
Submitted:
30 March 2024
Posted:
02 April 2024
You are already at the latest version
Abstract
IBD, encompassing CD and UC, are characterized by chronic gastrointestinal inflammation due to abnormal immune responses to gut microflora. The bidirectional communication between the gut and the brain, known as the GBA, is disrupted in IBD, leading to neurobiological imbalances and affective symptoms. Systemic inflammation in IBD affects the brain's inflammatory response system, hormonal axis, and BBB integrity, influencing gut microbiota and clinical responses to probiotics.
This review aims to explore the links between dysregulations in the GBA, serum biomarkers, and the development of MCI and NDDs. The objective is to identify potential correlations and propose future research directions to understand the impact of altered microbiomes and intestinal barrier functions on NDDs. Studies suggest a potential link between IBD and extraintestinal complications such as MCI and NDDs. Mechanisms include systemic inflammation, BBB dysfunction, autoimmune responses, GBA dysfunction, medication effects, and comorbidities. Serum biomarkers, including vitamin D3, C-reactive protein, high-sensitivity C-reactive protein, vitamin B12, homocysteine, serum amyloid, neuron-specific enolase, neurofilament light chain, S100 proteins, brain-derived neurotrophic factor, IL-6, LP-2 associated phospholipase, prostaglandin E2, IL-1β, and TNF-α, have been investigated for their potential to predict MCI but current results are lacking clarity.
Keywords:
IBD
; neurodegeneration
; mild cognitive impairment
; serum biomarker
; systemic inflammation
; gut-brain axis
Inflammatory Bowel Diseases (IBD), Gut-Brain Axis (GBA) Interactions and Neurodegeneration
Inflammatory bowel diseases (IBD) are chronic conditions characterized by repetitive episodes of inflammation in the gastrointestinal tract due to an abnormal immune response to gut microflora. The two main types of IBD are Crohn's disease (CD) and ulcerative colitis (UC). UC involves diffuse inflammation of the colonic mucosa, while CD results in transmural ulceration of any portion of the gastrointestinal tract, most often affecting the terminal ileum and colon [1].
The gut-brain axis (GBA) refers to the bidirectional communication between the gut and the brain, which involves neural, hormonal, and immune pathways. This communication allows the brain to influence intestinal functions, including the gut microbiota, and vice versa [2].
IBDs are associated with systemic inflammation and alterations of the GBA. In IBD, the GBA is disrupted, leading to neurobiological imbalances and clinical affective and/or behavioral symptoms [3].
Systemic inflammation in IBD can activate the inflammatory response system in the brain, the hypothalamic-pituitary-adrenal axis (HPAA), and brain areas implicated in altered behaviors. This can lead to changes in blood-brain barrier (BBB) integrity and an emerging role for gut microbiota and the clinical response to probiotics in IBD [4].
Inflammation can also disrupt the balance of the gut microbiota, a condition known as dysbiosis. The dysbiosis affects the GBA and might lead to changes in brain function, resulting in altered HPAA[2,5]. This gives rise to an overall proinflammatory phenotype and dysregulated HPAA and serotonergic functioning [6]. Additionally, the gut microbiota produces various metabolites, such as short-chain fatty acids (SCFA), that can influence brain function. Changes in the production of these metabolites due to dysbiosis could therefore impact the brain[2].
Aim
The purpose of this review is to identify some of the possible links between gut-brain axis dysregulations in terms of serum biomarkers and the development of mild cognitive impairment (MCI) and neurodegenerative diseases (NDDs) such as Alzheimer’s Disease (AD) or Parkinson’s Disease (PD) and what are the perspectives we could focus on near future to test those hypotheses. Actively knowing this, further research could focus more on the intestinal microbiome and other mechanisms to reduce the burden of neurodegenerative disease.
Considering that nearly 2500 years ago Hippocrates had a dazzling statement declaring that ‘All disease begins in the gut’ without having any of our modern clinical and laboratory exploration techniques, we strongly believe that now it would be a great time we get a clear understanding of how the altered microbiome and intestinal barrier function might lead to the development of NDDs. Also, life expectancy has greatly increased in the last 100 years, Due to this, we have to actively think about the burden of NDDs because they will probably become more frequent due to life expectancy increase but also due to lifestyle modifications[7,8].
Methodology
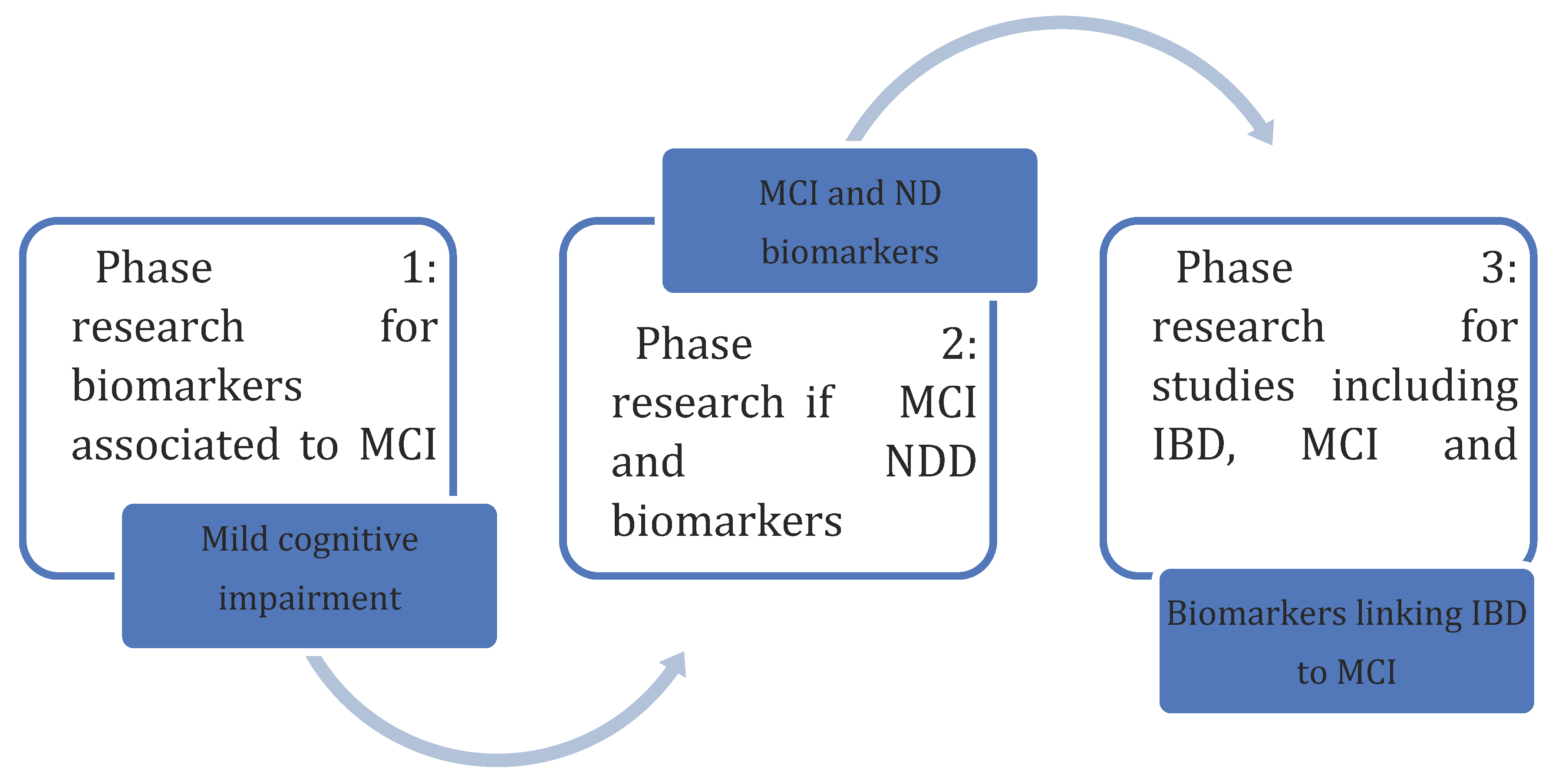
Articles were selected from the PubMed database by searching in the first time associations between [inflammatory bowel diseases], [inflammatory bowel disease], [IBD], [Crohn’s disease], [CD], [Ulcerative Colitis], [UC] and [serum biomarkers], [blood biomarkers]. Further on, biomarkers were screened if they associate with [neurodegeneration], [neurodegenerative diseases], [mild cognitive impairment], [Alzheimer’s Disease], [AD], [Alzheimer]. Combinations between all were also researched. Studies were chosen if the studied biomarker was both tested in IBD or MCI patients or both of them. Figure 1 synthetizes the methodology of research for this article.
