
Submitted:
22 March 2024
Posted:
25 March 2024
You are already at the latest version
Abstract
Abstract: Delayed initiation of effective antifibrotic therapy in patients with interstitial lung diseases (ILD) may influence the progression and outcome of the disease. This study analyzes the differences in the journey of patients with ILD in the Brazilian and Mexican health systems. An evaluative study was conducted in reference centers for interstitial lung diseases in Brazil and Mexico with a panel of four specialists. The patient's journey in both countries begins when the patient seeks medical care after observing a chronic respiratory symptom. In both countries, due to diagnostic complexity, these patients arrive at ILD referral centers at an advanced stage of the disease. Once diagnosis is established, the treatment onset differs between Mexico and Brazil. Antifibrotic drugs are not yet available by SUS in Brazil, and the purchase is unfeasible for most of the population, which forces specialists to only offer support to patients until the treatment can get the drug. In Mexico, antifibrotics have been available in health sectors since 2018. Brazil and Mexico have several similarities regarding the initial journey of the patient due to diagnosis difficulties, but the outcome tends to be different due to a difference in access to treatment with antifibrotics. For this reason, advancing health policies that ensure proper treatment for patients with ILD is crucial for the sustainability and reliability of the health system.
Keywords:
Interstitial Lung Diseases
; Pulmonares Intersticiais
; Enfermedades Pulmonares Intersticiales
; Therapy Access
1. Introduction
Interstitial Lung Disease (ILD) is a heterogeneous term for different diffuse parenchymal lung diseases of considerable variability in clinical, radiological, and pathological features, in addition to distinct treatment and prognosis.[1,2] Interstitial lung diseases (ILDs) may be related to systemic diseases, environmental exposures, or an unknown cause, the latter being referred to as idiopathic interstitial pneumonia. Due to the similarities in the clinical presentation, it is convenient to group interstitial diseases with the different forms of bronchiolitis, alveolar diseases, and pulmonary vasculitis.[2]
Pulmonary fibrosis is currently believed to be an epithelial-fibroblastic disease in which unknown endogenous or environmental stimuli disrupt the homeostasis of alveolar epithelial cells, resulting in diffuse epithelial cell activation and aberrant epithelial cell repair, that provokes the migration, proliferation, and activation of mesenchymal cells with the formation of fibroblastic/myofibroblastic foci, leading to the exaggerated accumulation of extracellular matrix with the irreversible destruction of the lung parenchyma.[3,4] Therefore, fibroblasts' and myofibroblasts’ apoptosis resistance in the repair of the alveolar epithelium may contribute to the fibrotic process in idiopathic pulmonary fibrosis.[5]The ILD group encompasses more than 200 diseases of different etiologies [5] , including autoimmune disorders, drug-induced respiratory disease, radiation therapies, occupational exposures (e.g., asbestosis), and allergens related to hypersensitivity pneumonitis (HP). [1]
Idiopathic Pulmonary Fibrosis (IPF) remains the prototype of progressive fibrotic interstitial lung disease.[6,7] Although less frequent than HP and ILD related to systemic connectopathies (CTD-ILD)[8], IPF has an apparently increasing incidence and assumes great clinical importance due to its severity.[7] IPF belongs to the family of idiopathic interstitial lung diseases, predominantly affecting elderly men, with a mean survival of 2.9 years in the absence of specific treatment.[9,10,11]
Distinguishing the various presentations of ILDs is a key factor in defining appropriate treatment and prognosis. Essentially, interstitial pneumonias are characterized by varying degrees of inflammation and fibrosis, determined by individual characteristics and pathophysiology of the disease. Histological findings are closely associated with specific radiological patterns, whose definitive diagnosis may require lung biopsy.[1]In this scenario, diagnosing and treating ILDs remains challenging even for the specialist. Therefore, diagnosing the disease requires the integration of clinical-radiological correlation with pulmonary pathology, which demands multidisciplinary work and introduces complexity to patient assistance.[2,12,13]
Early diagnosis based on the decline in lung function and chest computed tomography abnormalities is critical for the appropriate clinical management of these patients.[14]
Interstitial involvement in collagen diseases is associated with a worse prognosis and is indeed the most frequent cause of death in Systemic Sclerosis (SSc).[14,15]In the age of antifibrotic therapies, it is indisputable that imaging tests play a fundamental role in early diagnosis and prognosis. Diagnostic accuracy such as that of high-resolution computed tomography (HRCT) of the chest is, in fact, high enough to detect even subclinical changes that occur in early-stage ILD.[15]
ILD is characterized by early pulmonary infiltration and is classified into (1) usual interstitial pneumonia (UIP); (2) non-specific interstitial pneumonia (NSIP); (3) diffuse alveolar damage (DAD); (4) organizing pneumonia (OP); (5) lymphoid interstitial pneumonia, based on histopathological data. Some patients directly exhibit end-stage pulmonary fibrosis with unclassifiable ILD patterns.[14]
State-of-the-art care for ILD patients may include anti-inflammatory and anti-fibrotic drugs, pulmonary rehabilitation programs, nutritional and psychological support, and oxygen therapy. In severe cases with progressive worsening despite adequate therapy, lung transplantation may be considered.[8,16] ILD with progressive fibrosis shows similarities in the underlying pathogenetic mechanisms of IPF, suggesting that drugs that slow the progression of this pathology may also be effective in other progressive fibrosing ILDs.[2,8,17]
Data from the INBUILD study showed the efficacy and safety of nintedanib versus placebo in treating patients with fibrosing interstitial lung disease (ILD) with a progressive phenotype.[18,19]
This study aims to systematically analyze the journey performed by patients with ILD in the Brazilian and Mexican health systems. Additionally, a complementary assessment was carried out to understand the healthcare models in each country better, focusing on the difficulties, challenges, bottlenecks, unmet needs, and adherence to good practices in each of these reference centers in ILD in Brazil and Mexico.
