
Submitted:
29 March 2024
Posted:
29 March 2024
You are already at the latest version
Abstract
(1) Background: Globally, about 600 million people are afflicted with diabetes, and one of its most prevalent complications is neuropathy, a debilitating condition. At present, the exploration of novel therapies for alleviating diabetic neuropathy-associated pain is genuinely captivating, considering that current therapeutic options are characterized by poor efficacy and significant risk of side effects. In the current research, we evaluated the antihyperalgesic effect of sildenafil (phosphodiesterase-5 inhibitor) – metformin (antihyperglycemic agent) combination and its impact on biochemical markers in alloxan-induced diabetic neuropathy in rats; (2) Methods: The study comprised a cohort of 70 diabetic rats and 10 non-diabetic rats which were submitted to hot, cold, and tactile stimulus tests. Morover, we investigated the influence of this combination on TNF-α, IL-6 nitrites and thiols levels in brain and liver tissues; (3) Results: The results demonstrated that all sildenafil-metformin combinations decreased the pain sensitivity in von Frey test, Hot-plate test and Cold-plate test. Furthermore, alterations in nitrites and thiols concentrations and pro-inflammatory cytokines (specifically TNF-α and IL-6) were noted following a 15-day regimen of various sildenafil-metformin combinations. (4) Conclusions: The combination of sildenafil and metformin has a synergistic effect in alleviating pain in alloxan-induced diabetic neuropathy rats. Additionally, the combination effectively decreased inflammation, inhibited the rise in NOS activity, and provided protection against glutathione depletion.
Keywords:
diabetic neuropathy
; sildenafil
; metformin
; antihyperalgesic
; IL-6
; TNF-α
1. Introduction
Diabetes and its complications are growing challenges for healthcare systems around the world. Diabetes affects about 600 million people globally, and by 2045, that figure is expected to rise to 700 million [1].
Neuropathy is a frequently occurring complication of diabetes. This pathology is characterized by high morbidity and poor quality of life [2,3]. According to recent statistics, the incidence of neuropathy is higher in people with type-2 diabetes [4]. In addition, another recent study including 25,710 type-2 diabetic patients from China revealed a percentage of 57.2% diabetic neuropathy (DN) among them [5]. Moreover, a study including 3000 diabetics from 16 countries reported a 28% prevalence of DN [6]. Aldana et al estimated a prevalence of DN of 46.5% in a study including 8 countries from Latin America [7]. In Europe, the prevalence of this pathology ranges from 6% to 34% among diabetics [8].
The mechanisms underlying the onset and progression of DN remain poorly understood, resulting in undertreatment [9]. The present literature on the pathophysiology of DN demonstrates the involvement of oxidative stress, the polyol and hexosamine pathways, proinflammatory cytokines, the sodium and calcium channels, microvascular alterations, and insulin signaling pathways [4,10].
Over time, numerous preclinical and clinical studies have provided evidence that systemic inflammation is involved in the pathogenesis of DN. Both TNF-α (tumor necrosis factor) and IL-6 (interleukin-6) are pro-inflammatory cytokines whose production is increased in patients with DN [4,11]. Due to chronic hyperglycemia, nitric oxide synthase (NOS) depletion occurs, which consequently leads to free radical generation and an increase in the production of nitric oxide (NO) [12]. By altering the injured peripheral axons, NO plays an important role in the development of DN [4]. On the other hand, oxidative stress mediated by free radicals also has implications in the progression of diabetes and its complications and both types of diabetes demonstrated low levels of protein thiols, these decreases being attributed to metabolic and inflammatory changes [13,14].
Currently, besides the high risk of side effects, therapeutic strategies have limited success in reducing the pain caused by DN [3]. Considering these, the discovery of new treatments is of real interest. Sildenafil, a PDE5 (phosphodiesterase 5) inhibitor demonstrated its ability to reduce pain from neuropathy by increasing cGMP (cyclic guanosine monophosphate) which consequently enhances the production of γ-aminobutyric acid (GABA) [15,16]. Furthermore, chronic hyperglycemia produces an increase in the level of PDE5, and sildenafil, by inhibiting this enzyme, contributes to the enhancement of DN [17].
On the other hand, metformin, besides its antihyperglycemic effect, has also demonstrated an antinociception action in several studies. Thus, it alleviates pain through multiple mechanisms, including AMPK (adenosine monophosphate protein kinase) activation, mTOR (protein kinase complex mechanistic target of rapamycin) complex 1 inhibition or microglia and astrocyte activation in the spinal dorsal horn [18,19].
In this study, we proposed to evaluate the antihyperalgesic effect of the combination of sildenafil and metformin in an animal model of DN in rats and its influence on biochemical markers (TNF-α, IL-6, nitrites, and thiols levels). In previous research, we demonstrated the antinociceptive action of sildenafil and metformin in an animal model of DN in mice, in which DN was induced by 3 consecutive doses of 150 mg·kg−1 alloxan [20].
Currently, the treatment is only successful for a minority of patients, with less than half experiencing positive results. Additionally, the medications prescribed according to current guidelines often lead to severe side effects [21]. Moreover, it was reported that there was a decrease in the efficiency of drugs from all therapeutic classes, which consequently led to an increase in the number of patients needing to be treated [22]. As a consequence, combination therapy is considered to be preferred among clinicians in alleviating pain from DN [23,24,25,26]. This rationale is based on two theories: 1) a phenotypically guided treatment improves symptomatic control (it is suggested that different clinical signs and symptoms may give clues to the mechanisms that induced the pain) and offers the possibility of a treatment approach based on the physiopathology of pain; 2) targeting multiple mechanisms involved in neuropathy by administering a combination of active substances from different therapeutic classes which is considered to be superior to monotherapy [27,28]. All things considered, combined therapy may be a better and more efficient option for reducing pain from DN.
2. Results
2.1. Blood Glucose Levels
Following the administration of alloxan to induce diabetes, alterations in blood glucose levels were detected when comparing the ND group to the diabetic groups. This comparison was conducted using a univariate analysis of variance (ANOVA), yielding a significant F value of 32.09 (p < 0.0001). The results are illustrated in Figure 1A. The results of our study demonstrated statistically significant elevations in the measured values across all groups with diabetes, as compared to the non-diabetic group (p < 0.05, Figure 1A).
Significant variations in blood glucose levels across groups were seen after 7 days of therapy (univariate ANOVA, F=48.89, p< 0.0001, Figure 1B). All diabetic groups maintained a high level of blood glucose, except the S2.5+M300 and S3+M500 groups, which recorded significant decreases in blood glucose when compared to the D group (p < 0.01; p < 0.001, Figure 1B.).
At the end of the experiment, the blood glucose concentration was significantly changed following the treatment (univariate ANOVA, F=51.87, p< 0.0001, Figure 1C). We noticed significant decreases for all 3 groups treated with sildenafil-metformin combinations (p < 0.001, Figure 1C). Moreover, the groups S2.5+M300 and S3+M500 demonstrated the best glycemic control, with a percentage of lowering blood glucose levels of 62.53% and 65.35%, respectively, compared to the initial values (Figure 1D).
2.2. Tests for the Evaluations of antihyperalgesic Effect
2.2.1. Heat Hypersensitivity
The findings from our study indicate variations in pain reaction latency observed in the Hot-plate test when comparing the ND group to all diabetes groups before medication administration (univariate ANOVA, F=19.98, p < 0.0056, Figure 2. A). The diabetes groups had statistically reduced pain response values in comparison to the ND group (p < 0.01, Figure 2A).
After 7 days of treatment, we noted changes in the pain reaction latency (univariate ANOVA, F=21.69, p < 0.0029, Figure 2B). The G90 and G150 groups recorded significant increases in pain reaction latency when compared to the D group (p < 0.01, p < 0.001, Figure 2B). Group G150 demonstrated the most pronounced antihyperalgesic effect, with a pain sensitivity reduction effect of 97.52%. Regarding the groups treated with the sildenafil-metformin combinations, the S2.5+M300 and S3+M500 groups showed significant decreases in pain sensitivity when compared to the D group, with effects of 88.9% and 92.24%, respectively (p < 0.01, Figure 2B).
After administering the treatments for 14 consecutive days, our research revealed changes regarding the pain perception parameter (univariate ANOVA, F=27.85, p<0.0002, Figure 2. C). Administration of gabapentin at the dose of 150 mg·kg−1 produced the strongest antihyperalgesic effect of 97.52%, followed by gabapentin at the dose of 90 mg·kg−1 with an effect of increasing pain reaction latency by 78.4% versus the D group (p < 0.001, p < 0.05, Figure 2C). The S2.5+M300 and S3+M500 groups demonstrated significant decreases in pain sensitivity when compared to the D group, with comparable effects to the G150 group (p < 0.01, Figure 2C).
2.2.2. Cold Hypersensitivity
The Cold-plate test at -5℃ showed differences between the ND group and the diabetic groups (univariate ANOVA, F=22.92, p < 0.0018, Figure 2D), with increased pain sensitivity in the diabetic groups when compared to the ND group (p < 0.05, Figure 2D).
The administration of treatment produced variations among the groups, both after 8 days (univariate ANOVA, F=23.5, p < 0.0014, Figure 2E) and after 15 days of treatment (univariate ANOVA, F=30.88, p < 0.0001, Figure 2F). Thus, among the groups treated with gabapentin, only the G90 and G150 groups recorded significant increases in pain reaction latency versus the D group after 7 days of treatment (p < 0.001, p < 0.05, Figure 2E). At the end of the experiment, the highest antihyperalgesic effect was demonstrated by the G150 group (280.15%), followed by the G90 group (228.35%).
Among the sildenafil-metformin combinations, both after 8 days and after 15 days of treatment, only the S2.5+M300 and S3+M500 groups significantly reduced pain sensitivity when compared to the D group (p < 0.05, Figure 2E-F). The most striking effect was shown by the S3+M500 group in the 2 moments of the determination (177.1%, respectively 267.78%), followed by the S2.5+M300 group with an effect of reducing the pain sensitivity of 145.57% and 165.72%, respectively when compared to the D group. In addition, the S3+M500 group demonstrated pain reaction latency-increasing effects comparable to those of the G150 group after 15 days of treatment (267.78% vs. 280.15%).
2.2.3. Tactile Hypersensitivity
After inducing diabetes, an initial test was performed before administering the therapy, and variances among groups were noticed (ANOVA, F=2.26, p < 0.039, Figure 3A). Our research revealed that the diabetic groups showed significant increases in pain sensitivity when compared to the ND group (p < 0.05, Figure 3A).
Following the administration of the treatment, changes were detected after 7 days (ANOVA, F=20.61, p < 0.0044, Figure 3B), as well as at the end of the experiment (ANOVA, F=18.67, p < 0.0093, Figure 3C). Among the groups treated with gabapentin, only the group that received the dose of 150 mg·kg−1 recorded a significant decrease in tactile sensitivity when compared to the D group after 7 days of treatment (p < 0.05, Figure 3B). A comparable effect was demonstrated by the S3+M500 group (p < 0.05, Figure 3B), with a pain sensitivity reduction effect of 63.99%, compared to 66.88% in the G150 group.