Neurodegeneration as an Extraintestinal Manifestation of IBD
Several studies have been suggesting that MCI, multiple sclerosis (MS) and NDD could be extraintestinal complications of IBD [9,10,11,12]. Several mechanisms have been proposed for the link between IBD and further development of ND, such as systemic inflammation, BBB dysfunction, autoimmune mechanism, GBA dysfunction, the effects of medication and the effect of other comorbidities such as anxiety, depression, nutritional deficiencies, sleep disturbances or anemia[10,13,14]. There are also studies that suggested ND is not a direct cause of IBD because of the confounders and other concomitant pathologies [11,14,15]. Despite those results, IBD might still be risk factors for NDDs[9,10,11,12].
Mild Cognitive Impairment: Definition, Risk Factors and Diagnosis
MCI is a condition that involves a slight decline in cognitive abilities, such as memory, thinking, and reasoning, that is greater than what is expected with normal aging but not severe enough to be classified as dementia. People with MCI may experience memory problems, difficulty with decision-making, and challenges with language or visual perception. MCI is considered a transitional stage between normal aging and dementia, and not all individuals with MCI will progress to dementia [16,17]
MCI can be caused by a variety of factors. NDDs, such as AD, are often associated with MCI, and it can be a transitional stage between normal aging and dementia [17]. Vascular diseases that affect the blood supply to the brain can also lead to MCI [17]. Other potential causes include psychiatric conditions, certain medications, and diseases such as PD or LBD [17]. Additionally, traumatic brain injuries (TBI) and certain internal diseases can contribute to the development of MCI [17].
There is no consensus on the general recommendation for screening for MCI in older adults. One study found no significant differences in health-related quality of life at 12 months after screening for MCI, and there was no empirical evidence that screening for MCI improves patient or caregiver outcomes or causes harm [18]. Another study suggested that cognitive testing should occur for older patients when there is a reason to suspect dementia, such as an informant history of cognitive or functional decline, clinical observation, or very old age [18].
The Presumed Link between IBD and MCI
Studies have shown that people with IBD can exhibit cognitive deficits, particularly in attention and executive function, including working memory [20]. Another study found that patients with UC in remission showed impairments in cognitive functioning compared to healthy controls [21].
The exact causes of cognitive deficits in people with IBD are not fully understood, but several potential mechanisms have been proposed. One theory is that the gut-brain axis, which is the bidirectional communication between the gut and the brain, may play a role. Imbalances in the gut microbiota, which are common in IBD, could potentially affect brain function [22]. Chronic inflammation could also contribute to cognitive deficits by causing systemic inflammation that affects the brain [22]. Lastly, the adverse effects of disease-modifying medication used in IBD treatment could potentially contribute to cognitive impairment [32]. However, more research is needed to fully understand these mechanisms and their implications for the management of cognitive deficits in people with IBD [9,11,31,32]
Gut Microbiome Alterations and MCI
Alterations in the gut microbiome, a key component of the GBA, have been linked to NDDs. These alterations can influence the homeostasis of the central nervous system (CNS) through the modulation of the immune system and the production of molecules and metabolites [23]. Dysbiosis, or imbalance in the gut microbiota, has been associated with NDDs and is thought to contribute to their development and prognosis [24]. Inflammation-associated microbiome changes are particularly implicated in NDDs [24]. Moreover, the gut microbiota can interact with the brain through systemic chronic inflammation, which can impair the BBB and contribute to neuroinflammation, ND, and aging [25].
Some studies have shown alterations in the gut microbiota in individuals with MCI, including an increase in bacterial taxa such as Erysipelatoclostridiaceae, Erysipelotrichales, Patescibacteria, Saccharimonadales, and Saccharimonadia [26]. Another study identified Prevotella ruminicola, Bacteroides thetaiotaomicron, and Bacteroides xylanisolvens as taxa correlated with MCI [27]. On the other hand, the specific alterations in the gut microbiota associated with IBD were not provided in the given studies. But a study found that IBD patients with Cl. Difficile infection had more pronounced dysbiosis with higher levels of Ruminococcus gnavus and Enterococcus operational taxonomic units and lower levels of Blautia and Dorea operational taxonomic units [28]. Another study reported that IBD is associated with changes in bile acids, an important bacterial metabolite. Specifically, primary bile acids and conjugated bile acids are increased in fecal samples of IBD patients, while secondary bile acids are reduced [29]. Furthermore, a study found major differences in the gut microbiome between patients with and without a pathogen and IBD. In IBD, a higher proportion of patients without a pathogen required hospitalization and IBD therapies at flare and within the 2 years after flare, driven by a milder disease course in flares complicated by an E. Coli subtype or Norovirus [30].
Serum Biomarkers as Predictors for MCI
Serum biomarkers can serve as predictors for MCI. Several studies have investigated the relationship between serum biomarkers, MCI and NDDs. For example, low levels of vitamin D have been associated with worse cognitive performance in PD patients [31]. Additionally, serum levels of neuron-specific enolase (NSE) have been correlated with cognitive status and neurocognitive outcomes in patients with TBI [32]. Serum biomarkers, such as Neurofilament Light Chain (NfL), have also been identified as predictors of disease progression in prodromal fronto-temporal dementia (FTD) [33].
Vitamin D3
Vitamin D3, also known as cholecalciferol, is a type of vitamin D that plays a crucial role in both the immune system and the CNS. In terms of immunity, vitamin D3 has immunomodulatory effects, meaning it helps regulate the immune response. It can suppress excessive inflammation and promote immune tolerance, which is important for preventing autoimmune diseases. In the CNS, vitamin D3 acts as a neurosteroid, meaning it affects brain development and function. It plays a role in neuroprotection, neurotrophic actions, and neurotransmission [34,35,36].
Vitamin D deficiency has been associated with an increased risk of AD, PD, and MCI. Several studies have found that low levels of vitamin D are linked to an increased risk of developing AD and dementia [37]. Vitamin D deficiency has also been associated with reduced hippocampal volume and disrupted structural connectivity in patients with MCI [38]. Additionally, vitamin D supplementation has been shown to improve cognitive impairment and decrease the accumulation of amyloid-beta plaques, which are characteristic of AD [39].
In IBD, vitamin D deficiency is common and has been associated with increased inflammation and disease severity. Studies have shown that a significant proportion of IBD patients have vitamin D levels below the recommended range. For example, one study found that 58.6% of CD patients and 44.6% of UC patients had vitamin D levels below 50 nmol/L, which is considered deficient. CD patients tend to have lower vitamin D levels compared to patients with irritable bowel syndrome (IBS). Certain clinical factors, such as disease location, disease activity, and the use of specific medications, can also affect vitamin D levels in IBD patients. Vitamin D supplementation may help improve gut health, rebalance gut microbiota, and reduce inflammation in people with UC [40,41,42]. There are not studies that specifically investigated the serum levels of vitamin D3 in patients with IBD and MCI.
C reactive Protein and High-Sensivity C Reactive Protein
C-reactive protein (CRP) is an acute-phase reactant protein produced by the liver in response to inflammation or infection. CRP plays a crucial role in the immune system by modulating the inflammatory response and promoting host defense against infections. It interacts with components of both the innate and adaptive immune systems, including complement proteins and Fc receptors on immune cells. In the CNS, CRP is constitutively expressed by microglial cells, astrocytes, and neurons, and its expression can be increased in response to inflammation. CRP in the CNS is involved in brain development, maintenance of normal brain homeostasis, and neuroinflammation. However, the exact mechanisms and functions of CRP in the CNS are still being studied [43,44]. High-sensivity CRP (hsCRP) is a more sensitive test that can detect even very low levels of inflammation. It is often used to assess cardiovascular risk, as even low levels of inflammation in blood vessels can contribute to the development of heart disease. hsCRP is measured using specialized assays that can detect CRP levels as low as 0.3 mg/L [45].
There is evidence suggesting that CRP and hsCRP may be associated with IBD and MCI. In IBD, CRP has been studied as a diagnostic and prognostic marker.
