
Submitted:
15 March 2024
Posted:
18 March 2024
You are already at the latest version
Abstract
Older adults with obesity have an increased risk for cognitive decline and subsequent Alzheimer’s disease. Previous research has focused on the impact of individual nutrients and overall dietary patterns to improve cognitive function. The Brain and Body Health (BB-Health) study aims to demonstrate the feasibility of a multicomponent nutritional supplement (MCNS) and weight loss (WL) intervention for individuals with overweight and obesity who are not consuming a healthy diet. BB-Health is a parallel-group randomized placebo-controlled 2x2 factorial pilot trial comparing the MCNS, WL, and MCNS+WL with a Control group. Eligible participants are 55 to 85 years of age with a body mass index 27.0 to 39.9 kg/m2. Major exclusion criteria include type 2 diabetes, moderate or severe cognitive impairment, and self-reported healthy dietary pattern. The BB-Health feasibility trial is registered as NCT05542199 at clinicaltrials.gov. The BB-Health objectives are to report: 1) recruitment and enrollment, including pace and descriptive statistics of the study sample; 2) adherence to the administered interventions; 3) successful data collection and performance of outcome assessments, including evaluation of change in key outcomes over time that are powered for this pilot study; and 4) summary statistics on outcomes for use in planning a subsequent, larger trial. The outcomes of interest are age-sensitive cognitive assessments, cerebral hemodynamics, and related health parameters. All measurements are collected at baseline, 3-, 6-, and 12-month visits. If the BB-Health protocol demonstrates feasibility, the novel MCNS with and without a parallel WL intervention has potential to be administered in a confirmatory randomized trial to evaluate ability to prevent age-related cognitive decline and improve brain health. The BB-Health Feasibility Study could significantly contribute to our understanding of the influence of diet and weight management on cognitive health
Keywords:
cognitive decline
; aging
; obesity
; nutrition
; clinical trial
; protocol
; Alzheimer's
; neurodegenerative
; food
Introduction
Declines in age-sensitive cognitive functions occur in most adults as they grow older[1] and are the primary risk factor for the development of Alzheimer’s disease (AD) and other forms of dementia.[2] Although the severity of cognitive decline is variable, approximately 50% of adults older than 65 who exhibit reduced cognitive function will develop dementia within five years.[3,4] It is further estimated that the number of people living with dementia will increase from 57.4 million to 152.8 million cases globally from 2019 to 2050,[5] and preserving cognitive function in an increasingly older population is a global public health priority. Multiple lifestyle factors are known to impact the onset and progression of cognitive impairment,[6] presenting modifiable targets that could alleviate the burden of age-specific cognitive decline.
Individuals with overweight or obesity are especially vulnerable to major cognitive decline, dementia, and AD.[7,8,9,10,11,12,13] Obesity in particular is now considered a modifiable risk factor for dementia[6] because carrying excess weight may increase vulnerability by accelerating the cognitive aging process.[2] Individuals with obesity are also more likely to consume a lower-quality diet, and importantly, accumulating evidence suggests that improvements in nutrition might attenuate the rate of age-related cognitive decline.[14,15,16] In addition to poor diet, exercise is known to play a role in improving cognitive function and to prevent cognitive decline in healthy adults.[17,18]
Recent epidemiologic studies demonstrate positive associations between several dietary patterns and reduced progression of cognitive decline in old age, including consuming a healthy diet[19,20,21,22] and adherence to the Mediterranean[23] and MIND (Mediterranean-DASH Intervention for Neurodegenerative Delay) [24] dietary patterns. These patterns are typically characterized by high consumption of whole fruits and vegetables, fish, olive oil, nuts, whole grains, and legumes and are hypothesized to improve cognitive health due to routine, sufficient intake of essential nutrients, and anti-inflammatory and antioxidant components. Indeed, a recent meta-analysis of 56 studies of dietary patterns suggested that there may be stronger benefits from a MIND or Mediterranean-style dietary pattern compared with the U.S. Dietary Guidelines.[25] Regular intake of a diversity of specific nutrients, including choline,[26] vitamin E,[27] omega-3 fatty acids,[28] and cocoa,[29,30,31] have additionally been associated with beneficial cognitive effects in older adults. Taken together, these nutrients are hypothesized to promote cognitive improvements through beneficial effects on inflammatory markers and a reduction in reactive oxygen species,[32,33,34,35,36] as well as an increase in cerebral blood flow (CBF).[37,38,39,40,41] However, not all epidemiological studies report significant associations with observed intakes.[42,43] In addition, a recent MIND diet randomized trial demonstrated no significant effect, perhaps reflecting the difficulty of achieving sustainable dietary change through conventional behavioral approaches. However, to our knowledge, no interventional research has assessed the effect of a comprehensive multi-component nutritional supplement on cognition, which may be a more feasible method to implement long-term dietary change.
Identifying nutritional and lifestyle interventions that slow or prevent cognitive decline and neurodegeneration in older adults would have great societal value and reduce the number of individuals who become eligible for emerging drug treatments.[44] This paper describes the objectives of the Nutrition for Brain and Body Health (BB-Health) Feasibility Trial, a 12-month pilot randomized controlled trial designed to evaluate a comprehensive nutrition supplement and participation in a behavioral weight loss (WL) program in older adults with overweight or obesity. A SPIRIT (Standard Protocol Items: Recommendations for Interventional Trials) schedule of enrollment, interventions, and assessments is provided in Figure 1.
The working hypothesis is that comprehensive nutrition, supplied across four major areas of cerebral nutrition needs, creates a favorable brain milieu with no limiting nutritional factors to hamper the brain’s neuroregenerative potential. Our conceptual model is displayed in Figure 2, illustrating optimal nutritional support for the brain and consequent cognitive processes via a multi-component nutrition supplement (MCNS) in older adults with overweight and obesity. This model postulates that a single limiting nutritional factor has the potential to impede the collective work of supporting brain health, with potentially synergistic effects of a behavioral WL intervention.
Specific Aims and Hypotheses
Data collected during the BB-Health Feasibility trial will be used to support an NIH proposal for a fully- powered randomized trial with the primary hypothesis that improvements in cognitive function will occur with randomization to MCNS, WL, and MCNS+WL compared to a Control condition, with the greatest improvements occurring in the MCNS+WL participants. The primary objectives of the BB-Health Feasibility trial are to report: 1) recruitment and enrollment, including pace of recruitment and descriptive statistics of the study sample; 2) adherence to the allocated interventions; 3) successful data collection and performance of outcome assessments, including evaluation of change in key outcomes over time that are powered for this pilot study; and 4) summary statistics on outcomes for use in planning a subsequent, larger trial. We report herein the main design features of the BB-Health trial, including the study population, eligibility criteria, an overview of the intervention, and the frequency of outcome assessments.
Materials and Methods
The BB-Health study was approved by the Institutional Review Board at Tufts University. All participants provided written informed consent prior to enrollment in the study. The BB-Health Feasibility trial was prospectively registered at ClinicalTrials.gov (NCT05542199).
Study Design
This is a parallel-group randomized placebo-controlled 2x2 factorial trial to examine cognitive function, cerebral hemodynamics, and other health outcomes (e.g., weight loss, biospecimens, and self-reported health). Older adults (age 55 to 85 years) with overweight or obesity (body mass index [BMI] between 27.0 kg/m2 and < 40 kg/m2) were randomized to receive: 1) the MCNS alone; 2) the behavioral WL intervention alone (with placebo MCNS); 3) the MCNS with the behavioral WL intervention (MCNS+WL); or 4) a Control condition (placebo MCNS, no WL intervention). All interventions have a study duration of 12 months. Study outcomes were assessed at baseline, 3 months, 6 months, and 12 months. An overview of the study design is provided in Figure 3.
Setting and Recruitment
The BB-Health Feasibility Trial was conducted at the Jean Mayer USDA Human Nutrition Research Center on Aging (HNRCA) at Tufts University. Participants were recruited (July 1, 2022 to January 31, 2023) using several strategies by the research team and the HNRCA Volunteer Services unit. These included local print and electronic media (e.g., advertisements in newspapers, newsletters, bulletin boards, websites, and social media) as well as posting flyers in public places, such as local senior centers, health centers, supermarkets, libraries, laundromats, and local community organizations. The research team also gave informational presentations at local organizations and hosted information tables at these organizations and public meetings. Volunteer Services additionally has an existing roster of >40,000 potentially qualifying men and women who can be contacted using direct mailings if their age and BMI fall within the study’s inclusion criteria as outlined below.
Participants
Inclusion Criteria
Adult men and women 55 to 85 years of age; BMI of 27.0 kg/m2 to 39.9 kg/m2; score of 34 or greater on the Modified Telephone Interview for Cognitive Status (TICS-M); willingness to be randomized and participate in all study activities, including daily consumption of supplemental MCNS and attending scheduled outcome assessments; participating in WL intervention and using the provided home wireless scale and activity monitor; satisfactory screening review of health history questionnaire by nursing staff, including verbal confirmation of completing a course of vaccination against COVID-19 (two doses plus one booster); having access to a computer or smartphone with wireless and possessing a freezer at home with sufficient space for MCNS storage.
Exclusion Criteria
Ineligibility based on age, BMI, or baseline cognitive status; consuming ≥ 2 servings of fatty fish per month; routine consumption of a multivitamin, cacao/cocoa supplement, choline supplement, omega-3 fatty acids docosahexaenoic acid (DHA)/eicosapentaenoic acid (EPA) supplement, or any supplement advertised for brain health or cognitive function; dislikes or reports consuming > 1 serving per week of 60% chocolate or cocoa; significant health conditions including severe cardiovascular disease, history of neurological brain disease or traumatic brain injury (e.g., injury with loss of consciousness), history of major psychiatric disorder, inadequately controlled hypertension, diabetes (type 1 and type 2) or use of any pharmacologic treatment for diabetes or hemoglobin A1c (HbA1c) > 6.5%, history of stomach or bowel resection, bariatric weight loss procedure, gastrointestinal disease or conditions known to influence absorption, chronic kidney disease or history of kidney stones, history of diagnosed eating disorders, active treatment for cancer of any type in ≤ 3 years (excludes non-melanoma skin cancer), thyroid disease or other significant endocrine disorder, uncontrolled hypercholesterolemia, history of acute or chronic pancreatitis or gallbladder disease, metabolic disorders or conditions that interfere with nutrient absorption, dose adjustment to statin or antihypertensive medication within 3 months, screening lab results outside normal parameters that may interfere with study outcomes at the discretion of the study physician, inadequate venous access or history of a bilateral mastectomy with nodal dissection, history of inflammatory diseases; active WL or weight change > 4 kg in the past 6 months; consuming a restrictive diet (e.g., gluten-free, vegan); reports consumption of > 2 alcoholic drinks per day; reports consumption of > 2 cups of green or black tea per day; reports use of recreational or illegal drugs; reports regular smoking or vaping tobacco or marijuana including the use of edibles within the last 6 months; unwilling to use a mobile phone or computer with videoconference software to participate in intervention group meetings and adherence assessments; unwilling to consume MCNS on camera for weekly adherence assessment; non-English speakers; no social security number.
