
Submitted:
28 March 2024
Posted:
29 March 2024
You are already at the latest version
Abstract
Over the past years, burgeoning insights into the gut microbiota have unveiled its pivotal role in human health, influencing everything from metabolism to immune function. This article comprehensively reviews literature from the last seven years to dissect the link between gut microbiota and gestational diabetes (GD), a condition of glucose intolerance manifesting during pregnancy with long-term implications for both mother and offspring. Through detailed analysis, we highlight how alterations in the composition and function of the gut microbiota may contribute to the development of GD by influencing insulin resistance and glucose homeostasis. The underlying pathophysiological mechanisms, including dysbiosis and its impact on systemic inflammation, as well as the interplay with genetic, epigenetic, and environmental factors, are discussed. Furthermore, we review current and potential microbiota-targeted interventions, such as probiotic use, and their capability to modify GD risk and management. With a focus on recent studies, this article underscores the significance of considering microbial health in the prevention and treatment of GD, offering insights into future research directions and clinical applications to improve maternal-infant health outcomes.
Keywords:
Microbiota
; Diabetes
; Gestational Diabetes
; Probiotics
; Drugs.
1. Introduction
Recent research underscores the intricate relationship between the human gut microbiota and gestational diabetes (GD), a condition that affects a significant portion of pregnancies worldwide. The human microbiome, particularly the gut microbiota, plays a pivotal role in various metabolic functions, including glucose and lipid homeostasis. Alterations in the gut microbiota, known as dysbiosis, have been implicated in the pathogenesis of several metabolic diseases, including obesity, type 2 diabetes mellitus (T2D), and gestational diabetes (GD). GD not only complicates pregnancy but also poses long-term health risks for both the mother and the offspring [1].
Pregnancy induces significant changes in gut microbiota composition, which may influence the mother’s glucose metabolism and contribute to the development of GD. Research indicates that gut microbiota composition during pregnancy differs between women with GD and healthy pregnant women, suggesting potential targets for therapeutic interventions. Furthermore, the interaction between GD and gut microbiota composition extends to the offspring, affecting their metabolic pathways and possibly predisposing them to metabolic diseases later in life[2,3].
1.1. The Human Microbiome
The human microbiome plays a critical role in metabolic regulation, immune function and behaviour, comprising over 100 billion cells (mostly in the gastrointestinal tract) [2] and containing 27 times more genes than the human genome. [3,4]. The microbiota is defined as a complex ecosystem of microorganisms, including bacteria, viruses, and protozoa living in different areas of the body. Over 70% of the microbiota resides in the gastrointestinal tract in a mutually beneficial relationship with its host. The microbiota plays a significant role in many metabolic functions, including the modulation of glucose and lipid homeostasis, the regulation of satiety, and the production of energy and vitamins. There is growing evidence that any modification in the composition of the microbiota can lead to various diseases, including cardiometabolic diseases. This is because alterations in the composition of the microbiota can cause insulin resistance, inflammation, vascular, and metabolic disorders. For instance, dysbiosis or imbalance in the microbiota can lead to a chronic low-grade inflammatory state, which in turn can promote insulin resistance, a precursor to diabetes [1].
1.2. Gut Microbiota Dysbiosis in Diabetes.
Diabetes mellitus (DM) is a heterogeneous group of metabolism diseases characterized by hyperglycemia, which may result in long-term complications leading to damage to many of the body’s systems, especially kidneys, nerves, eyes, and blood vessels [5].
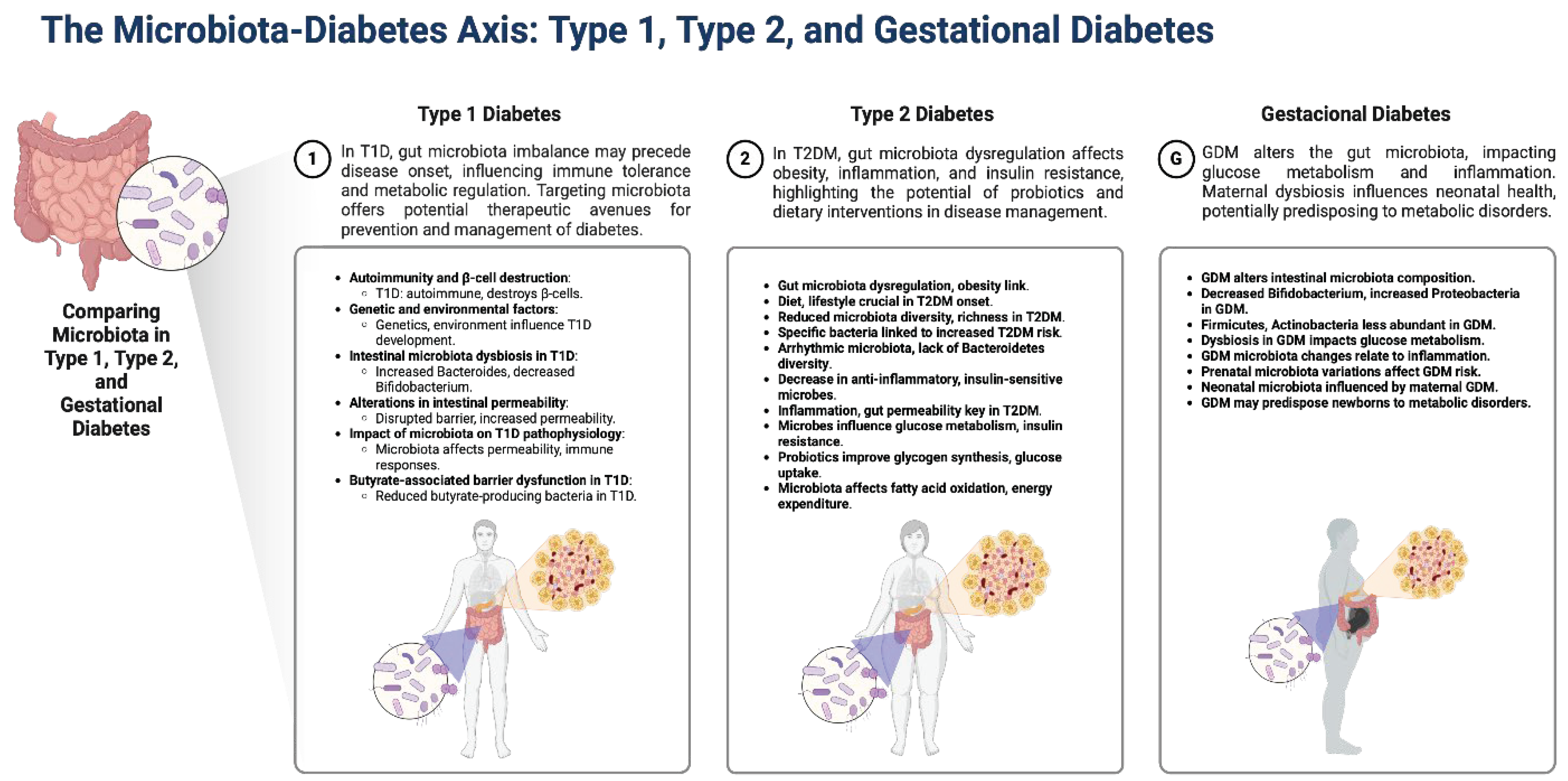
Type 1 diabetes (T1D) is primarily an autoimmune condition where the immune system mistakenly attacks and destroys the insulin-producing β-cells in the pancreas. Recent research highlights the influence of genetic, epigenetic, and environmental factors on the development of T1D, with a significant focus on the role of the gut microbiota. Alterations in this gut microbiota, due to dietary changes, antibiotic use, or infections, can lead to dysbiosis, contributing to autoimmune and inflammatory diseases, showing that the gut microbiota composition in T1D patients differs significantly from healthy individuals, suggesting a link between gut health and the development of T1D [6].