2. Health System in Latin America—A Brief Description of the Health Systems in Brazil and Mexico
2.1. Brazilian Health System
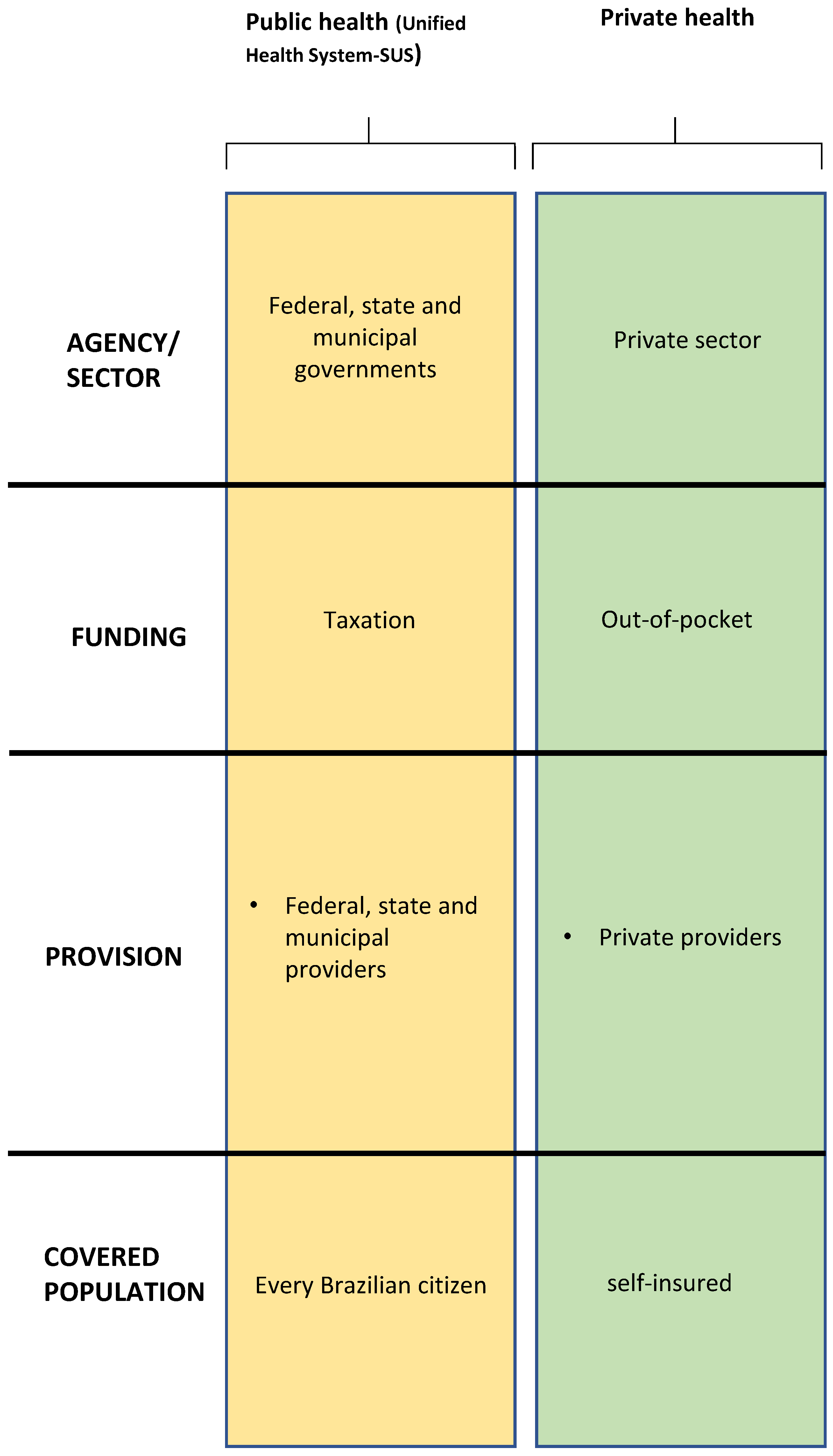
The Brazilian Constitution ensures universal, equitable, and comprehensive access to health.[20] Understanding the complexities of fulfilling this constitutional premise in a country of continental dimensions with so many social and demographic inequalities is essential.[21] The Brazilian health system comprises state public management through the Unified Health System (SUS) associated with a private supplementary health system (Figure 1).
The public system is based on SUS and is federally managed through the Ministry of Health. It provides a hybrid structure for health management with the simultaneous operation of a universal public service network and a complementary private sector.[22]The SUS is one of the world's largest and most complex public health systems, including primary care and access to medium and high-complexity medical procedures such as blood donation or organ transplantation, thus ensuring full and free access for the entire Brazilian population. With SUS, the Ministry of Health aims to ensure full, equal, and universal access to the public health system, without discrimination, guaranteed by the Federal Constitution of 1988.[20] SUS is financed with its own resources from the Union, States, and Municipalities, duly included in the Union's budget. Brazilian taxpayers share the tax burden on medical care and the coverage of the federal universal health system for everyone, regardless of whether they are employed or unemployed.[23]
The private health system is represented by private health insurance companies regulated by the National Agency for Supplementary Health (ANS). It is managed by companies that act as intermediaries between the health system's end users and service providers, using prepayment, health insurance, and compulsory contribution as financing.[22]
Figure 1.
Organization of the Brazilian health system. Adapted from: Health Systems in Transition Vol. 22 No. 2 2020.[24].
Figure 1.
Organization of the Brazilian health system. Adapted from: Health Systems in Transition Vol. 22 No. 2 2020.[24].
2.2. Mexican Health System
The Mexican health system has seven agencies divided into four sectors (Figure 2). It is segmented into several paying sources, public and private providers, organized under federal public institutions, private providers, and insurance companies. Thus, the organization of the Mexican health system varies according to financing, provision of health services, and population coverage.