After 14 days of treatment, the G90 and G150 groups demonstrated significant increases in the 50% withdrawal threshold in the von Frey test when compared to the D group (p < 0.01, Figure 3C). The most pronounced antihyperalgesic effect was demonstrated by the group treated with a dose of 150 mg·kg−1 of gabapentin (79.18%). On the other hand, our research highlighted the fact that the S2.5+M300 and S3+M500 combinations significantly reduced pain sensitivity when compared to the D group, with effects of 71.18% and 63.25%, respectively (p < 0.05, Figure 3C).
2.3. Biochemical Assay of Rat Brain and Liver Homogenates
2.3.1. Assessment of TNF-α and Il-6
Considering the cytotoxic effects of alloxan-induced diabetes on multiple organs, such as the brain, pancreas, liver, and kidney [29], we measured the levels of pro-inflammatory cytokines TNF-α and IL-6 in the brain and liver tissues after the experiment was finished. Furthermore, our aim was to investigate if the combination of sildenafil and metformin could efficiently reduce the concentration of these cytokines in tissues.
Regarding the level of TNF-α, the ANOVA test revealed significant variations among the groups, both in the brain tissues (F = 4.156, p = 0.0018, Figure 4A), and in the liver tissues (F = 26.15, p< 0.0001, Figure 4B). The D group and the G30 group showed significant increases when compared to the ND group, while all the other diabetic groups reduced the level of TNF-α, with significantly lower values for the G90 and S3+M500 groups in the brain tissue when compared to the D group (p <0.05, Figure 4A), with a percentage of 75.39% and 94.4%, respectively. On the other hand, in liver tissues, TNF-α concentration was markedly increased in the D group, while the G90, G150, S2.5+M300, and S3+M500 groups significantly reduced the level when compared to the D group ( p <0.05, Figure 4B).
Following the biochemical analysis of brain tissue samples (ANOVA, F=9.553, p< 0.0001, Figure 4C), and liver tissue samples (ANOVA, F=27.88, Figure 4D) significant variations of IL-6 levels were observed after 15 days of treatment. Thus, in both brain and liver tissues, we noted significant increases for the D group, G30 group, and S2+M100 group when compared to the group (p < 0.05, Figure 4C-D). IL-6 production was significantly decreased following treatment with the dose of 150 mg·kg−1 of gabapentin and the S2.5+M300 and S3+M500 combinations when compared to the D group in brain tissues (p <0.05, Figure 4C). On the other hand, in liver tissues, the administration of gabapentin in doses of 90 mg·kg−1 and 150 mg·kg−1, but also of S2.5+M300 and S3+M500 combinations significantly reduced the level of IL-6 when compared to the D group (p < 0.05, Figure 4D), with decreases of 67.08%, 72.29%, 39.95%, and 57.15%, respectively.
2.3.2. Assessment of NOS Activity
Besides pro-inflammatory cytokines, we also evaluated the concentration of nitrites and total nitrites as end products of NOS in brain and liver homogenates, seeing that iNOS (inducible nitric oxide synthase) produces cellular toxicity in many systems [30].
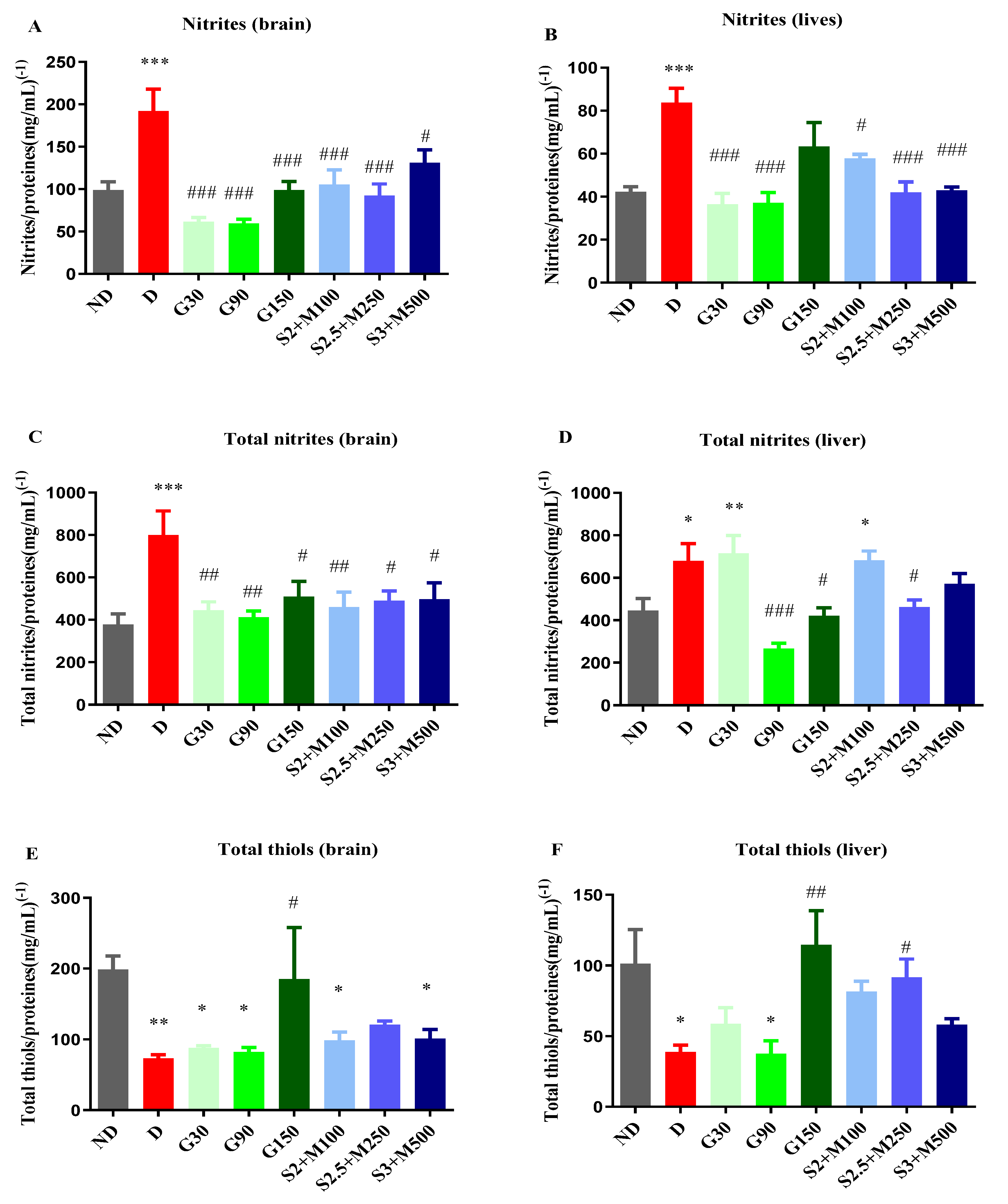
The unifactorial ANOVA test revealed significant differences between groups in terms of nitrites concentration in the brain tissues (F=8.667, p < 0.0001, Figure 5A) and the liver tissues (F=7.496, p < 0.0001, Figure 5B), but also regarding the concentration of total nitrites both in the brain tissues (F=3.562, p=0.0045, Figure 5C), and in the liver tissues (F=7.912, p < 0.0001, Figure 5D).
Regarding the concentration of nitrites, the D group recorded significant increases when compared to the ND group both in the brain and in the liver tissues (p < 0.001, Figure 5C-D). All diabetic groups that received treatment markedly reduced the concentration of nitrites in the brain tissue (p < 0.05, Figure 5A), while in the liver tissues, except the G150 group, all treated diabetic groups demonstrated significant decreases in nitrites when compared to the D group (p <0.05, Figure 5B).
In brain tissues, the concentration of total nitrites was significantly increased for the D group when compared to the ND group, while all other diabetic groups had significantly decreased total nitrites concentrations when compared to the D group (p < 0.05, Figure 5C). In liver tissues, the D group, G30 group, and S2+M100 combination recorded significantly increased levels when compared to the ND group (p <0.05, Figure 5D). The concentration of total nitrites was markedly reduced for the G90 and G150 groups, but also for the S2.5+M300 combination, with decreases of 60.87%, 38.13%, and 31.92%.
2.3.3. Assessment of Total Thiols
After 15 days of treatment, the concentration of total thiols was also evaluated in the brain and liver tissues.
The biochemical analysis showed significant variations in the concentration of total thiols among groups both in the brain tissues (univariate ANOVA, F= 3.535, p < 0.0053, Figure 5E), and in the liver tissues (univariate ANOVA, F= 4.517, p=0.053, Figure 5F). The D group showed significant decreases in the concentration of total thiols reported as glutathione equivalents in both liver and brain tissues (p < 0.05, Figure 5E-F). Among the groups that received treatment, all sildenafil-metformin combinations increased the concentration of total thiols, but only for the S2.5+M300 group, this increase was statistically significant and only in liver tissues when compared to the D group, with an increasing percentage of 136.57% (p < 0.05, Figure 5F).
Among the groups treated with different doses of gabapentin, only the G150 group produced significant increases in both brain and liver tissues when compared to the D group (p < 0.01, Figure 5 E-F).
3. Discusions
The objective of this research was to investigate the pain-relieving properties of using sildenafil and metformin in combination in rats with DN induced by alloxan. Furthermore, we assessed whether this combination influenced the levels of pro-inflammatory cytokines, nitrites, and thiols in the brain and liver tissues. Our previous study showed that the administration of sildenafil and metformin resulted in reduced sensitivity to pain in alloxan-induced DN mice. This effect was observed after 14 days of therapy and was evident in both cold and hot stimulus tests [20].
Diabetes commonly leads to erectile dysfunction (ED), which is a prevalent condition affecting approximately 75% of diabetic males. Furthermore, prior studies suggest that ED is significantly more prevalent in males with diabetes compared to those who are in good condition [31]. Sildenafil is a first-line therapeutic agent for ED, and its usefulness in enhancing the quality of life of diabetic men with ED is well documented [32]. Prior research suggests that a range of 57% to 74% of men with diabetes observed an improvement in ED following therapy with a PDE5 inhibitor [33].
Metformin has been widely recognized for decades as first line therapy for managing blood sugar levels in patients with type-2 diabetes, as indicated by the current guidelines (American Diabetes Association and the European Association for the Study of Diabetes) [34]. Considering that these two drugs are commonly prescribed for type-2 diabetic patients with ED, we aimed to investigate whether their combination could potentially alleviate neuropathy, which is another significant complication of diabetes.
In this study, we administered a single dose of 130 mg·kg−1 alloxan to develop DN. This approach is frequently employed to investigate the pathophysiology of diabetes and its associated consequences. This method is inexpensive, easily replicable, and yields a higher percentage of diabetic animals [35]. Previous studies have shown that continuous high blood sugar levels lead to oxidative stress in animals with diabetes, which in turn relates to increased sensitivity to pain [36]. Our results are in accordance with this observation, with the D group demonstrating an increase in pain sensitivity in the Hot-plate, Cold-plate, and von Frey tests during this experiment. In addition, the D group and all diabetic groups treated with gabapentin maintained high blood glucose levels, while sildenafil-metformin combinations significantly decreased the blood glucose level, due to the antihyperglycemic effect of metformin, when compared to the ND group during the 15 days of the experiment.