Elevated CRP levels have been observed in patients with IBD, particularly in those with CD compared to UC [46]. Another study found that high CRP levels are associated with poor sleep quality in patients with IBD, independent of nocturnal symptoms[47]. Another study showed that CRP is associated with disease severity and levels of CRP and cytokines in patients with IBD [48].
Studies have shown that higher hsCRP levels are associated with faster declines in cognitive function, including global cognitive scores, memory scores, and executive function scores [49]. Regarding MCI, a study has found that elevated CRP levels predict poorer cognition and increased dementia risk in cognitively healthy older adults [50]. Another study showed that higher baseline CRP levels are associated with poorer memory in elderly women [51]. A population-based case-control study found that baseline hsCRP levels were significantly associated with both MCI and amnestic MCI [119]. Furthermore, elevated hsCRP levels detected five years before diagnosis were associated with an increased probability of MCI [52]. However a causal relationship between CRP levels and these conditions was not proven by none of the studies. There was no study that evaluated the serum levels of CRP and hsCRP and the development of MCI in the IBD population.
Vitamin B12
Vitamin B12, also known as cobalamin, is an essential water-soluble vitamin that plays a crucial role in various bodily functions. It is necessary for the production of red blood cells, the maintenance of a healthy nervous system, and the metabolism of proteins and fats. Additionally, vitamin B12 contributes to DNA synthesis and supports brain function. In terms of immunity, vitamin B12 is involved in the regulation of immune cell production and function, helping to maintain a balanced immune response. In the CNS, vitamin B12 is important for cellular function, especially for the production of myelin, which is essential for proper nerve signal transmission [53].
Vitamin B12 deficiency is common in patients with IBD, particularly in those with CD. Studies have shown that the prevalence of vitamin B12 deficiency in patients with Crohn's disease ranges from 15.6% to 33% [54,55]. The main reason for this deficiency is the involvement of the terminal ileum, where vitamin B12 is absorbed [56]. Ileal resections and disease activity are risk factors for vitamin B12 deficiency in patients with CD [56]. Low levels of vitamin B12 have been associated with cognitive impairment and an increased risk of MCI and dementia [57,58]. Vitamin B12 deficiency (<150 ρmol/L) has been specifically linked to cognitive impairment [57]. However, the efficacy of vitamin B12 therapy for cognitive impairment and dementia is still debated. Vitamin B12 supplements have been shown to improve cognition in patients with pre-existing deficiency, but not in those without deficiency [57].
However, there is no proven role between the association of vitamin B12 deficiency in IBD patients and the development of MCI.
Homocysteine
Homocysteine is an amino acid that is involved in the methylation and sulfuration pathways and is derived from the metabolism of methionine, an essential amino acid. Elevated levels of homocysteine, known as hyperhomocysteinemia, have been associated with several disorders, including cardiovascular disease, NDDs, autoimmune disorders, and birth defects [59]. In terms of immunity, studies have shown that homocysteine can affect T-lymphocyte function. It has been found to promote T cell activation, differentiation, and activation-induced cell death [60]. These effects on immune function may contribute to age-related immune dysfunction and disease pathology.
In the CNS, homocysteine has been implicated in the pathogenesis of various neurological diseases, including stroke, AD, PD, epilepsy, MS, and amyotrophic lateral sclerosis (ALS) [61].
A study found that patients with IBD had significantly higher homocysteine levels compared to healthy individuals [62,63]. Elevated homocysteine levels have been associated with cognitive decline and an increased risk of dementia, including AD and also the progression from MCI to dementia [64,65,66,67,68]. Additionally, supplementation with folic acid and vitamin B12, which can lower homocysteine levels, has shown potential benefits in improving cognitive performance in individuals with MCI [69]. There may not be sufficient evidence or specific studies addressing the simultaneous dosing of homocysteine in patients with MCI and IBD.
Serum Amyloid
Serum amyloid A (SAA) is an acute-phase protein that is produced by the liver in response to inflammation or infection. It plays a role in the immune response and lipid metabolism. SAA is involved in innate immunity by promoting the development of T helper 17 cells and modulating various leukocyte functions. It can also bind to lipids and phospholipids, forming nanoparticles and sequestering them. In the CNS, SAA levels have been found to be increased in certain neurological disorders, such as neuromyelitis optica (NMO) and atypical MS, suggesting a potential role in the pathogenesis of these conditions. However, the exact mechanisms and functions of SAA in the CNS are still being investigated [70,71].
Several studies have investigated the role of SAA as a biomarker for disease activity and mucosal inflammation in IBD. One study found that SAA levels correlated with mucosal inflammation in patients with CD, even in those with normal CRP levels [72]. SAA has been implicated in NDDs. In AD, SAA has been shown to contribute to oxidative stress, mitochondrial dysfunction, impaired synaptic transmission, disruption of membrane integrity, and impaired axonal transport [73]. Additionally, SAA has been found to interact with other pathological proteins, such as beta-amyloid and alpha-synuclein, forming toxic heteroaggregates [74]. These findings suggest that SAA may play a role in the pathogenesis of neurodegenerative diseases. However, further research is needed to fully understand the mechanisms and potential therapeutic implications of SAA.
Neuron Specific Enolase
Neuron-specific enolase (NSE) is a glycolytic enzyme found in neurons and neuroendocrine cells. It's used as a marker for neuronal damage and is elevated in conditions like seizures, head injury, and autoimmune neurological diseases. NSE also plays a role in immunity, as its levels can indicate neuronal damage in various comas and autoimmune neurological diseases. In the CNS, NSE is a marker for synapse formation and can indicate neuronal lesions during various comas [75,76,77].
It has been identified in the intestinal neuronal and neuroendocrine cells of patients with CD [78]. It plays a dual role in promoting both neuroinflammation and neuroprotection in neurodegenerative events. Elevated NSE can promote extracellular matrix degradation, inflammatory glial cell proliferation, and actin remodeling, thereby affecting migration of activated macrophages and microglia to the injury site and promoting neuronal cell death [79]. NSE can also control neuronal survival, differentiation, and regeneration [79] Studies have shown abnormalities in the enteric nervous system (ENS) in tissue samples from patients with IBD, with an increase in neuronal cell bodies, enteroglia, and interstitial cells of Cajal ICC in the deep muscular plexus of CD patients [80]. However, reduced NSE levels have been observed in chronic severe TBI, suggesting ongoing neurodegeneration and neuronal loss [80]. Therefore, NSE could be a reliable, quantitative, and specific marker of neuronal injury and neurodegeneration [80,81]. Worth to mention, is that NSE has been found to be elevated in children with Autistic Spectrum Disease, a condition that involves neurodevelopmental disorders and could potentially be influenced by the GBA [82].
Neurofilament Light Chain
Neurofilament light chain (NfL) is a biomarker that can indicate neurodegeneration in various neurological disorders. NfL is a protein found in the axons of neurons, and its levels increase in the cerebrospinal fluid (CSF) and blood when there is axonal damage. Studies have shown that NfL levels are elevated in neurodegenerative diseases such as AD, PD, Huntington's disease (HD), and ALS. NfL can be used as a diagnostic, prognostic, and monitoring biomarker for these conditions. However, further research is needed to fully understand the relationship between NfL and neurodegeneration and to establish its clinical utility. [83,84] While NfL can indicate the presence of neurodegeneration, it does not provide information on the underlying cause, necessitating additional diagnostic tests [85]. There is no study that tested the serum or CSF level of NfL in patients with IBD.
S100 Proteins
S100 proteins are a family of small calcium-binding proteins that play important roles in various cellular processes such as calcium homeostasis, cell proliferation, apoptosis, differentiation, inflammation, and signal transduction. S100 proteins have been implicated in several diseases, including cancer, inflammatory disorders, neurological diseases, liver disease, and pulmonary diseases [86,87,88]. There is evidence to suggest that S100 proteins may play a role in both IBD and NDDs. In the context of IBD, S100B protein has been implicated in the onset and maintenance of inflammation in the gut [89]. It is believed to contribute to the regulation of inflammatory events in the gut and may have both trophic and toxic effects depending on its concentration [89]. In NDDs, S100B levels have been found to correlate with disease progression and severity [90]. High levels of S100B are suggestive of pathogenic processes in these diseases and may be involved in the activation of inflammatory pathways [91].
