
Submitted:
28 March 2024
Posted:
28 March 2024
You are already at the latest version
Abstract
Introduction the outbreak of the Israel-Gaza conflict, initiated by a major attack on the civilian population in Israel provided a tragic opportunity to study the community wide association between severe emotional stressors related to acts of war and the incidence and clinical characteristics of Takotsubo cardiomyopathy (TCM) in this scenario.
Methods Eight consecutive cases of TCM diagnosed during the first 50 days of the Israel-Gaza conflict were retrospectively collected from two southern medical centers who provided care to most of the war victims throughout the period of monitoring. The medical records were thoroughly reviewed and analyzed.
Results During the monitoring period, the incidence of TCM increased substantially compared to the control period. Eight patients were included in the analysis. All patients were female and 100% of patients presented within the first 3 weeks of conflict whereas after this initial phase, despite the continuing war, the incidence of TCM reverted to pre-conflict levels. Two patients (25%) were under 50 years of age. All patients had hazardous clinical characteristics including severe left ventricular (LV) dysfunction (≤35%) and prolonged QTc interval (>500 ms). Five patients (62.5%) experienced complications. Nevertheless, no in-hospital mortality was reported.
Conclusions Repeated exposure to severe emotional stress, on both personal and national level, due to mass crisis such as war is associated with an increased incidence of TCM potentially with high-risk phenotype in comparison to TCM following other, less potent, psychological insults.
Keywords:
Takotsubo cardiomyopathy
; left ventricular dysfunction
; stress-induced cardiomyopathy
; war
Introduction
The existence of a complex bidirectional “dialogue” between brain and heart is well established [1]. Multiple studies have shown that psychological stress is an independent risk factor for heart diseases including coronary artery disease (CAD), arrhythmias, heart failure and sudden death [2,3,4,5]. Takotsubo cardiomyopathy (TCM) is an acute and transient LV dysfunction of non-ischemic etiology, which predominantly affects post-menopausal women. Although considered characteristic, a preceding stressful event is evident in 30-40% of patients [6]. The salient clinical features and in-hospital complications of TCM are presented in Table 1 and Table 2, respectively.
On October 7th, 2023, Hamas organization launched a major attack against Israeli civilians leading to thousands of victims and escalating into a broad Israel-Gaza conflict. During the war numerous rocket barrages were fired daily from the Gaza strip towards towns and cities in Israel. Hence, the aim of the present study was to examine the incidence, clinical characteristics, and in-hospital course of patients with TCM in two large medical centers who provided care to most of the population in the conflict area.
Methods
Eight consecutive cases of emotionally triggered TCM precipitated by acts of war were retrospectively collected. We included individuals diagnosed with TCM from two medical centers (Barzilai Medical Center in Ashkelon and Soroka Medical Center in Beer Sheva) that provided care to most of the population affected by the acts of violence on October 7th and by the numerous rocket barrages during the Israel-Gaza war. Our study focused on the initial 50 days of the conflict, as this period witnessed the most intense acts of war. Furthermore, we hypothesized that the mental effects of the conflict would be greatest during the initial phases of the war, which started in a surprise attack and led to unprecedented acts of violence against Israeli civilians. The incidence of TCM during the study period was compared to control periods with the same duration, a year before the conflict.
Medical records were thoroughly reviewed and analyzed. Clinical presentation, ECG tracings, laboratory and imaging findings, and in-hospital course were monitored. The diagnosis of TCM was made in accordance with the international takotsubo diagnostic criteria (InterTAK diagnostic criteria) [7]. The Institutional review board approved the study on the basis of strict maintenance of participants’ anonymity by de-identifying during database analysis (BRZ-0101-23 and SOR-0442-23).
Results
Although a total of 13 cases were initially recruited during the first 50 days of the war (5 cases were diagnosed at Barzilai Medical Center and 8 cases were diagnosed at Soroka Medical center), a definite emotional trigger clearly associated with acts of terror was only identified in 8 patients that were included in the final analysis. A brief description of each case is presented. baseline characteristics are presented in Table 3, and ECG, echocardiographic, angiographic, and selected laboratory findings are reported in Table 4.
