
Submitted:
29 March 2024
Posted:
01 April 2024
You are already at the latest version
Abstract
Drugs are known to cause substantial liver injury, with hepatotoxicity ranging from asymptomatic increase of liver enzymes to hepatic failure. HIV/AIDS patients, with compromised immune systems, are especially vulnerable to opportunistic infections such as tuberculosis (TB). Patients with co-infection frequently get combined antiretroviral (ART) and antitubercular (ATD) regimens, which can cause hepatotoxicity. Hepatotoxicity has been linked to commonly administered antiretroviral drug regimens as well as first-line antitubercular agents such isoniazid, rifampin, and pyrazinamide, which are required for the treatment of both drug-sensitive and drug-resistant tuberculosis. As a result, there is an urgent need to investigate treatments based from traditional herbs known for their hepatoprotective abilities against ART and ATD-induced liver injury. Many researchers have investigated the effectiveness of medicinal plants in treating chemically caused hepatotoxicity. Medicinal plants are high in phytochemicals and secondary metabolites, both of which have a variety of medicinal benefits. Currently, there is a lack of specific therapeutic regimens to address this adverse effect, and management often relies on symptomatic treatment or therapy withdrawal. Traditional medicinal plants may have the potential to restore normal liver function, enzyme activity, and cellular structure in response to ART and ATD-induced hepatotoxicity. This review aims to examine the scientific evidence supporting the use of medicinal plants as hepatoprotective agents against liver damage induced by ART and ATDs.
Keywords:
Medicinal Plants
; Hepatoprotection
; Hepatotoxicity
; ARV
; ATD
; Drug-induced liver toxicity
1. Introduction
The liver performs essential functions such as protein synthesis, glycogen storage, and detoxification, making it susceptible to the harmful effects of foreign substances. Over 900 drugs and chemicals have been identified as potential causes of liver damage due to their metabolism in the liver [1]. This toxicity can result in acute, sub-acute, or chronic liver diseases, characterized by cellular stress leading to cell death [2]. The "Hy’s rule" defines liver toxicity as a significant increase in serum aminotransferases and bilirubin levels, causing hepatocellular injury and jaundice, with a mortality rate of at least 10% [3,4]. Various substances, including Chinese herbal medicines, immunosuppressive agents, and antibiotics, have been linked to liver toxicity in humans [5]. The generation of free radicals and reactive oxygen species during xenobiotic metabolism is believed to underlie hepatotoxicity, resulting in a range of liver conditions from degenerative changes to hepatocellular carcinoma (HCC) [6].
Individuals with Human Immunodeficiency Virus (HIV) and acquired immunodeficiency syndrome (AIDS) are at increased risk of contracting tuberculosis (TB) due to compromised immunity. They are often prescribed treatment regimens containing the antiretroviral drug (ART) and the antitubercular drug (ATDs). Globally, around 38 million people are expected to be living with HIV by the end of 2019. People infected with HIV are 18 times more likely to acquire active tuberculosis. Tuberculosis is the most common opportunistic illness in the world and the leading cause of death among HIV-positive people [7,8,9]. While effective, the concurrent use of ART and ATDs in HIV/AIDS patients with TB co-infection has been associated with adverse effects, including fulminant and sub-hepatic failure, with reported occurrences ranging from 4.5% to 11.5% in Indian and Western populations [10,11].
The ART regimen commonly known as highly active antiretroviral therapy (HAART), includes drugs categorized into nucleoside reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), and protease inhibitors (PIs). In the treatment of tuberculosis, short-term and long-term chemotherapy often involves Isoniazid (INH) and Rifampicin (RIF), sometimes combined with Pyrazinamide (PYR), Streptomycin, or Ethambutol, depending on the severity of the disease [12]. TB remains a significant contributor to illness and death among individuals living with HIV/AIDS. The emergence of multi-drug resistant TB has further complicated this situation [10,13]. While the use of ART can slow down the advancement of HIV, it also triggers liver damage in patients, resulting in fatalities attributed to lipid imbalance, liver enlargement, and impaired liver function, as observed in both human and animal studies [14,15]. Similarly, extended use of these ATDs can lead to liver damage, including necrosis, hepatitis, jaundice, and steatosis, affecting 10 to 20% of recipients [16,17]. Similarly, the simultaneous use of Zidovudine (AZT) and INH in HIV patients co-infected with TB has been shown to result in hepatotoxicity in both human [18] and animal [11] studies. The first-line ART and ATD drugs commonly exhibit similar adverse reactions, including skin rashes, gastrointestinal discomfort, liver toxicity, symptoms affecting the central nervous system, peripheral neuropathy, and blood disorders [19].
As a result, hepatoprotective agents are being utilized to mitigate these adverse effects without introducing further harm. HIV/AIDS patients co-infected with tuberculosis commonly receive a treatment with a combination of antiretroviral and antitubercular drugs, which has been linked to hepatotoxicity in certain instances. Nonetheless, there is a lack of well-defined solutions for preventing or managing drug-induced liver toxicity in this scenario, with current treatment primarily focused on symptomatic relief. The development of a standardized therapeutic agent to address this issue is imperative. This review concentrates on the utilization of plant-derived medications to combat the hepatotoxicity associated with ART and ATDs.
2. Antiretroviral (ARV) Drugs
HAART incorporates combination of reverse-transcriptase inhibitors i.e., lamivudine, zidovudine and abacavir and protease inhibitors like indinavir and ritonavir, have been claimed to be successful in reducing the mortality and morbidity of individuals infected with HIV [20]. HAART has drastically altered the course of HIV infection by lowering the disease and death rates associated with common opportunistic infections. However, the benefits of HAART are offset by its side effects, which provide significant obstacles in managing HIV-positive persons. Liver toxicity, which is especially common in patients co-infected with hepatitis C (HCV) and/or hepatitis B (HBV), is a major issue since it commonly results in the termination of HAART. The particular processes causing HAART-induced liver damage remains unknown, limiting treatment.
2.1. Nucleoside Analogues Reverse Transcriptase Inhibitors (NRTI)
2.1.1. Zidovudine (AZT)
Zidovudine (AZT), a nucleoside analogue, is frequently employed alongside other ARV medications to prevent and treat HIV infection. It stands as the initial FDA approved drug for HIV/AIDs treatment via antiretroviral therapy [21]. AZT is prescribed for HIV patients with CD4 cell counts below 500 cells/mm3. To achieve its antiretroviral effects, the recommended daily dose of AZT in humans is 600 mg, equivalent to approximately 10 mg/kg, with a target steady-state serum concentration of 0.8μM [22]. It is also recommended for prophylaxis in HIV-exposed healthcare workers, during pregnancy and labor, and for infants (within 6 to 12 hours after birth). The dosage varies, with options including 300 mg twice daily or 200 mg three times per day, typically continued for the first few weeks of the infant's life to prevent mother-to-child transmission of HIV [23]. AZT is available in various formulations such as tablets, capsules, and injections under trade names like apo-zidovudine, retrovir, and zidosan, among others. AZT therapy for HIV has been associated with various adverse effects. Among the major concerns are haematotoxicity, hepatotoxicity, myopathy, and neurotoxicity. Common side effects experienced during AZT treatment include headaches, anemia, granulocytopenia, fatigue, malaise, nausea, and gastrointestinal discomfort. Studies have reported more severe complications such as pancytopenia, fatal lactic acidosis, peripheral neuropathy, distal symmetrical neuropathy, carcinogenicity, and bone marrow suppression [15,24,25].
2.1.2. Lamivudine (3TC)
Lamivudine (3TC), the negative (cis) enantiomer of 2′-deoxy-3′-thiacytidine, is a synthetic cytidine 2′, 3′-dideoxynucleoside analogue. Originally developed as a racemic mixture, the (-) enantiomer exhibits lower cytotoxicity and higher antiretroviral activity. It demonstrates potent inhibitory effects against both HIV-I and HIV-II viruses. Phase I and II clinical trials have indicated that 3TC monotherapy, administered at doses ranging from 2 to 20 mg/kg body weight, can improve both asymptomatic and symptomatic HIV infections in patients with CD4 counts ≤ 400 cells/ml [26]. The recommended dosage for adults and adolescents (aged 12 to 16 years; weighing ≥ 50 kg) is 150 mg taken twice daily. 3TC is typically administered in combination with zidovudine (AZT) and is not recommended as a standalone treatment [27]. Clinical studies have generally found 3TC to be well tolerated in both adults and children, although common side effects such as diarrhea, malaise, fatigue, headache, nausea, vomiting, abdominal pain, and discomfort have been reported across different dosage levels. Recent experimental research has revealed that prolonged administration of 3TC leads to increased levels of hepatotoxic and lipid marker enzymes in the plasma of rats. Additionally, the animal study suggested that prolonged administration of 3TC caused hepatotoxicity in rats [28].
