
Submitted:
18 March 2024
Posted:
19 March 2024
You are already at the latest version
Abstract
Objectives: Recently, desert dust in Europe has been recognized as a cardiovascular health problem. In Spain, desert dust inflows in recent years have been associated with worsening air quality. The present study examines whether desert dust events are related to the incidence of acute coronary syndrome (ACS) in patients under 55 years of age.
Methods: Data from 2416 consecutive patients admitted to a tertiary hospital due to ACS were prospectively analyzed. A case-crossover time-stratified design using Poisson conditional regression models was applied to estimate the impact of desert dust events involving particulate matter concentrations of aerodynamic diameter < 10 μm (PM10) on the incidence of ACS.
Results: Desert dust intrusion on days 0 to 5 after ACS onset showed no significant association with the incidence of ACS in patients under 55 years of age. The incidence rate ratios of PM10 concentrations 1, 2, 3, 3, 4 and 5 days before ACS onset (for changes of 10 µg/m3) were 1.02 (95% CI 0.97-1.1; p = 0.41), 1.01 (95% CI 0.96-1.07; p = 0.66), 0.99 (95% CI 0.94-1.05; p = 0.78), 0.96 (95% CI 0.9-1.02; p = 0.18) and 0.97 (95% CI 0.91-1.04; p = 0.41).
Conclusions: Our findings suggest that desert dust is unlikely to be related to the incidence of premature coronary heart disease.
Keywords:
Desert dust
; acute coronary syndrome
; premature coronary heart disease
; air pollution
Introduction
The inhalation of combustion-related atmospheric pollutants has become a worldwide threat to human health. According to the World Health Organization (WHO), particulate material (PM) with an aerodynamic diameter of < 10 μm (PM10) and < 2.5 μm (PM2,5) has a very negative health impact [1]. The health consequences of the inhalation of desert dust particles carried by the wind in environmental air as a consequence of desert dust storms are becoming of growing interest throughout the world [1].
Northern Africa is the main world source of desert dust, representing 50-70% of the global emissions. The dust from northern Africa is regularly transported over the north Atlantic and also episodically over the Mediterranean and Europe [2]. Exposure to Saharan dust causes airway inflammation [3] and is associated with a 2% rise in cardiovascular mortality for every 10 µg/m3 increase in the concentration of PM10 [4].
Coronary disease (CD) is a chronic disorder that generally manifests after the sixth decade of life [5]. However, the reported worldwide prevalence of CD in young individuals (< 55 years of age) is 1-16%, with acute coronary syndrome (ACS) being the most frequent clinical presentation [6]. The manifestation of ACS in young subjects is associated with an important decrease in life expectancy [5]. To our knowledge, no previous studies have related desert dust exposure to premature CD.
The present case-crossover, time-stratified study was carried out to explore the association between desert dust exposure and the incidence of ACS in patients under 55 years of age.
Methods
Study Population
The study was carried out in Tenerife (Canary Islands, Spain). The climate is characterized by trade winds (March to August) that contribute to rapidly disperse the local atmospheric pollutants and help to preserve quite good air quality. Although desert dust episodes may occur over the course of the year, there are two dust seasons separated by the climate conditions: a) November to March and b) July to August [2].
The study was carried out in a tertiary hospital, and included all patients diagnosed with ACS between December 2012 and December 2017. These time intervals were chosen because all the required atmospheric data were available, collected on a retrospective basis. We defined premature coronary disease as CD diagnosed before 55 years of age [6]. A number of clinical variables were prospectively recorded: coronary risk factors, age and gender, previous vascular disease, presence of asthma or chronic obstructive pulmonary disease, chronic kidney disease, atrial fibrillation, the number of affected vessels (as determined by coronary angiography), left ventricular ejection fraction, Killip class, troponin I concentration, coronary interventions (percutaneous transluminal coronary angioplasty or coronary revascularization surgery), duration of hospital stay, in-hospital mortality and mortality at one year. The study was approved by the Clinical Research Ethics Committee of a tertiary hospital.
Air Quality and Meteorological Variables
Each day we prospectively recorded the climatic data, with the concentrations of PM10, PM2.5-10 PM2.5 and gaseous pollutants (sulfur dioxide, nitrogen dioxide and tropospheric ozone) between December 2012 and December 2017. These data were obtained from the Air Quality Network of the Canary Islands, which forms part of the European Air Quality Network and monitors the presence of particulate (PM10 and PM2.5) and gaseous pollutants, based on the mandatory reference methods and procedures established by the European Union (Directive 2008/50/EC). With an hourly resolution, the network produces the data that are transmitted to the European Environment Agency. The mean daily values were determined and analyzed. The occurrence of desert dust episodes was detected with the validated predictions of the Sand and Dust Storm – Warning Advisory and Assessment System (WMO SDS-WAS) of the World Meteorological Organization, with the Spanish State Meteorological Agency and Barcelona Supercomputing Center acting as regional reference centers for northern Africa, the Middle East and Europe. The WMO SDS-WAS dust prediction system consists of a meteorological prediction model that also includes a module for dust simulation (cycle of emissions, transport and deposit) [7].