The ability of metformin to alleviate pain was demonstrated in several studies. One of the main mechanisms implicated in the antinociceptive activity of metformin is the activation of AMPK, which consequently activates NEDD4-2 (neuronal precursor cell expressed developmentally downregulated-4 type 2), a protein ligase that downregulates the currents of the ENaC (epithelial sodium channel) [37]. Mia et al. demonstrated this mechanism of action also for potassium channels [38]. On the other hand, Brownlee et al. suggested that metformin is capable of removing a metabolite that is increased in diabetes and is associated with neuropathies, called methylglyoxal [39,40]. Another study showed that metformin alleviates pain from neuropathy by inhibiting mTOR (mammalian target of rapamycin) and reducing the activation of microglia [41]. According to Byrne et al., the antihyperalgesic effect of metformin is not completely related to its hypoglycemic action, because it was able to reduce pain sensitivity in mechanical withdrawal threshold in fructose-treated rats [42]. Melemedjian et al. experimentally demonstrated that metformin administered to mice after spared nerve injury reversed tactile allodynia [43], while Mao-Ying et al. showed this drug can prevent mechanical and thermal hypersensitivity in rodents after spinal cord injury [44]. Administered to rats, metformin reversed the activation of astrocytes in the spinal dorsal horn and reduced the hypersensitivity [19].
Sildenafil exerts its antihyperalgesic effect via PDE5 inhibition, which consequently leads to an accumulation of cGMP (cyclic guanosine monophosphate). Patil et al. suggested that sildenafil administered to rats with nerve injury activates the NO-cGMP pathway, which modulates the nociceptive responses in spinal dorsal horn neurons in animal models of neuropathic pain [45,46]. According to Wang et al., giving sildenafil to diabetic mice who are 36 weeks old improves their long-term neuropathy. Furthermore, sildenafil reversed the down-regulation of Ang1 (angiopoietin 1) and the reduction of capillary-like tube formation in mice, which is exhibited by dermal endothelial cells due to hyperglycemia [47]. In addition, preclinical studies showed that sildenafil improves neurological function, increases functional vascular density in the sciatic nerve, and induces axonal regeneration and remyelination [17,48]. Conversely, research findings indicate that diabetic patients using sildenafil for ED experienced a decrease in neuropathy symptoms [20].
Considering these results, in this study we investigated the antihyperalgesic effect of different sildenafil-metformin combinations in alloxan-induced DN in rats. The investigated doses were chosen based on previous studies. Naveen et al. demonstrated the antinociceptive activity of sildenafil in mice and rats at a dose of 2 mg·kg−1 i.p. [49], while Bezzera et al. administered the PDE5 inhibitor in doses of 2.5 mg·kg−1 and 5 mg·kg−1 in a study that demonstrated its ability to alleviate pain in the writhing test in mice [50]. Regarding metformin, Augusto et al. showed that doses of 250, 500, or 1000 mg·kg−1 reversed mechanical allodynia in an animal model of neuropathic pain [51]. Moreover, metformin in doses of 100 and 200 mg·kg−1 preserved the nerve injury due to hyperglycemia in streptozotocin-induced diabetes in mice [52]. In addition, we demonstrated the antihyperalgesic effect of different doses of sildenafil (1.5; 2.5; 3 mg·kg−1), and metformin (150; 250; 500 mg·kg−1) administered by oral gavage in 14 days study in an animal model of DN in mice [20]. The objective of this study was to examine whether there is a synergistic interaction between sildenafil and metformin in a rat model of DN. Considering that the oral route has better compliance, we administered the investigated substances orally.
In the present research, all 3 sildenafil-metformin combinations showed a decrease of the pain sensitivity in the hot stimulus test both after 7 and 14 days of treatment, but only for the S2.5+M250 and S3+M500 groups, the decrease was statistically significant when compared to the diabetic control group. The same antihyperalgesic effect was demonstrated in the von Frey test after 14 days of treatment. Regarding the cold stimulus test, all 3 sildenafil-metformin combinations significantly increase the pain reaction latency after 8 days of treatment, while only the S2.5+M250 and S3+M500 groups significantly decrease the thermal sensitivity after 15 days of experiment when compared to the diabetic control group.
Multi-drug therapy could be a more efficient option than single-drug therapy because combinations of 2 drugs could reduce the frequency of side effects by lowering the dose of each drug [27]. Moreover, sildenafil and metformin act through different mechanisms to reduce pain from neuropathy, which could be essential in a disease characterized by complex pathophysiology such as DN.
Being recommended as first-line therapy in neuropathic pain by current guidelines, especially in post-herpetic neuralgia and DN [53], gabapentin exhibited its efficacy in ameliorating the symptoms of neuropathy in several studies. Back et. al conducted a study using an animal model to investigate the effects of gabapentin on neuropathic pain. The results showed that injecting different doses of gabapentin (30, 100, and 130 mg·kg−1) i.p. led to a reversal of both mechanical and thermal allodynia in a dose-dependent manner. [54]. LaBuda et al.demonstrated the ability of gabapentin to reduce mechanical hyperalgesia in a rat model of neuropathic pain. In this study, gabapentin was administered in doses of 30 and 90 mg·kg−1 [55]. In addition, we demonstrated in a previous study that gabapentin in doses of 50, 100, and 150 mg·kg−1 orally increased the pain reaction latency in cold and hot stimulus tests in alloxan-induced DN in mice [20].
According to these results, in our current study, gabapentin reversed thermal and mechanical hyperalgesia in a dose-dependent manner in Hot-plate, Cold-plate, and von Frey tests in alloxan-induced DN in rats.
Many preclinical and clinical investigations have demonstrated over time that systemic inflammation plays a role in the etiology of diabetic peripheral neuropathy [56]. As a regulator of immune function, TNF-α related signaling may exacerbate the vascular inflammation and oxidative stress that occur in type 2 diabetes, further contributing to the development of DN [57]. The TNF-α system has also been observed to be activated in patients with type 1 diabetes and neuropathy independent of glycemic status or insulin resistance [58]. Metformin demonstrated its anti-inflammatory effects by reducing TNF-α production in diabetic patients with type 2 diabetes, but also in preclinical studies by suppressing the scavenger receptors [59,60]. Moreover, the antihyperglycemic agent decreased spinal microglial activation and consequently lowered the mRNA (messenger ribonucleic acid) expression of TNF-α induced by morphine [61]. On the other hand, sildenafil has also demonstrated the ability to decrease TNF-α production in numerous inflammatory diseases, by inhibiting NF-κB and MAPKs (mitogen-activated protein kinases) [62,63,64].
According to these observations, our research revealed a decrease in TNF-α production following the treatment with sildenafil-metformin combinations. However, the decrease was statistically significant for the S2.5+M250 and S3+M500 combinations in liver tissues and the S3+M500 combination in brain tissues. Furthermore, the effect of reducing TNF-α by the combination in brain tissues was more effective than that of the gabapentin, which showed its ability to suppress TNF-α by up-regulating the expression of the anti-inflammatory cytokine IL-10, which inhibits the expression of pro-inflammatory cytokines [65].
Previous studies showed that, among pro-inflammatory cytokines, IL-6 has been most consistently associated with DN, affecting glial cells and neurons [66] [67]. On the other hand, IL-6 has been shown to reduce neurotoxicity in vitro and participate in neuronal growth and neurotrophic activity in vivo [68]. Due to these contrasting findings, it cannot be concluded whether this cytokine causes nerve injury or exhibits neuroprotective mechanisms [69]. Sildenafil demonstrated its ability to reduce the cellular release of IL-6 [70], while metformin showed this effect by activating AMPK [71].
Our study showed that the S2.5+M250 and S3+M500 groups had markedly reduced IL-6 levels when compared to the D group in both brain and liver tissue. Moreover, in brain tissues, these 2 sildenafil-metformin combinations recorded superior effects compared to the groups treated with gabapentin. Gabapentin has been shown to reduce IL-6 production, and one of the mechanisms responsible for this effect is the activation of PPARγ (peroxisome proliferator-activated receptor gamma receptor) and inhibition of NF-κB (nuclear factor kappa B), thereby suppressing the activation of inflammatory genes [72].
By generating free radicals, iNOS increases NO production [73]. Activation of NO production by iNOS can be achieved by macrophages and ROS (reactive species of oxygen) [74]. NO contributes to the development of inflammatory diseases by reacting with the superoxide [75]. Being rapidly inactivated by O2-, NO is susceptible to the oxidative stress that occurs in diabetes. It has been shown that an increased level of nitrotyrosine indicates an increase in NO production, due to the up-regulation of endothelial NOS or the induction of iNOS in diabetic patients [12]. In addition, Douglas et al. demonstrated an increase in NOS activity in the medullary dorsal horn in diabetic rats [76]. Gabapentin reduced the concentration of nitrites in animal models of neuropathy [77], the same potential being demonstrated for metformin by down-regulating NF-κB translocation [61], but also for sildenafil by reducing mRNA (messenger ribonucleic acid) and protein levels of iNOS [62].
These findings align with our study's findings, which highlight a decrease in nitrite concentrations in the liver and brain tissues for all three sildenafil-metformin combinations after 15 days of treatment. Regarding the concentration of total nitrites, in brain tissues, all 3 sildenafil-metformin combinations markedly reduced the level, while in liver tissues only the S2.5+M250 group produced significant decreases when compared to the D group. Among the groups treated with gabapentin, all 3 groups significantly decreased the concentration of nitrites and total nitrites in brain tissues. In liver tissues, the G30 and G90 groups produced significant decreases in the concentration of nitrites, while the G90 and G150 groups demonstrated this effect on total nitrites.
Thiols are organic compounds that contain a sulfhydryl (-SH) group, called the thiol group. Plasma protein thiols include protein sulfhydryl and disulfide groups linked to homocysteine, cysteinylglycine, cysteine, and glutathione [78]. In our study, we evaluated the concentration of total thiols expressed as glutathione (GSH) equivalents. Among the main functions of GSH is the storage of cysteine which is highly sensitive extracellularly and rapidly auto-oxidizes to cysteine with the generation of potentially toxic oxygen free radicals [79]. Oxidative stress mediated by free radicals has implications for the progression of diabetes mellitus and its complications [13]. Both types of diabetes demonstrated decreased levels of protein thiols due to metabolic and inflammatory changes [14]. A preclinical study indicated a notable reduction in the levels of blood and liver GSH in diabetic rats [80]. Ewis et al. showed that metformin improved low levels of blood and liver GSH in diabetic rats [80]. Likewise, another research highlighted the ability of metformin to modulate the expression of several oxidative genes at the transcriptional level, managing to restore the inhibition of glutathione S-transferase mediated by diabetes complications [81]. On the other hand, sildenafil also demonstrated the ability to protect against low thiol content [82,83].
Our research revealed increases in the concentration of total thiols/protein ratio for all sildenafil-metformin combinations in both brain and liver tissues, but only for the S2.5+M250 group these increases were statistically significant and only in liver tissues. Regarding the groups treated with gabapentin, only the G150 group significantly increased the concentration of total thiols after 15 days of treatment. This effect is consistent with a previous study that demonstrated that gabapentin reversed low thiol concentrations in an animal model of neuropathic pain in rats [77].
