
Submitted:
27 March 2024
Posted:
28 March 2024
You are already at the latest version
Abstract
Scedosporium species are human pathogenic fungi, responsible for chronic, localised, and life-threatening disseminated infections in both immunocompetent and immunocompromised individuals. Diagnosis of Scedosporium infections currently relies on non-specific CT, lengthy and insensitive culture from invasive biopsy, and time-consuming histopathology of tissue samples. At present, there are no rapid antigen tests that detect Scedosporium-specific biomarkers. Here we report the development of a rapid (30 min) and sensitive (pmol/L sensitivity) lateral-flow device (LFD) test, incorporating a Scedosporium-specific IgG1 monoclonal antibody (mAb), HG12, which binds to extracellular polysaccharide (EPS) antigens of between ~15 kDa and 250 kDa secreted during hyphal growth of the pathogens. The test is compatible with human serum, and allows the detection of the Scedosporium species most-frequently reported as agents of human disease (Scedosporium apiospermum, Scedosporium aurantiacum, and Scedosporium boydii), with limits of detection (LOD) of the EPS biomarkers in human serum of ~0.81 ng/mL (S. apiospermum), ~0.94 ng/mL (S. aurantiacum), and ~1.95 ng/mL (S. boydii). The Scedosporium-specific LFD (ScedLFD) test therefore provides a potential novel opportunity for the detection of infections caused by different Scedosporium species.
Keywords:
Scedosporium
; scedosporiosis
; monoclonal antibody
; biomarker
; lateral-flow device
; enzyme-linked immunosorbent assay
1. Introduction
Scedosporium species are human pathogenic moulds. They are the agents of eumycetoma [1,2,3,4,5], a chronic deep fungal infection of the skin and subcutaneous tissues, and are responsible for a broad spectrum of localised and life-threatening disseminated infections in immunocompetent and immunocompromised individuals [6,7,8,9,10] affecting numerous organs of the body (Figure 1A), including the bones and joints [11,12,13], the central nervous system [14,15,16,17], the eyes [18,19,20,21,22,23,24], the lungs [14,25,26,27,28,29,30,31,32,33], the sinuses [34,35,36], and other body sites [37,38,39] of cystic fibrosis patients [8,28,40,41,42], hematopoietic stem-cell and solid organ transplant recipients [31,43,44,45,46,47], hospitalised patients with COVID-19 [48], victims of near-drowning following natural disasters [14,15,30,49,50], and in persons with traumatic injuries [51,52,53,54,55]. Recently assigned to the high (eumycetoma-causative agents) and moderate priority pathogen groupings by the World Health Organisation [56], Scedosporium diseases have an overall all-cause mortality rate of 42-46% [56].
The Scedosporium species most commonly associated with life-threatening infections are S. apiospermum, S. aurantiacum, and S. boydii [8,57,58,59,60,61]. Detection of these pathogens relies on a combination of techniques including histological examination and in situ hybridisation of tissue samples [62], isolation of the fungi from biopsy samples using semi-selective or selective media and microscopical examination of cultures for characteristic morphological features [58,63], with species identification requiring matrix-assisted laser desorption/ ionisation-time-of-flight mass spectrometry (MALDI-TOF MS) [64] or molecular methods such as polymerase chain reaction [58,63]. While immunoassays that employ patient sera have been developed for the detection of Scedosporium and Lomentospora species in cystic fibrosis patients [65,66], there is no rapid antigen test currently available for the specific detection of Scedosporium species [63].
Here we report the development of a lateral-flow device (ScedLFD) for the rapid (30 min) and sensitive (pmol/L) detection of a Scedosporium-specific biomarker. The immunoassay employs a Scedosporium-specific monoclonal antibody (mAb, HG12) which binds to extracellular polysaccharide (EPS) antigens present on the spore and hyphal cell wall of these fungi [67], and which is secreted during hyphal growth. The ScedLFD test is compatible with human serum, with limits of detection of EPS antigens in serum of ~0.81 ng/mL (S. apiospermum), ~0.94 ng/mL (S. aurantiacum), and ~1.95 ng/mL (S. boydii). The LFD therefore provides a novel opportunity for the rapid, sensitive and specific detection of these human pathogenic fungi.
2. Materials and Methods
2.1. Monoclonal Antibody
The mouse monoclonal antibody (mAb) HG12 [67] is an immunoglobulin G1 (IgG1) -light chain antibody, and is specific to species in the Scedosporium apiospermum complex (Scedosporium angustum, Scedosporium apiospermum, Scedosporium boydii, Scedosporium ellipsoideum, and Scedosporium fusoideum), Scedosporium aurantiacum, Scedosporium desertorum, and Scedosporium minutisporum. The mAb also recognizes the related fungi Parascedosporium tectonae, Petriellopsis africana, Lophotrichus fimeti, Graphium eumorphum (the Graphium type of S. apiospermum), and the teleomorph form of Graphium, Petriella setifera. The mAb does not react with Scedosporium dehoogii or with unrelated molds and yeasts of clinical importance including Lomentospora prolificans (formerly Scedosporium prolificans).
2.2. Fungal Culture
Fungi (Table 1) were routinely cultured on oatmeal agar (OA; P2182, Sigma) or malt extract agar (MEA; 70145, Sigma). Media were autoclaved at 121 oC for 15 min prior to use, and fungi were grown at 37 oC. Extracellular polysaccharides (EPS) were purified from 6-d-old culture filtrates of fungi grown at 30 oC in YNB+G liquid medium as described previously [68]. For ScedLFD and ScedELISA specificity tests, 72-h-old YNB+G culture filtrates of fungi [69] were used.
2.3. Antibody Purification and Enzyme Conjugation
Hybridoma tissue culture supernatant of mAb HG12 was harvested by centrifugation at 2,147 x g for 40 min at 4 °C, followed by filtration through a 0.8 μM cellulose acetate filter (10462240, GE Healthcare Life Sciences, UK). Culture supernatant was loaded onto a HiTrap Protein A column (17-0402-01, GE Healthcare Life Sciences) using a peristaltic pump P-1 (18-1110-91, GE Healthcare Life Sciences) with a low pulsation flow of 1 mL/min. Columns were equilibrated with 10 mL of phosphate-buffered saline (PBS; PBS; 137 mM NaCl, 2.7 mM KCl, 8 mM Na2HPO4, 1.5 mM KH2PO4 [pH 7.2]), and column-bound antibody was eluted with 5 mL of 0.1 M glycine-HCl buffer (pH 2.5) with a flow rate of 0.5 mL/min. The buffer of the purified antibody was exchanged to PBS using a disposable PD-10 desalting column (17-0851-01, GE Healthcare Life Sciences). Following purification, the antibody was sterile filtered with a 0.24 µm syringe filter (85037-574-44, Sartorius) and stored at 4 °C. Antibody purity was confirmed by SDS-PAGE and gel staining using Coomassie Brilliant Blue R-250 dye (Thermo Fisher Scientific). Protein A-purified mAb HG12 was conjugated to horseradish peroxidase (HRP) for ELISA studies using a Lightning-Link horseradish peroxidase conjugation kit (701-0000; Bio-Techne Ltd.), or to alkaline phosphatase (AKP) for western blotting studies using a Lightning-Link alkaline phosphatase conjugation kit (702-0010; Bio-Techne Ltd.).
2.4. Polyacrylamide Gel Electrophoresis and Western Blotting
Sodium-dodecyl-sulphate-polyacrylamide gel electrophoresis (SDS-PAGE) was carried out using 4–20% gradient polyacrylamide gels (161-1159, Bio-Rad) under denaturing conditions. Antigens were separated electrophoretically at 165 V and pre-stained markers (161-0318, Bio-Rad) were used for molecular weight determinations. For western blotting, separated antigens were transferred electrophoretically onto a PVDF membrane (162-0175, Bio-Rad) for 2 h at 75 V, and the membrane was blocked for 16 h at 4 °C in PBS containing 1% (wt:vol) BSA. Blocked membranes were incubated with HG12-AKP conjugate diluted 1:15,000 (vol:vol) in PBS containing 0.5% (wt/vol) BSA (PBSA) for 2 h at 23 °C. Membranes were washed three times with PBS, once with PBST and bound antibody visualised by incubation in substrate solution. Reactions were stopped by immersing membranes in dH2O, and membranes were then air dried between sheets of Whatman filter paper.
2.5. LFD and ELISA Specificities
2.5.1. Lateral-Flow Device
The Scedosporium lateral-flow device (ScedLFD) was manufactured by Lateral Dx (Alloa, Scotland, UK). The test consists of a Sartorius CN95 nitrocellulose (NC) membrane laminated with an absorbent pad, sample pad, and LDX-treated polyester conjugate pad containing 2.5 L of Protein A-purified mAb HG12 conjugated to RE1 red cellulose nanobeads (Asahi Kasei). The NC test (T) line consists of Protein A-purified mAb HG12 at a concentration of 2 mg/mL, while the internal test control (C) line consists of goat anti-mouse IgG (Arista Biologicals) at a concentration of 1 mg/mL. For specificity tests, 72-h-old culture filtrate was mixed 1:10 (vol:vol) with LFD running buffer (RB; PBS containing 0.1% (v/v) Tween-20), and 100 mL of the resultant solution added to the LFD test. The negative control for ScedLFD tests consisted of YNB+G medium only diluted 1:10 (vol:vol) with RB. After 30 min, the intensities of the test (T) and control (C) lines were determined as artificial units (a.u.) using a Cube reader [68,69].