Screening
A series of screening steps were conducted to implement comprehensive screening with minimal researcher burden, progressing from telephone screening to in-person screening. Potential participants were first screened for eligibility via telephone by research staff. One or more screening telephone interviews ensured that the volunteers were fully aware of all study activities, the full participant study burden, and exclusion criteria. A health history was conducted as part of this screening phase, as well as a cognitive screen, BMI screen, and preliminary diet screen.
If a potential participant was eligible during the initial phone screening, they were invited to an in-person screening visit to further assess eligibility. During the screening visit, written informed consent limited to the screening visit was obtained. Potential participants underwent routine blood tests, weight and height were measured, and the inclusion and exclusion criteria were reviewed. At screening, prospective participants also sampled a representative food with characteristics of the MCNS and were required to rate the food at least 4 on a 5-point scale and report that they were willing to consume the MCNS daily.
In the following 1-2 weeks, participants underwent three 24-hour dietary recalls on random days (i.e., two weekdays and one weekend day). to confirm their ability to give a plausible dietary record and to ensure that their intake fits the inclusion and exclusion criteria. The average energy intake for the dietary recalls were within a plausible range for all enrolled participants. Individuals who met all eligibility criteria were invited to enroll in the study with an additional informed consent procedure and undergo baseline assessments followed by randomization.
The first participant was enrolled on September 13, 2022, and completed the study on August 15, 2023. The final participant enrolled on March 20, 2023, and is scheduled to complete the study on March 1, 2024.
Randomization and Blinding
Randomization occurred after the completion of baseline testing. Participants were randomized in a 1:1:1:1 allocation and remained in their randomized group throughout the entire study. Randomization was stratified by age (55-69; 70-85) and BMI (27-32.9; 33-39.9). The built-in random number generator included in the Research Electronic Data Capture (REDCap) randomization module was used to randomly assign participants to one of the four study conditions: MCNS, WL, MCNS+WL, or Control.
For the MCNS supplement, only the Bioinformatics team leader and Metabolic Research Unit kitchen staff had access to the randomization schema. For the WL intervention, the Research Coordinator, Principal Investigator, Study Physician, interventionists, and participants were unblinded to their randomized assignment into the WL intervention but remained blinded for assignment to MCNS group assignment. The participants, research staff conducting outcome measurements, and statistician were blinded throughout the study except for above and when safety events require unblinding.
MCNS Intervention
Specific components of the MCNS are commercially available and are widely used by Americans, and therefore no investigational device exemption was required for use of the supplement. These components included epicatechin and epigallocatechin in green tea and cacao,[45,46,47,48,49,50,51] the cocoa-based product Cocovia as cocoa is the food with the strongest evidence for beneficial effects on brain health via reducing inflammation, [34,39,52,53,54,55,56,57] as well as omega-3 fatty acids DHA and EPA, which could theoretically improve brain health by the following mechanisms: suppression of inflammation via effects on fatty acid composition of cell membranes[35,36] and increased cerebral blood flow (CBF).[37,38,39,40] In addition, the MCNS includes essential micronutrients, specifically choline, that are consumed in generally inadequate amounts by U.S. older adults.[58] In addition to high nutrient density, low energy density (<200 kcal per serving), portability, and long-term storage, five considerations were applied to developing the MCNS: a) fidelity to the intervention requirements as outlined below; b) acceptability to participants (e.g., palatability and convenience); c) hunger suppression (as this is a population with overweight and obesity); d) multiple flavors and flexible ways to consume the food to leverage the science of dietary variety[59] to support high levels of adherence; e) food safety.
Three palatable food concentrates containing ~200 kcal/daily serving were developed. They contain a minimum of 990 mg total cocoa flavanols,[60,61] with a high-satiety profile to support weight management (10 g protein + 5 g fiber).[62,63,64] Based on prior studies of cognition, additional composition specifications are: 1600 mg DHA and 400 mg EPA;[65] 550 mg choline; >250 mg epicatechin and epigallocatechin; multivitamin/mineral supplements providing 75% all micronutrients except calcium (to prevent competitive absorption with other divalent cations).
The MRU at the HNRCA prepared the MCNS. Participants came to the center every four weeks to collect their supply of portioned daily servings and keep them in their freezer prior to daily consumption. The supply was provided as a frozen concentrate in individual plastic cups with lids. Multiple preparation methods were outlined for participants to enable the use of the concentrate as a reconstituted health shake, eaten thawed but otherwise unprepared as a pudding, or frozen and otherwise unprepared as a popsicle. All the supplements have similar composition and are interchangeable, allowing participants to request the flavors of their choice. The experimental MCNS is made with commonly available consumer products.
MCNS Control
An isocaloric control designed to imitate the color, taste, and texture of the active concentrate with the same range of applications was designed with a base of canola oil and smaller quantities of a culinary cocoa-alternative with a different flavonoid composition, and low or undetectable concentrations of the phenolic compounds of interest.[60] These placebos are also food concentrates, with equivalent palatability and appearance to the active intervention foods, and are also made with commonly available consumer products.
Weight Loss Intervention
For the WL intervention, an interventionist blinded to supplement randomization implemented a remote version of the behavioral intervention in the CDC-recognized Diabetes Prevention Program (DPP), which involves a total of 22 meetings: weekly meetings for 13 weeks, two to four biweekly meetings, and monthly group meetings thereafter, based on online materials.[66] The program utilized food logging, self-weighing, and activity monitoring with the support of wearable fitness devices and an online fitness dashboard. Starting Week 1, goals for exercise (5000 steps/day) and diet (calorie control with healthy food plan) were implemented in parallel with targets changing at increments throughout the intervention. We offered videoconference sessions[67] that were delivered by a member of the study team who completed the online DPP training. We also included regular individual check-ins by email, videoconference, or phone or text as in our previous use of this method.[67] Because the study featured rolling enrollment, new participants had individual or small-group meetings for 1-4 weeks before joining larger group sessions. Participants were assigned to group meetings without consideration of supplement randomization.
Meeting content and delivery were implemented consistent with our previous work after interventionist training.[68] Twenty-two weeks of DPP behavioral intervention content have been used by our team in a videoconference-delivered intervention for military families in five US states;[69] these materials, with updates to support remote delivery to older adults, were used. Meeting attendance, adherence to self-monitoring activities, and all contact with participants were tracked by the interventionist. In this study, participants were provided with information supporting consumption of foods in the Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diet, such as berries and green leafy vegetables.[24] They also received a set of measuring cups and a calorie-counting book for daily use. Each participant received a Wi-Fi-enabled scale (Fitbit Aria Air) and a wrist-worn activity monitor (Fitbit Inspire 2) to facilitate tracking for weight and activity. These tools and circumstances were only applicable to participants randomized to the WL intervention. No similar devices were provided to the WL control.
Weight Loss Control
Participants who were not assigned to the immediate WL group were wait-listed to receive a 12-week version of the DPP WL intervention after the end of the 12-month trial. They were instructed to continue with their current lifestyle activities during the study.
Monitoring Participant Adherence to the Administered Interventions
Adherence metrics for the MCNS/placebo were derived from weekly logs of food and supplement consumption plus 1 day/week videoconference monitoring for the first six months, and 1 day/month thereafter. Adherence metrics for the WL intervention included physical activity goal attainment, food logging, self-weighing, attendance, active engagement in sessions, and caloric intake goal attainment. Wireless scales and wrist-worn activity monitors were provided for remote data collection with daily use to reduce participant burden related to activity tracking. Participants connected their devices to personal cellphones for ease of use, self-monitoring, and data retrieval.
Data collection and Measures
Procedures and Training
All research team members involved in data collection were trained to ensure high-quality, standardized assessment procedures. A detailed manual of procedures was developed for all study measures. Data were collected at baseline, 3 months, 6 months, and 12 months.
Measures
An overview of all study measures and time points is presented in Table 1.

Table 1.
Brain and Body Health (BB-Health) Feasibility Trial measures and data collection.
| Measure | Screening | Baseline | 3-month | 6-month | 12-month |
|---|---|---|---|---|---|
| Demographics | x | ||||
| Medical history | x | ||||
| Anthropometry | |||||
| Height (cm) | x | ||||
| Weight (kg) | x | x | x | x | x |
| Blood pressure (mmHg) | x | x | x | x | x |
| Pulse (BPM) | x | x | x | x | x |
| Biological samples | |||||
| Blood | x | x | x | x | |
| Urine | x | x | x | x | |
| Cerebral hemodynamics | |||||
| Fasted | x | x | x | x | |
| Post-prandial | x | x | x | x | |
| Cognitive assessments | |||||
| Auditory Verbal Learning Test (AVLT) | x | x | x | x | |
| Controlled Oral Word Association Test (COWAT) | x | x | x | x | |
| Single Digit Modalities Test (SDMT) | x | x | x | x | |
| Stroop Interference Test | x | x | x | x | |
| Trails Making Test (A) | x | x | x | x | |
| Trails Making Test (B) | x | x | x | x | |
| NIH Toolbox (NIH-TB) | x | x | x | x | |
| Dietary | |||||
| Multi-pass 24-hour recall | x | x | x | x | |
| Questionnaires | |||||
| 36-Item Short Form Health Survey (SF-36) | x | x | x | x | |
| Adult Eating Behavior | x | x | x | x | |
| Center for Epidemiologic Studies Depression Scale (CES-D) | x | x | x | x | |
| Cognitive & Leisure Activity Scale (CLAS) | x | x | x | x | |
| Community Healthy Activities Model Programs for Seniors (CHAMPS) | x | x | x | x | |
| Factors Influencing Food Choice (FCQ) | x | x | x | x | |
| General Nutrition Knowledge Survey | x | x | x | x | |
| Sarason Social Support (SSQSR) | x | x | x | x | |
| Self-Regulation of Eating Behavior (SREBQ) | x | x | x | x | |
| Stigmatizing Situations Inventory | x | x | x | x | |
| Three-Factor Eating (TFEQ) | x | x | x | x | |
| Weight-Striving Stress Scale | x | x | x | x | |
| Yale Food Addiction Scale | x | x | x | x |
- Cognitive function (primary outcome). Assessments of cognitive function were derived from performance on well-established neuropsychological tests and the NIH-Toolbox cognitive module. All cognitive assessments were completed at baseline, 3 months, 6 months, and 12 months at 30 minutes postprandial. Five standardized scores from five tests were obtained and summed to yield a composite executive function z-score as the primary outcome. These tests include: Controlled Oral Word Association Test (COWAT),[70,71] Single Digit Modalities Test (SDMT),[72] Stroop Interference Test (Stroop),[73] Trails Making Test (TMTA, B).[74,75] The Auditory Verbal Learning Test (AVLT): Total Learning and Delayed Recall[76] and the NIH Toolbox (NIH-TB) will also be administered and were considered secondary outcomes. A detailed overview of the cognitive assessments is presented in Table 2. All cognitive assessments were audiotaped for quality control and proper coding of verbal tasks and were reviewed by a member of the research team.
Table 2.
