
Submitted:
24 March 2024
Posted:
26 March 2024
You are already at the latest version
Abstract
Introduction
Paramedic practice is highly variable, occurs in diverse contexts, and involves the assessment and management of a range of presentations of varying acuity across the lifespan. As a result, attempts to define paramedic practice have been challenging and incomplete. This has led to inaccurate or under-representations of practice that can ultimately affect education, assessment, and the delivery of care. In this study, we outline our efforts to better identify, explore, and represent professional practice when revising a national competency framework for paramedics in Canada.
Methods
We used a systems thinking approach to identify the settings, contexts, features, and influences on paramedic practice in Canada. This approach makes use of the role and influence of system features at the microsystem, mesosystem, exosystem, macrosystem, supra-macro system, and chronosystem levels in ways that can provide new insights. We used methods such as rich pictures, diagramming, and systems mapping to explore relationships between these contexts and features.
Findings
When we examine the system of practice in paramedicine, multiple layers become evident and within them we start to see details of features that ought to be considered in any future competency development work. Our exploration of the system highlights that paramedic practice considers the person-receiving care, caregivers, and paramedics. It involves collaboration within co-located and dispersed teams that are composed of other health and social care professionals, public safety personnel, and others. Practice is enacted across varying geographical, cultural, social, and technical contexts, and is subject to multiple levels of policy, regulatory, and legislative influence.
Conclusion
Using a systems thinking approach, we developed a detailed systems map of paramedic practice in Canada. This map can be used to inform the initial stages of a more representative, comprehensive, and contemporary national competency framework for paramedics in Canada.
Keywords:
systems thinking
; paramedicine
; Canada
; paramedic practice
; competency
Introduction
Defining or describing the competencies necessary for paramedic practice in Canada is challenging given the diverse range of clinical events, and variable contexts in which they practice. This requires a broad set of competencies that can be difficult to define due to the complexity, unpredictable nature, and broad range of clinical events and demands that then become inherently associated with paramedic practice. Clinical events may include a range of acute or chronic medical and trauma related concerns, comorbidities, and complex social conditions across the life span. Much like the utilization of emergency departments [1], the public has expanded its use of paramedic systems, without much restriction on when or where these events occur (e.g., industrial sites, homes, clinics, workplaces, remote communities, wilderness) [2,3,4,5,6], differentiating paramedics from nearly every other health professional. Consequently, scopes of practice and models of care are continuously shifting and expanding. For instance, emerging community-based models of care involve paramedics functioning beyond traditional emergency response, such as follow-up services for emergency calls, prevention programs, and active engagement in home support [7,8,9,10]. This evolving diversity of practice presents a challenge when attempts are made to describe it.
This challenge has resulted in a disconnect between the experiences of paramedics and the competencies and ultimately educational practices that guide them. Despite paramedics caring for people from a variety of environmental, social, and cultural contexts, these and likely other factors have traditionally been poorly addressed. For example, while older adults account for approximately 50% of paramedic patient encounters [11], there is a noticeable lack of attention on this patient population in paramedic curricula nationally. Paramedics regularly care for people with chronic and undifferentiated disease presentations, yet are often not part of the interdisciplinary primary care workforce [12,13]. Paramedic education - and the competency frameworks that guide it [14] - remains largely focused on acute exacerbations and an isolated, event based model of care. This pattern of misalignment of paramedic experiences with paramedic education is particularly noticeable when we look for competencies intended to guide the care of marginalized and under-served populations, such as those who are victims of human trafficking and modern-day slavery, or for those experiencing mental health issues, substance use, and homelessness [15,16,17].
Regional variation presents an additional challenge when we attempt to describe paramedic practice [18]. A paramedic who works in remote or isolated communities where health care resources may be more difficult to access, likely requires additional or varied competencies when compared to those whose practice in an urban setting. Similarly, simply adopting the competencies of international frameworks [19,20,21], is likely to discount regional differences in healthcare policy priorities and approaches, societal expectations, resources, and access to and distribution of services. Even if some competencies can be generalized, translating descriptions of paramedic practice from one jurisdiction to another ignores this local variation and contextual needs, leaving room for ongoing or introducing new, alignment concerns.
We previously examined competency framework development processes and outputs in detail [22]. Despite being a necessary link between practice and downstream processes such as curriculum or assessment [23], competency frameworks often fail to adequately define or describe practice, in part because of the methods or conceptual frameworks applied, leading to potential for missed details that threaten the validity and utility of the output. In response, we offered improved development guidance that included a conceptual framework to explore practice informed by systems thinking [23], a methodological approach that synthesized and advanced existing approaches [24], and a robustly developed reporting guideline [25]. Thus, we argue for the importance of accurately identifying and reporting competencies in a way that promotes access to proficiency in these competencies through entry-to-practice education.
In this study we leverage systems thinking as a conceptual framework intended to make visible features of ‘practice in context’ that may have or continue to be overlooked when developing competency frameworks [23]. Our intention here is not to develop the competency framework, but to identify the features that would need attention when that step is taken. While a competency framework can never fully represent the influences, contexts or competencies required for professional practice, in this paper we outline and demonstrate our efforts to apply our guidance related to competency framework development to better represent paramedic practice, to support the development of the National Competency Framework for Paramedics (NCFP) [26] and demonstrate the utility of that guidance in practice.
Methods
Overview
We used a systems thinking approach, which includes both ecological systems theory [27] and complexity theory [28] to guide our work. These two theories were recently combined by Batt et al. [23] as a means of better examining the various levels that may be useful in competency framework development. When examined using this combined systems lens, systems thinking obligates attention to micro, exo, macro, supra-macro and chrono-system levels (described in more detail below), providing new and often ignored insights. This approach permits the use of multiple methods and assumes an interpretive but predominantly realist philosophical stance [29]. In this study we used a literature review and system mapping process to identify relevant features that might be useful in structuring a competency framework. We describe how we defined our target system (a necessary boundary), and details about and positionality of the individuals who participated in the work (i.e., our development group), and then outline the existing framework and mapping process. We then present findings organized using the system thinking approach described above.
Defining the System
First, we defined the system of paramedic practice for this study as a system to provide person-centred care in emergency, urgent, unscheduled, and scheduled care contexts by means of educated and regulated paramedics, to reduce morbidity and mortality, improve quality of life and experience, and increase access to healthcare. Sensitized by our conceptual framework [23], we identified the relationships between system levels, and components, in ‘real-world’, non-linear contexts.