One limitation of our study is the relatively short duration of administration of the drugs (15 days) due to the high toxicity of alloxan. Consequently, we were unable to examine the impact of sildenafil-metformin on biochemical markers in the context of long-term pathology. The second limitation may be regarded as the heightened fluctuation in pain sensitivity [84].
Overall, our study demonstrated for the first time, to the best of our knowledge, that the sildenafil-metformin combination could efficiently reverse thermal and mechanical hyperalgesia in alloxan-induced DN in rats. Our results reinforce the observations made in other studies according to which a combination of 2 drugs could be more efficient in treating symptoms of DN [85]. Moreover, the combination of sildenafil and metformin raised the levels of total thiols in the liver and brain tissues while lowering the generation of TNF-α and Il-6 as well as the concentrations of nitrites and total nitrites.
4. Materials and Methods
4.1. Experimental Animals
The research was conducted on male Wistar rats aged 8-10 weeks from the INCDMI Cantacuzino (Cantacuzino National Institute of Research, Bucharest, Romania). The rats were kept in plexiglass cages and were given unlimited access to food and water. The research was conducted under controlled conditions, with the temperature maintained between 21 and 24 ℃, and the humidity levels kept between 45% and 60%, monitored using a hygrothermometer.
The experiment was conducted according to the bioethical regulations governing research on experimental animals as outlined in Directive 2010/63/EU of the European Parliament and Law 43/2014, which has been subsequently amended and expanded by Law 199/2018. The experimental protocol (CFF07/10.04.2023) was authorized by the Bioethics Committee of the Faculty of Pharmacy, Carol Davila University of Medicine and Pharmacy, Bucharest, Romania.
4.2. Induction of Diabetes Mellitus and Treatments
The diabetes was induced by alloxan (Sigma Aldrich, Hamburg, Germany, product no. A7413) injection i.p. (intraperitoneally) in a single dose of 130 mg·kg−1 to rats (n=100, 320 ± 10 g) that were prior kept fasting for 24h. After 48 hours, we determined the blood sugar of the animals with an ACCU-CHEK Active glucometer (Roche Diagnostic, Germany), by collecting blood from the veins of the tail (puncture) [84]. The animals with diabetes were chosen for additional testing if their blood glucose level was greater than 180 mg/dL.
For this study, we divided 70 diabetic rats and 10 non-diabetic rats into equal groups (n=10). The substances were administered daily for 15 days by oral gavage as follows: ND group – non-diabetic control group that received distilled water 1 mL·kg−1; D group – diabetic control group that received distilled water 1 mL·kg−1; G30 group - gabapentin 30 mg·kg−1; G90 group - gabapentin 90 mg·kg−1; G150 group - gabapentin 150 mg·kg−1; S2+M100 group-sildenafil 2 mg·kg−1 + metformin 100 mg·kg−1; S2.5+M300 group – sildenafil 2.5 mg·kg−1 + metformin 300 mg·kg−1; S3+M500 group - sildenafil 3 mg·kg−1 + metformin 500 mg·kg−1. Sildenafil was procured from Actavis Group PTC EHF (Hafnarfirdi, Island), metformin from Gedeon Richter PLC (Budapest, Hungary), and gabapentin from Egis Pharmaceuticals PLC (Budapest, Hungary).
4.3. Blood Glucose Levels
Blood glucose levels (measured in mg/dL) were assessed at three-time points: initially, as well as 7 and 15 days after the formation of the experimental groups. Blood samples were collected from the tail veins (puncture).
4.4. Tests for the Evaluation of Antihyperalgesic Effect
4.4.1. Heat Hypersensitivity
The evaluation of heat hypersensitivity was conducted using the hot-plate test, both at the beginning and after 7 and 14 days of treatment. The experimental subjects, in this case rats, were subjected to a thermal stimulus by being placed on a hot plate with a temperature of 53℃. The time interval between the initiation of the thermal stimulus and the onset of the first observable indication of pain ((licking/shaking of paws or jumping) was recorded as the latency period [86].
4.4.2. Cold Hypersensitivity
For the evaluation of cold hypersensitivity, we used the Cold-plate test. It was recorded the first manifestation of pain (licking/shaking of paws or jumping) for the rats placed on a plate cooled to -5℃. The evaluation was determined initially and after 8 and 15 days of treatment [87,88].
For both cold and heat hypersensitivity, a maximum of 25 seconds of latency was maintained to avoid possible tissue damage.
4.4.3. Tactile Hypersensitivity
Tactile hypersensitivity was assessed using von Frey filaments (Ugo Basile, Italy) initially and after 7 and 14 days of treatment. Animals were allowed to acclimate for 30 minutes in individual plexiglas cages positioned on top of a perforated wire platform. Afterwards, von Frey filaments with increasing stiffness were used (1.4; 2; 4; 6; 8; 10; 15, and 26 g corresponding to the sizes 4.17; 4.31; 4.56; 4.74; 4.93; 5.07; 5.18; 5.46) and applied with a moderate pressure to allow the filament to bend slightly for 6 sec. The filaments were applied to the 2 hind paws, respectively on their plantar surfaces. The choice of filaments was made so that the filament with the highest resistance was less than or equal to 10% of the weight of the rats. Using filament number 4 in the series and a force of 6 g, the test was started. The filament with the following stiffness was utilized if the animal did not remove its paw, which was regarded as a negative response (denoted O). The filament with the lesser stiffness was employed if the animal removed its paw, which was recorded as a positive reaction and marked with an X. Following the receipt of an OX or XO series, or four consecutive positive or negative responses, a total of four responses were conducted. Dixon's method [89] was applied and validated by Chaplan et al. [90], was used to calculate the 50% withdrawal threshold.
4.5. Biochemical Assay of Rat Brain and Liver Homogenates
For euthanasia, the animals were administered a dosage of 200 mg·kg−1 of thiopental sodium (St. Louis, MO, USA) [33]. Subsequently, the brains and livers were collected for subsequent analysis. Tissue homogenates were prepared by homogenizing tissue and phosphate Buffered Saline (PBS) at a ratio of 1:10 (w/v) using a RW 14 basic homogenizer (IKA, Staufen, Germany). Then, the homogenates were diluted 1:10 with PBS before being subjected to experimental methods.
4.5.1. Assessment of TNF-α and Il-6
The levels of TNF-α (catalog no. LS-F2558-1) and Il-6 (catalog no. LS-F5113-1) were evaluated by the instructions provided in the manual guide (LifeSpan BioSciences, Inc., Seattle, WA, USA).
4.5.2. Assessment of NOS Activity
Utilizing the previously adjusted Griess method [91] (which reduced nitrate to nitrites using vanadium (III) [92], we were able to identify nitrites and total nitrites as NOS end products in the liver and brain. After five minutes at room temperature, the tissue homogenate (50 µL) was mixed with 100 µL of modified Griess reagent (Sigma Aldrich, USA). The optical density (OD) was then measured at 540 nm. After measuring a NaNO standard curve (Sigma Aldrich, USA), the protein content was expressed as NO2 equivalents (µM). For every sample, a blank was read, and any necessary adjustments were performed.
4.5.3. Assessment of Total Thiols
A previously described method [93] using a sample to Ellman reagent ratio of 1:4 was used to determine total thiols. Results are expressed as the ratio of glutathione (GSH) equivalents (pM) to protein content (mg/mL).
4.5.4. Protein Content
The widely recognized Lowry method was utilized to assess the total protein content in tissue homogenates and mitochondrial preparations [94].
2.6. Statistical Analysis
The statistical analysis of the results was conducted using GraphPad Prism v.5.00 software developed by GraphPad Software in San Diego, California, USA. The distribution of the data was evaluated using the D'Agostino-Pearson test. For normally distributed data, one-way analysis of variance (ANOVA) test and Dunnet's post hoc test were employed for analysis. In cases of non-parametric data, the Kruskal-Wallis test and Dunn's post hoc test were utilized. It is considered that the observed differences between the groups are statistically significant when the value of p < 0.05. We used the following Formula (1) to calculate the percentage differences in the experimental outcomes between the groups [95]:
>
where, Mx is the mean value for D when compared vs. ND, or G30, G90, G150, S2 + M100, S2.5 + M300 and S3 + M500 groups when compared vs. D; My is the mean value for either ND or D.
Δ%=(Mx-My)/My×100
5. Conclusions
The purpose of our study was to investigate if the combination of sildenafil and metformin acts synergistically in reducing pain in alloxan-induced DN in rats. Our study found that this combination enhanced pain reaction latency in the Cold-plate, Hot-plate, and von Frey tests. Moreover, the sildenafil-metformin combination reduced inflammation by lowering TNF-α and IL-6 levels, prevented the increase of NOS activity, and protected against glutathione depletion.
Considering all these, the treatment of DN with a combination of sildenafil and metformin may be a better option than those recommended in the present by current guidelines.
Author Contributions
Conceptualization, C.P. and S.N.; methodology, C.P., C.E.Z., E.Ș., C.C., A.U. and S.N.; validation, C.P. and S.N.; formal analysis, C.P., N.M.B. and S.N.; investigation, C.P., N.M.B. and A.U.; data curation, C.P.; writing—original draft preparation, C.P. and A.U.; writing—review and editing, C.E.Z. and C.C.; visualization, S.N.; supervision, S.N. All authors have read and agreed to the published version of the manuscript.
Funding
Publication of this paper was supported by the University of Medicine and Pharmacy Carol Davila, through the institutional program Publish not Perish.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Bioethics Committee of the Faculty of Pharmacy, Carol Davila University of Medicine and Pharmacy, Bucharest, Romania (CFF38/05.12.2022).
Informed Consent Statement
Not applicable.
Data Availability Statement
All data generated or analyzed during this study are included in this published article.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Oshitari T. Advanced Glycation End-Products and Diabetic Neuropathy of the Retina. Int J Mol Sci 2023; 24(3):2927. [CrossRef]
- Feldman EL, Callaghan BC, Pop-Busui R, et al. Diabetic neuropathy. Nat Rev Dis Prim 2019 51 2019; 5(1):1–18.