Statistical Analysis
Quantitative and categorical variables were reported as the mean ± standard deviation (SD) and number (%), respectively. Comparisons of the PM levels according to the number of ACS a day were made using analysis of variance (ANOVA).
Use was made of time series regression analyses, as these are commonly employed to study associations between pooled exposures and health outcomes. The result is a count (generally the number of events a day), and the main unit of analysis is the day, not the individual person. Since the individual confounding factors (e.g., age, gender, diabetes) do not vary significantly from one day to another, these factors have no impact upon the effect estimates of the environmental variables. To control for seasonality and long-term trends, we used a case-crossover time-stratified design, with the strata being the day of the week within the same month [8,9]. In other words, the number of events in a day of the week, such as for example Tuesday, were compared with the number of events in the rest of Tuesdays of that same month. In this way we controlled for the patient baseline characteristics and changes occurring over time, such as the seasons, demographic changes, day of the week, or any time trend.
Conditional logistic regression is used in many studies that analyze the impact of environmental variables upon clinical events. However, due to the influence of non-measured causes, the counts of observed events usually show variations wider than those predicted by a Poisson distribution [8,9]. When a logistic regression model is used, such overdispersion cannot be controlled, because the results are binary and thus overdispersion, although present, is not apparent. However, the model implicitly assumes that there is no excessive dispersion of the counts [9]. Furthermore, conditional logistic regression assumes that the observations are independent. However, observations that lie close in time are probably more similar than those that are distant in time [10], and autocorrelation will very probably be present. The logistic regression model cannot be adjusted for overdispersion and autocorrelation - both being frequent causes of underestimated uncertainty and type 1 error.
To overcome these methodological limitations, and based on the method of Armstrong et al. [9], we used a conditional Poisson regression model capable of controlling for overdispersion and autocorrelation. The dependent variable was the number of ACS diagnosed a day. For this analysis we had to modify the data matrix (Figure S1 of the Supplementary Material).
The incidence rate ratio (IRR) was calculated with its 95% confidence interval (CI). In order to determine the influence of PM10, adjustment was made for the following pollutants and environmental variables: PM2.5-10, PM2.5, sulfur dioxide, nitrogen dioxide, tropospheric ozone, temperature and humidity. The maximum model was constructed with PM10, the aforementioned pollutants, environmental variables and two-way interactions between PM10 and the rest of the variables. These interactions were evaluated and eliminated if no statistical significance was observed. We also took into account the possibility that the impact of PM could be produced some days before the occurrence of ACS. Therefore, we studied the possible effect from the day before to 5 days before the occurrence of ACS.
We also adjusted these lag effects for each other effect (e.g., the effect referred to PM10 of one lag day controlling for the effect of 2 lag days), developing a stratified distribution model [9]. However, in this latter model it is probable that the effects in the different lag days are closely correlated. In order to reduce collinearity of the lag days, we placed some restrictions on the model; we postulated that the influence of PM10 for lag days 0, 1 and 2, and also for days 3, 4 and 5, is the same, in line with the recommendations of Armstrong et al. [9]. Lastly, the diagnoses of the model were assessed. Statistical significance was considered for p < 0.05. All the statistical analyses were carried out using the STATA version 16 package (StataCorp, USA).
Results
Study Population
A total of 2416 patients were diagnosed with ACS during the study inclusion period. There were 649 women (26.9%), and the mean age was 63.9 ± 12.5 years. The in-hospital mortality rate was 5.3% (n = 129). A total of 1730 patients were over 55 years of age and 686 were under 55 years of age. The characteristics of the patients under and over 55 years of age are shown in Table 1.
Patients with ACS under 55 years of age
During the 1824 days of the study, there was one admission due to ACS in a patient under 55 years of age on 481 days, two admissions due to ACS on 83 days, and three admissions due to ACS on 13 days. Table 2 reports the PM10 concentrations according to the number of admissions. The impact of PM10 in the air upon the risk of suffering ACS on the same day was (per 10 μg/m3) IRR = 1.1 (95% CI 0.8-1.52; p = 0.55). Table 3 shows the impact of PM, gaseous pollutants, temperature and humidity according to the Poisson regression model.