2.1.3. Stavudine (d4T)
Stavudine, a thymidine analogue, is a widely recognized antiretroviral (ARV) medication known for its propensity to induce hepatotoxicity and, in severe cases, acute liver failure. Treatment with d4T can lead to mild to transient increases in liver marker enzymes, indicative of hepatotoxicity, observed in up to 50% of patients. Lactic acidosis, often associated with high mortality rates, is frequently reported in these patients [29,30]. Chronic exposure to d4T in primates has been documented to cause mitochondrial toxicity, with significant damage to hepatocyte mitochondrial DNA observed in the livers of d4T-exposed monkeys [29]. Similar to other ARV medications, d4T disrupts mitochondrial catabolic β-oxidation of free fatty acids, resulting in the accumulation of lipid droplets in liver cells, leading to severe macrovesicular steatosis and hepatomegaly [31,32].
2.2. Non-Nucleoside Analogues Reverse Transcriptase Inhibitors (NNRTI)
2.2.1 Nevirapine (NVP)
NVP is not presently recommended as part of initial anti-HIV treatment regimens [33,34]. However, it remains in use among a subset of HIV-1 patients due to its notable effectiveness, favorable metabolic characteristics, ease of use, and affordability, particularly in simplified combined antiretroviral therapy (cART) approaches [35,36]. It is routinely recommended to HIV-positive pregnant women in order to avoid transmission during pregnancy. Nevirapine-induced hepatotoxicity manifests in a variety of ways, including increased serum enzyme markers, bile duct obstruction, jaundice, hepatic necrosis, hepatitis, and hepatic failure [37]. A significant proportion of people exposed to NVP develop early and short-term hypersensitivity reactions, which can lead to hepatotoxicity and/or cutaneous side effects ranging from rashes to severe skin reactions [38,39]. Symptomatic hepatitis is clinically recorded in approximately 4% of people taking nevirapine. Hepatotoxicity development appears to be more common in females than in males. Chronic nevirapine medication in children has resulted in elevated liver enzyme markers such as AST and ALT. As a result, if patients exhibit any clinical hepatitis signs, they should discontinue their nevirapine treatment. Nevirapine, like other antiretroviral medicines, should be discontinued if serum aminotransferase levels rise, which is related with rashes [40]. Several in vivo investigations have proposed probable pathways for NVP-induced hepatotoxicity. Female Sprague Dawley rats treated with NVP at a dose of 150 mg/kg/day for 5 weeks via food treatment developed rash and liver changes [41]. Another study found that NVP (200 mg/kg/day orally) generated subclinical liver injury in rats, while plasma liver enzyme levels remained unchanged [42].
2.2.2. Efavirenz (EFV)
Efavirenz is thought to cause hepatotoxicity via interfering with bile acid transport. The liver's ability to produce bile is critical, and any disturbance in this process, such as bile duct obstruction or retention, can cause cholestasis. Retained bile in hepatocytes during cholestasis has been associated to death in these cells [43]. Studies on human and rat hepatocytes have shown that efavirenz affects bile acid transport [44]. When taken with Emtricitabine/Tenofovir, one of the principal HIV treatment medicines, efavirenz might cause hepatotoxicity, as seen by increased levels of hepatic aminotransferases [45].
Although the exact mechanisms causing Efavirenz-induced hepatotoxicity are unknown, new study suggests that mitochondrial toxicity of the drug may cause endoplasmic reticulum (ER) stress in human hepatocytes [46,47]. A recent study identified mitochondrial and ER stress as important contributors in Efavirenz-induced hepatotoxicity [48]. However, when compared to Nevirapine, the incidence of Efavirenz-induced hepatotoxicity appears to be minimal [49].
2.3. Protease Inhibitors (PIs)
PIs are an important component of HIV therapy, particularly for people who have previously received treatment. Modern PIs, including as atazanavir, darunavir, and lopinavir, are frequently coupled with low-dose ritonavir or cobicistat to improve their pharmacological effects [50]. However, PIs are known to cause side effects such as dyslipidemia, hepatotoxicity, and lipodystrophy [51]. They come with cautions for high ALT/AST values, acute hepatitis that can lead to hepatic failure, and even death, especially in people with viral hepatitis or pre-existing liver disorders.
2.3.1. Ritonavir/Lopinavir
Ritonavir, a commonly used PI, is known for its hepatotoxicity. Ritonavir, which is typically used in combination with other NRTIs or NNRTIs, has been demonstrated to reduce hepatocyte growth and induce apoptosis by activating caspase 3. The mechanism of ritonavir-induced hepatotoxicity is thought to be the stimulation of hepatocyte apoptosis via the caspase-cascade system [52]. Previous studies have shown that ritonavir inhibits bile acid transport in both human and rat hepatocytes [44]. HIV patients often suffer from numerous concurrent infections, including tuberculosis. Treatment for these co-infections often includes a combination of antitubercular drugs and antiretroviral (ARV) drugs [11,13,53]. Co-administration of ritonavir-based PIs such as saquinavir/ritonavir and rifampin in HIV-negative volunteers has been demonstrated to rapidly boost liver enzyme levels, indicating possible hepatotoxicity concerns. As a result, HIV patients should exercise caution when taking saquinavir/ritonavir in combination with rifampicin [54].
3. ARV Induced Hepatotoxicity
Liver toxicity is a significant concern associated with ART, whether used alone or in combination with other HAART drugs. Typically, these toxic effects become apparent within weeks to months after initiating treatment. ART has been linked to a range of liver-related issues, including hepatocellular necrosis, lipid droplet accumulation in liver cells, and an increase in the ratio of blood lactate to pyruvate. These adverse effects can manifest as lactic acidosis, often accompanied by hepatic abnormalities such as elevated liver enzyme markers, hepatomegaly, or hepatic steatosis and liver failure [55,56,57]. Studies have reported severity rates ranging from 5 to 10 per 100 patients, with hepatotoxicity rates reaching up to 30% in some cases of AZT-containing antiretroviral regimens [58,59]. Elevated levels of liver enzymes such as transaminases, alkaline phosphatases, bilirubin, and gamma-glutamyl transpeptidase, as well as instances of mortality, have been observed in individuals undergoing ART for HIV treatment. Liver biopsies of affected patients have shown significant micro and macrovesicular steatosis, portal and periportal fibrosis, mild mononuclear inflammatory changes, and minimal hepatocellular necrosis [60,61]. Liver abnormalities have been documented in animal models, characterized by microvesicular steatosis and mitochondrial alterations observed under electron microscopy [62]. Previous work from our lab has revealed the onset of AZT-induced degenerative changes in hepatocytes in rats receiving doses equivalent to those used in human therapy. These changes include parenchymal cell enlargement, sinusoidal space dilation, and infiltration of inflammatory cells in the liver. Additionally, elevated levels of transaminases, alkaline phosphatases, arginosuccinic acid lyase, bilirubin, and hyperlipidemia were detected in serum samples. These alterations were associated with oxidative stress parameters, indicating an imbalance in oxidative homeostasis [11,13,15]. These studies suggest that mitochondrial dysfunction or disruption of oxidant-antioxidant homeostasis may contribute to this adverse effect [60].
4. Antitubercular (ATD) Drugs
The resurgence of tuberculosis peaked in the early 1990s, coinciding with the expansion of the HIV epidemic. According to the World Health Organization, tuberculosis is the top cause of death from infectious diseases worldwide, accounting for about 214,000 deaths among HIV-positive people in 2020 [63]. Tuberculosis is still a major infectious illness, primarily affecting people in developing nations. It is a prevalent problem in India and the world's second greatest cause of mortality, killing around 1.8 million people each year [64]. The conventional treatment for tuberculosis is to deliver "first-line" medications such as Isoniazid (INH) + Rifampicin (RIF), combined with Pyrazinamide (PYR), Ethambutol, or Streptomycin, for a period of 2 to 6 months or longer, depending on disease severity. The directly observed treatment short-course (DOTS) strategy is usually recognized as the most cost-effective method of tuberculosis control [64]. However, using these medications for tuberculosis treatment can result in side effects such as hepatotoxicity, skin responses, and neurological issues. Hepatotoxicity is a major concern in chemotherapy, with reports indicating that 11.5% of the Indian population is at risk, compared to 4.3% in Western populations, and a quarter of these patients may experience severe complications such as fulminant and sub-acute hepatic failure [65,66]. Ironically, even four decades after its introduction, there is still debate about the use of INH preventive therapy for tuberculosis and co-infection with HIV due to concerns about the hepatotoxicity associated with the prescription of INH and other antitubercular drugs [67,68].
4.1. Isoniazid (INH)
Meyer and Mally produced isonicotinic acid hydrazide, often known as isoniazid (INH), in 1912, but its therapeutic potential was not discovered until 40 years later. Initial experiments in mice [69], guinea pigs, and rabbits [70] indicated bacteriostatic action against Mycobacterium tuberculosis, shedding light on its efficacy against tuberculosis. Subsequent clinical trials showed its efficacy against both pulmonary and non-pulmonary tuberculosis [71], cementing INH's position as the first choice for tuberculosis chemotherapy. INH operates by blocking the manufacture of mycolic acid, a critical component of bacterial cell walls, with the inhA gene serving as its major target [72].
INH is commonly supplied at a dose of 5 mg/kg in adults, and 10 to 20 mg/kg in children. Adult dose typically consists of a 300 mg capsule taken once daily, either one hour before or two hours after eating. Pyridoxine (15 to 50 mg/day) is used in conjunction with INH to reduce peripheral neuritis, particularly in malnourished children, HIV patients, diabetics, alcoholics, and those with uremia. Adverse responses to INH are thought to occur in 5.4% of patients, with rashes (2%), fever (1.2%), jaundice (0.6%), and peripheral neuritis (0.2%). Hepatotoxicity is the most serious toxicity associated with INH, and it can manifest as hepatic necrosis, steatosis, or a combination of the two in both humans and experimental animals [11,13,73,74].