- Pușcașu C, Zanfirescu A, Negreș S. Recent Progress in Gels for Neuropathic Pain. Gels 2023; 9(5):417. [CrossRef]
- Pușcașu C, Ungurianu A, Șeremet OC, Andrei C, Mihai DP, Negreș S. The Influence of Sildenafil–Metformin Combination on Hyperalgesia and Biochemical Markers in Diabetic Neuropathy in Mice. Medicina (B Aires) 2023; 59(8):1375. [CrossRef]
- Li C, Wang W, Ji Q, et al. Prevalence of painful diabetic peripheral neuropathy in type 2 diabetes mellitus and diabetic peripheral neuropathy: A nationwide cross-sectional study in mainland China. Diabetes Res Clin Pract 2023; 198:110602. [CrossRef]
- Tesfaye S, Chaturvedi N, Eaton SEM, et al. Vascular Risk Factors and Diabetic Neuropathy. N Engl J Med 2005; 352(4):341–350. [CrossRef]
- Yovera-Aldana M, Velásquez-Rimachi V, Huerta-Rosario A, et al. Prevalence and incidence of diabetic peripheral neuropathy in Latin America and the Caribbean: A systematic review and meta-analysis. Negida A, ed. PLoS One 2021; 16(5):e0251642. [CrossRef]
- Alleman CJM, Westerhout KY, Hensen M, et al. Humanistic and economic burden of painful diabetic peripheral neuropathy in Europe: A review of the literature. Diabetes Res Clin Pract 2015; 109(2):215–225. [CrossRef]
- Rosenberger DC, Blechschmidt V, Timmerman H, Wolff A, Treede R-D. Challenges of neuropathic pain: focus on diabetic neuropathy. J Neural Transm 2020; 127(4):589–624. [CrossRef]
- Kaur M, Mishra S, Swarnkar P, et al. Understanding the role of hyperglycemia and the molecular mechanism associated with diabetic neuropathy and possible therapeutic strategies. Biochem Pharmacol 2023:115723. [CrossRef]
- Hills CE, Brunskill NJ. Cellular and physiological effects of C-peptide. Clin Sci 2009; 116(7):565–574. [CrossRef]
- Pop-Busui R, Sima A, Stevens M. Diabetic neuropathy and oxidative stress. Diabetes Metab Res Rev 2006; 22(4):257–273.
- Dröge W. Free Radicals in the Physiological Control of Cell Function. Physiol Rev 2002; 82(1):47–95. [CrossRef]
- Van Campenhout A, Van Campenhout C, Lagrou AR, et al. Impact of diabetes mellitus on the relationships between iron-, inflammatory- and oxidative stress status. Diabetes Metab Res Rev 2006; 22(6):444–454.
- Pușcașu C, Zanfirescu A, Negreș S, Șeremet OC. Exploring the Multifaceted Potential of Sildenafil in Medicine. Medicina (B Aires) 2023; 59(12):2190. [CrossRef]
- Huang LJ, Yoon MH, Choi J Il, Kim WM, Lee HG, Kim YO. Effect of Sildenafil on Neuropathic Pain and Hemodynamics in Rats. Yonsei Med J 2010; 51(1):82. [CrossRef]
- Wang L, Chopp M, Szalad A, et al. Phosphodiesterase-5 is a therapeutic target for peripheral neuropathy in diabetic mice. Neuroscience 2011; 193:399–410. [CrossRef]
- Deftu A-F, Chu Sin Chung P, Laedermann CJ, et al. The Antidiabetic Drug Metformin Regulates Voltage-Gated Sodium Channel Na V 1.7 via the Ubiquitin-Ligase NEDD4-2. eneuro 2022; 9(2):ENEURO.0409-21.2022.
- Ge A, Wang S, Miao B, Yan M. Effects of metformin on the expression of AMPK and STAT3 in the spinal dorsal horn of rats with neuropathic pain. Mol Med Rep 2018; 17(4):5229–5237. [CrossRef]
- Pușcașu C, Mihai P, Zbârcea CE, et al. Investigation of antihyperalgesic effects of different doses of sildenafil and metformin in alloxan-induced diabetic neuropathy in mice. Farmacia 2023; 71:3.
- Finnerup NB, Haroutounian S, Kamerman P, et al. Neuropathic pain: an updated grading system for research and clinical practice. Pain 2016; 157(8):1599–1606. [CrossRef]
- Finnerup NB, Haroutounian S, Baron R, et al. Neuropathic pain clinical trials: factors associated with decreases in estimated drug efficacy. Pain 2018; 159(11):2339–2346. [CrossRef]
- Pușcașu C, Văleanu A, Ștefănescu E, Mirela Blebea N, Negreș S. Evaluating the synergism between sildenafil and metformin in an animal model of diabetic neuropathy induced by alloxan. Farmacia 2023; 71:4.
- Moisset X, Bouhassira D, Avez Couturier J, et al. Pharmacological and non-pharmacological treatments for neuropathic pain: Systematic review and French recommendations. Rev Neurol (Paris) 2020; 176(5):325–352. [CrossRef]
- Oliveira RAA de, Baptista AF, Sá KN, et al. Pharmacological treatment of central neuropathic pain: consensus of the Brazilian Academy of Neurology. Arq Neuropsiquiatr 2020; 78(11):741–752.
- Holbech JV, Jung A, Jonsson T, Wanning M, Bredahl C, Bach F. Combination treatment of neuropathic pain: Danish expert recommendations based on a Delphi process. J Pain Res 2017; Volume 10:1467–1475. [CrossRef]
- Gilron I, Jensen TS, Dickenson AH. Combination pharmacotherapy for management of chronic pain: from bench to bedside. Lancet Neurol 2013; 12(11):1084–1095. [CrossRef]
- Eisenberg E, Suzan E. Drug Combinations in the Treatment of Neuropathic Pain. Curr Pain Headache Rep 2014; 18(12):463. [CrossRef]
- Saleem Mir M, Maqbool Darzi M, Musadiq Khan H, Ahmad Kamil S, Hassan Sofi A, Ahmad Wani S. Pathomorphological effects of Alloxan induced acute hypoglycaemia in rabbits. Alexandria J Med 2013; 49(4):343–353.
- Olivenza R, Moro MA, Lizasoain I, et al. Chronic Stress Induces the Expression of Inducible Nitric Oxide Synthase in Rat Brain Cortex. J Neurochem 2001; 74(2):785–791. [CrossRef]
- Kouidrat Y, Pizzol D, Cosco T, et al. High prevalence of erectile dysfunction in diabetes: a systematic review and meta-analysis of 145 studies. Diabet Med 2017; 34(9):1185–1192. [CrossRef]
- Escobar-Jiménez F. Eficacia y seguridad del sildenafilo en varones con diabetes mellitus tipo 2 y disfunción eréctil. Med Clin (Barc) 2002; 119(4):121–124. [CrossRef]
- Phé V, Rouprêt M. Erectile dysfunction and diabetes: A review of the current evidence-based medicine and a synthesis of the main available therapies. Diabetes Metab 2012; 38(1):1–13. [CrossRef]
- Buse JB, Wexler DJ, Tsapas A, et al. 2019 Update to: Management of Hyperglycemia in Type 2 Diabetes, 2018. A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2020; 43(2):487–493. [CrossRef]
- Sun WT, Lei CL, Bi CC, Chen ZL, Zhang L. Effect of alloxan time administerDrug on establishing diabetic rabbit model. Int J Ophthalmol 2010; 3(3):200. [CrossRef]
- Raafat K, Aboul-Ela M, El-Lakany A. Alloxan-induced diabetic thermal hyperalgesia, prophylaxis and phytotherapeutic effects of Rheum ribes L. in mouse model. Arch Pharm Res 2021; 44(8):1–10. [CrossRef]
- Bhalla V, Oyster NM, Fitch AC, et al. AMP-activated Kinase Inhibits the Epithelial Na+ Channel through Functional Regulation of the Ubiquitin Ligase Nedd4-2. J Biol Chem 2006; 281(36):26159–26169. [CrossRef]
- Mia S, Munoz C, Pakladok T, et al. Downregulation of Kv1.5 K + Channels by the AMP-Activated Protein Kinase. Cell Physiol Biochem 2012; 30(4):1039–1050.
- Wei J, Wei Y, Huang M, Wang P, Jia S. Is metformin a possible treatment for diabetic neuropathy? J Diabetes 2022; 14(10):658–669.
- A. Shamsaldeen Y, S. Mackenzie L, A. Lione L, D. Benham C. Methylglyoxal, A Metabolite Increased in Diabetes is Associated with Insulin Resistance, Vascular Dysfunction and Neuropathies. Curr Drug Metab 2016; 17(4):359–367.
- Afshari K, Dehdashtian A, Haddadi N-S, et al. Anti-inflammatory effects of Metformin improve the neuropathic pain and locomotor activity in spinal cord injured rats: introduction of an alternative therapy. Spinal Cord 2018; 56(11):1032–1041. [CrossRef]
- Byrne FM, Cheetham S, Vickers S, Chapman V. Characterisation of Pain Responses in the High Fat Diet/Streptozotocin Model of Diabetes and the Analgesic Effects of Antidiabetic Treatments. J Diabetes Res 2015; 2015:1–13. [CrossRef]
- Melemedjian OK, Asiedu MN, Tillu D V., et al. Targeting adenosine monophosphate-activated protein kinase (AMPK) in preclinical models reveals a potential mechanism for the treatment of neuropathic pain. Mol Pain 2011; 7. [CrossRef]
- Mao-Ying QL, Kavelaars A, Krukowski K, et al. The Anti-Diabetic Drug Metformin Protects against Chemotherapy-Induced Peripheral Neuropathy in a Mouse Model. PLoS One 2014; 9(6):e100701. [CrossRef]
- Meller ST, Pechman PS, Gebhart GF, Maves TJ. Nitric oxide mediates the thermal hyperalgesia produced in a model of neuropathic pain in the rat. Neuroscience 1992; 50(1):7–10. [CrossRef]
- Patil CS, Padi S V., Singh VP, Kulkarni SK. Sildenafil induces hyperalgesia via activation of the NO-cGMP pathway in the rat neuropathic pain model. Inflammopharmacology 2006; 14(1–2):22–27.
- Wang L, Chopp M, Szalad A, et al. Sildenafil ameliorates long term peripheral neuropathy in type II diabetic mice. PLoS One 2015; 10(2). [CrossRef]
- Ebenezer GJ, O’Donnell R, Hauer P, Cimino NP, McArthur JC, Polydefkis M. Impaired neurovascular repair in subjects with diabetes following experimental intracutaneous axotomy. Brain 2011; 134(6):1853–1863. [CrossRef]
- Jain NK, Patil CS, Singh A, Kulkarni SK. Sildenafil-induced peripheral analgesia and activation of the nitric oxide–cyclic GMP pathway. Brain Res 2001; 909(1–2):170–178. [CrossRef]
- Bezerra MM, Lima V, Girão VCC, Teixeira RC, Graça JR V. Antinociceptive activity of sildenafil and adrenergic agents in the writhing test in mice. Pharmacol Rep 2008; 60(3):339–344.
- Augusto PSA, Braga A V., Rodrigues FF, et al. Metformin antinociceptive effect in models of nociceptive and neuropathic pain is partially mediated by activation of opioidergic mechanisms. Eur J Pharmacol 2019; 858:172497. [CrossRef]
- Lós DB, Oliveira WH de, Duarte-Silva E, et al. Preventive role of metformin on peripheral neuropathy induced by diabetes. Int Immunopharmacol 2019; 74:105672. [CrossRef]
- Kukkar A, Bali A, Singh N, Jaggi AS. Implications and mechanism of action of gabapentin in neuropathic pain. Arch Pharm Res 2013; 36(3):237–251. [CrossRef]
- Back SK, Won SY, Hong SK, Na HS. Gabapentin relieves mechanical, warm and cold allodynia in a rat model of peripheral neuropathy. Neurosci Lett 2004; 368(3):341–344. [CrossRef]
- LaBuda CJ, Fuchs PN. Morphine and gabapentin decrease mechanical hyperalgesia and escape/avoidance behavior in a rat model of neuropathic pain. Neurosci Lett 2000; 290(2):137–140. [CrossRef]
- Zheng H, Sun W, Zhang Q, et al. Proinflammatory cytokines predict the incidence of diabetic peripheral neuropathy over 5 years in Chinese type 2 diabetes patients: A prospective cohort study. EClinicalMedicine 2021; 31:100649. [CrossRef]
- Fischer R, Maier O. Interrelation of Oxidative Stress and Inflammation in Neurodegenerative Disease: Role of TNF. Oxid Med Cell Longev 2015; 2015:1–18. [CrossRef]
- Gonzalez-Clemente JM, Mauricio D, Richart C, et al. Diabetic neuropathy is associated with activation of the TNF-alpha system in subjects with type 1 diabetes mellitus. Clin Endocrinol (Oxf) 2005; 63(5):525–529. [CrossRef]
- Andrews M, Soto N, Arredondo M. Efecto de metformina sobre la expresión del factor de necrosis tumoral-α, los receptores Toll-like 2/4 y la PCR ultra sensible en sujetos obesos con diabetes tipo 2. Rev Med Chil 2012; 140(11):1377–1382.
