
Submitted:
24 March 2024
Posted:
26 March 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
: The objetive of this study was to evaluated the quality of sleep, degree of drowsiness, and stress index of dentistry students during the COVID-19 pandemic. Methods: This study was conducted among dentistry students from two universities, obtaining data at baseline and 10 months after the pandemic. The Pittsburgh questionnaire, Epworth sleepiness scale, and Cohen perceived stress scale were used to assess sleep quality, sleepiness index, and stress level, respectively. Statistical analyses were performed using Generalized Estimating Equations, with binary, ordinal, and linear logistic regression. Results: Baseline sleep quality had a positive influence on sleep quality compared with the assessment after 10 months. Drowsiness is influenced by factors, such as the time of assessment, income of up to one salary, and physical activity. There was greater drowsiness 10 months after the pandemic. High stress levels were observed during both assessments. Female sex, deteriorated family relationships, and lack of physical activity increase the risk of stress. Conclusion: The quality of sleep was positively affected during the pandemic period, remaining high, and drowsiness increased.
Keywords:
sleep
; drowsiness
; stress
; COVID-19
1. Introduction
The pandemic decree issued by the World Health Organization (WHO) and the recommendation to practice social isolation to control the spread of the new coronavirus strain, SARS-CoV-2, were unforeseen external shocks for healthcare teaching institutions and has significantly affected the routines of students around the world.
In Brazil, most public educational institutions initially opted to suspend their activities completely. Conversely, private institutions implemented diverse and dynamically modified policies to ensure the viability of their academic activities. Therefore, their classrooms became virtual [1,2].
The challenge was even greater for undergraduate courses in health, in which contact with patients and laboratory practices are common forms of teaching and learning, which are unfeasible in remote teaching. Given that before the pandemic, health courses were already known to cause stress and poor sleep quality [3,4,5], the question was raised about how these students would fair biopsychosocially during the isolation period.
High levels of stress and deficiencies in sleep quality often lead to compromised body homeostasis, which can result in mental and dietary imbalances, decreased cognition, and even suicide [6,7,8].
Therefore, the objective of this study was to evaluate the quality of sleep, degree of drowsiness, and stress index during the COVID-19 pandemic, to gain deeper understanding of the physical and emotional well-being of students during this period. It is important to develop strategies that effectively support preventive measures for unexpected and adverse situations such as COVID-19, particularly to foster healthier academic routines. We hypothesized that there would be no change in sleep quality, drowsiness, or stress levels during the COVID-19 pandemic.
2. Materials and Methods
2.1. Study Design
This study was approved by the Research Ethics Committee of the Universidade Ceuma (No. 3,893,922) and conducted in accordance with the principles of the Declaration of Helsinki. This was a longitudinal study in which participants were evaluated in two stages: the first in April 2020 (baseline) and the second in February 2021, following the reporting guidelines of Observational Studies in Epidemiology [9].
A sample was selected consisting of dentistry students from a private university in São Luís, Maranhão, Brazil (UPR), and from a public university in Uberlândia, Minas Gerais, Brazil (UPU).
At the baseline of the UPR group, 136 students who were in remote classes participated. In the second assessment, 96 students participated, who, in that period, were in hybrid activity (remote theoretical classes and in-person clinical/laboratory practical activities).
At the baseline of the UPU group, which had a total interruption of activities for 5 months, 283 students participated. In the second evaluation, 256 students who were in remote activities participated.
2.2. Inclusion and Exclusion Criteria
Dentistry students who accepted the invitation to participate in the study, who were enrolled at the participating universities were included. Those who completed their degrees before the second stage of the study were excluded.
2.3. Sampling
Convenience sampling was used, and the students were invited to participate with an explanatory and motivational video about the research to be conducted. To participate, volunteers joined a WhatsApp® group created for the research. A link to the Google Forms survey was sent to potential research participants. The form contained an informed consent form, granting access to sociodemographic, sleep quality, drowsiness, and stress questionnaires. The link remained open for 48 h.
2.4. Sociodemographic Data
Participants answered questions related to their sociodemographic profiles, including age, gender, marital status, family income, and type of residence. In addition, they answered questions related to their social life (what they missed most and whether they engaged in physical activity), family life (who they lived with, the number of people in their household, and their relationships with these individuals), and academic life. In the second stage, four questions were added that addressed the impact of COVID-19 on family and professional lives.
2.5. Assessment of Sleep and Drowsiness
We used Pittsburgh sleep quality index [10] in association with the Brazilian version of the Epworth sleepiness scale [11]. Sleep quality was considered poor when the sum of the seven components evaluated (quality, latency, duration, efficiency, disturbance, medication use, and daytime dysfunction) was greater than five, indicating poor sleep quality in two components or moderate difficulty in more than three components. If the result was less than five, the sleep was considered of good quality.
The Epworth Drowsiness Assessment Questionnaire contains eight questions about everyday situations in which the individual feels like dozing or sleeping, with a maximum score of 24 points. Values of up to 10 indicate little drowsiness, while values greater than 10 indicates excessive drowsiness, and greater than 16 indicates severe drowsiness.
2.6. Stress Assessment
The full version of Cohen's Perceived Stress Scale [12], consisting of 14 questions, was used. The response scores ranged from 0 to 4 (0= never; 1= almost never; 2= sometimes; 3= almost always; and 4= always). However, for questions 4, 5, 6, 7, 9, 10, and 13, their scores were inverted because of their positive connotation (4= never, 3= almost never, 2= sometimes, 1= almost always, and 0= always). The total score ranges from 0 to 56 and the higher the score, the higher the stress level.