Positionality of the Researchers
A development group (DG) led the data collection, analysis, and drafting of the competency framework for the NCFP project. Members were recruited by the DG lead (**) to represent a variety of clinical practice, education, research, governance, regulatory, policy, leadership, and advocacy experiences within and outside of paramedicine. The DG was composed of 19 individuals from across Canada with experience across multiple contexts of paramedic practice in urban and rural settings, including emergency care, community, military, remote and isolated, critical care, substance use, special operations, interprofessional primary care, and palliative care. They also had experience in regulation, clinical governance, health systems leadership, research, education, policy and strategy, social work, and private industry. Most of the group had postgraduate qualifications, and resided in Ontario, followed by British Columbia. Several of the group were bilingual (English and French), while the remainder spoke English as their primary language. Most of the group identified as Canadian, female, and white. ** is a member of the Mohawks of the Bay of Quinte First Nation.
This collaborative project was conducted on colonised Indigenous lands now referred to as Canada. These lands are home to the many diverse First Nations, Inuit and Métis Peoples whose ancestors have stewarded this land since time immemorial.
Existing Descriptions of Practice
While it can be difficult to identify existing representations of practice, we identified several sources that were used as stimuli for additional sources until we had reached a representative sample of how the community was describing itself. Our explorations of paramedic practice in Canada started with existing descriptions - namely the National Occupational Competency Profile 2011 [14], the Paramedic Profile [30,31], the Canadian Paramedicine Education Guidance document [32], and the Principles to Guide the Future of Paramedicine in Canada [18,33]. Following this, we sought contemporary literature related to paramedicine in Canada [34,35,36]. informed by three recent comprehensive reviews of the Canadian paramedicine literature [37,38,39].
System Mapping
We enacted our systems thinking using a multi-stage system diagramming approach [40]. First we aimed to capture and represent layers of our complex system using “onion diagrams” [40]. This also allowed us to brainstorm potential elements and features of the system. Next we used “rich pictures” [40,41] to explore paramedic practice in differing contexts. Some of these were created by attendees at a community paramedicine workshop in February 2020 after we asked attendees to draw rich pictures of what it is that paramedics do in the community. We then translated these initial ‘messy’ visual explorations of the system into an overall concept map [40,42] intended to organize and represent our developing knowledge (See Supplementary File 1).
Next we undertook an iterative process of “influence mapping” [40], to identify the relationships between elements in the concept map, and as a means of capturing and expressing the complex web of relationships within and between levels. This allowed us to analyze identified items and their relationships particularly with how systems thinking is organized and with insights from the paramedicine literature described above. For example, we used the previously published system level principles intended to guide paramedicine in Canada [18] to identify gaps and/or where alignment could be found. Finally, we combined the results of our diagramming methods and insights from the paramedicine literature to create a system map [40] of paramedic practice in Canada; collectively visually representing the complex systems, various components, and their interactions.
Using iterative group sessions, the systems map was refined at several instances from 2021 to 2024 and left open to identify contemporary data sources that might have emerged as we continued developing the NCFP. Copies of these diagrams are contained in Supplementary File 1. Next, we describe our findings, illustrate the complexity evident at each system level, and offer some potential implications for development of the NCFP.
Results
Person-Centred - Putting Patients and Their Communities First
Clinical microsystems are embedded in larger systems and are by their definition “patient centred” [23,43]. This obligates attention to the person receiving care and their individual circumstances [18]. When we applied this lens we were sensitized to the fact that influences on individuals’ health status are often complex [44]. People may have a history of chronic medical conditions, social barriers, or other influences on their health that paramedics should be aware of in order to inform a collaborative approach to decision making, care management and disposition planning [44,45,46].These may include multiple, often intersecting social and structural determinants of health such as: class, income, poverty, housing, education, employment status, food security, access to health services, environment, social exclusion, social safety nets, gender, disability, race, ethnicity, and early childhood development [47,48]. Additional influences on peoples’ health may include age, cultural norms, colonial influences, religious beliefs, dependencies, and occupational demands [47,49,50,51]. These findings indicated the importance of social determinants of health, socially responsive advocacy, and the need for culturally competent paramedics.
Microsystem - Considering the Paramedic as a Person
The microsystem refers to the immediate clinical practice environment, and all components within it [43]. This necessitates attention to the people involved, their relationships, and their influences on person-centred care [23]. We observed that paramedic practice is unique in that it can encompass all forms of clinical presentations, in unpredictable environments, and with diverse social and cultural contexts [52,53,54,55]. Paramedics are regularly subject to emotionally challenging work, violence [56,57], high rates of occupational injury [54,58,59], stress and mental health issues [60,61,62,63], poor physical health status [18,64,65], and the effects of shift-work [66,67,68,69]. In addition, paramedics are often required to make clinical decisions with limited information [70,71,72]. Despite such limited information, they must maintain a high level of situational awareness (Hunter 2019) and must possess other non-clinical attributes such as empathy, honesty, professionalism, conflict resolution and assertiveness [36,73,74,75]. Our observations of features at this level of the system highlighted the need to engage meaningfully with Indigenous communities around the impacts of colonialism and systemic racism and the implications for practice.[76] A focus on paramedic health and wellbeing should be considered when developing the competency framework. Finally, our findings supported the pursuit of inclusivity, diversity, equity, and accessibility when developing the NCFP [77].
Mesosystem - Appreciating the Influence of People, Policies, and Procedures
The mesosystem represents the interactions that occur between people, and the enactment of policies and procedures [23]. While healthcare services exist at the exosystem level (described in more detail below), the delivery of such services takes place via the mesosystem and this obligates attention to policies, relationships, and professional values. Policy trends at the exosystem level can inform aspects of interprofessional care, and this is enacted in the mesosystem. Within the mesosystem, paramedics interact and communicate with other agents, directly and indirectly related to patient care [58]. These include people receiving care, caregivers and care team members, members of the interdisciplinary team (e.g., other health and social care professionals, personal support workers), public safety personnel (e.g., dispatchers, police, and fire personnel), health services leadership, and members of the public [78,79]. Differences in professional values and cultural expectations could be another instance where practice (reflected in a competency framework) and care needs are poorly aligned. Interprofessional relationships risk being overlooked when professions develop a competency framework - defining professional competencies may be viewed as an activity exclusive to that profession and may disregard the role of other agents and the relationships between them. Our findings at the mesosystem level suggest that it is necessary to engage other health and social care professionals, people receiving care, caregivers, Indigenous paramedics and communities, and the public when developing the NCFP [80,81,82] .