- Hyun B, Shin S, Lee A, et al. Metformin Down-regulates TNF-α Secretion via Suppression of Scavenger Receptors in Macrophages. Immune Netw 2013; 13(4):123. [CrossRef]
- Pan Y, Sun X, Jiang L, et al. Metformin reduces morphine tolerance by inhibiting microglial-mediated neuroinflammation. J Neuroinflammation 2016; 13(1):294. [CrossRef]
- Zhao S, Zhang L, Lian G, et al. Sildenafil attenuates LPS-induced pro-inflammatory responses through down-regulation of intracellular ROS-related MAPK/NF-κB signaling pathways in N9 microglia. Int Immunopharmacol 2011; 11(4):468–474.
- Karakoyun B, Uslu U, Ercan F, et al. The effect of phosphodiesterase-5 inhibition by sildenafil citrate on inflammation and apoptosis in rat experimental colitis. Life Sci 2011; 89(11–12):402–407. [CrossRef]
- Hube F, Lee Y-M, Röhrig K, Hauner H. The Phosphodiesterase Inhibitor IBMX Suppresses TNF-α Expression in Human Adipocyte Precursor Cells: A Possible Explanation for its Adipogenic Effect. Horm Metab Res 1999; 31(06):359–362. [CrossRef]
- Lee B-S, Jun I-G, Kim S-H, Park JY. Intrathecal Gabapentin Increases Interleukin-10 Expression and Inhibits Pro-Inflammatory Cytokine in a Rat Model of Neuropathic Pain. J Korean Med Sci 2013; 28(2):308. [CrossRef]
- Herder C, Bongaerts BWC, Rathmann W, et al. Association of Subclinical Inflammation With Polyneuropathy in the Older Population. Diabetes Care 2013; 36(11):3663–3670. [CrossRef]
- Zhou J, Zhou S. Inflammation: Therapeutic Targets for Diabetic Neuropathy. Mol Neurobiol 2014; 49(1):536–546. [CrossRef]
- Cameron N, Cotter M. The neurocytokine, interleukin-6, corrects nerve dysfunction in experimental diabetes. Exp Neurol 2007; 207(1):23–29. [CrossRef]
- Magrinelli F, Briani C, Romano M, et al. The Association between Serum Cytokines and Damage to Large and Small Nerve Fibers in Diabetic Peripheral Neuropathy. J Diabetes Res 2015; 2015:1–7. [CrossRef]
- Di Luigi L, Sgrò P, Duranti G, et al. Sildenafil Reduces Expression and Release of IL-6 and IL-8 Induced by Reactive Oxygen Species in Systemic Sclerosis Fibroblasts. Int J Mol Sci 2020; 21(9):3161.
- Kim YD, Kim YH, Cho YM, et al. Metformin ameliorates IL-6-induced hepatic insulin resistance via induction of orphan nuclear receptor small heterodimer partner (SHP) in mouse models. Diabetologia 2012; 55(5):1482–1494. [CrossRef]
- de Brito TV, Júnior GJD, da Cruz Júnior JS, et al. Gabapentin attenuates intestinal inflammation: Role of PPAR-gamma receptor. Eur J Pharmacol 2020; 873:172974.
- Phaniendra A, Jestadi DB, Periyasamy L. Free Radicals: Properties, Sources, Targets, and Their Implication in Various Diseases. Indian J Clin Biochem 2015; 30(1):11–26. [CrossRef]
- Zhao K, Huang Z, Lu H, Zhou J, Wei T. Induction of inducible nitric oxide synthase increases the production of reactive oxygen species in RAW264.7 macrophages. Biosci Rep 2010; 30(4):233–241. [CrossRef]
- Lubos E. Role of oxidative stress and nitric oxide in atherothrombosis. Front Biosci 2008; Volume(13):5323. [CrossRef]
- Zochodne DW, Verge VMK, Cheng C, et al. Nitric Oxide Synthase Activity and Expression in Experimental Diabetic Neuropathy. J Neuropathol Exp Neurol 2000; 59(9):798–807. [CrossRef]
- Forouzanfar F, Tanha NK, Pourbagher-Shahri AM, Mahdianpour S, Esmaeili M, Ghazavi H. Synergistic effect of ellagic acid and gabapentin in a rat model of neuropathic pain. Metab Brain Dis 2023; 38(4):1421–1432. [CrossRef]
- Rossi R, Giustarini D, Milzani A, Dalle-Donne I. Cysteinylation and homocysteinylation of plasma protein thiols during ageing of healthy human beings. J Cell Mol Med 2009; 13(9B):3131–3140. [CrossRef]
- Lu SC. Regulation of hepatic glutathione synthesis: current concepts and controversies. FASEB J 1999; 13(10):1169–1183. [CrossRef]
- Ewis SA, Abdel-Rahman MS. Effect of metformin on glutathione and magnesium in normal and streptozotocin-induced diabetic rats. J Appl Toxicol 1995; 15(5):387–390. [CrossRef]
- Alhaider AA, Korashy HM, Sayed-Ahmed MM, Mobark M, Kfoury H, Mansour MA. Metformin attenuates streptozotocin-induced diabetic nephropathy in rats through modulation of oxidative stress genes expression. Chem Biol Interact 2011; 192(3):233–242. [CrossRef]
- Abdollahi M, Fooladian F, Emami B, Zafari K, Bahreini-Moghadam A. Protection by sildenafil and theophylline of lead acetate-induced oxidative stress in rat submandibular gland and saliva. Hum Exp Toxicol 2003; 22(11):587–592. [CrossRef]
- Hüsamettin Baran A, Berk A, Bahadır Kaymaz M, Aktay G, Corresponding °, Baran AH. Antioxidant Effect of Sildenafil on Cadmium-Induced Liver, Lung and Kidney Injury. J Pharm Sci 2020; 45:37–44.
- Negreş S, Chiriţă C, Moroşan E, Arsene AL. Experimental pharmacological model of diabetes induction with aloxan in rat. Farmacia 2013; 61(2).
- Gilron I, Max MB. Combination pharmacotherapy for neuropathic pain: current evidence and future directions. Expert Rev Neurother 2005; 5(6):823–830. [CrossRef]
- New, RAT. Screening Methods in Pharmacology. Yale J. Biol. Med. 1965, 38, 309. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2591164 (accessed on 7 February 2023).
- Tsagareli MG, Tsiklauri N, Zanotto KL, et al. Behavioral evidence of thermal hyperalgesia and mechanical allodynia induced by intradermal cinnamaldehyde in rats. Neurosci Lett 2010; 473(3):233–236. [CrossRef]
- Akiyama T, Carstens MI, Carstens E. Spontaneous itch in the absence of hyperalgesia in a mouse hindpaw dry skin model. Neurosci Lett 2010; 484(1):62–65. [CrossRef]
- Dixon WJ. The Up-and-Down Method for Small Samples. J Am Stat Assoc 1965; 60(312):967–978.
- Chaplan SR, Bach FW, Pogrel JW, Chung JM, Yaksh TL. Quantitative assessment of tactile allodynia in the rat paw. J Neurosci Methods 1994; 53(1):55–63.
- Gradinaru D, Margina D, Borsa C, et al. Adiponectin: possible link between metabolic stress and oxidative stress in the elderly. Aging Clin Exp Res 2017; 29(4):621–629. [CrossRef]
- Miranda KM, Espey MG, Wink DA. A rapid, simple spectrophotometric method for simultaneous detection of nitrate and nitrite. Nitric oxide Biol Chem 2001; 5(1):62–71. [CrossRef]
- Nitulescu G, Mihai DP, Nicorescu IM, et al. Discovery of natural naphthoquinones as sortase A inhibitors and potential anti-infective solutions against Staphylococcus aureus. Drug Dev Res 2019; 80(8):1136–1145. [CrossRef]
- Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurement with the Folin phenol reagent. J Biol Chem 1951; 193(1):265–275.
- Mihai DP, Ungurianu A, Ciotu CI, et al. Effects of venlafaxine, risperidone and febuxostat on cuprizone-induced demyelination, behavioral deficits and oxidative stress. Int J Mol Sci 2021; 22(13):7183. [CrossRef]
Figure 1.
(A) Initial glycemia. (B) Glycemia at 7 days (C) Glycemia at 15 days (D) Evolution of the mean blood glucose levels during the experiment. Values are expressed as mean ± S.E.M (standard error of the mean). ND - non-diabetic control; D - diabetic control; G30 - gabapentin 30 mg·kg−1; G90 - gabapentin 90 mg·kg−1; G150 – gabapentin 150 mg·kg−1; S2+M100 – sildenafil 2 mg·kg−1+ metformin 100 mg·kg−1; S2.5+M300 – sildenafil 2.5 mg·kg−1 + metformin 300 mg·kg−1; S3+M500 – sildenafil 3 mg·kg−1+ metformin 500 mg·kg−1; *p < 0.05; **p < 0.01; ***p < 0.001 vs. ND. #p < 0.05; ##p < 0.01; ###p < 0.001 vs. D.
Figure 1.
(A) Initial glycemia. (B) Glycemia at 7 days (C) Glycemia at 15 days (D) Evolution of the mean blood glucose levels during the experiment. Values are expressed as mean ± S.E.M (standard error of the mean). ND - non-diabetic control; D - diabetic control; G30 - gabapentin 30 mg·kg−1; G90 - gabapentin 90 mg·kg−1; G150 – gabapentin 150 mg·kg−1; S2+M100 – sildenafil 2 mg·kg−1+ metformin 100 mg·kg−1; S2.5+M300 – sildenafil 2.5 mg·kg−1 + metformin 300 mg·kg−1; S3+M500 – sildenafil 3 mg·kg−1+ metformin 500 mg·kg−1; *p < 0.05; **p < 0.01; ***p < 0.001 vs. ND. #p < 0.05; ##p < 0.01; ###p < 0.001 vs. D.
