
Submitted:
02 April 2024
Posted:
02 April 2024
You are already at the latest version
Abstract
Prostate cancer lung metastasis represents a clinical conundrum due to their implication of advanced disease progression and the complexities they introduce in treatment planning. As the disease progresses to distant sites such as the lung, the clinical management becomes increasingly intricate, requiring tailored therapeutic strategies to address the unique characteristics of metastatic lesions. This review seeks to synthesize the current state of knowledge surrounding prostate cancer metastasis to the lung, shedding light on the diverse array of clinical presentations encountered, ranging from subtle radiological findings to overt symptomatic manifestations. By examining the diagnostic modalities utilized in identifying this metastasis, including advanced imaging techniques and histopathological analyses, the review aims to provide insights into the diagnostic landscape and the challenges associated with accurately characterizing lung metastatic lesions in prostate cancer patients. Moreover, the review delves into the nuances of therapeutic interventions employed in managing prostate cancer lung metastasis, encompassing systemic treatments such as hormonal therapies and chemotherapy, as well as metastasis-directed therapies including surgery and radiotherapy.
Keywords:
Prostate Cancer
; Lung Metastasis
; Systemic Therapy
; Metastasis-Directed therapy
1. Introduction
Prostate cancer (PCa) remains the most predominant and second-leading cause of cancer-related deaths among males, as well as, it has attained the status of being the primary cancer with a high incidence-to-mortality ratio in the US [1,2]. Despite the favorable control of the disease and survival outcomes following the radical prostatectomy for the localized disease, distant metastasis ultimately occurs in 17%, and out of those patients, 20-30% acquire visceral metastasis [3,4,5]. Distant metastasis, particularly visceral metastasis, has a significant negative prognostic factor, resulting in poorer health-related quality of life and a rise in cancer-related mortalities [3,6,7]. Despite this, not all patients with visceral metastasis have a consistently severe disease progression. Indeed, patients with lung metastasis often have a more favorable course of disease than those with liver metastasis, and the prognosis is more akin to lymph node or bone metastasis [8,9].
As reported by autopsy studies, lung metastasis have been identified as the second most prevalent extranodal metastasis in PCa (46%), behind bone metastasis (90%) [10]. With different pathways of PCa dissemination, the most common pathway for lung involvement with PCa is through the Caval pathway, which signifies a critical juncture in the disease course, indicating both the aggressiveness of the cancer and its potential to infiltrate vital circulatory pathways. The inferior vena cava, as a major conduit for venous blood return to the heart, becomes a conduit for cancer cells originating from the prostate gland. This infiltration not only poses challenges in terms of treatment but also raises concerns regarding the potential for systemic dissemination [10]. The lungs, being a common destination for metastatic spread due to their rich vascularization, become a site where these cancer cells may seed and form secondary tumors, further compromising respiratory function and overall health [10].
Over the past years, there has been a noticeable rise in the occurrence of lung metastasis stemming from prostate cancer (PCa) [11]. Enhanced imaging techniques such as C11-Choline and Ga-68 prostate-specific membrane antigen (PSMA) PET scans are believed to offer improved capabilities in detecting lung metastasis in the early stages. Additionally, the introduction of new systemic treatment options has contributed to enhanced longevity and improved survival outcomes for patients with PCa [12]. With different lines of treatment proposed for this group of patients, there are still various obstacles encountered in adequately understanding, diagnosing, and treating PCa patients with lung metastasis. Given the dearth of understanding about metastatic lung lesions in PCa, we decided to conduct a comprehensive review of the most recent evidence on the clinical presentations, diagnostic methods, therapeutic approaches, and prognosis of lung metastasis in PCa.
2. Materials and Methods
2.1. Literature Search Strategy
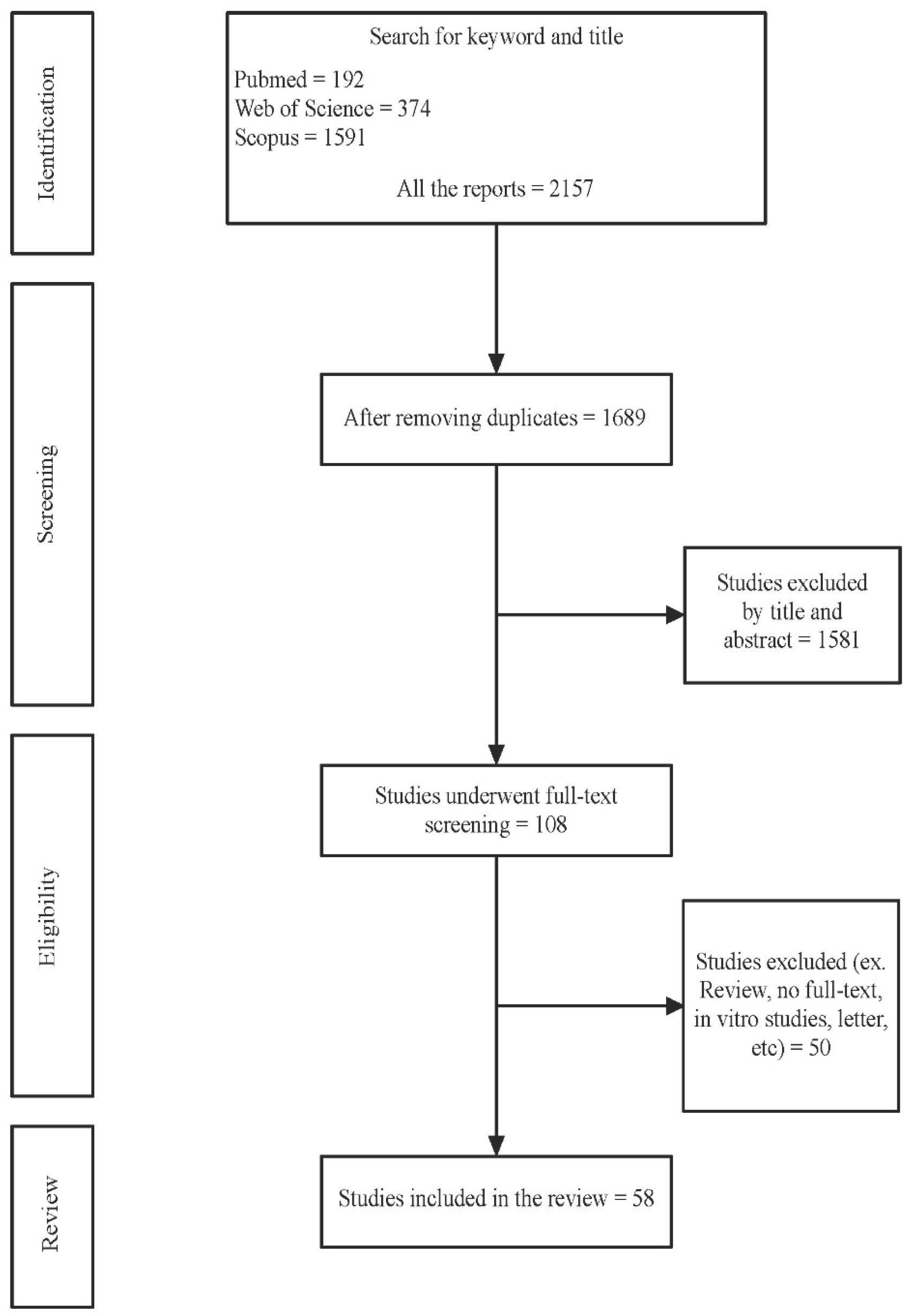
We conducted a comprehensive literature search to identify relevant studies focusing on prostate cancer metastasis to the lung. Electronic databases including PubMed/MEDLINE, Embase, and Web of Science were searched up to February 1st, 2024, without any language restrictions. The search strategy included a combination of keywords and medical subject headings (MeSH) terms related to prostate cancer lung metastasis such as “prostate cancer,” “metastatic prostate cancer,” “advanced prostate cancer,” “lung metastasis, “ “lung neoplasm,” “pulmonary metastasis,” and “prostate lung metastasis,”. Additionally, manual searches of reference lists from retrieved articles and relevant review papers were performed to ensure the inclusivity of the review. Figure 1 presents the flowchart of our searching through the literature.
2.2. Literature Search Strategy
Studies were included if they met the following criteria: (1) original research articles, case reports, or review articles investigating prostate cancer metastasis to the lung, (2) studies reporting clinical characteristics, diagnostic modalities, treatment approaches, or outcomes related to prostate cancer lung metastasis, and (3) availability of full-text articles. Studies were excluded if they were duplicates, conference abstracts, editorials, letters, commentaries or describing patients who had other primary malignancies.