No significant impact of PM10 was observed for any of the studied days prior to the onset of ACS. Specifically, on the day before the syndrome, IRR = 1.02 (95% CI 0.97-1.1; p = 0.41); two days before, IRR = 1.01 (95% CI 0.96-1.07; p = 0.66); three days before, IRR = 0.99 (95% CI 0.94-1.05; p = 0.78); four days before, IRR = 0.96 (95% CI 0.9-1.02; p = 0.18); and five days before, IRR = 0.97 (95% CI 0.91-1.04; p = 0.41). Figure 1 shows the IRR values with the corresponding confidence intervals.
No association was found in the model with restrictions assuming that the effect on day 0 and days 1 and 2 before ACS presented the same IRR = 1.02 (95% CI 0.98-1.1; p = 0.38); the same applied to days 3, 4 and 5 before, with IRR = 0.99 (95% CI 0.96-1.02; p = 0.51). Figure 2 shows the IRR values with the corresponding confidence intervals.
Patients with ACS over 55 Years of Age
During the 1824 days of the study, there was one admission due to ACS in a patient over 55 years of age on 646 days, two admissions on 321 days, three admissions on 98 days, four admissions on 32 days, and five admissions on four days. Table 4 reports the PM10 concentrations according to the number of admissions. The impact of PM10 in the air upon the risk of suffering ACS on the same day was (per 10 μg/m3) IRR = 1.02 (95% CI 0.9-1.15; p = 0.74).
No significant impact of PM10 was observed for any of the studied days prior to the onset of ACS. Specifically, on the day before the syndrome, IRR=1.2 (95% CI 0.82-1.64; p = 0.38); two days before, IRR = 0.99 (95% CI 0.85-1.16; p = 0.91); three days before, IRR = 0.87 (95% CI 0.75-1.01; p = 0.055); four days before, IRR = 1.05 (95% CI 0.91-1.2; p = 0.49); and five days before, IRR = 0.89 (95% CI 0.78-1.02; p = 0.09). Figure 1 shows the IRR values with the corresponding confidence intervals (CI).
No association was found in the model with restrictions assuming that the effect on day 0 and days 1 and 2 before ACS presented the same IRR = 1 (95% CI 0.98-1.02; p = 0.69); the same applied to days 3, 4 and 5 before, with IRR=1 (95% CI 0.98-1.02). Figure 2 shows the IRR values with the corresponding confidence intervals.
Discussion
The present study analyzed the possibility that desert dust produced by natural phenomena can trigger premature CD. The results obtained indicate that exposure to Saharan dust is not a potential triggering cause of premature CD.
Climate change and the global air quality crisis are having an impact on numerous aspects of society [1]. The concentrations of pollutants that affect air quality can vary notoriously in a matter of a few days, depending on the daily emissions and particularly on the meteorological conditions. Due to variations in wind speed, the vertical stability of the atmosphere, or the arrival of polluted air from other regions, the concentrations of these pollutants may vary between 50-500% in just a few days [11].
The proximity of the Canary Islands to the African continent defines the islands as an area of great interest, taking into account the frequency of intrusions of desert dust mineral components and their impact upon the population. It is therefore very important to characterize the intrusions of desert dust that affect the archipelago [2]. Sand storms are common in desert regions and lift an amalgam of fine polluting particles into the air. These particles, if inhaled, can have a negative impact upon cardiovascular health. These particles transported with the wind may contain chemical compounds and heavy metals that trigger a series of inflammatory responses on penetrating into the body [3,12].
Studies on the influence of desert dust upon CD are few, and the results are moreover discordant. Three recent studies have examined the relationship between dust storms and ACS [13,14,15]. Kojima et al. [13] studied the effect of desert dust upon the incidence of myocardial infarction, and concluded that desert dust episodes the day before lead to the appearance of CD (odds ratio [OR]=1.46; 95% CI 1.09-1.95). Vodonos et al. [14] reported an increased incidence of ACS related to PM10 (with one lag day) during the days of dust storm (OR = 1.007; 95% CI 1.002-1.012), though no significant impact was observed on the days without this atmospheric phenomenon (OR = 1.011; 95% CI 0.998-1.025). A recent study in Spain found no association between PM10 concentrations derived from desert dust and the incidence of CD [15]. It therefore may be inferred that cardiovascular pathophysiology may differ in terms of the impact of PM10 generated by combustion processes and those of natural origin (desert dust), suggesting likely variations in their influence [1,11,16,17].
Due to the use of ambiguous language in reference to desert dust episodes, the uncertainty regarding the composition of the particles during such episodes, and the presence of undocumented or uncontrolled factors, the epidemiological relationships between desert dust and CD generate significant controversy, with a lack of firm conclusions [15]. The present study evaluated desert dust events according to the PM10 concentrations, applying a control to mitigate possible confounding factors (particularly other particles in suspension and pollutants), and a novel and appropriate statistical method was used to avoid underestimating type 1 errors [8,9,10].