Exosystem - Identifying Service Delivery Models and Contexts of Paramedic Practice
The exosystem refers to the community level or the service delivery level (e.g., hospitals, clinics, healthcare services) [23]. This requires identifying and attending to different models of service delivery, populations served, and places in which paramedic practice is enacted. We identified multiple forms of paramedic service delivery, which included emergency response, patient transport, community paramedicine, virtual care, and clinic or hospital based practice [10,18,44,83,84]. Each of these models of care influence the practice of paramedics within them. For example, community engagement and “practice in context” distinguish community paramedicine models [85], and these along with integration models of paramedic practice have emerged as a solution to local healthcare needs. Many paramedicine models evolved in response to the COVID-19 pandemic, embracing further social initiatives, and expanding the diverse communities and populations served by programs [34,83,86,87]. Research highlighted paramedics providing care for people with non-urgent presentations [88], and palliative needs [52,89]. Paramedic practice is enacted through various models in remote and rural, military, industrial, expedition, and [2,90]. Our findings in the exosystem directly suggest the need to explore a variety of diverse practice settings and models of care when developing the competency framework. This might be achieved, for example, by establishing working groups composed of those with expertise in these various settings and models.
Macrosystem - Acknowledging Regional, Provincial, and Federal Influences
The macro-system contains regional, provincial, and federal influences such as government policies, culture, religious movements, the economy, and societal issues [23]. This requires attention to how paramedics are educated, regulated, funded, and positioned to provide care. We identified that paramedics are governed by a variety of clinical oversight or regulatory models across Canada, along a spectrum from no regulation, to government body regulated, to self-regulated [91,92]. Regulatory models exert significant influence on education, service design and delivery, clinical scope of practice, and clinician autonomy. Paramedic education standards are as diverse as the regulatory models that exist and vary significantly in duration, form and intended outcomes across, and within jurisdictions. Education exerts subsequent influence on clinician autonomy, career development, decision making, and the development of both clinical and non-clinical attributes. Socio-political impacts on health are also evident at this level in relation to health policy choices such as promoting (or not) public health interventions, funding (or de-funding) services, expanding (or limiting) access to certain health services, and the introduction of legislation that impacts health. Funding of paramedic services ranges from government-funded at all levels to subsidized programs and those that depend on payment from individuals or their health insurance plans [93]. Our observations at this level suggest the need to attend to the variations in regulation, education, funding, scope of practice, and other elements across Canada when developing the NCFP. This may be achievable by avoiding granularity when identifying competencies that may be influenced by such variations and prioritising a focus on common features. Broad representation and the use of consensus-based approaches will be required to ensure the competency framework is applicable across Canada.
Supra-Macro System - Harnessing Insights from Global Events to Determine Influences on Practice
Global influences such as pandemics, and geopolitical issues such as war, and mass immigration exist at the supra-macro level [23]. Although such issues may seem far removed from the microsystem of paramedic practice [94], they can exert significant influence and contribute to the complexity within the system. For example, although paramedics may be some distance from the focal point of the war, an influx of refugee populations to their local area will influence their clinical practice on several levels. The unpredictable nature of war, and the subsequent impact migration may have on practice illustrates the challenge of determining in advance the competencies required of health professionals but highlights the need for improved guidance by which to approach such uncertainty. Our observations at this level suggest the need to explore and attend to emerging concepts, evolving events [38], and societal shifts, and a need to ‘future-proof’ competencies related to these issues, while acknowledging the inability to ‘predict’ future competency needs. This can be mitigated by regular updates and maintenance of the competency framework to ensure it remains contemporary and relevant.
Chronosystem - Reflecting on History to Better Prepare for the Future
The chronosystem refers to the changes, both within the system, and to the dynamic change to the totality of the system over time [23]. Paramedic practice has evolved since 2011 to provide increasingly complex levels of autonomous care in highly variable clinical contexts. In addition, paramedic education has progressed, and service delivery models have evolved across Canada [18]. A broader perspective at this level would suggest that changes have occurred over time in response to changing societal expectations of health and social care and changing public health care policy. Modern day health service perspectives include a move toward increased equity of access to healthcare (resulting in changes to how paramedics deliver care), and reflecting on demographic changes within society and within professions (affecting the clinical workload and the impact on paramedics). Widespread societal influences such as the Truth and Reconciliation Commission’s (TRC) Calls to Action [82], and cultural influences such as the increasing popularity of the internet and social media (which have influenced how paramedics are educated and should behave) must also be acknowledged. Our observations on how the system has changed over time suggest that competency framework development must attend to equity, the impacts of increasing workloads, and the TRC Calls to Action related to health.
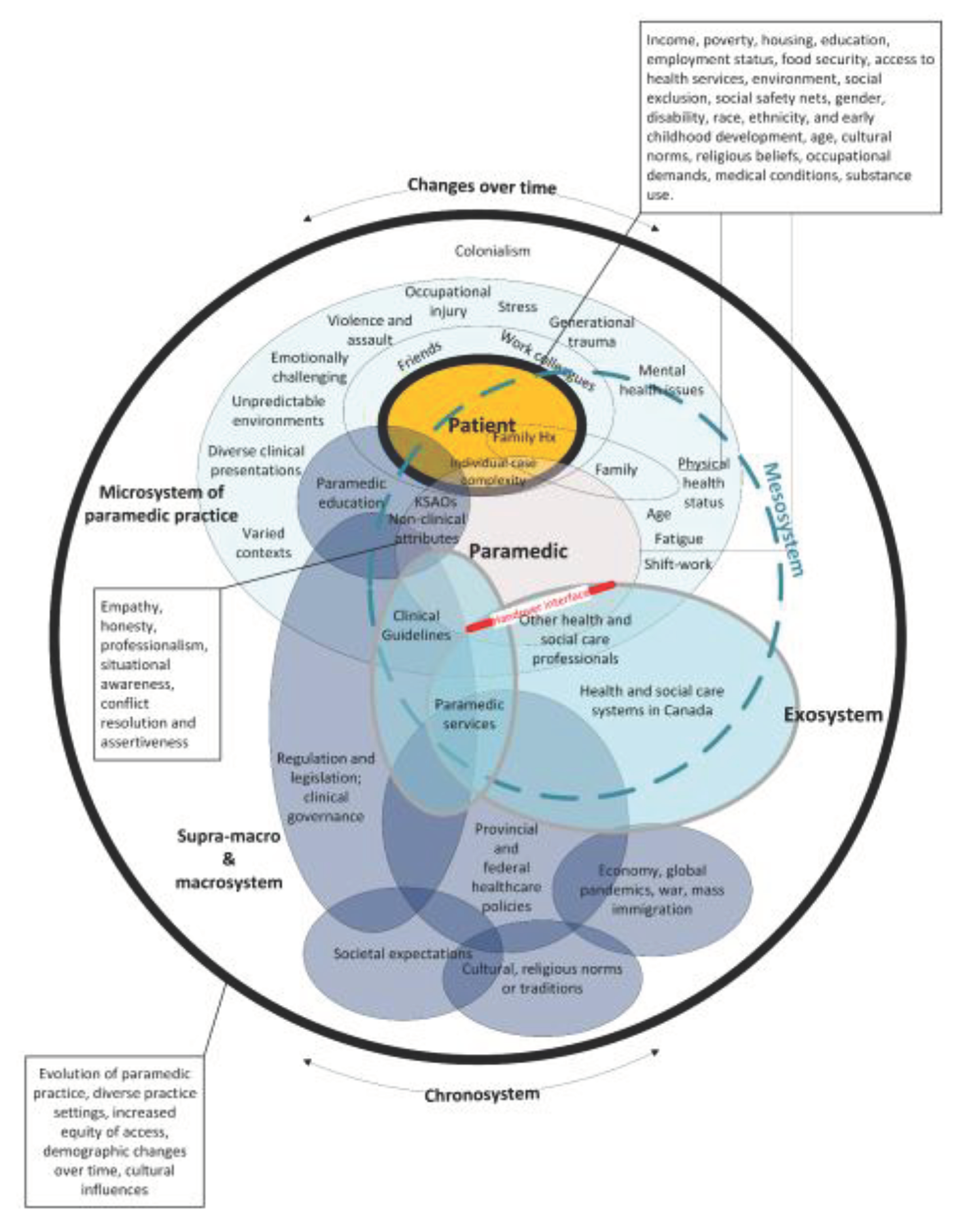
Figure 1.