2.5.2. Sandwich Enzyme-Linked Immunosorbent Assay
For the Scedosporium sandwich ELISA (ScedELISA), wells of Maxisorp microtiter plates (Nunc) were coated with 50 µL volumes of Protein A-purified mAb HG12 at a concentration of 3 mg/mL PBS. After incubation for 16 h at 4 oC, the wells were washed three times (5 min each wash) with PBST (PBS containing 0.05% (vol:vol) Tween-20), once with PBS for 5 min, and then given a final rinse with dH2O before air-drying at 23 oC. Antibody-coated wells were incubated at 23 oC for 1 h with 50 µL of 72-h-old culture filtrates diluted 1:10 (vol:vol) with PBST (control wells incubated with YNB+G medium only diluted 1:10 (vol:vol) with PBST), after which they were given four 5-min washes with PBST. Washed wells were then incubated for 1 h at 23 oC with HG12-HRP conjugate diluted 1 in 5000 (v/v) in PBST, after which they were washed four times with PBST as described, given a final 5-min wash with PBS, and bound antibody visualised by incubating wells with tetramethyl benzidine (TMB) substrate solution for 30 min. Enzyme-substrate reactions were stopped by the addition of 3 M H2SO4, and absorbance values were determined at 450 nm using a microplate reader (infinite F50, Tecan Austria GmbH). All incubation steps were performed at 23 °C in sealed plastic bags.
2.6. Serological Detection and Limits of Detection
Normal serum from healthy AB blood group males (H6914, Sigma) was spiked with purified EPS from S. apiospermum isolate CBS8353, S. aurantiacum isolate CBS121926, and S. boydii isolate CBS835.96, and stored as aliquots at -20 oC prior to use. The standard operating procedure (SOP) for serum pre-treatment and testing using the ScedLFD test is illustrated in Figure 1B. On thawing of serum, 50 L spiked or control (unspiked) serum was mixed 1:2 (vol:vol) with PBS containing 0.5% (wt:vol) Na2-EDTA (pH6.0), and heated in a boiling water bath for 3 min. The heated mixture was centrifuged at 16,000 x g for 5 min, the clear supernatant mixed 1:1 (vol:vol) with LFD RB, and the resultant solution assayed by ScedLFD (100 L per test) as described. For testing by ScedELISA (50 L per well), supernatants were diluted in PBST and assayed as described, but with an antigen incubation step of 2 h.
2.7. Statistical Analysis
Numerical data were analysed using a Student’s t-test (independent, two-tailed) to determine statistical significance.
3. Results
3.1. Lateral-Flow Device and ELISA
3.1.1. Specificities
Using culture filtrates from yeasts and moulds grown for 72 h in YNB+G liquid medium, both the ScedLFD and the ScedELISA were shown to be Scedosporium-specific (Table 1), reacting strongly with filtrates from species in the Scedosporium apiospermum complex (Scedosporium angustum, Scedosporium apiospermum, Scedosporium boydii, Scedosporium ellipsoideum, and Scedosporium fusoideum), and with filtrates from Petriella setifera, Scedosporium aurantiacum, Scedosporium desertorum, and Scedosporium minutisporum. Neither of the immunoassays cross-reacted with filtrates from unrelated yeasts and moulds of clinical importance including Candida albicans, Cryptococcus neoformans, Aspergillus spp., Fusarium spp., Mucorales fungi (species of Apophysomyces, Cunninghamella, Lichtheimia, Mucor, and Rhizopus), and Lomentospora prolificans.
3.1.2. Limits of Detection with Human Serum
Both the ScedLFD and the ScedELISA are compatible with human serum. In western blotting studies of extracellular polysaccharides (EPS) purified from culture filtrates of Scedosporium apiospermum, Scedosporium aurantiacum, and Scedosporium boydii, mAb HG12 reacted strongly with antigens with molecular weights of between ~15 kDa and 250 kDa, but did not cross-react with EPS antigen purified from Aspergillus fumigatus culture filtrate (Figure 2). Using the purified EPS samples, the ScedLFD was shown to have limits of detection of ~0.26 ng/mL running buffer (RB), ~0.24 ng/mL RB, and ~0.98 ng/mL RB for S. aurantiacum (Figure 3A), S. apiospermum (Figure 3C), and S. boydii (Figure 3E), respectively. In serum tests, the ScedLFD showed limits of detection of ~0.94 ng/mL serum, ~0.81 ng/mL serum, and ~1.95 ng/mL serum for S. aurantiacum (Figure 3B), S. apiospermum (Figure 3D), and S. boydii (Figure 3F), respectively. In serum tests, the ScedELISA was less sensitive than the ScedLFD test, with limits of detection of ~62.5 ng/mL serum, ~15.6 ng/mL serum, and ~125 ng/mL serum for S. apiospermum, S. aurantiacum, and S. boydii, respectively (Figure 4).
4. Discussion
In this paper, we describe the development of a lateral-flow device (ScedLFD) test for the rapid detection of Scedosporium species, fungal pathogens responsible for myriad chronic and life-threatening infections of the skin and sub-cutaneous tissues (eumycetoma), bones and joints, central nervous system, sinuses, eyes, and lungs of humans (Figure 1A).
The ScedLFD incorporates a monoclonal antibody (mAb), HG12, previously raised against Scedosporium boydii [67] and which is specific, recognising species in the Scedosporium apiospermum complex (Scedosporium angustum, Scedosporium apiospermum, Scedosporium boydii, Scedosporium ellipsoideum, and Scedosporium fusoideum), and also Scedosporium aurantiacum, Scedosporium desertorum, and Scedosporium minutisporum. In addition, mAb HG12 the recognises Graphium and Petriella states of Scedosporium, also reported as human pathogens [20,37,70]. Importantly, the mAb does not cross-react with unrelated yeasts and moulds of clinical importance including Aspergillus spp., Candida and Cryptococcus spp., Mucorales spp., and species of Fusarium. This high degree of specificity is of critical importance given the occurrence of mixed fungal co-infections in humans [1,19,40,71,72,73,74].
Current detection of infectious Scedosporium species relies on sophisticated laboratory tests, including (MALDI-TOF MS) [64] or molecular methods such as polymerase chain reaction (PCR) [58,63]. While a potential diagnostic antigen (a 50-80 kDa peptidorhamnomannan (PRM)) from Scedosporium boydii has been reported [75], and mAbs raised against Scedosporium apiospermum PRM, their lack of specificity, cross-reacting with Candida spp., Histoplasma capsulatum, and Lomentospora prolificans [76], limits their use in diagnostic test development. Consequently, this is the first time, to the best of our knowledge, that a mAb-based lateral-flow test has been developed for the specific detection of Scedosporium species.
For point-of-care diagnostics employing lateral-flow technology, extracellular antigens are needed that can act as signature molecules of infection [77]. Ideally, these should be produced during active growth of a pathogen, and the target epitope should be heat-stable allowing pre-treatment of biofluids such as serum for biomarker detection [68,69]. The Scedosporium-specific mAb HG12 used in the ScedLFD test binds to a heat-stable extracellular polysaccharide (EPS) antigen present on the spore and hyphal cell wall [67], and which is secreted during hyphal growth of Scedosporium species (this study). It therefore represents an ideal biomarker for the serological detection of these pathogens.
Using a simple and quick serum pre-treatment method (Figure 1B), we have shown that the ScedLFD test is compatible with human serum. As with other sandwich-format LFD tests [78], a negative test result is shown by the presence of the control (C) line only (Figure 1C), while a positive test result is shown by the presence of a test (T) line and the C line (Figure 1D). This gain-of-signal at the T line allows for the simple visual appraisal of test positivity, but can introduce bias due to the subjective nature of test interpretation. To eliminate bias, the presence and intensity of the T line can be established using a Cube reader, with test output recorded as artificial units (a.u.). When combined with a Cube reader, the limits of detection of the ScedLFD for the three most common agents of disease in humans (S. apiospermum, S. aurantiacum, and S. boydii) were shown to be <2 ng EPS/mL serum. This high level of test sensitivity (pmol/L) is consistent with other sandwich LFD tests [79]. We found that the lateral-flow format to be more sensitive than an enzyme-linked immunosorbent assay (ELISA) using the same mAb, HG12. Furthermore, the speed of the ScedLFD test (30 min), compared to the ScedELISA (>3 h), adds to its superiority in terms of speed, sensitivity and ease-of-use, and satisfies the ASSURED criteria for diagnostics for the developing world [80]. The ScedLFD test is therefore ideally suited to resource-limited settings that lack sophisticated diagnostic facilities and equipment needed to run laboratory-based ELISA, MALD-TOF or PCR tests.