4.2. Rifampicin (RIF)
In 1963, the Lepitet S.P.A. research laboratory in Milan, Italy, created rifampicin (RIF) [75]. It's a zwitterion and a semi-synthetic derivative. The recommended dose of RIF for tuberculosis treatment in adults is 600 mg/day orally, while children should get 10 mg/kg orally daily. RIF is available either alone or in fixed-dose combinations with INH. RIF, like INH, should not be used alone since it can cause Mycobacterium tuberculosis resistance. The occurrence of side effects with RIF is dependent on the combination in which it is delivered, particularly INH+RIF. At standard doses, fewer than 4% of tuberculosis patients experience significant adverse reactions, such as rashes (0.8%), fever (0.5%), nausea and vomiting (1.5%), and a variety of other gastrointestinal and nervous system-related symptoms such as epigastric distress, abdominal cramps, fatigue, drowsiness, headache, dizziness, ataxia, confusion, muscular weakness, and hypersensitivity reactions such as pruritus, skin eruptions, eosinophilia, and oral mucosal changes. Given the unknown potential teratogenicity of RIF and its ability to cross the placenta, it's advisable to avoid using this drug during pregnancy [76].
4.3. Pyrazinamide (PYR)
Pyrazinamide, a synthetic pyrazine analog of nicotinamide and a pro-drug, is recommended by the American Thoracic Society's Centers for Disease Control and Prevention (CDC) for preventative treatment in conjunction with two months of RIF+PYR therapy. Recent studies have shown that a 2-month regimen of PYR combined with RIF is as effective as 6 months of INH treatment in preventing tuberculosis in HIV patients [77]. The most serious adverse effect of PYR is liver damage, with signs and symptoms of hepatic disease developing in around 15% of patients receiving oral dosages of 40 to 50 mg of PYR, with necrosis leading to mortality in 2 to 3% of cases. Other side effects of PYR include arthralgias, anorexia, nausea and vomiting, dysuria, and fever. Human investigations have shown that administering RIF+PYR for two months might cause serious and deadly hepatotoxicity [77]. Compared to a 6-month regimen of INH+RIF, RIF+PYR combination therapy is linked with a higher frequency and severity of hepatotoxicity [78,79]. The reasons for the higher toxicity of RIF+PYR combinations compared to INH+RIF+PYR remain unknown. The incidence of hepatotoxicity caused by RIF+PYR therapy has been found to be between 5.3 and 13% in patients receiving these medications [78,79,80].
5. ATDs Induced Hepatotoxicity
INH has been the recommended treatment for tuberculosis since 1952, whether administered alone or in combination with other medications such as RIF, PYR, streptomycin, ethambutol, and aminosalicylic acid. Despite its effectiveness, combining INH with other anti-tubercular medications has been related to serious adverse effects such as jaundice, hepatitis, liver necrosis, hepatic coma, and even mortality in multiple studies conducted over the last few decades [81,82]. Studies reported asymptomatic liver disorders, with increased transaminase values occurring in around 10% of INH-treated patients within the first month of therapy. Subsequent research found that the frequency of INH-induced liver damage varies by individual, ranging from 8.7 to 23%, with mild or transient increases in transaminase, alkaline phosphatase, and bilirubin levels in the blood, typically appearing 2 to 6 months after starting INH treatment [83,84]. Previous studies found hepatitis in 5 to 8% of individuals receiving INH and RIF [85]. High rates of jaundice and fulminant hepatitis were recorded in both adults and children after tuberculosis treatment with these medicines. Furthermore, the combination of INH, RIF, and PYR in short-term tuberculosis treatment was related with hepatotoxic symptoms in 15% of patients, with 2 to 3% developing jaundice [16,86]. Hepatotoxicity caused by anti-tubercular medicines is now widely recognized as a serious and sometimes fatal adverse effect, especially among patients receiving active tuberculosis treatment [82]. Toxic metabolites produced by these medicines are thought to have an important role in hepatotoxicity development. RIF, for example, is hypothesized to worsen INH toxicity by boosting the synthesis of its poisonous metabolite, hydrazine, and raising CYP450 isoenzymes [87,88]. PYR administration has also been linked to antitubercular drug-induced hepatotoxicity [89].
6. HIV/AIDS Co-Infection with TB in Humans and Use of AZT and INH for Therapy
The first HAART medication sanctioned by the US FDA for managing HIV/AIDS patients is AZT, which remains fundamental in HIV treatment protocols. AZT has demonstrated favorable therapeutic outcomes in Phase-I and Phase-II clinical trials [21,90]. Tuberculosis (TB) poses a widespread epidemic, particularly concerning its control. In the late 1990s, over 4 million individuals worldwide were afflicted with acute or chronic TB, a figure that has since surged, particularly in developing regions [91]. It is estimated that one-third of the global populace is infected with Mycobacterium tuberculosis, with nearly nine million new cases and 2 million TB-related fatalities annually [92]. INH continues to be the “drug of first choice” towards the therapy of TB even today.
HIV/AIDS patients exhibit compromised immune systems, rendering them susceptible to opportunistic infections, including TB. Approximately 2.6 million HIV patients are co-infected with TB, contributing to 1.8 million HIV-related deaths globally. TB stands as a leading cause of morbidity and mortality among HIV/AIDS patients, with WHO projecting that one-third of HIV-positive individuals will develop TB during their lifetime, exacerbated by the emergence of multi-drug resistant TB strains [63]. While HAART drugs and AZT have effectively slowed HIV progression, they have also induced hepatotoxic complications in recipients [93]. AZT treatment has been associated with hepatotoxicity-related fatalities, characterized by lipid dysregulation, steatosis, steatohepatitis, hepatomegaly, and abnormal liver function [14,94]. Despite INH's proven efficacy in TB prevention, its administration has been linked to hepatic necrosis and steatosis, with approximately 15% of TB patients undergoing INH therapy experiencing hepatotoxicity, including 2 to 3% developing jaundice [86]. Combined AZT and INH treatments in HIV patients co-infected with TB have been shown to induce severe hepatotoxicity, for which remedial measures remain undefined [11,13,18] (Figure 1). Treatment strategies for drug-induced liver damage are predominantly symptomatic, lacking a standardized therapeutic regimen. The pharmacokinetics studies also affirms that AZT treatment does not exhibit any drug interaction with INH and their respective metabolites, HYD and ACHY [95]. This necessitates exploration of alternative remedies for alleviating ARV and ATDs induced hepatotoxicity in HIV patients co-infected with TB.
7. Herbal Medicine as Alternative for Drugs Induced Hepatotoxicity
Traditionally, herbal remedies have served as alternatives in healthcare systems worldwide, generally perceived as non-toxic and benign due to their natural origins [96,97]. Ayurvedha and Siddha medicinal practices, dating back over 5000 years, have been known to effectively treat a range of ailments, including liver disorders and jaundice [98]. Medicinal plants continue to be regarded as vast repositories of untapped therapeutic agents, with their molecular diversity offering promise for discovering novel compounds against drugs and chemical-induced hepatotoxicity [99,100]. Recently, there has been a resurgence in screening numerous medicinal plants to uncover pharmaceutical compounds with hepatoprotective and antioxidant properties. Various traditional medicinal plants, such as Solanum nigrum, Cichorium intybus, Picrorhiza kuroa, Curcuma longa, Camellia sinensis, and Silybum marianum etc, have been investigated for their hepatoprotective, antioxidant, and free radical scavenging abilities against drugs and chemicals that induce hepatotoxicity in experimental animals. The concept of developing a herbal treatment to prevent the liver damage induced by ARV and ATD medications is very new, and there is only a limited amount of literature on this topic. This review examines the effectiveness of herbal remedies as a possible alternative for protecting the liver from the adverse effects of these medications which are listed in Table 1.
8. Conclusion
Liver cell damage is not determined solely by the kind and dosage of a given medication. Multiple pathways contribute to the onset of liver damage and exacerbate existing injuries. Drug-induced liver damage is primarily caused by increased ROS generation, oxidative stress, and reduced immunological responses. Hepatotoxicity remains a significant cause for medications being withdrawn from the market. Despite the various benefits of modern medicine, it is frequently limited by the risk of side effects and costs, particularly in underdeveloped countries. As a result, a more effective method to addressing ART and ATD-induced liver damage could include combining traditional drugs with hepatoprotective herbs, thereby lowering the risk of hepatotoxicity while also providing alternative treatments. This review aims to compile knowledge on hepatoprotective plants in order to establish evidence-based alternative medicines to attenuate drug-induced liver damage, notably in AIDS patients co-infected with TB.