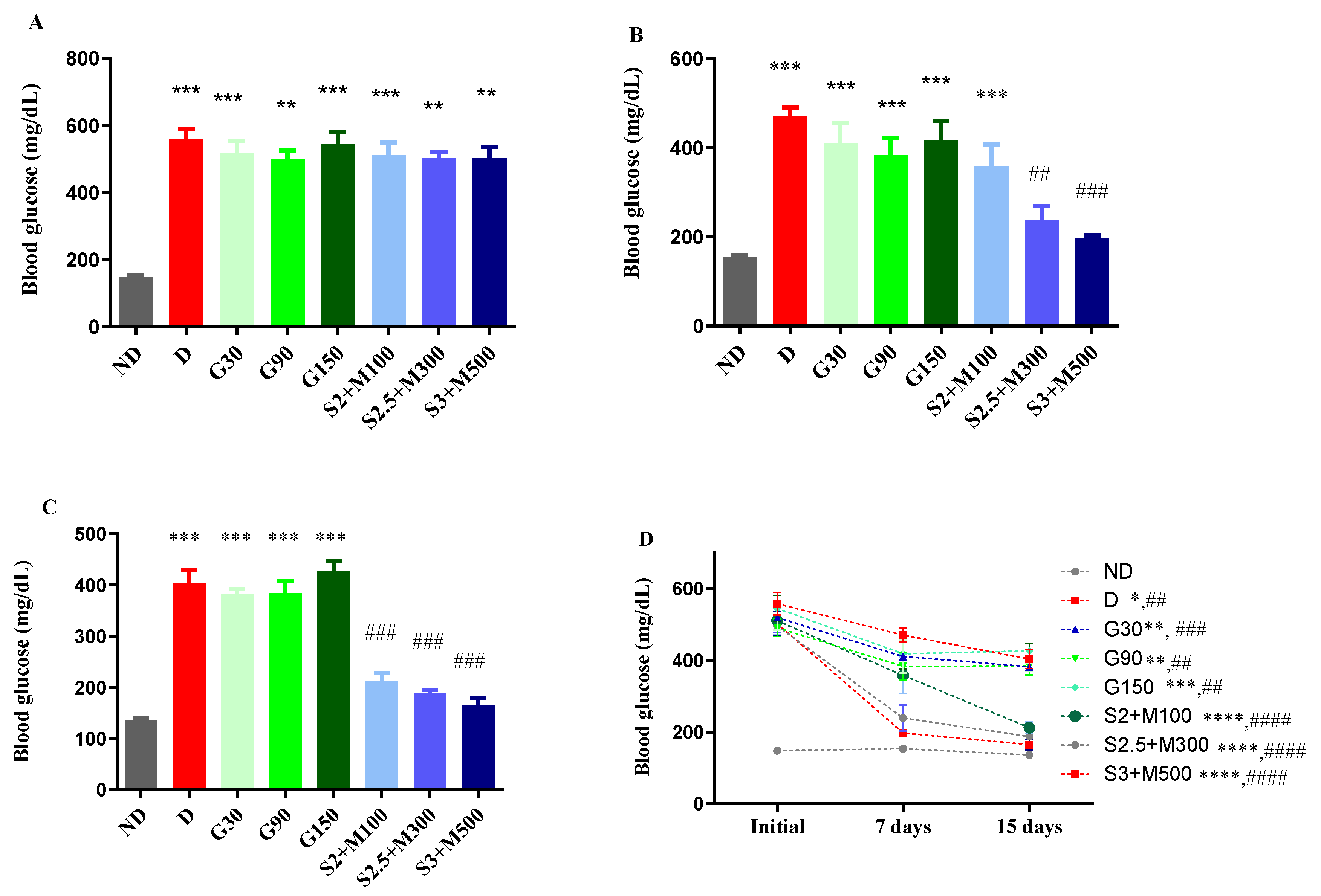
Figure 2.
(A) Hot plate test initial pain reaction latency (B) Hot plate test-pain reaction latency after 7 days (C) Hot-plate test - pain reaction latency after 14 days (D) Cold-plate test - initial pain reaction latency (E) Cold-plate test - pain reaction latency after 8 days (F) Cold-plate test - pain reaction latency after 15 days. Values are expressed as mean ± S.E.M. ND - non-diabetic control; D - diabetic control; G30 - gabapentin 30 mg·kg−1; G90 - gabapentin 90 mg·kg−1; G150 – gabapentin 150 mg·kg−1; S2+M100 – sildenafil 2 mg·kg−1+ metformin 100 mg·kg−1; S2.5+M300 – sildenafil 2.5 mg·kg−1 + metformin 300 mg·kg−1; S3+M500 – sildenafil 3 mg·kg−1+ metformin 500 mg·kg−1; *p < 0.05; **p < 0.01; ***p < 0.001 vs. ND. #p < 0.05; ##p < 0.01; ###p < 0.001 vs. D.
Figure 2.
(A) Hot plate test initial pain reaction latency (B) Hot plate test-pain reaction latency after 7 days (C) Hot-plate test - pain reaction latency after 14 days (D) Cold-plate test - initial pain reaction latency (E) Cold-plate test - pain reaction latency after 8 days (F) Cold-plate test - pain reaction latency after 15 days. Values are expressed as mean ± S.E.M. ND - non-diabetic control; D - diabetic control; G30 - gabapentin 30 mg·kg−1; G90 - gabapentin 90 mg·kg−1; G150 – gabapentin 150 mg·kg−1; S2+M100 – sildenafil 2 mg·kg−1+ metformin 100 mg·kg−1; S2.5+M300 – sildenafil 2.5 mg·kg−1 + metformin 300 mg·kg−1; S3+M500 – sildenafil 3 mg·kg−1+ metformin 500 mg·kg−1; *p < 0.05; **p < 0.01; ***p < 0.001 vs. ND. #p < 0.05; ##p < 0.01; ###p < 0.001 vs. D.
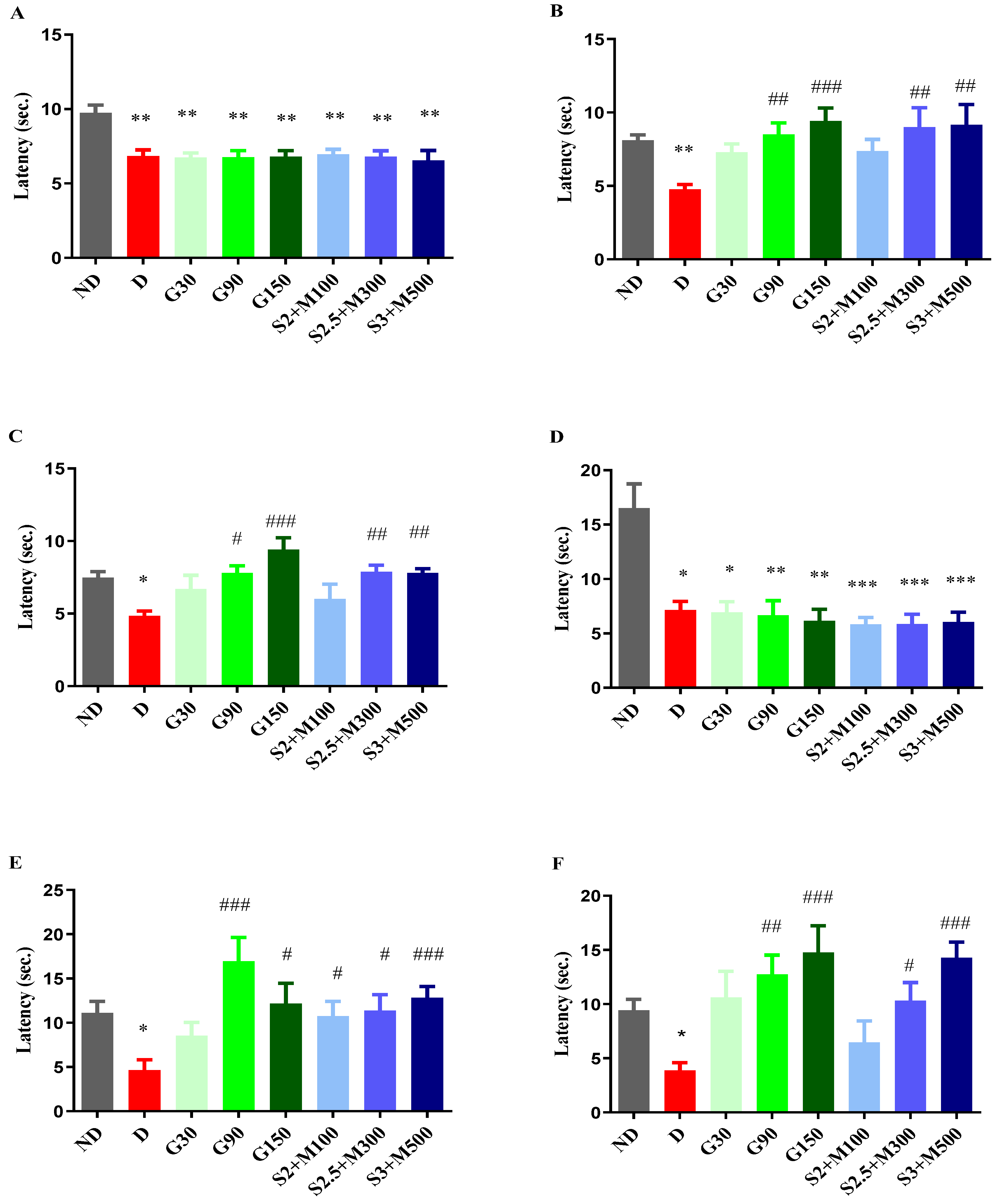
Figure 3.
(A) 50% withdrawal threshold in von Frey test initial (B) 50% withdrawal threshold in von Frey test at 7 days (C) 50% withdrawal threshold in von Frey test at 14 days. Values are expressed as mean ± S.E.M. ND - non-diabetic control; D - diabetic control; G30 - gabapentin 30 mg·kg−1; G90 - gabapentin 90 mg·kg−1; G150 – gabapentin 150 mg·kg−1; S2+M100 – sildenafil 2 mg·kg−1+ metformin 100 mg·kg−1; S2.5+M300 – sildenafil 2.5 mg·kg−1 + metformin 300 mg·kg−1; S3+M500 – sildenafil 3 mg·kg−1+ metformin 500 mg·kg−1; z*p < 0.05; **p < 0.01 vs. ND. #p < 0.05; ##p < 0.01 vs. D.
Figure 3.
(A) 50% withdrawal threshold in von Frey test initial (B) 50% withdrawal threshold in von Frey test at 7 days (C) 50% withdrawal threshold in von Frey test at 14 days. Values are expressed as mean ± S.E.M. ND - non-diabetic control; D - diabetic control; G30 - gabapentin 30 mg·kg−1; G90 - gabapentin 90 mg·kg−1; G150 – gabapentin 150 mg·kg−1; S2+M100 – sildenafil 2 mg·kg−1+ metformin 100 mg·kg−1; S2.5+M300 – sildenafil 2.5 mg·kg−1 + metformin 300 mg·kg−1; S3+M500 – sildenafil 3 mg·kg−1+ metformin 500 mg·kg−1; z*p < 0.05; **p < 0.01 vs. ND. #p < 0.05; ##p < 0.01 vs. D.