Systems map of paramedic practice in Canada. This figure illustrates the proposed relationships or interactions between various system levels, and was created via a process of influence mapping, whereby the relationships between various features of the system were identified. This figure places the person receiving care as the central focus of the system of paramedic practice in Canada. There are multiple areas of influence between system levels (and their features). The mesosystem is ‘constructed’ via interactions between the micro-system and the exo-system. The chrono-system represents both changes in system features over time, and the dynamic change to the totality of the system over time. Notes: the size of elements is irrelevant; overlaps do not illustrate significance but rather illustrate influence; the model is a partial representation of paramedic practice in Canada and does not claim to be a validated or complete map of the system.
Figure 1.
Systems map of paramedic practice in Canada. This figure illustrates the proposed relationships or interactions between various system levels, and was created via a process of influence mapping, whereby the relationships between various features of the system were identified. This figure places the person receiving care as the central focus of the system of paramedic practice in Canada. There are multiple areas of influence between system levels (and their features). The mesosystem is ‘constructed’ via interactions between the micro-system and the exo-system. The chrono-system represents both changes in system features over time, and the dynamic change to the totality of the system over time. Notes: the size of elements is irrelevant; overlaps do not illustrate significance but rather illustrate influence; the model is a partial representation of paramedic practice in Canada and does not claim to be a validated or complete map of the system.
Discussion
Competency frameworks play an integral role in reflecting and shaping the practices of the health professions they are intended to represent. They provide a structured way for the profession, public, educators and accreditors, regulators, and policy makers, to guide strategies and ways forward, assuming they are trustworthy in their representation of practice and the profession. Using recently developed guidance that provides a conceptual map for investigation, we examined paramedicine comprehensively such that findings could inform future paramedic competency framework development. In summary, we identified several interacting layers and influences centered around patients, as well as their unique communities, social and environmental contexts. Bringing these influences and insights together requires a structured approach and a coordinated team to consider these insights in more detail, and how best to capture and translate them for inclusion when developing the NCFP. This attempt to better reflect paramedic practice used a recently published systems-thinking approach to identify the features of professional practice [23]. This led to influences that had previously been ignored. From this experience, we offer three critical reflections on implementing such an approach.
First, we enacted a systems thinking approach within a six-step competency framework development model [24]. The steps of this model include (1) identifying purpose, intended uses, scope, and stakeholders; (2) theoretically informed ways of identifying the contexts of complex, “real-world” professional practice, which includes (3) aligned methods and means by which practice can be explored; (4) the identification and specification of competencies required for professional practice, (5) how to report the process and outputs of identifying such competencies, and (6) built-in strategies to continuously evaluate, update and maintain competency framework development processes and outputs. Identifying the features and elements of the system of paramedic practice is part of Step 2 of this model and addressed in this study. However, our systems thinking approach was influenced by decisions made during Step 1 of the six-step model. For example, the scope of the competency framework (e.g., to not include Emergency Medical Responders) placed some natural boundaries on the ‘scope’ of the system, and the elements that required identification (e.g., the NCFP did not address leadership competencies). On reflection, we considered the boundaries placed by Step 1 of the NCFP development process overall to be beneficial in that they helped to shape the structure of the system that we needed to understand. While such boundaries may be helpful in focusing a systems thinking approach, they also represent a risk in failing to identify elements that are considered ‘out of scope’. Developers should remain aware of these implications when choosing to develop competency frameworks using either or both guiding models.
Second, the need to consider geographical, discipline-specific, societal, social, and cultural boundaries is a challenging request of any process. It is inevitable that we missed some features of the system with our approach, and yet also likely that we included too many other features to make the model useful or precise. We created a model of paramedic practice, and as with all models, it is a partial representation that is socially constructed. However, we made concerted efforts to mitigate the impacts of ‘missing features’ including broadly engaging with literature in paramedicine and health systems, recruiting a development group with diverse identities and experiences, and engaging a systematic approach to consider each system level. In doing so, we also had to mitigate accounting for everything in the system resulting in an unusable model. We did this by guidance from the scope of the overall project and keeping our focus on paramedic practice through intimate involvement of those in practice. We suggest developers of competency frameworks pay particular attention to engaging a group of experts from within and outside of the profession, select the members of the group to provide a diversity of intersecting positions and experiences, and involve them in enacting the process of identifying (and subsequently exploring) the features of the system.
Finally, given the national scope of the NCFP it was deemed necessary to consider the macro and supra-macro systems in our understanding of the system of paramedic practice. Given the dynamic nature of systems at this scale, we revisited our understanding of the system as events unfolded to ensure we had attended to any novel considerations. Examples of such events included civil unrest in Canada related to COVID-19 vaccine mandates [95], the need to protect the reproductive rights of women given developments in the USA [96], ongoing economic and financial pressures [97], wildfires across the country [98], and the outbreak of conflict in Ukraine [99]. These and other events had implications for all health professions’ practice including the safety and wellbeing of professionals, cultural competency expectations, awareness of health and social system access, and the importance of social and structural determinants of health. The need to revisit and iterate an understanding of the system should be considered from the outset. How best to translate these events for the purpose of a competency framework remains a challenge but worthy of pursuit. A process by which to systematically undertake this ongoing element would be beneficial and should be considered by those developing competency frameworks.
Translating and Transforming These Findings
The collection of these findings will require the work of translation and transformation into a competency framework. This is an iterative process guided by various factors, influences, and their interactions identified in this study. This process is expected to navigate and resolve issues of messiness, comprehensiveness, and of potential feasibility and utility. However, we expect that this future competency framework development work will be strengthened by the comprehensive foundation presented here.