The compatibility of the ScedLFD test (and ScedELISA) with serum means it may be suitable for the detection of disseminated Scedosporium infections in humans. It should be noted that the test has yet to be validated in the clinic, but its development using a previously characterised mAb [67] is an important first step towards point-of-care testing for Scedosporium diseases. While serum is an appropriate biofluid for biomarker detection of hematogenous dissemination, other biofluids might serve as better sources of the antigenic EPS biomarkers for rapid detection of sinus, eye, lung and skin infections, as has been postulated for the point-of-care detection of mucormycosis [81]. Notwithstanding this, the availability of a rapid antigen test for a complex of fungi recently assigned to the high (eumycetoma-causative agents) and moderate priority pathogen groupings by the World Health Organisation [56], and its compatibility with a minimally-invasive biofluid (serum), makes the ScedLFD a potentially valuable diagnostic tool for this destructive group of pathogens.
5. Conclusions
We have developed a specific, sensitive and simple lateral-flow immunoassay (ScedLFD) for the rapid detection of human-pathogenic Scedosporium species. The test is compatible with human serum, potentially enabling the accurate and minimally-invasive detection of Scedsoporium species at point-of-care.
Author Contributions
Conceptualisation, CRT and GED; methodology, CRT and GED; investigation, CRT and GED; formal analysis, CRT and GED; resources, CRT; data curation, CRT and GED; writing—original draft preparation, CRT; writing, review and editing, CRT and GED; supervision, CRT; project administration, CRT; funding acquisition, CRT. The authors have read and agreed to the content of the manuscript.
Funding
This work was supported by ISCA Diagnostics Ltd. (project title: ScedLFD–a novel lateral-flow test for Scedosporium).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author, but are not publicly available due to commercial confidentialities. Monoclonal antibody HG12 and the LFD are available through ISCA Diagnostics Ltd.
Conflicts of Interest
CRT is a Director of ISCA Diagnostics Ltd., and GED is an employee of ISCA Diagnostics Ltd. This manuscript does not have any potential conflict of interest with ISCA Diagnostics Ltd.
References
- Gulati, V. , Bakare, S, Tibrewal, S., Ismail, N., Sayani, J., Baghla, D.P.S. A rare presentation of concurrent Scedosporium apiospermum and Madurella grisea eumycetoma in an immunocompetent host. Case Rep. Pathol. 2012, 2012, 154201. [Google Scholar] [PubMed]
- Gupta, M.K., Banerjee, T, Kumar, D., Rastogi, A., Tilak, R. White grain mycetoma caused by Scedosporium apiospermum in north India: as case report. Int. J. Low. Extrem. Wounds. 2013, 12, 286–288.
- Oliveira, F.d.M.; Unis, G.; Hochhegger, B.; Severo, L.C. Scedosporium apiospermum eumycetoma successfully treated with oral voriconazole: report of a case and review of the Brazilian reports on scedosporiosis. Rev. Inst. Med. Trop. Sao Paulo 2013, 55, 121–123. [CrossRef]
- Tóth, E.J.; Nagy, G.R.; Homa, M.; Ábrók, M.; Kiss, I. .; Nagy, G.; Bata-Csörgő, Z.; Kemény, L.; Urbán, E.; Vágvölgyi, C.; et al. Recurrent Scedosporium apiospermum mycetoma successfully treated by surgical excision and terbinafine treatment: a case report and review of the literature. Ann. Clin. Microbiol. Antimicrob. 2017, 16, 31. [Google Scholar] [CrossRef] [PubMed]
- Emery, D.; Denning, D.W. The global distribution of actinomycetoma and eumycetoma. PLOS Neglected Trop. Dis. 2020, 14, e0008397. [Google Scholar] [CrossRef] [PubMed]
- Cortez, K.J., Roilides, E, Quiroz-Telles, F., Meletiadis, J., Antachopoulos, C., Knudsen, T., Buchanan, W., Milanovich, J., Sutton, D.A., Fothergill, A., et al. Infections caused by Scedosporium spp. Clin. Microbiol. Rev. 2008, 21, 157–197.
- Ramirez-Garcia, A.; Pellon, A.; Rementeria, A.; Buldain, I.; Barreto-Bergter, E.; Rollin-Pinheiro, R.; de Meirelles, J.V.; Xisto, M.I.D.S.; Ranque, S.; Havlicek, V.; et al. Scedosporium and Lomentospora: an updated overview of underrated opportunists. Med Mycol. 2018, 56, S102–S125. [Google Scholar] [CrossRef] [PubMed]
- Bouchara, J.-P. , Papon, N. Scedosporium apiospermum. Trends Microbiol. 2019, 27, 12. [Google Scholar]
- Seidel, D. , Meißner, A. , Lackner, M., Piepenbrock, E., Salmanton-García, J., Stecher, M., Mellinghoff, S., Hamprecht, A., Graeff, L.D., Köhler, P., et al. Prognostic factors in 264 adults with invasive Scedosporium spp. and Lomentospora prolificans infection reported in the literature and FungiScope. Crit. Rev. Microbiol. 2019, 45, 1–21. [Google Scholar]
- Bronnimann, D.; Garcia-Hermoso, D.; Dromer, F.; Lanternier, F.; Maulin, L.; Leprince, Y.; Brieu, N.; Gruson, B.; El-Samad, Y.; Chouaki, T.; et al. Scedosporiosis/lomentosporiosis observational study (SOS): Clinical significance of Scedosporium species identification. Med Mycol. 2020, 59, 486–497. [Google Scholar] [CrossRef]
- Koehler, P. , Tacke, D. , Cornely, O.A. Bone and joint infections by Mucorales, Scedosporium, Fusarium and even rarer fungi. Crit. Rev. Microbiol. 2016, 42, 158–171. [Google Scholar]
- Mello, T.P.; Bittencourt, V.C.B.; Liporagi-Lopes, L.C.; Aor, A.C.; Branquinha, M.H.; Santos, A.L. Insights into the social life and obscure side of Scedosporium/Lomentospora species: ubiquitous, emerging and multidrug-resistant opportunistic pathogens. Fungal Biol. Rev. 2018, 33, 16–46. [Google Scholar] [CrossRef]
- Shi, X.-W.; Li, S.-T.; Lou, J.-P.; Xu, B.; Wang, J.; Wang, X.; Liu, H.; Li, S.-K.; Zhen, P.; Zhang, T. Scedosporium apiospermum infection of the lumbar vertebrae: A case report. World J. Clin. Cases 2022, 10, 3251–3260. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Utsumi, Y.; Suzuki, N.; Nakajima, Y.; Murata, O.; Sasaki, N.; Nitanai, H.; Nagashima, H.; Miyamoto, S.; Yaegashi, J.; et al. Multiple Scedosporium apiospermum abscesses in a woman survivor of a tsunami in northeastern Japan: a case report. J. Med Case Rep. 2011, 5, 526–526. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y. , Suzuki, N. , Nakajima, Y., Utsumi, Y., Murata, O., Nagashima, H., Saito, H., Sasaki, N., Fujimura, I., Ogino, Y., et al. Scedosporium auarantiacum brain abscess after near-drowning in a survivor of a tsunami in Japan. Respir. Investig. 2013, 51, 207–211. [Google Scholar]
- Miceli, M.H. Central Nervous System Infections Due to Aspergillus and Other Hyaline Molds. J. Fungi 2019, 5, 79. [Google Scholar] [CrossRef] [PubMed]
- Lauerer, R.J.; Rosenow, E.; Beschorner, R.; Hempel, J.-M.; Naros, G.; Hofmann, A.; Berger, K.; Sartor-Pfeiffer, J.; Mengel, A.; Ziemann, U.; et al. Rapid Diagnosis of Central Nervous System Scedosporiosis by Specific Quantitative Polymerase Chain Reaction Applied to Formalin-Fixed, Paraffin-Embedded Tissue. J. Fungi 2021, 8, 19. [Google Scholar] [CrossRef]
- zkan, A. , Susever, S. , Erturan, Z., Uzun, M., Alparslan, N., Öz, Y., Yeenoglu, Y. A case of keratitis caused by Scedosporium apiospermum. J. Microbiol. Infect. Dis. 2013, 3, 45–48. [Google Scholar]
- Hayashi, Y.; Eguchi, H.; Toibana, T.; Mitamura, Y.; Yaguchi, T. Polymicrobial Sclerokeratitis Caused by Scedosporium apiospermum and Aspergillus cibarius. Cornea 2014, 33, 875–877. [Google Scholar] [CrossRef]
- Palanisamy, M. , Venkatapathy, N. , Rajendram, V., Shobana, C.S. Keratomycosis caused by Graphium eumorphum (Graphium state of Scedosporium apiospermum). J. Clin. Diagn. Res. 2015, 9, DD03–DD04. [Google Scholar]
- Baskaran, P.; Ramakrishnan, S.; Mandlik, K.; Sathe, T.S.; Gubert, J.; Krishnan, T. Ocular infections caused by Scedosporium apiospermum: A case series. Indian J. Ophthalmol. 2018, 66, 137. [Google Scholar] [CrossRef]
- Carnovale, S.; Epelbaum, C.; Abrantes, R.; Córdoba, S.; Cabrera, C.; Caracciolo, B. Scedosporium aurantiacum: First isolation in Argentina from a previously healthy patient after traumatic inoculation. 2022, 54, 318–321. [CrossRef]
- Karaca, U. Scedosporium apiospermum keratitis: a case report. J. Med. Case Rep. 2022, 16, 91. [Google Scholar] [CrossRef] [PubMed]
- Ali, D.; Vijayan, A.; Shenoy, K.; Antony, A.T.; Ramachandran, R. Challenges in the diagnosis and management of atypical fungal keratitis during the COVID-19 pandemic: a case series. Access Microbiol. 2023, 5, 000570–v3. [Google Scholar] [CrossRef] [PubMed]