Case 1
An 80-year-old female presented to the emergency department (ED) after an episode of pre-syncope. On questioning, the patient revealed that few hours earlier her home was directly hit by a rocket while she was in the residential protected room. She appeared anxious but denied chest pain or dyspnea. Her medical history included hypertension and hyperlipidemia. Her vital signs were within normal limits. Treatment included beta-blockers and angiotensin receptor blocker (ARB). The patient was discharged after 5 days of admission. No adverse events were recorded.
Case 2
A 75-year-old female presented to the ED with acute chest pain and ECG showing sinus tachycardia and ST-segment elevation (STE) with hyperacute T waves. On arrival, she appeared in distress but except for tachycardia, her vital signs were normal. Several hours prior to the onset of chest pain the patient had been startled by the warning sirens that indicate an imminent rocket barrage. Emergency coronary angiography for presumed ST-segment elevation myocardial infarction (STEMI) revealed only mild irregularities. Treatment included beta-blockers and ARB. The patient had an uneventful clinical course and was discharged after 3 days of admission.
Case 3
A 76-year-old female, presented to the ED complaining of 2 hours of dyspnea. On arrival, she appeared anxious and was diaphoretic and tachypneic. Her blood oxygen saturation was 88% and a chest x-ray evidenced pulmonary congestion. An emergent coronary angiography revealed a calcified stenosis in the middle part of the right coronary artery (RCA). The patient had been repeatedly exposed to the sound of warning sirens and rockets explosions in the days before admission. Despite the significant stenosis of the RCA, the initial ECG demonstrated ST segment elevation in the antero-lateral leads, coupled with echocardiographic evidence of diffuse and severely reduced left ventricular (LV) function, did not support the occurrence of an acute coronary event. Treatment was supportive. During her stay in the intensive cardiac care unit the patient underwent coronary revascularization to the RCA. She was discharged after a total of 6 days of hospital stay.
Case 4
A 53-year-old female, smoker, with unremarkable medical history presented to the ED with chest pain, a few hours after hearing warning sirens. On arrival, her vital signs were within normal limits. The patient was treated conservatively, had an uneventful clinical course, and was discharged after 4 days.
Case 5
A 49-years old female was brought to the ED following a syncope episode. On October 7th, during the major terrorist attack on multiple urban and rural areas, armed terrorists invaded her home prompting the patient and her family to seek shelter in the residential protected room. While in hiding, she unexpectedly lost consciousness and exhibited involuntary movements. Given her history of epilepsy, it was initially presumed she was having a seizure. An ECG performed in the ED revealed brief runs of ventricular tachycardia. Shortly thereafter, she developed ventricular fibrillation. The patient underwent cardiopulmonary resuscitation and recovered. Coronary arteries were normal on angiography. She spent 2 weeks in the hospital and was discharged without neurological sequelae.
Case 6
A 60-years old female presented with chest pain. Her vital signs in the ED were within normal limits. The patient disclosed that she was deeply disturbed by the terror attack and extremely worried by the threat of war.
Case 7
A 38-years old female was admitted with chest pain and ECG showing ST-segment elevation. The patient was exposed to multiple warning sirens and rocket attacks prior to admission.
Case 8
A 81-year old female, with permanent pacemaker due to complete atrio-ventricular block was admitted with chest pain after learning that her son had been killed in battle. Her ECG at presentation revealed a ventricular paced rhythm, without ST-T changes.
Remarkedly, between October 7th to November 25th, 2023, patients diagnosed with TCM made up approximately 8.5% of all acute coronary syndrome (ACS) cases admitted to Barzilai Medical Center. In contrast, in the corresponding timeframe in 2022, only 1 patient with TCM was recorded alongside 95 ACS cases, constituting ~ 1% of the total ACS admissions (Figure 1). Interestingly, the higher incidence of TCM was accompanied by a concomitant decrease in ACS admissions. At Soroka Medical center, 8 patients were diagnosed with TCM within 50 days of the war’s outbreak in comparison to only 2 cases reported during the equivalent control period.