The social security system is composed of three national institutions that cover formal salaried employees. The Mexican Institute of Social Security (Instituto Mexicano del Seguro Social—IMSS) covers employees in the private sector, and ISSSTE covers employees of the federal government.
The private sector, although regulated by the government, operates essentially independently. Private health insurance covers part of the population, mostly provided as an employment benefit provided by the private sector or by individual membership in higher income classes, in addition to the coverage by the IMSS or ISSSTE.[24]
3. Methods
We conducted an evaluative study in reference centers for interstitial lung diseases in Brazil and Mexico in May 2021 with a panel of four medical center program coordinators with significant regional and population heterogeneities in the cities of Porto Alegre (Brazil), Feira de Santana (Brazil), Culiacán (Mexico) and Veracruz (Mexico). The medical center program coordinators and professionals are involved in access and advocacy. This model created a favorable environment for a better understanding of the processes related to the patient's journey to encourage suggestions, share experiences, and solve problems.
3.1. Panel Study Methodology
This research design collected data from the same set of stakeholders simultaneously. This approach allows researchers to observe insights into trends, relationships, and causality. To successfully compare the healthcare systems of Brazil and Mexico, we follow a robust methodology. Panel questions were previously formulated to investigate how healthcare access changes over time in both countries and analyze the impact of policy interventions on health outcomes. A representative sample of healthcare facilities from Brazil and Mexico was selected to capture demographic variations, socioeconomic status, and geographical regions. A comparative qualitative analysis of patients´ journeys in the two countries aimed to identify patterns, trends, and differences in healthcare utilization, access, quality, and outcomes over time. Since data were collected simultaneously, we have not employed appropriate statistical techniques to analyze the longitudinal data.
3.2. Data Acquisition
At first, four focal construction panels (workshops) were held with four pulmonologists specializing in ILDs. The choice of participants followed, as a homogeneity criterion, the institutional insertion of those involved and their role in the health system.[26] Each of the specialists was interviewed individually to understand better the journey of patients in each location and the determinants related to the functioning of each local health system, access to the specialized center, diagnosis, and treatment.
In a second moment, a workshop was conducted in a web conference format, where the same specialists had the opportunity to discuss and share their experiences in treating patients with ILD. This discussion addressed patient access and flow, the centers' infrastructure, diagnosis, treatment, and multidisciplinary teams.
The meeting was held in an open discussion format, led by an external professional moderator. It was guided by standardized questions built after exploratory analysis extracted from the results of the first stage, in which panelists were encouraged to share experiences, problems, solutions, and controversies.
4. Results
4.1. Patient’s Journey
In both countries, the patient's journey begins when he or she seeks medical care after observing a chronic respiratory symptom.
In Brazil, the patient is admitted to the health system by a general practitioner from SUS or the supplementary health system. This patient may experience a long gap between the first appointment and the final diagnosis of an ILD, often established by a pulmonologist. In the Brazilian health system, according to local specialists, up to 40% of patients have private health insurance, which provides easier access to complementary exams and specialized care; the other 60% depend exclusively on SUS, where there are usually barriers to quick access to more complex tests, such as HRCT and biopsy, as well as appointments with specialized physicians.
The Brazilian public centers for interstitial lung diseases included in this study have different management and funding systems, which can influence the treatment dynamics for these patients. Santa Casa de Misericórdia is a non-profit organization that receives resources from the Ministry of Health and state government, and the Hospital Estadual Cleriston Andrade is linked to the State University of Feira De Santana, which receives resources from SUS and, as a teaching hospital, also receives funds from the Ministry of Education.
In Mexico, two different realities were presented with variable autonomy and speed of resolution according to the funding source. However, access to specific treatment was similar in both ways.
In a navy hospital serving Mexican armed forces workers, access to specialized care is usually shorter. When suspecting lung disease, the primary care physician requests a thoracic image test and forwards the patient to a pulmonologist.
In hospitals linked to the ISSSTE, the patient is initially evaluated by the primary care that, upon noticing an abnormality, requests a HRCT scan or chest x-ray. In case of radiological abnormalities, the physician presents the case to a specialist and if necessary, the patient is referred to a pulmonologist.
In Mexico, the distance between hospitals and a referral center seems to influence access to a specialist. According to Mexican specialists, patients at institutions closer to the referral hospital may experience faster access to specialized care. The average waiting time for an evaluation by a pulmonologist is more than 30 days, and most patients have already undergone an HRCT scan.
Patients from other cities or states may experience a longer journey due to the bureaucratic access barriers to specialized centers. However, according to experts, telemedicine has been an extremely useful tool in this process, allowing physicians from different provinces to consult an ILD specialist. A face-to-face consultation can be promptly scheduled if the diagnostic suspicion is confirmed.
Both countries face a very similar reality regarding the long delay between initial symptoms and the diagnosis of ILD. Generally, these patients are admitted to the ILD referral centers at an advanced stage of the disease due to diagnostic complexity. This trend may be partially explained by ILD symptoms that are also common to other respiratory diseases such as asthma or COPD.
The patient journey begins at the primary care level (Figure 3), where a general practitioner usually conducts the patient’s initial investigation. In this scenario, interstitial pulmonary pathologies are often misdiagnosed as more prevalent illnesses such as COPD, asthma, or heart failure. This patient may receive inaccurate management until achieving a confident ILD diagnosis. Indeed, a crucial step in this patient's trajectory is HRCT scanning. Radiologists used to identify patterns of interstitial pulmonary involvement usually suggest the diagnosis of lung fibrotic disease, which speeds up the patient's referral to a specialist. According to experts, The elapsed time between the patient's first contact with a doctor and the definitive diagnosis of ILD can be long. In Brazil, the diagnostic process can take from 6 to 18 months. In the Mexican system, the time for the patient to reach the specialist can vary from 1 to 12 months.
In ILD referral centers, the patient undergoes a clinical investigation aimed at underlying pathology that usually includes pulmonary function testing with lung volumes and diffusion capacity, autoantibody testing, a 6-minute walk test, and, sometimes, a lung biopsy or a follow-up HRCT scan.