Details of BB-Health cognitive assessment measures.
| TEST | DOMAIN(S) ASSESSED | DESCRIPTION |
| Primary Outcomes | ||
| COWAT | Controlled response generation | Examines phonemic verbal fluency and response generation. Participants verbalize during 1-minute periods as many words as possible that begin with particular letters (e.g., H, O). The restriction of response set requires executive control and executive function for controlled response production. |
| SDMT | Working memory, focused attention, processing speed | Widely used and well standardized test speed and accuracy in the coding symbols associated with specific numbers is a highly sensitive tests of brain dysfunction. The final score is the total number of correctly entered symbols in 90 seconds. |
| Stroop | Executive inhibitory control, focused attention | Assesses the extent of slowing created by attentional interference created by the demand of naming colors that are discordant with the printed word of a different color. The score on the Color-Word interference trial is compared with scores on color word reading and color naming in the absence of interference. For each of the 3 tasks, scores are based on the number of colors correctly named in 45 seconds, with these scores computed to yield a Stroop Interference z-score. |
| TMT-A | Attention, speed of processing | Involves the use of a pencil to connect a series of numbers in ascending order that are distributed over a sheet of paper as quickly as possible. Completion time provides the performance measure that is converted to a z-score. |
| TMT-B | Attention and executive control – inhibition (set switching, processing speed) | Similar to Trail A, except that alternation of an ascending sequence between numbers and letters distributed over the page is required (e.g., 1-A-2-B…). The number-letter sequence is connected by pencil. Completion time provides the performance measure that is converted to a z-score. |
| Additional Outcomes | ||
| AVLT | Learning and memory | The AVLT is a verbal learning and memory test. A list of 15 words is presented to the participant over five trials with recall assessed immediately following each trial. Recall for these words is assessed after presentation of an interference list B after the five trials. Delayed recall of the first 15 word list is then assessed after a 15-minute interval. |
| NIH-TB | Fluid and crystalized cognitive function | The cognitive module of the NIH-TB was developed to assess fluid and crystalized cognitive functions via computerized (IPAD) administration. It takes 30-45 minutes to complete and contains seven primary tasks (Flanker Inhibitory Control and Attention Test, Dimensional Change Card Sort Test, List Sorting Test, Pattern Comparison Processing Speed Test, Picture Sequence Memory Test, Picture Vocabulary Test, and Oral Reading Test). |
- 2.
- Cerebral hemodynamics. Measures of cerebral blood flow (CBF) and oxygenation were collected at each study visit in fasted and two-to three-hours postprandial states. Microvascular CBF was measured using continuous-wave diffuse correlation spectroscopy (CW-DCS) equipped with a 785 nm laser source and four single-photon avalanche diode detectors, which provided a continuous index of blood flow (BFi).[77,78] A 3D-printed flexible sensing probe was designed with a short source-detector distance of 5 mm for scalp blood flow and two long distances of 25 and 30 mm for cerebral blood flow monitoring, which was connected to the DCS source and detectors and positioned on the subject’s forehead.[79,80,81] The DCS optical data were acquired at 150 MHz. On the opposite forehead, cerebral oxygenation was measured using near-infrared spectroscopy (NIRS), an established method which measures light attenuation due to absorption of hemoglobin to non-invasively monitor hemoglobin oxygen saturation in biological tissues.[82,83] This metric was also used as a surrogate measure of cerebral blood volume (CBV) changes. The NIRS was a battery-operated headband with source-detector distances of 8, 28, and 33 mm, made of 735 and 850 nm LED light sources and photodiode detectors on a flexible printed circuit board, as originally described.[84] The NIRS data were acquired at 266 Hz. Together, DCS and NIRS provide an array of cerebral hemodynamic biomarkers that uniquely characterize brain health and function. Respiratory pattern and EKG was recorded via Biopac. The acquired data were time-synchronized using the devices’ timestamps and common trigger signals.
- 3.
- Fasting duplicate measurements of weight were taken to ±0.1 kg at each study visit. Our standard protocol[85,86] requires the use of the same calibrated scale, and removal of shoes, outer clothing, and heavy items. Brachial systolic and diastolic blood pressure were measured after weight measurements, as an index of the effects of the supplements on cardiometabolic health. Three measurements were performed after a defined rest period, with the last 2 averaged.[86] An automatic blood pressure cuff was used, with cuff sizes based on each subject’s left arm circumference.
- 4.
- Biospecimens. Fasting blood samples (25 ml) were taken at baseline, 6, and 12 months, and processed for storage in our Clinical Laboratory Improvements Amendment (CLIA)-certified laboratory. Because of anticipated changes in blood glucose and insulin sensitivity,[87] HbA1c, fasting plasma glucose and fasting serum insulin levels were measured at each timepoint. Apolipoprotein E4 (ApoE4) genotypes also influence risk of AD and were measured in our core facility.[88,89] Fasting urine samples were also collected in order to evaluate adherence to supplement consumption by assessing catechin metabolites.
- 5.
- Self-reported health outcomes via validated questionnaires. Demographic variables and family history of dementia and AD were assessed at the start of the study and updated as relevant. In addition, health-related quality of life, functional activities, sleep, depression, eating behaviors, activity and activities of daily living were assessed, using NIH-recommended instruments when available.[90,91,92,93,94,95,96] A complete list of questionnaires is included in Table 1.
- 6.
- Dietary adherence. For dietary adherence, we used the multiple-pass interviewer-administered 24-hour dietary recall method.[97] In past studies, we have achieved 90% accuracy relative to gold-standard assessments with this method.[98] Three daily recalls were performed on random days by telephone at screening (to determine if plausible records can be obtained[99]) and these data were used as baseline data for enrollees. Three recalls were collected on random days after each visit at the 3-, 6- and 12-month timepoints. The collected data includes efforts to obtain both general dietary intake information for the period of collection and specific information relevant to this study (e.g., type of chocolate consumed, if any). The records will be analyzed to quantify daily nutrient intakes and intakes of nutrients of particular interest (cocoa polyphenols, DHA+EPA, % adequacy of micronutrients relative to Dietary Reference Intakes), using Nutrition Data System for Research software (Nutrition Coordinating Center, University of Minnesota, Version 2021 or latest). Information will be used to calculate a Healthy Eating Index score[100] and a MIND diet score,[24] which will be used as metrics for adherence to the dietary recommendations of the WL intervention.
Participant Rights and Safety
The BB-Health Feasibility trial is being conducted in accordance with the tenets of the Declaration of Helsinki. All participants review and sign an informed consent form prior to completing any study-related assessments and are advised that they may withdraw from the study at any time and for any reason. Oversight of the BB-Health Feasibility trial is provided by a data and safety monitoring board (DSMB) that is independent of the study sponsor. Members were approved by NIH prior to committee formation and provide NIH with their independent report on study progress. The study protocol (including amendments) is reviewed and approved by the Institutional Review Board at Tufts University. Reports summarizing participant safety and adverse events are presented to the DSMB every 6 months. The occurrence of adverse events is inquired about during each study visit and during each videoconferencing session. Adverse events are promptly reported to the study physician on a schedule defined by the Tufts IRB, including serious adverse events within 24 hours.
Power Calculations
Statistical power was calculated using simulations based on a mixed-effects linear model with subject-specific random intercepts and fixed effects for group, time, and group by time interaction using outcome-specific correlations among the four repeated measures. The primary outcome is age-sensitive cognitive composite z-score based on well-established standardized scores on 5 neuropsychological tests: Controlled Oral Word Association Test (COWAT),[70,71] Single Digit Modalities Test (SDMT),[72] Stroop Interference Test (Stroop),[73] Trails Making Test (TMTA, B).[74,75] Secondary endpoints are cerebral hemodynamics (i.e., CBFi measured with NIRS/DCS and macrovascular CBFV measured with TCD) during fasting and postprandial states. We aimed to screen 144 participants (all at Tufts), enroll and randomize 48 participants, and have at least 36 completers.
Primary outcome: In a previous study, high cocoa flavanol supplementation (8 week change=0.7, SE=0.03, n=30) improved cognition z score 0.63 units more than the low flavanol group (8 week change=0.1, SE=0.07, n=30).[53] In a 12-month diet and exercise study, where the diet-only group is similar to WL group in this study, the diet-only group (12 month change=1.7, SE=0.4, n=26) improved 3MS by 1.5 compared to the control group (12 month change=0.1, SE=0.4, n=27).[101] With 50 subjects per group, we have 87% statistical power for the omnibus test for group effects (time by group interaction term in the mixed-effects model) for changes in the cognitive z-score of 0.31 between control group compared to each of MCNS and WL arms.
Secondary Outcomes: In a previous 12 month study, mean for overall perfusion increased from 74.4 ml/100g/min (SE=1.7, n=107) at baseline to 87.0 ml/100g/min (SE=2.4, n=107) at 12 months.[102] The sample size yields 80% power to detect 12.6 ml/100g/min change in CBF in MCNS and WL arms. Neurovascular coupling (NVC%) was reported in a previous 30-day cocoa intervention to measure blood flow velocity. NVC had an 8% difference between flavanol-rich and flavanol-poor groups (5.6%, SD=7.2% vs. -2.4%, SD=4.8%; n=17) in those with impaired NVC at baseline.[103] For CBFV, the sample size yields 82% power to detect 5% change in neurovascular coupling in MCNS and WL arms. Power calculations for all outcomes assume 25% additive increases in the MCNS+WL combined treatment group over treatment arms with individual agents. As this is a pilot study, no multiple comparison correction is incorporated into the power calculations.
Data Management
This study will generate primary data consisting of recruitment and retention statistics, adherence metrics, and data on the primary and secondary outcomes: cognitive testing (administered electronically via tablet or using hard copy forms), cerebral hemodynamic data, electronic survey questionnaires, clinical measures (weight, vitals, cerebral hemodynamics, cognitive measures), multi-pass 24-hour dietary recalls, and blood measures. The cognitive and cerebral hemodynamic measures were captured using instrument-specific software. Other data were collected primarily through REDCap, a secure web-based portal for maintaining research-related data that includes features to ensure data quality. Dietary data were recorded separately, stored in NDSR, and copied into REDCap. We will utilize REDCap’s built-in features to ensure data quality, including features for data validation and data range functions to prevent entry of impossible values (e.g., negative body weight or implausible weight changes). All data entry was blinded to randomization, and raw scores were entered in duplicate into REDCap by two different individuals. Hard copies and/or electronic records of all responses on tests were stored as backup.
Statistical Analysis Plan
The primary analysis by intention-to-treat will include all randomized participants in their assigned treatment arm. Treatment effects of MCNS, WL, and combined MCNS+WL will be estimated through contrasts for comparisons between 1) MCNS vs. control, 2) WL vs. control, and 3) MCNS+WL vs. control in the primary analysis.
Cognition (Primary Outcome)
Cognitive tests were administered at baseline, 3, 6, and 12 months. Duplicate measures on separate days were obtained at baseline and averaged. The overall z-score will be computed by converting log-transformed scores from the individual tests to standardized scores (all individual tests except for global cognition), summing the individual tests and rescaling to obtain a standardized composite score as the primary outcome. The intervention effect will be tested using linear mixed-effects linear models to partition the fixed effects of treatment group, time, and their interaction. Subject will be included as a grouping term and a random intercept will be included in the model. Statistical significance will be set at a two-sided alpha of 0.05. The primary hypothesis will be tested by assessment of the interaction term between treatment group and time, assuming a linear time trend which tests the overall group effect (omnibus test) between all 4 arms. Planned comparisons will be estimated after the fitting of the model using contrasts with Dunnett’s method to control experiment-wise type I error rate. Sphericity assumption will be examined using Mauchly’s test and variable transformations will be applied for outcomes that do not satisfy linear modeling assumptions of normality. We will report primary analysis results from minimally adjusted models as recommended in CONSORT guidelines,[104] adjusted for stratifying variables (age and BMI) and baseline outcome measure only. Additional covariates will be used in sensitivity analyses to increase precision in the estimated treatment effect and address potential confounding including sex, ApoE4 variant, education, race/ethnicity, presence of a known risk factor for accelerated cognitive decline (any of the following diabetes, hypertension, family risk of dementia or AD before 60), physical activity, and any subject characteristics found to be imbalanced at baseline. Treatment effects by sex and ApoE4 gene will be estimated and reported from analyses.