2.6. Statistical Analysis
After calculating the absolute and relative frequencies of the responses to each question for the UPU and UPR groups, a chi-square test was used to assess whether there was a significant difference between the participants from the two universities for each question in the questionnaire. In cases where the chi-square test was not applicable, the Fisher's exact test was used.
Generalized Estimating Equations (GEE) were used to examine the impact of whether university, gender, family income, relationship with household members, daily activities, and engagement in physical activity on sleep quality, degree of drowsiness, and stress during the research period. Analysis options included binary logistic regression, ordinal logistic regression, and linear regression.
All analyses were performed using the IBM SPSS Statistics for Windows software, v.26 (IBM Corp, Armonk, NY, USA) with a significance level of 5%.
3. Results
A total of 419 and 352 participants were selected according to the eligibility criteria at baseline and after 10 months, respectively (Figure 1).
Table 1 shows the absolute and relative frequencies of responses for each sociodemographic variable according to the groups, together with the p-values resulting from the chi-square or Fisher 's exact test.
The only independent variable that influenced sleep quality was the moment of assessment (ExpB =0.627; 95%CI=0.480-0.819), indicating that the baseline had a positive influence on sleep (Exp 0.627; 95%CI=0.480-0.819 ) (Table 2).
The type of university, relationships with the household members, and routine did not influence the degree of drowsiness (p>0.05). However, gender (p=0.009), assessment time (p<0.001), family income (p=0.017), and physical activity (p=0.027) were associated with degree of drowsiness (Table 3). Additionally, females were more likely to experience severe drowsiness (ExpB =1.736, 95%CI=1.149-2.622). The frequency of “little drowsiness” was more at baseline than in the second assessment (ExpB = 0.579; 95% CI=0.454-0.737). Low family income of up to one minimum wage, was associated with severe sleepiness (ExpB = 3.266; 95% CI=1.241-8.594). Additionally, lack of physical activity was found to contribute to higher rates of severe sleepiness (ExpB =1.411; 95% CI=1.039 -1.917).
The female gender (ExpB =38.264; IC 95%=6.357-230.304), the relationship with household members (ExpB =1233; CI 95%=17.872-85116.035) and the lack of physical activity (ExpB =7.800; CI 95 %=1.786-34.077) influenced the degree of stress (Table 4).
4. Discussion
Unexpected events can trigger biopsychosocial imbalances, which manifest in varied ways and intensities, depending on the vulnerability of the affected groups.
In this study, participants were predominantly young, single, without children, and primarily professional students, with a family income exceeding one minimum wage. Throughout the first and second assessments during the pandemic, they continued to reside with their parents, maintaining an unchanged family dynamic.
These findings suggest that the socioeconomic and familial circumstances of the participants were privileged, since during that period, a substantial portion of Brazilian society faced emotional support deficits and precarious economic conditions, such as food insecurity and reliance on financial assistance from government or third-party sources [13,14]. Despite this apparent shielding, the participants showed a high level of stress at baseline, and the proposed hypothesis was rejected because of the influence of the pandemic on all variables.
Stress is expected in student groups, especially in the health aspect, irrespective of the pandemic, as they are young adults navigating the transition from high school to university or from education to professional life, facing the academic and social pressures inherent in working directly with human life [7,15,16,17,18,19,20]. However, at baseline, activity was suspended in the UPU and reduced in the UPR. Therefore, it is inferred that this high percentage of stress was caused not only by the changes imposed by COVID-19 in the social and academic routines of students but also by the fear instilled by the spread of the disease, which resulted in fatalities worldwide [21,22,23].
It is important to note that even after 10 months, stress levels remained high. Therefore, the passage of time did not sufficiently alleviate the impact of COVID-19. This persistence is attributed to the ongoing disruption in the students' social and academic routines, exacerbated by fears of the disease perpetuated by emerging variants. Furthermore, apprehension about the job market persisted amid the economic recession in Brazil and globally [6,13,23].
Although the literature indicates that sleep is altered in situations of high stress [8,22,23,24,25], this relationship was only observed at baseline in this study. During this period, despite students being outside of their academic routines and having more flexibility to adhere to their natural sleep patterns, it did not lead to an improvement in sleep quality. Several surveys conducted with university students during the pandemic revealed that while sleep duration had increased, sleep quality was low owing to emotional instability [8,21,22,26,27,28,29]. In a group of students at the University of Toronto, there was an observed increase in the frequency of stressful dreams and nightmares, with 40% reporting dreams specifically related to the pandemic [30].
In addition to stress, the students' sleep patterns were significantly influenced even after 10 months. Despite the initial impact of the pandemic subsiding and social restrictions easing, their sleep quality worsened over time. [7,16,22,29,31,32].
Pre-pandemic research has demonstrated that university/education-related pressures, social life, and the abusive use of technology are the main factors contributing to jet leg, and, consequently, poor sleep quality and drowsiness. However, during the pandemic, only screen time was increased [28,33,34].
A study conducted with medical students in Greece in the second year of the pandemic revealed data that were partially divergent from this research. Sleep quality was poor, stress levels were high, and 16% of the sample revealed suicidal ideation. Considering that vaccines were not yet been released in Greece and that the second wave of the disease was beginning, these facts may have contributed to the results [32],
Drowsiness, which is generally linked to poor sleep quality [29,35], presented lower rates at baseline in this study, despite sleep during this period being considered of poor quality. Apparently, this was owing to a possible increase in sleep duration, as confirmed by several studies conducted during the pandemic [15,21,26,27]. Another factor that must have contributed was the elimination of the time spent commuting [15,17,27,35], as activities at the UPR were online, and at the UPU, there was absence of activity. However, after 10 months, an increase in drowsiness was observed. This result is believed to be due to greater academic demand, which led to a decrease in the freedom of time to plan breaks.