Type 2 Diabetes Mellitus (T2D), a prevalent metabolic disorder globally, arises mainly due to inadequate insulin secretion from pancreatic β-cells and the reduced responsiveness of insulin-sensitive tissues [7]. Emerging research highlights the significant role of gut microbiota dysregulation alongside adipokine imbalance and inflammation in its pathogenesis [8]. In patients with T2D, a dysbiosis has been observed. This dysbiosis is characterized by a reduced overall diversity and richness of the gut microbiota. Specific bacterial taxa such as Granulicatella and Prevotella have been associated with an increased risk of developing T2D. Some differences include higher abundances of Escherichia, Shigella, Collinsella, among others [9]. Unlike healthy controls who exhibit daily oscillations in numerous operational taxonomic units, T2D patients show an arrhythmic microbiota lacking diversity in Bacteroidetes and Firmicutes. This dysbiosis in the gut microbiome of T2D patients underscores the intricate relationship between metabolic health and gut microbiota composition [10]. Through these mechanisms, the gut microbiota emerges as a pivotal factor in the development and progression of T2D, offering promising avenues for future research aimed at restoring gut microbiota balance and function.
The dysbiosis characteristic of T2D, marked by a reduced diversity and changes in specific bacterial taxa, is visually summarized in Figure 1, illustrating the unique microbial profiles associated with each type of diabetes and their potential consequences on host metabolism and immune responses.
1.3. Gestational Diabetes
Gestational diabetes (GD) is defined as the dysregulation of glucose tolerance that initiates or occurs in pregnant women [11]. The International Association of Diabetes and Pregnancy Study Group (IADPSG) recommends that all women in the gestational stage maintain the following glucose goals: fasting glucose <95 mg/dL and either 1-h postprandial glucose <140 mg/dL or 2-h postprandial glucose <120 mg/dL [12]. The American College of Obstetricians and Gynecologists (ACOG) recommends fasting glucose of 70-95 mg/dl, glucose at 1-hour postprandial 110-140 mg/dl, and glucose at 2 hours postprandial 100-120 mg/dl. Among these criteria, those of IADPSG currently have the highest diagnostic capability for GD [13].
The pathophysiological mechanisms of the disease described so far explore different pathways, of which the following stand out: 1) dysfunction of beta cells caused by the hyperglycemic state secondary to physiological changes of pregnancy (such as insulin sensitivity adaptation); in the early stage of pregnancy, its sensitivity increases, promoting energy reserves within adipose tissue in preparation for gestation, these changes promote insulin resistance. 2) Insulin resistance, which causes inadequate translocation of glucose transporter 4 (GLUT4), through reduced tyrosine phosphorylation and increased threonine/serine in the insulin receptor [14]. 3) Studies have found differences in gut microbiota composition between healthy and GD-affected pregnant women, including variations in microbial diversity and specific bacterial abundances[15]. These findings suggest the gut microbiota’s potential as a biomarker for early detection of GD and a target for interventions to reduce GD risk. Moreover, alterations in the gut microbiota may be associated with GD’s metabolic dysregulations, including glucose intolerance and insulin resistance. The role of the gut microbiota in GD underscores the importance of considering microbial health in managing and preventing this condition.
1.3.1. Pregnancy, and Its Impact on Gut Microbiota Composition
The microbiota, present not only in the gastrointestinal tract but also in the oral cavity, skin, lungs, and genitourinary tract, and even intrauterinely in the placenta, previously considered sterile [16], undergoes modifications during pregnancy.
Pregnancy is a unique physiological state that brings temporary changes in physical structure, hormonal levels, metabolism, and the immune system of a woman [2,4]. These changes are vital for maintaining a stable state between mother and fetus, influencing the composition of microorganisms in various areas of the pregnant woman’s body [3,4]. Moreover, physiological, hormonal, and dietary changes linked to this state also impact the likelihood of developing conditions [3,4,17,18]. Variations are observed across different trimesters of pregnancy, with a shift in the intestinal microbiota composition from the first to the second trimester [17]. At least 1,800 genera and approximately 15,000 to 36,000 species of bacteria, of which 94-98% belong to four phyla (Firmicutes (64%), Bacteroidetes (23%), Proteobacteria (8%), and Actinobacteria (3%) [17,19], specifically show an increase in the Firmicutes/Bacteroidetes ratio, among others [20]. Such changes are linked to insulin resistance and the development of GD in up to 10% of patients, which normalizes after delivery.
Temporal changes in the vaginal microbiome associated with term pregnancies have been identified, with a more homogenous microbiome dominated by Lactobacillus emerging in the second trimester [19,21]. Furthermore, an increased abundance of various taxa, including those produced by Sneathia amnii, Prevotella clades, Lachnospiraceae, and Saccharibacteria (associated with low levels of vitamin D), has been linked to the risk of preterm birth [21].
Regarding the placental microbiota, Ruiz-Treviño et al. (2023) note that the placenta contains a microbiome of low abundance but high metabolic activity, mainly composed of non-pathogenic commensal microbiota from the phyla Firmicutes, Tenericutes, Proteobacteria, Bacteroidetes, and Fusobacteria [22]. The placental microbiome profiles showed significant similarities with the oral microbiome of non-pregnant individuals. Sequence-based operational taxonomic unit analyses indicated a correlation between the placental microbiome and a history of long-term prenatal infection, as well as with preterm births before 37 weeks.
1.3.2. Drugs that Can Affect the Microbiota Used in Pregnancy.
Gut microbiota has an essential and wide role in the physiology of the human body, ranging from modulation of immune aspects to drug metabolism [23]. Several conditions, such environmental factors, diseases, drug intake, lifestyle and even pregnancy can be associated with gut microbiota alterations [24,25].
Regardless drugs, these alterations can be described as a bidirectional interaction, meaning that the drug response can be altered by the gut microbiota and the drug can modify the environment related to gut microbiota [26]. Some drug families have been described to modify this environment, including antibiotics, proton pump inhibitors, selective serotonin reuptake inhibitors, Angiotensin-converting-enzyme inhibitors (ACEIs), angiotensin-II-receptor antagonists (ARA-II), antihistamines, opiates, statins, oral contraceptives, paracetamol and metformin [23,26].
During the pregnancy, the changes in the microbiota can occur before the onset of the GD and, it must be considered carefully due to the impact in the maternal and neonatal health [17]. During pregnancy, Prevotella, Ruminococcaceae, and Parabacteroides distasonis, were shown to be increased in metagenomics studies. Even though the insulin has been the regular therapy for GD, treatment based on metformin, diet and lifestyle changing evidenced improvement in glucose levels [27,28,29]. This metformin-based treatment showed a reduction in Firmicutes and, Peptoestreptococcaceae, as well as an increase in Proteobacteria, Enterobacteriaceae and, Coprococcus catus, finding a correlation with the mean postprandial glycemia, BMI and weight increase [7].