Cerebral Hemodynamics (Secondary Outcomes)
CBFi and CBFV were measured in fasting state and fed state on each study visit. Acute effects of the interventions will also be explored using repeated measures ANOVA (within-subject change between fasting and fed states on a single day) in subgroup analysis by intervention. If there are no significant differences between the two states, an average of each will be used for analyses, while if differences are observed the measurements will be analyzed separately. The statistical modeling approach for CBFi and CBFV will be implemented in the same way as described for the primary outcome. Statistical significance will be set at a two-sided alpha of 0.05 for each cerebral hemodynamic outcome and no multiple comparison adjustment will be applied as these are secondary outcomes. Descriptive outcomes (changes in cardiometabolic health, self-reported health, and activities of daily living) will be summarized by randomized intervention group.
Time-Course Effects and Adherence (Exploratory Outcomes)
To examine the pattern of intervention effects over time for all cognitive variables, CBFi, and CBFV, nonlinear time trends within the mixed-effects models will be fit using restricted cubic splines or polynomial terms, and their use will be informed by local regression smoothing plots. Exploratory per-protocol analysis will be conducted excluding low-adherent participants.
Predictors of Cognitive and Cerebral Hemodynamic Responses (Exploratory Outcomes)
Predictors of cognitive and cerebral hemodynamic responses will be identified using association analysis. Predictors in consideration include adherence for the intervention, measured dietary intake of constituents of the MCNS (flavanol, vitamins, and omega-3 fatty acids), and cardiometabolic measures (including blood pressure, lipid panel, HbA1c, type 2 diabetes, obstructive sleep apnea, and genetic variants of the ApoE4 gene). Multiple linear regression models will be used with adjustment on the intervention group.
Individual Cognitive Functions (Exploratory Outcomes)
Assessment of individual cognitive functions will be performed using the modeling approach described for the primary outcome.
Discussion
Due to rapid growth in the population of older adults, strategies specific to reducing the increasing burden of cognitive decline[5,105,106] are a global public health priority and are critical to a healthy and successful aging process.[107] Older adults will spend a comparatively larger proportion of their lives at an older age compared to previous generations and consequently have a marked increase in their risk of developing an age-related chronic disease.[108,109] Extending the healthspan, or the number years spent in good health,[110] is therefore critically important. While great interest in compromised cognitive health is a top public health and research priority, the extent to which nutritional components can help alleviate this burden has not been determined.
We recently reported the benefit of an MCNS approach for undernourished children,[111,112] and observed significant improvements in cognitive function and CBF during a six-month intervention. While this work was not conducted in older adults with obesity, similar principles of comprehensive nutrition theoretically apply to children and adults, particularly because both groups have low micronutrient intakes[113,114] and are known to have a vulnerability to cerebral inflammation and oxidative damage[115,116,117,118,119,120] that amplify risk for cognitive impairment.
The prevalence of overweight and obesity in adults is high (currently >70% of adults over age 60 years have overweight and >40% have obesity).[121] Multiple factors are thought to be important to the etiology of obesity-related cognitive impairment in older adulthood. The brain has the highest energy expenditure per unit mass of any organ, and structural and functional integrity of the brain depends on high blood flow to ensure an adequate supply of nutrients and oxygen plus structural building blocks for synthesis of neurotransmitters and remodeling and repair of brain tissues.[80,122,123] Cerebral blood flow (CBF) is therefore suspected to be a core biomarker of cognitive health,[39,80,124] especially since declining CBF precedes longer-term changes in cognition.[125] The reduced CBF observed in obesity[126] is likely both a cause and a consequence of neuronal death, resulting in a negative cycle of obesity and reduced CBF contributing to progressively worsening cognitive impairment.[123] Common comorbidities associated with obesity, including hypertension and sleep apnea, cause additional reductions in CBF,[8,127,128,129,130] and several of the biochemical processes associated with dementia and AD appear to share common mechanisms with cerebrovascular disease markers.[130,131,132] Vascular etiologies increase AD risk, and reduced CBF occurring with AD is linked to amyloid deposition.[133,134,135,136,137] The aging brain is also susceptible to inflammation, oxidative damage, a negative cycle of reduced CBF, neuronal injury, and suppression of neurogenesis.[115,116,117,118,119] Systemic inflammation due to obesity is also harmful because it promotes cerebral inflammation and reduces the functionality of the blood-brain barrier.[138,139]
If proven efficacious, the novel MCNS has potential to attenuate age-related cognitive decline and improve brain health. The BB-Health Feasibility Study could significantly contribute to our understanding of the influence of diet and weight management. Further interventional studies will be needed to elucidate our understanding of the relationship between food components, weight loss, and cognitive health. This research is relevant to dietary recommendations for an older adult population, and our results will contribute to the long-term understanding of how nutrition modulates a variety of outcomes and may ultimately inform new preventative and therapeutic strategies.
Funding Sources
NIH R56AG065236; USDA Agricultural Research Service under Cooperative Agreement No. 58-1950-7-707. The study sponsors had no role in the study design, collection, or management of preliminary data, and had no role in the preparation of this manuscript nor the decision to submit for publication. Upon study completion, the study sponsor will have no role in the analysis or interpretation of data nor will they have a role in the preparation of additional manuscripts for submission.
Author Contributions
Conceptualization (SBR, SKD, RC, MAF, RES, SG, SD), funding acquisition (SBR, SKD, RC, MAF), investigation (SBR, SKD, RC, MAF, MCD, RES, SG, SG, LC, JS), methodology (SBR, RC, MAF, RES, SG, JS, KB), project administration (RES, SG, SG, SD), supervision (SBR, SKD, RC, MAF, LC), writing original manuscript draft (RES), review and editing (all authors).
Data Availability Statement
This manuscript describes the BB-Health Feasibility trial study protocol and does not report any data, including preliminary data. The data availability policy is therefore not applicable to this manuscript.
Acknowledgments
The authors would like to thank the BB-Health participants for their important contributions and support of this study.
Declaration of Interests: SBR is a named person on a U.S. Patent 17/475,513 (real/fram # 057755/0739) ‘Compositions and method for treating and preventing malnutrition’. Because of these potential conflicts, a Tufts management plan for SBR was created and she had no role in data collection after randomization, no access to data and did not oversee or conduct statistical analyses. There are no other conflicts to disclose.
References
- Harada, C.N.; Natelson Love, M.C.N.; Triebel, K.L. Normal Cognitive Aging. Clin. Geriatr. Med. 2013, 29, 737–752. [Google Scholar] [CrossRef]
- Dye, L.; Boyle, N.B.; Champ, C.; Lawton, C. The relationship between obesity and cognitive health and decline. Proc. Nutr. Soc. 2017, 76, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Gauthier S, Reisberg B, Zaudig M; et al. Mild cognitive impairment. Lancet 2006, 367(9518), 1262-70. [Google Scholar] [CrossRef]
- Moore, K.; Hughes, C.F.; Ward, M.; Hoey, L.; McNulty, H. Diet, nutrition and the ageing brain: current evidence and new directions. Proc. Nutr. Soc. 2018, 77, 152–163. [Google Scholar] [CrossRef]
- Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7(2), e105-e25.
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- Bischof GN, Park DC. Obesity and Aging: Consequences for Cognition, Brain Structure, and Brain Function. Psychosom Med. 2015, 77(6), 697–709. [Google Scholar] [CrossRef] [PubMed]
- Alosco, M.L.; Spitznagel, M.B.; Raz, N.; Cohen, R.; Sweet, L.H.; Colbert, L.H.; Josephson, R.; van Dulmen, M.; Hughes, J.; Rosneck, J.; et al. Obesity Interacts with Cerebral Hypoperfusion to Exacerbate Cognitive Impairment in Older Adults with Heart Failure. Cerebrovasc. Dis. Extra 2012, 2, 88–98. [Google Scholar] [CrossRef] [PubMed]
- Willeumier, K.C.; Taylor, D.V.; Amen, D.G. Elevated BMI Is Associated With Decreased Blood Flow in the Prefrontal Cortex Using SPECT Imaging in Healthy Adults. Obesity 2011, 19, 1095–1097. [Google Scholar] [CrossRef]
- Selim, M.; Jones, R.; Novak, P.; Zhao, P.; Novak, V. The effects of body mass index on cerebral blood flow velocity. Clin. Auton. Res. 2008, 18, 331–338. [Google Scholar] [CrossRef]
- Anstey, K.J.; Cherbuin, N.; Budge, M.; Young, J. Body mass index in midlife and late-life as a risk factor for dementia: a meta-analysis of prospective studies. Obes. Rev. 2011, 12, e426–e437. [Google Scholar] [CrossRef]
- Wang, F.; Zhao, M.; Han, Z.; Li, D.; Zhang, S.; Zhang, Y.; Kong, X.; Sun, N.; Zhang, Q.; Lei, P. Association of body mass index with amnestic and non-amnestic mild cognitive impairment risk in elderly. BMC Psychiatry 2017, 17, 334–334. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.; Hay, P.; Campbell, L.; Trollor, J.N. A review of the association between obesity and cognitive function across the lifespan: implications for novel approaches to prevention and treatment. Obes. Rev. 2011, 12, 740–755. [Google Scholar] [CrossRef] [PubMed]
- Parletta, N.; Milte, C.M.; Meyer, B.J. Nutritional modulation of cognitive function and mental health. J. Nutr. Biochem. 2013, 24, 725–743. [Google Scholar] [CrossRef] [PubMed]
- Miquel S, Champ C, Day J; et al. Poor cognitive ageing: Vulnerabilities, mechanisms and the impact of nutritional interventions. Ageing Res Rev. 2018, 42, 40–55. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Barbagallo, M. Nutritional prevention of cognitive decline and dementia. Acta Biomed. 2018, 89, 276–290. [Google Scholar]
- Key, M.N.; Szabo-Reed, A.N. Impact of Diet and Exercise Interventions on Cognition and Brain Health in Older Adults: A Narrative Review. Nutrients 2023, 15, 2495. [Google Scholar] [CrossRef]
- Yamasaki, T. Preventive Strategies for Cognitive Decline and Dementia: Benefits of Aerobic Physical Activity, Especially Open-Skill Exercise. Brain Sci. 2023, 13, 521. [Google Scholar] [CrossRef]
- Kesse-Guyot E, Peneau S, Ferry M; et al. Thirteen-year prospective study between fish consumption, long-chain n-3 fatty acids intakes and cognitive function. The Journal of Nutrition, Health & Aging 2011, 15(2), 115-20. [Google Scholar]
- Daiello, L.A.; Gongvatana, A.; Dunsiger, S.; Cohen, R.A.; Ott, B.R.; Initiative, A.D.N. Association of fish oil supplement use with preservation of brain volume and cognitive function. Alzheimer's Dement. 2014, 11, 226–235. [Google Scholar] [CrossRef]
- Parrott, M.D.; Shatenstein, B.; Ferland, G.; Payette, H.; Morais, J.A.; Belleville, S.; Kergoat, M.-J.; Gaudreau, P.; Greenwood, C.E. Relationship between Diet Quality and Cognition Depends on Socioeconomic Position in Healthy Older Adults. J. Nutr. 2013, 143, 1767–1773. [Google Scholar] [CrossRef]
- Tangney, C.C.; Kwasny, M.J.; Li, H.; Wilson, R.S.; Evans, A.D.; Morris, M.C. Adherence to a Mediterranean-type dietary pattern and cognitive decline in a community population. Am. J. Clin. Nutr. 2011, 93, 601–607. [Google Scholar] [CrossRef]
- Masana, M.F.; Koyanagi, A.; Haro, J.M.; Tyrovolas, S. n-3 Fatty acids, Mediterranean diet and cognitive function in normal aging: A systematic review. Exp. Gerontol. 2017, 91, 39–50. [Google Scholar] [CrossRef]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND diet associated with reduced incidence of Alzheimer's disease. Alzheimer's Dement. 2015, 11, 1007–1014. [Google Scholar] [CrossRef] [PubMed]
- van den Brink AC, Brouwer-Brolsma EM, Berendsen AAM. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease-A Review. Adv Nutr. 2019, 10(6), 1040-65. [Google Scholar] [CrossRef] [PubMed]
- Nurk, E.; Refsum, H.; Bjelland, I.; Drevon, C.A.; Tell, G.S.; Ueland, P.M.; Vollset, S.E.; Engedal, K.; Nygaard, H.A.; Smith, D.A. Plasma free choline, betaine and cognitive performance: the Hordaland Health Study. Br. J. Nutr. 2012, 109, 511–519. [Google Scholar] [CrossRef] [PubMed]
- La Fata, G.; Weber, P.; Mohajeri, M.H. Effects of Vitamin E on Cognitive Performance during Ageing and in Alzheimer’s Disease. Nutrients 2014, 6, 5453–5472. [Google Scholar] [CrossRef]
- Zhang, X.-W.; Hou, W.-S.; Li, M.; Tang, Z.-Y. Omega-3 fatty acids and risk of cognitive decline in the elderly: a meta-analysis of randomized controlled trials. Aging Clin. Exp. Res. 2015, 28, 165–166. [Google Scholar] [CrossRef]
- Salem, N.; Vandal, M.; Calon, F. The benefit of docosahexaenoic acid for the adult brain in aging and dementia. Prostaglandins, Leukot. Essent. Fat. Acids 2014, 92, 15–22. [Google Scholar] [CrossRef]
- Moreira, A.; Diógenes, M.J.; de Mendonça, A.; Lunet, N.; Barros, H. Chocolate Consumption is Associated with a Lower Risk of Cognitive Decline. J. Alzheimer's Dis. 2016, 53, 85–93. [Google Scholar] [CrossRef]
- Alonso-Alonso M. Cocoa flavanols and cognition: regaining chocolate in old age? : Oxford University Press; 2015.