2.3. Study Selection and Data Extraction
Two independent reviewers (A.M.M and A.M) screened the titles and abstracts of the identified records to assess their eligibility for inclusion. Discrepancies were resolved through discussion or consultation with a third reviewer (C.A). Full-text articles of potentially eligible studies were retrieved and assessed for final inclusion based on predefined criteria. Data were extracted using a standardized data extraction form, including study characteristics (e.g., author, year of publication), patient demographics, primary tumor characteristics, diagnostic methods, treatment modalities, and outcomes related to prostate cancer lung metastasis.
Figure 1.
Flow diagram of the study selection.
3. Prostate Cancer Lung Metastasis Presentations
3.1. Clinical and Laboratories
PCa lung metastasis may manifest with symptoms that primarily result from the spread of cancer cells to the lungs. In the early stages, individuals may not experience noticeable symptoms, and the metastasis may be asymptomatic [13,14,15]. However, as the disease progresses and the metastatic lesions affect lung function and adjacent structures, various symptoms may emerge. Persistent coughing, often accompanied by the production of sputum, can develop as a consequence of parenchymal lung involvement. Shortness of breath, or dyspnea, may occur due to impaired respiratory function caused by the presence of metastatic nodules. Chest pain may be present, resulting from the irritation or compression of surrounding tissues by the growing metastasis. In some cases, hemoptysis, or coughing up blood, may occur, though this is relatively uncommon. Generalized fatigue and weakness may be attributed to the overall burden of the disease on the body [16].
As in Table 1, most of the patients across all the studies were asymptomatic, while only 13 out of the 58 studies included reported variable clinical symptoms ranging from general symptoms such as hematuria, increased urinary frequency, and weight loss to pulmonary symptoms like cough, dyspnea, chest pain, and hemoptysis [17,18,19,20,21,22,23,24,25,26,27,28,29]. Several factors contributed to the presenting symptoms, including the number and location of the metastatic lesions. In terms of clinical characteristics for those patients, the median age was 69 years, with a median Gleason score and PSA at the time of lung metastasis diagnosis of 8 and 3.8 ng/ml, respectively.
3.2. Diagnostic Methods
Although the involvement of the lung by prostate cancer is infrequent compared with lymph nodes or bone, it represents a significant presentation, especially in patients with widespread metastasis and the dissemination of the tumor to various organs. This situation carries substantial consequences for patient prognosis and overall survival. Hence, it is imperative to prioritize early diagnosis and intervention, particularly in patients with a heightened clinical suspicion of metastasis [30]. With different diagnostic methods of PCa lung metastasis, herein we have sorted and examined them distinctly, considering the specific characteristics of each diagnostic approach.
3.2.1. Imaging Modalities
Various imaging techniques can be utilized to detect lung metastasis as mentioned in Table 1, including chest X-ray (CXR), computed tomography (CT) scan, magnetic resonance imaging (MRI), and positron emission tomography (PET) scan. The selection of the optimal imaging method depends on factors like the tumor’s biological behavior, the sensitivity and specificity of the imaging modality, considerations regarding radiation exposure, and cost-effectiveness. The decision is tailored to the specific clinical situation to ensure precise diagnosis and effective treatment planning. Lung metastasis in advanced prostate cancer often exhibits either a lymphangitic or nodular radiological profile. The higher occurrence of the lymphangitic pattern is attributed to the direct invasion of lung lymphatics, while the nodular pattern results from hematogenous spread [10].
Nodular involvement is the most common observation, whereas pulmonary lymphangitic involvement by prostate cancer is extremely rare, occurring in less than 0.2% of patients [31]. Lymphangitic involvement termed pulmonary lymphangitic carcinomatosis is pathologically defined by the presence of tumor thrombi within the lymphatic vessels of bronchovascular bundles, interlobular septa, and pleura. On imaging, it typically presents as multiple linear densities forming a reticular network with thickened and irregular broncho-vascular bundles. Another frequently observed radiographic presentation is the “tree-in-bud” pattern, which illustrates bronchiolar luminal impaction outlining the usually unseen peripheral airway branching [32,33,34]. Atypical PCa lung metastasis presentations were reported in the literature including cavitating, excavated, cystic lesions, and nodules with ground glass appearance [27,35,36].
Historically, chest X-rays were used as the primary imaging modality for detecting lung metastasis in PCa. On X-rays, the lung metastasis usually appears as multiple round or oval-shaped nodules with calcification in some cases. However, X-rays have limitations in detecting smaller lesions and providing detailed information [26,37,38,39,40,41]. Even though, in some cases, chest X-ray may be part of the initial diagnostic workup or used for monitoring purposes. It can offer a broad overview of the lungs and may detect larger or more advanced lung metastasis [42].
Therefore, more advanced imaging techniques, such as CT scans and MRI, are generally preferred for evaluating the presence of metastasis in the lungs. The CT scan is the most sensitive imaging method for detecting pulmonary metastasis due to its superior spatial and contrast resolution and the absence of overlap with adjacent structures like bones and vessels [43]. In comparison to Chest X-ray (CXR), a CT scan can identify a greater number of nodules, including those smaller than 5 mm, and it can detect approximately three times as many noncalcified nodules. Additionally, CT scans can reveal various findings, such as lymphadenopathy, involvement of the pleura, chest wall, airways, and blood vessels, as well as abnormalities in the upper abdomen and bones, all of which may have an impact on treatment decisions [44].
PCa lung metastasis can appear differently on CT chest and MRI images. In a CT chest scan, metastatic lesions may present as nodules or masses within the lung tissue. These nodules can vary in size and density [42]. On MRI images of the chest, metastatic lesions may appear as areas with abnormal signal intensity. MRI is particularly useful for soft tissue imaging, and it can provide detailed information about the anatomy and characteristics of lesions [45]. It’s important to note that the appearance of prostate cancer lung metastasis on imaging studies can be diverse, and the interpretation may depend on various factors such as the size and location of the lesions, as well as the specific imaging techniques used [45].
Nowadays, PET scans play a significant role in the assessment of PCa patients in general and lung metastasis specifically, offering valuable insights into the metabolic activity of tissues. Unlike anatomical imaging techniques like CT or MRI, PET scans provide functional information by detecting areas of increased metabolism, which aids in distinguishing between benign and malignant lesions. particularly advantageous for detecting widespread or multifocal metastasis [46]. The use of PET scans in conjunction with CT scans, known as PET/CT fusion imaging, further enhances diagnostic accuracy by combining anatomical and functional information. This hybrid imaging approach allows for precise localization of hypermetabolic lesions within the lung tissue and facilitates a comprehensive assessment of the extent and distribution of metastasis. Additionally, PET scans can be instrumental in monitoring treatment response and detecting disease recurrence, aiding clinicians in making informed decisions regarding the management of lung metastasis [46].
Despite the advantages of PET scans, few research articles investigate the use of Ga-PSMA PET/CT in evaluating lung metastasis in prostate cancer (PCa). Damjanovic et al. (2019) conducted a study encompassing 739 PCa patients, revealing 91 confirmed lung metastases in 20 individuals. Their findings demonstrated that 72.5% of this metastasis exhibited PSMA-positive characteristics, while 27.5% were PSMA-negative. Despite the prevalent PSMA expression in most lung metastasis, a significant subset displayed PSMA negativity. Additionally, benign pulmonary lesions exhibited a moderate tracer uptake, lower than that seen in PSMA-positive lung metastasis but higher than PSMA-negative ones. Consequently, the sole reliance on the SUVmax of 68Ga-PSMA PET proved inadequate for distinguishing pulmonary metastasis from benign lung lesions [47]. This conclusion corresponds with the outcomes of Pyka et al., which similarly emphasized the difficulty in discerning lung metastasis of PCa from primary lung cancer based on the SUVmax values of 68Ga-PSMA PET [48].
3.2.2. Histopathology
Histopathological analysis of lung metastasis in prostate cancer provides invaluable insights into the biological behavior and characteristics of the metastatic lesions. PCa cells in lung metastasis often retain the glandular features seen in the primary tumor, aiding in their identification. The majority of lung metastasis in prostate cancer arise from prostate adenocarcinoma, given its status as the most prevalent histological subtype of PCa [14,15,49,50]. Nevertheless, less common histological subtypes, such as small cell carcinoma and neuroendocrine carcinoma of the prostate, have been documented [51,52,53,54]. In addition to its role in tumor staging, histology plays a significant role in understanding the dissemination of prostate cancer to the lungs. Hematoxylin and eosin staining of lung metastasis in prostate adenocarcinoma reveal glandular patterns, a characteristic further confirmed by positive prostate-specific antigen (PSA) staining in immunohistochemistry [16].