References
- Singh, O.; Garg, T.; Rath, G.; Goyal, A.K. Microbicides for the Treatment of Sexually Transmitted HIV Infections. J Pharm (Cairo) 2014, 2014, 352425. [Google Scholar] [CrossRef] [PubMed]
- Kaplowitz, N. Biochemical and Cellular Mechanisms of Toxic Liver Injury. Semin Liver Dis 2002, 22, 137–144. [Google Scholar] [CrossRef]
- Zimmerman, H.J. Drug-Induced Liver Disease. Clin Liver Dis 2000, 4, 73–96. [Google Scholar] [CrossRef] [PubMed]
- Robles-Diaz, M.; Lucena, M.I.; Kaplowitz, N.; Stephens, C.; Medina-Cáliz, I.; González-Jimenez, A.; Ulzurrun, E.; Gonzalez, A.F.; Fernandez, M.C.; Romero-Gómez, M.; et al. Use of Hy’s Law and a New Composite Algorithm to Predict Acute Liver Failure in Patients with Drug-Induced Liver Injury. Gastroenterology 2014, 147, 109–118.e5. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Wang, Z.; Fang, J.-J.; Xu, C.-Y.; Chen, W.-X. Evaluation of Prognostic Markers in Severe Drug-Induced Liver Disease. World J Gastroenterol 2007, 13, 628–632. [Google Scholar] [CrossRef]
- Zimmerman, H.J. Hepatotoxicity. Dis Mon 1993, 39, 675–787. [Google Scholar]
- Organization, WH. HIV/AIDS. Geneva. 2020 [Accessed on 2024 Mar 24]. Available from: Https://Www.Who.
- Girardi, E.; Sabin, C.A.; d’Arminio Monforte, A.; Hogg, B.; Phillips, A.N.; Gill, M.J.; Dabis, F.; Reiss, P.; Kirk, O.; Bernasconi, E.; et al. Incidence of Tuberculosis among HIV-Infected Patients Receiving Highly Active Antiretroviral Therapy in Europe and North America. Clin Infect Dis 2005, 41, 1772–1782. [Google Scholar] [CrossRef] [PubMed]
- 9. World Health Organization. GLOBAL TB REPORT 2016 WITH HIV + TB, 2016.
- Onyebujoh, P. An Evaluation of the Impact of Early Initiation of Highly Active Anti-Retroviral Therapy (HAART) on Tuberculosis (TB) Treatment Outcomes for TB Patients Co-Infected with Human Immunodeficiency Virus (HIV) 2014.
- Raghu, R.; Karthikeyan, S. Zidovudine and Isoniazid Induced Liver Toxicity and Oxidative Stress: Evaluation of Mitigating Properties of Silibinin. Environ Toxicol Pharmacol 2016, 46, 217–226. [Google Scholar] [CrossRef]
- Nahid, P.; Dorman, S.E.; Alipanah, N.; Barry, P.M.; Brozek, J.L.; Cattamanchi, A.; Chaisson, L.H.; Chaisson, R.E.; Daley, C.L.; Grzemska, M.; et al. Official American Thoracic Society/Centers for Disease Control and Prevention/Infectious Diseases Society of America Clinical Practice Guidelines: Treatment of Drug-Susceptible Tuberculosis. Clin Infect Dis 2016, 63, e147–e195. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, R.; Sivanesan, K. Evaluation of Ameliorative Ability of Silibinin against Zidovudine and Isoniazid-Induced Hepatotoxicity and Hyperlipidaemia in Rats: Role of Silibinin in Phase I and II Drug Metabolism. Chem Biol Interact 2017, 273, 142–153. [Google Scholar] [CrossRef]
- Shah, I. Adverse Effects of Antiretroviral Therapy in HIV-1 Infected Children. J Trop Pediatr 2006, 52, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Raghu, R.; Jesudas, B.; Bhavani, G.; Ezhilarasan, D.; Karthikeyan, S. Silibinin Mitigates Zidovudine-Induced Hepatocellular Degenerative Changes, Oxidative Stress and Hyperlipidaemia in Rats. Hum Exp Toxicol 2015, 34, 1031–1042. [Google Scholar] [CrossRef] [PubMed]
- van Hest, R.; Baars, H.; Kik, S.; van Gerven, P.; Trompenaars, M.-C.; Kalisvaart, N.; Keizer, S.; Borgdorff, M.; Mensen, M.; Cobelens, F. Hepatotoxicity of Rifampin-Pyrazinamide and Isoniazid Preventive Therapy and Tuberculosis Treatment. Clin Infect Dis 2004, 39, 488–496. [Google Scholar] [CrossRef]
- Yee, D.; Valiquette, C.; Pelletier, M.; Parisien, I.; Rocher, I.; Menzies, D. Incidence of Serious Side Effects from First-Line Antituberculosis Drugs among Patients Treated for Active Tuberculosis. Am J Respir Crit Care Med 2003, 167, 1472–1477. [Google Scholar] [CrossRef] [PubMed]
- Awodele, O.; Agbaje, E.O.; Adesina, E.A.; Akintonwa, A. Hepatoprotective Role of neutrosecR on Hepatic Damage Induced by Combination of Zidovudine and Combined Anti-Tuberculous Agents in Rats. Tokai J Exp Clin Med 2011, 36, 31–36. [Google Scholar] [PubMed]
- Dean, G.L.; Edwards, S.G.; Ives, N.J.; Matthews, G.; Fox, E.F.; Navaratne, L.; Fisher, M.; Taylor, G.P.; Miller, R.; Taylor, C.B.; et al. Treatment of Tuberculosis in HIV-Infected Persons in the Era of Highly Active Antiretroviral Therapy. AIDS 2002, 16, 75–83. [Google Scholar] [CrossRef]
- Palella, F.J.; Delaney, K.M.; Moorman, A.C.; Loveless, M.O.; Fuhrer, J.; Satten, G.A.; Aschman, D.J.; Holmberg, S.D. Declining Morbidity and Mortality among Patients with Advanced Human Immunodeficiency Virus Infection. HIV Outpatient Study Investigators. N Engl J Med 1998, 338, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Fischl, M.A.; Richman, D.D.; Grieco, M.H.; Gottlieb, M.S.; Volberding, P.A.; Laskin, O.L.; Leedom, J.M.; Groopman, J.E.; Mildvan, D.; Schooley, R.T. The Efficacy of Azidothymidine (AZT) in the Treatment of Patients with AIDS and AIDS-Related Complex. A Double-Blind, Placebo-Controlled Trial. N Engl J Med 1987, 317, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, C.V.; Anderson, P.L.; Kakuda, T.N.; Schacker, T.W.; Henry, K.; Gross, C.R.; Brundage, R.C. Concentration-Controlled Compared with Conventional Antiretroviral Therapy for HIV Infection. AIDS 2002, 16, 551–560. [Google Scholar] [CrossRef]
- Chasela, C.S.; Hudgens, M.G.; Jamieson, D.J.; Kayira, D.; Hosseinipour, M.C.; Kourtis, A.P.; Martinson, F.; Tegha, G.; Knight, R.J.; Ahmed, Y.I.; et al. Maternal or Infant Antiretroviral Drugs to Reduce HIV-1 Transmission. N Engl J Med 2010, 362, 2271–2281. [Google Scholar] [CrossRef]
- Lewis, W.; Day, B.J.; Copeland, W.C. Mitochondrial Toxicity of NRTI Antiviral Drugs: An Integrated Cellular Perspective. Nat Rev Drug Discov 2003, 2, 812–822. [Google Scholar] [CrossRef] [PubMed]
- Torres, S.M.; Walker, D.M.; Carter, M.M.; Cook, D.L.; McCash, C.L.; Cordova, E.M.; Olivero, O.A.; Poirier, M.C.; Walker, V.E. Mutagenicity of Zidovudine, Lamivudine, and Abacavir Following in Vitro Exposure of Human Lymphoblastoid Cells or in Utero Exposure of CD-1 Mice to Single Agents or Drug Combinations. Environ Mol Mutagen 2007, 48, 224–238. [Google Scholar] [CrossRef] [PubMed]
- van Leeuwen, R.; Katlama, C.; Kitchen, V.; Boucher, C.A.; Tubiana, R.; McBride, M.; Ingrand, D.; Weber, J.; Hill, A.; McDade, H. Evaluation of Safety and Efficacy of 3TC (Lamivudine) in Patients with Asymptomatic or Mildly Symptomatic Human Immunodeficiency Virus Infection: A Phase I/II Study. J Infect Dis 1995, 171, 1166–1171. [Google Scholar] [CrossRef] [PubMed]
- Perry, C.M.; Faulds, D. Lamivudine. A Review of Its Antiviral Activity, Pharmacokinetic Properties and Therapeutic Efficacy in the Management of HIV Infection. Drugs 1997, 53, 657–680. [Google Scholar] [CrossRef] [PubMed]
- Olaniyan, L.W.B.; Maduagwu, E.N.; Akintunde, O.W.; Oluwayelu, O.O.; Brai, B.I.C. Lamivudine-Induced Liver Injury. Open Access Maced J Med Sci 2015, 3, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Gerschenson, M.; Nguyen, V.T.; St Claire, M.C.; Harbaugh, S.W.; Harbaugh, J.W.; Proia, L.A.; Poirier, M.C. Chronic Stavudine Exposure Induces Hepatic Mitochondrial Toxicity in Adult Erythrocebus Patas Monkeys. J Hum Virol 2001, 4, 335–342. [Google Scholar] [PubMed]
- Lea, A.P.; Faulds, D. Stavudine: A Review of Its Pharmacodynamic and Pharmacokinetic Properties and Clinical Potential in HIV Infection. Drugs 1996, 51, 846–864. [Google Scholar] [CrossRef]
- Johri, S.; Alkhuja, S.; Siviglia, G.; Soni, A. Steatosis-Lactic Acidosis Syndrome Associated with Stavudine and Lamivudine Therapy. AIDS 2000, 14, 1286–1287. [Google Scholar] [CrossRef] [PubMed]
- Devaraj, E.; Mohan, S.; Ramanathan, R. HAART and Hepatotoxicity. J App Pharma Sci 2017. [Google Scholar] [CrossRef]
- European AIDS Clinical Society (EACS) Guidelines for the Treatment of Adult HIV-Positive Persons. Version 10.1. October 2020.
- Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIVS.
- Reliquet, V.; Allavena, C.; Morineau-Le Houssine, P.; Mounoury, O.; Raffi, F. Twelve-Year Experience of Nevirapine Use: Benefits and Convenience for Long-Term Management in a French Cohort of HIV-1-Infected Patients. HIV Clin Trials 2010, 11, 110–117. [Google Scholar] [CrossRef]
- de Boissieu, P.; Dramé, M.; Raffi, F.; Cabie, A.; Poizot-Martin, I.; Cotte, L.; Garraffo, R.; Delobel, P.; Huleux, T.; Rey, D.; et al. Long-Term Efficacy and Toxicity of Abacavir/Lamivudine/Nevirapine Compared to the Most Prescribed ARV Regimens before 2013 in a French Nationwide Cohort Study. Medicine (Baltimore) 2016, 95, e4890. [Google Scholar] [CrossRef] [PubMed]
- Hitti, J.; Frenkel, L.M.; Stek, A.M.; Nachman, S.A.; Baker, D.; Gonzalez-Garcia, A.; Provisor, A.; Thorpe, E.M.; Paul, M.E.; Foca, M.; et al. Maternal Toxicity With Continuous Nevirapine in Pregnancy: Results From PACTG 1022. JAIDS Journal of Acquired Immune Deficiency Syndromes 2004, 36, 772–776. [Google Scholar] [CrossRef]
- Gao, S.; Gui, X.; Deng, L.; Zhang, Y.; Liang, K.; Yang, R.; Yan, Y.; Rong, Y. Antiretroviral Therapy Hepatotoxicity: Prevalence, Risk Factors, and Clinical Characteristics in a Cohort of Han Chinese. Hepatology Research 2010, 40, 287–294. [Google Scholar] [CrossRef]
- Patel, S.M.; Johnson, S.; Belknap, S.M.; Chan, J.; Sha, B.E.; Bennett, C. Serious Adverse Cutaneous and Hepatic Toxicities Associated with Nevirapine Use by Non-HIV-Infected Individuals. J Acquir Immune Defic Syndr 2004, 35, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Ajulo, M.O.; Omole, M.K.; Moody, J.O.; Dixon-Umo, O.T.; Salami, O.L. Liver Aminotransferases in Under-Five HIV-Positive Children on HAART. Afr J Med Med Sci 2015, 44, 197–204. [Google Scholar] [PubMed]
- Shenton, J.M.; Teranishi, M.; Abu-Asab, M.S.; Yager, J.A.; Uetrecht, J.P. Characterization of a Potential Animal Model of an Idiosyncratic Drug Reaction: Nevirapine-Induced Skin Rash in the Rat. Chem Res Toxicol 2003, 16, 1078–1089. [Google Scholar] [CrossRef]
- Bekker, Z.; Walubo, A.; du Plessis, J.B. The Role of the Immune System in Nevirapine-Induced Subclinical Liver Injury of a Rat Model. ISRN Pharm 2012, 2012, 932542. [Google Scholar] [CrossRef]
- Patel, T.; Roberts, L.R.; Jones, B.A.; Gores, G.J. Dysregulation of Apoptosis as a Mechanism of Liver Disease: An Overview. Semin Liver Dis 1998, 18, 105–114. [Google Scholar] [CrossRef]
- McRae, M.P.; Lowe, C.M.; Tian, X.; Bourdet, D.L.; Ho, R.H.; Leake, B.F.; Kim, R.B.; Brouwer, K.L.R.; Kashuba, A.D.M. Ritonavir, Saquinavir, and Efavirenz, but Not Nevirapine, Inhibit Bile Acid Transport in Human and Rat Hepatocytes. J Pharmacol Exp Ther 2006, 318, 1068–1075. [Google Scholar] [CrossRef]
- Patil, R.; Ona, M.A.; Papafragkakis, H.; Carey, J.; Moshenyat, Y.; Alhaddad, A.; Anand, S. Acute Liver Toxicity Due to Efavirenz/Emtricitabine/Tenofovir. Case Reports Hepatol 2015, 2015, 280353. [Google Scholar] [CrossRef] [PubMed]
- Apostolova, N.; Gomez-Sucerquia, L.J.; Alegre, F.; Funes, H.A.; Victor, V.M.; Barrachina, M.D.; Blas-Garcia, A.; Esplugues, J.V. ER Stress in Human Hepatic Cells Treated with Efavirenz: Mitochondria Again. J Hepatol 2013, 59, 780–789. [Google Scholar] [CrossRef]
- Gwag, T.; Meng, Z.; Sui, Y.; Helsley, R.N.; Park, S.-H.; Wang, S.; Greenberg, R.N.; Zhou, C. Non-Nucleoside Reverse Transcriptase Inhibitor Efavirenz Activates PXR to Induce Hypercholesterolemia and Hepatic Steatosis. Journal of Hepatology 2019, 70, 930–940. [Google Scholar] [CrossRef] [PubMed]
- Polo, M.; Alegre, F.; Funes, H.A.; Blas-Garcia, A.; Victor, V.M.; Esplugues, J.V.; Apostolova, N. Mitochondrial (Dys)Function - a Factor Underlying the Variability of Efavirenz-Induced Hepatotoxicity? Br J Pharmacol 2015, 172, 1713–1727. [Google Scholar] [CrossRef] [PubMed]
- Sonderup, M.W.; Maughan, D.; Gogela, N.; Setshedi, M.; Wainwright, H.; Meintjes, G.; Spearman, W. Identification of a Novel and Severe Pattern of Efavirenz Drug-Induced Liver Injury in South Africa. AIDS 2016, 30, 1483–1485. [Google Scholar] [CrossRef] [PubMed]
- Sulkowski, M.S.; Thomas, D.L.; Chaisson, R.E.; Moore, R.D. Hepatotoxicity Associated with Antiretroviral Therapy in Adults Infected with Human Immunodeficiency Virus and the Role of Hepatitis C or B Virus Infection. JAMA 2000, 283, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Tsiodras, S.; Mantzoros, C.; Hammer, S.; Samore, M. Effects of Protease Inhibitors on Hyperglycemia, Hyperlipidemia, and Lipodystrophy: A 5-Year Cohort Study. Arch Intern Med 2000, 160, 2050–2056. [Google Scholar] [CrossRef] [PubMed]
- Kuang, C.-C.; Wang, Y.; Hu, P.-C.; Gao, F.-F.; Bu, L.; Wen, X.-M.; Xiang, Q.-M.; Song, H.; Li, Q.; Wei, L.; et al. Ritonavir-Induced Hepatotoxicity and Ultrastructural Changes of Hepatocytes. Ultrastruct Pathol 2014, 38, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Mchunu, G.; van Griensven, J.; Hinderaker, S.G.; Kizito, W.; Sikhondze, W.; Manzi, M.; Dlamini, T.; Harries, A.D. High Mortality in Tuberculosis Patients despite HIV Interventions in Swaziland. Public Health Action 2016, 6, 105–110. [Google Scholar] [CrossRef]
- Schmitt, C.; Riek, M.; Winters, K.; Schutz, M.; Grange, S. Unexpected Hepatotoxicity of Rifampin and Saquinavir/Ritonavir in Healthy Male Volunteers. Arch Drug Inf 2009, 2, 8–16. [Google Scholar] [CrossRef]
- Neff, G.W.; Jayaweera, D.; Sherman, K.E. Drug-Induced Liver Injury in HIV Patients. Gastroenterol Hepatol (N Y) 2006, 2, 430–437. [Google Scholar]
- Benedicto, A.M.; Fuster-Martínez, I.; Tosca, J.; Esplugues, J.V.; Blas-García, A.; Apostolova, N. NNRTI and Liver Damage: Evidence of Their Association and the Mechanisms Involved. Cells 2021, 10, 1687. [Google Scholar] [CrossRef]
- Fortgang, I.S.; Belitsos, P.C.; Chaisson, R.E.; Moore, R.D. Hepatomegaly and Steatosis in HIV-Infected Patients Receiving Nucleoside Analog Antiretroviral Therapy. Am J Gastroenterol 1995, 90, 1433–1436. [Google Scholar]
- Martínez, E.; Blanco, J.L.; Arnaiz, J.A.; Pérez-Cuevas, J.B.; Mocroft, A.; Cruceta, A.; Marcos, M.A.; Milinkovic, A.; García-Viejo, M.A.; Mallolas, J.; et al. Hepatotoxicity in HIV-1-Infected Patients Receiving Nevirapine-Containing Antiretroviral Therapy. AIDS 2001, 15, 1261–1268. [Google Scholar] [CrossRef]
- Wit, F.W.N.M.; Weverling, G.J.; Weel, J.; Jurriaans, S.; Lange, J.M.A. Incidence of and Risk Factors for Severe Hepatotoxicity Associated with Antiretroviral Combination Therapy. J Infect Dis 2002, 186, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Chariot, P.; Drogou, I.; de Lacroix-Szmania, I.; Eliezer-Vanerot, M.C.; Chazaud, B.; Lombès, A.; Schaeffer, A.; Zafrani, E.S. Zidovudine-Induced Mitochondrial Disorder with Massive Liver Steatosis, Myopathy, Lactic Acidosis, and Mitochondrial DNA Depletion. J Hepatol 1999, 30, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Gradon, J.D.; Chapnick, E.K.; Sepkowitz, D.V. Zidovudine-Induced Hepatitis. J Intern Med 1992, 231, 317–318. [Google Scholar] [CrossRef] [PubMed]
- Corcuera, T.; Alonso, M.J.; Picazo, A.; Gómez, F.; Roldán, M.; Abad, M.; Muñoz, E.; López-Bravo, A. Hepatic Morphological Alterations Induced by Zidovudine (ZDV) in an Experimental Model. Pathol Res Pract 1996, 192, 182–187. [Google Scholar] [CrossRef]
- 63. Global Tuberculosis Report 2021.[Accessed on 2024 Mar 24]. Available from: Https://Www.Who.Int/Publications/i/Item/9789240037021.