All patients experienced episodes of intense fear stemming from a perceived risk of annihilation, representing an exceptionally intense psychological upset. Furthermore, the perception of impending doom was not only felt at the personal levels but also at the national level. All patients were females with a median age of 61.5 (38–80) years with two patients (25%) younger than 50 years old. Clinically, chest pain was the most common presenting symptom (62.5%) whereas STE was evident in 50% of cases on the first ECG. In addition, 100% of patients had a QTc interval above 500 ms. On initial echocardiography, all patients had severely reduced LV function with the same pattern of wall motion abnormalities (WMA) – a symmetric hypo- and\or akinesis of the apical and midventricular regions and a hypercontractile basal segments (Table 5). The initial mean LV ejection fraction (LVEF) was 28%. Five patients (62.5%) experienced complications. All patients recovered and were discharged from the hospital.
Discussion
To the best of our knowledge, this is the largest study to examine the association between a major national, rather than a personal, crisis and the incidence and clinical characteristics of TCM in the general population.
Our main findings were: 1. The incidence of TCM increased substantially during the period of monitoring compared to control periods; 2. Seven patients were diagnosed within the more intense first 3 weeks of conflict whereas only one was identified at the end of the period of monitoring, despite the continuing acts of war; 3. two patients (25%) were young, <50 years old; 4. All patients had high-risk features, including severe LV dysfunction and long QTc interval (>500 ms) and five patients (62.5%) experienced complications including one case of significant acute MR, two cases of LVOTO and functional MR, one case of pulmonary edema and one case of cardiac arrest.
Despite the substantial rise in the incidence of TCM, we assume that the overall number of cases was even higher not only because TCM is generally underdiagnosed [8], but also due to the lower tendency of patients to seek medical care at times of war [9]. Hence, it is likely that TCM is one of the underlying etiologies responsible for the higher incidence of sudden cardiac death related to psychological insults among civilians during war [5,10,11,12,13].
Interestingly, seven patients presented within the first 3 weeks of the conflict, with only 1 patient detected at the end of the period of monitoring, despite the continuing acts of terror. Such distribution has been described regarding the incidence of acute MI among civilians during periods of sustained missile attacks suggesting a psychological adaptation and tolerance to repeated emotional stressors [5]. Indeed, after the initial sharp rise in TCM diagnoses we noted a decline in incidence, similar to pre-conflict levels.
Several studies have investigated the correlation between the trigger type (emotional, physical, or none) and outcomes. Patients with emotionally triggered TCM had higher LVEF at presentation, lower rate of in-hospital complications, shorter hospital stay, and lower long-term mortality rate compared with patients with TCM triggered by physical stressor or without an apparent preceding stressor [6,14,15]. However, among emotionally triggered cases, the effect on clinical presentation and outcomes of the intensity of the emotional stressor remains unknown.
In a study based on the InterTAK registry that evaluated age-related clinical features and outcomes in patients with TCM, about 10% of patients were below 50 years of age. Compared to patients > 50 years of age, younger individuals have an increased prevalence of coexisting neurological and\or psychiatric disorders, present more commonly with atypical forms of TCM and have higher rate of cardiogenic shock [16]. In our cohort, 25% of individuals were under 50 years of age and 4 patients (50%) had coexisting neurological and\or psychiatric disorders. Although speculative, age-related changes in neurologic reactivity and myocardial susceptibility to stress, particularly in individuals with concomitant neurologic and\or psychiatric conditions, may be responsible for higher prevalence of emotionally triggered TCM in patients <50 years old, as shown in our analysis [16,17].
In the current series, all patients presented with high-risk features. Such ominous clinical presentation is in contradiction to the benign phenotype reported in large cohorts of patients with emotionally triggered TCM (Table 5).

Table 5.
The clinical characteristics of emotionally triggered TCM from the GEIST registry [6].
Table 5.
The clinical characteristics of emotionally triggered TCM from the GEIST registry [6].
| Emotionally triggered TCM (910) | |
| Age, y | 70 (61-77) |
| Female sex | 859/910 (94.1) |
| Clinical presentation | |
| Chest pain | 630/818 (77) |
| Dyspnea | 225/818 (27) |
| ST-segment change | 658/805 (81.7) |
| Ballooning pattern | 790/909 (86.9) |
| Initial LVEF% | 40 (35-45) |
| In-hospital complications* | 110/910 (12.1) |
| Pulmonary edema | 55/910 (6) |
| In-hospital death | 11/910 (1.2) |
| Length of hospital stay, d | 6 (4-8) |
Data are presented as number (percentage) of patients and median (interquartile range); * death, cardiogenic shock, pulmonary edema, or stroke; GEIST German-Italian-Spanish Takotsubo; TCM takotsubo cardiomyopathy; LVEF left ventricular ejection fraction.