Limitations
Our study has certain limitations. Firstly, the measurements were made at static points to assess the atmospheric pollutant concentrations in the exterior, despite the fact that people spend most of their time indoors. Secondly, the challenge of correctly measuring exposure is a basic limitation in studies comprising time series, since the average taken from static monitoring stations does not precisely represent the mean exposure experienced by the population. This could result in downward bias in the estimations of time series analyses, as suggested by some data [18]. Lastly, the inconsistencies in the existing evidence suggest that more in-depth studies are needed of the characteristics associated with the short-term effects of desert dust, with special attention to its composition and biological properties [19].
Conclusions
This pioneering study analyzes the possible links between desert dust episodes and premature CD. The findings suggest that desert dust is unlikely to be related to the incidence of premature CD.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Conflicts of Interests
None.
Source of Funding
The present study was partially funded by the Instituto de Salud Carlos III (PI21/00404 – A.D.R.) and the Sociedad Española de Cardiología / Fundación Española del Corazón (SEC/FEC-INV-CLI 22/25 – A.D.R).
Acknowledgements
The authors thank the Sand and Dust Storm – Warning Advisory and Assessment System of the World Meteorological Organization, co-managed by the Spanish State Meteorological Agency and the Barcelona Supercomputing Center, for the dust modeling procedure, and the Environmental Authorities of the Government of the Canary Islands, for the air quality data.
Author Contributions
Conception, methodology, research, resources, drafting of the article, review and editing: A. Domínguez-Rodríguez. Data collection, critical review and final approval: N. Báez-Ferrer. Conceptualization, validation, critical review and final approval: P. Avanzas. Data collection, critical review and final approval: E. Trujillo-Martin, G. Burillo-Putze and S. Rodríguez. Formal analysis, resources, critical review and final approval: P. Abreu-González. Drafting of the initial proposal, methodology, data interpretation, critical review and final approval: D. Hernández-Vaquero.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The study was approved by the Institutional Review Board of the Hospital Universitario de Canarias (CHUC_2021_130, approval date 24 February 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability
The data presented in this study are available on request from the corresponding author.
References
- Benito Lozano, M.; Rodríguez, S. La imperiosa necesidad de programar la asistencia a urgencias, atendiendo al cambio climático y las crisis de calidad del aire. Rev Esp Urg Emerg. 2023, 2, 194–1977. [Google Scholar]
- Rodríguez, S.; Cuevas, E.; Prospero, J.M.; et al. Modulation of Saharan dust export by the North African dipole Atmos. Chem. Phys. 2015, 15, 7471–7486. [Google Scholar]
- Dominguez-Rodriguez, A.; Rodríguez, S.; Baez-Ferrer, N.; Abreu-Gonzalez, P.; Abreu-Gonzalez, J.; Avanzas, P.; Carnero, M.; Moris, C.; López-Darias, J.; Hernández-Vaquero, D. Impact of Saharan dust exposure on airway inflammation in patients with ischemic heart disease. Transl. Res. 2020, 224, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Rodríguez, A.; Báez-Ferrer, N.; Abreu-González, P.; Rodríguez, S.; Díaz, R.; Avanzas, P.; Hernández-Vaquero, D. Impact of Desert Dust Events on the Cardiovascular Disease: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 727. [Google Scholar] [CrossRef] [PubMed]
- Pascual, I.; Avanzas, P.; Almendárez, M.; et al. STEMI, primary percutaneous coronary intervention and recovering of life expectancy: insights from the SurviSTEMI study. Rev Esp Cardiol (Engl Ed). 2021, 74, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.L.; Seigerman, M.; Adusumalli, S.; Giri, J.; Fiorilli, P.N.; Kolansky, D.M.; Kobayashi, T. Evolution and Outcomes of Premature Coronary Artery Disease. Curr. Cardiol. Rep. 2021, 23, 36. [Google Scholar] [CrossRef] [PubMed]
- Pérez, C.; Haustein, K.; Janjic, Z.; et al. Atmospheric dust modeling from meso to global scales with the online NMMB/BSC-Dust model – Part 1: Model description, annual simulations and evaluation, Atmos. Chem. Phys. 2011, 11, 13001–13027. [Google Scholar] [CrossRef]
- Lu, Y.; Zeger, S.L. On the equivalence of case-crossover and time series methods in environmental epidemiology. Biostatistics 2006, 8, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.G.; Gasparrini, A.; Tobias, A. Conditional Poisson models: a flexible alternative to conditional logistic case cross-over analysis. BMC Med Res. Methodol. 2014, 14, 122. [Google Scholar] [CrossRef] [PubMed]
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time series regression studies in environmental epidemiology. Leuk. Res. 2013, 42, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Bañeras, J.; Iglesies-Grau, J.; Téllez-Plaza, M.; Arrarte, V.; Báez-Ferrer, N.; Benito, B.; Ruiz, R.C.; Cecconi, A.; Domínguez-Rodríguez, A.; Rodríguez-Sinovas, A.; et al. Environment and cardiovascular health: causes, consequences and opportunities in prevention and treatment. 2022, 75, 1050–1058. [CrossRef]