- Ellinger, S.; Stehle, P. Impact of Cocoa Consumption on Inflammation Processes—A Critical Review of Randomized Controlled Trials. Nutrients 2016, 8, 321. [Google Scholar] [CrossRef]
- Vauzour, D. Polyphenols and brain health. OCL 2017, 24, A202. [Google Scholar] [CrossRef]
- Sokolov, A.N.; Pavlova, M.A.; Klosterhalfen, S.; Enck, P. Chocolate and the brain: Neurobiological impact of cocoa flavanols on cognition and behavior. Neurosci. Biobehav. Rev. 2013, 37, 2445–2453. [Google Scholar] [CrossRef]
- Calder, P.C. Omega-3 Fatty Acids and Inflammatory Processes. Nutrients 2010, 2, 355–374. [Google Scholar] [CrossRef]
- Dyall, S.C. Long-chain omega-3 fatty acids and the brain: a review of the independent and shared effects of EPA, DPA and DHA. Front. Aging Neurosci. 2015, 7, 52–52. [Google Scholar] [CrossRef]
- Michael-Titus AT, Priestley JV. Omega-3 fatty acids and traumatic neurological injury: from neuroprotection to neuroplasticity? Trends Neurosci. 2014, 37(1), 30-8. [Google Scholar] [CrossRef] [PubMed]
- Tsukada, H.; Kakiuchi, T.; Fukumoto, D.; Nishiyama, S.; Koga, K. Docosahexaenoic acid (DHA) improves the age-related impairment of the coupling mechanism between neuronal activation and functional cerebral blood flow response: a PET study in conscious monkeys. Brain Res. 2000, 862, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Joris, P.J.; Mensink, R.P.; Adam, T.C.; Liu, T.T. Cerebral Blood Flow Measurements in Adults: A Review on the Effects of Dietary Factors and Exercise. Nutrients 2018, 10, 530. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, C.; Wirth, M.; Gerischer, L.; Grittner, U.; Witte, A.V.; Köbe, T.; Flöel, A. EFFECTS OF OMEGA-3 FATTY ACIDS ON RESTING CEREBRAL PERFUSION IN PATIENTS WITH MILD COGNITIVE IMPAIRMENT: A RANDOMIZED CONTROLLED TRIAL. J. Prev. Alzheimer's Dis. 2017, 5, 1–5. [Google Scholar] [CrossRef]
- Schliebs, R.; Arendt, T. The cholinergic system in aging and neuronal degeneration. Behav. Brain Res. 2011, 221, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Crichton, G.E.; Elias, M.F.; Alkerwi, A. Chocolate intake is associated with better cognitive function: The Maine-Syracuse Longitudinal Study. Appetite 2016, 100, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Teo, L.; Crawford, C.; Snow, J.; Deuster, P.A.; Bingham, J.J.; Gallon, M.D.; O’connell, M.L.; Chittum, H.K.; Arzola, S.M.; Berry, K. Phytochemicals to optimize cognitive function for military mission-readiness: a systematic review and recommendations for the field. Nutr. Rev. 2017, 75, 49–72. [Google Scholar] [CrossRef] [PubMed]
- van Dyck CH, Swanson CJ, Aisen P; et al. Lecanemab in Early Alzheimer’s Disease. N Engl J Med. 2023, 388(1), 9–21. [Google Scholar] [CrossRef] [PubMed]
- Pervin, M.; Unno, K.; Takagaki, A.; Isemura, M.; Nakamura, Y. Function of Green Tea Catechins in the Brain: Epigallocatechin Gallate and its Metabolites. Int. J. Mol. Sci. 2019, 20, 3630. [Google Scholar] [CrossRef] [PubMed]
- Afzal, O.; Dalhat, M.H.; Altamimi, A.S.A.; Rasool, R.; Alzarea, S.I.; Almalki, W.H.; Murtaza, B.N.; Iftikhar, S.; Nadeem, S.; Nadeem, M.S.; et al. Green Tea Catechins Attenuate Neurodegenerative Diseases and Cognitive Deficits. Molecules 2022, 27, 7604. [Google Scholar] [CrossRef] [PubMed]
- Unno, K.; Nakamura, Y. Green Tea Suppresses Brain Aging. Molecules 2021, 26, 4897. [Google Scholar] [CrossRef]
- Singh, N.A.; Mandal, A.K.A.; Khan, Z.A. Potential neuroprotective properties of epigallocatechin-3-gallate (EGCG). Nutr. J. 2015, 15, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Nehlig, A. The neuroprotective effects of cocoa flavanol and its influence on cognitive performance. Br. J. Clin. Pharmacol. 2013, 75, 716–727. [Google Scholar] [CrossRef]
- Socci, V.; Tempesta, D.; Desideri, G.; De Gennaro, L.; Ferrara, M. Enhancing Human Cognition with Cocoa Flavonoids. Front. Nutr. 2017, 4, 19. [Google Scholar] [CrossRef]
- Gratton G, Weaver SR, Burley CV; et al. Dietary flavanols improve cerebral cortical oxygenation and cognition in healthy adults. Sci Rep. 2020, 10(1), 19409. [Google Scholar] [CrossRef]
- Bapir, M.; Campagnolo, P.; Rodriguez-Mateos, A.; Skene, S.S.; Heiss, C. Assessing Variability in Vascular Response to Cocoa With Personal Devices: A Series of Double-Blind Randomized Crossover n-of-1 Trials. Front. Nutr. 2022, 9, 886597. [Google Scholar] [CrossRef] [PubMed]
- Mastroiacovo, D.; Kwik-Uribe, C.; Grassi, D.; Necozione, S.; Raffaele, A.; Pistacchio, L.; Righetti, R.; Bocale, R.; Lechiara, M.C.; Marini, C.; et al. Cocoa flavanol consumption improves cognitive function, blood pressure control, and metabolic profile in elderly subjects: the Cocoa, Cognition, and Aging (CoCoA) Study—a randomized controlled trial. Am. J. Clin. Nutr. 2015, 101, 538–548. [Google Scholar] [CrossRef] [PubMed]
- Francis, S.T.; Head, K.; Morris, P.G.; Macdonald, I.A. The Effect of Flavanol-rich Cocoa on the fMRI Response to a Cognitive Task in Healthy Young People. J. Cardiovasc. Pharmacol. 2006, 47, S215–S220. [Google Scholar] [CrossRef]
- Farzaneh; A Sorond, F. ; A Lipsitz, L.; Hollenberg, N.K.; Fisher, N.D. Cerebral blood flow response to flavanol-rich cocoa in healthy elderly humans. Neuropsychiatr. Dis. Treat. 2008, 4, 433–440. [Google Scholar] [CrossRef]
- Scholey, A.; Owen, L. Effects of chocolate on cognitive function and mood: a systematic review. Nutr. Rev. 2013, 71, 665–681. [Google Scholar] [CrossRef]
- Castelli V, Grassi D, Bocale R; et al. Diet and Brain Health: Which Role for Polyphenols? Curr Pharm Des. 2018, 24(2), 227-38. [Google Scholar] [CrossRef]
- Roberts, S.B.; E Silver, R.; Das, S.K.; A Fielding, R.; Gilhooly, C.H.; Jacques, P.F.; Kelly, J.M.; Mason, J.B.; McKeown, N.M.; A Reardon, M.; et al. Healthy Aging—Nutrition Matters: Start Early and Screen Often. Adv. Nutr. Int. Rev. J. 2021, 12, 1438–1448. [Google Scholar] [CrossRef]
- A McCrory, M.; Fuss, P.J.; E McCallum, J.; Yao, M.; Vinken, A.G.; Hays, N.P.; Roberts, S.B. Dietary variety within food groups: association with energy intake and body fatness in men and women. Am. J. Clin. Nutr. 1999, 69, 440–447. [Google Scholar] [CrossRef]
- Desideri G, Kwik-Uribe C, Grassi D; et al. Benefits in cognitive function, blood pressure, and insulin resistance through cocoa flavanol consumption in elderly subjects with mild cognitive impairment: the Cocoa, Cognition, and Aging (CoCoA) study. Hypertension 2012, 60(3), 794–801. [Google Scholar] [CrossRef]
- Lamport, D.J.; Pal, D.; Moutsiana, C.; Field, D.T.; Williams, C.M.; Spencer, J.P.E.; Butler, L.T. The effect of flavanol-rich cocoa on cerebral perfusion in healthy older adults during conscious resting state: a placebo controlled, crossover, acute trial. Psychopharmacol. 2015, 232, 3227–3234. [Google Scholar] [CrossRef]
- Karl, J.P.; Meydani, M.; Barnett, J.B.; Vanegas, S.M.; Goldin, B.; Kane, A.; Rasmussen, H.; Saltzman, E.; Vangay, P.; Knights, D.; et al. Substituting whole grains for refined grains in a 6-wk randomized trial favorably affects energy-balance metrics in healthy men and postmenopausal women. Am. J. Clin. Nutr. 2017, 105, 589–599. [Google Scholar] [CrossRef]
- Gilhooly, C.H.; Das, S.K.; Golden, J.K.; McCrory, M.A.; Rochon, J.; DeLany, J.P.; Freed, A.M.; Fuss, P.J.; Dallal, G.E.; Saltzman, E.; et al. Use of cereal fiber to facilitate adherence to a human caloric restriction program. Aging Clin. Exp. Res. 2008, 20, 513–520. [Google Scholar] [CrossRef]
- Howarth, N.C.; Saltzman, E.; Roberts, S.B. Dietary Fiber and Weight Regulation. Nutr. Rev. 2001, 59, 129–139. [Google Scholar] [CrossRef]
- Howe, P.R.C.; Evans, H.M.; Kuszewski, J.C.; Wong, R.H.X. Effects of Long Chain Omega-3 Polyunsaturated Fatty Acids on Brain Function in Mildly Hypertensive Older Adults. Nutrients 2018, 10, 1413. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.K.; Kriska, A.M.; Venditti, E.M.; Miller, R.G.; Brooks, M.M.; Burke, L.E.; Siminerio, L.M.; Solano, F.X.; Orchard, T.J. Translating the Diabetes Prevention Program: A Comprehensive Model for Prevention Training and Program Delivery. Am. J. Prev. Med. 2009, 37, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Taetzsch, A.; Gilhooly, C.H.; Bukhari, A.; Das, S.K.; Martin, E.; Hatch, A.M.; E Silver, R.; Montain, S.J.; Roberts, S.B. Development of a Videoconference-Adapted Version of the Community Diabetes Prevention Program, and Comparison of Weight Loss With In-Person Program Delivery. Mil. Med. 2019, 184, 647–652. [Google Scholar] [CrossRef]
- Control CfD, Prevention. National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention. 2011;201(1):1-12.