A correlation between the intensity of the emotional trigger and the potency of the neurobiological response is well known. Indeed, an intense and\or repetitive psychological insult can precipitate a dysfunctional stress response characterized by sympathetic overstimulation, dysregulation of the hypothalamus-pituitary-adrenal axis and abnormal immune-inflammatory response [26]. In the current study, the psychological insult was particularly intense, stemming not only from the freight of losing one’s life but also from the profound worry about the potential loss of one’s country.
Our findings suggest that intense, life-threatening, emotional stressors could precipitate a high-risk variant of TCM, potentially at a younger age and with complicated clinical course.
Additional evidence is needed to corroborate our findings.
Conclusions
The incidence of stress-induced cardiomyopathy is substantially increased among civilians living in areas of active armed conflict. Importantly, a severe national crisis may precipitate a form of TCM with high-risk features, at a younger age, and with potentially poor outcomes in comparison to TCM induced by emotional stressors related to personal calamities.
Abbreviations
TCM takotsubo cardiomyopathy; ACS Acute coronary syndrome; LV Left ventricle, WMA wall motion abnormalities, MR mitral regurgitation
References
- Tawakol, A.; Ishai, A.; AP Takx, R.; Figueroa, A.L.; Ali, A.; Kaiser, Y.; A Truong, Q.; Solomon, C.J.; Calcagno, C.; Mani, V.; et al. Relation between resting amygdalar activity and cardiovascular events: a longitudinal and cohort study. Lancet 2017, 389, 834–845, . [CrossRef]
- Batty, G.D.; Russ, T.C.; Stamatakis, E.; Kivimäki, M. Psychological distress and risk of peripheral vascular disease, abdominal aortic aneurysm, and heart failure: Pooling of sixteen cohort studies. Atherosclerosis 2014, 236, 385–388, . [CrossRef]
- Nabi, H.; Kivimäki, M.; Batty, G.D.; Shipley, M.J.; Britton, A.; Brunner, E.J.; Vahtera, J.; Lemogne, C.; Elbaz, A.; Singh-Manoux, A. Increased risk of coronary heart disease among individuals reporting adverse impact of stress on their health: the Whitehall II prospective cohort study. Eur. Hear. J. 2013, 34, 2697–2705, . [CrossRef]
- Lampert, R. Mental Stress and Ventricular Arrhythmias. Curr. Cardiol. Rep. 2016, 18, 118, . [CrossRef]
- Meisel SR, Kutz I, Dayan KI, Pauzner H, Chetboun I, Arbel Y, et al. Effect of Iraqi missile war on incidence of acute myocardial infarction and sudden death in Israeli civilians. Lancet. 1991;338(8768):660-1.
- Pätz, T.; Santoro, F.; Cetera, R.; Ragnatela, I.; El-Battrawy, I.; Mezger, M.; Rawish, E.; Andrés-Villarreal, M.; Almendro-Delia, M.; Martinez-Sellés, M.; et al. Trigger-Associated Clinical Implications and Outcomes in Takotsubo Syndrome: Results From the Multicenter GEIST Registry. J. Am. Hear. Assoc. 2023, 12, e028511, . [CrossRef]
- Ghadri JR, Wittstein IS, Prasad A, Sharkey S, Dote K, Akashi YJ, et al. International Expert Consensus Document on Takotsubo Syndrome (Part I): Clinical Characteristics, Diagnostic Criteria, and Pathophysiology. Eur Heart J. 2018;39(22):2032-46.
- Medina de Chazal H, Del Buono MG, Keyser-Marcus L, Ma L, Moeller FG, Berrocal D, et al. Stress Cardiomyopathy Diagnosis and Treatment: JACC State-of-the-Art Review. J Am Coll Cardiol. 2018;72(16):1955-71.