- Motokawa, N.; Miyazaki, T.; Hara, A.; Fukuda, Y.; Morino, S.; Nakamura, H.; Iwasaki, K.; Soda, H.; Izumikawa, K.; Yanagihara, K.; et al. Pulmonary Scedosporium apiospermum Infection with Pulmonary Tumorlet in an Immunocompetent Patient. Intern. Med. 2018, 57, 3485–3490. [Google Scholar] [CrossRef] [PubMed]
- Liu, W. , Feng, R. , Jiang, H. Scedosporium spp. lung infection in immunocompetent patients. A systematic review and MOOSE-compliant meta-analysis. Medicine 2019, 98, 41. [Google Scholar]
- Liu, W.; Feng, R.; Jiang, H. Management of pulmonary Scedosporium apiospermum infection by thoracoscopic surgery in an immunocompetent woman. J. Int. Med Res. 2020, 48. [Google Scholar] [CrossRef] [PubMed]
- Renner, S.; Nachbaur, E.; Jaksch, P.; Dehlink, E. Update on Respiratory Fungal Infections in Cystic Fibrosis Lung Disease and after Lung Transplantation. J. Fungi 2020, 6, 381. [Google Scholar] [CrossRef]
- Sav, H.; Altinbas, R.; Dursun, Z.B. A fatal invasive Scedosporium apiospermum pulmonary infection in an adult patient with malignant lung adenocarcinoma. Curr. Med Mycol. 2020, 6, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Ghasemian, R.; Bandegani, A.; Kermani, F.; Faeli, L.; Roohi, B.; YousefiAbdolmaleki, E.; Hedayati, M.T.; Roilides, E.; Shokohi, T. Fatal pulmonary Scedosporium aurantiacum infection in a patient after near-drowning: A case report. Curr. Med Mycol. 2022, 7, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez-Martínez, E.; Solé, A.; Cañada-Martínez, A.; Muñoz-Núñez, C.F.; Pastor, A.; Montull, B.; Falomir-Salcedo, P.; Valentín, A.; López-Hontangas, J.L.; Pemán, J. Invasive scedosporiosis in lung transplant recipients: A nine-year retrospective study in a tertiary care hospital. 2021, 38, 184–187. [CrossRef]
- Mizusawa, M.; Totten, M.; Zhang, S.X. A Case of Scedosporium aurantiacum Infection in the United States. Mycopathologia 2021, 186, 127–130. [Google Scholar] [CrossRef]
- Puerta-Alcalde, P. , Garcia-Vidal, C. Non-Aspergillus mould lung infections. Eur. Respir. Rev. 2022, 31, 220104. [Google Scholar]
- Kishimoto, I.; Shinohara, S.; Ueda, T.; Tani, S.; Yoshimura, H.; Imai, Y. Orbital apex syndrome secondary to a fungal nasal septal abscess caused by Scedosporium apiospermum in a patient with uncontrolled diabetes: a case report. BMC Infect. Dis. 2017, 17, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Loh, U.L.; Tai, P.Y.; Hussein, A.; A Qamarruddin, F. Scedosporium apiospermum: A Rare Cause of Aggressive Orbital Apex Syndrome. Cureus 2018, 10, e3743. [Google Scholar] [CrossRef] [PubMed]
- Singla, S.; Singh, V.; Bansal, A.; Sharma, J.P.; Wadhwa, T.; Sarma, S. Post COVID-19 acute invasive fungal rhinosinusitis caused by Scedosporium apiospermum: a covert pathogen. Int. J. Otorhinolaryngol. Head Neck Surg. 2021, 7, 1187–1192. [Google Scholar] [CrossRef]
- K, S.; B, P.; M, P.; M, A.; V, L. A case of bilateral injection abscesses caused by Graphium type of Scedosporium apiospermum. Med Mycol. Case Rep. 2022, 37, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Pan, S.-F.; Huang, S.-M.; Xie, L.; Zhang, Y.-Y.; Tang, Y.-R.; Wang, X.-Z.; Pan, &. S.-F.; Ast; Huang, &.S.-M.; Lian Xie, Yuan-Yuan Zhang, Yu-Rong Tang, Xiao-Zhen Wang Department of Clinical Laboratory, Shengli Oilfield Central Hospital, Dongying, People’s Republic of China& et al. A Case of Invasive Fungal Infection Due to Scedosporium apiospermum in a Patient with Psoriasis. Infect. Drug Resist. 2023, ume 16, 5085–5090. [Google Scholar] [CrossRef]
- Pieta, A.; Venetsanopoulou, A.I.; Kittas, C.; Christaki, E.; Voulgari, P.V. Recurrent Scedosporium apiospermum Cutaneous Infection in a Patient with Rheumatoid Arthritis: The Potent Role of IL-6 Signaling Pathway Blockade: A Case-Based Review. J. Fungi 2023, 9, 683. [Google Scholar] [CrossRef]
- Hirschi, S.; Letscher-Bru, V.; Pottecher, J.; Lannes, B.; Jeung, M.Y.; Degot, T.; Santelmo, N.; Sabou, A.M.; Herbrecht, R.; Kessler, R. Disseminated Trichosporon mycotoxinivorans, Aspergillus fumigatus, and Scedosporium apiospermum Coinfection after Lung and Liver Transplantation in a Cystic Fibrosis Patient. J. Clin. Microbiol. 2012, 50, 4168–4170. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, C.; Brandt, C.; Melichar, V.; Runge, C.; Heuer, E.; Sahly, H.; Schebek, M.; Köster, H.; Bouchara, J.-P.; Biedermann, T.; et al. Combined antifungal therapy is superior to monotherapy in pulmonary scedosporiosis in cystic fibrosis. J. Cyst. Fibros. 2019, 18, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Viñado, C. , Girón, R. M., Ilbáñez, E., García-Ortega, A., Pérez, I., Polanco, D., Pemán, J., Solé, A. Filamentous fungi in the airway of patients with cystic fibrosis: just spectators? Rev. Iberoam. Micol. 2012, 38, 168–174. [Google Scholar]
- Marr, K.A.; Carter, R.A.; Crippa, F.; Wald, A.; Corey, L. Epidemiology and Outcome of Mould Infections in Hematopoietic Stem Cell Transplant Recipients. Clin. Infect. Dis. 2002, 34, 909–917. [Google Scholar] [CrossRef]
- Kubak, B.M.; Huprikar, S.S. ; the AST Infectious Diseases Community of Practice Emerging & Rare Fungal Infections in Solid Organ Transplant Recipients. Am. J. Transplant. 2009, 9, S208–S226. [Google Scholar] [CrossRef]
- Rahi, M.S.; Jindal, V.; Pednekar, P.; Parekh, J.; Gunasekaran, K.; Sharma, S.; Stender, M.; Jaiyesimi, I.A. Fungal infections in hematopoietic stem-cell transplant patients: a review of epidemiology, diagnosis, and management. Ther. Adv. Infect. Dis. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Bourlond, B.; Cipriano, A.; Regamey, J.; Papadimitriou-Olivgeris, M.; Kamani, C.; Seidel, D.; Lamoth, F.; Muller, O.; Yerly, P. Case report: Disseminated Scedosporium apiospermum infection with invasive right atrial mass in a heart transplant patient. Front. Cardiovasc. Med. 2022, 9, 1045353. [Google Scholar] [CrossRef]
- Zeng, C.; Ma, Y.-S.; Zhou, J.-Y.; Xue, C.-B.; Xiong, Y.; Zhou, W.; Zhou, L.-H.; Li, J.-G.; Ye, S.-J.; Ye, Q.-F. Donor-Derived Transmission of Scedosporiosis in Kidney Transplant Recipients from a Systemic lupus erythematosus donor. Curr. Med Sci. 2023, 43, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Cattaneo, L. , Buonomo, A. R., Iacovazzo, C., Giaccone, A., Scotto, R., Viceconte, G., Mercinelli, S., Vargas, M., Roscetto, E., Cacciatore, F., et al. Invasive fungal infections in hospitalised patients with COVID-19: a non-intensive care single-centre experience during the first pandemic. J. Fungi 2023, 9, 86. [Google Scholar]
- Lee, M.-G.; Choi, J.-G.; Son, B.-C. Scedosporium apiospermum: An emerging fatal cause of fungal abscess and ventriculitis after near-drowning. Asian J. Neurosurg. 2018, 13, 792–796. [Google Scholar] [CrossRef]
- Mavrouli, M.; Mavroulis, S.; Lekkas, E.; Tsakris, A. Respiratory Infections Following Earthquake-Induced Tsunamis: Transmission Risk Factors and Lessons Learned for Disaster Risk Management. Int. J. Environ. Res. Public Heal. 2021, 18, 4952. [Google Scholar] [CrossRef]
- Warkentien, T.; Rodriguez, C.; Lloyd, B.; Wells, J.; Weintrob, A.; Dunne, J.R.; Ganesan, A.; Li, P.; Bradley, W.; Gaskins, L.J.; et al. Invasive Mold Infections Following Combat-related Injuries. Clin. Infect. Dis. 2012, 55, 1441–1449. [Google Scholar] [CrossRef] [PubMed]
- Angelini, A.; Drago, G.; Ruggieri, P. Post-tsunami primary Scedosporium apiospermum osteomyelitis of the knee in an immunocompetent patient. Int. J. Infect. Dis. 2013, 17, e646–e649. [Google Scholar] [CrossRef]
- Tribble, D.R. , Rodriguez, C. J. Combat-related fungal invasive wound infections. Curr. Fungal Infect. Rep. 2014, 8, 277–286. [Google Scholar]
- Kronen, R.; Liang, S.Y.; Bochicchio, G.; Bochicchio, K.; Powderly, W.G.; Spec, A. Invasive Fungal Infections Secondary to Traumatic Injury. Int. J. Infect. Dis. 2017, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, A.; Shaikh, F.; Bradley, W.; Blyth, D.M.; Bennett, D.; Petfield, J.L.; Carson, M.L.; Wells, J.M.; Tribble, D.R. ; Infectious Disease Clinical Research Program Trauma Infectious Disease Outcomes Study Group Classification of Trauma-Associated Invasive Fungal Infections to Support Wound Treatment Decisions. Emerg. Infect. Dis. 2019, 25, 1639–1647. [Google Scholar] [CrossRef] [PubMed]
- WHO (2022). WHO fungal priority pathogens list to guide research, development and public health action (Geneva: World Health Organization). License: CC BY-NC-SA 3.0 IGO.