When correlating the variables—physical activity, income, interpersonal relationships, sex, and university—with sleep, drowsiness, and stress, it was observed that sleep was the only factor that was not influenced by these variables. However, this has not always been reported in the literature, where a relationship with some of these factors has generally been found [25,36,37]. It seems plausible to infer that this relationship was not established because of the sociodemographic and economic characteristics of the participants and their confinement [16,29,31].
Drowsiness was influenced by family income, physical activity, and sex, the latter two of which also influenced stress. Severe drowsiness has been observed among students with low family incomes. Economic restrictions lead to greater participation in domestic activities, reducing the chances of a more adequate environmental structure, and limiting the practice of physical activity. These factors may have contributed to the increased drowsiness. In a study in Germany, it was observed that support programs for students with a low family income, which facilitated participation in physical activity, reduced the degree of drowsiness [38].
Frequent physical activity is considered one of the pillars of a healthy life and an effective strategy to help reduce negative emotions, as it contributes to the production of serotonin. Serotonin, also known as the feel-good hormone, is a vital neurotransmitter for emotional regulation, hunger, sleep, and pain; therefore, it is an important factor for better quality sleep, less daytime drowsiness, balanced diet, and lower stress [25,39,40]. This explains why this study observed a relationship between students who did not practice physical activity and higher rates of severe drowsiness, as well as higher stress scores.
In most studies involving stress, the female sex is the most affected. In this study, there was no significant difference, and a greater association with severe drowsiness was observed. Several studies have associated this with women's greater sensitivity to external factors, greater concern for their family, and increased domestic obligations during the COVID-19 pandemic. Hormonal factors, especially estrogen, are increasingly being highlighted. Studies have shown that an increase in cortisol levels as a result of a prolonged period of stress can cause a decrease in estrogen and serotonin levels. This can result in sleep problems and can affect mood, leaving women more depressed and vulnerable [6,18,23,30,41,42,43].
Family relationships and university-related pressures were found to influence only the stress variable. Students who reported worse relationships with the people with whom they lived had higher levels of stress. Social confinement causes a series of psychological changes, with the family being the most effective means of social interaction. An emotionally and economically balanced family is of utmost importance in reducing young adults’ vulnerability [22,39,40].
The influence of university type on stress is believed to stem from differing educational policies implemented across the groups. It was observed that UPR students, who had been attending remote classes since the baseline, mostly reported being able to maintain their study routine at an average level at both time points evaluated. Despite having a high level of stress, this index was significantly lower than the rate for UPU students. At baseline, the vast majority said that they were unable to maintain their study routine, and after 10 months (already in remote teaching), this percentage was reduced by half, which generated a significant difference between the two time points evaluated for this group.
In a study conducted with medical students from nine countries (Chile, Colombia, Brazil, Venezuela, Mexico, Italy, Spain, Germany, and Japan), those without any academic activities reported the highest level of dissatisfaction, which subsequently impacted both their physical and mental well-being [44]. In another study, remote teaching was associated with learning deficits and stressful workloads that began to generate anxiety and depressive symptoms [45]. However, it is necessary to consider that the research was conducted at the beginning of the pandemic, a period of greater restrictions in the country, including curfews. Furthermore, the difficulty in accessing the Internet was constant.
Having an academic activity during a period of isolation was reported as important for emotional control and reducing stress, in addition to maintaining “social-virtual” contact with teachers and colleagues [46,47,48,49]. Based on the previous discussions, it is believed that a lack of academic activity contributed to increased stress. This inference is more credible when considering that the students, despite being in different geographic regions, were socioeconomically similar, and both groups were located outside the COVID-19 epicenter.
5. Conclusions
The COVID-19 pandemic has affected sleep, drowsiness, and stress levels in dental students. The confinement period enhanced sleep quality while also leading to higher levels of drowsiness and stress.
Author Contributions
Conceptualization, A.S.M. and R.R.J.T.; methodology, A.S.M., N.E.N. and N.A.B.R.; formal analysis, E.M.M.F. and M.C.F..; investigation, P.C.S.J.; P.P.A. and D.B.D.; writing—original draft preparation, A.S.M. writing—review & editing, R.R.J.T. and M.C.F.; administration: A.S.M. and R.R.J.T.; and All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
he study was conducted according to the guidelines of the Declaration of Helsinki and approved by the ethics committee of the Ceuma Universit (approval nymber: No. 3,893,922).