- Das, S.K.; Bukhari, A.S.; Taetzsch, A.G.; Ernst, A.K.; Rogers, G.T.; Gilhooly, C.H.; Hatch-McChesney, A.; Blanchard, C.M.; A Livingston, K.; E Silver, R.; et al. Randomized trial of a novel lifestyle intervention compared with the Diabetes Prevention Program for weight loss in adult dependents of military service members. Am. J. Clin. Nutr. 2021, 114, 1546–1559. [Google Scholar] [CrossRef]
- Heaton, R.K.; Akshoomoff, N.; Tulsky, D.; Mungas, D.; Weintraub, S.; Dikmen, S.; Beaumont, J.; Casaletto, K.B.; Conway, K.; Slotkin, J.; et al. Reliability and Validity of Composite Scores from the NIH Toolbox Cognition Battery in Adults. J. Int. Neuropsychol. Soc. 2014, 20, 588–598. [Google Scholar] [CrossRef]
- Benton AL, Abigail B, Sivan AB, Hamsher Kd, Varney NR, Spreen O. Contributions to neuropsychological assessment: A clinical manual: Oxford University Press, USA; 1994.
- Smith, A. Symbol digit modalities test: Western psychological services Los Angeles; 1973.
- Stroop, JR. Studies of interference in serial verbal reactions. Journal of Experimental Psychology 1935, 18(6), 643. [Google Scholar] [CrossRef]
- Reitan RM, Wolfson D. The Halstead-Reitan neuropsychological test battery: Theory and clinical interpretation: Reitan Neuropsychology; 1985.
- Reitan, R.M. VALIDITY OF THE TRAIL MAKING TEST AS AN INDICATOR OF ORGANIC BRAIN DAMAGE. Percept. Mot. Ski. 1958, 8. [Google Scholar] [CrossRef]
- Shapiro, D.M.; Harrison, D.W. Alternate forms of the AVLT: a procedure and test of form equivalency. . 1990, 5, 405–10. [Google Scholar]
- Cheung C, Culver JP, Takahashi K. In vivo cerebrovascular measurement combining diffuse near-infrared absorption and correlation spectroscopies. Phys Med Biol. 2001, 46(8), 2053-65. [Google Scholar]
- Sunwoo, J.; Zavriyev, A.I.; Kaya, K.; Martin, A.; Munster, C.; Steele, T.; Cuddyer, D.; Sheldon, Y.; Orihuela-Espina, F.; Herzberg, E.M.; et al. Diffuse correlation spectroscopy blood flow monitoring for intraventricular hemorrhage vulnerability in extremely low gestational age newborns. Sci. Rep. 2022, 12, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, R.C.; Durduran, T.; Yu, G.; Buckley, E.M.; Kim, M.N.; Zhou, C.; Choe, R.; Sunar, U.; Yodh, A.G.; C., M.R.; et al. Direct measurement of tissue blood flow and metabolism with diffuse optics. Philos. Trans. R. Soc. A: Math. Phys. Eng. Sci. 2011, 369, 4390–4406. [Google Scholar] [CrossRef] [PubMed]
- Durduran, T.; Yodh, A.G. Diffuse correlation spectroscopy for non-invasive, micro-vascular cerebral blood flow measurement. NeuroImage 2013, 85, 51–63. [Google Scholar] [CrossRef]
- Buckley, E.M.; Parthasarathy, A.B.; Grant, P.E.; Yodh, A.G.; Franceschini, M.A. Diffuse correlation spectroscopy for measurement of cerebral blood flow: future prospects. Neurophotonics 2014, 1, 011009–011009. [Google Scholar] [CrossRef]
- Green MS, Sehgal S, Tariq R. Near-Infrared Spectroscopy: The New Must Have Tool in the Intensive Care Unit? Semin Cardiothorac Vasc Anesth. 2016, 20(3), 213-24. [Google Scholar] [CrossRef] [PubMed]
- Hogue, C.W.; Levine, A.; Hudson, A.; Lewis, C. Clinical Applications of Near-infrared Spectroscopy Monitoring in Cardiovascular Surgery. Anesthesiology 2021, 134, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.-C.; Tamborini, D.; Renna, M.; Peruch, A.; Huang, Y.; Martin, A.; Kaya, K.; Starkweather, Z.; Zavriyev, A.I.; Carp, S.A.; et al. Open-source FlexNIRS: A low-cost, wireless and wearable cerebral health tracker. NeuroImage 2022, 256, 119216. [Google Scholar] [CrossRef] [PubMed]
- Das, S.K.; Gilhooly, C.H.; Golden, J.K.; Pittas, A.G.; Fuss, P.J.; A Cheatham, R.; Tyler, S.; Tsay, M.; A McCrory, M.; Lichtenstein, A.H.; et al. Long-term effects of 2 energy-restricted diets differing in glycemic load on dietary adherence, body composition, and metabolism in CALERIE: a 1-y randomized controlled trial. Am. J. Clin. Nutr. 2007, 85, 1023–1030. [Google Scholar] [CrossRef]
- Salinardi, T.C.; Batra, P.; Roberts, S.B.; E Urban, L.; Robinson, L.M.; Pittas, A.G.; Lichtenstein, A.H.; Deckersbach, T.; Saltzman, E.; Das, S.K. Lifestyle intervention reduces body weight and improves cardiometabolic risk factors in worksites. Am. J. Clin. Nutr. 2013, 97, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.C.; Matthews, D.R.; Hermans, M.P. Correct Homeostasis Model Assessment (HOMA) Evaluation Uses the Computer Program. Diabetes Care 1998, 21, 2191–2192. [Google Scholar] [CrossRef]
- Bangen, K.J.; Beiser, A.; Delano-Wood, L.; Nation, D.A.; Lamar, M.; Libon, D.J.; Bondi, M.W.; Seshadri, S.; Wolf, P.A.; Au, R. APOE Genotype Modifies the Relationship between Midlife Vascular Risk Factors and Later Cognitive Decline. J. Stroke Cerebrovasc. Dis. 2013, 22, 1361–1369. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Basak, J.M.; Holtzman, D.M. The Role of Apolipoprotein E in Alzheimer's Disease. Neuron 2009, 63, 287–303. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 health survey: manual and interpretation guide. Boston: The Health Institute, New England Medical Center; 1993.
- Buysse DJ, Reynolds CF, 3rd. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28(2), 193–213. [Google Scholar] [CrossRef]
- Beck AT, Steer RA, Brown GK. Beck Depression Inventory-II. San Antonio. 1996;78(2):490-8.