The histopathological examination may also reveal the extent of differentiation and the presence of any unique markers, contributing to a more comprehensive understanding of the tumor’s molecular profile. This detailed examination is crucial for accurate diagnosis, determining the appropriate course of treatment, and assessing the potential impact on patient prognosis. Additionally, histopathology plays a pivotal role in guiding personalized therapeutic approaches and advancing our knowledge of the complex nature of prostate cancer metastasis to the lungs. In light of our research findings, which indicate that ultrasound or CT-guided biopsy and tissue evaluation were commonly employed in most of the studies, it can be inferred that histopathology stands out as the most accurate method for diagnosing lung metastasis in PCa [12,13,21].
3.2.3. Molecular and Genetics
The molecular and genetic landscape of prostate cancer lung metastasis is intricate, reflecting the heterogeneity of the disease. Recent advancements in genomic profiling have unveiled a spectrum of genetic alterations that influence the evolution of metastatic lesions. Dysregulation of genes involved in DNA repair mechanisms, cell cycle control, and chromatin modification pathways are among the molecular events associated with prostate cancer metastasis to the lungs [55]. Notably, studies have highlighted the role of specific genetic markers, including TMPRSS2-ERG rearrangements and alterations in the TP53 gene, in driving the metastatic potential of prostate cancer cells [56,57]. The evolving field of somatic cancer genotyping plays a pivotal role in categorizing metastatic diseases, aiding in the differentiation of aggressive and indolent phenotypes [55,58]. Specific genomic alterations, notably compound disruptions of tumor suppressor genes or deficiencies in DNA damage repair genes, are frequently observed in prostate cancers with high-risk clinical features [59].
Historically, the genomic features of lung metastasis were poorly explored in the literature apart from two case series that investigated the genomics of lung metastasis on metastatic hormone sensitive PCa (mHSPC) patients [56,60]. Shenderoev et al. identified 16 mHSPC patients with plenty of variations in mismatch repair (MMR) genes, homologous recombination deficit (HRD) genes, PI3K pathway genes, Wnt signaling pathway genes, and TP53 mutations [56]. Another study by Fonseca et al. observed a potential, increase in changes affecting PTEN and the Wnt/β-catenin signaling genes RNF43 and APC, which underscores the necessity for further studies into the cellular pathways facilitating the spread of metastasis in the lung. Additionally, in some rare cases, the immunohistochemical assessment may reveal negative results for PSA, NKX3.1, and p501s, which are commonly used biomarkers for prostatic adenocarcinoma and showed a positivity for synaptophysin and chromogranin A which indicates adenocarcinoma of the prostate with neuroendocrine differentiation [61].
The identification of these molecular and genetic signatures not only contributes to a deeper understanding of the disease’s biology but also holds promise for the development of targeted therapies tailored to the genetic makeup of individual tumors. The evolving field of targeted therapies seek to capitalize on these molecular insights to design more effective and personalized treatment strategies for PCa patients with lung metastasis [60].
4. Treatment Approaches
The management of PCa lung metastasis necessitates a comprehensive approach tailored to individual patient characteristics and disease factors. As in Table 1, treatment options typically involve systemic therapies, such as androgen deprivation therapy (ADT), androgen receptor pathway inhibitor (ARPI), chemotherapy, and radioligand drug, along with metastasis-directed therapies which aimed at alleviating symptoms and controlling disease progression.
4.1. Systemic Therapies
Androgen deprivation therapy (ADT) serves as a pivotal component in managing lung metastasis stemming from prostate cancer, offering a multifaceted approach to impede disease progression. By curtailing the production of testosterone and other androgens, ADT exerts palliative effects, effectively slowing the advancement of metastatic prostate cancer. This therapeutic strategy remains a cornerstone in the treatment arsenal, contributing significantly to improving patient outcomes [12,15,17,18,20,21,23,25,28,29,39,40,52,62,63,64,65,66,67,68,69,70,71,72,73,74,75]. Another class which is the ARPIs represent promising therapeutic options in the management of prostate cancer lung metastasis, offering targeted inhibition of the androgen receptor pathway to impede disease progression and alleviate symptoms [29,74]. ARPIs disrupt the signaling cascade essential for prostate cancer cell growth and survival, thereby exerting a profound anti-tumor effect. Clinical trials and real-world evidence have demonstrated the efficacy of ARPI in delaying disease progression, and prolonging overall survival in patients with metastatic prostate cancer, including those with lung involvement [30,76]. By specifically targeting the androgen receptor pathway, ARPI addresses the underlying molecular drivers of prostate cancer metastasis, offering a targeted and personalized approach to treatment. Its favorable safety profile and oral administration further enhance its appeal as a therapeutic option for patients with prostate cancer lung metastasis, underscoring its role as a cornerstone in the evolving landscape of prostate cancer management [77,78].
Chemotherapy plays a significant role in the management of prostate cancer lung metastasis, particularly in cases of castration-resistant prostate cancer (CRPC) where other treatments may have limited efficacy. Chemotherapeutic agents such as docetaxel and cabazitaxel are commonly used to target rapidly dividing cancer cells and inhibit tumor growth [79]. These agents are administered either alone or in combination with other treatments to maximize their effectiveness. While chemotherapy may not be curative, it can help alleviate symptoms, and prolong survival in patients with metastatic prostate cancer, including those with lung involvement [79].
177Lu-PSMA therapy represents a promising and evolving radioligand treatment approach for patients with prostate cancer lung metastasis, offering targeted radiation therapy directed at prostate-specific membrane antigen (PSMA)-expressing tumor cells [80]. This innovative therapy utilizes radiolabeled PSMA ligands to deliver therapeutic doses of beta radiation selectively to prostate cancer cells while sparing surrounding healthy tissues. By targeting PSMA, which is highly expressed on prostate cancer cells, 177Lu-PSMA therapy holds the potential to effectively eradicate metastatic lesions in the lungs, offering a personalized and precise treatment option [80,81]. Several studies have demonstrated encouraging results, with significant reductions in PSA levels, tumor burden, and in some cases a complete regression of multiple lung lesions as reported by Zhang et al. [81,82,83,84]. While further research is needed to optimize treatment protocols and assess long-term outcomes, 177Lu-PSMA therapy represents a promising therapeutic strategy in the management of prostate cancer lung metastasis, offering hope for improved outcomes for affected patients [80,84].
4.2. Metastasis-Directed Therapies (MDT)
Localized approaches such as radiation therapy or surgical resection may also be considered for palliation of symptoms or to address oligometastatic disease. The choice of treatment modality depends on various factors, including the extent of metastatic spread, the aggressiveness of the disease, the patient’s overall health status, and individual treatment goals [68]. Multidisciplinary collaboration among oncologists, urologists, radiation oncologists, thoracic surgeons, and other specialists is crucial in formulating personalized treatment plans that optimize survival outcomes for patients with prostate cancer lung metastasis.
Surgical resection of prostate cancer lung metastasis remains a controversial yet potentially beneficial option in select cases, particularly when metastases are localized and deemed resectable [68,85]. While systemic therapies such as hormone therapy and chemotherapy are often the mainstays of treatment for metastatic prostate cancer, surgical intervention may be considered for patients with limited metastatic burden and good overall health. The goal of surgical resection is to remove visible metastatic lesions from the lungs, potentially providing symptomatic relief, prolonging progression-free survival, and offering a chance for cure in some cases [85]. In a retrospective cohort study, surgical resection either alone or combined with systemic therapy was linked with favorable survival outcomes compared with systemic therapy alone [68]. However, the decision to proceed with surgery requires careful consideration of various factors including the location and size of metastatic lesions, the extent of metastatic disease, the patient’s general health status, and their willingness to undergo surgery [86]. Additionally, surgical resection is typically reserved for patients with oligometastatic disease, where metastasis are confined to a limited number of sites [86]. While surgical resection of prostate cancer lung metastasis may offer potential benefits, including improved quality of life and prolonged survival, it is essential to weigh the risks and benefits carefully and to individualize treatment decisions based on each patient’s unique circumstances [63,85].
Radiotherapy emerges as a vital component in the multimodal approach to managing prostate cancer lung metastasis, offering targeted and localized treatment to control disease progression [87]. With advancements in radiotherapy techniques such as intensity-modulated radiation therapy (IMRT) and image-guided radiotherapy (IGRT), precise delivery of radiation to metastatic lesions in the lungs is achievable while minimizing toxicity to surrounding healthy tissues. Moreover, emerging evidence supports the efficacy of stereotactic ablative radiotherapy (SABR), also known as stereotactic body radiotherapy (SBRT), in delivering high doses of radiation in a limited number of treatment sessions, thereby providing a convenient and effective treatment option for patients [83,84,85]. By delivering focused radiation to metastatic lesions, several studies showed that radiotherapy can induce tumor regression, improve local control, and complete resolution for patients with prostate cancer lung metastasis [12,15,24,29,41,49,73,87].