1.4. The Microbiota and Its Intervention in the Metabolism of Antidiabetic Drugs
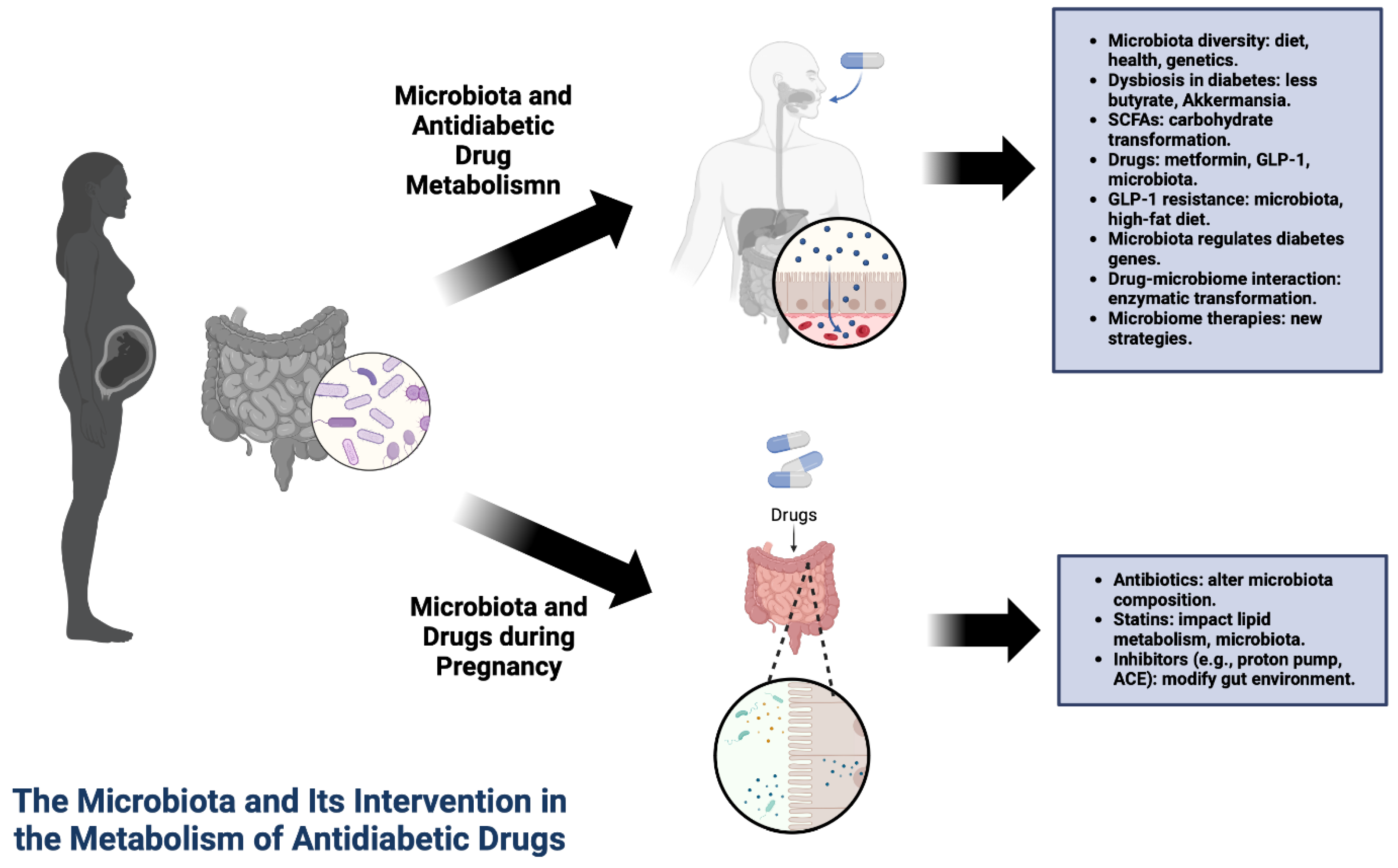
The composition and diversity of the intestinal microbiota are subject to the influence of various factors, such as diet, host health, age, ethnicity, and genetics, leading to significant variations among individuals [3,30,31]. Obesity and type 2 diabetes cause dysbiosis in the intestinal microbiota, affecting the abundance of butyrate-producing bacteria and Akkermansia muciniphila, the latter considered a biomarker for glucose intolerance [30]. Thus, the key role of the intestinal microbiota in regulating host metabolism and the associations of intestinal microbial dysbiosis with the development of obesity and diabetes [32] have been extensively explored, serving as a mediating pathway for the therapeutic effects of antidiabetic medications [26,31,32].
The intestinal microbiota plays a crucial role in transforming non-digestible carbohydrates into short-chain fatty acids (SCFAs), such as propionate, acetate, and butyrate, which in turn positively affect the action of hypoglycemic agents in type 2 diabetes [19,30]. It has been observed that hypoglycemic agents can alter the intestinal microbiota, improving glucose metabolism and energy balance [26,32,33]. Additionally, the intestinal microbiota can influence the efficacy of orally taken drugs, as microbiota enzymes can metabolize xenobiotics and affect the pharmacogenetics of medications [30,34]. Supplementation with probiotic strains and nutraceuticals has also shown health benefits in obesity and related diseases, in both animal and human studies [26,31,35]. For example, metabolites mediated by SGLT-1 produced by Lactobacillus result in increased glucose absorption in Caco-2 cells, aiding in the modulation of metformin’s glucose effects [36]. Gu et al. (2017) found that differential therapeutic responses are related to distinct abilities of microbial communities in two microbiome groups to metabolize bile acids (BA) driven by Bacteroides, compared to those belonging to a group predominantly of Prevotella [37].
Grasset et al. observed that GLP-1-induced insulin secretion and gastric emptying were disrupted in mice fed a high-fat diet, noting a deregulated intestinal microbiota that mechanically damaged the GLP-1-activated gut-brain axis, thus leading to GLP-1 resistance [38]. Translating these results, it’s possible that a deregulated microbiota could lead to resistance to GLP-1 agonist antidiabetics. Furthermore, intestinal microbes have been shown to contribute to the efficacy and safety of drugs by enzymatically transforming the structure of drugs and altering their bioavailability, bioactivity, or toxicity [34,39,40]. For example, Wang et al. (2023) found that the intestinal microbial isoenzyme Dau-d4 (a derivative of daurisoline), which selectively inhibits the activity of mDPP4 compared to hDPP4, increases active GLP-1 levels and improves glucose metabolism in diabetic mice, suggesting that variations in microbial DPP4 activities could possibly contribute to the heterogeneous responses to sitagliptin observed among patients with type 2 diabetes [41].
The composition of the intestinal microbiota also influences the regulation of various genes in T2D. Although reports are limited, they suggest a complex interaction between genes and microbes in the etiology of the disease, in addition to playing a fundamental role in the epigenetic regulation of genes by modifying DNA methylation [31]. The interaction between the human intestinal microbiome, drugs, and related xenobiotics is extremely complex and must be considered bidirectional. Based on the aforementioned connections between the intestinal microbiota and the therapeutic effects of antidiabetics, there arises the possibility of identifying new therapeutic intervention modalities aimed at the intestinal microbiome, selecting the best medication strategies and predicting the efficacy of antidiabetic drugs.