- 64. Global Tuberculosis Control : Surveillance, Planning, Financing : WHO Report 2007. [Accessed on 2024 Mar 24]. Available from:Https://Www.Who.Int/Publications/i/Item/9789241563141.
- Anand, A.C.; Seth, A.K.; Paul, M.; Puri, P. Risk Factors of Hepatotoxicity During Anti-Tuberculosis Treatment. Med J Armed Forces India 2006, 62, 45–49. [Google Scholar] [CrossRef]
- Adhvaryu, M.R.; Reddy, N.; Vakharia, B.C. Prevention of Hepatotoxicity Due to Anti Tuberculosis Treatment: A Novel Integrative Approach. World J Gastroenterol 2008, 14, 4753–4762. [Google Scholar] [CrossRef]
- Sarasin, F.P.; Perrier, A.; Rochat, T. Isoniazid Preventive Therapy for Pulmonary Tuberculosis Sequelae: Which Patients up to Which Age? Tuber Lung Dis 1995, 76, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Israel, H.L.; Gottlieb, J.E.; Maddrey, W.C. Perspective: Preventive Isoniazid Therapy and the Liver. Chest 1992, 101, 1298–1301. [Google Scholar] [CrossRef] [PubMed]
- Grunberg, E.; Schnitzer, R.J. Studies on the Activity of Hydrazine Derivatives of Isonicotinic Acid in the Experimental Tuberculosis of Mice. Q Bull Sea View Hosp 1952, 13, 3–11. [Google Scholar] [PubMed]
- Steenken, W.; Wolinsky, E. Antituberculous Properties of Hydrazines of Isonicotinic Acid (Rimifon, Marsilid). Am Rev Tuberc 1952, 65, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Robitzek, E.H.; Selikoff, I.J. Hydrazine Derivatives of Isonicotinic Acid (Rimifon Marsilid) in the Treatment of Active Progressive Caseous-Pneumonic Tuberculosis; a Preliminary Report. Am Rev Tuberc 1952, 65, 402–428. [Google Scholar] [CrossRef] [PubMed]
- Vilchèze, C.; Morbidoni, H.R.; Weisbrod, T.R.; Iwamoto, H.; Kuo, M.; Sacchettini, J.C.; Jacobs, W.R. Inactivation of the inhA-Encoded Fatty Acid Synthase II (FASII) Enoyl-Acyl Carrier Protein Reductase Induces Accumulation of the FASI End Products and Cell Lysis of Mycobacterium Smegmatis. J Bacteriol 2000, 182, 4059–4067. [Google Scholar] [CrossRef]
- Selvaraj, H.; Dhamothrasamy, K.; Duraisamy, K.; Dhanasekaran, M. Isoniazid-Induced Hepatic Injury: A Case Report and Its Mechanism of Liver Injury. J Adv Pharm Educ Res 2022, 12, 1–5. [Google Scholar] [CrossRef]
- Nolan, C.M.; Goldberg, S.V.; Buskin, S.E. Hepatotoxicity Associated with Isoniazid Preventive Therapy: A 7-Year Survey from a Public Health Tuberculosis Clinic. JAMA 1999, 281, 1014–1018. [Google Scholar] [CrossRef]
- Fueresz, S.; Timbal, M.T. ANTIBACTERIAL ACTIVITY OF RIFAMYCINS. Chemotherapia (Basel) 1963, 257, 200–208. [Google Scholar] [CrossRef]
- Grosset, J.; Leventis, S. Adverse Effects of Rifampin. Rev Infect Dis 1983, 5 Suppl 3, S440–450. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC) Update: Fatal and Severe Liver Injuries Associated with Rifampin and Pyrazinamide for Latent Tuberculosis Infection, and Revisions in American Thoracic Society/CDC Recommendations--United States, 2001. MMWR Morb Mortal Wkly Rep 2001, 50, 733–735.
- McNeill, L.; Allen, M.; Estrada, C.; Cook, P. Pyrazinamide and Rifampin vs Isoniazid for the Treatment of Latent Tuberculosis: Improved Completion Rates but More Hepatotoxicity. Chest 2003, 123, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Stout, J.E.; Engemann, J.J.; Cheng, A.C.; Fortenberry, E.R.; Hamilton, C.D. Safety of 2 Months of Rifampin and Pyrazinamide for Treatment of Latent Tuberculosis. Am J Respir Crit Care Med 2003, 167, 824–827. [Google Scholar] [CrossRef]
- Hussain, Z.; Zhu, J.; Ma, X. Metabolism and Hepatotoxicity of Pyrazinamide, an Antituberculosis Drug. Drug Metab Dispos 2021, 49, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Lei, S.; Gu, R.; Ma, X. Clinical Perspectives of Isoniazid-Induced Liver Injury. Liver Research 2021, 5, 45–52. [Google Scholar] [CrossRef]
- Ramappa, V.; Aithal, G.P. Hepatotoxicity Related to Anti-Tuberculosis Drugs: Mechanisms and Management. J Clin Exp Hepatol 2013, 3, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Philipose, J.; Suchman, K.I.; Aronsky, D.; Lee, T.-P. A Case of Acute Liver Failure in a Patient on Isoniazid Prophylaxis for Latent Tuberculosis. Cureus 2022, 14, e22452. [Google Scholar] [CrossRef] [PubMed]
- Malakouti, M.; Kataria, A.; Ali, S.K.; Schenker, S. Elevated Liver Enzymes in Asymptomatic Patients - What Should I Do? J Clin Transl Hepatol 2017, 5, 394–403. [Google Scholar] [CrossRef] [PubMed]
- Lees, A.W.; Allan, G.W.; Smith, J.; Tyrrell, W.F.; Fallon, R.J. Toxicity Form Rifampicin plus Isoniazid and Rifampicin plus Ethambutol Therapy. Tubercle 1971, 52, 182–190. [Google Scholar] [CrossRef]
- Pilheu, J.A.; de Salvo, M.C.; Koch, O.; Barcat, J.A. [Light and electron microscopy studies of the liver in tuberculosis patients receiving rifampin and isoniazid]. Medicina (B Aires) 1981, 41, 439–445. [Google Scholar]
- Lee, W.M. Drug-Induced Hepatotoxicity. N Engl J Med 1995, 333, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Sarma, G.R.; Immanuel, C.; Kailasam, S.; Narayana, A.S.; Venkatesan, P. Rifampin-Induced Release of Hydrazine from Isoniazid. A Possible Cause of Hepatitis during Treatment of Tuberculosis with Regimens Containing Isoniazid and Rifampin. Am Rev Respir Dis 1986, 133, 1072–1075. [Google Scholar] [CrossRef] [PubMed]
- Tostmann, A.; Boeree, M.J.; Peters, W.H.M.; Roelofs, H.M.J.; Aarnoutse, R.E.; van der Ven, A.J.A.M.; Dekhuijzen, P.N.R. Isoniazid and Its Toxic Metabolite Hydrazine Induce in Vitro Pyrazinamide Toxicity. Int J Antimicrob Agents 2008, 31, 577–580. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, R.; Klecker, R.W.; Weinhold, K.J.; Markham, P.D.; Lyerly, H.K.; Durack, D.T.; Gelmann, E.; Lehrman, S.N.; Blum, R.M.; Barry, D.W. Administration of 3’-Azido-3’-Deoxythymidine, an Inhibitor of HTLV-III/LAV Replication, to Patients with AIDS or AIDS-Related Complex. Lancet 1986, 1, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Zuber, P.L.; McKenna, M.T.; Binkin, N.J.; Onorato, I.M.; Castro, K.G. Long-Term Risk of Tuberculosis among Foreign-Born Persons in the United States. JAMA 1997, 278, 304–307. [Google Scholar] [CrossRef]
- Corbett, E.L.; Watt, C.J.; Walker, N.; Maher, D.; Williams, B.G.; Raviglione, M.C.; Dye, C. The Growing Burden of Tuberculosis: Global Trends and Interactions with the HIV Epidemic. Arch Intern Med 2003, 163, 1009–1021. [Google Scholar] [CrossRef] [PubMed]
- Dubin, G.; Braffman, M.N. Zidovudine-Induced Hepatotoxicity. Ann Intern Med 1989, 110, 85–86. [Google Scholar] [CrossRef]
- Acosta, B.S.; Grimsley, E.W. Zidovudine-Associated Type B Lactic Acidosis and Hepatic Steatosis in an HIV-Infected Patient. South Med J 1999, 92, 421–423. [Google Scholar] [CrossRef]
- Ramanathan, R.; Sivanesan, K. Investigations on the Influence of Zidovudine in the Pharmacokinetics of Isoniazid and Its Hepatotoxic Metabolites in Rats. J Pharm Pract 2019, 32, 9–18. [Google Scholar] [CrossRef]
- Sheldon, J.W.; Michael, B.; Sarah, L.; George, M. Medicinal Plants: Can Utilization and Conservation Coexist?”. In Advances in Economic Botany; 1997; Vol. 12.