5. Prognosis and Oncological Outcomes
Metastasis to visceral organs in prostate cancer (PCa) typically indicate unfavorable disease outcomes [3,90]. Nevertheless, the clinical progression of patients with visceral metastasis can vary significantly. Specifically, patients with lung metastasis tend to experience a more favorable disease course compared to other sites of visceral metastasis [8]. As in Table 1, prognosis and survival outcomes in prostate cancer lung metastasis vary significantly according to the present studies, with survival ranging from 3 to 88 months and a median survival of 26 months [13,15,17,18,20,21,23,24,25,28,29,37,39,40,49,51,52,62,63,64,65,66,67,69,70,73,74,75,85,86,91,92,93,94,95,96]. The survival outcomes depend on several factors, including the extent of metastatic spread, the aggressiveness of the disease, the presence of comorbidities, and the effectiveness of treatment interventions [76].
Generally, prostate cancer lung metastasis is associated with a poorer prognosis compared to localized disease, reflecting the advanced stage of the cancer and the challenges in managing metastatic spread [30,76]. However, with advancements in treatment modalities such as systemic therapies and MDT, there has been a notable improvement in survival outcomes for those patients [30,68,76]. Despite these advancements, prognosis remains variable, and individualized treatment plans tailored to each patient’s specific circumstances are crucial in optimizing outcomes [68]. Multidisciplinary collaboration among healthcare providers is essential in providing comprehensive care and support to patients with prostate cancer lung metastasis, with the ultimate goal of improving prognosis and enhancing overall survival.
6. Conclusions
Prostate cancer lung metastasis represents a significant clinical challenge, often indicating advanced disease progression and posing therapeutic dilemmas for clinicians. Through this comprehensive review, we have synthesized current evidence regarding the wide variety of clinical presentations, diagnostic methods, therapeutic approaches, and prognosis associated with prostate cancer metastasizing to the lung. With the complexity of prostate cancer lung metastasis presentations, continued research efforts aimed at elucidating underlying mechanisms, identifying novel therapeutic targets, and optimizing treatment strategies are paramount. Furthermore, interdisciplinary collaboration and patient-centered care are essential in navigating the complexities of managing these metastatic lesions and improving the quality of life and survival outcomes of those patients.
Author Contributions
Conceptualization, A.M.M. and A.M.; methodology, A.M.M.; data collection, A.M., C.D., W.Z, and M.E.A.; writing—original draft preparation, A.M.M. and A.M.; writing—review and editing, S.B., R.H, M.M., M.M., D.S.C., J.J.O., I.B.R., A.T.K., B.J.S., and B.J.D.; supervision, J.R.A., and E.D.K; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer Statistics, 2021. CA Cancer J Clin. 2021;71(1):7-33.
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17-48.
- Goodman, O.B.; Flaig, T.W.; Molina, A.; A Mulders, P.F.; Fizazi, K.; Suttmann, H.; Li, J.; Kheoh, T.; de Bono, J.S.; I Scher, H. Exploratory analysis of the visceral disease subgroup in a phase III study of abiraterone acetate in metastatic castration-resistant prostate cancer. Prostate Cancer Prostatic Dis. 2013, 17, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Schymura MJ, Sun L, Percy-Laurry A. Prostate cancer collaborative stage data items--their definitions, quality, usage, and clinical implications: a review of SEER data for 2004-2010. Cancer. 2014;120 Suppl 23:3758-3770.
- Scosyrev E, Messing EM, Mohile S, Golijanin D, Wu G. Prostate cancer in the elderly: frequency of advanced disease at presentation and disease-specific mortality. Cancer. 2012;118(12):3062-3070.
- Norgaard M, Jensen AO, Jacobsen JB, Cetin K, Fryzek JP, Sorensen HT. Skeletal related events, bone metastasis and survival of prostate cancer: a population-based cohort study in Denmark (1999 to 2007). J Urol. 2010;184(1):162-167.
- Rigaud J, Tiguert R, Le Normand L, et al. Prognostic value of bone scan in patients with metastatic prostate cancer treated initially with androgen deprivation therapy. J Urol. 2002;168(4 Pt 1):1423-1426.
- Nakamachi H, Suzuki H, Akakura K, et al. Clinical significance of pulmonary metastasis in stage D2 prostate cancer patients. Prostate Cancer Prostatic Dis. 2002;5(2):159-163.
- Pond, G.R.; Sonpavde, G.; de Wit, R.; Eisenberger, M.A.; Tannock, I.F.; Armstrong, A.J. The Prognostic Importance of Metastatic Site in Men with Metastatic Castration-resistant Prostate Cancer. Eur. Urol. 2014, 65, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Bubendorf, L.; Schöpfer, A.; Wagner, U.; Sauter, G.; Moch, H.; Willi, N.; Gasser, T.C.; Mihatsch, M.J. Metastatic patterns of prostate cancer: An autopsy study of 1,589 patients. Hum. Pathol. 2000, 31, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Chen H, Stoltzfus KC, Lehrer EJ, et al. The Epidemiology of Lung Metastasis. Front Med (Lausanne). 2021;8:723396.
- Damjanovic J, Janssen JC, Furth C, et al. (68) Ga-PSMA-PET/CT for the evaluation of pulmonary metastasis and opacities in patients with prostate cancer. Cancer Imaging. 2018;18(1):20.
- Ceylan KC, Batihan G, Kaya SO. Pulmonary metastasis in urogenital cancers: Surgical treatment and outcomes. Cir Esp (Engl Ed). 2023;101(2):116-122.
- Delbare F, Villeirs G. Cavitary Lung Metastasis in Prostate Cancer. J Belg Soc Radiol. 2022;106(1):137.
- Kosaka, T.; Iizuka, S.; Yoneda, T.; Otsuki, Y.; Nakamura, T. Solitary pulmonary nodule as the initial manifestation of isolated metastasis from prostate cancer without bone involvement: A case report. Int. J. Surg. Case Rep. 2021, 90, 106681. [Google Scholar] [CrossRef] [PubMed]
- Tohfe, M.; Baki, S.A.; Saliba, W.; Ghandour, F.; Ashou, R.; Ghazal, G.; Bahous, J.; Chamseddine, N. Metastatic prostate adenocarcinoma presenting with pulmonary symptoms: a case report and review of the literature. Cases J. 2008, 1, 316–4. [Google Scholar] [CrossRef] [PubMed]
- Chao, D.H.; Higgins, J.P.; Brooks, J.D. Biochemical remission after resection of prostate cancer lung metastasis. Urology 2004, 63, 584–585. [Google Scholar] [CrossRef]
- Cui, Y.; Miao, C.; Xu, A.; Wang, Z.; Liu, B. Acinar with ductal and mucinous adenocarcinoma of prostate cancer complicated with lung metastasis: a case report and literature review. Ann. Palliat. Med. 2021, 10, 2366–2370. [Google Scholar] [CrossRef] [PubMed]
- Erdogan, E.; Aydin, M.; Buyukpinarbasili, N.; Ziyade, S.; Akman, T.; Turk, H. Incidental detection of prostate-specific antigen-negative metastatic prostate cancer initially presented with solitary pulmonary nodule on fluorodeoxyglucose positron emission tomography/computed tomography. Indian J. Nucl. Med. 2015, 30, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Fukuoka, T. Prostate cancer in a patient with multiple pulmonary metastasis alone and respiratory symptoms. J Rural Med. 2014;9(1):27-31.
- Gago, J.P.; Câmara, G.; Dionísio, J.; Opinião, A. Pulmonary metastasis as sole manifestation of relapse in previously treated localised prostate cancer: three exceptional case reports. ecancermedicalscience 2016, 10. [Google Scholar] [CrossRef]
- Khandani AH, Funkhouser WK, Feins R, Socinski MA. Simultaneous FDG PET+/Glut1+ lung and FDG PET-/Glut1- subcarinal lymph node metastasis from prostate cancer. Ann Nucl Med. 2009;23(6):595-597.
- Kirby, R. Case study: management of advanced prostate cancer with soft tissue metastasis. Prostate Cancer Prostatic Dis. 2005;8(3):290-292.