Conclusion
Paramedic practice in Canada continues to evolve and there is a duty to ensure that documents that guide education, assessment, regulation, and professional development reflect the evolving complexity of contemporary paramedic practice, and outline the features required for competent practice in diverse contexts across Canada. In this study, leveraging a conceptual framework informed by systems thinking, we identified the diverse contexts, presentations, and populations in which paramedic practice is enacted in Canada. These findings suggest that this broad information and contexts be considered and integrated when attempts are made to describe or represent paramedic practice through competency frameworks. Not doing so presents a risk to our understanding of professional practice and ultimately the validity and utility of proposed frameworks. In doing so, we may realise that paramedic practice comprises interdependent health and social care aspects. This in turn suggests that as a profession we have an opportunity through a robust competency framework to better align education with practice, to prepare learners for their professional roles, to align with system advances, and to improve service delivery models to meet the needs of the communities they serve.
Author Contributions
Conceptualization: **; Methodology: **. Formal analysis: **. Data Curation: **. Writing - Original Draft: **. Writing - Review & Editing: **. Visualization: **. Project administration: **. Funding acquisition: **.
Funding
This project was funded by the Paramedic Association of Canada (PAC) and the CSA Group.
Data availability
Data are available from the corresponding author on reasonable request.
Acknowledgments
We wish to gratefully acknowledge the inputs of **, **, **, and **.
Conflicts of Interest
** is a former faculty member and research associate at **. He has received funding from CSA Group and PAC for multiple projects. ** were remunerated for their time on this project through **. ** is a faculty member at **. ** and ** are employed by **.
References
- Duffy, J.; Jones, P.; McNaughton, C.D.; Ling, V.; Matelski, J.; Hsia, R.Y.; Landon, B.E.; Cram, P. Emergency Department Utilization, Admissions, and Revisits in the United States (New York), Canada (Ontario), and New Zealand: A Retrospective Cross-Sectional Analysis. Academic Emergency Medicine 2023, 30, 946–954. [Google Scholar] [CrossRef] [PubMed]
- Acker, J.J.; Johnston, T.M.; Lazarsfeld-Jensen, A. Industrial Paramedics, out on Site but Not out of Mind. Rural Remote Health 2014, 14, 2856. [Google Scholar] [CrossRef] [PubMed]
- Tien, H. How Air Ambulance Services Can Improve Care Delivered to Remote Indigenous Communities. Air Medical Journal 2018, 37, 294–295. [Google Scholar] [CrossRef]
- Besserer, F.; Banner-Lukaris, D.; Tallon, J.; Kandola, D. MP44: Implementing Rural Advanced Care Community Paramedics in Rural and Remote British Columbia: A Qualitative Research Approach. Canadian Journal of Emergency Medicine 2020, 22, S58–S58. [Google Scholar] [CrossRef]
- Keenan, A.; Sadri, P.; Marzanek, F.; Pirrie, M.; Angeles, R.; Agarwal, G. Adapting the Community Paramedicine at Clinic (CP@clinic) Program to a Remote Northern First Nation Community: A Qualitative Study of Community Members’ and Local Health Care Providers’ Views. International Journal of Circumpolar Health 2023, 82, 2258025. [Google Scholar] [CrossRef] [PubMed]
- Orkin, A.; Vanderburgh, D.; Born, K.; Webster, M.; Strickland, S.; Beardy, J. Where There Is No Paramedic: The Sachigo Lake Wilderness Emergency Response Education Initiative. PLoS medicine 2012, 9, e1001322. [Google Scholar] [CrossRef] [PubMed]
- Ruest, M.; Stitchman, A.; Day, C. Evaluating the Impact on 911 Calls by an In-Home Programme with a Multidisciplinary Team. International Paramedic Practice 2012, 2, 41–48. [Google Scholar] [CrossRef]
- Leyenaar, M. Report on the Status of Community Paramedicine in Ontario; Ontario Community Paramedicine Secretariat, 2019.
- Agarwal, G.; Angeles, R.N.; McDonough, B.; McLeod, B.; Marzanek, F.; Pirrie, M.; Dolovich, L. Development of a Community Health and Wellness Pilot in a Subsidised Seniors’ Apartment Building in Hamilton, Ontario: Community Health Awareness Program Delivered by Emergency Medical Services (CHAP-EMS). BMC Research Notes 2015, 8, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Brydges, M.; Denton, M.; Agarwal, G. The CHAP-EMS Health Promotion Program: A Qualitative Study on Participants’ Views of the Role of Paramedics. BMC health services research 2016, 16, 435–435. [Google Scholar] [CrossRef]
- Goldstein, J.; Jensen, J.L.; Carter, A.J.E.; Travers, A.H.; Rockwood, K. The Epidemiology of Prehospital Emergency Responses for Older Adults in a Provincial EMS System. Canadian Journal of Emergency Medicine 2015, 17, 491–496. [Google Scholar] [CrossRef]
- Allana, A.; Kuluski, K.; Pinto, A.; Tavares, W. The Role of Paramedics in Integrated Models of Care. International Journal of Integrated Care 2022, 22, 145. [Google Scholar] [CrossRef]
- Allana, A.T. , Walter; Pinto, Andrew D; Kuluski, Kerry Designing and Governing Responsive Local Care Systems - Insights from a Scoping Review of Paramedics in Integrated Models of Care. International journal of integrated care 2022, 22, 5. [Google Scholar] [CrossRef] [PubMed]
- Paramedic Association of Canada. National Occupational Competency Profile; Paramedic Association of Canada: Ottawa, 2011. [Google Scholar]
- Donnelly, E.A.; Oehme, K.; Barris, D.; Melvin, R. What Do EMS Professionals Know about Human Trafficking? An Exploratory Study. Journal of Human Trafficking 2019, 5, 325–335. [Google Scholar] [CrossRef]
- Bolster, J.; Armour, R.; O’Toole, M.; Lysko, M.; Batt, A.M. The Role of Paramedics in Substance Use Disorder: A Scoping Review. Canadian Paramedicine 2022, 45. [Google Scholar]
- Ford-Jones, P.C.; Chaufan, C. A Critical Analysis of Debates Around Mental Health Calls in the Prehospital Setting. Inquiry: a journal of medical care organization, provision and financing 2017, 54, 46958017704608. [Google Scholar] [CrossRef]
- Tavares, W.; Allana, A.; Beaune, L.; Weiss, D.; Blanchard, I. Principles to Guide the Future of Paramedicine in Canada. Prehospital Emergency Care 2021, 0, 1–11. [Google Scholar] [CrossRef]
- National Highway Traffic Safety Administration. National EMS Education Standards; National Highway Traffic Safety Administration: Washington DC, 2021. [Google Scholar]
- Australasia, P. Australasian Competency Standards for Paramedics; 2011.