Figure 2.
Interplay between the gut microbiota and antidiabetic drug metabolism in pregnant women. This illustration depicts the influence of diet, health, genetics, and medications such as metformin and GLP-1 on microbiota diversity and function. It also highlights the potential resistance mechanisms to GLP-1 and the therapeutic interventions targeting the microbiome.
Figure 2.
Interplay between the gut microbiota and antidiabetic drug metabolism in pregnant women. This illustration depicts the influence of diet, health, genetics, and medications such as metformin and GLP-1 on microbiota diversity and function. It also highlights the potential resistance mechanisms to GLP-1 and the therapeutic interventions targeting the microbiome.
1.5. Use of Probiotics in Diabetes Gestational
Recently, probiotic supplementation has emerged as a potential strategy to mitigate some GD-associated risks, though studies show varied results. In this review, we examine the recent literature on the effects of probiotics on GD and its potential mechanisms of action. A systematic review and meta-analysis by Masulli et al. (2020) found a minor but statistically significant reduction in fasting plasma glucose, but not in the incidence of GD, suggesting probiotics may moderately impact glycemic parameters but their efficacy in preventing GD is limited [42]. Conversely, Davidson et al. (2021) highlighted an increased risk of pre-eclampsia associated with probiotic administration compared to placebo. This finding indicates a potential adverse effect of probiotics, emphasizing the need for caution and further investigation into the safety profile of probiotic supplementation during pregnancy [43].
Pakmehr et al. (2022) focused on the preventive effects of probiotics on GD occurrence. The study concluded that while probiotics might reduce the incidence of GD, the evidence is not conclusive, and no significant benefits or harms related to probiotics supplements on secondary outcomes were observed [44]. Shahriari et al. (2021) investigated the effects of probiotic supplementation from the early second trimester until the 24th week of pregnancy. The study found no significant reduction in the risk of GD or improvement in other neonatal and maternal outcomes, questioning the efficacy of probiotics in preventing GD [45]. The reviewed studies present a complex picture of the role of probiotics in managing GD. While there is some evidence to suggest that probiotics can marginally improve fasting plasma glucose (FPG) levels, their impact on reducing the incidence of GD is not substantial. Moreover, the potential risk of pre-eclampsia associated with probiotic use underscores the importance of a cautious approach to their application in pregnant populations. The variability in study outcomes highlights the need for personalized considerations, further research, and a deeper understanding of the mechanisms through which probiotics influence maternal and fetal health. Probiotic supplementation during pregnancy presents a potentially beneficial but complex intervention for managing GD. Although minor improvements in metabolic parameters has been observed, the lack of significant impact on GD incidence and potential safety concerns, such as an increased risk of pre-eclampsia, necessitate further investigation. Future studies should aim to clarify the efficacy, safety, and mechanism of action of probiotics, guiding healthcare professionals in optimizing maternal and neonatal health outcomes.
1.6. Types of Dysbiosis in Gestational Diabetes
Pregnancy itself induces significant changes in the gut microbiome, affecting various bacterial populations from the first trimester; Bifidobacterium [46], Proteobacteria, and Actinobacteria increase during pregnancy, while populations of Faecalibacterium decrease [47]. While the precise mechanisms behind these alterations are not fully described, they are suggested to result from the radical change in the hormonal profile typical of gestation, and while some alterations may lead to pathological states, others are suggested to be beneficial and necessary for fetal growth [46].
In the context of GD, a large number of studies provide evidence on the changes in the gut microbiota accompanying this metabolic alteration. Different studies have explored and identified that populations of various bacterial species increase or decrease during GD. Chen et al. described that species of the genus Firmicutes and Actinobacteria are less abundant, while those of the genus Bacteroidetes increase excessively [48]; similar results were found by Li et al. when comparing fecal microbiota between women with GD and normoglycemic women [49]. Liu Y et al. described a decrease in gut microbiota richness in GD, specifically, a decrease in Bacteroides and Akkermansia, and an increased abundance of Faecalibacterium [50]. Gammaproteobacteria and Hemophilus populations also abound in GD [51], as do Ruminococcaceae [52]. Wang et al. found abundant populations of Lachnospiraceae but a scarcity of Enterobacteriaceae and Ruminococcaceae, results that differ from those obtained by other authors [18].
It has been proposed that the microbiota not only coincides with GD but also plays a relevant role in its pathogenesis, as suggested by the findings of Crusell et al., who, when comparing the intestinal bacterial profile of women with GD and women with T2D without pregnancy, found in both an excess of colonies of bacteria from the genera Collinsella, Desulfovibrio, and Blautia [53]. Various research have shown that certain changes in bacterial colonies are related to specific mechanisms associated with the pathogenesis of GD; Faecalibacterium, Sutterella, Collinsella, and Blautia were associated with alterations in fasting glucose, insulin, Homeostasis Model Assessment of Insulin Resistance (HOMA-IR) index, and CRP levels respectively [54]. Liu et al. also associated the abundance of Faecalibacterium with a higher production of inflammatory factors and the presence of hyperglycemia [50], while Crusell et al. correlated a higher number of Christensenella with increased fasting glucose and Akkermansia with decreased insulin sensitivity [55]
Numerous studies have identified that the microbiota in GD also varies throughout pregnancy. Zheng et al. observed that, during the first trimester, the genera Acinetobacter, Bacteroides, Parabacteroides, Sphingomonas, Streptophyta, Holdemania, Haemophilus, Erysipelotrichaceae, and various species of Clostridium are more abundant. In contrast, during the second trimester (T2), bacteria from the genera Blautia, Rothia, Bilophila, Bifidobacterium, Anaerococcus, Deltaproteobacteria, and Firmicutes increase [20]. Finally, during the third trimester, Bacteroidetes, Proteobacteria, Faecalibacterium, Anaerotruncus, Collinsella, and Rothia abound, while the populations of Firmicutes and Veillonella decrease [53,56]. Similarly, it has been researched that the abundance of bacteria from the Ruminoccaceae family is directly related to the development of GD in late stages of pregnancy [52].
1.7. Effects on the Fetus
The bacterial colonization of the intestine is vitally important for the development and maturation of the offspring’s metabolic pathways; this occurs mainly through vertical transmission of maternal microbiota or during breastfeeding. Significant changes in it, such as those occurring during GD, also impact the varieties of bacteria that can be found in their offspring [57]. It has been described that the intestinal flora of newborns from mothers with GD have a greater abundance of Firmicutes and Turicibacter, while the populations of Proteobacteria, Veillonella, Megasphaera, Prevotella, Bacteroidetes, Rothia, and Actinobacteria are impoverished [55]. Su et al. conducted a similar experiment and found an increased abundance in phyla of bacteria Proteobacteria and Actinobacteria, while those of Firmicutes, Bacteroidetes, Synergistetes, Thermi, Spirochaetes, Chloroflexi, and Euryarchaeota decreased compared to the healthy control group [58]. In feces of newborns from mothers with GD, Ponzo et al. found a greater relative abundance of bacteria from the genera Bifidobacterium, Streptococcus, Staphylococcus, Escherichia, and Enterococcaceae. They also described that infants who are breastfed have a fecal microbiota with a greater abundance of Actinobacteria and Proteobacteria than those fed formula [59].