- Maebayashi, T.; Abe, K.; Aizawa, T.; Sakaguchi, M.; Ishibash, N.; Fukushima, S.; Honma, T.; Kusumi, Y.; Matsui, T.; Kawata, N. Solitary pulmonary metastasis from prostate cancer with neuroendocrine differentiation: a case report and review of relevant cases from the literature. World J. Surg. Oncol. 2015, 13, 1–7. [Google Scholar] [CrossRef]
- Mosca, A.; Mantica, G.; Giavarra, M.; Perrone, V.; De Marchi, L.; Gennari, A.; Toncini, C.; Terrone, C. Curative Lung Metastasectomy Without Concomitant Androgen Deprivation Therapy in Oligometastatic Castration-resistant Prostate Cancer: A Case Report and Review of the Literature. Clin. Genitourin. Cancer 2019, 18, e295–e299. [Google Scholar] [CrossRef] [PubMed]
- Petras, A.F.; Wollett, F.C. Metastatic prostatic pulmonary nodules with normal bone image. . 1983, 24, 1026–7. [Google Scholar] [PubMed]
- Polistina, G.; Matarese, A.; Cariello, P.; Caroppo, D.; Zamparelli, A. Cavitary lung metastasis as relapse of prostate cancer. Respir. Med. Case Rep. 2019, 29, 100973. [Google Scholar] [CrossRef] [PubMed]
- Tang, T.; Wang, L.-A.; Wang, P.; Tong, D.; Liu, G.; Zhang, J.; Dai, N.; Zhang, Y.; Yuan, G.; Geary, K.; et al. Case Report: Co-Existence of BRCA2 and PALB2 Germline Mutations in Familial Prostate Cancer With Solitary Lung Metastasis. Front. Oncol. 2020, 10, 564694. [Google Scholar] [CrossRef]
- Tsakiridis, T.; Bonert, M.; Zukotynski, K.; Anagnostopoulos, A. Radiographic and metabolic evolution of prostate cancer lung metastasis detected by prostate-specific membrane antigen and fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography. World J. Nucl. Med. 2020, 19, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Alumkal, J.J.; Chowdhury, S.; Loriot, Y.; Sternberg, C.N.; de Bono, J.S.; Tombal, B.; Carles, J.; Flaig, T.W.; Dorff, T.B.; Phung, D.; et al. Effect of Visceral Disease Site on Outcomes in Patients With Metastatic Castration-resistant Prostate Cancer Treated With Enzalutamide in the PREVAIL Trial. Clin. Genitourin. Cancer 2017, 15, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Lindell, M.M.; Doubleday, L.C.; Von Eschenbach, A.C.; Libshitz, H.I. Mediastinal Metastases from Prostatic Carcinoma. J. Urol. 1982, 128, 331–333. [Google Scholar] [CrossRef] [PubMed]
- Miseria, S.; Torresi, U.; Menichetti, E.T.; Tummarello, D.; Baldelli, S.; Murer, B.; Cenerino, R. Lymphangitic Carcinomas of the Lung as Presentation of Prostatic Cancer. A Case Report. Tumori J. 1991, 77, 86–89. [Google Scholar] [CrossRef]
- Miller, K.S.; Miller, J.M. Imaging case of the month. Pulmonary lymphangitic carcinomatosis from adenocarcinoma of the prostate.. 1994, 43, 989–90. [Google Scholar]
- Wu, J.W.; Chiles, C. Lymphangitic Carcinomatosis from Prostate Carcinoma. J. Comput. Assist. Tomogr. 1999, 23, 761–763. [Google Scholar] [CrossRef]
- A Cilento, M.; Hocking, C.M. Cystic and cavitating lung lesions as a presenting finding of metastatic prostate cancer. The Medical Journal of Australia 2021, 214, 459. [Google Scholar] [CrossRef] [PubMed]
- Lubin, D.J.; Holden, S.B.; Rettig, M.B.; Reiter, R.E.; King, C.R.; Lee, J.M.; Wallace, D.W.; Calais, J. Prostate Cancer Pulmonary Metastasis Presenting as a Ground-Glass Pulmonary Nodule on 68Ga-PSMA-11 PET/CT. Clin. Nucl. Med. 2019, 44, e353–e356. [Google Scholar] [CrossRef] [PubMed]
- Allen FJ, Van Velden DJ. Haemospermia and nodular lung metastasis without bone involvement: an unusual presentation of prostate carcinoma. Br J Urol. 1996;78(5):801-803.
- Eastham JA, Esensten ML, Wilson TG. Isolated pulmonary metastasis from prostatic adenocarcinoma. West J Med. 1993;159(4):489-490.
- Fabozzi SJ, Schellhammer PF, el-Mahdi AM. Pulmonary metastasis from prostate cancer. Cancer. 1995;75(11):2706-2709.
- Harris, S.; Cowley, N. Pulmonary metastases, an occult prostatic adenocarcinoma and delayed administration of antiandrogens. Clin. Oncol. 1996, 8, 118–119. [Google Scholar] [CrossRef] [PubMed]
- Panella, J.; Mintzer, R.A. Multiple Calcified Pulmonary Nodules in an Elderly Man. JAMA 1980, 244, 2559–2560. [Google Scholar] [CrossRef] [PubMed]
- Christie-Large M, James SL, Tiessen L, Davies AM, Grimer RJ. Imaging strategy for detecting lung metastasis at presentation in patients with soft tissue sarcomas. Eur J Cancer. 2008;44(13):1841-1845.
- Cardinale L, Ardissone F, Novello S, et al. The pulmonary nodule: clinical and radiological characteristics affecting a diagnosis of malignancy. Radiol Med. 2009;114(6):871-889.
- Henschke, CI. Early lung cancer action project: overall design and findings from baseline screening. Cancer. 2000;89(11 Suppl):2474-2482.
- Kobayashi, N.; Idiyatullin, D.; Corum, C.; Weber, J.; Garwood, M.; Sachdev, D. SWIFT MRI enhances detection of breast cancer metastasis to the lung. Magn. Reson. Med. 2014, 73, 1812–1819. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Wu, R.; Wang, W.; Zhao, Y.; Liu, X. 68Ga-PSMA PET/CT for the evaluation of metastasis in patients with prostate cancer: A systematic review and meta-analysis. 2022, 25, 297–311. 25.
- Damjanovic J, Janssen JC, Prasad V, et al. (68)Ga-PSMA-PET/CT for the evaluation of liver metastasis in patients with prostate cancer. Cancer Imaging. 2019;19(1):37.
- Pyka, T.; Weirich, G.; Einspieler, I.; Maurer, T.; Theisen, J.; Hatzichristodoulou, G.; Schwamborn, K.; Schwaiger, M.; Eiber, M. 68Ga-PSMA-HBED-CC PET for Differential Diagnosis of Suggestive Lung Lesions in Patients with Prostate Cancer. J. Nucl. Med. 2015, 57, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Ciriaco, P.; Briganti, A.; Bernabei, A.; Gandaglia, G.; Carretta, A.; Viola, C.; Montorsi, F.; Negri, G. Safety and Early Oncologic Outcomes of Lung Resection in Patients with Isolated Pulmonary Recurrent Prostate Cancer: A Single-center Experience. Eur. Urol. 2019, 75, 871–874. [Google Scholar] [CrossRef] [PubMed]
- Tarabaih, M.; A Degheili, J.; Nasser, M. Isolated Solitary Lung Nodule in a Patient With Idiopathic Pulmonary Fibrosis and Concomitant Prostate Cancer: A Challenging Diagnosis. Cureus 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Geraldo, L.; Ceci, F.; Uprimny, C.; Kendler, D.; Virgolini, I. Detection of Sarcomatoid Lung Metastasis With 68GA-PSMA PET/CT in a Patient With Prostate Cancer. Clin. Nucl. Med. 2016, 41, 421–422. [Google Scholar] [CrossRef]
- Goto, T.; Maeshima, A.; Oyamada, Y.; Kato, R. Solitary pulmonary metastasis from prostate sarcomatoid cancer. World J. Surg. Oncol. 2010, 8, 101–101. [Google Scholar] [CrossRef]
- Kaneko, Y.; Kosaka, T.; Nakamura, K.; Mikami, S.; Nishihara, H.; Oya, M. Squamous cell carcinoma of the prostate with SMARCA4 alteration in a Japanese patient. IJU Case Rep. 2022, 5, 323–326. [Google Scholar] [CrossRef] [PubMed]
- Treglia, G.; Lococo, F.; Petrone, G.; Inzani, F.; Perotti, G.; Porziella, V.; Granone, P.; Rindi, G.; Giordano, A.; Rufini, V. Pulmonary Neuroendocrine Tumor Incidentally Detected by 18F-CH PET/CT. Clin. Nucl. Med. 2013, 38, e196–e199. [Google Scholar] [CrossRef] [PubMed]
- Swanton, C.; Soria, J.-C.; Bardelli, A.; Biankin, A.; Caldas, C.; Chandarlapaty, S.; de Koning, L.; Dive, C.; Feunteun, J.; Leung, S.-Y.; et al. Consensus on precision medicine for metastatic cancers: a report from the MAP conference. Ann. Oncol. 2016, 27, 1443–1448. [Google Scholar] [CrossRef] [PubMed]
- Shenderov, E.; Velho, P.I.; Awan, A.H.; Wang, H.; Mirkheshti, N.; Lotan, T.L.; Carducci, M.A.; Pardoll, D.M.; Eisenberger, M.A.; Antonarakis, E.S. Genomic and clinical characterization of pulmonary-only metastatic prostate cancer: A unique molecular subtype. Prostate 2019, 79, 1572–1579. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Yu, L.; Wang, Z. PCA3 and TMPRSS2-ERG gene fusions as diagnostic biomarkers for prostate cancer. 28, 71. [CrossRef]
- Malone, E.R.; Oliva, M.; Sabatini, P.J.B.; Stockley, T.L.; Siu, L.L. Molecular profiling for precision cancer therapies. Genome Med. 2020, 12, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Sumiyoshi, T.; Chi, K.N.; Wyatt, A.W. Clinical implications of genomic alterations in metastatic prostate cancer. Prostate Cancer Prostatic Dis. 2021, 24, 310–322. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, N.M.; Van der Eecken, K.; Herberts, C.; Verbeke, S.; Ng, S.W.; Lumen, N.; Ritch, E.; Murtha, A.J.; Bernales, C.Q.; Schönlau, E.; et al. Genomic Features of Lung-Recurrent Hormone-Sensitive Prostate Cancer. JCO Precis. Oncol. 2022, 6, e2100543. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, T.; Hongo, H.; Aimono, E.; Matsumoto, K.; Hayashida, T.; Mikami, S.; Nishihara, H.; Oya, M. A first Japanese case of neuroendocrine prostate cancer accompanied by lung and brain metastasis with somatic and germline BRCA2 mutation. Pathol. Int. 2019, 69, 715–720. [Google Scholar] [CrossRef] [PubMed]
- Behrakis P, Koutsilieris M. Pulmonary metastasis in metastatic prostate cancer: host tissue-tumor cell interactions and response to hormone therapy. Anticancer Res. 1997;17(3A):1517-1518.