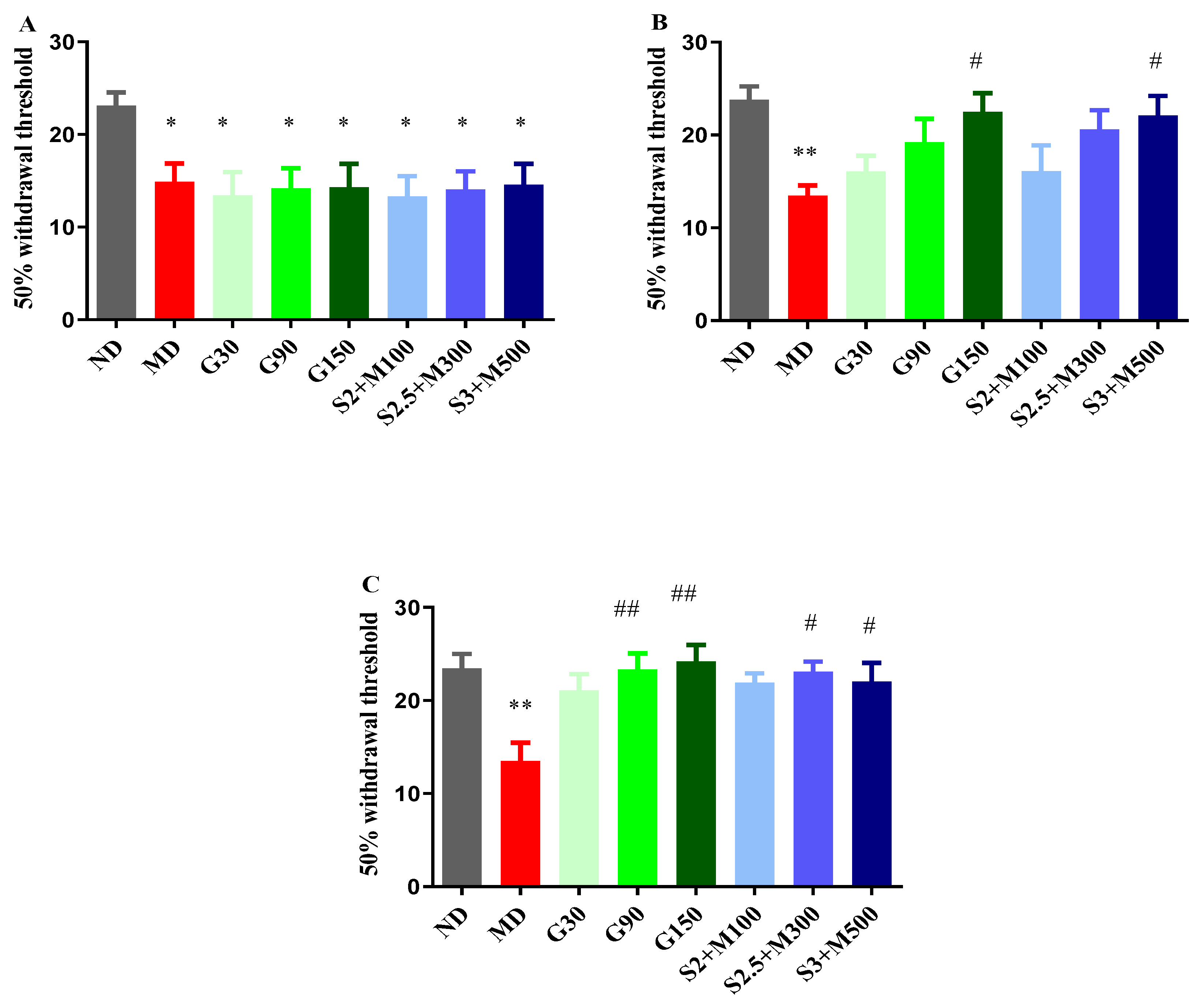
Figure 4.
(A) Variation of TNF-α in rat brain tissues (B) Variation TNF-α in rat liver tissues (C) Variation of IL-6 in rat brain tissues (D) Variation of IL-6 in rat liver tissues. Values are expressed as mean ± S.E.M. ND – non-diabetic control; D-diabetic control; GBN-gabapentin 100 mg·kg−1; S1.5+M150-sildenafil 1.5 mg·kg−1 + metformin 150mg·kg−1; S2.5+M250-sildenafil 2.5 mg·kg−1 + metformin 250 mg·kg−1; S3+M500 - sildenafil 3 mg·kg−1 + metformin 500 mg·kg−1; *p < 0.05; **p < 0.01; ***p < 0.001 vs. ND. #p < 0.05; ##p < 0.01; ###p < 0.001 vs. D.
Figure 4.
(A) Variation of TNF-α in rat brain tissues (B) Variation TNF-α in rat liver tissues (C) Variation of IL-6 in rat brain tissues (D) Variation of IL-6 in rat liver tissues. Values are expressed as mean ± S.E.M. ND – non-diabetic control; D-diabetic control; GBN-gabapentin 100 mg·kg−1; S1.5+M150-sildenafil 1.5 mg·kg−1 + metformin 150mg·kg−1; S2.5+M250-sildenafil 2.5 mg·kg−1 + metformin 250 mg·kg−1; S3+M500 - sildenafil 3 mg·kg−1 + metformin 500 mg·kg−1; *p < 0.05; **p < 0.01; ***p < 0.001 vs. ND. #p < 0.05; ##p < 0.01; ###p < 0.001 vs. D.
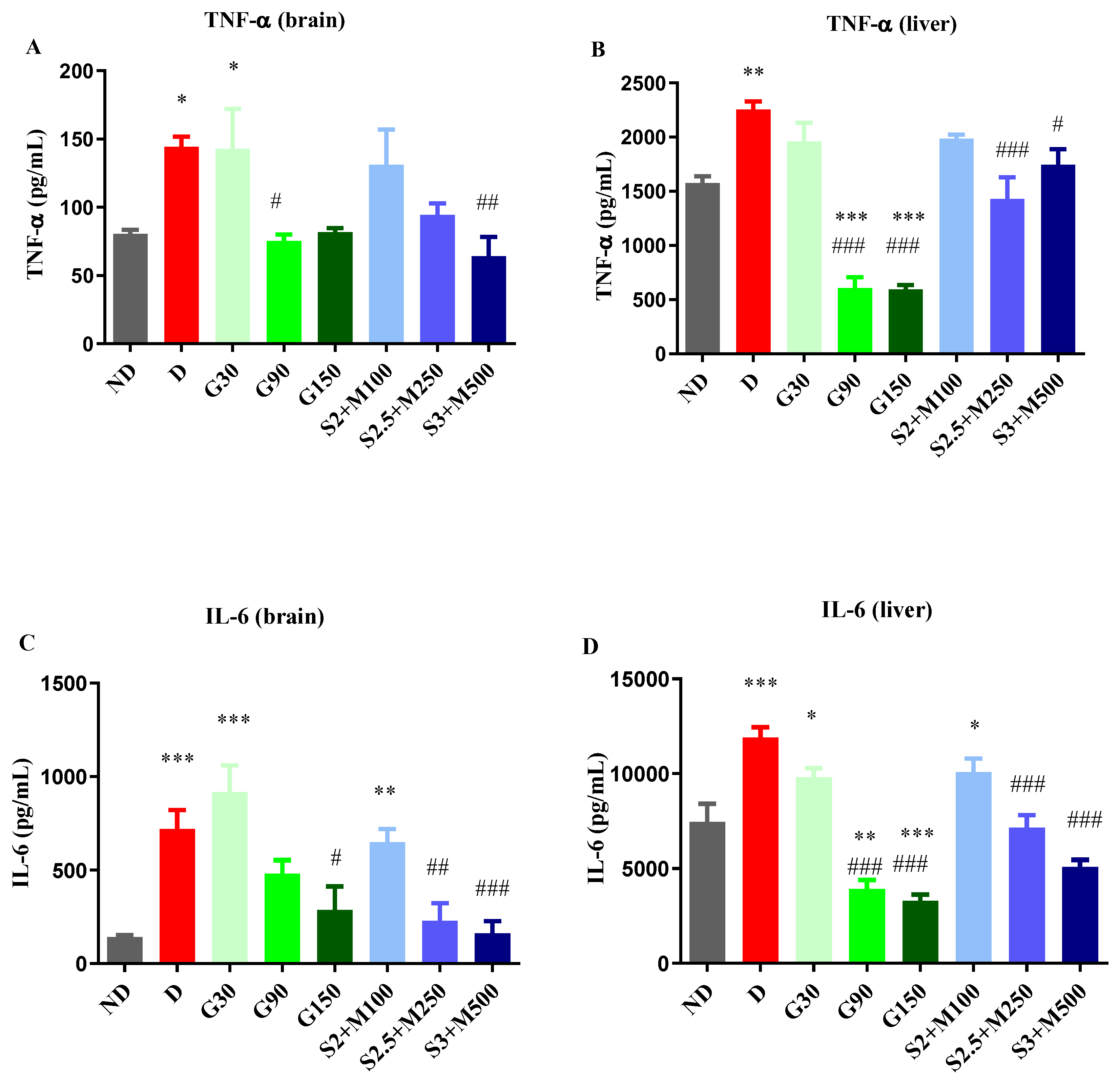
Figure 5.
(A) Variation of nitrites/proteins ratio in rat brain tissues (B) Variation of nitrites/proteins ratio in rat liver tissues (C) Variation of total nitrites/proteins ratio in rat brain tissues (D) Variation of total nitrites/proteins ratio in rat liver tissues (E) Variation of total thiols/proteins ratio in rat brain tissues (F) Variation of total thiols/proteins ratio in rat liver tissues. Values are expressed as mean ± S.E.M. ND – non-diabetic control; D-diabetic control; GBN-gabapentin 100 mg·kg−1; S1.5+M150-sildenafil 1.5 mg·kg−1 + metformin 150mg·kg−1; S2.5+M250-sildenafil 2.5 mg·kg−1 + metformin 250 mg·kg−1; S3+M500 - sildenafil 3 mg·kg−1 + metformin 500 mg·kg−1; *p < 0.05; **p < 0.01; ***p < 0.001 vs. ND. #p < 0.05; ##p < 0.01; ###p < 0.001 vs. D.
Figure 5.
(A) Variation of nitrites/proteins ratio in rat brain tissues (B) Variation of nitrites/proteins ratio in rat liver tissues (C) Variation of total nitrites/proteins ratio in rat brain tissues (D) Variation of total nitrites/proteins ratio in rat liver tissues (E) Variation of total thiols/proteins ratio in rat brain tissues (F) Variation of total thiols/proteins ratio in rat liver tissues. Values are expressed as mean ± S.E.M. ND – non-diabetic control; D-diabetic control; GBN-gabapentin 100 mg·kg−1; S1.5+M150-sildenafil 1.5 mg·kg−1 + metformin 150mg·kg−1; S2.5+M250-sildenafil 2.5 mg·kg−1 + metformin 250 mg·kg−1; S3+M500 - sildenafil 3 mg·kg−1 + metformin 500 mg·kg−1; *p < 0.05; **p < 0.01; ***p < 0.001 vs. ND. #p < 0.05; ##p < 0.01; ###p < 0.001 vs. D.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