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Castioni R, Melo AAS de, Nascimento PM, Ramos DL. Federal universities in the Covid-19 pandemic: student access to the internet and 12 emergency remote teaching Essay: avalpolpúblEduc [Internet]. 2021Apr;29(111):399–419. [CrossRef]
- Cavalcanti LMR, Guerra M das GGV. The challenges of public universities post-Covid-19 pandemic: the Brazilian case. Essay: avalpolpúblEduc [Internet]. 2022Jan;30(114):73–93. [CrossRef]
- Çelik N, Ceylan B, Ünsal A, Çağan Ö. Depression in health college students: relationship factors and sleep quality. Psychol Health Med. 2019Jun;24(5):625-630. [CrossRef]
- Pacheco JP, Giacomin HT, Tam WW, Ribeiro TB, Arab C, Bezerra IM, Pinasco GC.Mental health problems among medical students in Brazil: a systematic review and meta-analysis. Braz J Psychiatry. 2017 Oct Dec;39(4):369-378. [CrossRef]
- Basudan S, Binanzan N, Alhassan A. Depression, anxiety and stress in dental students. Int J Med Educ. 2017 May 24;8:179-186. [CrossRef]
- 6. León-Manco RA, Agudelo -Suárez AA, Armas -Vega A, Figueiredo MC, Verdugo- PaivaF , Santana-Pérez Y, Viteri -García A. Perceived Stress in Dentists and Dental Students of Latin America and the Caribbean during the Mandatory Social Isolation Measures for the COVID-19 Pandemic: A Cross-Sectional Study. Int J Environ Res Public Health. 2021 May 30;18(11):5889. [CrossRef]
- Wright KP Jr, Linton SK, Withrow D, Casiraghi L, Lanza SM, Iglesia H, Vetter C, Depner CM. Sleep in university students prior to and during COVID-19 Stay-at-Home orders. Curr Biol. 2020 Jul 20;30(14):R797-R798. [CrossRef]
- Du C, Adjepong M, Zan MCH, Cho MJ, Fenton JI, Hsiao PY, Keaver L, Lee H, LudyMJ, Shen W, Swee WCS, Thrivikraman J, Amoah-Agyei F, de Kanter E, Wang W, TuckerRM. Gender Differences in the Relationships between Perceived Stress, Eating Behaviors, Sleep, Dietary Risk, and Body Mass Index. Nutrients. 2022 Feb28;14(5):1045. [CrossRef]
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP;STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. Int J Surg. 2014 Dec;12(12):1495-9. [CrossRef]
- Bertolazi AN, Fagondes SC, Hoff LS, Dartora EG, Miozzo IC, de Barba ME, Barreto SS. Validation of the Brazilian Portuguese version of the Pittsburgh Sleep Quality Index. Sleep Med. 2011 Jan;12(1):70-5. [CrossRef]
- Bertolazi AN, Fagondes SC, Hoff LS, Pedro VD, Menna Barreto SS, Johns MW.Portuguese -language version of the Epworth sleepiness scale: validation for use in Brazil. J Bras Pneumol. 2009 Sep;35(9):877-83. English, Portuguese. [CrossRef]
- Luft CD, Sanches Sde O, Mazo GZ, Andrade A. Brazilian version of the Perceived Stress Scale: translation and validation for the elderly [ Brazilian version of the Perceived Stress Scale : translation and validation for the elderly ]. rev Public health. 2007 Aug;41(4):606-15. Portuguese. [CrossRef]
- Sott MK, Bender MS, da Silva Baum K. Covid-19 Outbreak in Brazil: Health, Social, Political, and Economic Implications. Int J Health Serv. 2022Oct;52(4):442-454. [CrossRef]
- Rodrigues EC, Mendonça RD, Camargo PP, Menezes MC, Carvalho NC, Meireles AL. Home food insecurity during the suspension of classes in Brazilian public schools due to the COVID-19 pandemic. Nutrition. 2022 Jan;93:111448. Erratum in: Nutrition. 2022 Mar;95:111563. [CrossRef]
- Ramos Socarras L, Potvin J, Forest G. COVID-19 and sleep patterns in adolescents and young adults. Sleep Med. 2021 Jul;83:26 -33. [CrossRef]
- Smit AN, Juda M, Livingstone A, U SR, Mistlberger RE. Impact of COVID-19 social-distancing on sleep timing and duration during a university semester. PloS One. 2021 Apr 26;16(4):e 0250793. [CrossRef]
- Benham G. Stress and sleep in college students prior to and during the COVID-19 pandemic. Stress Health. 2021 Aug;37(3):504-515. [CrossRef]
- Alyoubi A, Halstead EJ, Zambelli Z, Dimitriou D. The Impact of the COVID-19 Pandemic on Students' Mental Health and Sleep in Saudi Arabia. Int J Environ Res Public Health. 2021 Sep 4;18(17):9344. [CrossRef]