- Deng, J.F.; Lin, T.J.; Kao, W.F.; Chen, S.S. The Difficulty in Handling Poisonings Associated with Chinese Traditional Medicine: A Poison Control Center Experience for 1991-1993. Vet Hum Toxicol 1997, 39, 106–114. [Google Scholar]
- Chandrakumar, A.; Xavier, A.; Xavier, A.; Manakkadiyil, A.; Reghu, A.; Thomas, L. Implications of Traditional Medicine in the Treatment of Hepatitis A in Kerala. J Tradit Complement Med 2016, 6, 316–320. [Google Scholar] [CrossRef] [PubMed]
- Mangwani, N.; Singh, P.K.; Kumar, V. Medicinal Plants: Adjunct Treatment to Tuberculosis Chemotherapy to Prevent Hepatic Damage. J Ayurveda Integr Med 2020, 11, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Wainwright, C.L.; Teixeira, M.M.; Adelson, D.L.; Braga, F.C.; Buenz, E.J.; Campana, P.R.V.; David, B.; Glaser, K.B.; Harata-Lee, Y.; Howes, M.-J.R.; et al. Future Directions for the Discovery of Natural Product-Derived Immunomodulating Drugs: An IUPHAR Positional Review. Pharmacological Research 2022, 177, 106076. [Google Scholar] [CrossRef]
- Ogunlade, B.; Jeje, S.O.; Adelakun, S.A.; Akingbade, G.T. Moringa Oleifera Restored Semen Quality, Hormonal Profile, and Testicular Morphology against Highly Active Antiretroviral Therapy-Induced Toxicity in Adult Male Wistar Rats. JBRA Assist Reprod 2022, 26, 3–12. [Google Scholar] [CrossRef]
- Enyang, D.; Sonibare, M.A.; Tchamgoue, A.D.; Tchokouaha, L.R.Y.; Yadang, F.S.; Nfor, G.N.; Kom, C.W.; Betote, P.D.H.; Tchinda, C.F.; Tiogo, S.S.K.; et al. Protective and Ameliorative Effects of Hydroethanolic Extract of Piper Nigrum (L.) Stem against Antiretroviral Therapy-Induced Hepatotoxicity and Dyslipidemia in Wistar Rats. J Toxicol 2024, 2024, 5811080. [Google Scholar] [CrossRef] [PubMed]
- Amujal, M.; Ikwap, K.; Tamale, A.; Tumwine, G.; Kateregga, J.; Wamala, S.P.; Kato, C.D. Hepatoprotective Effect of Cymbopogon Citratus Essential Oils against Nevirapine-Induced Hepatic Damage in Wistar Albino Rats. Afr J Tradit Complement Altern Med 2018, 15, 64–71. [Google Scholar] [CrossRef]
- Mudie, K.; Daniel, S.; Feyissa, C.; Abiy, A.; Asfaw, D.; Atsbeha, G. Hepatoprotective Activity of Aqueous Seed Extract of Nigella Sativa against Highly Active Antiretroviral Therapy Induced Hepatotoxicity in Rats. Pharmacology OnLine 2014, 3, 11–21. [Google Scholar]
- Abdullah Jan Panezai; Moosa Khan; Syed Muhammad Ishaque; Raheem Ullah; Ahmad Ali Khan; Noshaba Rahat Variable Doses of Nigella Sativa in Isoniazid Induced Liver Toxicity in Rabbits. Pak Euro. J. Med & LS 2022, 5, 187–194. [CrossRef]
- Sankar, M.; Rajkumar, J.; Sridhar, D. Hepatoprotective Activity of Heptoplus on Isoniazid and Rifampicin Induced Liver Damage in Rats. Indian J Pharm Sci 2015, 77, 556–562. [Google Scholar] [CrossRef]
- Parameswari, S.A.; Chetty, C.M.; Chandrasekhar, K.B. Hepatoprotective Activity of Ficus Religiosa Leaves against Isoniazid+rifampicin and Paracetamol Induced Hepatotoxicity. Pharmacognosy Res 2013, 5, 271–276. [Google Scholar] [CrossRef]
- Li, G.; Yang, Y.; Yang, J.; Suo, Y.; Xu, H.; Liu, P.; Wang, J.; Deng, G.; Feng, T. Hepatoprotective Effects of Malus Hupehensis Tea against Isoniazid- and Rifampicin-Induced Liver Injury by Regulating Cytochrome P450 in Mice. Journal of Functional Foods 2021, 84, 104580. [Google Scholar] [CrossRef]
- P E, S.K.; Mishra, A.; Mandal, S.; Chawla, S.; Kalra, B.S. Hepatoprotective Potential of Phyllanthus Niruri and Andrographis Paniculata in Isoniazid-Rifampicin Induced Hepatotoxicity in Rats. Indian Journal of Tuberculosis 2023, S0019570723002263. [Google Scholar] [CrossRef]
- Dubiwak, A.D.; Damtew, T.W.; Senbetu, M.W.; Yewhalaw, D.; Asere, T.G.; Nemo, G.; Baye, M.F. Hepatoprotective Effect of Corm of Ensete Ventricosum (Welw.) Cheesman Extract against Isoniazid and Rifampicin Induced Hepatotoxicity in Swiss Albino Mice. Journal of Toxicology 2021, 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Palanisamy, N.; Manian, S. Protective Effects of Asparagus Racemosus on Oxidative Damage in Isoniazid-Induced Hepatotoxic Rats: An in Vivo Study. Toxicol Ind Health 2012, 28, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Darvin, S.S.; Esakkimuthu, S.; Toppo, E.; Balakrishna, K.; Paulraj, M.G.; Pandikumar, P.; Ignacimuthu, S.; Al-Dhabi, N.A. Hepatoprotective Effect of Lawsone on Rifampicin-Isoniazid Induced Hepatotoxicity in in Vitro and in Vivo Models. Environmental Toxicology and Pharmacology 2018, 61, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Pelapelapon, A.A.; Rohmawaty, E.; Herman, H. Evaluation of The Hepatoprotective Effect of Plantago Major Extract in A Rifampicin-Isoniazid Induced Hepatitis Rat Model. Trends Sci 2023, 20, 6331. [Google Scholar] [CrossRef]
- Haldkar, C.; Jaiswal, A.; Ganeshpurkar, A.; Dubey, N. Evaluation of Protective Effect of Glycyrrhiza Glabra L. Extract on Isoniazid-Rifampicin Induced Hepatocellular Damage in Rats. PC 2019, 10, 18–22. [Google Scholar] [CrossRef]
- Eminzade, S.; Uraz, F.; Izzettin, F.V. Silymarin Protects Liver against Toxic Effects of Anti-Tuberculosis Drugs in Experimental Animals. Nutr Metab (Lond) 2008, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Tasduq, S.A.; Peerzada, K.; Koul, S.; Bhat, R.; Johri, R.K. Biochemical Manifestations of Anti-Tuberculosis Drugs Induced Hepatotoxicity and the Effect of Silymarin. Hepatol Res 2005, 31, 132–135. [Google Scholar] [CrossRef]
- Victorrajmohan, C.; Pradeep, K.; Karthikeyan, S. Influence of Silymarin Administration on Hepatic Glutathione-Conjugating Enzyme System in Rats Treated with Antitubercular Drugs. Drugs R D 2005, 6, 395–400. [Google Scholar] [CrossRef]
- Samuel, A.J.S.J.; Mohan, S.; Chellappan, D.K.; Kalusalingam, A.; Ariamuthu, S. Hibiscus Vitifolius (Linn.) Root Extracts Shows Potent Protective Action against Anti-Tubercular Drug Induced Hepatotoxicity. Journal of Ethnopharmacology 2012, 141, 396–402. [Google Scholar] [CrossRef]
- Pari, L.; Kumar, N.A. Hepatoprotective Activity of Moringa Oleifera on Antitubercular Drug-Induced Liver Damage in Rats. J Med Food 2002, 5, 171–177. [Google Scholar] [CrossRef]
Figure 1.