- Ekzayez, A.; Ahmad, Y.A.; Alhaleb, H.; Checchi, F. The impact of armed conflict on utilisation of health services in north-west Syria: an observational study. Confl. Heal. 2021, 15, 91, . [CrossRef]
- Pignalberi, C.; Ricci, R.; Santini, M. [Psychological stress and sudden death]. Ital Heart J Suppl. 2002, 3, 1011–21.
- Jawad, M.; Hone, T.; Vamos, E.P.; Roderick, P.; Sullivan, R.; Millett, C. Estimating indirect mortality impacts of armed conflict in civilian populations: panel regression analyses of 193 countries, 1990–2017. BMC Med. 2020, 18, 266, . [CrossRef]
- Gold, L.S.; Kane, L.B.; Sotoodehnia, N.; Rea, T. Disaster Events and the Risk of Sudden Cardiac Death: A Washington State Investigation. Prehospital Disaster Med. 2007, 22, 313–317, . [CrossRef]
- Wang Y, Xia L, Shen X, Han G, Feng D, Xiao H, et al. A New Insight Into Sudden Cardiac Death in Young People: A Systematic Review of Cases of Takotsubo Cardiomyopathy. Medicine (Baltimore). 2015;94(32):e1174.
- Uribarri, A.; Núñez-Gil, I.J.; Conty, D.A.; Vedia, O.; Almendro-Delia, M.; Cambra, A.D.; Martin-Garcia, A.C.; Barrionuevo-Sánchez, M.; Martínez-Sellés, M.; Raposeiras-Roubín, S.; et al. Short- and Long-Term Prognosis of Patients With Takotsubo Syndrome Based on Different Triggers: Importance of the Physical Nature. J. Am. Hear. Assoc. 2019, 8, e013701, . [CrossRef]
- Ghadri JR, Kato K, Cammann VL, Gili S, Jurisic S, Di Vece D, et al. Long-Term Prognosis of Patients With Takotsubo Syndrome. J Am Coll Cardiol. 2018;72(8):874-82.
- Cammann, V.L.; Szawan, K.A.; Stähli, B.E.; Kato, K.; Budnik, M.; Wischnewsky, M.; Dreiding, S.; Levinson, R.A.; Di Vece, D.; Gili, S.; et al. Age-Related Variations in Takotsubo Syndrome. J. Am. Coll. Cardiol. 2020, 75, 1869–1877, . [CrossRef]
- Burger, I.A.; Lohmann, C.; Messerli, M.; Bengs, S.; Becker, A.; Maredziak, M.; Treyer, V.; Haider, A.; Schwyzer, M.; Benz, D.C.; et al. Age- and sex-dependent changes in sympathetic activity of the left ventricular apex assessed by 18F-DOPA PET imaging. PLOS ONE 2018, 13, e0202302, . [CrossRef]
- Chu B, Marwaha K, Sanvictores T, Ayers D. Physiology, Stress reaction. StatPearls [Internet]: Treasure Island (FL): StatPearls publishing; 2022.
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N Engl J Med. 2015;373(10):929-38.
- Gil, I.J.N.; Andrés, M.; Delia, M.A.; Sionis, A.; Martin, A.; Bastante, T.; Soriano, J.G.C.; Vicente, J.A.L.; Sucarrats, S.G.; Flecha, A.S.-G. Characterization of Tako-tsubo Cardiomyopathy in Spain: Results from the RETAKO National Registry. Rev. Española Cardiol 2015, 68, 505–512, doi:10.1016/j.rec.2014.07.026.