- Henning K, Ey S, Shaw D. Perfectionism, the imposter phenomenon and psychological adjustment in medical, dental, nursing and pharmacy students. MedEduc. 1998 Sep;32(5):456-64. [CrossRef]
- 20. Basudan S, Binanzan N, Alhassan A. Depression, anxiety and stress in dental students. Int J Med Educ. 2017 May 24;8:179-186. [CrossRef]
- Marelli S, Castelnuovo A, Somma A, Castronovo V, Mombelli S, Bottoni D,Leitner C, Fossati A, Ferini-Strambi L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J Neurol. 2021Jan;268(1):8-15. [CrossRef]
- Gusman MS, Grimm KJ, Cohen AB, Doane LD. Stress and sleep across the onset of the novel coronavirus disease 2019 pandemic: impact of distance learning on US college students' health trajectories. Sleep. 2021 Dec 10;44(12 ):zsab 193. [CrossRef]
- Pelucio L, Simões P, Dourado MCN, Quagliato LA, Nardi AE. Depression and anxiety among online learning students during the COVID-19 pandemic: a cross-sectional survey in Rio de Janeiro, Brazil. BMC Psychol. 2022 Aug 3;10(1):192. [CrossRef]
- Alqahtani JS, AlRabeeah SM, Aldhahir AM, Siraj R, Aldabayan YS, Alghamdi SM,Alqahtani AS, Alsaif SS, Naser AY, Alwafi H. Sleep Quality, Insomnia, Anxiety, Fatigue, Stress, Memory and Active Coping during the COVID-19 Pandemic. Int J Environ Res Public Health. 2022 Apr 19;19(9):4940. [CrossRef]
- Ghrouz AK, Noohu MM, Dilshad Manzar M, Warren Spence D, Ba Hammam AS, Pandi -Perumal SR. Physical activity and sleep quality in relation to mental health among college students. Sleep Breath. 2019 Jun;23(2):627-634. [CrossRef]
- Du C, Zan MCH, Cho MJ, Fenton JI, Hsiao PY, Hsiao R, Keaver L, Lai CC, Lee H, Ludy MJ, Shen W, Swee WCS, Thrivikraman J, Tseng KW, Tseng WC, Doak S, Folk SYL,Tucker RM. The Effects of Sleep Quality and Resilience on Perceived Stress, Dietary Behaviors, and Alcohol Misuse: A Mediation-Moderation Analysis of Higher Education Students from Asia, Europe, and North America during the COVID-19Pandemic. Nutrients. 2021 Jan 29;13(2):442. [CrossRef]
- Kumar N, Gupta R. Disrupted Sleep During a Pandemic. Sleep Med Clin. 2022Mar;17(1):41-52. [CrossRef]
- Lu P, Yang L, Wang C, Xia G, Xiang H, Chen G, Jiang N, Ye T, Pang Y, Sun H, Yan L, Su Z, Heyworth J, Huxley R, Fisher J, Li S, Guo Y. Mental health of new undergraduate students before and after COVID-19 in China. Sci Rep. 2021 Sep22;11(1):18783. [CrossRef]
- Neculicioiu VS, Colosi IA, Costache C, Sevastre-Berghian A, Clichici S. Time to Sleep?- A Review of the Impact of the COVID-19 Pandemic on Sleep and MentalHealth. Int J Environ Res Public Health. 2022 Mar 16;19(6):3497. [CrossRef]
- Kilius E, Abbas NH, McKinnon L, Samson DR. Pandemic Nightmares: COVID-19Lockdown Associated With Increased Aggression in Female University Students'Dreams. Front Psychol. 2021 Mar 5;12:644636. [CrossRef]
- Genta FD, Rodrigues Neto GB, Sunfeld JPV, Porto JF, Xavier AD, Moreno CRC, Lorenzi -Filho G, Genta PR. COVID-19 pandemic impact on sleep habits, chronotype, and health-related quality of life among high school students: a longitudinal study. J Clin Sleep Med 2021 Jul 1;17(7):1371-1377. [CrossRef]
- Eleftheriou A, Rokou A, Arvaniti A, Nena E, Steiropoulos P. Sleep Quality and Mental Health of Medical Students in Greece During the COVID-19 Pandemic. FrontPublic Health. 2021 Nov 19;9:775374. [CrossRef]
- Paiva T, Reis C, Feliciano A, Canas-Simião H, Machado MA, Gaspar T, Tomé G, Branquinho C, Silva MR, Ramiro L, Gaspar S, Bentes C, Sampaio F, Pinho L, Pereira C, Carreiro A, Moreira S, Luzeiro I, Pimentel J, Videira G, Fonseca J, Bernarda A, Vaz Castro J, Rebocho S, Almondes K, Canhão H, Matos MG. Sleep and Awakening Quality during COVID-19 Confinement: Complexity and Relevance for Health and Behavior. Int J Environ Res Public Health. 2021 Mar 28;18(7 ):3506. [CrossRef]
- Viselli L, Salfi F, D'Atri A, Amicucci G, Ferrara M. Sleep Quality, Insomnia Symptoms, and Depressive Symptomatology among Italian University Students before and during the Covid-19 Lockdown. Int J Environ Res Public Health. 2021 Dec18;18(24):13346. [CrossRef]