With the definitive diagnosis, the next step in this patient's journey is access to adequate treatment, which may be challenging (Figure 3). At this specific point, there is a difference between Mexico and Brazil, as in the latter, antifibrotic drugs are not yet available by SUS. Elevated cost is a significant barrier to the direct purchase of antifibrotic drugs by most of the population. Most of the time, patients must resort to the judicial system to guarantee access to medication through SUS (Figure 3).
The judicialization consists of the search for treatments (medicines, exams, surgeries) through lawsuits. This occurs when the patient cannot obtain these resources through the Unified Health System (SUS) or a private supplementary health system. The judicialization of health is characterized by the court's claim of medicines developed to treat rare or highly complex clinical conditions unavailable in the public network or the supplementary health system.
In Brazil, the lack of availability of these drugs in SUS leads specialists to offer only supportive care, such as oxygen supplementation, until the patient can obtain the medication through litigation; differently, in Mexico, antifibrotic drugs have been available in different health sectors since 2018, and it may take from 1 week to 1 month until treatment is initiated.
4.2. Antifibrotic Therapy for ILD
The Brazilian National Health Surveillance Agency (ANVISA) has already approved both antifibrotics, Nintedanibe esilate and Pirfenidone,[27,28] for use in Brazil. Still, the National Commission for the Incorporation of Technologies (CONITEC) has not yet incorporated these antifibrotics into the public health system.[29]According to experts, Brazilian patients have access to antifibrotics through litigation, a process that can take up to 8 months to complete. In Mexico, antifibrotics were analyzed and incorporated in different sectors of public health, thus making it possible to offer a broader antifibrotic treatment to patients with idiopathic pulmonary fibrosis (IPF). [30]
In 2018, the Mexican government, through the Comisión Permanente del H. Congreso de la Unión, classified Idiopathic Pulmonary Fibrosis (IPF) as a catastrophic disease, supporting actions and strategies to prevent, detect and, when appropriate, provide timely treatment for this condition.[31]
The classification of IPF as a catastrophic disease is due to its high cost of treatment associated not only with the direct costs of antifibrotic therapies but also with other associated expenses, such as nutritional and psychological therapy, pulmonary rehabilitation, supplementary oxygen, hospitalization, and the increased risk of acute exacerbations.[30]
The Mexican coordinators explained that antifibrotic drugs can only be prescribed by a specialist inside the registered reference centers, thus allowing for greater control over prescriptions.
Mexican specialists highlighted that the treatment of IPF, the integration of the centers of reference in a network, and the consequent reduction of the bureaucracy to prescribe antifibrotic drugs are key factors for the clinical care of IPF patients. Essential factors for proper patient care include staff familiarity with this disease and the necessary resources such as HRCT and pulmonary function tests. The Mexican specialists also emphasize that patients under antifibrotic treatment are monitored exclusively by pulmonologists, improving patient safety.
About the decision-making regarding the use of the antifibrotic medication, we notice certain autonomy that may vary depending on the health sector. The Naval hospital receives a portion of the funds allocated to the armed forces by the federal government, and validation by a pulmonologist is required to request the use of antifibrotic for a patient. For most patients, the decision takes place in a multidisciplinary discussion with a pulmonologist, a rheumatologist, a pathologist, a chest surgeon, and a radiologist. In hospitals linked to ISSSTE, which have a previously established budget, it is mandatory to rule out other alternative diagnoses, since IPF is an idiopathic disease, and to complete a checklist to allow the prescription of antifibrotics. A central committee must validate all data regarding the diagnostic criteria.
4.3. ILD Associated to COVID-19
According to the experts who participated in the panel, both countries experienced a significant burden of COVID-19 in the health systems.[32] The prevalence of post-COVID-19 fibrosis will become apparent with time, but early analysis from patients with COVID-19 on hospital discharge suggests that more than a third of recovered patients develop fibrotic abnormalities.[33] One study showed that 4% of patients with a disease duration of less than 1 week, 24% between weeks 1 and 3, and 61% of patients with a disease duration of greater than 3 weeks developed fibrosis.[34]
In Brazil, COVID-19 profoundly impacted clinical follow-up and diagnostic procedures in ILD patients. With social isolation and lack of medical follow-up, the progression of the disease has been frequently described with a potentially higher risk of acute exacerbations, in addition to numerous cases of fibrosing disease secondary to COVID-19, including the need for specific outpatient clinics for the follow-up of these patients. There is particular concern that patients with COVID-19 remain symptomatic, a condition known as long-term COVID-19, and are at increased risk of bronchial remodeling and fibrosis.[35] The pandemic overloaded the health system and limited access to pulmonary medical specialists, thoracic imaging, and pulmonary function tests. This complex scenario favored further diagnostic delays, including new cases of interstitial disease that were not adequately evaluated.
In Mexico, patients were instructed to maintain social isolation at home with their medications dispensed in the hospital to a proxy. Enough antifibrotic medication has been dispensed for several months of treatment, and some patients have remote medical follow-ups by telemedicine.
Additionally, imaging tests performed in patients with a suspected or confirmed diagnosis of COVID-19 have favored the identification of radiological findings compatible with ILD; as patients seek urgent medical care for suspected COVID-19, previous underlying interstitial disease could be early detected.
5. Discussion
Brazil and Mexico share several similarities regarding the patient's journey with interstitial disease. In both countries, the advanced stage of the disease is unfortunately common at the first evaluation at the referral center due to the diagnostic challenges, barriers to accessing specialized care, and high complexity testing. Furthermore, the patient is initially evaluated by a general practitioner who is usually not trained to identify the signs of interstitial disease, favoring misdiagnoses with more prevalent diseases, such as asthma or COPD. This is similar to what is reported in other countries.[36]
This interstitial patient may receive several diagnoses until referred to a pulmonologist. This pre-diagnostic period, which takes place before the patient arrives at the referral center, is very important in the patient's journey and one of the main bottlenecks. In Brazil, the patient takes an average of 12 months to be referred to a pulmonologist; in Mexico, this period lasts 8 months on average. This delay in concluding the diagnosis and the consequent initiation of treatment may potentially favor the progression of the disease.