- Boyer, B.P.; Boyer, M.J. An elusive tumor in a man who has evidence of prostate cancer metastasis. J. Am. Acad. Physician Assist. 2009, 22, 22–5. [Google Scholar] [CrossRef] [PubMed]
- Hokamp, N.G.; Kobe, C.; Linzenich, E.; Maintz, D.; Drzezga, A. Solitary PSMA-Positive Pulmonary Metastasis in Biochemical Relapse of Prostate Cancer. Clin. Nucl. Med. 2017, 42, 406–407. [Google Scholar] [CrossRef]
- Kamiyama, Y.; Mitsuzuka, K.; Watanabe, M.; Kawamorita, N.; Yamada, S.; Kaiho, Y.; Ito, A.; Nakagawa, H.; Arai, Y. Chemotherapy with Gemcitabine and Cisplatin for Advanced Ductal Adenocarcinoma of the Prostate: Clinical Courses of Two Patients. Tohoku J. Exp. Med. 2015, 237, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Kume, H.; Takai, K.; Kameyama, S.; Kawabe, K. Multiple Pulmonary Metastasis of Prostatic Carcinoma with Little or No Bone or Lymph Node Metastasis. Urol. Int. 1999, 62, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Leibman, B.D.; Dillioglugil. ; Wheeler, T.M.; Scardino, P.T. Distant metastasis after radical prostatectomy in patients without an elevated serum prostate specific antigen level. Cancer 1995, 76, 2530–2534. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, A.M.; Gao, R.W.; Ahmed, M.E.; Orme, J.J.; Rincón, M.M.; Harmsen, W.S.; Johnson, G.B.; Cassivi, S.D.; Kwon, E.D.; Phillips, R.M.; et al. Metastasis-Directed Therapy for Metachronous Lung Metastases in Prostate Cancer. Ju Open Plus 2023, 1. [Google Scholar] [CrossRef]
- Mortier, D.; Baten, E.; Vandeurzen, K.; van Renterghem, K. The Benefit of a Surgical Resection of a Solitary Pulmonary Metastasis of Prostate Cancer after Radical Prostatectomy. Curr. Urol. 2017, 10, 210–212. [Google Scholar] [CrossRef] [PubMed]
- Pruthi, R.S.; Hubbard, J.S.; Kouba, E.; Wallen, E. Androgen-Independent Prostate Cancer Treated with Resection of the Solitary Metastatic Site. Urol. Int. 2007, 79, 371–373. [Google Scholar] [CrossRef] [PubMed]
- Reinstatler, L.; Dupuis, J.; Dillon, J.L.; Black, C.C.; Phillips, J.D.; Hyams, E.S. Lung malignancy in prostate cancer: A report of both metastatic and primary lung lesions. Urol. Case Rep. 2017, 16, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Rockey, K.E.; Graham, T.E. Prostate adenocarcinoma metastatic to the lung. Postgrad. Med. 1990, 87, 199–208. [Google Scholar] [CrossRef] [PubMed]
- Varkarakis MJ, Winterberger AR, Gaeta J, Moore RH, Murphy GP. Lung metastasis in prostatic carcinoma. Clinical significance. Urology. 1974;3(4):447-452.
- Vaz, S.C.; Silva. ; Oliveira, C.; Marques, R.; Galzerano, A.; Castillo-Martin, M. Impact of PSMA PET/CT in prostate cancer patient’s clinical management: a pictorial essay of interesting cases with histologic confirmation. Clin. Transl. Imaging 2020, 8, 207–226. [Google Scholar] [CrossRef]
- Wu LX, Lei L, Zhu YC, et al. A prostate cancer patient with isolated lung metastasis: a case report. Transl Cancer Res. 2020;9(3):2064-2068.
- Loriot, Y.; Fizazi, K.; de Bono, J.S.; Forer, D.; Hirmand, M.; Scher, H.I. Enzalutamide in castration-resistant prostate cancer patients with visceral disease in the liver and/or lung: Outcomes from the randomized controlled phase 3 AFFIRM trial. Cancer 2016, 123, 253–262. [Google Scholar] [CrossRef]
- I Scher, H.; Beer, T.M.; Higano, C.S.; Anand, A.; Taplin, M.-E.; Efstathiou, E.; Rathkopf, D.; Shelkey, J.; Yu, E.Y.; Alumkal, J.; et al. Antitumour activity of MDV3100 in castration-resistant prostate cancer: a phase 1–2 study. Lancet 2010, 375, 1437–1446. [Google Scholar] [CrossRef] [PubMed]
- Tran, C.; Ouk, S.; Clegg, N.J.; Chen, Y.; Watson, P.A.; Arora, V.; Wongvipat, J.; Smith-Jones, P.M.; Yoo, D.; Kwon, A.; et al. Development of a Second-Generation Antiandrogen for Treatment of Advanced Prostate Cancer. Science 2009, 324, 787–790. [Google Scholar] [CrossRef] [PubMed]
- de Bono, J.S.; Oudard, S.; Ozguroglu, M.; Hansen, S.; Machiels, J.-P.; Kocak, I.; Gravis, G.; Bodrogi, I.; Mackenzie, M.J.; Shen, L.; et al. Prednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a randomised open-label trial. Lancet 2010, 376, 1147–1154. [Google Scholar] [CrossRef]
- Sartor, O.; de Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G.; et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. New Engl. J. Med. 2021, 385, 1091–1103. [Google Scholar] [CrossRef] [PubMed]
- Gupta M, Karthikeyan G, Choudhury PS, Sharma A, Singh A, Rawal S. Is (177)Lu-PSMA an effective treatment modality for mCRPC patients with bone and visceral metastasis? Hell J Nucl Med. 2020;23(3):312-320.
- Heck MM, Tauber R, Schwaiger S, et al. Treatment Outcome, Toxicity, and Predictive Factors for Radioligand Therapy with (177)Lu-PSMA-I&T in Metastatic Castration-resistant Prostate Cancer. Eur Urol. 2019;75(6):920-926.
- Kessel K, Seifert R, Schafers M, et al. Second line chemotherapy and visceral metastasis are associated with poor survival in patients with mCRPC receiving (177)Lu-PSMA-617. Theranostics. 2019;9(17):4841-4848.
- Zhang J, Kulkarni HR, Singh A, Baum RP. Complete Regression of Lung Metastasis in a Patient With Metastatic Castration-Resistant Prostate Cancer Using 177Lu-PSMA Radioligand Therapy. Clin Nucl Med. 2020;45(1):e48-e50.