- Stone JE, Phillips AJK, Chachos E, Hand AJ, Lu S, Carskadon MA, Klerman EB, Lockley SW, Wiley JF, Bei B, Rajaratnam SMW; CLASS Study Team. In-person vs home schooling during the COVID-19 pandemic: Differences in sleep, circadian timing, and mood in early adolescence. J Pineal Res. 2021 Sep;71(2 ):e 12757. [CrossRef]
- Galindo- Aldana GM, Padilla-López LA, Torres-González C, García-León IA, Padilla -Bautista JA, Alvarez- Núñez DN. Effects of Socio-Familial Behavior on Sleep Quality Predictive Risk Factors in Individuals under Social Isolation. Int J Environ Res Public Health. 2022 Mar 20;19(6):3702. [CrossRef]
- Saguem BN, Nakhli J, Romdhane I, Nasr SB. Predictors of sleep quality in medical students during COVID-19 confinement. Encephale. 2022 Feb;48(1 ):3-12. [CrossRef]
- Blume M, Rattay P. Association between Physical Activity and Sleep Difficulties among Adolescents in Germany: The Role of Socioeconomic Status. Int J Environ Res Public Health. 2021 Sep 14;18(18):9664. [CrossRef]
- Markofski MM, Jennings K, Hodgman CF, Warren VE, LaVoy EC. Physical activity during the SARS-CoV-2 pandemic is linked to improved mood and emotion. Stress Health. 2022 Aug;38(3):490-499. [CrossRef]
- Muradyan A, Macheiner T, Mardiyan M, Sekoyan E, Sargsyan K. The Evaluation of Biomarkers of Physical Activity on Stress Resistance and Wellness. Appl Psychophysiol Biofeedback. 2022 Jun;47(2):121-129. [CrossRef]
- Albert KM, Newhouse PA. Estrogen, Stress, and Depression: Cognitive and Biological Interactions. Annu Rev Clin Psychol. 2019 May 7;15:399-423. [CrossRef]
- Sikka N, Juneja R, Kumar V, Bala S. Effect of Dental Environmental Stressors and Coping Mechanisms on Perceived Stress in Postgraduate Dental Students. Int J Clin Pediatr Dent. 2021 Sep-Oct;14(5):681-688. [CrossRef]
- Rijal D, Paudel K, Adhikari TB, Bhurtyal A. Stress and coping strategies among higher secondary and undergraduate students during COVID-19 pandemic in Nepal. PLOS Glob Public Health. 2023 Feb 15;3(2 ):e 0001533. [CrossRef]
- Michaeli D, Keough G, Perez-Dominguez F, Polanco- Ilabaca F, Pinto-Toledo F, Michaeli J, Albers S, Achiardi J, Santana V, Urnelli C, Sawaguchi Y, RodríguezP, Maldonado M, Raffeeq Z, de Araujo Madeiros O, Michaeli T. Medical education and mental health during COVID-19: a survey across 9 countries. Int J Med Educ.2022 Feb 26;13:35 -46. [CrossRef]
- Fawaz M, Samaha A. E-learning: Depression, anxiety, and stress symptomatology among Lebanese university students during COVID-19 quarantine. Nurs Forum. 2021Jan;56(1):52-57. [CrossRef]
- Dpereira MB, Casagrande AV, Almeida BC, Neves BA, da Silva TCRP, Miskulin FPC, Perissotto T, Ribeiz SRI, Nunes PV. Mental Health of Medical Students Before and During COVID-19 Pandemic: a 3-Year Prospective Study. Med Sci Educ. 2022 Jun29;32(4):873-881. [CrossRef]
- David MCMM, Vieira GR, Leôncio LML, Neves LDS, Bezerra CG, Mattos MSB, Santos NFD, Santana FH, Antunes RB, Araújo JF, Matos RJB. Predictors of stress in college students during the COVID-19 pandemic. J Affect Disord Rep. 2022 Dec;10:100377. [CrossRef]
- Raccanello D, Balbontín -Alvarado R, Bezerra DDS, Burro R, Cheraghi M, Dobrowolska B, Fagbamigbe AF, Faris ME, França T, González-Fernández B, Hall R, Inasius F, Kar SK, Keržič D, Lazányi K, Lazăr F, Machin- Mastromatteo JD, MarôcoJ, Marques BP, Mejía-Rodríguez O, Méndez Prado SM, Mishra A, Mollica C, NavarroJiménez SG, Obadić A, Mamun-Ur-Rashid M, Ravšelj D, Tatalović Vorkapić S,Tomaževič N, Uleanya C, Umek L, Vicentini G, Yorulmaz Ö, Zamfir AM, AristovnikA. Higher education students' achievement emotions and their antecedents in e-learning amid COVID-19 pandemic: A multi-country survey. Learn Instr. 2022 Aug;80:101629. [CrossRef]
- Camargo CP, Tempski PZ, Busnardo FF, Martins MA, Gemperli R. Online learning and COVID-19: a meta-synthesis analysis. Clinics (Sao Paulo). 2020 Nov6;75:e2286. [CrossRef]
Figure 1.
Flowchart of the different phases of the study.
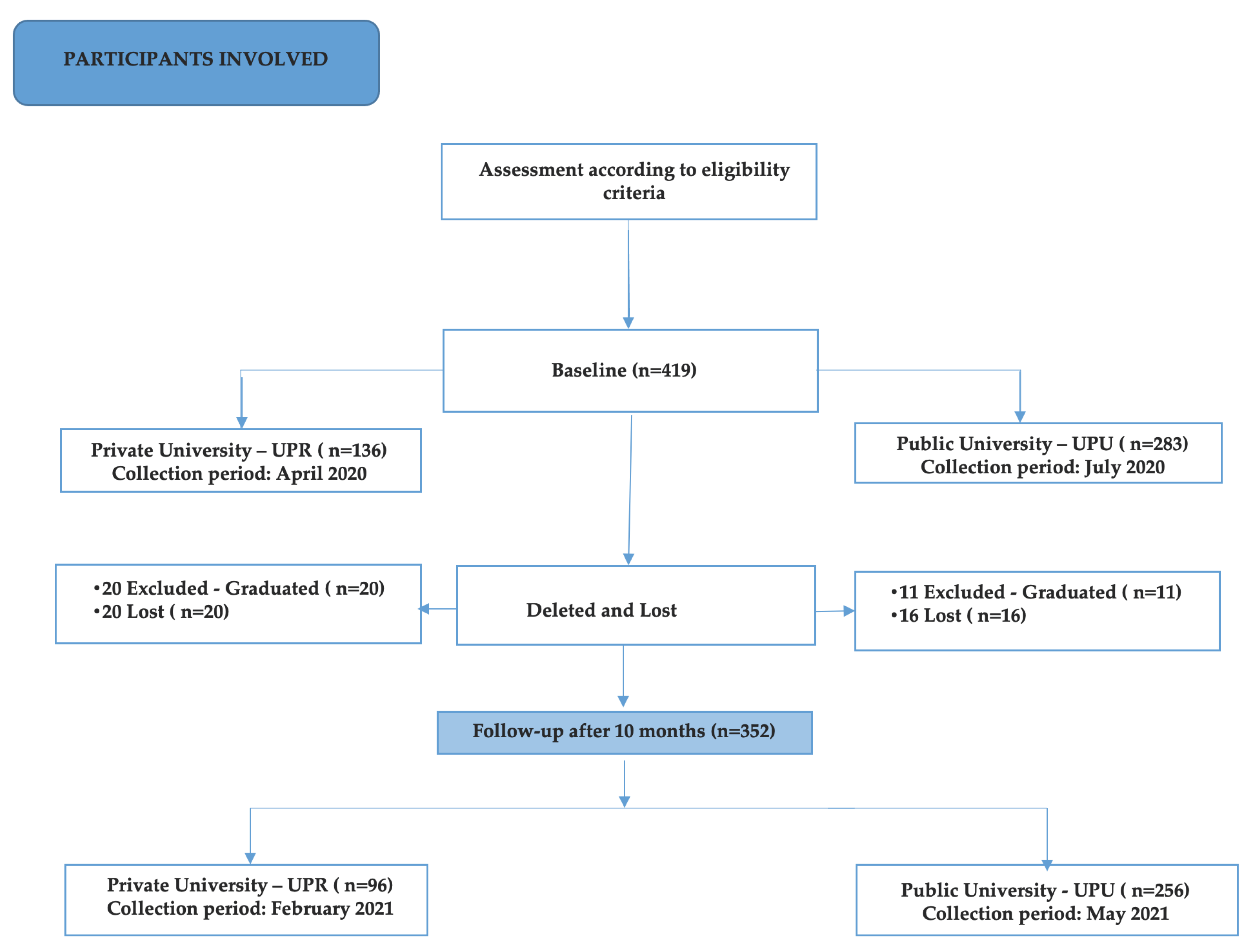

Table 1.