- Münzel, T.; Hahad, O.; Sørensen, M.; Lelieveld, J.; Duerr, G.D.; Nieuwenhuijsen, M.; Daiber, A. Environmental risk factors and cardiovascular diseases: a comprehensive expert review. Cardiovasc. Res. 2022, 118, 2880–2902. [Google Scholar] [CrossRef] [PubMed]
- Kojima, S.; Michikawa, T.; Ueda, K.; Sakamoto, T.; Matsui, K.; Kojima, T.; Tsujita, K.; Ogawa, H.; Nitta, H.; Takami, A. Asian dust exposure triggers acute myocardial infarction. Eur. Hear. J. 2017, 38, 3202–3208. [Google Scholar] [CrossRef] [PubMed]
- Vodonos, A.; Friger, M.; Katra, I.; Krasnov, H.; Zahger, D.; Schwartz, J.; Novack, V. Individual Effect Modifiers of Dust Exposure Effect on Cardiovascular Morbidity. PLOS ONE 2015, 10, e0137714. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Rodríguez, A.; Rodríguez, S.; Baez-Ferrer, N.; et al. Impact of Saharan dust on the incidence of acute coronary syndrome. Rev Esp Cardiol (Engl Ed). 2021, 74, 321–328. [Google Scholar] [CrossRef] [PubMed]
- de Longueville, F.; Ozer, P.; Doumbia, S.; Henry, S. Desert dust impacts on human health: an alarming worldwide reality and a need for studies in West Africa. Int. J. Biometeorol. 2013, 57, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Bañeras, J.; Ferreira-González, I.; Marsal, J.R.; Barrabés, J.A.; Ribera, A.; Lidón, R.M.; Domingo, E.; Martí, G.; García-Dorado, D. Short-term exposure to air pollutants increases the risk of ST elevation myocardial infarction and of infarct-related ventricular arrhythmias and mortality. Int. J. Cardiol. 2018, 250, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Zeger, S.L.; Thomas, D.; Dominici, F.; Samet, J.M.; Schwartz, J.; Dockery, D.; Cohen, A. Exposure Measurement Error in Time-Series Studies of Air Pollution: Concepts and Consequences. Environ. Heal. Perspect. 2000, 108, 419. [Google Scholar] [CrossRef] [PubMed]
- Domínguez-Rodríguez, A.; Avanzas, P.; Báez-Ferrer, N.; Abreu-González, P.; Rodríguez, S.; Matos-Castro, S.; Hernández-Vaquero, D. Rationale and Design of the Impact of Air Pollution Due to DESERT Dust in Patients with HEART Failure (DESERT HEART). J. Clin. Med. 2023, 12, 4990. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Impact of the PM10 concentrations in air upon the incidence of ACS in patients under and over 55 years of age. The influence of these concentrations in the previous 5 days are reported. IRR: incidence rate ratio.
