named Icarifil®, seems an interesting therapeutic alternative in patients affected by mild–moderate erectile dysfunction. Moreover, Icarifil® is able to significantly improve the clinical efficacy of tadalafil 5 mg daily use and could be represent an interesting alternative treatment in patients experiencing adverse effects or with contraindications for chronic treatment with PDE5-is.
Author Contributions
Conceptualization, T.C. and F.P.; methodology, L.G. and G.L.; software, T.C.; formal analysis, C.M.; data curation, G.L., C.C., M.R.; writing—original draft preparation, T.C.; writing—review and editing, L.G. and A.P.; supervision, A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Regione Calabria, approval protocol number 258, 2019.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is unavailable due to privacy or ethical restrictions in accordance to Italian bylaw.
Conflicts of Interest
The authors declare no conflict of interest.
References
- La Croce, G.; Schifano, N.; Pescatori, E.; Caraceni E.; Colombo, F.; Bettocchi, C.; Carrino, M.; Vitarelli, A.; Pozza, D.; Fiordelise, S.; Varvello, F.; Paradiso, M.; Silvani, M.; Mondaini, N.; Natali, A.; Falcone, M.; Ceruti, C.; Salonia, A.; Antonini, G.; Cai, T.; Palmieri, A.; Dehò, F.; Capogrosso, P. Which patient may benefit the most from penile prosthesis implantation? Andrology 2022, 10(8):1567-1574. [CrossRef]
- Yafi, F.A.; Jenkins, L.; Albersen, M.; Corona, G.; Isidori, A.M.; Goldfarb, S.; Maggi, M.; Nelson, C.J.; Parish, S.; Salonia, A.; Tan, R.; Mulhall, J.P.; Hellstrom, W.J. Erectile dysfunction. Nat Rev Dis Primers 2016, 2:16003. PMID: 27188339; PMCID: PMC5027992. [CrossRef]
- Shamloul, R.; Ghanem, H. Erectile dysfunction. Lancet 2013, 381(9861):153–165. [CrossRef]
- Lewis, R.W.; Fugl-Meyer, K.S.; Corona, G.; Hayes, R.D.; Laumann, E.O.; Moreira, E.D. Jr.; Rellini, A.H.; Segraves, T. Definitions/epidemiology/risk factors for sexual dysfunction. J Sex Med 2010, 7(4 Pt 2):1598-607. PMID: 20388160. [CrossRef]
- https://www.marketdataforecast.com/market-reports/pde-inhibitors-market-revenue. Access on 3th, Febraury, 2024.
- Salonia, A.; Bettocchi, C.; Boeri, L.; Capogrosso, P.; Carvalho, J.; Cilesiz, N.C.; Cocci, A.; Corona, G.; Dimitropoulos, K.; Gül, M.; Hatzichristodoulou, G.; Jones, T.H.; Kadioglu, A.; Martínez Salamanca, J.I.; Milenkovic, U.; Modgil, V.; Russo, G.I.; Serefoglu, E.C.; Tharakan, T.; Verze, P.; Minhas, S.; EAU Working Group on Male Sexual and Reproductive Health. European Association of Urology Guidelines on Sexual and Reproductive Health-2021 Update: Male Sexual Dysfunction. Eur Urol 2021, 80(3):333-357. [CrossRef]
- Wang, J.; Song, J.; Song, G.; Feng, Y.; Pan, J.; Yang, X.; Xin, Z.; Hu, P.; Sun, T.; Liu, K.; Xu, W.; Wang, T.; Wang, S.; Liu, J.; Ruan, Y. Acetyl-L-carnitine improves erectile function in bilateral cavernous nerve injury rats via promoting cavernous nerve regeneration. Andrology 2022, 10(5):984-996. Epub 2022 May 1. PMID: 35420721.Gingseng. [CrossRef]
- Nobili, S.; Lucarini, E.; Murzilli, S.; Vanelli, A.; Di Cesare Mannelli, L.; Ghelardini, C. Efficacy Evaluation of Plant Products in the Treatment of Erectile Dysfunction Related to Diabetes. Nutrients 2021, 13(12):4520. PMID: 34960072; PMCID: PMC8707335. [CrossRef]
- Ștefănescu, R.; Farczadi, L.; Huțanu, A.; Ősz, B.E.; Mărușteri, M.; Negroiu, A.; Vari, C.E. Tribulus terrestris Efficacy and Safety Concerns in Diabetes and Erectile Dysfunction, Assessed in an Experimental Model. Plants (Basel) 2021, 10(4):744. PMID: 33920217; PMCID: PMC8069229. [CrossRef]
- Amante, C.; De Soricellis, C.; Luccheo, G.; Di Vernieri, A.; Luccheo, L.; Falcone, G.; Del Gaudio, P. Icarifil, a Natural Mixture Based on L-Citrulline and L-Carnitine as a Novel Multicomponent Nutraceutical to Modulate ROS and PDE5. Appl Sci 2023, 13, 12358. [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340:c332. PMID: 20332509; PMCID: PMC2844940. [CrossRef]
- Cappelleri, J.C.; Rosen, R.C.; Smith, M.D.; Mishra, A.; Osterloh, I.H. Diagnostic evaluation of the erectile function domain of the International Index of Erectile Function. Urology 1999, 54:346–351.