Brain Derived Neurotrophic Factor
Brain-Derived Neurotrophic Factor (BDNF) is a molecule that plays a crucial role in neuronal survival, growth, and neurogenesis. Changes in BDNF levels and signaling pathways have been identified in several neurodegenerative diseases, including AD, PD, and HD, and have been linked with the symptoms and course of these diseases [92,93]. Lowering BDNF level mediates neurodegeneration of neurons, including dopaminergic neurons in PD [94]. Moreover, BDNF improves synaptic plasticity and contributes to long-lasting memory formation [95]. Several studies have shown that a high level of BDNF is associated with a lower risk for developing a neurodegenerative disease [95]. In IBS and IBD, BDNF plays a significant role in modulation of abdominal pain [96,97]. BDNF expression is found to be upregulated in the colonic mucosa of IBS patients, contributing to visceral hyperalgesia [97]. IBD patients often have sleep and mood disorders, and BDNF is shown to modulate interactions between the CNS and the gastrointestinal tract, possibly contributing to these psychological issues [98].
IL-6
Interleukin-6 (IL-6) is a cytokine that plays a role in cell signaling and communication within the immune system. It is produced by various cells, including immune cells, and is involved in regulating inflammation and immune responses. IL-6 has diverse functions and can influence the activity of different cell types, such as T cells, B cells, and macrophages. It is known to play a role in various physiological processes, including the immune response to infection, inflammation, and tissue repair. However, excessive or dysregulated production of IL-6 has been implicated in the pathogenesis of several diseases, including IBD and AD [99,100]. In a study investigating the association between IBD and the development of AD, it was found that IBD patients had a higher risk of developing AD compared to those without IBD. The study also found that higher levels of IL-6 were associated with an increased risk of cognitive impairment in IBD patients [101]. Additionally, another study examined the association between inflammatory markers and MCI in a population-based sample. It found that higher levels of CRP, that is regulated by IL-6, were associated with an increased risk of MCI, particularly nonamnestic MCI [102].
LP-2 Associated Phospholipase
LP2-associated phospholipase (SPLA2) is an enzyme that plays a role in various physiological and pathological processes, including inflammation and host defense mechanisms against bacteria. In the context of IBD, SPLA2 has been found to have increased mass concentrations in the serum and colonic mucosa of patients with CD. SPLA2 has also been implicated in the pathogenesis of AD and MCI, where it is associated with elevated levels of bacterial lipopolysaccharides and cyclooxygenases. In patients with CD, the mass concentration of group II phospholipase A2 is increased in both serum and colonic mucosa, and it is associated with the degree of inflammatory activity in the intestinal wall [103]. In the context of cognitive impairment, elevated levels of bacterial lipopolysaccharides and cyclooxygenases (COX1 and COX2) have been observed in the blood serum and CSF of patients with AD and MCI. LPSs positively correlate with LP2-associated phospholipase, Aβ-42, and tau, and negatively correlate with mental state. These findings suggest that LP2-associated phospholipase and LPSs may play a role in the pathogenesis of AD and MCI [104].
Prostaglandin E2
Prostaglandin E2 (PGE2) is a type of prostaglandin, which is a group of lipid compounds involved in various physiological processes, including inflammation. PGE2 is produced in the body and plays a role in regulating inflammation, pain, and fever. In relation to IBD, studies have shown that PGE2 levels are increased in the inflamed mucosa of patients with IBD [105]. Regarding MCI and PGE2, there is limited direct evidence linking the two. However, PGE2 has been implicated in neuroinflammation, which is believed to play a role in the pathogenesis of AD [106]. PGE2 has been found to have complex actions on neural signaling and can influence the electrical activity of neurons [107]. While the specific relationship between PGE2 and MCI is not well-established, it is possible that PGE2 may play a role in neuroinflammation, and neuronal dysfunction associated with cognitive impairment.
IL-1β
Interleukin-1 beta (IL-1β) is a cytokine that plays a crucial role in the inflammatory response. It is involved in various physiological and pathological processes, including immune regulation and inflammation. In the context of IBD, IL-1β has been implicated in the development and progression of the disease. Studies have shown increased IL-1β levels in the intestines of IBD patients, and blocking IL-1β activity has been found to reduce inflammation and improve symptoms in experimental colitis models [108,109]. In terms of MCI and AD, IL-1β has also been investigated. Elevated levels of IL-1β have been observed in the brains of AD patients, and it is believed to contribute to the neuroinflammation, and neuronal degeneration seen in the disease [110]. However, the relationship between IL-1β and cognitive function is complex, and conflicting results have been reported. Some studies suggest that IL-1β may impair cognitive function, while others show no effect or even a beneficial role [111,112]. Overall, IL-1β is a key player in the inflammatory response and has been implicated in both IBD and cognitive impairment.
TNF- ɑ
Tumor necrosis factor-alpha (TNF-α) is a pro-inflammatory cytokine that plays a crucial role in the pathogenesis of IBD and NDDs. It activates immune responses against infection, injury, or inflammation, and is involved in the regulation of various immune cells. TNF-α is also implicated in the regulation of T cell responses, including development, homeostasis, primary antigenic responses, apoptosis, effector functions, and memory cell formation. It is a key mediator of the innate immune response and has strong proinflammatory and immunomodulatory properties[112]. In patients with IBD, increased circulating TNF-α levels have been associated with the intensity of gastrointestinal symptoms and cognitive-affective biases [113]. A study on Chinese older adults found that IL-1β and IL-18, which are mediated by TNF-α, partially explain the association between vitamin D deficiency and MCI [114].
Conclusions
Several biomarkers have been studies in the both IBD and MCI separately and some of them were chosen to be measured in order to see if they correlate with the intensity of MCI or if they predict the installment. However, much more studies are required to uncover the mechanisms between the MCI development in patients who suffer from IBD.
Abbreviation list
| AD | Alzheimer's Disease |
| ALS | Amyotrophic lateral sclerosis |
| BBB | Blood brain barrier |
| BDNF | Brain derived neurotrophic factor |
| CD | Crohn’s Disease |
| CNS | Central nervous system |
| CRP | C reactive protein |
| CSF | Cerebrospinal fluid |