- Imori, Y.; Kato, K.; Cammann, V.L.; Szawan, K.A.; Wischnewsky, M.; Dreiding, S.; Würdinger, M.; Schönberger, M.; Petkova, V.; Niederseer, D.; et al. Ethnic comparison in takotsubo syndrome: novel insights from the International Takotsubo Registry. Clin. Res. Cardiol. 2021, 111, 186–196, . [CrossRef]
- Murakami, T.; Yoshikawa, T.; Maekawa, Y.; Ueda, T.; Isogai, T.; Sakata, K.; Nagao, K.; Yamamoto, T.; Takayama, M. Gender Differences in Patients with Takotsubo Cardiomyopathy: Multi-Center Registry from Tokyo CCU Network. PLOS ONE 2015, 10, e0136655, . [CrossRef]
- Brinjikji, W.; El-Sayed, A.M.; Salka, S. In-hospital mortality among patients with takotsubo cardiomyopathy: A study of the National Inpatient Sample 2008 to 2009. Am. Hear. J. 2012, 164, 215–221, . [CrossRef]
- Santoro, F.; Gil, I.J.N.; Stiermaier, T.; El-Battrawy, I.; Guerra, F.; Novo, G.; Guastafierro, F.; Tarantino, N.; Novo, S.; Mariano, E.; et al. Assessment of the German and Italian Stress Cardiomyopathy Score for Risk Stratification for In-hospital Complications in Patients With Takotsubo Syndrome. JAMA Cardiol. 2019, 4, 892–899, . [CrossRef]
- Santoro, F.; Stiermaier, T.; El-Battrawy, I.; Guastafierro, F.; Guerra, F.; Novo, G.; Mariano, E.; Montisci, R.; Tarantino, N.; Caldarola, P.; et al. P4391In-hospital complications in patients with takotsubo syndrome: a novel score from a cohort of 1002 patients from the multi-center international GEIST registry. Eur. Hear. J. 2018, 39, . [CrossRef]
- Möller, C.; Eitel, C.; Thiele, H.; Eitel, I.; Stiermaier, T. WITHDRAWN: Ventricular Arrhythmias in Patients with Takotsubo Syndrome. J. Arrhythmia 2018, 34, 369–375. [CrossRef]
Figure 1.
ACS admissions at Barzilai Medical Center between October 7th and November 25th, 2023, and the corresponding period in 2022. (a) Quotative comparison of ACS cases arrived at the ER between October 7th and November 25th, 2022, vs 2023. (b) percentage representation of ACS cases. ACS acute coronary syndrome; TCM takotsubo cardiomyopathy; UA unstable angina; STEMI ST-elevation myocardial infarction; NSTEMI non- ST-elevation myocardial infarction.
Figure 1.
ACS admissions at Barzilai Medical Center between October 7th and November 25th, 2023, and the corresponding period in 2022. (a) Quotative comparison of ACS cases arrived at the ER between October 7th and November 25th, 2022, vs 2023. (b) percentage representation of ACS cases. ACS acute coronary syndrome; TCM takotsubo cardiomyopathy; UA unstable angina; STEMI ST-elevation myocardial infarction; NSTEMI non- ST-elevation myocardial infarction.
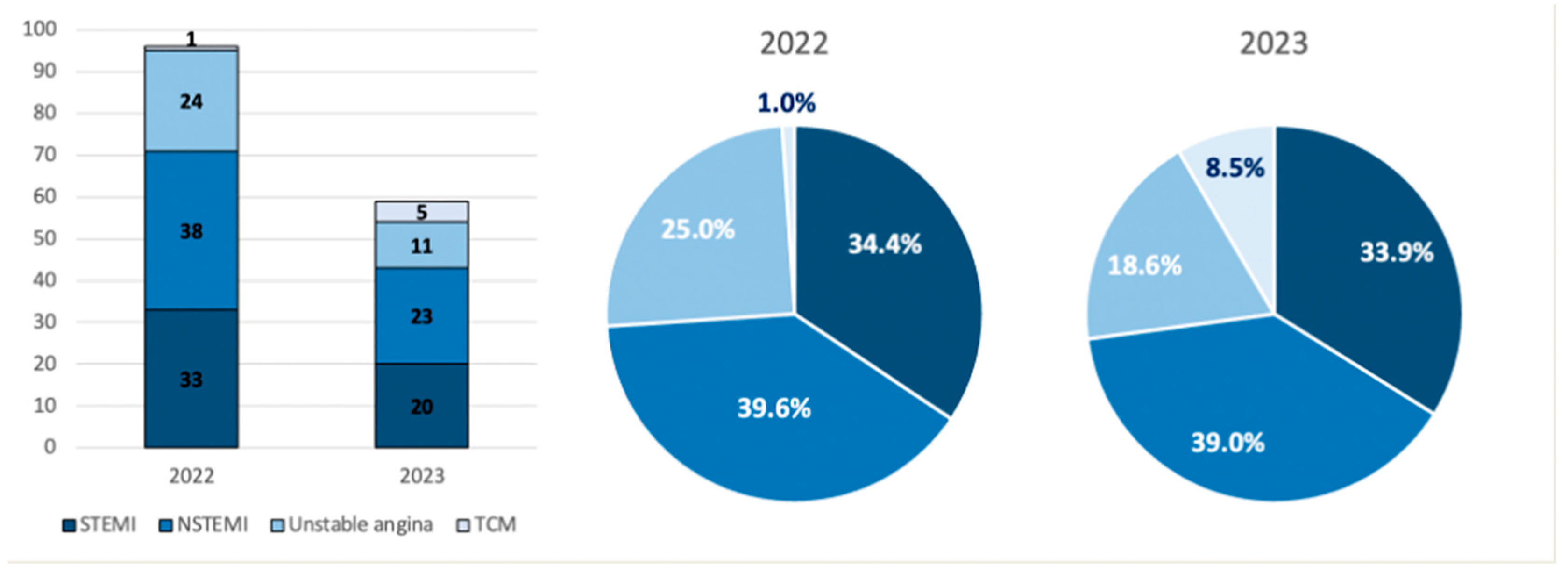
Table 1.