- Tang, Z.; Li, D.; Zhang, X.; Yi, L.; Zhu, X.; Zeng, X.; Tang, Y. Comparison of the simplified International Index of Erectile Function (IIEF-5) in patients of erectile dysfunction with different pathophysiologies. BMC Urol 2014, 14:52. PMID: 24996819; PMCID: PMC4094415. [CrossRef]
- Araujo, A.B.; Allen, K.R.; Ni, X.; Rosen, R.C. Minimal clinically import-ant differences in the vaginal insertion and successful intercourse items of the sexual encounter profile. J Sex Med 2012, 9(1):169-179. [CrossRef]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology 1997, 49(6):822-30. PMID: 9187685. [CrossRef]
- Goldstein, I.; Lue, T.F.; Padma-Nathan, H.; Rosen, R.C.; Steers, W.D.; Wicker, P.A. Oral sildenafil in the treatment of erectile dysfunction. Sildenafil Study Group. N Engl J Med 1998, 338(20):1397-404. [CrossRef]
- Cai, T.; Palumbo, F.; Liguori, G.; Mondaini, N.; Scroppo, F.I.; Di Trapani, D.; Cocci, A.; Zucchi, A.; Verze, P.; Salonia, A.; Palmieri, A. The intra-meatal application of alprostadil cream (Vitaros®) improves drug efficacy and patient's satisfaction: results from a randomized, two-administration route, cross-over clinical trial. Int J Impot Res 2019, 31(2):119-125. Epub 2018 Oct 15. PMID: 30323234. [CrossRef]
- Rhim, H.C.; Kim, M.S.; Park, Y.-J.; Choi, W.S.; Park, H.K.; Kim, H.G.; Kim, A.; Paick, S.H. The potential role of arginine supplements on erectile dysfunction: A systemic review and meta-analysis. J Sex Med 2019, 16, 223–234.
- Trinchieri, M.; Perletti, G.; Magri, V.; Stamatiou, K.; Cai, T.; Montanari, E.; Trinchieri, A. Erectile and Ejaculatory Dysfunction Associated with Use of Psychotropic Drugs: A Systematic Review. J Sex Med 2021, 18(8):1354-1363. Epub 2021 Jul 8. PMID: 34247952. [CrossRef]
- Aguayo, E.; Martínez-Sánchez, A.; Fernández-Lobato, B.; Alacid, F. L-Citrulline: A Non-Essential Amino Acid with Important Roles in Human Health. Appl Sci 2021, 11, 3293.
- Cormio, L.; De Siati, M.; Lorusso, F.; Selvaggio, O.; Mirabella, L.; Sanguedolce, F.; Carrieri, G. Oral L-citrulline supplementation improves erection hardness in men with mild erectile dysfunction. Urology 2011, 77, 119–122.
- Choi, Y.D.; Park, C.W.; Jang, J.; Kim, S.H.; Jeon, H.Y.; Kim, W.G.; Lee, S.J.; Chung, W.S. Effects of Korean ginseng berry extract on sexual function in men with erectile dysfunction: A multicenter, placebo-controlled, double-blind clinical study. Int J Impot Res 2013, 25, 45–50.
- Ciccone, V.; Piragine, E.; Gorica, E.; Citi, V.; Testai, L.; Pagnotta, E.; Matteo, R.; Pecchioni, N.; Montanaro, R.; Di Cesare Mannelli, L.; et al. Anti-Inflammatory Effect of the Natural H2S-Donor Erucin in Vascular Endothelium. Int J Mol Sci 2022, 23, 15593.
- Jupiter, R.C.; Yoo, D.; Pankey, E.A.; Reddy, V.V.; Edward, J.A.; Polhemus, D.J.; Peak, T.C.; Katakam, P.; Kadowitz, P.J. Analysis of erectile responses to H2S donors in the anesthetized rat. Am J Physiol Heart Circ Physiol 2015, 309, H835–H843.