| ENS | Enteric nervous system |
| FTD | Fronto-temporal dementia |
| GBA | Gut-brain axis |
| HD | Huntignton’s Disease |
| HPAA | Hypothalamic-pituitary-adrenal axis |
| IBDs | Inflammatory bowel disease(s) |
| IBS | Irritable bowel syndrome |
| IL-1β | Interleukin-1 beta |
| IL-6 | Interleukin 6 |
| LBD | Lewy body dementia |
| MCI | Mild cognitive impairment |
| MS | Multiple sclerosis |
| ND | Neurodegeneration |
| NDDs | Neurodegenerative disease(s) |
| NfL | Neurofilament light chain |
| NMO | Neuromielytis optica |
| NSE | Neuron specific enoloase |
| PD | Parkinson’s Disease |
| PGE2 | Prostaglandin E2 |
| SAA | Serum amyloid A |
| SCFA | Short chain fatty acids |
| TBI | Traumatic brain injury |
| UC | Ulcerative Colitis |
References
- McDowell C, Farooq U, Haseeb M. Inflammatory Bowel Disease. 2023 Aug 4. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan–. [PubMed]
- Bonaz, B.L.; Bernstein, C.N. Brain-Gut Interactions in Inflammatory Bowel Disease. Gastroenterology 2013, 144, 36–49. [Google Scholar] [CrossRef] [PubMed]
- Gîlcă-Blanariu, G.-E.; Șchiopu, C.G.; Ștefănescu, G.; Mihai, C.; Diaconescu, S.; Afrăsânie, V.A.; Lupu, V.V.; Lupu, A.; Boloș, A.; Ștefănescu, C. The Intertwining Roads between Psychological Distress and Gut Microbiota in Inflammatory Bowel Disease. Microorganisms 2023, 11, 2268. [Google Scholar] [CrossRef] [PubMed]
- Abautret-Daly. ; Dempsey, E.; Parra-Blanco, A.; Medina, C.; Harkin, A. Gut–brain actions underlying comorbid anxiety and depression associated with inflammatory bowel disease. Acta Neuropsychiatr. 2017, 30, 275–296. [Google Scholar] [CrossRef]
- Ng, Q.X.; Soh, A.Y.S.; Loke, W.; Lim, D.Y.; Yeo, W.-S. The role of inflammation in irritable bowel syndrome (IBS). J. Inflamm. Res. 2018, 11, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Banfi, D.; Moro, E.; Bosi, A.; Bistoletti, M.; Cerantola, S.; Crema, F.; Maggi, F.; Giron, M.C.; Giaroni, C.; Baj, A. Impact of Microbial Metabolites on Microbiota–Gut–Brain Axis in Inflammatory Bowel Disease. Int. J. Mol. Sci. 2021, 22, 1623. [Google Scholar] [CrossRef] [PubMed]
- Lyon, L. ‘All disease begins in the gut’: was Hippocrates right? Brain 2018, 141, e20–e20. [Google Scholar] [CrossRef]
- Kinsella, K.G. Changes in life expectancy 1900–1990. Am. J. Clin. Nutr. 1992, 55, 1196S–1202S. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.S.; Chen, M.-H.; Wang, H.E.; Lu, C.-L.; Wang, Y.-P.; Zhang, B. Inflammatory Bowel Disease and Neurodegenerative Diseases. Gut Liver 2023, 17, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Cui, G.; Li, S.; Ye, H.; Yang, Y.; Huang, Q.; Chu, Y.; Shi, Z.; Zhang, X. Are neurodegenerative diseases associated with an increased risk of inflammatory bowel disease? A two-sample Mendelian randomization study. Front. Immunol. 2022, 13, 956005. [Google Scholar] [CrossRef]
- Kim, G.H.; Lee, Y.C.; Kim, T.J.; Kim, E.R.; Hong, S.N.; Chang, D.K.; Kim, Y.-H. Risk of Neurodegenerative Diseases in Patients with Inflammatory Bowel Disease: A Nationwide Population-based Cohort Study. J. Crohn’s Colitis 2021, 16, 436–443. [Google Scholar] [CrossRef]
- Szandruk-Bender, M.; Wiatrak, B.; Szeląg, A. The Risk of Developing Alzheimer’s Disease and Parkinson’s Disease in Patients with Inflammatory Bowel Disease: A Meta-Analysis. J. Clin. Med. 2022, 11, 3704. [Google Scholar] [CrossRef]
- Kim, J.S.; Chen, M.-H.; Wang, H.E.; Lu, C.-L.; Wang, Y.-P.; Zhang, B. Inflammatory Bowel Disease and Neurodegenerative Diseases. Gut Liver 2023, 17, 495–504. [Google Scholar] [CrossRef]
- Lee, H.-S.; Lobbestael, E.; Vermeire, S.; Sabino, J.; Cleynen, I. Inflammatory bowel disease and Parkinson’s disease: common pathophysiological links. Gut 2020, 70, 408–417. [Google Scholar] [CrossRef]
- Zeng, R.; Wang, J.; Zheng, C.; Jiang, R.; Tong, S.; Wu, H.; Zhuo, Z.; Yang, Q.; Leung, F.W.; Sha, W.; et al. Lack of Causal Associations of Inflammatory Bowel Disease with Parkinson's Disease and Other Neurodegenerative Disorders. Mov. Disord. 2023, 38, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- Feldman, H.H. Mild Cognitive Impairment. Am. J. Geriatr. Psychiatry 2005, 13, 645–655. [Google Scholar] [CrossRef] [PubMed]
- Anderson, N.D. State of the science on mild cognitive impairment (MCI). CNS Spectrums 2019, 24, 78–87. [Google Scholar] [CrossRef]
- Patnode, C.D.; Perdue, L.A.; Rossom, R.C.; Rushkin, M.C.; Redmond, N.; Thomas, R.G.; Lin, J.S. Screening for Cognitive Impairment in Older Adults. JAMA 2020, 323, 764–785. [Google Scholar] [CrossRef]
- Wang, Z.; Dong, B. Screening for Cognitive Impairment in Geriatrics. Clin. Geriatr. Med. 2018, 34, 515–536. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, C.W.; Powell, N.; Norton, C.; Dumbrill, J.L.; Hayee, B.; Moulton, C.D. Cognitive Impairment in Adult Inflammatory Bowel Disease: A Systematic Review and Meta-Analysis. Psychosom. 2021, 62, 387–403. [Google Scholar] [CrossRef]
- Sharma, N.; Dhiman, S.; Bodh, V.; Sharma, D.; Sharma, R.; Sharma, S.; Sharma, B. Cognitive dysfunction in ulcerative colitis patients in remission and its comparison with patients with irritable bowel syndrome and healthy controls. Indian J. Gastroenterol. 2021, 40, 169–175. [Google Scholar] [CrossRef]
- Wang, D.; Zhang, X.; Du, H. Inflammatory bowel disease: A potential pathogenic factor of Alzheimer's disease. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2022, 119, 110610. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, L.; Cantoni, C.; Rotondo, E.; Galimberti, D. The Gut Microbiome–Brain Crosstalk in Neurodegenerative Diseases. Biomedicines 2022, 10, 1486. [Google Scholar] [CrossRef] [PubMed]
- Toledo, A.R.L.; Monroy, G.R.; Salazar, F.E.; Lee, J.-Y.; Jain, S.; Yadav, H.; Borlongan, C.V. Gut–Brain Axis as a Pathological and Therapeutic Target for Neurodegenerative Disorders. Int. J. Mol. Sci. 2022, 23, 1184. [Google Scholar] [CrossRef] [PubMed]
- Mou, Y.; Du, Y.; Zhou, L.; Yue, J.; Hu, X.; Liu, Y.; Chen, S.; Lin, X.; Zhang, G.; Xiao, H.; et al. Gut Microbiota Interact With the Brain Through Systemic Chronic Inflammation: Implications on Neuroinflammation, Neurodegeneration, and Aging. Front. Immunol. 2022, 13, 796288. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Z.; Ma, X.; Wu, J.; Xiao, Z.; Wu, W.; Ding, S.; Zheng, L.; Liang, X.; Luo, J.; Ding, D.; et al. Altered Gut Microbiota and Its Clinical Relevance in Mild Cognitive Impairment and Alzheimer’s Disease: Shanghai Aging Study and Shanghai Memory Study. Nutrients 2022, 14, 3959. [Google Scholar] [CrossRef]
- Aljumaah, M.R.; Bhatia, U.; Roach, J.; Gunstad, J.; Peril, M.A.A. The gut microbiome, mild cognitive impairment, and probiotics: A randomized clinical trial in middle-aged and older adults. Clin. Nutr. 2022, 41, 2565–2576. [Google Scholar] [CrossRef] [PubMed]
- Sokol, H.; Jegou, S.; McQuitty, C.; Straub, M.; Leducq, V.; Landman, C.; Kirchgesner, J.; Le Gall, G.; Bourrier, A.; Nion-Larmurier, I.; et al. Specificities of the intestinal microbiota in patients with inflammatory bowel disease and Clostridium difficile infection. Gut Microbes 2017, 9, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Zhan, S.; Tian, Z.; Liu, C.; Xie, Z.; Zhang, S.; Chen, M.; Zeng, Z.; Zhuang, X. Alterations in Bile Acid Metabolism Associated With Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2021, 27, 1525–1540. [Google Scholar] [CrossRef]