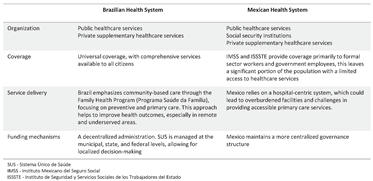
The health systems of Brazil and Mexico exhibit notable differences in organization, funding, coverage, and service delivery. Each country's unique socio-economic and political landscapes shape these distinctions, resulting in a distinct approach to healthcare provision (Table 1).
One of the main differences lies in the funding mechanisms. Although hiring a private supplementary healthcare service in Brazil is possible, the Brazilian health system is based on the Unified Health System (SUS), which guarantees all citizens free access to healthcare services. Nevertheless, Mexico operates a segmented healthcare system where individuals may receive coverage through various channels: social security institutions, private insurance, or public healthcare services. This fragmented approach can lead to disparities in access based on employment status and income.
Coverage is another distinguishing factor. Brazilian SUS aims for universal coverage, with comprehensive services available to all citizens. However, due to resource limitations, service quality and availability disparities can still exist between regions. In contrast, Mexico's system has multiple insurance schemes, including the Instituto Mexicano del Seguro Social (IMSS) and the Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (ISSSTE), which provide coverage primarily to formal sector workers and government employees. This leaves a significant portion of the population, often in the informal sector, with limited access to healthcare services.[24]
Service delivery approaches also diverge. Brazil emphasizes community-based care through the Family Health Program (Programa Saúde da Família), focusing on preventive and primary care. This approach helps to improve health outcomes, especially in remote and underserved areas.[21] While having a similar community healthcare model in place, Mexico also relies on a hospital-centric system, which can sometimes lead to overburdened facilities and challenges in providing accessible primary care services.[24]
A further aspect of differentiation lies in the decentralization of healthcare management. Brazil's Unified Health System (SUS) operates at municipal, state, and federal tiers, facilitating decision-making tailored to local needs. Conversely, although Mexico has decentralized some elements of its healthcare system, it predominantly upholds a more centralized approach to governance. Cultural diversity and indigenous populations are some other characteristics that affect health policies.[21,24] In Mexico, indigenous communities often face cultural and linguistic barriers to accessing healthcare, while Brazil has established policies to address the health needs of its diverse population.
In summary, the Brazilian and Mexican health systems differ regarding funding mechanisms, coverage models, and service delivery strategies (Table 1). Brazil's SUS prioritizes universal coverage and preventive care, while Mexico's system encompasses social security and public and private insurance schemes. Both systems face challenges in ensuring equitable access to quality healthcare, but their strategies reflect their respective societal and economic contexts.
Despite the similarities in the initial journey of patients with interstitial disease in both countries, the outcome tends to be different, largely due to access to treatment with the use of antifibrotics.
Restrictions on the direct dispensing of antifibrotics through SUS hampered the treatment of patients with interstitial disease in Brazil.[27,28] Despite being approved by ANVISA, their incorporation into SUS for treating IPF was disapproved by CONITEC, and no other interstitial disease has been analyzed to date.[29]
The Brazilian Society of Pulmonology (SBPT) [2] guidelines, published in 2012, reinforced the efficacy and safety of antifibrotic drugs in treating interstitial disease.
The long delay for treatment, especially in advanced disease with forced vital capacity (FVC) below 50%, can potentially impair the quality of life and increase the risk of exacerbations and progression of fibrosis.[12,37,38]
The diagnosis and treatment of interstitial diseases also seem to have been affected by the COVID-19 pandemic that has raged worldwide since 2019. In addition to the delay in performing complementary exams and following up on patients, there were also new diagnoses of previous ILDs related to COVID-19.
6. Conclusion
Brazil and Mexico have several similarities regarding the initial journey of the patient with interstitial disease; due to diagnosis difficulties, this patient may receive several different diagnoses until referred to a specialist. Despite the similarities in the initial journey of patients, the outcome tends to be different, mostly due to a difference in access to treatment with the use of antifibrotics.
Comprehending the patient's healthcare journey is key to increasing access to proper treatment in middle-income countries. Socioeconomic factors, cultural nuances, and access barriers may influence effective treatments. These insights enhance healthcare delivery, improve outcomes, and promote equity in resource-constrained settings.
Enhancing the patient experience for those with interstitial lung diseases (ILD) could be achieved through several strategic approaches: the expansion and integration of ILD reference centers, minimizing bureaucratic hurdles in the prescription of expensive medications, comprehensive training for healthcare teams, and improved access to diagnostic evaluations. Additionally, advocating for health policies that ensure proper treatment for patients with interstitial diseases, alongside promoting the sustainability and predictability of the healthcare system, is paramount.
Author Contributions
Conceptualization: Nathalia Filgueiras Vilaça Duarte, Daniela Carla Barbosa Campos and Gabriela Tannus Branco de Araujo.; Methodology: Nathalia Filgueiras Vilaça Duarte and Gabriela Tannus Branco de Araujo.; Validation: Nathalia Filgueiras Vilaça Duarte, Daniela Carla Barbosa Campos.; Formal analysis: Gabriela Tannus Branco de Araujo.; Data curation: Nathalia Filgueiras Vilaça Duarte and Gabriela Tannus Branco de Araujo.; Writing—original draft preparation: Gabriela Tannus Branco de Araujo.; Writing—review and editing: Nathalia Filgueiras Vilaça Duarte, Daniela Carla Barbosa Campos and Gabriela Tannus Branco de Araujo.; Visualization: Ricardo G. Figueiredo, Nathalia Filgueiras Vilaça Duarte, Daniela Carla Barbosa Campos, Manuel de Jesus Diaz Verduzco, Ángel Alemán Márquez, Adalberto Sperb Rubin.; Supervision: Adalberto Sperb Rubin.; Project administration: Nathalia Filgueiras Vilaça Duarte and Gabriela Tannus Branco de Araujo.; Funding acquisition: Nathalia Filgueiras Vilaça Duarte, Branco de Araujo.