- Health and Care Professions Council Standards of Proficiency – Paramedics; 2014.
- Batt, A.M.; Tavares, W.; Williams, B. The Development of Competency Frameworks in Healthcare Professions: A Scoping Review. Advances in Health Sciences Education 2020, 25, 913–987. [Google Scholar] [CrossRef] [PubMed]
- Batt, A.M.; Williams, B.; Brydges, M.; Leyenaar, M.; Tavares, W. New Ways of Seeing: Supplementing Existing Competency Framework Development Guidelines with Systems Thinking. Advances in Health Sciences Education 2021. [Google Scholar] [CrossRef]
- Batt, A.; Williams, B.; Rich, J.; Tavares, W. A Six-Step Model for Developing Competency Frameworks in the Healthcare Professions. Frontiers in Medicine 2021, 8, 2601. [Google Scholar] [CrossRef]
- Batt, A.M.; Tavares, W.; Horsley, T.; Rich, J.V.; Williams, B. ; CONFERD-HP Collaborators CONFERD-HP: Recommendations for Reporting COmpeteNcy FramEwoRk Development in Health Professions. British Journal of Surgery 2023, 110, 233–241. [Google Scholar] [CrossRef]
- Batt, A.; Poirier, P.; Bank, J.; Bolster, J.; Cameron, C.; Donelon, B.; Dunn, N.; Essington, T.; Johnston, C.W.; Lapierre, R.; et al. Developing the National Occupational Standard for Paramedics in Canada – Update 3. Canadian Paramedicine 2022, 45, 6–8. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, Mass, 1979; ISBN 978-0-674-22456-8. [Google Scholar]
- Complexity and Healthcare: An Introduction; Sweeney, K., Griffiths, F., Eds.; Radcliffe Medical Press: Oxford, 2002; ISBN 1-85775-559-6. [Google Scholar]
- Mingers, J. Systems Thinking, Critical Realism and Philosophy: A Confluence of Ideas; Routledge, 2014; ISBN 978-1-317-68462-6.
- Paramedic Association of Canada. Canadian Paramedic Profile: Paramedic Roles; Paramedic Association of Canada: Ottawa, 2016. [Google Scholar]
- Tavares, W.; Bowles, R.; Donelon, B. Informing a Canadian Paramedic Profile: Framing Concepts, Roles and Crosscutting Themes. BMC Health Serv Res 2016, 16, 477. [Google Scholar] [CrossRef] [PubMed]
- Paramedic Association of Canada. The Canadian Paramedicine Education Guidance Document; Paramedic Association of Canada: Ottawa, 2018. [Google Scholar]
- Tavares, W.; Allana, A.; Weiss, D.; Blanchard, I. Principles and Enabling Factors Guiding Paramedicine in Canada; Paramedic Chiefs of Canada: Ottawa, 2023. [Google Scholar]
- Batt, A.; Hultink, A.; Lanos, C.; Tierney, B.; Grenier, M.; Heffern, J. Advances in Community Paramedicine in Response to COVID-19; CSA Group: Ottawa, 2021. [Google Scholar]
- Cavanagh, N.; Tavares, W.; Taplin, J.; Hall, C.; Weiss, D.; Blanchard, I. A Rapid Review of Pandemic Studies in Paramedicine. Australasian Journal of Paramedicine 2020, 17. [Google Scholar] [CrossRef]
- Bowles, R.R.; van Beet, C.; Anderson, G.S. Four Dimensions of Paramedic Practice in Canada: Defining and Describing the Profession. Australasian Journal of Paramedicine 2017, 14. [Google Scholar] [CrossRef]
- Cavanagh, N.; Blanchard, I.E.; Weiss, D.; Tavares, W. Looking Back to Inform the Future: A Review of Published Paramedicine Research. BMC Health Services Research 2023, 23, 108. [Google Scholar] [CrossRef] [PubMed]
- Bolster, J.; Pithia, P.; Batt, A.M. Emerging Concepts in the Paramedicine Literature to Inform the Revision of a Pan-Canadian Competency Framework for Paramedics: A Restricted Review. Cureus 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Batt, A.M.; Bank, J.; Bolster, J.; Pithia, P. Canadian Paramedic Landscape Review and Standards Roadmap; CSA Group: Toronto, 2023. [Google Scholar]
- Armson, R. Growing Wings on the Way; Triarchy Press, 2011; ISBN 978-1-908009-29-6.
- Bell, S.; Morse, S. How People Use Rich Pictures to Help Them Think and Act. Syst Pract Action Res 2013, 26, 331–348. [Google Scholar] [CrossRef]
- Brandstädter, K.; Harms, U.; Großschedl, J. Assessing System Thinking Through Different Concept-Mapping Practices. International Journal of Science Education 2012, 34, 2147–2170. [Google Scholar] [CrossRef]
- Nelson, E.C.; Batalden, P.B.; Huber, T.P.; Mohr, J.J.; Godfrey, M.M.; Headrick, L.A.; Wasson, J.H. Microsystems in Health Care: Part 1. Learning from High-Performing Front-Line Clinical Units. The Joint Commission Journal on Quality Improvement 2002, 28, 472–493. [Google Scholar] [CrossRef]
- Dainty, K.N.; Seaton, M.B.; Drennan, I.R.; Morrison, L.J. Home Visit-Based Community Paramedicine and Its Potential Role in Improving Patient-Centered Primary Care: A Grounded Theory Study and Framework. Health Services Research 2018, 53, 3455–3470. [Google Scholar] [CrossRef]
- Leyenaar, M.; McLeod, B.; Jones, A.; Brousseau, A.-A.; Mercier, E.; Strum, R.P.; Nolan, M.; Sinha, S.K.; Agarwal, G.; Tavares, W.; et al. Paramedics Assessing Patients with Complex Comorbidities in Community Settings: Results from the CARPE Study. CJEM 2021, 23, 828–836. [Google Scholar] [CrossRef]
- Leyenaar, M.S.; McLeod, B.; Penhearow, S.; Strum, R.; Brydges, M.; Mercier, E.; Brousseau, A.-A.; Besserer, F.; Agarwal, G.; Tavares, W.; et al. What Do Community Paramedics Assess? An Environmental Scan and Content Analysis of Patient Assessment in Community Paramedicine. Canadian Journal of Emergency Medicine 2019, 21, 766–775. [Google Scholar] [CrossRef]
- Second Opinion: An Introduction to Health Sociology, 2nd Canadi.; Germov, J., Hornosty, J., Eds.; Oxford University Press: Don Mills, 2014; ISBN 978-0-19-543198-8. [Google Scholar]
- Lunn, T.; Bolster, J.; Batt, A. Community Paramedicine Supporting Community Needs: A Scoping Review 2024.