- Axelrad, J.E.; Chen, Z.; Devlin, J.; Ruggles, K.V.; Cadwell, K. Pathogen-Specific Alterations in the Gut Microbiota Predict Outcomes in Flare of Inflammatory Bowel Disease Complicated by Gastrointestinal Infection. Clin. Transl. Gastroenterol. 2022, 14, e00550. [Google Scholar] [CrossRef]
- Santangelo, G.; Raimo, S.; Erro, R.; Picillo, M.; Amboni, M.; Pellecchia, M.T.; Pivonello, C.; Barone, P.; Vitale, C. Vitamin D as a possible biomarker of mild cognitive impairment in parkinsonians. Aging Ment. Heal. 2020, 25, 1998–2002. [Google Scholar] [CrossRef]
- Slavoaca, D.; Birle, C.; Stan, A.; Tatomir, A.; Popa, O.; Rosu, P.; Vulcan, A.-M.; Chira, D.; Popa, L.L.; Dina, C.; et al. Prediction of Neurocognitive Outcome after Moderate-Severe Traumatic Brain Injury Using Serum Neuron-Specific Enolase and S100 biomarkers. J. Med. Life 2020, 13, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Benussi, A.; Ashton, N.J.; Karikari, T.K.; Alberici, A.; Saraceno, C.; Ghidoni, R.; Benussi, L.; Zetterberg, H.; Blennow, K.; Borroni, B. Prodromal frontotemporal dementia: clinical features and predictors of progression. Alzheimer's Res. Ther. 2021, 13, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wei, R.; Christakos, S. Mechanisms Underlying the Regulation of Innate and Adaptive Immunity by Vitamin D. Nutrients 2015, 7, 8251–8260. [Google Scholar] [CrossRef]
- Bivona, G.; Agnello, L.; Ciaccio, M. The immunological implication of the new vitamin D metabolism. Cent. Eur. J. Immunol. 2018, 43, 331–334. [Google Scholar] [CrossRef]
- Gombash, S.E.; Lee, P.W.; Sawdai, E.; Lovett-Racke, A.E. Vitamin D as a Risk Factor for Multiple Sclerosis: Immunoregulatory or Neuroprotective? Front. Neurol. 2022, 13, 796933. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.; Ji, H.-F. Vitamin D deficiency is associated with increased risk of Alzheimer’s disease and dementia: evidence from meta-analysis. Nutr. J. 2015, 14, 76. [Google Scholar] [CrossRef] [PubMed]
- Al-Amin, M.; Bradford, D.; Sullivan, R.K.P.; Kurniawan, N.D.; Moon, Y.; Han, S.; Zalesky, A.; Burne, T.H.J. Vitamin D deficiency is associated with reduced hippocampal volume and disrupted structural connectivity in patients with mild cognitive impairment. Hum. Brain Mapp. 2018, 40, 394–406. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Shah, J. Vitamin D3 supplementation ameliorates cognitive impairment and alters neurodegenerative and inflammatory markers in scopolamine induced rat model. Metab. Brain Dis. 2022, 37, 2653–2667. [Google Scholar] [CrossRef]
- Syed, S.; Michalski, E.S.; Tangpricha, V.; Chesdachai, S.; Kumar, A.; Prince, J.; Ziegler, T.R.; Suchdev, P.S.; Kugathasan, S. Vitamin D Status Is Associated with Hepcidin and Hemoglobin Concentrations in Children with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2017, 23, 1650–1658. [Google Scholar] [CrossRef]
- Caviezel, D.; Maissen, S.; Niess, J.H.; Kiss, C.; Hruz, P. High Prevalence of Vitamin D Deficiency among Patients with Inflammatory Bowel Disease. Inflamm. Intest. Dis. 2017, 2, 200–210. [Google Scholar] [CrossRef]
- Schäffler, H.; Schmidt, M.; Huth, A.; Reiner, J.; Glass. ; Lamprecht, G. Clinical factors are associated with vitamin D levels in IBD patients: A retrospective analysis. J. Dig. Dis. 2017, 19, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef] [PubMed]
- Bajettoab, A.; Bonaviaab, R.; Barberoab, S.; Florioa, T.; Schettiniab, G. Chemokines and Their Receptors in the Central Nervous System. Front. Neuroendocr. 2001, 22, 147–184. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Fritzer-Szekeres, M.; Szekeres, T.; Gehrig, T.; Gyöngyösi, M.; Bergler-Klein, J. Comparison of High-Sensitivity C-Reactive Protein vs C-reactive Protein for Cardiovascular Risk Prediction in Chronic Cardiac Disease. J. Appl. Lab. Med. 2022, 7, 1259–1271. [Google Scholar] [CrossRef] [PubMed]
- Mańkowska-Wierzbicka, D.; Karczewski, J.; Poniedziałek, B.; Grzymisławska, M.; Staszewski, R.; Królczyk, A.; Dobrowolska, A.; Grzymisławski, M. C-reactive protein as a diagnostic and prognostic factor in inflammatory bowel diseases. 70, 1124. [Google Scholar] [CrossRef]
- Wilson, R.G.; Stevens, B.W.; Guo, A.Y.; Russell, C.N.; Thornton, A.; Cohen, M.A.; Sturgeon, H.C.; Giallourakis, C.; Khalili, H.; Nguyen, D.D.; et al. High C-Reactive Protein Is Associated with Poor Sleep Quality Independent of Nocturnal Symptoms in Patients with Inflammatory Bowel Disease. Dig. Dis. Sci. 2015, 60, 2136–2143. [Google Scholar] [CrossRef] [PubMed]
- Vinni, E. Alexithymic characteristics and interoceptive abilities are associated with disease severity and levels of C-reactive protein and cytokines in patients with inflammatory bowel disease. Ann. Gastroenterol. 2023, 36, 412. [Google Scholar] [CrossRef] [PubMed]
- Zheng, F.; Xie, W. High-sensitivity C-reactive protein and cognitive decline: the English Longitudinal Study of Ageing. Psychol. Med. 2017, 48, 1381–1389. [Google Scholar] [CrossRef]
- A Lewis, N.; E Knight, J. Longitudinal associations between C-reactive protein and cognitive performance in normative cognitive ageing and dementia. J. Am. Geriatr. Soc. 2021, 50, 2199–2205. [Google Scholar] [CrossRef]
- Komulainen, P.; Lakka, T.A.; Kivipelto, M.; Hassinen, M.; Penttilä, I.M.; Helkala, E.-L.; Gylling, H.; Nissinen, A.; Rauramaa, R. Serum high sensitivity C-reactive protein and cognitive function in elderly women. J. Am. Geriatr. Soc. 2007, 36, 443–448. [Google Scholar] [CrossRef]
- Dlugaj, M.; Gerwig, M.; Wege, N.; Siegrist, J.; Mann, K.; Bröcker-Preuß, M.; Dragano, N.; Moebus, S.; Jöckel, K.-H.; Bokhof, B.; et al. Elevated Levels of High-Sensitivity C-Reactive Protein are Associated with Mild Cognitive Impairment and its Subtypes: Results of a Population-Based Case-Control Study. J. Alzheimer's Dis. 2012, 28, 503–514. [Google Scholar] [CrossRef]
- Calderón-Ospina, C.A.; Nava-Mesa, M.O. B Vitamins in the nervous system: Current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS Neurosci. Ther. 2019, 26, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Akbulut, S. An assessment of serum vitamin B12 and folate in patients with Crohn’s disease. Medicine 2022, 101, e31892. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.G.; Kariyawasam, V.C.; Mogan, S.B.; Patel, K.V.; Pantelidou, M.; Sobczyńska-Malefora, A.; Porté, F.; Griffin, N.; Anderson, S.H.C.; Sanderson, J.D.; et al. Prevalence and Risk Factors for Functional Vitamin B12 Deficiency in Patients with Crohnʼs Disease. Inflamm. Bowel Dis. 2015, 21, 2839–2847. [Google Scholar] [CrossRef] [PubMed]
- Headstrom, P.D.; Rulyak, S.J.; Lee, S.D. Prevalence of and risk factors for vitamin B12 deficiency in patients with Crohnʼs disease. Inflamm. Bowel Dis. 2008, 14, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.; Mander, A.; Ames, D.; Carne, R.; Sanders, K.; Watters, D. Cognitive impairment and vitamin B12: a review. Int. Psychogeriatrics 2012, 24, 541–556. [Google Scholar] [CrossRef] [PubMed]