Funding
This research was funded by Boehringer Ingelheim do Brasil Química e Farmacêutica Brazil.
References
- Mikolasch TA, Garthwaite HS, Porter JC. Update in diagnosis and management of interstitial lung disease. Clin Med. 2017, 17, 146–153. [Google Scholar] [CrossRef]
- Sociedade Brasileira De Pneumologia E Tisiologia. Diretrizes De Doenças Pulmonares Intersticiais Da Sociedade Brasileira De Pneumologia E Tisiologia. Jornal Brasileiro De Pneumologia. J Bras Pneumol. 2012, 38 Suppl. 2, S1–S133.
- Verma S, Slutsky AS. Idiopathic Pulmonary Fibrosis — New Insights. N Engl J Med. 2007, 356, 1370–1372. [Google Scholar] [CrossRef]
- Harari S, Caminati A. IPF: new insight on pathogenesis and treatment. Allergy. 2010, 65, 537–553. [Google Scholar] [CrossRef]
- Mueller-Mang C, Ringl H, Herold C. Interstitial Lung Diseases. In: Nikolaou K, Bamberg F, Laghi A, Rubin GD, eds. Multislice CT. Medical Radiology. Springer International Publishing; 2017:261-288. 2. [CrossRef]
- Spagnolo P, Ryerson CJ, Putman R, et al. Early diagnosis of fibrotic interstitial lung disease: challenges and opportunities. The Lancet Respiratory Medicine. 2021, 9, 1065–1076. [Google Scholar] [CrossRef]
- Lederer DJ, Martinez FJ. Idiopathic Pulmonary Fibrosis. Longo DL, ed. N Engl J Med. 2018, 378, 1811–1823. [Google Scholar] [CrossRef]
- Maher TM, Bendstrup E, Dron L, et al. Global incidence and prevalence of idiopathic pulmonary fibrosis. Respir Res. 2021, 22, 197. [Google Scholar] [CrossRef]
- Baddini-Martinez J, Ferreira J, Tanni S, et al. Brazilian guidelines for the pharmacological treatment of idiopathic pulmonary fibrosis. Official document of the Brazilian Thoracic Association based on the GRADE methodology. J Bras Pneumol. 2020, 46, e20190423–e20190423. [Google Scholar] [CrossRef]
- Martinez FJ, Safrin S, Weycker D, et al. The Clinical Course of Patients with Idiopathic Pulmonary Fibrosis. Ann Intern Med 2005, 142(12_Part_1), 963. [CrossRef]
- Raghu G, Remy-Jardin M, Myers JL, et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am J Respir Crit Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Elicker B, Pereira CADC, Webb R, Leslie KO. Padrões tomográficos das doenças intersticiais pulmonares difusas com correlação clínica e patológica. J bras pneumol. 2008, 34, 715–744. [Google Scholar] [CrossRef]
- Flaherty KR, Andrei AC, King TE, et al. Idiopathic Interstitial Pneumonia: Do Community and Academic Physicians Agree on Diagnosis? Am J Respir Crit Care Med. 2007, 175, 1054–1060. [Google Scholar] [CrossRef] [PubMed]
- Giacomelli R, Liakouli V, Berardicurti O, et al. Interstitial lung disease in systemic sclerosis: current and future treatment. Rheumatol Int. 2017, 37, 853–863. [Google Scholar] [CrossRef]
- Rea1 G, Bocchino2 M. The challenge of diagnosing interstitial lung disease by HRCT: state of the art and future perspectives. J Bras Pneumol 2021, e20210199. [CrossRef] [PubMed]
- European lung foundation. Interstitial lung disease (ILD). accessed in 13/04/2021 available in: https://europeanlung.org/en/information-hub/lung-conditions/interstitial-lung-disease/.
- Brown KK, Martinez FJ, Walsh SLF, et al. The natural history of progressive fibrosing interstitial lung diseases. Eur Respir J. 2020, 55, 2000085. [Google Scholar] [CrossRef] [PubMed]
- Flaherty KR, Wells AU, Cottin V, et al. Nintedanib in Progressive Fibrosing Interstitial Lung Diseases. N Engl J Med. 2019, 381, 1718–1727. [Google Scholar] [CrossRef] [PubMed]
- Lamb, YN. Nintedanib: A Review in Fibrotic Interstitial Lung Diseases. Drugs. 2021, 81, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Brasil. Constituição (1988). Constituição da República Federativa do Brasil. Brasília, DF: Senado; 1988.
- PAIM Jairnilson, Travassos CMR, Almeida CM, Bahia L, Macinko J. O sistema de saúde brasileiro: história, avanços e desafios. The Lancet 2011, 377, 11–31.
- Fiocruz. PublicoxPrivado. Acessado em junho de 2021. Disponível em: https://pensesus.fiocruz.br/publico-x-privado.
- Minas Gerais - Secretaria de Estado de Saúde. Acessado em junho de 2021. Disponível em: https://www.saude.mg.gov.br/sus.
- Mexico. Health Systems in Transition-Mexico Health System Review 2020 Vol. 22 No. 2 2020.
- Health Systems in Transition Vol. 22 No. 2 2020.
- Campos RTO, Miranda L, Gama CAP, Ferrer AL, Diaz AR, Gonçalves L, et al. Oficinas de construção de indicadores e dispositivos de avaliação: uma nova técnica de consenso. Estudos e pesquisas em psicologia 2010, 10, 221.