- Gauthaman, K.; Ganesan, A.P.; Prasad, R.N.V. Sexual Effects of Puncturevine (Tribulus terrestris) Extract (Protodioscin): An Evaluation Using a Rat Model. J Altern Complement Med 2003, 9, 257–265.
- Porst, H.; Brock, G.B.; Kula, K.; Moncada, I.; Montorsi, F.; Basson, B.R.; Kinchen, K.; Aversa, A. Effects of once-daily tadalafil on treatment satisfaction, psychosocial outcomes, spontaneous erections, and measures of endothelial function in men with erectile dysfunction but naive to phosphodiesterase type 5 inhibitors. J Androl 2012, 33(6):1305-22. Epub 2012 Jul 12. PMID: 22790642. [CrossRef]
- Mirone, V.; Napolitano, L.; D'Emmanuele di Villa Bianca, R.; Mitidieri, E.; Sorrentino, R.; Vanelli, A.; Vanacore, D.; Turnaturi, C.; La Rocca, R.; Celentano, G.; Arcaniolo, D.; Cirino, G. A new original nutraceutical formulation ameliorates the effect of Tadalafil on clinical score and cGMP accumulation. Arch Ital Urol Androl 2021, 93(2):221-226. PMID: 34286560. [CrossRef]
Figure 1.
The figure shows the study schedule.
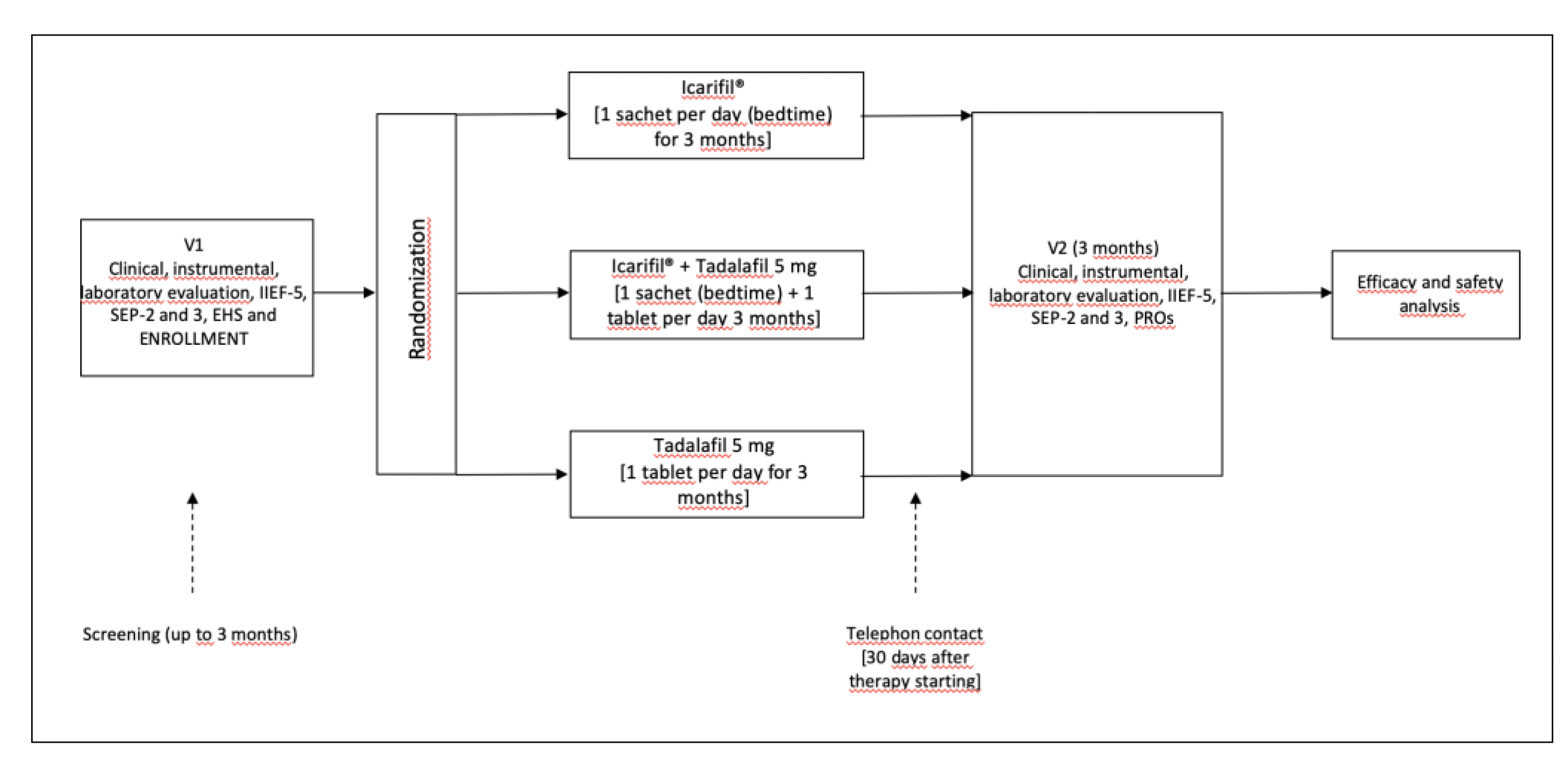

Table 1.