- Jatoi, S.; Hafeez, A.; Riaz, S.U.; Ali, A.; Ghauri, M.I.; Zehra, M. Low Vitamin B12 Levels: An Underestimated Cause Of Minimal Cognitive Impairment And Dementia. Cureus 2020, 12, e6976. [Google Scholar] [CrossRef] [PubMed]
- Guilland, J.-C.; Favier, A.; de Courcy, G.P.; Galan, P.; Hercberg, S. L’hyperhomocystéinémie : facteur de risque cardiovasculaire ou simple marqueur ?: 1. Données fondamentales. Pathol. Biol. 2003, 51, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Dawson, H.; Collins, G.; Pyle, R.; Deep-Dixit, V.; Taub, D.D. The immunoregulatory effects of homocysteine and its intermediates on T-lymphocyte function. Mech. Ageing Dev. 2004, 125, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Ientile, R.; Curro', M.; Ferlazzo, N.; Condello, S.; Caccamo, D.; Pisani, F. Homocysteine vitamin determinants and neurological diseases. Front. Biosci. 2010, S2, 359–372. [Google Scholar] [CrossRef]
- Danese, S.; Sgambato, A.; Papa, A.; Scaldaferri, F.; Pola, R.; Sans, M.; Lovecchio, M.; Gasbarrini, G.; Cittadini, A.; Gasbarrini, A. Homocysteine Triggers Mucosal Microvascular Activation in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2005, 100, 886–895. [Google Scholar] [CrossRef]
- Morgenstern, I.; Raijmakers, M.; Peters, W.; Hoensch, H.; Kirch, W. Homocysteine, Cysteine, and Glutathione in Human Colonic Mucosa: Elevated Levels of Homocysteine in Patients with Inflammatory Bowel Disease. Dig. Dis. Sci. 2003, 48, 2083–2090. [Google Scholar] [CrossRef] [PubMed]
- Levitt, A.J.; Karlinsky, H. Folate, vitamin B12 and cognitive impairment in patients with Alzheimer's disease. Acta Psychiatr. Scand. 1992, 86, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Levels of Vitamins and Homocysteine in Older Adults with Alzheimer Disease or Mild Cognitive Impairment in Cuba. MEDICC Rev. 2020, 22, 40. [CrossRef] [PubMed]
- Schulz, R.-J. Homocysteine as a biomarker for cognitive dysfunction in the elderly. Curr. Opin. Clin. Nutr. Metab. Care 2007, 10, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Farina, N.; Jernerén, F.; Turner, C.; Hart, K.; Tabet, N. Homocysteine concentrations in the cognitive progression of Alzheimer's disease. Exp. Gerontol. 2017, 99, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Busse, S.; von Hoff, F.; Borucki, K.; Frodl, T.; Busse, M. Association Between Homocysteine and Vitamin Levels in Demented Patients. J. Alzheimer's Dis. 2021, 81, 1781–1792. [Google Scholar] [CrossRef] [PubMed]
- Ma, F.; Zhou, X.; Li, Q.; Zhao, J.; Song, A.; An, P.; Du, Y.; Xu, W.; Huang, G. Effects of Folic Acid and Vitamin B12, Alone and in Combination on Cognitive Function and Inflammatory Factors in the Elderly with Mild Cognitive Impairment: A Single-blind Experimental Design. Curr. Alzheimer Res. 2019, 16, 622–632. [Google Scholar] [CrossRef]
- Jensen, L.E.; Whitehead, A.S. Regulation of serum amyloid A protein expression during the acute-phase response. Biochem. J. 1998, 334, 489–503. [Google Scholar] [CrossRef]
- Yokote, H.; Yagi, Y.; Watanabe, Y.; Amino, T.; Kamata, T.; Mizusawa, H. Serum amyloid A level is increased in neuromyelitis optica and atypical multiple sclerosis with smaller T2 lesion volume in brain MRI. J. Neuroimmunol. 2013, 259, 92–95. [Google Scholar] [CrossRef] [PubMed]
- Yarur, A.J.; Quintero, M.A.; Jain, A.; Czul, F.; Barkin, J.S.; Abreu, M.T. Serum Amyloid A as a Surrogate Marker for Mucosal and Histologic Inflammation in Patients with Crohnʼs Disease. Inflamm. Bowel Dis. 2017, 23, 158–164. [Google Scholar] [CrossRef]
- 10.1186/s12876-020-01229-8. PMID: 32245401; PMCID: PMC7118889.
- Crouch, P.J.; Harding, S.-M.E.; White, A.R.; Camakaris, J.; Bush, A.I.; Masters, C.L. Mechanisms of Aβ mediated neurodegeneration in Alzheimer's disease. Int. J. Biochem. Cell Biol. 2008, 40, 181–198. [Google Scholar] [CrossRef] [PubMed]
- Shim, K.H.; Kang, M.J.; Youn, Y.C.; An, S.S.A.; Kim, S. Alpha-synuclein: a pathological factor with Aβ and tau and biomarker in Alzheimer’s disease. Alzheimer's Res. Ther. 2022, 14, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Kirino, T.; Brightman, M.; Oertel, W.; Schmechel, D.; Marangos, P. Neuron-specific enolase as an index of neuronal regeneration and reinnervation. J. Neurosci. 1983, 3, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Shaik, A.J.; Reddy, K.; Mohammed, N.; Tandra, S.R.; Kandadai, R.M.; Kss, S.B. Neuron specific enolase as a marker of seizure related neuronal injury. Neurochem. Int. 2019, 131, 104509. [Google Scholar] [CrossRef] [PubMed]
- Scarna, H.; Delafosse, B.; Steinberg, R.; Debilly, G.; Mandrand, B.; Keller, A.; Pujol, J. Neuron-specific enolase as a marker of neuronal lesions during various comas in man. Neurochem. Int. 1982, 4, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Busikova-Malenovska, P.; Danis, D.; Bencat, M.; Galfiova, P.; Kopani, M.; Labajova, V.; El Hassoun, O.; Porubsky, J.; Galatova, J. Neuron-specific enolase in the intestinal wall in Crohn´s disease. Bratisl. Med J. 2014, 115, 381–382. [Google Scholar] [CrossRef] [PubMed]
- Haque, A.; Polcyn, R.; Matzelle, D.; Banik, N.L. New Insights into the Role of Neuron-Specific Enolase in Neuro-Inflammation, Neurodegeneration, and Neuroprotection. Brain Sci. 2018, 8, 33. [Google Scholar] [CrossRef] [PubMed]
- Villanacci, V.; Bassotti, G.; Nascimbeni, R.; Antonelli, E.; Cadei, M.; Fisogni, S.; Salerni, B.; Geboes, K.; Villanacci, V.; Bassotti, G.; et al. Enteric nervous system abnormalities in inflammatory bowel diseases. Neurogastroenterol. Motil. 2008, 20, 1009–1016. [Google Scholar] [CrossRef] [PubMed]
- Bagnato, S.; Andriolo, M.; Boccagni, C.; Lucca, L.F.; De Tanti, A.; Pistarini, C.; Barone, T.; Galardi, G. Reduced Neuron-Specific Enolase Levels in Chronic Severe Traumatic Brain Injury. J. Neurotrauma 2020, 37, 423–427. [Google Scholar] [CrossRef]
- Stancioiu, F.; Bogdan, R.; Dumitrescu, R. Neuron-Specific Enolase (NSE) as a Biomarker for Autistic Spectrum Disease (ASD). Life 2023, 13, 1736. [Google Scholar] [CrossRef]
- Gaetani, L.; Blennow, K.; Calabresi, P.; Di Filippo, M.; Parnetti, L.; Zetterberg, H. Neurofilament light chain as a biomarker in neurological disorders. J. Neurol. Neurosurg. Psychiatry 2019, 90, 870–881. [Google Scholar] [CrossRef]
- Wang, S.-Y.; Chen, W.; Xu, W.; Li, J.-Q.; Hou, X.-H.; Ou, Y.-N.; Yu, J.-T.; Tan, L. Neurofilament Light Chain in Cerebrospinal Fluid and Blood as a Biomarker for Neurodegenerative Diseases: A Systematic Review and Meta-Analysis. J. Alzheimer's Dis. 2019, 72, 1353–1361. [Google Scholar] [CrossRef]
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 2018, 14, 577–589. [Google Scholar] [CrossRef] [PubMed]
- Heizmann, C.W.; Fritz, G.; Schäfer, B.W. S100 proteins structure functions and pathology. Front. Biosci. 2002, 7, d1356–1368. [Google Scholar] [CrossRef]
- Kiss B, Ecsédi P, Simon M, Nyitray L. Isolation and Characterization of S100 Protein-Protein Complexes. Methods Mol Biol. 2019;1929:325-338. [CrossRef] [PubMed]