- Delhaes, L. , Harun, A. , Chen, S.C.A., Nguyen, Q., Slavin, M., Heath, C.H., Maszewska, K., Halliday, C., Robert, V., Sorrell, T.C., et al. Molecular typing of Australian Scedosporium isolates showing genetic variability and numerous S. aurantiacum. Emerg. Infect. Dis. 2008, 14, 282–290. [Google Scholar]
- Giraud, S.; Bouchara, J.-P. Scedosporium apiospermum Complex: Diagnosis and Species Identification. Curr. Fungal Infect. Rep. 2014, 8, 211–219. [Google Scholar] [CrossRef]
- Subedi, S.; Chen, S.C.-A. Epidemiology of Scedosporiosis. Curr. Fungal Infect. Rep. 2015, 9, 275–284. [Google Scholar] [CrossRef]
- Abrantes, R.A. , Refojo, N. , Hevia, A.I., Fernández, J., Isla, G., Córdoba, S., Dávalos, M.F., Lubovich, S., Maldonado, I., Davel, G.O., et al. Scedosporium spp. from clinical setting in Argentina, with the proposal of the new pathogenic species Scedosporium americanum. J. Fungi 2021, 7, 160. [Google Scholar]
- Neoh, C.F. , Chen, S. C-A., Crowe, A., Hamilton K., Nguyen, Q.A., Marriot, D., Trubiano, J.A., Spelman, T., Kong, D.C.M., Slavin, M.A. Invasive Scedosporium and Lomentospora prolificans infections in Australia: a multicentre retrospective cohort study. Open Forum Infect. Dis. 2023, 10, ofad059. [Google Scholar]
- Hayden, R.T. , Isotalo, P. A., Parrett, T., Wolk, D.M., Qian, X., Roberts, G.D., Lloyd, R.V. In situ hybridisation for the differentiation of Aspergillus, Fusarium, and Pseudallescheria species in tissue section. Diagn. Mol. Pathol. 2003, 12, 21–26. [Google Scholar] [PubMed]
- Chen, S.C.-A.; Halliday, C.L.; Hoenigl, M.; Cornely, O.A.; Meyer, W. Scedosporium and Lomentospora Infections: Contemporary Microbiological Tools for the Diagnosis of Invasive Disease. J. Fungi 2021, 7, 23. [Google Scholar] [CrossRef]
- Rai, P.; Singh, A.K.; Anand, K.B.; Singh, S.P.; Tomar, K. Time versus tissue: Timely identification of Scedosporium Rhinosinusitis in a post-COVID-19 case by MALDI-TOF MS leading to successful management. Med J. Armed Forces India 2022, 78, 360–364. [Google Scholar] [CrossRef]
- Mina, S. , Marot-Leblond, A. , Cimon, B., Fleury, M.J.J., Larcher, G., Bouchara, J.-P. Purification and characterisation of a mycelial catalase from Scedosporium boydii, a useful tool for specific antibody detection patients with cystic fibrosis. Clin. Vacc. Immunol. 2015, 22, 37–45. [Google Scholar]
- Martin-Souto, L. , Antoran, A. , Areitio, M., Aparicio-Fernandez, L., Martín-Gómez, M.T., Fernandez, R., Astigarraga, E., Barreda- Gómez, G., Schwarz, C., Rickerts, V., et al. Dot immunoblotting assay for the rapid serodetection of Scedosporium/Lomentospora in cystic fibrosis patients. J. Fungi 2023, 9, 158. [Google Scholar]
- Thornton, C.R. Tracking the Emerging Human Pathogen Pseudallescheria boydii by Using Highly Specific Monoclonal Antibodies. Clin. Vaccine Immunol. 2009, 16, 756–764. [Google Scholar] [CrossRef] [PubMed]
- Davies, G.E. , Thornton, C. R. Development of a monoclonal antibody and a serodiagnostic lateral-flow device specific to Rhizopus arrhizus (Syn. R. oryzae), the principal global agent of mucormycosis in humans. J. Fungi 2022, 8, 756. [Google Scholar]
- Thornton, C.R.; Davies, G.E.; Dougherty, L. Development of a monoclonal antibody and a lateral-flow device for the rapid detection of a Mucorales-specific biomarker. Front. Cell. Infect. Microbiol. 2023, 13, 1305662. [Google Scholar] [CrossRef]
- Cerne, C.; Seyedmousavi, S.; Bennett, J.E. Cutaneous hyalohyphomycosis due to Petriella setifera following traumatic inoculation in an immunocompetent host. Med Mycol. Case Rep. 2021, 32, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Marques, D.S. , Vaz, C. P., Branca, R., Campilho, F., Lamelas, C., Afonso, L.P., et al. Rhizomucor and Scedosporium infection post hematopoietic stem-cell transplant. Case Rep. Med. 2011, 2011, 830769. [Google Scholar]
- Shand, J.M.; Albrecht, R.M.; Burnett, H.F.; Miyake, A. Invasive fungal infection of the midfacial and orbital complex due to Scedosporium apiospermum and mucormycosis. J. Oral Maxillofac. Surg. 2004, 62, 231–234. [Google Scholar] [CrossRef]
- Song, Y.; Zhou, M.; Gong, Q.; Guo, J. Scedosporium apiospermum and Lichtheimia corymbifera Co-Infection Due to Inhalation of Biogas in Immunocompetent Patients: A Case Series. Infect. Drug Resist. 2022, ume 15, 6423–6430. [Google Scholar] [CrossRef]
- Kanaujia, R.; Muthu, V.; Singh, S.; Rudramurthy, S.M.; Kaur, H. Rapidly progressive lung coinfection due to Rhizopus and Scedosporium in a diabetic marijuana smoker. Clin. Microbiol. Infect. 2022, 29, 51–53. [Google Scholar] [CrossRef]
- Pinto, M.R.; Mulloy, B.; Haido, R.M.T.; Travassos, L.R.; Bergter, E.B. A peptidorhamnomannan from the mycelium of Pseudallescheria boydii is a potential diagnostic antigen of this emerging human pathogen. Microbiology 2001, 147, 1499–1506. [Google Scholar] [CrossRef] [PubMed]
- Lopes, L.C.L.; Rollin-Pinheiro, R.; Guimarães, A.J.; Bittencourt, V.C.B.; Martinez, L.R.; Koba, W.; Farias, S.E.; Nosanchuk, J.D.; Barreto-Bergter, E. Monoclonal Antibodies Against Peptidorhamnomannans of Scedosporium apiospermum Enhance the Pathogenicity of the Fungus. PLOS Neglected Trop. Dis. 2010, 4, e853. [Google Scholar] [CrossRef] [PubMed]
- Thornton, C.R. Detection of the ‘big five’ mold killers of humans: Aspergillus, Fusarium, Lomentospora, Scedosporium and Mucormycetes. Adv. Appl. Microbiol. 2020, 110, 1–61. [Google Scholar] [PubMed]
- Thornton, C.R. Development of an Immunochromatographic Lateral-Flow Device for Rapid Serodiagnosis of Invasive Aspergillosis. Clin. Vaccine Immunol. 2008, 15, 1095–1105. [Google Scholar] [CrossRef] [PubMed]
- Di Nardo, F.; Chiarello, M.; Cavalera, S.; Baggiani, C.; Anfossi, L. Ten Years of Lateral Flow Immunoassay Technique Applications: Trends, Challenges and Future Perspectives. Sensors 2021, 21, 5185. [Google Scholar] [CrossRef] [PubMed]
- Land, K.J.; Boeras, D.I.; Chen, X.-S.; Ramsay, A.R.; Peeling, R.W. REASSURED diagnostics to inform disease control strategies, strengthen health systems and improve patient outcomes. Nat. Microbiol. 2018, 4, 46–54. [Google Scholar] [CrossRef]
- Thornton, C.R. The potential for rapid antigen testing for mucormycosis in the context of COVID-19. Expert Rev. Mol. Diagn. 2023, 1–7. [Google Scholar] [CrossRef]
Figure 1.