Molecular mechanisms of hepatotoxicity by ARV and ATD drugs.
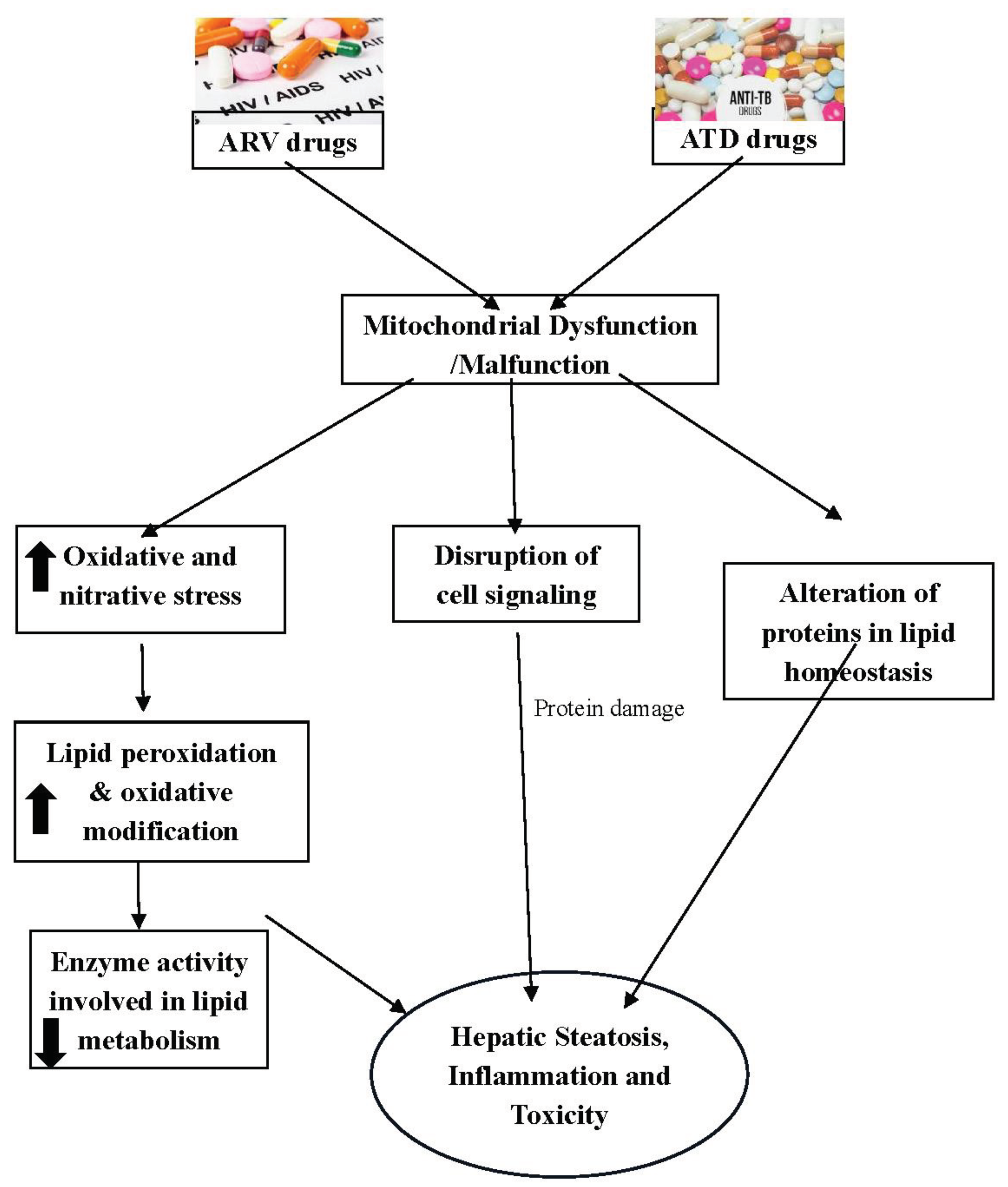

Table 1.
List of Hepatoprotective medicinal plants used against drugs induced hepatotoxicity.
| Medicinal Plant/active compound | Model and Extract dose | Study findings | Impact on liver | References |
|---|---|---|---|---|
| ARV Drugs | ||||
| Silibinin | Wistar albino rats; 100mg/kg b. w; orally | Reduction of liver enzymes, oxidative stress markers, hyperlipidemia and liver histology | Protects liver against AZT induced hepatotoxicity | [15] |
| Moringa Oleifera (MO) | Male wistar rats; 100 and 300 mg/kg MO leaf extract; orally |
Increased antioxidant markers and liver function | Protects against HAART induced hepatotoxicity | [101] |
| Piper Nigrum Stem (PNS) | Male wistar rats; 200, 400 and 600 mg/kg PNS extract; orally |
Reduction in triglycerides and alkaline phosphatase, increase in antioxidant enzymes and histological improvement | Hepatoprotective activity against tenofovir/ lamivudine/efavirenz (TLE)-induced hepatotoxicity and dyslipidemia | [102] |
| Cymbopogon citratus | Wistar albino rats; 200, 400 and 800 mg/kg Cymbopogon citratus oil extract; oral intubation |
Improvement in liver architecture and liver serum biochemistry. | Hepatoprotection activity against Nevirapine induced hepatotoxicity | [103] |
| Nigella Sativa Seed | Wistar albino rats; 100, 200, 400 and 800 mg/kg Nigella sativa aqueous extract; oral intubation |
Improvement in liver histology and liver biochemistry. | Hepatoprotection activity against AZT, 3TC and EFV induced hepatotoxicity | [104] |
| ATD Drugs | ||||
| Nigella Sativa | Oryctolagus cuniculus Rabbits; 500 and 1000 mg/kg orally |
Improvement in liver biochemistry. | Hepatoprotection activity against INH induced hepatotoxicity | [105] |
| Heptoplus (Polyherbal formulation) | Sprague Dawely rats; 50 and 100 mg/kg b. w; orally |
Improvement in liver biochemistry, antioxidant and histology. | Hepatoprotection activity against INH and RIF induced hepatotoxicity | [106] |
| Ficus religiosa (Moraceae) | Male Wistar albino rats; 100, 200 and 300 mg/kg b. w; p.o extract | Improvement in liver marker enzymes, antioxidant and histology. | Hepatoprotection activity against INH and RIF induced hepatotoxicity | [107] |
| Malus hupehensis (MHE) | Kunming male mice; 30, 60 and 120 mg/kg b. w; p.o of methanolic extract | Improvement in liver serum markers, antioxidant and histology. | Hepatoprotection activity against INH and RIF induced hepatotoxicity | [108] |
| Phyllanthus niruri and Andrographis paniculata | Sprague Dawley rats; 125 mg/kg b. w; p.o | Improvement in liver serum markers, antioxidant and histology. | Hepatoprotection activity against INH and RIF induced hepatotoxicity | [109] |
| Corn of Ensete Ventricosum (Welw) cheesman extract | Swiss albino mice; 200 and 400 mg/kg b. w; p.o | Improvement in liver serum markers, antioxidant and histology. | Hepatoprotection activity against INH and RIF induced hepatotoxicity | [110] |
| Asparagus racemosus extract | Male albino rats; 50 mg/kg b. w; p.o | Improvement in liver serum markers, antioxidant and histology. | Hepatoprotection activity against INH induced hepatotoxicity | [111] |
| Lawsonia inermis | Male wistar rats; 50 and 100 mg/kg b. w; intraperitoneal | Improvement in liver serum markers, antioxidant and histology. | Hepatoprotection activity against INH and RIF induced hepatotoxicity | [112] |
| Plantago major extract | Male wistar rats; 20.3, 40.5 and 81 mg/kg b. w; p.o | Improvement in liver serum markers, antioxidant and histology. | Hepatoprotection activity against INH and RIF induced hepatotoxicity | [113] |
| Glycyrrhiza glabra L. Extract | Wistar rats; 100, 200 and 400 mg/kg b. w; p.o | Improvement in liver serum markers, antioxidant and histology. | Hepatoprotection activity against INH and RIF induced hepatotoxicity | [114] |
| Silibinin | Wistar albino rats; 100mg/kg b. w; orally | Reduction of liver enzymes, oxidative stress markers, hyperlipidemia and liver histology | Protects liver against INH + AZT induced hepatotoxicity | [11,13] |
| Silymarin | Male Wistar albino rats; 200mg/kg b. w; intra-gastric administration | Reduction of liver enzymes, oxidative stress markers and liver histology | Protects liver against INH + RIF + PYR induced hepatotoxicity | [115,116,117] |
| Hibiscus Vitifolius (Linn.) root extract | Wistar albino rats; 400mg/kg b. w; orally | Reduction of liver enzymes, oxidative stress markers, hyperlipidemia and liver histology | Protects liver against INH + AZT induced hepatotoxicity | [118] |
| Moringa Oleifera (MO) extract |
Male Wistar albino rats; 150, 200 and 250mg/kg b. w; intra-gastric administration | Reduction of liver enzymes, oxidative stress markers and liver histology | Protects liver against INH + RIF + PYR induced hepatotoxicity | [119] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