- Agência Nacional de Vigilância Sanitária (ANVISA) (Brasil). Consultas. Access in 21.Available in: https://consultas.anvisa.gov.br/#/medicamentos/25351456304201563/. 20 June.
- Agência Nacional de Vigilância Sanitária (ANVISA) (Brasil).Consultas. Access in 21. Available in: https://consultas.anvisa.gov.br/#/medicamentos/25351496519201517/. 20 June.
- Comissão Nacional de Incorporação de Tecnologias no SUS (CONITEC) (Brasil). Access in 21. Available at: http://conitec.gov.br/tecnologias-em-avaliacao-demandas-por-status. 20 June.
- Mexico - Secretaria de Salud Estados Unidos Mexicanos. Access in 21. Available in: https://www.gob.mx/cms/uploads/attachment/file/196773/Huerfanos_Otorgados_2015.pdf. 20 June.
- Mexico. Proposición con punto de acuerdo por el que la comisiòn permanente del h. congreso de la unión con pleno respeto a la división de poderes, exhorta a la secretaría de salud para que, en coordinación con las autoridades competentes analice definir a la fibrosis pulmonar idiopática (fpi) como una enfermedad catastrófica y fortalezca las acciones y estrategias para su prevención, detección y, en su caso, brindar el tratamiento oportuno en dicho padecimiento. Ciudad de México a, 24 de julio de 2018.
- Expert Panel: Rubin Adalberto MD, Grassman Ricardo MD, Díaz-Verduzco Manuel de Jesús MD, and Alemán-Márquez Ángel, from the Expert Panel of Reference Centers in Interstitial Lung Diseases in Latin America. June 2021.
- Rai DK, Sharma P, Kumar R. Post covid 19 pulmonary fibrosis. Is it real threat? Indian Journal of Tuberculosis. 2021, 68, 330–333. [Google Scholar] [CrossRef] [PubMed]
- Liu X, Zhou H, Zhou Y, et al. Risk factors associated with disease severity and length of hospital stay in COVID-19 patients. Journal of Infection. 2020, 81, e95–e97. [Google Scholar] [CrossRef] [PubMed]