(A) The organs of the human body infected by Scedosporium spp. Eumycetoma is a chronic deep infection of the skin and subcutaneous tissues. (B). Standard operating procedure (SOP) for treatment of human serum and use of the ScedLFD test. Step 1: human serum is mixed 1:2 (vol:vol) with PBS buffer containing Na2EDTA, and then heated for 3 min at 100 oC in a boiling water bath. Step 2: the heated serum is centrifuged at 16,000 x g for 5 min to pellet insoluble serum proteins. Step 3: following centrifugation, the clear supernatant is mixed 1:1 (vol:vol) with LFD running buffer, 100 mL is added to the sample port of the LFD test and, after 30 min, the control (C) and test (T) line intensities determined using a Cube reader. (C) Negative test result for unrelated yeasts (Candida and Cryptococcus) and moulds (Aspergillus, Fusarium, Mucorales) of clinical significance. Note the absence of the test (T) line but presence of the control (C) line showing that the test has run correctly. (D) Positive test result for Scedosporium spp. detected by the ScedLFD test. The species in bold are responsible for the majority of infections in humans. Note the presence of the test (T) and control (C) lines. Figure ”Created with BioRender.com”.
Figure 1.
(A) The organs of the human body infected by Scedosporium spp. Eumycetoma is a chronic deep infection of the skin and subcutaneous tissues. (B). Standard operating procedure (SOP) for treatment of human serum and use of the ScedLFD test. Step 1: human serum is mixed 1:2 (vol:vol) with PBS buffer containing Na2EDTA, and then heated for 3 min at 100 oC in a boiling water bath. Step 2: the heated serum is centrifuged at 16,000 x g for 5 min to pellet insoluble serum proteins. Step 3: following centrifugation, the clear supernatant is mixed 1:1 (vol:vol) with LFD running buffer, 100 mL is added to the sample port of the LFD test and, after 30 min, the control (C) and test (T) line intensities determined using a Cube reader. (C) Negative test result for unrelated yeasts (Candida and Cryptococcus) and moulds (Aspergillus, Fusarium, Mucorales) of clinical significance. Note the absence of the test (T) line but presence of the control (C) line showing that the test has run correctly. (D) Positive test result for Scedosporium spp. detected by the ScedLFD test. The species in bold are responsible for the majority of infections in humans. Note the presence of the test (T) and control (C) lines. Figure ”Created with BioRender.com”.
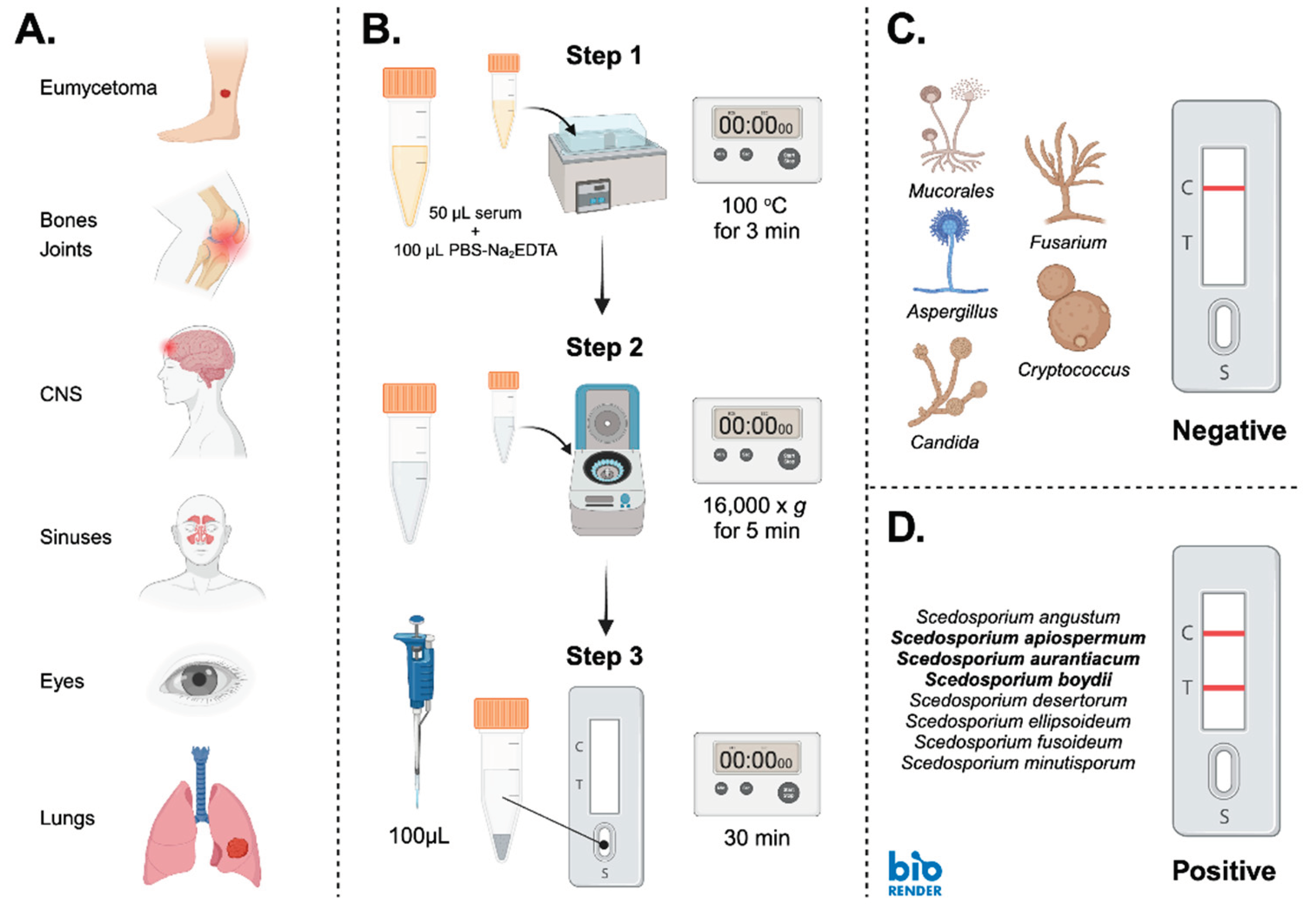
Figure 2.
Western blot of EPS antigens (20 mg EPS/lane) from Scedosporium apiospermum isolate RMRL8353, Scedosporium aurantiacum isolate CBS121926, Scedosporium boydii isolate CBS835.96, and Aspergillus fumigatus isolate Af293. Note the strong binding of mAb HG12 with Scedosporium antigens with molecular weights of between ~15 kDa and 250 kDa, and lack of reactivity with A. fumigatus antigens.
Figure 2.
Western blot of EPS antigens (20 mg EPS/lane) from Scedosporium apiospermum isolate RMRL8353, Scedosporium aurantiacum isolate CBS121926, Scedosporium boydii isolate CBS835.96, and Aspergillus fumigatus isolate Af293. Note the strong binding of mAb HG12 with Scedosporium antigens with molecular weights of between ~15 kDa and 250 kDa, and lack of reactivity with A. fumigatus antigens.