- ALLANA, A.; PINTO, A.D. Paramedics Have Untapped Potential to Address Social Determinants of Health in Canada. Healthcare Policy 2021, 16, 67–75. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, M.; Leeuw, S.D.; Lindsay, N.M. Determinants of Indigenous Peoples’ Health: Beyond the Social; Canadian Scholars, 2018; ISBN 978-1-77338-038-4.
- Indigenous Primary Health Council; Ontario Public Health Cultural Competency Guideline for Ontario Public Health Units to Engage Successfully with Aboriginal Communities; Indigenous Primary Health Council, 2018.
- Carter, A.J.E.; Arab, M.; Cameron, C.; Harrison, M.; Pooler, C.; McEwan, I.; Austin, M.; Helmer, J.; Ozel, G.; Heathcote, J.; et al. A National Collaborative to Spread and Scale Paramedics Providing Palliative Care in Canada: Breaking down Silos Is Essential to Success. Progress in Palliative Care 2021, 29, 59–65. [Google Scholar] [CrossRef]
- Clarke, B.J.; Campbell, S.G.; Froese, P.; Mann, K. A Description of a Unique Paramedic Role in a Canadian Emergency Department. International Paramedic Practice 2019, 9, 28–33. [Google Scholar] [CrossRef]
- Coffey, B.; MacPhee, R.; Socha, D.; Fischer, S.L. A Physical Demands Description of Paramedic Work in Canada. International Journal of Industrial Ergonomics 2016, 53, 355–362. [Google Scholar] [CrossRef]
- Nolan, M. The Disparity between Urban, Rural and Remote Paramedic Service in Canada. Canadian Paramedicine 2015, 38, 8–9. [Google Scholar]
- Mausz, J.; Johnston, M.; Donnelly, E.A. The Role of Organizational Culture in Normalizing Paramedic Exposure to Violence. JACPR 2022, 14, 112–122. [Google Scholar] [CrossRef]
- Mausz, J.; Johnston, M.; Arseneau-Bruneau, D.; Batt, A.M.; Donnelly, E.A. Prevalence and Characteristics of Violence against Paramedics in a Single Canadian Site. International Journal of Environmental Research and Public Health 2023, 20, 6644. [Google Scholar] [CrossRef]
- Oliphant, A.; Faulds, C.; Bengall, S.; Nouvet, E. At the Front of the Front-Line: Ontario Paramedics’ Experiences of Occupational Safety, Risk and Communication during the 2020 COVID-19 Pandemic. International Journal of Emergency Services, 2022; ahead-of-print . [Google Scholar] [CrossRef]
- Carleton, R.N.; Afifi, T.O.; Turner, S.; Taillieu, T.; El-Gabalawy, R.; Sareen, J.; Asmundson, G.J.G. Chronic Pain among Public Safety Personnel in Canada. Canadian journal of pain/Revue canadienne de la douleur 2017, 1, 237–246. [Google Scholar] [CrossRef]
- Mausz, J.; Donnelly, E.A.; Moll, S.; Harms, S.; McConnell, M. Role Identity, Dissonance, and Distress among Paramedics. IJERPH 2022, 19, 2115. [Google Scholar] [CrossRef] [PubMed]
- Mausz, J.; Donnelly, E.A.; Moll, S.; Harms, S.; Tavares, W.; McConnell, M. The Relationship between Role Identity and Mental Health among Paramedics. Journal of Workplace Behavioral Health 2022, 37, 31–46. [Google Scholar] [CrossRef]
- Carleton, R.N.; Krakauer, R.; MacPhee, R.S.; Cramm, H.A.; Groll, D.; Afifi, T.O.; Taillieu, T.; Turner, S.; Anderson, G.S.; Ricciardelli, R.; et al. Exposures to Potentially Traumatic Events Among Public Safety Personnel in Canada. Canadian Journal of Behavioural Science 2019, 51, 37–52. [Google Scholar] [CrossRef]
- Smith-MacDonald, L.; Lentz, L.; Malloy, D.; Brémault-Phillips, S.; Carleton, R.N. Meat in a Seat: A Grounded Theory Study Exploring Moral Injury in Canadian Public Safety Communicators, Firefighters, and Paramedics. International journal of environmental research and public health 2021, 18, 12145. [Google Scholar] [CrossRef] [PubMed]
- MacQuarrie, S. Fit for Duty: The Demands of Paramedic Performance. Canadian Paramedicine 2014, 37, 14–15. [Google Scholar]
- Sheridan, S. Review Paramedic Health Status, Fitness and Physical Tasks: A Review of the Literature. Australasian Journal of Paramedicine 2019, 16, 1–7. [Google Scholar] [CrossRef]
- Angehrn, A.; Sapach, M.J.N.T.; Ricciardelli, R.; MacPhee, R.S.; Anderson, G.S.; Carleton, R.N. Sleep Quality and Mental Disorder Symptoms among Canadian Public Safety Personnel. International journal of environmental research and public health 2020, 17, 2708. [Google Scholar] [CrossRef] [PubMed]
- CSA Group. CSA Z1615:22 First responder fatigue risk management system; CSA Group: Toronto, 2022. [Google Scholar]
- Yung, M.; Du, B.; Gruber, J.; Yazdani, A. Developing a Canadian Fatigue Risk Management Standard for First Responders: Defining the Scope. Safety Science 2021, 134, 105044. [Google Scholar] [CrossRef]
- Donnelly, E.A.; Bradford, P.; Davis, M.; Hedges, C.; Socha, D.; Morassutti, P. Fatigue and Safety in Paramedicine. CJEM 2019, 21, 762–765. [Google Scholar] [CrossRef]
- Jensen, J.L.; Croskerry, P.; Travers, A.H. Consensus on Paramedic Clinical Decisions during High-Acuity Emergency Calls: Results of a Canadian Delphi Study. Canadian Journal of Emergency Medicine 2011, 13, 310–318. [Google Scholar] [CrossRef]
- Eby, M. Clinical Decision Making in Paramedicine. PhD Thesis, McMaster University, 2016.
- Sheffield, K.; Verrinder, G. Decision-Making Processes When Paramedics Refer Low Acuity Patients Away from Hospital: A Scoping Review. NA 2016, NA, NA-NA.