Figure 1.
Impact of the PM10 concentrations in air upon the incidence of ACS in patients under and over 55 years of age. The influence of these concentrations in the previous 5 days are reported. IRR: incidence rate ratio.
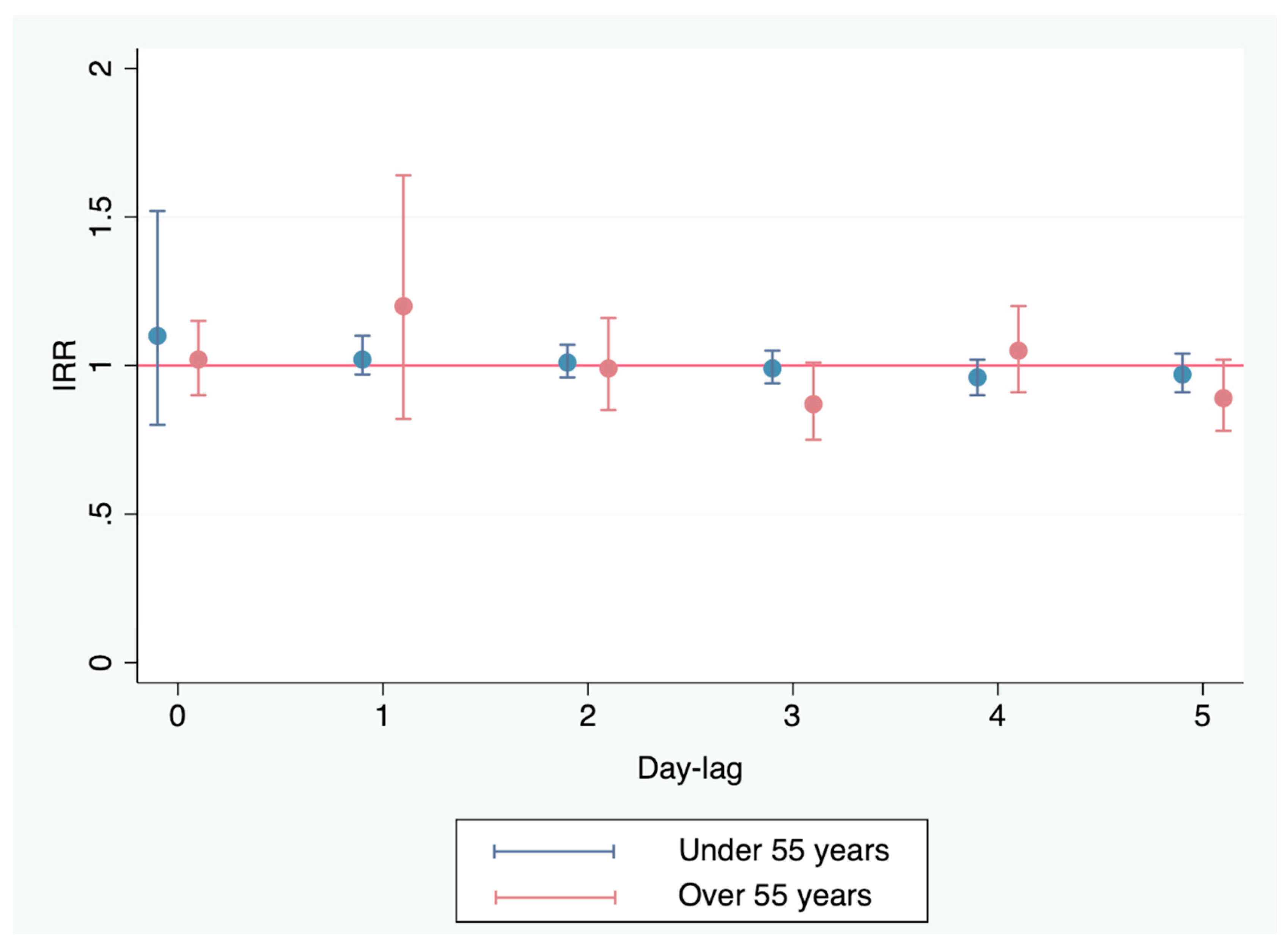
Figure 2.
Impact of the PM10 concentrations in air upon the incidence of ACS in patients under and over 55 years of age, controlled for different lag effects with restrictions (to avoid collinearity), assuming that the influence is the same for the previous 0, 1 and 2 days and for the previous 3, 4 and 5 days. IRR: incidence rate ratio.
Figure 2.
Impact of the PM10 concentrations in air upon the incidence of ACS in patients under and over 55 years of age, controlled for different lag effects with restrictions (to avoid collinearity), assuming that the influence is the same for the previous 0, 1 and 2 days and for the previous 3, 4 and 5 days. IRR: incidence rate ratio.
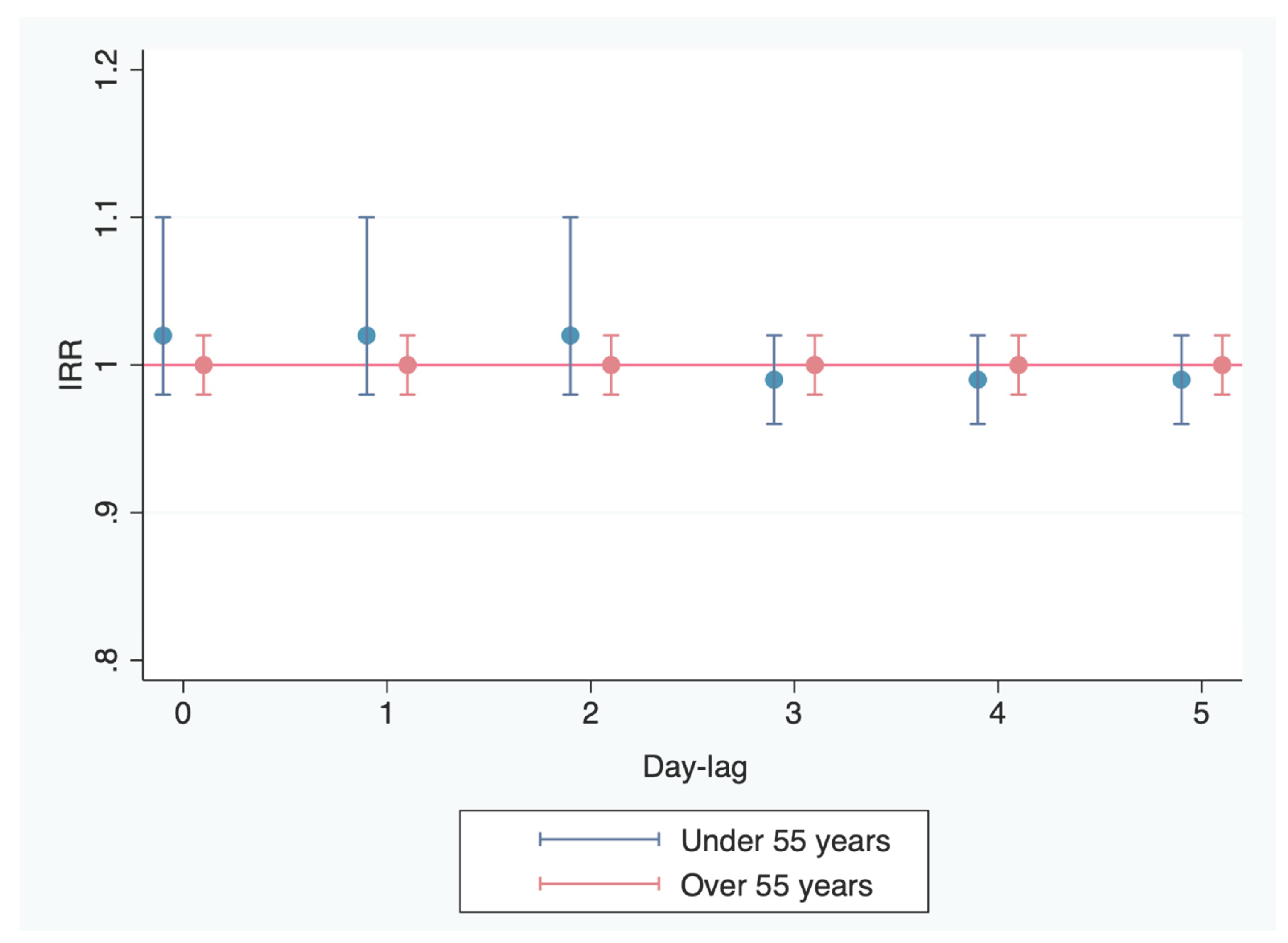

Table 1.
Clinical and hemodynamic characteristics of the study population.
| Variable |
Under 55 years N = 686 |
Over 55 years N = 1730 |
P-value |
|---|---|---|---|
| Age (years) | 48.9 ± 5 | 69.9 ± 9 | < 0.001 |
| Women | 131 (19.1%) | 518 (29.9%) | < 0.001 |
| Arterial hypertension | 285 (41.6%) | 1257 (72.7%) | < 0.001 |
| Dyslipidemia | 333 (48.6%) | 1067 (61.7%) | < 0.001 |
| Diabetes | 129 (18.8%) | 754 (43.6%) | < 0.001 |
| Asthma | 24 (3.5%) | 58 (3.4%) | 0.9 |
| Chronic obstructive pulmonary disease | 10 (1.5%) | 122 (7.1%) | < 0.001 |
| Chronic kidney disease | 12 (1.8%) | 243 (14.1%) | < 0.001 |
| Previously known coronary disease | 108 (15.8%) | 566 (32.7%) | < 0.001 |
| Supraventricular arrhythmia | 3 (0.4%) | 146 (8.4%) | < 0.001 |
| Acute myocardial infarction | 438 (63.9%) | 912 (52.8%) | < 0.001 |
| Left ventricular dysfunction | 124 (18.1%) | 439 (25.4%) | < 0.001 |
| Killip class I II III IV |
648 (94.5%) 12 (1.8%) 2 (0.3%) 24 (3.5%) |
1423 (82.3%) 146 (8.5%) 46 (2.7%) 113 (6.5%) |
< 0.001 |
| Coronary artery lesions No lesions Single-vessel disease Two-vessel disease Three-vessel disease |
43 (6.4%) 409 (60.5%) 158 (23.4%) 66 (9.8%) |
135 (8.4%) 639 (39.7%) 442 (27.5%) 394 (24.5%) |
< 0.001 |
| Troponin I peak (ng/ml) | 26.6 ± 29.7 | 21.2 ± 27.7 | < 0.001 |
| Percutaneous transluminal coronary angioplasty treatment | 552 (80.5%) | 1090 (63.1%) | < 0.001 |
| Surgical treatment | 33 (4.8%) | 137 (7.9%) | 0.01 |
| In-hospital mortality | 9 (1.3%) | 120 (6.9%) | < 0.001 |
| One-year mortality among the survivors | 3 (0.4%) | 15 (0.9%) | 0.43 |
Table 2.