- Wallis CJ, English JC, Goldenberg SL. The role of resection of pulmonary metastasis from prostate cancer: a case report and literature review. Can Urol Assoc J. 2011;5(6):E104-108.
- Hofland CA, Bagg MD. An isolated pulmonary metastasis in prostate cancer. Mil Med. 2000;165(12):973-974.
- Franzese, C.; Zucali, P.A.; Di Brina, L.; D'Agostino, G.; Navarria, P.; Franceschini, D.; Santoro, A.; Scorsetti, M. The efficacy of Stereotactic body radiation therapy and the impact of systemic treatments in oligometastatic patients from prostate cancer. Cancer Med. 2018, 7, 4379–4386. [Google Scholar] [CrossRef]
- Berkovic P, De Meerleer G, Delrue L, et al. Salvage stereotactic body radiotherapy for patients with limited prostate cancer metastasis: deferring androgen deprivation therapy. Clin Genitourin Cancer. 2013;11(1):27-32.
- Ost, P.; Jereczek-Fossa, B.A.; Van As, N.; Zilli, T.; Muacevic, A.; Olivier, K.; Henderson, D.; Casamassima, F.; Orecchia, R.; Surgo, A.; et al. Progression-free Survival Following Stereotactic Body Radiotherapy for Oligometastatic Prostate Cancer Treatment-naive Recurrence: A Multi-institutional Analysis. Eur. Urol. 2016, 69, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Conteduca V, Caffo O, Fratino L, et al. Impact of visceral metastasis on outcome to abiraterone after docetaxel in castration-resistant prostate cancer patients. Future Oncol. 2015;11(21):2881-2891.
- Boschian, R.; Rizzo, M.; Zandonà, L.; Trombetta, C.; Liguori, G. Pulmonary recurrence from prostate cancer and biochemical remission after metastasis directed therapy. A case report. Arch. Ital. di Urol. e Androl. 2018, 90, 74–75. [Google Scholar] [CrossRef]
- Bromberg WD, Gaylis FD, Bauer KD, Schaeffer AJ. Isolated pulmonary metastasis from carcinoma of the prostate: a case report and deoxyribonucleic acid analysis using flow cytometry. J Urol. 1989;141(1):137-139.
- Cusan, L.; Gomez, J.; Dupont, A.; Diamond, P.; Lemay, M.; Labrie, F.; Moore, S. Metastatic prostate cancer pulmonary nodules: Beneficial effects of combination therapy and subsequent withdrawal of flutamide. Prostate 1994, 24, 257–261. [Google Scholar] [CrossRef]
- Izawa, M.; Kosaka, T.; Nakamura, K.; Oba, J.; Hishida, T.; Hongo, H.; Mikami, S.; Nishihara, H.; Oya, M. Pulmonary metastasis secondary to abiraterone-resistant prostate cancer with homozygous deletions of BRCA2: First Japanese case. IJU Case Rep. 2020, 4, 14–17. [Google Scholar] [CrossRef]
- Rush, J.; Pai, R.; Parikh, R.A. Complete biochemical response after pulmonary metastasectomy in prostate adenocarcinoma. Exp. Hematol. Oncol. 2017, 6, 25. [Google Scholar] [CrossRef]
- Smith, C.P.; Sharma, A.; Ayala, G.; Cagle, P.; Kadmon, D. SOLITARY PULMONARY METASTASIS FROM PROSTATE CANCER. J. Urol. 1999, 162, 2102–2102. [Google Scholar] [CrossRef]
- Kase AM, Copland JA 3rd, Zhai Q, Tan W. Complete response in Patients With Lung-Only Metastatic Prostate Cancer: Outcome Analysis. Clin Genitourin Cancer. 2022;20(6):e485-e489.
- Yoshitake, H.; Oura, S.; Yamaguchi, T.; Makimoto, S. Solitary Lung Metastasis of Prostate Cancer with a Long Disease-Free Interval and Normal Prostate-Specific Antigen Level. Case Rep. Oncol. 2021, 14, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Katsui, M.; Ohigashi, T.; Kosaka, T.; Bessho, H.; Arakawa, T. Remarkable response to abiraterone acetate in castration-resistant prostate cancer patient with aggressive liver metastasis. IJU Case Rep. 2018, 2, 12–14. [Google Scholar] [CrossRef]
- Seniaray N, Verma R, Belho E, Malik D, Mahajan H. Diffuse Pulmonary Metastasis From Prostate Cancer on 68Ga PSMA PET/CT. Clin Nucl Med. 2019;44(11):898-900.
- Polverari, G.; Ceci, F.; Allen-Auerbach, M.; Gupta, P.; Fishbein, M.C.; Reiter, R.E.; Lee, J.M.; Hope, T.A.; Carroll, R.M.; Czernin, J.; et al. Solitary Mucinous Prostate Adenocarcinoma Lung Metastasis Detected by 68Ga-PSMA-11 PET/CT. Clin. Genitourin. Cancer 2018, 17, e53–e55. [Google Scholar] [CrossRef] [PubMed]
- Su, H.-Y.; Chen, M.-L.; Hsieh, P.-J.; Hsieh, T.-S.; Chao, I.-M. Lung Metastasis From Prostate Cancer Revealed by 18F-FDG PET/CT Without Osseous Metastasis on Bone Scan. Clin. Nucl. Med. 2016, 41, 392–393. [Google Scholar] [CrossRef] [PubMed]
- Pepe, P.; Fraggetta, F.; Tornabene, F.; Nicolosi, M.; Aragona, F. Solitary lung metastasis after radical prostatectomy in presence of undetectable PSA. . 2012, 84, 208–10. [Google Scholar]
- Sakai T, Kimura D, Hatanaka R, et al. Kyobu Geka. 2010;63(4):340-343.
- Maeda, T.; Tateishi, U.; Komiyama, M.; Fujimoto, H.; Watanabe, S.-I.; Terauchi, T.; Moriyama, N.; Arai, Y.; Sugimura, K.; Kakizoe, T. Distant Metastasis of Prostate Cancer: Early Detection of Recurrent Tumor with Dual-Phase Carbon-11 Choline Positron Emission Tomography/Computed Tomography in Two Cases. Ultrasound Med. Biol. 2006, 36, 598–601. [Google Scholar] [CrossRef]

Table 1.
Patients’ characteristics from studies reported lung metastasis in prostate cancer.