Absolute and relative frequencies of sociodemographic data responses and the influence of COVID-19 on students’ family and professional lives.
Table 1.
Absolute and relative frequencies of sociodemographic data responses and the influence of COVID-19 on students’ family and professional lives.
| UPU (%) | UPR (%) | P | ||
|---|---|---|---|---|
| Gender | Feminine | 208 (73.5) | 101 (74.3) | 0.867 |
| Masculine | 75 (26.5) | 35 (25.7) | ||
| Race | Mixed race or brown | 75 (26.5) | 61(44.9) | <0.001 |
| White | 183 (64.7) | 60 (44.1) | ||
| Black | 21 (7.4) | 11 (8.1) | ||
| Yellow | 4 (1.4) | 4 (2.9) | ||
| marital status | Single | 279 (98.6) | 126 (92.6) | 0.006 |
| Married | 2 (0.7) | 6 (4.4) | ||
| Unity stable | 2 (0.7) | 4 (2.9) | ||
| Family income | up to 1 salary | 14 (4.9) | 7 (5.1) | 0.907 |
| +from 1 to 3 salaries | 91 (32.2) | 49 (36.0) | ||
| + from 3 to 5 salaries | 91 (32.2) | 39 (28.7) | ||
| + from 5 to 15 salaries | 73 (25.8) | 33 (24.3) | ||
| + 15 salaries | 14 (4.9) | 8 (5.9) | ||
| Lives with | Spouse | 15 (5.3) | 1 (0.7) | 0.229 |
| Parents / sibling | 242 (85.5) | 123 (90.4) | ||
| Relatives | 17 (6.0) | 9 (6.6) | ||
| Friends | 3 (1.1) | 1 (0.7) | ||
| Alone | 6 (2.1) | 2 (1.5) | ||
| Number of children | No he has son | 283 100.0) | 128 (94.1) | <0.001 |
| 1 | 0 (0.0) | 6 (4.4) | ||
| 2 | 0 (0.0) | 1 (0.7) | ||
| 3 or more | 0 (0.0) | 1 (0.7) | ||
| Improved a little | 51 (19.9) | 19 (19.8) | 0.009 | |
| Improved very much | 29 (11.3) | 13 (13.5) | ||
| The relationship with the | It got a little worse | 43 (16.8) | 8 (8.3) | |
| people who live with | It got very worse | 8 (3.1) | 1 (1.0) | |
| you: | Stays the same | 118 (46.1) | 44 (45.8) | |
| I live alone | 7 (2.7) | 11 (11.5) | ||
| Comparing the beginning of the Pandemic with the current moment, please select the option that best represents you current health status | 1. I don't worry as much as I used to | 6 (2.3) | 3 (3.1) | 0.103 |
| 2. I worry more about my family than about myself | 155 (60.5) | 46 (47.9) | ||
| 3. I worry about myself and my family | 95 (37.1) | 47 (49.0) | ||
| Considering the Pandemic situation, select the option that best represents you professionally | 1. I worry a little because I will soon be part of the job market | 94 (36.7) | 53 (55.2) | <0.001 |
| 2. I have no concerns about this at the moment | 41 (16.0) | 4 (4.2) | ||
| 3. I have great concerns because the recession is big | 121 (47.3) | 39 (40.6) | ||
| Had COVID | Yes | 55 (21.5) | 27 (28.1) | <0.001 |
| No | 173 (67.6) | 43 (44.8) | ||
| Perhaps | 28 (10.9) | 26 (27.1) | ||
| I lost a family member or | Yes | 110 (43.0) | 49 (51.0) | 0.175 |
| friend | No | 146 (57.0) | 47 (49.0) |
Table 2.
Generalized Estimating Equations with the option of binary logistic regression, to assess the impact of university, gender, family income, relationship with household members, the daily routine and engagement in physical activity on quality of sleep over time.
Table 2.