- Shang, X.; Cheng, H.; Zhou, R. Chromosomal mapping, differential origin and evolution of the S100 gene family. Genet. Sel. Evol. 2008, 40, 1–16. [Google Scholar] [CrossRef]
- Cirillo, C. S100B protein in the gut: The evidence for enteroglial-sustained intestinal inflammation. World J. Gastroenterol. 2011, 17, 1261–6. [Google Scholar] [CrossRef] [PubMed]
- Michetti, F.; Di Sante, G.; Clementi, M.E.; Sampaolese, B.; Casalbore, P.; Volonté, C.; Spica, V.R.; Parnigotto, P.P.; Di Liddo, R.; Amadio, S.; et al. Growing role of S100B protein as a putative therapeutic target for neurological- and nonneurological-disorders. Neurosci. Biobehav. Rev. 2021, 127, 446–458. [Google Scholar] [CrossRef] [PubMed]
- Bresnick, A.R. S100 proteins as therapeutic targets. Biophys. Rev. 2018, 10, 1617–1629. [Google Scholar] [CrossRef] [PubMed]
- Azman, K.F.; Zakaria, R. Recent Advances on the Role of Brain-Derived Neurotrophic Factor (BDNF) in Neurodegenerative Diseases. Int. J. Mol. Sci. 2022, 23, 6827. [Google Scholar] [CrossRef]
- Zuccato, C.; Cattaneo, E. Brain-derived neurotrophic factor in neurodegenerative diseases. Nat. Rev. Neurol. 2009, 5, 311–322. [Google Scholar] [CrossRef]
- Małczyńska, P.; Piotrowicz, Z.; Drabarek, D.; Langfort, J.; Chalimoniuk, M. Rola mózgowego czynnika neurotroficznego (BDNF) w procesach neurodegeneracji oraz w mechanizmach neuroregeneracji wywołanej wzmożoną aktywnością fizyczną. 65, 8. [CrossRef]
- Ibrahim, A.M.; Chauhan, L.; Bhardwaj, A.; Sharma, A.; Fayaz, F.; Kumar, B.; Alhashmi, M.; AlHajri, N.; Alam, S.; Pottoo, F.H. Brain-Derived Neurotropic Factor in Neurodegenerative Disorders. Biomedicines 2022, 10, 1143. [Google Scholar] [CrossRef] [PubMed]
- Konturek, T.J.; Martinez, C.; Niesler, B.; van der Voort, I.; Mönnikes, H.; Stengel, A.; Goebel-Stengel, M. The Role of Brain-Derived Neurotrophic Factor in Irritable Bowel Syndrome. Front. Psychiatry 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.-B.; Zuo, X.-L.; Zhao, Q.-J.; Chen, F.-X.; Yang, J.; Dong, Y.-Y.; Wang, P.; Li, Y.-Q. Brain-derived neurotrophic factor contributes to abdominal pain in irritable bowel syndrome. Gut 2011, 61, 685–694. [Google Scholar] [CrossRef]
- Sochal, M.; Ditmer, M.; Binienda, A.; Gabryelska, A.; Białasiewicz, P.; Talar-Wojnarowska, R.; Fichna, J.; Małecka-Wojciesko, E. Relation between Selected Sleep Parameters, Depression, Anti-Tumor Necrosis Factor Therapy, and the Brain-Derived Neurotrophic Factor Pathway in Inflammatory Bowel Disease. Metabolites 2023, 13, 450. [Google Scholar] [CrossRef] [PubMed]
- Economos, A.; Wright, C.B.; Moon, Y.P.; Rundek, T.; Rabbani, L.; Paik, M.C.; Sacco, R.L.; Elkind, M.S. Interleukin 6 Plasma Concentration Associates with Cognitive Decline: The Northern Manhattan Study. Neuroepidemiology 2013, 40, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Hosokawa, T.; Kusugami, K.; Ina, K.; Ando, T.; Shinoda, M.; Imada, A.; Ohsuga, M.; Sakai, T.; Matsuura, T.; Ito, K.; et al. Interleukin-6 and soluble interleukin-6 receptor in the colonic mucosa of inflammatory bowel disease. J. Gastroenterol. Hepatol. 1999, 14, 987–996. [Google Scholar] [CrossRef]
- Aggarwal, M.M.; Alkhayyat, M.; Saleh, M.A.; Sarmini, M.T.; Singh, A.; Garg, R.; Garg, P.M.; Mansoor, E.; Padival, R.; Cohen, B.L.M. Alzheimer Disease Occurs More Frequently In Patients With Inflammatory Bowel Disease. J. Clin. Gastroenterol. 2022, 57, 501–507. [Google Scholar] [CrossRef] [PubMed]
- Roberts, R.O.; Geda, Y.E.; Knopman, D.S.; Boeve, B.F.; Christianson, T.J.; Pankratz, V.S.; Kullo, I.J.; Tangalos, E.G.; Ivnik, R.J.; Petersen, R.C. Association of C-reactive protein with mild cognitive impairment. Alzheimer's Dement. 2009, 5, 398–405. [Google Scholar] [CrossRef] [PubMed]
- Haapamäki, M.M.; Grönroos, J.M.; Nurmi, H.; Söderlund, K.; Peuravuori, H.; Alanen, K.; Nevalainen, T.J. Elevated Group 11 Phospholipase A2 Mass Concentration in Serum and Colonic Mucosa in Crohn's Disease. cclm 1998, 36, 751–755. [Google Scholar] [CrossRef]
- Andreadou, E.G.; Katsipis, G.; Tsolaki, M.; Pantazaki, A.A. Involvement and relationship of bacterial lipopolysaccharides and cyclooxygenases levels in Alzheimer's Disease and Mild Cognitive Impairment patients. J. Neuroimmunol. 2021, 357, 577561. [Google Scholar] [CrossRef]
- Otani, T.; Yamaguchi, K.; Scherl, E.; Du, B.; Tai, H.-H.; Greifer, M.; Petrovic, L.; Daikoku, T.; Dey, S.K.; Subbaramaiah, K.; et al. Levels of NAD+-dependent 15-hydroxyprostaglandin dehydrogenase are reduced in inflammatory bowel disease: evidence for involvement of TNF-α. Am. J. Physiol. Liver Physiol. 2006, 290, G361–G368. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.-L.; Shen, Y.-D.; Zhang, Y.-C.; Hu, X.-Y.; Lu, P.-L.; Wang, L.; Chen, W. Roles of the prostaglandin E2 receptors EP subtypes in Alzheimer’s disease. Neurosci. Bull. 2010, 26, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Manning, B.P.; Sharkey, K.A.; Mawe, G.M. Effects of PGE2 in guinea pig colonic myenteric ganglia. Am. J. Physiol. Liver Physiol. 2002, 283, G1388–G1397. [Google Scholar] [CrossRef]
- Li, L.; Liu, Z.; Yang, X.; Yan, H.; Bao, S.; Fei, J. Bioluminescence imaging for IL-1β expression in experimental colitis. J. Inflamm. 2013, 10, 16–6. [Google Scholar] [CrossRef] [PubMed]
- Cominelli, F.; Nast, C.C.; Clark, B.D.; Schindler, R.; Lierena, R.; E Eysselein, V.; Thompson, R.C.; A Dinarello, C. Interleukin 1 (IL-1) gene expression, synthesis, and effect of specific IL-1 receptor blockade in rabbit immune complex colitis. J. Clin. Investig. 1990, 86, 972–980. [Google Scholar] [CrossRef] [PubMed]
- Griffin WS, Mrak RE. Interleukin-1 in the genesis and progression of and risk for development of neuronal degeneration in Alzheimer's disease. J Leukoc Biol. 2002;72(2):233-238.
- Berrill, J.W.; Gallacher, J.; Hood, K.; Green, J.T.; Matthews, S.B.; Campbell, A.K.; Smith, A.; Berrill, J.W.; Gallacher, J.; Hood, K.; et al. An observational study of cognitive function in patients with irritable bowel syndrome and inflammatory bowel disease. Neurogastroenterol. Motil. 2013, 25, 918–e704. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.-B.; Sheng, G.-Q. 白介素1β 与学习和记忆. Neurosci. Bull. 2010, 26, 455–468. [Google Scholar] [CrossRef] [PubMed]
- Silva, L.C.; Ortigosa, L.C.; Benard, G. Anti-TNF-α agents in the treatment of immune-mediated inflammatory diseases: mechanisms of action and pitfalls. Immunotherapy 2010, 2, 817–833. [Google Scholar] [CrossRef] [PubMed]
- Gray, M.A.; Chao, C.-Y.; Staudacher, H.M.; Kolosky, N.A.; Talley, N.J.; Holtmann, G. Anti-TNFα therapy in IBD alters brain activity reflecting visceral sensory function and cognitive-affective biases. PLOS ONE 2018, 13, e0193542. [Google Scholar] [CrossRef]
- Cheng, L.; Dong, R.; Song, C.; Li, X.; Zhang, L.; Shi, M.; Lv, C.; Wang, L.; Kou, J.; Xie, H.; et al. Mediation Effects of IL-1β and IL-18 on the Association Between Vitamin D Levels and Mild Cognitive Impairment Among Chinese Older Adults: A Case–Control Study in Taiyuan, China. Front. Aging Neurosci. 2022, 14, 836311. [Google Scholar] [CrossRef]
Figure 1.
Methodology of research.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