Some changes in the microbiota of neonates from pregnancies with GD affect bacterial populations that are fundamental for the development of neonatal immunity. Soderborg et al. analyzed fecal samples from newborns and found decreased colonies of Lactobacillus, Flavonifractor, Erysipelotrichaceae, and Gammaproteobacteria, bacteria that fulfill the mentioned function. At the same time, Phascolarctobacterium, a microorganism associated with the suppression of early immune system functions, was found in increased proportions [60]. These changes may predispose the newborn to inflammatory and metabolic changes in later stages of extrauterine life.
2. Materials and Methods
2.1. Search Strategy.
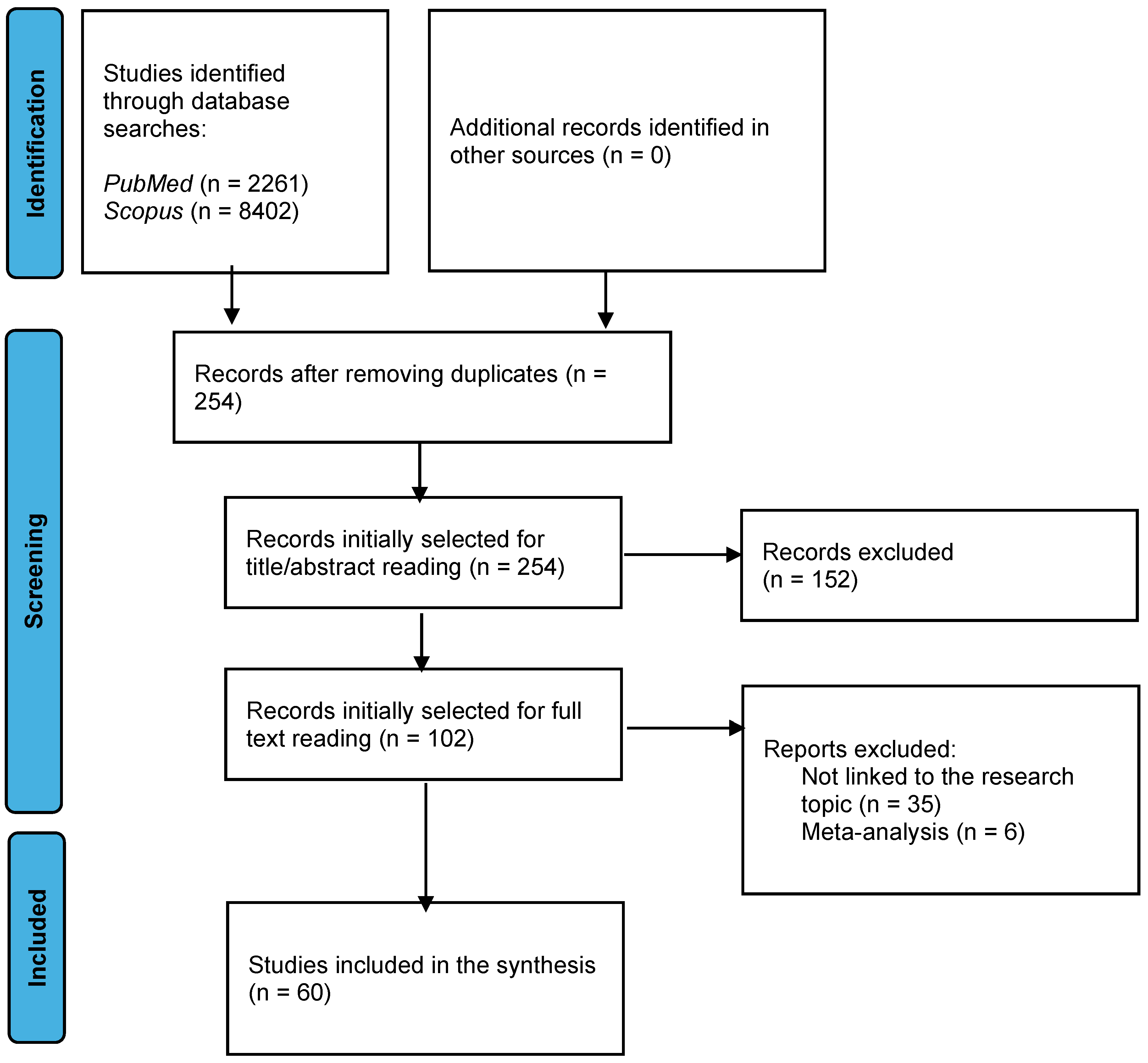
Two electronic databases (Medline/PubMed and Scopus) were systematically searched from 2017 to January 2024. The following search terms, Boolean operators and combinations were used: ‘Gestational diabetes’ OR ‘pregnan*’ AND/OR ‘ type 1 diabetes’ AND/OR ‘type 2 diabetes’ AND ‘microbiome’ OR ‘gut microbiome’ AND ‘drug metabolism’ OR ‘probiotic’.
2.2. Eligibility Criteria.
Clinical trials randomized controlled trials and reviews that provided information regarding the effects of the intestinal microbiota and its relationship with gestational diabetes were considered eligible.
Research was excluded in the case of systematic reviews and meta-analyses, and if the research was not written in English or Spanish.
2.3. Study Selection.
We examined the titles and abstracts of the identified studies to determine their eligibility. After independently reviewing the studies selected for inclusion, two authors compared them to reach agreement. Once agreement was reached, a full-text copy of each potentially relevant study was obtained. If it was unclear whether the study met the selection criteria, advice was sought from a third author and consensus was reached.
2.4. Data Extraction
The researchers extracted information on the characteristics of gestational diabetes, the microbiome and its modifications throughout pregnancy, microbiome interactions and drug metabolism.
Figure 3.
Schematic representation of the study selection process for the systematic review on the gut microbiota-gestational diabetes link. The flow diagram details the phases of identification, screening, and inclusion of the studies, reflecting the systematic approach to narrowing down the relevant literature over the past seven years.
Figure 3.
Schematic representation of the study selection process for the systematic review on the gut microbiota-gestational diabetes link. The flow diagram details the phases of identification, screening, and inclusion of the studies, reflecting the systematic approach to narrowing down the relevant literature over the past seven years.
3. Discussion
The exploration of the gut microbiota’s role in gestational diabetes (GD) unveils a complex interplay between maternal health, environmental factors, and microbial communities. This review has underscored the profound impact of gut dysbiosis on the pathogenesis of GD, illuminating potential avenues for therapeutic intervention and early detection.
3.1. Significant Findings:
Research delineates a clear divergence in the gut microbiota composition between GD-affected pregnancies and healthy controls. Notably, variations in microbial diversity and specific bacterial abundances have been linked to metabolic dysregulations inherent in GD. For instance, the reduction in the richness of Bacteroides and Akkermansia and an increase in inflammatory-inducing taxa underscore the microbiota’s contributory role in insulin resistance and glucose intolerance, foundational aspects of GD pathophysiology [50,51].