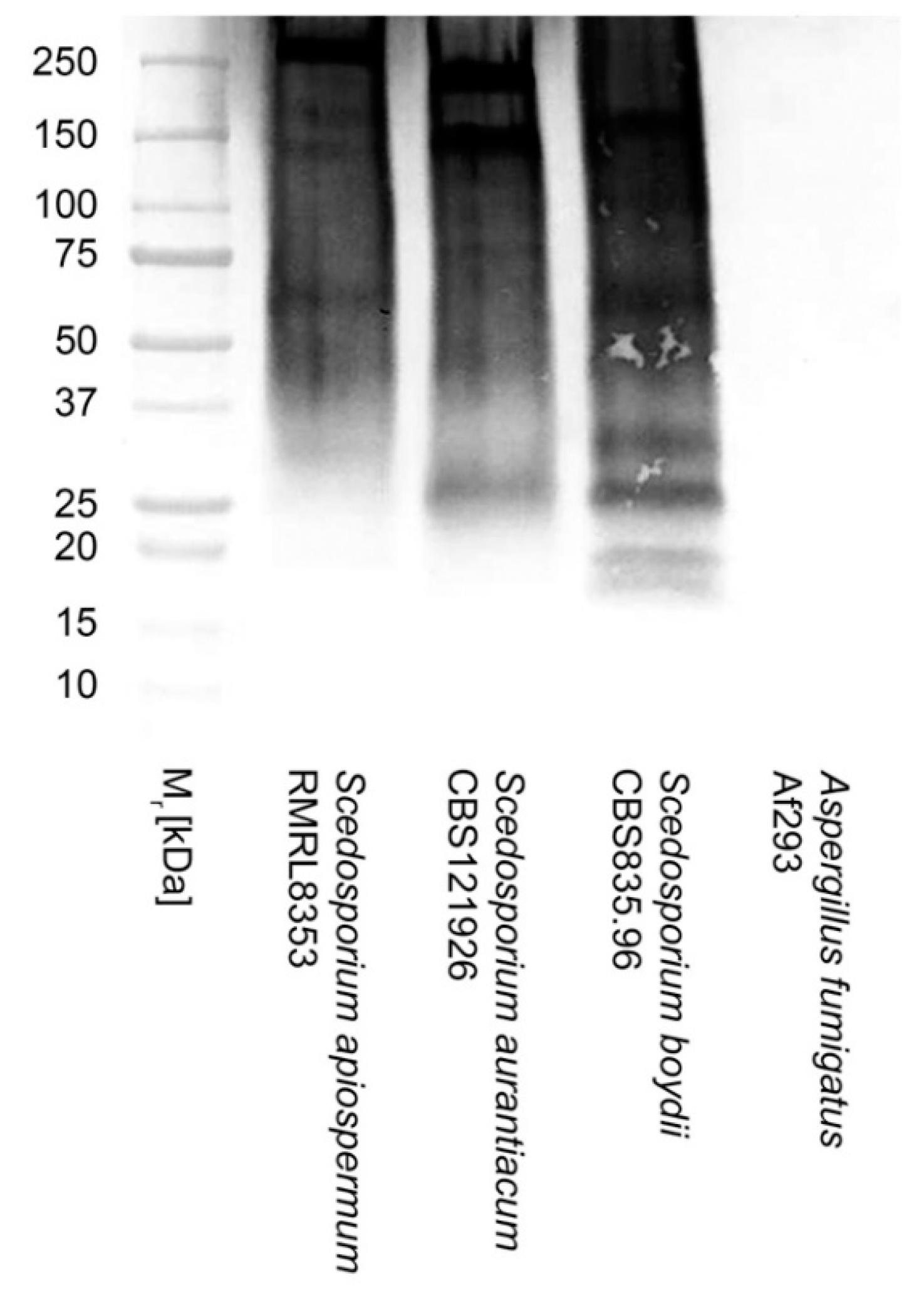
Figure 3.
Limits of detection (LOD) of the ScedLFD test using purified extracellular polysaccharide (EPS) antigens from S. aurantiacum isolate CBS121926 (A,B), S. apiospermum isolate RMRL8353 (C,D), and S. boydii isolate CBS835.96 (E,F). Cube readings of test (T) line intensities measured as artificial units (a.u) for EPS diluted into LFD running buffer (A,C,E), and for EPS diluted into serum (B,D,F). Data points are the means of 2 replicates ±SE. All ScedLFD tests had control (C) line scores of >600 a.u. using the Cube reader. The LODs are indicated by asterisks (*), which show a significant (Student’s t-test [p<0.05]) difference in a.u. values compared to control samples (unspiked LFD running buffer (0.00ng/mL RB), and normal unspiked serum (0.00ng/mL serum), respectively.
Figure 3.
Limits of detection (LOD) of the ScedLFD test using purified extracellular polysaccharide (EPS) antigens from S. aurantiacum isolate CBS121926 (A,B), S. apiospermum isolate RMRL8353 (C,D), and S. boydii isolate CBS835.96 (E,F). Cube readings of test (T) line intensities measured as artificial units (a.u) for EPS diluted into LFD running buffer (A,C,E), and for EPS diluted into serum (B,D,F). Data points are the means of 2 replicates ±SE. All ScedLFD tests had control (C) line scores of >600 a.u. using the Cube reader. The LODs are indicated by asterisks (*), which show a significant (Student’s t-test [p<0.05]) difference in a.u. values compared to control samples (unspiked LFD running buffer (0.00ng/mL RB), and normal unspiked serum (0.00ng/mL serum), respectively.
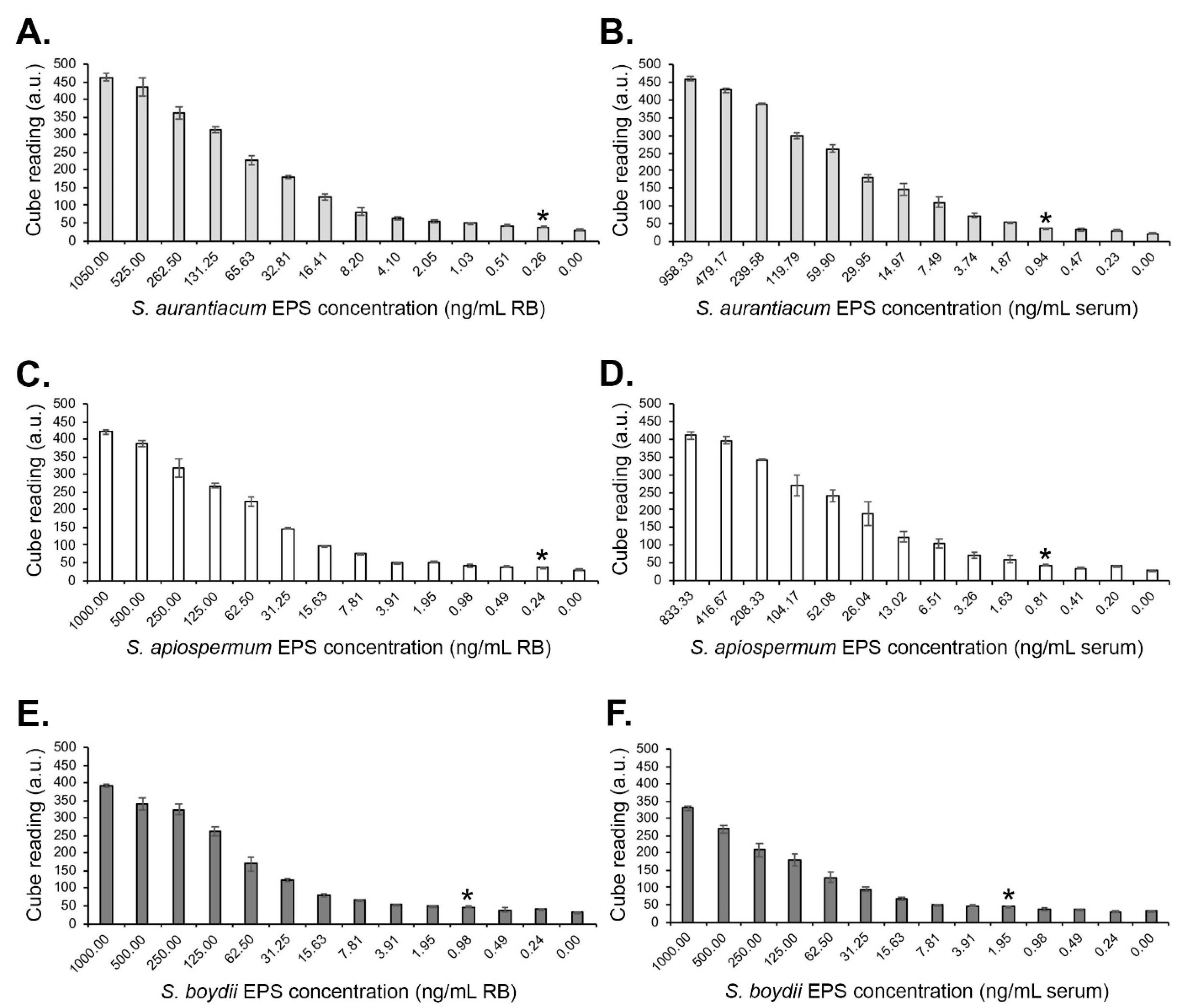
Figure 4.
Limits of detection (LOD) in serum of the ScedELISA using purified extracellular polysaccharide (EPS) antigens from S. aurantiacum isolate CBS121926, S. apiospermum isolate RMRL8353, and S. boydii isolate CBS835.96. Each data point is the mean of three replicates ±SE, and the threshold absorbance value for test positivity, determined from the negative control (normal serum only), is ≥0.100. Using this threshold value, the limits of detection of the ScedELISA are ~62.5 ng/mL serum, ~15.6 ng/mL serum, and ~125 ng/mL serum for S. apiospermum, S. aurantiacum, and S. boydii, respectively.
Figure 4.
Limits of detection (LOD) in serum of the ScedELISA using purified extracellular polysaccharide (EPS) antigens from S. aurantiacum isolate CBS121926, S. apiospermum isolate RMRL8353, and S. boydii isolate CBS835.96. Each data point is the mean of three replicates ±SE, and the threshold absorbance value for test positivity, determined from the negative control (normal serum only), is ≥0.100. Using this threshold value, the limits of detection of the ScedELISA are ~62.5 ng/mL serum, ~15.6 ng/mL serum, and ~125 ng/mL serum for S. apiospermum, S. aurantiacum, and S. boydii, respectively.