Clinical features of Takotsubo cardiomyopathy in selected cohorts.
| Baseline and clinical characteristics* | Pätz T [11] | Templin C [15] | Núñez Gil, I. J. [16] | Imori Y – European Cohort [17] |
Imori Y - Japanese Cohort [17] |
Tokyo CCU network database [18] |
| Patients N | 2492 | 1750 | 202 | 1670 | 503 | 368 |
| Age (years; mean) | 72 | 66.8 | 70 | 68 | 72,6 | 76 |
| Women | 88.5 | 89.8 | 90.1 | 91.6 | 81.5 | 77.1 |
| No trigger | 28.9 | 28.5 | 27.2 | 29.2 | 35.4 | 36.1 |
| Physical trigger | 34.4 | 36 | 19.8 | 32 | 45.5 | 35.6 |
| Emotional trigger | 36.7 | 27.7 | 50 | 31.5 | 17.5 | 28.3 |
| Emotional & physical triggers | - | 7.8 | 3 | 7.3 | 1.6 | - |
| Presenting symptom | ||||||
| Chest pain | 59.9 | 75.9 | 80.2 | - | - | 48.6 |
| Dyspnea | 35.8 | 46.9 | 44.5 | - | - | 33.4 |
| Syncope | - | 7.7 | 8.9 | - | - | |
| ST-segment change | 81.9 | 51.4 | 60.9** | 45** | 70.3** | 73.9 |
| Echocardiographic findings | ||||||
| Initial LVEF % (mean) | 40 | 40.7 | 44 | 41.8 | 44.5 | 50 |
| Apical ballooning | 85.8 | 81.7 | - | 70 | 71.2 | 90.8 |
| midventricular | 11.9 | 14.6 | - | - | - | - |
| Basal | 1.9 | 2.2 | - | - | - | - |
| Focal | 0.3 | 1.5 | - | - | - | - |
| Normal or near normal coronary arteries % | 90.5 | 84.7 | 100 | - | - | 91.6 |
* Data is presented as percentage unless indicated otherwise. ** refers to ST-segment elevation only. LVEF left ventricular ejection fraction.
| Variable | Frequency (%) |
| In hospital complications | 20-23 |
| In hospital death | 4.2 |
| Pulmonary edema | 6-9 |
| Ventricular arrhythmias | 4-9 |
| Invasive ventilation | 6-6.4 |
| Cardiogenic shock | 9-10 |
| LV thrombus | 2.7 |
| Stroke | 1.5-2.2 |
TCM takotsubo cardiomyopathy; LV left ventricle.
Table 3.
Patients’ baseline characteristics.