3.2. Implications for Future Research:
The dynamic nature of the gut microbiota throughout pregnancy and its influence on maternal and fetal health invites further investigation. Longitudinal studies could elucidate the temporal shifts in microbiota composition and their correlation with GD onset and progression. Additionally, the intriguing similarities between the placental microbiome and the oral microbiome of non-pregnant individuals suggest an interconnectedness that warrants exploration, particularly regarding the mechanisms of microbial transmission and colonization [22].
3.3. Clinical Applications:
Given the emerging evidence, gut microbiota modulation presents a promising strategy for GD management and prevention. Probiotic supplementation, and dietary interventions are potential modalities to restore gut microbiota balance. Moreover, identifying gut microbiota signatures that predict GD risk could guide in the early detection of these disease, an allow for timely intervention and monitoring [42,59].
3.4. Potential Limitations:
While the link between gut microbiota and GD is compelling, the field faces several limitations. The causal relationships remain to be fully elucidated. Additionally, the variability in populations, and methodologies challenges the comparability of findings and the derivation of consensus guidelines. There is also a need to address the safety and efficacy of microbiota-targeted interventions in pregnant populations, especially considering the potential risks associated with probiotic use [43].
4. Conclusions
The exploration of the gut microbiota’s role in GD has opened new horizons for understanding this complex condition. As we deepen our knowledge of the microbiome’s impact on metabolic health during pregnancy, the potential to develop novel diagnostics and therapeutic interventions grows. Future research should aim to unravel the causal mechanisms, optimize microbiota-based treatments, and establish tailored nutritional and lifestyle recommendations to mitigate GD risk, ensuring healthier outcomes for both mothers and their offspring.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, D.O.S.-R. and L.R.B.-A.; methodology, D.O.S.-R. and L.R.B.-A; validation, D.O.S.-R.; formal analysis, D.O.S.-R.; investigation, L.R.B.-A.; E.P.-D.; A.B.-R.; A.S.R.-R.; L.D.S.-A.; J.J.G.-G. and D.O.S.-R writing—original draft preparation, L.R.B.-A.; E.P.-D.; A.B.-R.; A.S.R.-R.; L.D.S.-A.; J.J.G.-G. and D.O.S.-R; writing—review and editing, D.O.S.-R. and L.R.B.-A.; visualization, L.R.B-A. and E.P.-D.; supervision, D.O.S.-R.; project administration, D.O.S.-R.; All authors have read and agreed to the published version of the manuscript.”
Funding
“This research received no external funding”.
Data Availability Statement
Not applicable.
Acknowledgments
We are grateful to Dr. Angel Emilio Suárez-Rincón for his expert advice and technical assistance, which greatly enhanced our manuscript.
Conflicts of Interest
The authors declare no conflict of interest. Figure 1 and Figure 2 were created with BioRender software (https://biorender.com/, accessed on 18 March 2024).
References
- Pascale, A.; Marchesi, N.; Marelli, C.; Coppola, A.; Luzi, L.; Govoni, S.; Giustina, A.; Gazzaruso, C. Microbiota and metabolic diseases. Endocrine 2018, 61, 357–371. [Google Scholar] [CrossRef]
- Fuhler, G. The immune system and microbiome in pregnancy. Best Pr. Res. Clin. Gastroenterol. 2020, 44-45, 101671. [Google Scholar] [CrossRef] [PubMed]
- Neri, C.; Serafino, E.; Morlando, M.; Familiari, A. Microbiome and Gestational Diabetes: Interactions with Pregnancy Outcome and Long-Term Infant Health. J. Diabetes Res. 2021, 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Jang, H.; Patoine, A.; Wu, T.T.; Castillo, D.A.; Xiao, J. Oral microflora and pregnancy: a systematic review and meta-analysis. Sci. Rep. 2021, 11, 1–31. [Google Scholar] [CrossRef]
- Iatcu, C.O.; Steen, A.; Covasa, M. Gut Microbiota and Complications of Type-2 Diabetes. Nutrients 2021, 14, 166. [Google Scholar] [CrossRef]
- Del Chierico, F.; Rapini, N.; Deodati, A.; Matteoli, M.C.; Cianfarani, S.; Putignani, L. Pathophysiology of Type 1 Diabetes and Gut Microbiota Role. Int. J. Mol. Sci. 2022, 23, 14650. [Google Scholar] [CrossRef] [PubMed]
- Bielka, W.; Przezak, A.; Pawlik, A. The Role of the Gut Microbiota in the Pathogenesis of Diabetes. Int. J. Mol. Sci. 2022, 23, 480. [Google Scholar] [CrossRef] [PubMed]
- Galicia-Garcia, U.; Benito-Vicente, A.; Jebari, S.; Larrea-Sebal, A.; Siddiqi, H.; Uribe, K.B.; Ostolaza, H.; Martín, C. Pathophysiology of Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2020, 21, 6275. [Google Scholar] [CrossRef] [PubMed]
- Slouha, E.; Rezazadah, A.; Farahbod, K.; Gerts, A.; A Clunes, L.; Kollias, T.F. Type-2 Diabetes Mellitus and the Gut Microbiota: Systematic Review. Cureus 2023, 15, e49740. [Google Scholar] [CrossRef]
- Gurung, M.; Li, Z.; You, H.; Rodrigues, R.; Jump, D.B.; Morgun, A.; Shulzhenko, N. Role of gut microbiota in type 2 diabetes pathophysiology. EBioMedicine 2020, 51, 102590. [Google Scholar] [CrossRef]
- Choudhury AA, Devi Rajeswari V. Gestational diabetes mellitus—A metabolic and reproductive disorder. Biomed Pharmacother. 2021;143:112183.
- Committee ADAPP. 15. Management of Diabetes in Pregnancy: Standards of Care in Diabetes—2024. Diabetes Care. 2023;47(Supplement_1):S282-S94.
- McIntyre HD, Catalano P, Zhang C, Desoye G, Mathiesen ER, Damm P. Gestational diabetes mellitus. Nat Rev Dis Primers. 2019;5(1):47.
- Plows, J.F.; Stanley, J.L.; Baker, P.N.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [PubMed]
- Kuang, Y.-S.; Lu, J.-H.; Li, S.-H.; Li, J.; Yuan, M.-Y.; He, J.R.; Chen, N.-N.; Xiao, W.-Q.; Shen, S.-Y.; Qiu, L.; et al. Connections between the human gut microbiome and gestational diabetes mellitus. GigaScience 2017, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Panzer, J.J.; Romero, R.; Greenberg, J.M.; Winters, A.D.; Galaz, J.; Gomez-Lopez, N.; Theis, K.R. Is there a placental microbiota? A critical review and re-analysis of published placental microbiota datasets. BMC Microbiol. 2023, 23, 1–20. [Google Scholar] [CrossRef]
- Ponzo, V.; Fedele, D.; Goitre, I.; Leone, F.; Lezo, A.; Monzeglio, C.; Finocchiaro, C.; Ghigo, E.; Bo, S. Diet-Gut Microbiota Interactions and Gestational Diabetes Mellitus (GDM). Nutrients 2019, 11, 330. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Liu, H.; Li, Y.; Huang, S.; Zhang, L.; Cao, C.; Baker, P.N.; Tong, C.; Zheng, P.; Qi, H. Altered gut bacterial and metabolic signatures and their interaction in gestational diabetes mellitus. Gut Microbes 2020, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Ziętek, M.; Celewicz, Z.; Szczuko, M. Short-Chain Fatty Acids, Maternal Microbiota and Metabolism in Pregnancy. Nutrients 2021, 13, 1244. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Xu, Q.; Huang, W.; Yan, Q.; Chen, Y.; Zhang, L.; Tian, Z.; Liu, T.; Yuan, X.; Liu, C.; et al. Gestational Diabetes Mellitus Is Associated with Reduced Dynamics of Gut Microbiota during the First Half of Pregnancy. mSystems 2020, 5. [Google Scholar] [CrossRef]
- The Integrative Human Microbiome Project. Nature. 2019;569(7758):641-8.