- Tavares, W.; Mausz, J. Assessment of Non-Clinical Attributes in Paramedicine Using Multiple Mini-Interviews. Emergency Medicine Journal 2015, 32, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Maunder, E.; Maguire, D. Breaking Bad News: The Need for a Coping Mechanism in Paramedicine. International Paramedic Practice 2017, 7, 3–7. [Google Scholar] [CrossRef]
- Brydges, M.; Spearen, C.; Birze, A.; Tavares, W. A Culture in Transition: Paramedic Experiences with Community Referral Programs. CJEM 2015, 17, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Kim, P.J. Social Determinants of Health Inequities in Indigenous Canadians Through a Life Course Approach to Colonialism and the Residential School System. Health Equity 2019, 3, 378–381. [Google Scholar] [CrossRef] [PubMed]
- Barnabe, C.; Osei-Tutu, K.; Maniate, J.M.; Razack, S.; Wong, B.M.; Thoma, B.; Duchesne, N. Equity, Diversity, Inclusion, and Social Justice in CanMEDS 2025. Canadian Medical Education Journal 2023. [Google Scholar] [CrossRef] [PubMed]
- Downar, J.; Arya, A.; LaLumiere, G.; Bercier, G.; Leduc, S.; Charbonneau, V. Practice Innovations: Rapid Deployment of Palliative Care in Clinical Response Teams to Support Long-Term Care Facilities: The Community Paramedic Perspective. Canadian Paramedicine 2020, 44, 9–13. [Google Scholar]
- Leduc, S.; Cantor, Z.; Kelly, P.; Thiruganasambandamoorthy, V.; Wells, G.; Vaillancourt, C. The Safety and Effectiveness of On-Site Paramedic and Allied Health Treatment Interventions Targeting the Reduction of Emergency Department Visits by Long-Term Care Patients: Systematic Review. Prehospital Emergency Care 2020, 0, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Murray, N.; Palermo, C.; Batt, A.; Bell, K. Does Patient and Public Involvement Influence the Development of Competency Frameworks for the Health Professions? A Systematic Review. Frontiers in Medicine 2022, 9. [Google Scholar] [CrossRef] [PubMed]
- Lepre, B.; Palermo, C.; Mansfield, K.J.; Beck, E.J. Stakeholder Engagement in Competency Framework Development in Health Professions: A Systematic Review. Frontiers in Medicine 2021, 8, 2226. [Google Scholar] [CrossRef]
- Truth and Reconcilliation Commission of Canada Honouring the Truth, Reconciling for the Future: Summary of the Final Report of the Truth and Reconciliation Commission of Canada.; 2015; ISBN 978-1-5147-5190-9.
- Fitzsimon, J.; Gervais, O.; Lanos, C. COVID-19 Assessment and Testing in Rural Communities During the Pandemic: Cross-Sectional Analysis. JMIR Public Health and Surveillance 2022, 8, e30063. [Google Scholar] [CrossRef]
- Agarwal, G.; Angeles, R.; Pirrie, M.; Marzanek, F.; McLeod, B.; Parascandalo, J.; Dolovich, L. Effectiveness of a Community Paramedic-Led Health Assessment and Education Initiative in a Seniors’ Residence Building: The Community Health Assessment Program through Emergency Medical Services (CHAP-EMS). BMC Emerg Med 2016, 17, 8. [Google Scholar] [CrossRef] [PubMed]
- O’Meara, P.; Stirling, C.; Ruest, M.; Martin, A. Community Paramedicine Model of Care: An Observational, Ethnographic Case Study. BMC health services research 2016, 16, 39–39. [Google Scholar] [CrossRef]
- Brittain, M.; Michel, C.; Baranowski, L.; Armour, R.; Helmer, J.; Poll, A. Community Paramedicine in British Columbia: A Virtual Response to COVID-19. Australasian Journal of Paramedicine 2020, 17, 1–3. [Google Scholar] [CrossRef]
- Ferron, R.; Munkley, D.; Agarwal, G.; Cooper, R. The Effect of COVID-19 on Emergency Medical Service Call Volumes and Patient Acuity: A Cross-Sectional Study in Niagara, Ontario. BMC Emergency Medicine 2021, 21, 39. [Google Scholar] [CrossRef]
- Strum, R.P.; Mowbray, F.I.; Worster, A.; Tavares, W.; Leyenaar, M.S.; Correia, R.H.; Costa, A.P. Examining the Association between Paramedic Transport to the Emergency Department and Hospital Admission: A Population-Based Cohort Study. BMC emergency medicine 2021, 21, 117. [Google Scholar] [CrossRef]
- Johnston, T.; Armour, R.; Muinoi, G.; Helmer, J.; Bilton, N. Characteristics and Paramedic Management of Patients Enrolled in a Novel Assess, See, Treat and Refer Palliative Care Clinical Pathway: A Retrospective Descriptive Cohort Study. Paramedicine 2023, 20, 198–205. [Google Scholar] [CrossRef]
- Stirling, C.; O’Meara, P.; Pedler, D.; Tourle, V.; Walker, J. Engaging Rural Communities in Health Care through a Paramedic Expanded Scope of Practice. 9.
- Brydges, M. Fractured: A Study of Intraprofessional Paramedic Dynamics on Professionalization in Ontario, Canada. Thesis, 2022.
- Makrides, T.; Ross, L.; Gosling, C.; Acker, J.; O’Meara, P. Exploring the Structure and Characteristics of the Anglo-American Paramedic System in Developed Countries: A Scoping Review. International Journal of Emergency Services 2021, 11, 248–262. [Google Scholar] [CrossRef]
- Rowland, E.; Brydges, M. Paramedics. In Introduction to the Health Workforce in Canada; Bourgeault, I., Ed.; Canadian Health Workforce Network: Ottawa, 2023. [Google Scholar]
- Pask, S.; Pinto, C.; Bristowe, K.; van Vliet, L.; Nicholson, C.; Evans, C.J.; George, R.; Bailey, K.; Davies, J.M.; Guo, P.; et al. A Framework for Complexity in Palliative Care: A Qualitative Study with Patients, Family Carers and Professionals. Palliative Medicine 2018, 32, 1078–1090. [Google Scholar] [CrossRef]
- Ottawa Paramedics Leaning on Out-of-Town Support as Convoy Protest Continues. Available online: https://ottawa.citynews.ca/2022/02/01/ottawa-paramedics-leaning-on-out-of-town-support-as-convoy-protest-continues-5015469/ (accessed on 4 March 2024).
- Vogel, L.; Duong, D. What the U.S. Overturning Roe v. Wade Means for Canada. CMAJ 2022, 194, E711–E712. [Google Scholar] [CrossRef]
- How Could a Recession Affect Canadians? What You Should Know - National | Globalnews.Ca. Available online: https://globalnews.ca/news/9198519/canada-recession-impact-explained/ (accessed on 4 March 2024).
- News ·, G.B.· C. Canada’s Wildfires: Where They Are, How Much Has Burned and How It’s Changing Air Quality | CBC News. Available online: https://www.cbc.ca/news/canada/canada-fires-map-air-quality-1.6871563 (accessed on 4 March 2024).
- Immigration, R. and C.C. Canada to Welcome Those Fleeing the War in Ukraine. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/news/2022/03/canada-to-welcome-those-fleeing-the-war-in-ukraine.html (accessed on 4 March 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