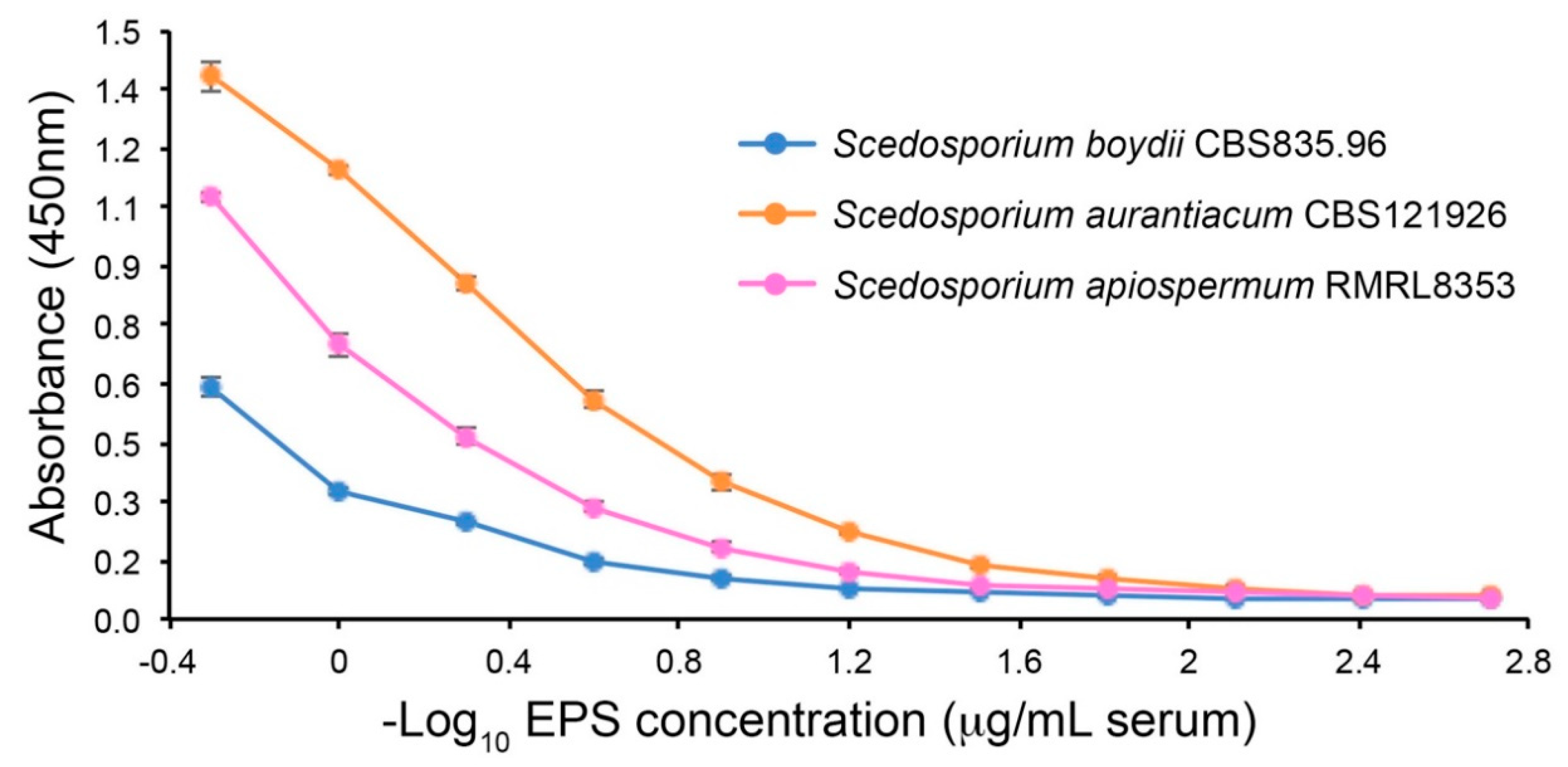

Table 1.
Details of fungi used in this study, and results of ScedLFD and ScedELISA tests using culture filtrates from fungi grown as shake cultures for 72 h in YNB+G medium. 1CBS; Westerdijk Fungal Biodiversity Institute, The Netherlands. CRT; C. R. Thornton, University of Exeter, UK. RMRL; Regional Mycology Reference Laboratory, University Hospital, South Manchester, England, UK. FGSC; 2For ScedLFD tests, test (T) line Cube readings in artificial units (a.u.) are the means of two replicate values. The threshold T line value for LFD test positivity is ≥60 a.u. (2 x a.u. value for the YNB+G only negative control). All LFD tests had control (C) line values of ≥600 a.u.. 3For ELISA tests, the threshold absorbance value for test positivity is ≥0.100 (2 x absorbance value for the YNB+G only negative control).
Table 1.
Details of fungi used in this study, and results of ScedLFD and ScedELISA tests using culture filtrates from fungi grown as shake cultures for 72 h in YNB+G medium. 1CBS; Westerdijk Fungal Biodiversity Institute, The Netherlands. CRT; C. R. Thornton, University of Exeter, UK. RMRL; Regional Mycology Reference Laboratory, University Hospital, South Manchester, England, UK. FGSC; 2For ScedLFD tests, test (T) line Cube readings in artificial units (a.u.) are the means of two replicate values. The threshold T line value for LFD test positivity is ≥60 a.u. (2 x a.u. value for the YNB+G only negative control). All LFD tests had control (C) line values of ≥600 a.u.. 3For ELISA tests, the threshold absorbance value for test positivity is ≥0.100 (2 x absorbance value for the YNB+G only negative control).
| Species | Isolate Number | Source1 |
ScedLFD a.u.2 |
ScedELISA (Abs 450nm)3 |
|
|---|---|---|---|---|---|
| Apophysomyces variabilis | 658.93 | CBS | 28.8 | 0.052 | |
| Aspergillus fumigatus | Af293 | FGSC | 35.7 | 0.046 | |
| Aspergillus flavus | 144B | CRT | 27.9 | 0.049 | |
| Aspergillus nidulans | A4 | FGSC | 35.1 | 0.044 | |
| Aspergillus niger | 102.4 | CBS | 32.7 | 0.052 | |
| Aspergillus terreus var. terreus | 601.65 | CBS | 30.3 | 0.049 | |
| Candida albicans | SC5314 | SB | 37.1 | 0.060 | |
| Cryptococcus neoformans | 8710 | CBS | 46.5 | 0.055 | |
| Cunninghamella bertholletiae | 151.80 | CBS | 34.5 | 0.053 | |
| Fusarium oxysporum | 167.3 | CBS | 34.0 | 0.052 | |
| Fusarium solani | 224.34 | CBS | 31.7 | 0.047 | |
| Lichtheimia corymbifera | 109940 | CBS | 30.5 | 0.053 | |
| Lichtheimia hyalospora | 146576 | CBS | 33.0 | 0.045 | |
| Lichtheimia ornata | 142195 | CBS | 33.7 | 0.050 | |
| Lichtheimia ramosa | 124197 | CBS | 32.4 | 0.049 | |
| Lomentospora prolificans | 3.1 | CRT | 33.0 | 0.090 | |
| Lomentospora prolificans | 742.96 | CBS | 41.3 | 0.048 | |
| Lomentospora prolificans | 100390 | CBS | 43.0 | 0.046 | |
| Mucor circinelloides | 123973 | CBS | 33.8 | 0.056 | |
| Mucor circinelloides | 124429 | CBS | 38.2 | 0.056 | |
| Mucor circinelloides f. circinelloides | 120582 | CBS | 36.7 | 0.051 | |
| Mucor indicus | 120.08 | CBS | 34.4 | 0.044 | |
| Petriella setifera | 109039 | CBS | 622.3 | 1.431 | |
| Rhizomucor pusillus | 120586 | CBS | 31.7 | 0.051 | |
| Rhizopus arrhizus var. arrhizus | 112.07 | CBS | 37.5 | 0.056 | |
| Rhizopus arrhizus var. delemar | 607.68 | CBS | 38.8 | 0.051 | |
| Rhizopus rhizopodiformis | 102277 | CBS | 32.3 | 0.050 | |
| Scedosporium angustum | 254.72 | CBS | 489.4 | 1.042 | |
| Scedosporium apiospermum | 8353 | RMRL | 426.2 | 0.815 | |
| Scedosporium apiospermum | 117407 | CBS | 469.5 | 1.337 | |
| Scedosporium aurantiacum | 118934 | CBS | 691.1 | 1.403 | |
| Scedosporium aurantiacum | 121926 | CBS | 737.1 | 1.427 | |
| Scedosporium boydii | 835.96 | CBS | 373.4 | 1.190 | |
| Scedosporium boydii | 100393 | CBS | 593.5 | 1.394 | |
| Scedosporium boydii | 100395 | CBS | 435.4 | 0.786 | |
| Scedosporium boydii | 100870 | CBS | 474.3 | 1.126 | |
| Scedosporium boydii | Exton 22A | CRT | 449.7 | 1.121 | |
| Scedosporium dehoogii | 117406 | CBS | 28.1 | 0.049 | |
| Scedosporium desertorum | 489.72 | CBS | 500.2 | 1.310 | |
| Scedosporium ellipsoideum | 438.75 | CBS | 525.1 | 1.315 | |
| Scedosporium fusoideum | 106.53 | CBS | 598.0 | 1.290 | |
| Scedosporium minutisporum | 116911 | CBS | 383.3 | 0.592 | |
| YNB+G only | - | - | 29.8 | 0.048 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