The table shows demographic, anamnestic, clinical and laboratory data of all patients at enrollment. BMI = Body Mass Index; IQR† = interquartile range.
Table 1.
The table shows demographic, anamnestic, clinical and laboratory data of all patients at enrollment. BMI = Body Mass Index; IQR† = interquartile range.
| Group 1 | Group 2 | Group 3 | ||
| p | ||||
| Number of enrolled patients | 51 | 50 | 51 | |
| Age (years) | 0.71 | |||
| Median (IQR †) | 51 (42-67) | 53 (43-66) | 53 (42-69) | |
| BMI (Kg/m2) | 0.72 | |||
| Median (IQR †) | 28 (26-30) | 27 (25–30) | 27 (26–31) | |
| Charlson Comorbidity index (CCI) | 0.12 | |||
| 0 | 49 (96.1) | 48 (96.0) | 50 (98.1) | |
| 1 | 2 (3.9) | 2 (4.0) | 1 (1.9) | |
| 2 | 0 (-) | 0 (-) | 0 (-) | |
| Number of sexual partners | 0.37 | |||
| 1 | 41 (80.3) | 39 (76.4) | 40 (78.4) | |
| 2 or more | 10 (19.7) | 11 (23.6) | 11 (22.6) | |
| Sexual partners age | 0.84 | |||
| Median (IQR †) | 48 (39-65) | 48 (38-66) | 49 (39-67) | |
| Duration of erectile dysfunction (months) | 0.91 | |||
| Median (IQR †) | 7 (6-9) | 8 (6-9) | 8 (6-9) | |
| Etiology of the disease | 0.09 | |||
| Organic | 5 (9.8) | 4 (8.0) | 5 (9.8) | |
| Psycogenic | 18 (35.3) | 20 (40.0) | 19 (37.2) | |
| Mixed | 28 (54.9) | 26 (52.0) | 27 (53.0) | |
Table 2.
The table shows all follow-up results according to the Groups in terms of questionnaires. IIEF-5 = Index of Erectile Function (IIEF); SEP = Sexual Encounter Profile; EHS = Erection hardness score; IQR† = interquartile range; * = difference between Group 2 and Group 1; # = difference between Group 2 and Group 3.
Table 2.
The table shows all follow-up results according to the Groups in terms of questionnaires. IIEF-5 = Index of Erectile Function (IIEF); SEP = Sexual Encounter Profile; EHS = Erection hardness score; IQR† = interquartile range; * = difference between Group 2 and Group 1; # = difference between Group 2 and Group 3.
| Group 1 | Group 2 | Group 3 | |||||
| p | |||||||
| Baseline | Follow-up | Baseline | Follow-up | Baseline | Follow-up | ||
| IIEF-5 |
<0.001* 0.82# |
||||||
| Median (IQR †) | 15 (13-15) | 19 (18-21) | 14 (13-15) | 23 (21-25) | 14 (13-15) | 22 (21-25) | |
| p | <0.003 | <0.001 | <0.001 | ||||
| SEP-2 |
<0.001* <0.001# |
||||||
| Positive response (%) | 19 (37.2) | 29 (56.9) | 19 (38.0) | 47 (94.0) | 20 (39.2) | 42 (82.3) | |
| p | <0.001 | <0.001 | <0.001 | ||||
| SEP-3 |
<0.001* <0.001# |
||||||
| Positive response (%) | 11 (21.5) | 30 (58.8) | 13 (26.0) | 47 (94.0) | 12 (23.5) | 43 (84.3) | |
| p | <0.001 | <0.001 | <0.001 | ||||
| EHS |
<0.001* 0.09# |
||||||
| Median (IQR †) | 2 (1-3) | 3 (3) | 2 (1-3) | 4 (3-4) | 2 (1-3) | 3 (3-4) | |
| p | <0.001 | <0.001 | <0.001 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