Generalized Estimating Equations with the option of binary logistic regression, to assess the impact of university, gender, family income, relationship with household members, the daily routine and engagement in physical activity on quality of sleep over time.
| Parameter | Exp(B) | 95%CI | P | ||
|---|---|---|---|---|---|
| University | UPR | 1,137 | 0.776 | 1,666 | 0.510 |
| UPU | 1 | . | . | . | |
| Gender | F | 1,064 | 0.726 | 1,560 | 0.750 |
| M | 1 | . | . | . | |
| Assessment moment _ | Baseline | 0.627 | 0.480 | 0.819 | 0.001 |
| 10 months | 1 | . | . | . | |
| Income | up to 1 salary | 3,229 | 0.966 | 10,799 | 0.057 |
| 1 to 3 salaries | 1,079 | 0.560 | 2,079 | 0.820 | |
| 3 to 5 salaries | 1,085 | 0.554 | 2,126 | 0.812 | |
| 5 to 15 salaries | 0.876 | 0.447 | 1,718 | 0.700 | |
| + 15 salaries | 1 | . | . | . | |
| Relationship with household members | I live alone | 1,179 | 0.388 | 3,581 | 0.771 |
| It got worse very | 2,292 | 0.809 | 6,496 | 0.119 | |
| It got a little worse | 1,665 | 0.881 | 3,145 | 0.116 | |
| Stays the same | 0.890 | 0.538 | 1,473 | 0.650 | |
| Improved a little | 0.738 | 0.407 | 1,338 | 0.317 | |
| Very improved | 1 | . | . | . | |
| Routine | Only study | .667 | 0.405 | 1,096 | 0.110 |
| Study and others activities | 1 | . | . | . | |
| Physical activity | No | 1,303 | 0.955 | 1,778 | 0.095 |
| Yes | 1 | . | . | . | |
Table 3.
Generalized Estimating Equations with the option of ordinal logistic regression, to assess the impact of university, gender, family income, relationship with household members, the daily routine and engagement in physical activity on the degree of drowsiness over time.
Table 3.
Generalized Estimating Equations with the option of ordinal logistic regression, to assess the impact of university, gender, family income, relationship with household members, the daily routine and engagement in physical activity on the degree of drowsiness over time.
| Parameter | Exp(B) | 95%CI | P | ||
|---|---|---|---|---|---|
| University | UPR | 0.881 | 0.612 | 1,269 | 0.496 |
| UPU | 1 | . | . | . | |
| Gender | F | 1,736 | 1,149 | 2,622 | 0.009 |
| M | 1 | . | . | . | |
| Assessment moment | Baseline | 0.579 | 0.454 | 0.737 | <0.001 |
| 10 months | 1 | . | . | . | |
| Income | up to 1 salary | 3,266 | 1,241 | 8,594 | 0.017 |
| 1 to 3 salaries | 1,355 | 0.661 | 2,777 | 0.407 | |
| 3 to 5 salaries | 1,487 | 0.719 | 3,075 | 0.285 | |
| 5 to 15 salaries | 0.894 | 0.429 | 1,860 | 0.764 | |
| + 15 salaries | 1 | . | . | . | |
| Relationship with household members | I live alone | 1,352 | 0.547 | 3,340 | 0.514 |
| It got very worse | 1,529 | 0.610 | 3,829 | 0.365 | |
| It got a little worse | 0.928 | 0.512 | 1,682 | 0.806 | |
| Stays the same | 0.710 | 0.435 | 1,160 | 0.171 | |
| Improved a little | 0.818 | 0.467 | 1,436 | 0.485 | |
| Improved very | 1 | . | . | . | |
| Routine | Only study | .787 | 0.493 | 1,257 | 0.317 |
| Study and others activities | 1 | . | . | . | |
| Activity physical | No | 1,411 | 1,039 | 1,917 | 0.027 |
| Yes | 1 | . | . | . | |
Table 4.
Generalized Estimating Equations with the linear regression option, to assess the impact of university, gender, family income, relationship with household members, daily routine and engagement in physical activity on the degree of stress over time.
Table 4.
Generalized Estimating Equations with the linear regression option, to assess the impact of university, gender, family income, relationship with household members, daily routine and engagement in physical activity on the degree of stress over time.
| Parameter | Exp(B) | 95% CI | P | ||
|---|---|---|---|---|---|
| University | UPR | 0.093 | 0.013 | 0.680 | 0.019 |
| UPU | 1 | . | . | . | |
| Gender | F | 38,264 | 6,357 | 230,304 | 0.001 |
| M | 1 | . | . | . | |
| Assessment moment | Baseline | 1,535 | 0.483 | 4,879 | 0.468 |
| 10 months | 1 | . | . | . | |
| Income | up to 1 salary | 2,413 | 0.055 | 106,059 | 0.648 |
| 1 to 3 salaries | 5,200 | 0.392 | 68,971 | 0.211 | |
| 3 to 5 salaries | 4,833 | 0.364 | 64,087 | 0.232 | |
| 5 to 15 salaries | 2,982 | 0.237 | 37,582 | 0.398 | |
| + 15 salaries | 1 | . | . | . | |
| Relationship with household members | I live alone | 2,390 | 0.020 | 290,518 | 0.722 |
| It got very worse | 1233.357 | 17,872 | 85116.035 | 0.001 | |
| It got a little worse | 26,878 | 1,714 | 421,372 | 0.019 | |
| Stays the same | 0.986 | 0.114 | 8,552 | 0.990 | |
| Improved a little | 1,141 | 0.091 | 14,249 | 0.919 | |
| Improved very | 1 | . | . | . | |
| Routine | Only study | 0.200 | 0.020 | 1,984 | 0.169 |
| Study and others activities | 1 | . | . | . | |
| Activity physical | No | 7,800 | 1,786 | 34,077 | 0.006 |
| Yes | 1 | . | . | . | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