- Karlsson, J.; Persson, L.-O.; Sjöström, L.; Sullivan, M. Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int. J. Obes. 2000, 24, 1715–1725. [Google Scholar] [CrossRef]
- Pfeffer, R.I.; Kurosaki, T.T.; Harrah, C.H.; Chance, J.M.; Filos, S. Measurement of Functional Activities in Older Adults in the Community. J. Gerontol. 1982, 37, 323–329. [Google Scholar] [CrossRef]
- Keating, X.D.; Zhou, K.; Liu, X.; Hodges, M.; Liu, J.; Guan, J.; Phelps, A.; Castro-Piñero, J. Reliability and Concurrent Validity of Global Physical Activity Questionnaire (GPAQ): A Systematic Review. Int. J. Environ. Res. Public Heal. 2019, 16, 4128. [Google Scholar] [CrossRef]
- Lytle, L.A.; Nicastro, H.L.; Roberts, S.B.; Evans, M.; Jakicic, J.M.; Laposky, A.D.; Loria, C.M. Accumulating Data to Optimally Predict Obesity Treatment (ADOPT) Core Measures: Behavioral Domain. Obesity 2018, 26, S16–S24. [Google Scholar] [CrossRef]
- Bathalon, G.P.; Tucker, K.L.; Hays, N.P.; Vinken, A.G.; Greenberg, A.S.; A McCrory, M.; Roberts, S.B. Psychological measures of eating behavior and the accuracy of 3 common dietary assessment methods in healthy postmenopausal women. Am. J. Clin. Nutr. 2000, 71, 739–745. [Google Scholar] [CrossRef]
- Huang, T.T.; Roberts, S.B.; Howarth, N.C.; McCrory, M.A. Effect of Screening Out Implausible Energy Intake Reports on Relationships between Diet and BMI. Obes. Res. 2005, 13, 1205–1217. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Bogensberger, B.; Hoffmann, G. Diet Quality as Assessed by the Healthy Eating Index, Alternate Healthy Eating Index, Dietary Approaches to Stop Hypertension Score, and Health Outcomes: An Updated Systematic Review and Meta-Analysis of Cohort Studies. J. Acad. Nutr. Diet. 2018, 118, 74–100. [Google Scholar] [CrossRef] [PubMed]
- Napoli, N.; Shah, K.; Waters, D.L.; Sinacore, D.R.; Qualls, C.; Villareal, D.T. Effect of weight loss, exercise, or both on cognition and quality of life in obese older adults. Am. J. Clin. Nutr. 2014, 100, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Stillman, C.M.; Jakicic, J.; Rogers, R.; Alfini, A.J.; Smith, J.C.; Watt, J.; Kang, C.; Erickson, K.I. Changes in cerebral perfusion following a 12-month exercise and diet intervention. Psychophysiology 2020, 58, e13589. [Google Scholar] [CrossRef] [PubMed]
- Sorond, F.A.; Hurwitz, S.; Salat, D.H.; Greve, D.N.; Fisher, N.D. Neurovascular coupling, cerebral white matter integrity, and response to cocoa in older people. Neurology 2013, 81, 904–909. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: updated guidelines for reporting parallel group randomised trials. J. Clin. Epidemiology 2010, 63, e1–e37. [Google Scholar] [CrossRef] [PubMed]
- Herrman, H.; Kieling, C.; McGorry, P.; Horton, R.; Sargent, J.; Patel, V. Reducing the global burden of depression: a Lancet–World Psychiatric Association Commission. Lancet 2018, 393, e42–e43. [Google Scholar] [CrossRef]
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; O'Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2014, 385, 549–562. [Google Scholar] [CrossRef]
- Lutz, W.; Sanderson, W.; Scherbov, S. The coming acceleration of global population ageing. Nature 2008, 451, 716–719. [Google Scholar] [CrossRef]
- Kennedy, B.K.; Berger, S.L.; Brunet, A.; Campisi, J.; Cuervo, A.M.; Epel, E.S.; Franceschi, C.; Lithgow, G.J.; Morimoto, R.I.; Pessin, J.E.; et al. Geroscience: Linking Aging to Chronic Disease. Cell 2014, 159, 709–713. [Google Scholar] [CrossRef]
- Milte, C.M.; McNaughton, S. Dietary patterns and successful ageing: a systematic review. Eur. J. Nutr. 2015, 55, 423–450. [Google Scholar] [CrossRef]
- Crimmins, E.M. Lifespan and Healthspan: Past, Present, and Promise. Gerontol. 2015, 55, 901–911. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.B.; Franceschini, M.A.; Krauss, A.; Lin, P.-Y.; de Sa, A.B.; Có, R.; Taylor, S.; Brown, C.; Chen, O.; Johnson, E.J.; et al. A Pilot Randomized Controlled Trial of a New Supplementary Food Designed to Enhance Cognitive Performance during Prevention and Treatment of Malnutrition in Childhood. Curr. Dev. Nutr. 2017, 1, e000885. [Google Scholar] [CrossRef] [PubMed]
- Roberts SB, Franceschini MA, Taylor SF; et al. Effects of food supplementation on cognitive function, and cerebral blood flow and nutritional status, in young children at risk of undernutrition: a family-randomized controlled trial. BMJ 2020, 370, m2397. [Google Scholar] [CrossRef] [PubMed]
- Roust, L.R.; DiBaise, J.K. Nutrient deficiencies prior to bariatric surgery. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 138–144. [Google Scholar] [CrossRef]
- Caulfield LE, Richard SA, Rivera JA, Musgrove P, Black RE. Stunting, Wasting, and Micronutrient Deficiency Disorders. In: Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, et al., editors. Disease Control Priorities in Developing Countries. 2nd ed. Washington (DC) New York: The International Bank for Reconstruction and Development/The World Bank; 2006.
- Mattson, M.P.; Magnus, T. Ageing and neuronal vulnerability. Nat. Rev. Neurosci. 2006, 7, 278–294. [Google Scholar] [CrossRef] [PubMed]
- Gemma, C.; Vila, J.; Bachstetter, A.; Bickford, P.C. Oxidative stress and the aging brain: From theory to prevention. In Frontiers in Neuroscience. Brain Aging: Models, Methods, and Mechanisms; Riddle, D.R., Ed.; CRC Press; American Publishing Group: Boca Raton, FL, USA, 2007; pp. 353–374. [Google Scholar]
- Murray, K.N.; Girard, S.; Holmes, W.M.; Parkes, L.M.; Williams, S.R.; Parry-Jones, A.R.; Allan, S.M. Systemic Inflammation Impairs Tissue Reperfusion Through Endothelin-Dependent Mechanisms in Cerebral Ischemia. Stroke 2014, 45, 3412–3419. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Lin, H.; Lu, C.; Chen, P.; Huang, C.; Chou, K.; Su, M.; Friedman, M.; Chen, Y.; Lin, W. Systemic inflammation and alterations to cerebral blood flow in obstructive sleep apnea. J. Sleep Res. 2017, 26, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Ekdahl, C.T.; Claasen, J.-H.; Bonde, S.; Kokaia, Z.; Lindvall, O. Inflammation is detrimental for neurogenesis in adult brain. Proc. Natl. Acad. Sci. USA 2003, 100, 13632–13637. [Google Scholar] [CrossRef] [PubMed]
- John, C.C.; Black, M.M.; Nelson, C.A. Neurodevelopment: The Impact of Nutrition and Inflammation During Early to Middle Childhood in Low-Resource Settings. PEDIATRICS 2017, 139, S59–S71. [Google Scholar] [CrossRef]
- Fryar C, Carrol M, Afful J. Prevalence of overweight, obesity, and severe obesity among adults aged 20 and over: United States, 1960–1962 through 2017–2018. Centers for Disease Control and Prevention. 2020;NCHS Health E-Stats.
- Attwell, D.; Buchan, A.M.; Charpak, S.; Lauritzen, M.J.; MacVicar, B.A.; Newman, E.A. Glial and neuronal control of brain blood flow. Nature 2010, 468, 232–243. [Google Scholar] [CrossRef]
- Sabayan B, van der Grond J, Westendorp RG; et al. Total cerebral blood flow and mortality in old age: a 12-year follow-up study. Neurology 2013, 81(22), 1922-9. [Google Scholar] [CrossRef]
- Vestergaard, M.B.; Jensen, M.L.; Arngrim, N.; Lindberg, U.; Larsson, H.B. Higher physiological vulnerability to hypoxic exposure with advancing age in the human brain. J. Cereb. Blood Flow Metab. 2018, 40, 341–353. [Google Scholar] [CrossRef]
- Beason-Held, L.L.; Goh, J.O.; An, Y.; Kraut, M.A.; O'Brien, R.J.; Ferrucci, L.; Resnick, S.M. Changes in Brain Function Occur Years before the Onset of Cognitive Impairment. J. Neurosci. 2013, 33, 18008–18014. [Google Scholar] [CrossRef]
- Dorrance, A.M.; Matin, N.; Pires, P.W. The effects of obesity on the cerebral vasculature. Curr. Vasc. Pharmacol. 2014, 12, 462–72. [Google Scholar] [CrossRef] [PubMed]
- Yadav, S.K.; Kumar, R.; Macey, P.M.; Richardson, H.L.; Wang, D.J.; Woo, M.A.; Harper, R.M. Regional cerebral blood flow alterations in obstructive sleep apnea. Neurosci. Lett. 2013, 555, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.L.F.; Vestergaard, M.B.; Tønnesen, P.; Larsson, H.B.W.; Jennum, P.J. Cerebral blood flow, oxygen metabolism, and lactate during hypoxia in patients with obstructive sleep apnea. Sleep 2018, 41, zsy001. [Google Scholar] [CrossRef]
- Shen, Y.; Zhao, B.; Yan, L.; Jann, K.; Wang, G.; Wang, J.; Wang, B.; Pfeuffer, J.; Qian, T.; Wang, D.J.J. Cerebral Hemodynamic and White Matter Changes of Type 2 Diabetes Revealed by Multi-TI Arterial Spin Labeling and Double Inversion Recovery Sequence. Front. Neurol. 2017, 8, 717. [Google Scholar] [CrossRef] [PubMed]
- Cohen, RA. Hypertension and cerebral blood flow: implications for the development of vascular cognitive impairment in the elderly. Stroke 2007, 38(6), 1715-7. [Google Scholar] [CrossRef]
- Stopa, E.G.; Butala, P.; Salloway, S.; Johanson, C.E.; Gonzalez, L.; Tavares, R.; Hovanesian, V.; Hulette, C.M.; Vitek, M.P.; Cohen, R.A.; et al. Cerebral Cortical Arteriolar Angiopathy, Vascular Beta-Amyloid, Smooth Muscle Actin, Braak Stage, and APOE Genotype. Stroke 2008, 39, 814–821. [Google Scholar] [CrossRef]
- Salloway, S.; Gur, T.; Berzin, T.; Zipser, B.; Correia, S.; Hovanesian, V.; Fallon, J.; Kuo-Leblanc, V.; Glass, D.; Hulette, C.; et al. Effect of APOE genotype on microvascular basement membrane in Alzheimer's disease. J. Neurol. Sci. 2002, 203-204, 183–187. [Google Scholar] [CrossRef]
- Alsop, D.C.; Dai, W.; Grossman, M.; Detre, J.A. Arterial Spin Labeling Blood Flow MRI: Its Role in the Early Characterization of Alzheimer's Disease. J. Alzheimer's Dis. 2010, 20, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Bangen KJ, Clark AL, Edmonds EC; et al. Cerebral Blood Flow and Amyloid-beta Interact to Affect Memory Performance in Cognitively Normal Older Adults. Front Aging Neurosci. 2017, 9, 181. [Google Scholar] [CrossRef] [PubMed]
- Bangen, K.J.; Werhane, M.L.; Weigand, A.J.; Edmonds, E.C.; Delano-Wood, L.; Thomas, K.R.; Nation, D.A.; Evangelista, N.D.; Clark, A.L.; Liu, T.T.; et al. Reduced Regional Cerebral Blood Flow Relates to Poorer Cognition in Older Adults With Type 2 Diabetes. Front. Aging Neurosci. 2018, 10, 270. [Google Scholar] [CrossRef] [PubMed]
- Dolui, S.; Tisdall, D.; Vidorreta, M.; Jacobs, D.R.; Nasrallah, I.M.; Bryan, R.N.; Wolk, D.A.; Detre, J.A. Characterizing a perfusion-based periventricular small vessel region of interest. NeuroImage: Clin. 2019, 23, 101897. [Google Scholar] [CrossRef] [PubMed]
- Glodzik, L.; Rusinek, H.; Brys, M.; Tsui, W.H.; Switalski, R.; Mosconi, L.; Mistur, R.; Pirraglia, E.; de Santi, S.; Li, Y.; et al. Framingham Cardiovascular Risk Profile Correlates with Impaired Hippocampal and Cortical Vasoreactivity to Hypercapnia. J. Cereb. Blood Flow Metab. 2010, 31, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Perry, V. The influence of systemic inflammation on inflammation in the brain: implications for chronic neurodegenerative disease. Brain, Behav. Immun. 2004, 18, 407–413. [Google Scholar] [CrossRef]
- Elwood, E.; Lim, Z.; Naveed, H.; Galea, I. The effect of systemic inflammation on human brain barrier function. Brain, Behav. Immun. 2016, 62, 35–40. [Google Scholar] [CrossRef]
Figure 1.