- Guler SA, Ebner L, Aubry-Beigelman C, et al. Pulmonary function and radiological features 4 months after COVID-19: first results from the national prospective observational Swiss COVID-19 lung study. Eur Respir J. 2021, 57, 2003690. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove GP, Bianchi P, Danese S, Lederer DJ. Barriers to timely diagnosis of interstitial lung disease in the real world: the INTENSITY survey. BMC Pulm Med. 2018, 18, 9. [Google Scholar] [CrossRef]
- Vašáková M, Mogulkoc N, Šterclová M, Zolnowska B, Bartoš V, Pla ková M, et al. Does timeliness of diagnosis influence survival and treatment response in idiopathic pulmonary fibrosis? Real-world results from the EMPIRE registry. European Respiratory Journal 2017; 50 (Suppl 61): PA4880. Poster presentation at the ERS International Congress 2017, 9–13/9/2017, Milan.
- Dempsey TM, Sangaralingham LR, Yao X, Sanghavi D, Shah ND, Limper AH. Clinical Effectiveness of Antifibrotic Medications for Idiopathic Pulmonary Fibrosis. Am J Respir Crit Care Med. 2019, 200, 168–174. [Google Scholar] [CrossRef]
Figure 2.
Organization of the Mexican health system. IMSS - Mexican Institute of Social Security, ISSSTE - Institute of Social Security and Services for State Employees, PMEX - Mexican Petroleum, MoH - Ministry of Health. Adapted from: Health Systems in Transition Vol. 22 No. 2 2020.[25].
Figure 2.
Organization of the Mexican health system. IMSS - Mexican Institute of Social Security, ISSSTE - Institute of Social Security and Services for State Employees, PMEX - Mexican Petroleum, MoH - Ministry of Health. Adapted from: Health Systems in Transition Vol. 22 No. 2 2020.[25].
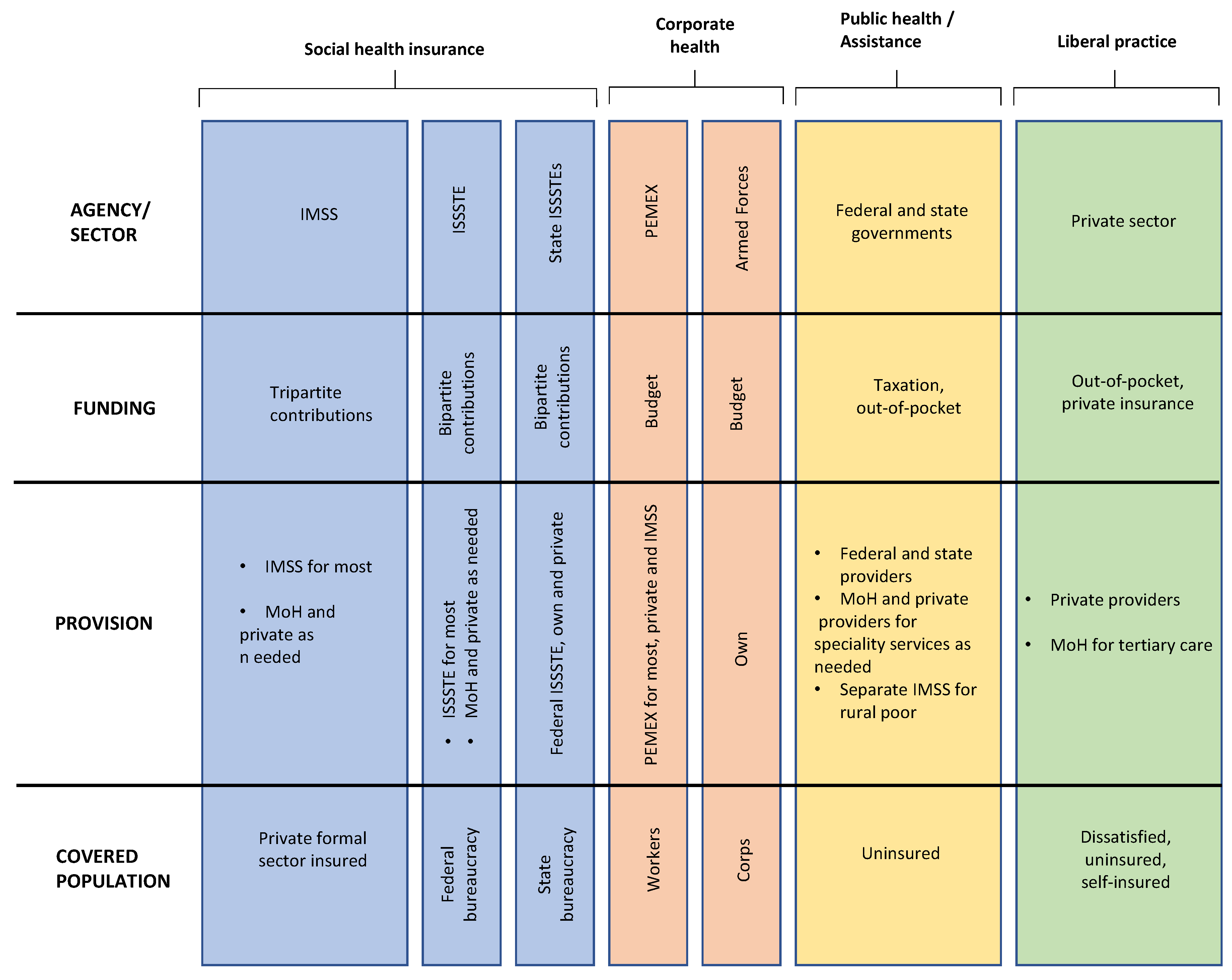
Figure 3.
Figure one schematically shows the patient's journey in the treatment of ILD as reported by experts.
Figure 3.
Figure one schematically shows the patient's journey in the treatment of ILD as reported by experts.
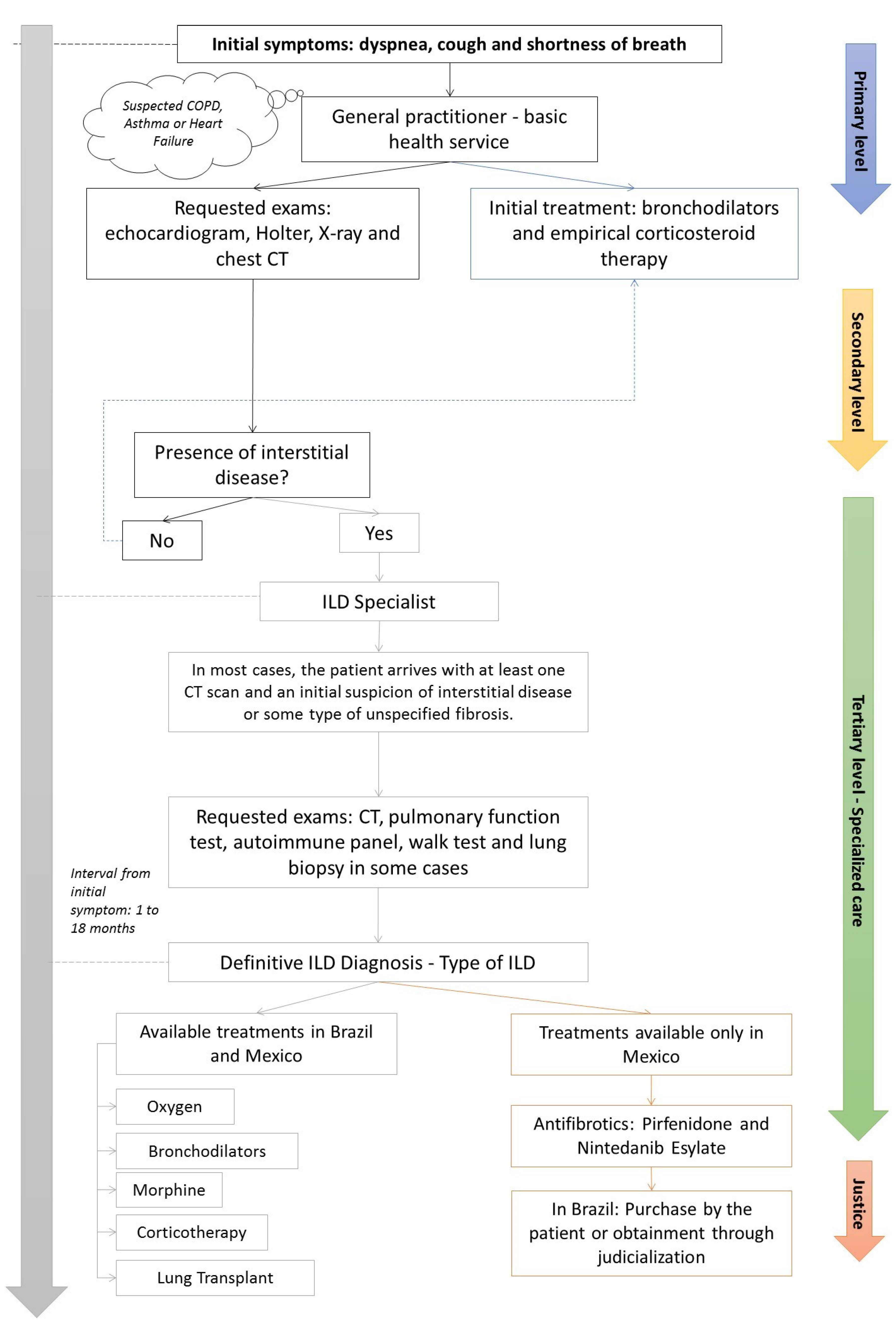

Table 1.
Differences between the Brazilian and Mexican Health systems.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