- Ruiz-Triviño, J.; Álvarez, D.; J. ,.P.C.; Alvarez, A.M. From gut to placenta: understanding how the maternal microbiome models life-long conditions. Front. Endocrinol. 2023, 14, 1304727. [Google Scholar] [CrossRef]
- Lindell, A.E.; Zimmermann-Kogadeeva, M.; Patil, K.R. Multimodal interactions of drugs, natural compounds and pollutants with the gut microbiota. Nat. Rev. Microbiol. 2022, 20, 431–443. [Google Scholar] [CrossRef]
- Pant, A.; Maiti, T.K.; Mahajan, D.; Das, B. Human Gut Microbiota and Drug Metabolism. Microb. Ecol. 2022, 86, 97–111. [Google Scholar] [CrossRef]
- Tang, B.; Tang, L.; Li, S.; Liu, S.; He, J.; Li, P.; Wang, S.; Yang, M.; Zhang, L.; Lei, Y.; et al. Gut microbiota alters host bile acid metabolism to contribute to intrahepatic cholestasis of pregnancy. Nat. Commun. 2023, 14, 1–17. [Google Scholar] [CrossRef]
- Weersma, R.K.; Zhernakova, A.; Fu, J. Interaction between drugs and the gut microbiome. Gut 2020, 69, 1510–1519. [Google Scholar] [CrossRef]
- Hasain, Z.; Mokhtar, N.M.; Kamaruddin, N.A.; Ismail, N.A.M.; Razalli, N.H.; Gnanou, J.V.; Ali, R.A.R. Gut Microbiota and Gestational Diabetes Mellitus: A Review of Host-Gut Microbiota Interactions and Their Therapeutic Potential. Front. Cell. Infect. Microbiol. 2020, 10, 188. [Google Scholar] [CrossRef] [PubMed]
- Molina-Vega, M.; Picón-César, M.J.; Gutiérrez-Repiso, C.; Fernández-Valero, A.; Lima-Rubio, F.; González-Romero, S.; Moreno-Indias, I.; Tinahones, F.J. Metformin action over gut microbiota is related to weight and glycemic control in gestational diabetes mellitus: A randomized trial. Biomed. Pharmacother. 2021, 145, 112465. [Google Scholar] [CrossRef]
- Mu, J.; Guo, X.; Zhou, Y.; Cao, G. The Effects of Probiotics/Synbiotics on Glucose and Lipid Metabolism in Women with Gestational Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trials. Nutrients 2023, 15, 1375. [Google Scholar] [CrossRef] [PubMed]
- Kyriachenko, Y.; Falalyeyeva, T.; Korotkyi, O.; Molochek, N.; Kobyliak, N. Crosstalk between gut microbiota and antidiabetic drug action. World J. Diabetes 2019, 10, 154–168. [Google Scholar] [CrossRef] [PubMed]
- Borse, S.P.; Chhipa, A.S.; Sharma, V.; Singh, D.P.; Nivsarkar, M. Management of Type 2 Diabetes: Current Strategies, Unfocussed Aspects, Challenges, and Alternatives. Med Princ. Pr. 2020, 30, 109–121. [Google Scholar] [CrossRef]
- Zhang, Y.; Gu, Y.; Ren, H.; Wang, S.; Zhong, H.; Zhao, X.; Ma, J.; Gu, X.; Xue, Y.; Huang, S.; et al. Gut microbiome-related effects of berberine and probiotics on type 2 diabetes (the PREMOTE study). Nat. Commun. 2020, 11, 1–12. [Google Scholar] [CrossRef]
- Induri SNR, Kansara P, Thomas SC, Xu F, Saxena D, Li X. The Gut Microbiome, Metformin, and Aging. Annu Rev Pharmacol Toxicol. 2022;62:85-108.
- Zimmermann, M.; Zimmermann-Kogadeeva, M.; Wegmann, R.; Goodman, A.L. Mapping human microbiome drug metabolism by gut bacteria and their genes. Nature 2019, 570, 462–467. [Google Scholar] [CrossRef]
- Maskarinec, G.; Raquinio, P.; Kristal, B.S.; Setiawan, V.W.; Wilkens, L.R.; Franke, A.A.; Lim, U.; Le Marchand, L.; Randolph, T.W.; Lampe, J.W.; et al. The gut microbiome and type 2 diabetes status in the Multiethnic Cohort. PLOS ONE 2021, 16, e0250855. [Google Scholar] [CrossRef]
- Bin Lee, C.; Chae, S.U.; Jo, S.J.; Jerng, U.M.; Bae, S.K. The Relationship between the Gut Microbiome and Metformin as a Key for Treating Type 2 Diabetes Mellitus. Int. J. Mol. Sci. 2021, 22, 3566. [Google Scholar] [CrossRef]
- Gu, Y.; Wang, X.; Li, J.; Zhang, Y.; Zhong, H.; Liu, R.; Zhang, D.; Feng, Q.; Xie, X.; Hong, J.; et al. Analyses of gut microbiota and plasma bile acids enable stratification of patients for antidiabetic treatment. Nat. Commun. 2017, 8, 1785. [Google Scholar] [CrossRef]
- Grasset, E.; Puel, A.; Charpentier, J.; Collet, X.; Christensen, J.E.; Tercé, F.; Burcelin, R. A Specific Gut Microbiota Dysbiosis of Type 2 Diabetic Mice Induces GLP-1 Resistance through an Enteric NO-Dependent and Gut-Brain Axis Mechanism. Cell Metab. 2017, 25, 1075–1090. [Google Scholar] [CrossRef]
- Maier, L.; Pruteanu, M.; Kuhn, M.; Zeller, G.; Telzerow, A.; Anderson, E.E.; Brochado, A.R.; Fernandez, K.C.; Dose, H.; Mori, H.; et al. Extensive impact of non-antibiotic drugs on human gut bacteria. Nature 2018, 555, 623–628. Available online: http://www.ncbi.nlm.nih.gov/pubmed/29555994 (accessed on 19 January 2019). [CrossRef] [PubMed]
- Zimmermann, M.; Zimmermann-Kogadeeva, M.; Wegmann, R.; Goodman, A.L. Separating host and microbiome contributions to drug pharmacokinetics and toxicity. Science 2019, 363, 600. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Zhang, Z.; Hang, J.; Liu, J.; Guo, F.; Ding, Y.; Li, M.; Nie, Q.; Lin, J.; Zhuo, Y.; et al. Microbial-host-isozyme analyses reveal microbial DPP4 as a potential antidiabetic target. Science 2023, 381, 501. [Google Scholar] [CrossRef] [PubMed]
- Masulli, M.; Vitacolonna, E.; Fraticelli, F.; Della Pepa, G.; Mannucci, E.; Monami, M. Effects of probiotic supplementation during pregnancy on metabolic outcomes: A systematic review and meta-analysis of randomized controlled trials. Diabetes Res. Clin. Pr. 2020, 162, 108111. [Google Scholar] [CrossRef]
- Davidson SJ, Barrett HL, Price SA, Callaway LK, Dekker Nitert M. Probiotics for preventing gestational diabetes. Cochrane Database Syst Rev. 2021;4(4):Cd009951.