PM10 concentrations (µg/m3) according to the number of ACS a day in patients under 55 years of age.
Table 2.
PM10 concentrations (µg/m3) according to the number of ACS a day in patients under 55 years of age.
| Day | No ACS/day N = 1246 |
1 ACS/day N = 481 |
2 ACS/day N = 83 |
3 ACS/day N = 13 |
P-value |
|---|---|---|---|---|---|
| Day of admission PM10 (μg/m3) |
21.5 ± 23.4 | 21.5 ± 22.2 | 20.6 ± 18.7 | 14.3 ± 7.8 | 0.71 |
| 1 Day before PM10 (μg/m3) |
21.3 ± 21.2 | 21.4 ± 25.8 | 24 ± 28.1 | 16.2 ± 10.7 | 0.62 |
| 2 Days before PM10 (μg/m3) |
20.8 ± 19.2 | 22.6 ± 29.3 | 24.4 ± 29.2 | 16.6 ± 11.3 | 0.24 |
| 3 Days before PM10 (μg/m3) |
21.3 ± 21.6 | 21.7 ± 26.9 | 20.4 ± 13.2 | 17.2 ± 13.4 | 0.87 |
| 4 Days before PM10 (μg/m3) |
21.7 ± 24.2 | 20.6 ± 20.3 | 19.8 ± 12.9 | 20.8 ± 14.4 | 0.75 |
| 5 Days before PM10 (μg/m3) |
21.6 ± 23.8 | 20.8 ± 21.2 | 20.6 ± 16.1 | 19.2 ± 15 | 0.89 |
ACS: acute coronary syndrome; PM: particulate material; PM10: particulate material with diameter < 10 µm.
Table 3.
Influence of the levels of PM, gaseous pollutants, temperature and humidity upon the incidence of ACS (on the day of admission) in patients under 55 years of age. The influence of PM is reported per variations of 10 μg/m3.
Table 3.
Influence of the levels of PM, gaseous pollutants, temperature and humidity upon the incidence of ACS (on the day of admission) in patients under 55 years of age. The influence of PM is reported per variations of 10 μg/m3.
| Atmospheric variable | IRR (95% CI) |
|---|---|
| PM10 (μg/m3) | 1.1 (95% CI 0.8-1.52) |
| PM2.5-10 (μg/m3) | 0.84 (95% CI 0.55-1.29) |
| PM2.5 (μg/m3) | 1.01 (95% CI 0.82-1.24) |
| SO2 (μg/m3) | 1.01 (95% CI 0.91-1.1) |
| NO2 (μg/m3) | 1.03 (95% CI 0.98-1.1) |
| O3 (μg/m3) | 1 (95% CI 0.99-1.01) |
| Temperature (ºC) | 1 (95% CI 0.89-1.1) |
| Humidity (%) | 1 (95% CI 0.99-1) |
PM: particulate material; PM10: particulate material with diameter < 10 μm; PM2.5-10: particulate material with diameter 2.5-10 μm; PM2.5: particulate material with diameter < 2.5 μm; SO2: sulfur dioxide; NO2: nitrogen dioxide; O3: tropospheric ozone.
Table 4.
PM10 concentrations (µg/m3) according to the number of ACS a day in patients over 55 years of age.
Table 4.
PM10 concentrations (µg/m3) according to the number of ACS a day in patients over 55 years of age.
| Day | No ACS/day N = 723 |
1 ACS/day N = 646 |
2 ACS/day N = 321 |
3 or more ACS/day N = 134 |
P-value |
|---|---|---|---|---|---|
| Day of admission PM10 (μg/m3) |
22.1 ± 25.9 | 20.4 ± 19.3 | 22.2 ± 24.2 | 20.4 ± 15.5 | 0.84 |
| 1 Day before PM10 (μg/m3) |
22.5 ± 25.8 | 21.1 ± 22.7 | 20.9 ± 14.7 | 18.1 ± 21.12 | 0.64 |
| 2 Days before PM10 (μg/m3) |
22 ± 22.8 | 20.8 ± 22.4 | 21.4 ± 23.9 | 21.8 ± 23.4 | 0.89 |
| 3 Days before PM10 (μg/m3) |
21.9 ± 22.4 | 20.5 ± 21.6 | 22 ± 26.4 | 20.7 ± 23.1 | 0.85 |
| 4 Days before PM10 (μg/m3) |
21.1 ± 20.9 | 21.3 ± 22.4 | 22 ± 26.8 | 21.1 ± 25.7 | 0.99 |
| 5 Days before PM10 (μg/m3) |
21.4 ± 24.4 | 20.5 ± 19.5 | 22.2 ± 24.9 | 23.9 ± 25.9 | 0.75 |
ACS: acute coronary syndrome; PM: particulate material; PM10: particulate material with diameter < 10 µm.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