SPIRIT schedule of enrollment, interventions, and assessments.*.
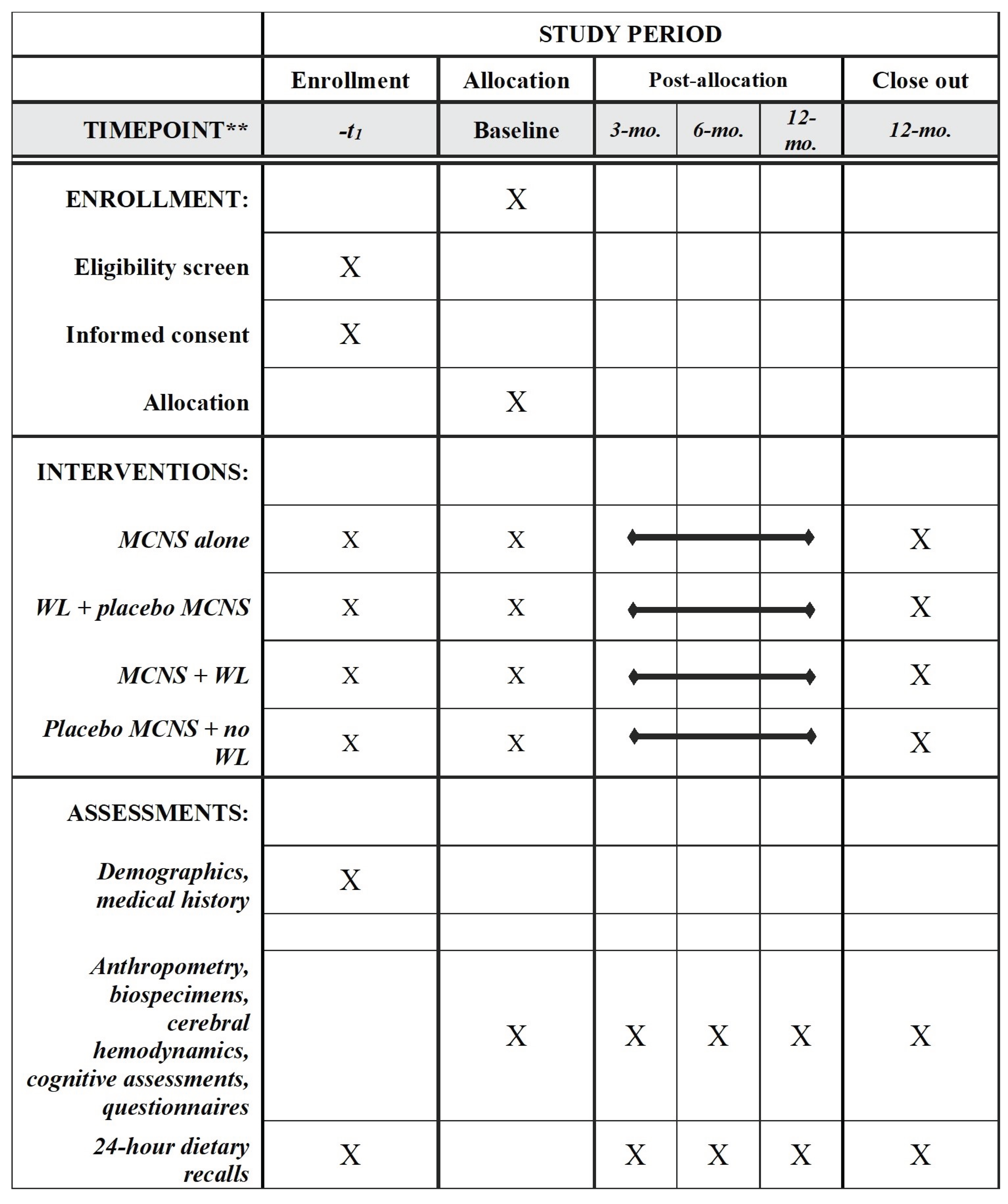
Figure 2.
Conceptual framework for nutritional synergy to promote brain health.
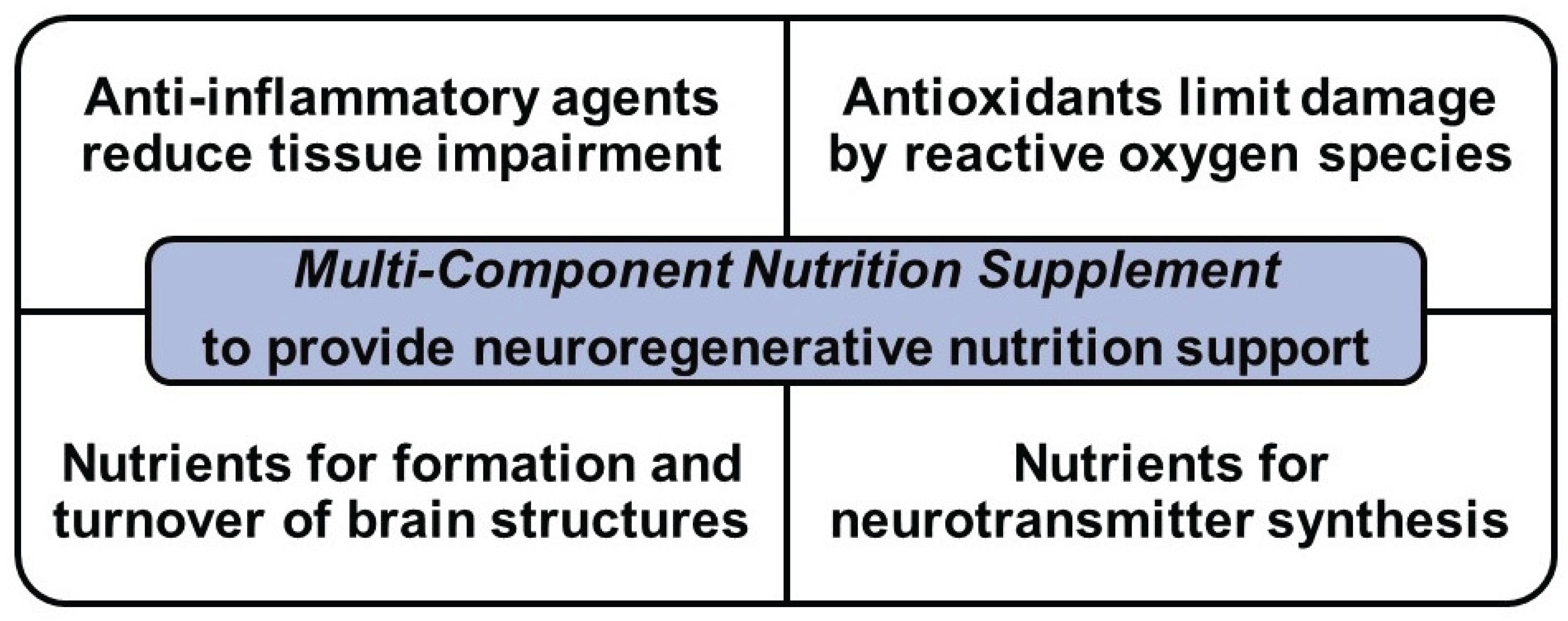
Figure 3.
Overview of the BB-Health Feasibility Trial.
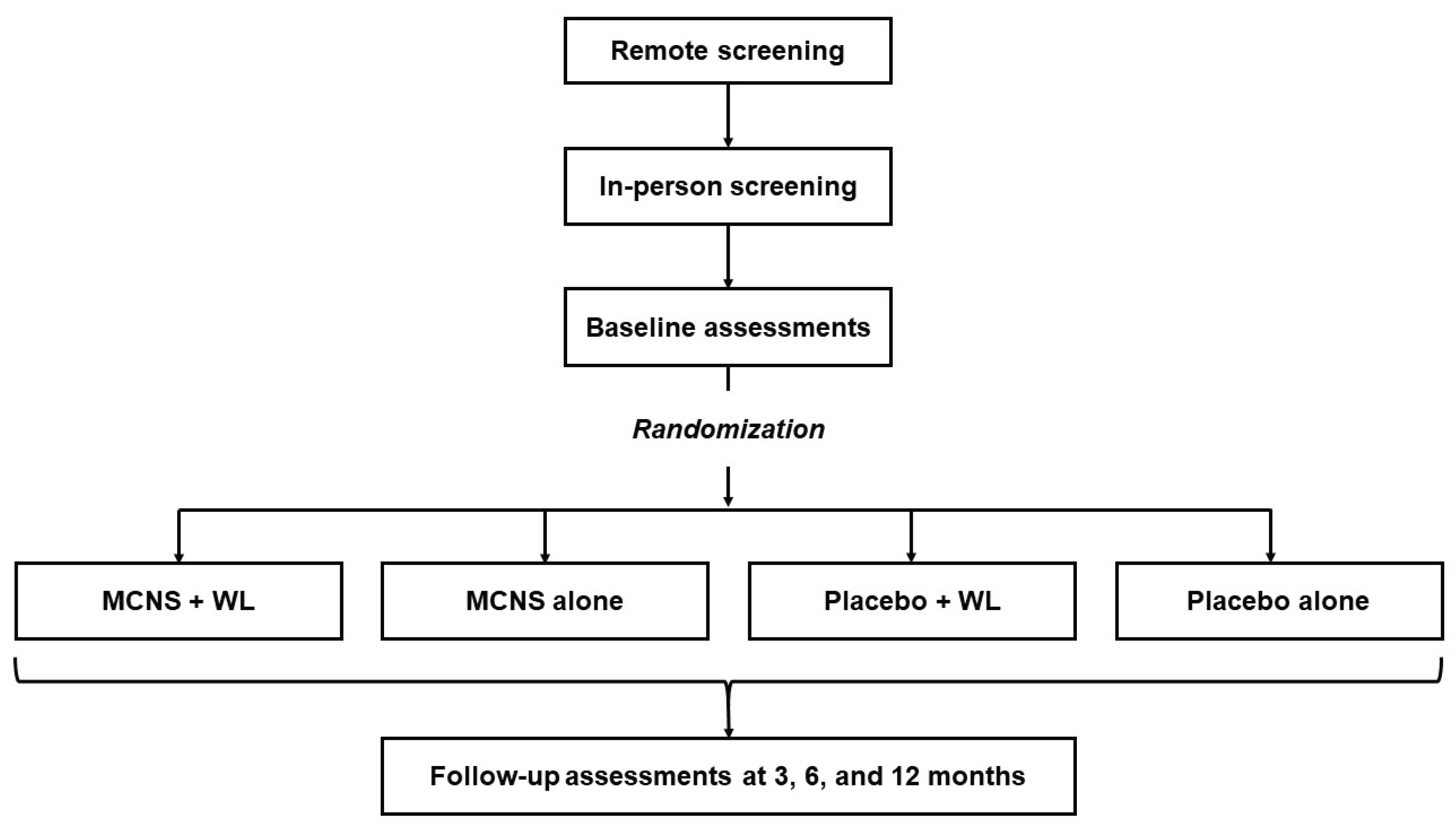
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