- Pakmehr, A.; Ejtahed, H.-S.; Shirzad, N.; Hemmatabadi, M.; Farhat, S.; Larijani, B. Preventive effect of probiotics supplementation on occurrence of gestational diabetes mellitus: A systematic review and meta-analysis of randomized controlled trials. Front. Med. 2022, 9, 1031915. [Google Scholar] [CrossRef] [PubMed]
- Shahriari, A.; Karimi, E.; Shahriari, M.; Aslani, N.; Khooshideh, M.; Arab, A. The effect of probiotic supplementation on the risk of gestational diabetes mellitus among high-risk pregnant women: A parallel double-blind, randomized, placebo-controlled clinical trial. Biomed. Pharmacother. 2021, 141, 111915. [Google Scholar] [CrossRef]
- Nuriel-Ohayon, M.; Neuman, H.; Ziv, O.; Belogolovski, A.; Barsheshet, Y.; Bloch, N.; Uzan, A.; Lahav, R.; Peretz, A.; Frishman, S.; et al. Progesterone Increases Bifidobacterium Relative Abundance during Late Pregnancy. Cell Rep. 2019, 27, 730–736. [Google Scholar] [CrossRef]
- Ionescu, R.F.; Enache, R.M.; Cretoiu, S.M.; Gaspar, B.S. Gut Microbiome Changes in Gestational Diabetes. Int. J. Mol. Sci. 2022, 23, 12839. [Google Scholar] [CrossRef] [PubMed]
- Chen T, Zhang Y, Zhang Y, Shan C, Zhang Y, Fang K, et al. Relationships between gut microbiota, plasma glucose and gestational diabetes mellitus. J Diabetes Investig. 2021;12(4):641-50.
- Li, G.; Yin, P.; Chu, S.; Gao, W.; Cui, S.; Guo, S.; Xu, Y.; Yuan, E.; Zhu, T.; You, J.; et al. Correlation Analysis between GDM and Gut Microbial Composition in Late Pregnancy. J. Diabetes Res. 2021, 2021, 1–17. [Google Scholar] [CrossRef]
- Liu, Y.; Qin, S.; Feng, Y.; Song, Y.; Lv, N.; Liu, F.; Zhang, X.; Wang, S.; Wei, Y.; Li, S.; et al. Perturbations of gut microbiota in gestational diabetes mellitus patients induce hyperglycemia in germ-free mice. J. Dev. Orig. Heal. Dis. 2020, 11, 580–588. [Google Scholar] [CrossRef]
- Xu, Y.; Zhang, M.; Zhang, J.; Sun, Z.; Ran, L.; Ban, Y.; Wang, B.; Hou, X.; Zhai, S.; Ren, L.; et al. Differential intestinal and oral microbiota features associated with gestational diabetes and maternal inflammation. Am. J. Physiol. Metab. 2020, 319, E247–E253. [Google Scholar] [CrossRef]
- Mokkala, K.; Houttu, N.; Vahlberg, T.; Munukka, E.; Rönnemaa, T.; Laitinen, K. Gut microbiota aberrations precede diagnosis of gestational diabetes mellitus. Acta Diabetol. 2017, 54, 1147–1149. [Google Scholar] [CrossRef] [PubMed]
- Crusell, M.K.W.; Hansen, T.H.; Nielsen, T.; Allin, K.H.; Rühlemann, M.C.; Damm, P.; Vestergaard, H.; Rørbye, C.; Jørgensen, N.R.; Christiansen, O.B.; et al. Gestational diabetes is associated with change in the gut microbiota composition in third trimester of pregnancy and postpartum. Microbiome 2018, 6, 89. [Google Scholar] [CrossRef]
- Ferrocino, I.; Ponzo, V.; Gambino, R.; Zarovska, A.; Leone, F.; Monzeglio, C.; Goitre, I.; Rosato, R.; Romano, A.; Grassi, G.; et al. Changes in the gut microbiota composition during pregnancy in patients with gestational diabetes mellitus (GDM). Sci. Rep. 2018, 8, 1–13. [Google Scholar] [CrossRef]
- Crusell, M.K.W.; Hansen, T.H.; Nielsen, T.; Allin, K.H.; Rühlemann, M.C.; Damm, P.; Vestergaard, H.; Rørbye, C.; Jørgensen, N.R.; Christiansen, O.B.; et al. Comparative Studies of the Gut Microbiota in the Offspring of Mothers With and Without Gestational Diabetes. Front. Cell. Infect. Microbiol. 2020, 10, 536282. [Google Scholar] [CrossRef]
- Cui M, Qi C, Yang L, Zhang M, Wang H, She G, et al. A pregnancy complication-dependent change in SIgA-targeted microbiota during third trimester. Food Funct. 2020;11(2):1513-24.
- Li, X.; Yu, D.; Wang, Y.; Yuan, H.; Ning, X.; Rui, B.; Lei, Z.; Yuan, J.; Yan, J.; Li, M. The Intestinal Dysbiosis of Mothers with Gestational Diabetes Mellitus (GDM) and Its Impact on the Gut Microbiota of Their Newborns. Can. J. Infect. Dis. Med Microbiol. 2021, 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Nie, Y.; Shao, R.; Duan, S.; Jiang, Y.; Wang, M.; Xing, Z.; Sun, Q.; Liu, X.; Xu, W. Diversified gut microbiota in newborns of mothers with gestational diabetes mellitus. PLOS ONE 2018, 13, e0205695. [Google Scholar] [CrossRef]
- Ponzo, V.; Ferrocino, I.; Zarovska, A.; Amenta, M.B.; Leone, F.; Monzeglio, C.; Rosato, R.; Pellegrini, M.; Gambino, R.; Cassader, M.; et al. The microbiota composition of the offspring of patients with gestational diabetes mellitus (GDM). PLOS ONE 2019, 14, e0226545. [Google Scholar] [CrossRef] [PubMed]
- Soderborg, T.K.; Carpenter, C.M.; Janssen, R.C.; Weir, T.L.; Robertson, C.E.; Ir, D.; Young, B.E.; Krebs, N.F.; Hernandez, T.L.; Barbour, L.A.; et al. Gestational Diabetes Is Uniquely Associated With Altered Early Seeding of the Infant Gut Microbiota. Front. Endocrinol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Comparative overview of the gut microbiota in Type 1, Type 2, and Gd. The diagram illustrates distinctive microbial profiles associated with each diabetes type and their potential consequences on host metabolism and immune responses, emphasizing the microbiota’s role in disease mechanisms and therapeutic opportunities.
Figure 1.
Comparative overview of the gut microbiota in Type 1, Type 2, and Gd. The diagram illustrates distinctive microbial profiles associated with each diabetes type and their potential consequences on host metabolism and immune responses, emphasizing the microbiota’s role in disease mechanisms and therapeutic opportunities.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