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8 | |
| Gender | F | F | F | F | F | F | F | F |
| Age | 80 | 75 | 76 | 53 | 81 | 49 | 60 | 38 |
| Smoking | No | No | Yes | Yes | No | No | No | No |
| Diabetes mellitus | No | No | No | No | Yes | No | Yes | No |
| Hypertension | Yes | Yes | No | No | Yes | No | Yes | No |
| Dyslipidemia | Yes | Yes | Yes | No | Yes | No | Yes | No |
| Obesity | No | No | No | No | Yes | No | Yes | Yes |
| COPD | No | No | Yes | No | No | No | No | No |
| Psychiatric and\or neurologic disorders | No | Dementia | No | No | No | Anxiety, Epilepsy | Schizophrenia | Wernicke’s encephalopathy |
| Ischemic heart disease | No | No | No | No | No | No | No | No |
| Other | No | No | No | No | CAVB, PM | No | No | No |
COPD chronic obstructive pulmonary disease; CAVB complete atrioventricular block; PM pacemaker.
Table 4.
Patients’ clinical characteristics.
| Patient 1 | Patient 2 | Patient 3 | Patient 4 | Patient 5 | Patient 6 | Patient 7 | Patient 8 | |
| Trigger | Emotional | Emotional | Emotional | Emotional | Emotional | Emotional | Emotional | Emotional |
| Presenting symptom | Pre-syncope | Dyspnea | Chest pain | Chest pain | Chest pain | Syncope | Chest pain | Chest pain |
| ECG at presentation | ||||||||
| ST-segment | STE lateral leads | STE antero-lateral leads | STE antero-lateral leads; Hyperacute T | TWI in lateral leads | Ventricular pacing | TWI antero-lateral leads | No ST-T changes | STE antero-lateral leads |
| QTc (ms) | 450 | 449 | 456 | 513 | 500 | 520 | 520 | 532 |
| ECG at 48 hours | ||||||||
| ST-segment | Diffuse TWI | Diffuse Subtle STE and TWI | Diffuse subtle STE and bi-phasic T waves | Diffuse TWI | Ventricular pacing | Diffuse TWI | No ST-T | STE antero-lateral leads |
| QTc (ms) | 512 | 589 | 501 | 507 | 520 | 419 | 460 | 506 |
| Echocardiography at presentation | ||||||||
| EF Simpson % | 23% | 28% | 30% | 30% | 15-20% | 20% | 35% | 30% |
| Functional MR grade | Mild-moderate | Moderate | Moderate-severe | Mild-moderate | Mild | Mild-moderate | Moderate-severe | Moderate |
| LVOTO (rest gradient, mmHg) | No | Yes (46) | Yes (53) | No | No | No | No | Yes (44) |
| Hypokinesis pattern | Mid-Apical | Mid-Apical | Mid-Apical | Mid-Apical | Mid-Apical | Mid-Apical | Mid-Apical | Mid-Apical |
| Echocardiography at follow up | ||||||||
| EF Simpson % | 45 | 39 | 45 | 44 | 55 | 55-60 | 40-45 | 65 |
| Functional MR grade | Mild | Mild | Moderate | Mild | No | No | No | No |
| Cardiac magnetic resonance imaging | No | No | No | No | No | No myocardial LGE | No myocardial Edema | No |
| Initial Hs-TnT ng\L | 109 | 106 | 346 | 348 | 484 | 49 | 37 | 200 |
| Peak Hs-TnT ng\L | 830 | 611 | 445 | 372 | 1120 | 59 | 70 | 200 |
| CK U\L | 224 | 176 | 231 | 218 | 119 | 68 | 54 | 48 |
| Pro BNP pg\mL | - | 8486 | - | 2595 | >35,000 | 8145 | 1925 | 10800 |
| CRP-s-B mg\L | 12.90 | 2.3 | 7.40 | 8.2 | 275 | 6.8 | 6.8 | 8.1 |
| Coronary artery disease | NOC | No | RCA 80% stenosis | No | No | No | No | No |
| Ballooning on angiography | - | - | - | - | Yes | - | - | - |
| Revascularization during admission | - | - | Yes | - | No | - | - | - |
| Length of hospital stay, days | 7 | 4 | 7 | 5 | 9 | 14 | 5 | 11 |
COPD chronic obstructive pulmonary disease; ECG electrocardiography; STE ST-segment elevation; TWI T-wave inversion; EF ejection fraction; MR mitral regurgitation; LVOTO Left ventricular outflow tract obstruction; Hs-TnT high sensitivity troponin T; LGE late gadolinium enhancement; CK creatine kinase; BNP brain natriuretic peptide; RCA right coronary artery; NOC non-obstructive coronary disease.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