| Articles | Year of publication | Type of study | Number of cases | Age /median | Pathology | Gleason score /median | PSA /median | Symptoms | Lines of treatment | Prognosis | Survival (months) | Methods of diagnosing | Number of met | Met’s location | Concomitant met |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mahmoud, et al. [64] | 2023 | Retrospective | 75 | 69 | Adeno | 7 | 4 | N/A | ADT, Surgical resection, Chemo | 72% Survived | N/A | Chest CT and PET/CT | Multiple | Bilateral | N/A |
| Ceylan, et al. [13] | 2023 | Case report | 2 | 57.11 | Adeno | N/A | N/A | Asymptomatic | Surgical resection | Died | 6 | Chest CT, PET/CT | N/A | N/A | N/A |
| Kase, et al. [97] | 2022 | Case series | 8 | N/A | Adeno | 7 | 3.1 | N/A | ADT, Surgical resection | Survived | 64 | Chest CT | Multiple | Bilateral | N/A |
| Delbare, et al. [14] | 2022 | Case report | 1 | 75 | Adeno | 7 | 6 | Asymptomatic | N/A | N/A | N/A | Chest CT, F18-PSMA-PET/CT | Multiple | Bilateral | L.N |
| Kaneko, et al. [53] | 2022 | Case report | 1 | 79 | SCC | N/A | 0.12 | Asymptomatic | Chemo | Died | N/A | Chest CT, SCC antigen | Multiple | Bilateral | Liver, L.N |
| Kosaka, et al. [15] | 2022 | Case report | 1 | 61 | Adeno | 7 | 0.76 | Asymptomatic | ADT, RT, Surgical resection | Survived | 84 | Chest CT, PET/CT | Multiple | Bilateral | None |
| Cui, et al. [18] | 2021 | Case report | 1 | 72 | Adeno | 8 | 12.64 | Frequent urination | ADT | Survived | 12 | Chest CT | Solitary | Right | None |
| Tarabaih, et al. [50] | 2021 | Case report | 1 | 70 | Adeno | 7 | 1.97 | Asymptomatic | Surgical resection | Survived | N/A | Chest CT | Solitary | Right base | None |
| Yoshitake, et al. [98] | 2021 | Case report | 1 | 83 | Adeno | 5 | N/A | Asymptomatic | Surgical resection | Survived | N/A | Chest CT | 2 | Bilateral | None |
| Carrilho Vaz, et al. [74] | 2020 | Case reports | 4 | 77, 76, 76, 75 |
Adeno | N/A, N/A, 7, N/A |
1.69, 7.55, 6.36, 2.6 |
N/A | ADT, ARPI, Chemo, Surgical resection | Survived | N/A, 4, 9, N/A |
Ga-PSMA PET/CT | 1- Multiple, 2-Solitary, 3- Multiple, 4-Solitary |
1- Bilateral, 2- Left upper, 3- Bilateral, 4- Right |
N/A |
| Izawa, et al. [94] | 2020 | Case report | 1 | 62 | Adeno | 9 | 4.25 | Asymptomatic | VATS, Chemo | Survived | 10 | Chest CT | Multiple | Bilateral | None |
| Tang, et al. [28] | 2020 | Case report | 1 | 48 | Adeno | 8 | 3.03 | Hematuria | ADT, Chemo | Survived | 19 | Chest CT, PET/CT | 2 | Right | None |
| Tsakiridis, et al. [29] | 2020 | Case report | 1 | 75 | Adeno | 7 | 5 | Shortness of breath | ADT, ARPI, SBRT | Survived | 48 | Chest CT, 18F-NaF-PET/CT, 18F-DCFPyL PET/CT | 2 | Left lower, Left hilar | None |
| Polistina, et al. [27] | 2020 | Case report | 1 | 74 | Adeno | 9 | N/A | weight loss | N/A | N/A | N/A | Chest CT, 18F PET/CT, FDG PET/CT | Multiple | Bilateral | N/A |
| Wu, et al. [75] | 2020 | Case report | 1 | 74 | Adeno | 8 | 2 | Asymptomatic | ADT | Survived | 36 | Chest CT | Solitary | Right | N/A |
| Ciriaco, et al. [49] | 2019 | Case series | 9 | 61 | Adeno | 8 | 1.66 | Asymptomatic | RT, Surgical resection | Survived | 24.5 | Ga-PSMA PET/CT | 4 Solitary, 5 multiple | Left, Right | None |
| Mosca, et al. [25] | 2019 | Case report | 1 | 63 | Adeno | 8 | 1.32 | Cough | ADT, Surgical resection | Survived | 32 | Chest CT, PET/CT | 2 | Left | None |
| Katsui, et al. [99] | 2019 | Case report | 1 | 62 | Adeno | 8 | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A | N/A |
| Seniaray, et al. [100] | 2019 | Case report | 1 | 63 | Adeno | 8 | 189.2 | Asymptomatic | N/A | N/A | N/A | Ga PSMA PET/CT | Multiple | Bilateral | L.N |
| Boschian, et al. [91] | 2018 | Case report | 1 | 69 | Adeno | 7 | 0.4 | Asymptomatic | Surgical resection | Survived | 36 | FDG-PET/CT | Solitary | Left | N/A |
| Damjanovic, et al. [12] | 2018 | Retrospective | 34 | 70.6 | Adeno | 9 | 123.6 | N/A | ADT, Chemo, RT | N/A | N/A | Ga-PSMA-PET/CT | Multiple | Bilateral | N/A |
| Polverari, et al. [101] | 2018 | Case report | 1 | 78 | Adeno | 7 | 0.3 | Asymptomatic | Surgical resection | N/A | N/A | 68Ga-PSMA-11 PET/CT, FDG PET/CT | Solitary | Upper Right | None |
| Reinstatler, et al. [71] | 2018 | Case report | 1 | 60 | Adeno | 8 | 44 | Asymptomatic | ADT, Surgical resection, Chemo | N/A | N/A | Chest CT | Multiple | Left | L.N |
| Hokamp, et al. [64] | 2017 | Case report | 1 | 63 | Adeno | N/A | 1.60 | Asymptomatic | ADT, Surgical resection | Survived | N/A | 68Ga PSMA PET/CT | Solitary | Right | L.N |
| Mortier, et al. [69] | 2017 | Case report | 1 | 82 | Adeno | 6 | 3.32 | Asymptomatic | ADT, Surgical resection | Survived | 12 | Chest CT, PET/CT | Solitary | Right | N/A |
| Rush, et al. [95] | 2017 | Case report | 1 | 70 | Adeno | 8 | 2.9 | Asymptomatic | Surgical resection | Survived | 24 | Chest CT, PET-CT | Solitary | Left | N/A |
| Gago, et al. [21] | 2016 | Case reports | 3 | 63, 62, 79 |
Adeno | 9, 7, 7 |
12.3, N/A, 2 |
Cough | ADT, Surgical resection, Chemo | Died, Survived, Survived | 24, 60, 5 |
Chest CT, PET/CT, Endobronchial US | Multiple | Right, Left, Bilateral |
None |
| Geraldo, et al. [51] | 2016 | Case report | 1 | 60 | Sarcomatoid | 8 | 4.63 | Asymptomatic | Surgical resection | Survived | 12 | Ga-PSMA PET/CT, F-FDG PET/CT | Solitary | Left | L.N |
| Hung-Yi Su, et al. [102] | 2016 | Case report | 1 | 54 | Adeno | 7 | 11.08 | Asymptomatic | Surgical resection | Survived | N/A | F-FDG PET/CT | 3 | Right, mediastinum | L.N |
| Erdogan, et al. [19] | 2015 | Case report | 1 | 71 | Adeno | 7 | 3.83 | Chest pain | Surgical resection | N/A | N/A | FDG PET/CT | Solitary | Right | Bone |
| Kamiyama, et al. [65] | 2015 | Case report | 2 | 59, 69 | Adeno | 8, 9 | 0, 5.6 | Asymptomatic | ADT, Chemo | Died | 6 | Chest CT | Multiple | N/A | L.N, Bone, Brain |
| Maebayashi, et al. [24] | 2015 | Case report | 1 | 50 | Adeno | 9 | N/A | Bloody sputum | Chemo, RT, Surgical resection | Died | 30 | Chest CT, PET/CT | Solitary | Left | systemic |
| Fukuoka, et al. [20] | 2014 | Case report | 1 | 87 | Adeno | 7 | 66.6 | Cough | ADT | Died | 18 | CXR, Chest-CT | Multiple | Bilateral | Liver |
| Treglia, et al. [54] | 2013 | Case report | 1 | 68 | Neuroendocrine | N/A | N/A | N/A | Surgical resection | N/A | N/A | PET/CT | N/A | N/A | N/A |
| Pepe, et al. [103] | 2012 | Case report | 1 | 75 | Adeno | 7 | 0 | Asymptomatic | Surgical resection | Survived | N/A | FDG PET/CT | N/A | N/A | N/A |
| Wallis, et al. [85] | 2011 | Case report | 1 | 53 | Adeno | 9 | N/A | Asymptomatic | Surgical resection | Survived | 12 | Chest CT, PET/CT | Multiple | Right | None |
| Sakai, et al. [104] | 2010 | Case report | 1 | 74 | Adeno | N/A | N/A | Surgical resection | N/A | N/A | N/A | N/A | N/A | N/A | |
| Goto, et al. [52] | 2010 | Case report | 1 | 73 | Sarcomatoid | 9 | N/A | Asymptomatic | ADT, Surgical resection | Survived | 10 | Chest CT, Bronchoscopy, PET scan | Solitary | Right | None |
| Khandani, et al. [22] | 2009 | Case report | 1 | 78 | Adeno | 8 | 8.5 | Chest pain and hemoptysis | Surgical resection | Survived | N/A | Chest CT, FDG PET/CT | Solitary | Left | Subcarinal L.N |
| Boyer, et al. [63] | 2009 | Case report | 1 | 65 | Adeno | 9 | 10.56 | Asymptomatic | ADT, Surgical resection | Survived | 11 | Chest CT | Solitary | Upper Left | N/A |
| Pruthi, et al. [70] | 2007 | Case report | 1 | 72 | Adeno | 6 | 1.9 | Asymptomatic | ADT, Surgical resection | Survived | 36 | Chest CT, PET CT, Bone scan | Solitary | Right | None |
| Maeda, et al. [105] | 2006 | Case report | 1 | 71 | Adeno | N/A | 4 | Asymptomatic | Surgical resection | Survived | N/A | Carbon-11 Choline PET-/CT | Solitary | Left upper | None |
| Kirby, et al. [23] | 2005 | Case report | 1 | 59 | Adeno | 9 | 23 | Dyspnea and hemoptysis | ADT | Survived | 7 | Chest CT | Multiple | Right | None |
| Chao, et al. [17] | 2004 | Case report | 1 | 68 | Adeno | 9 | 0.4 | Cough and dyspnea | ADT, Surgical resection | Survived | 144 | CXR | Solitary | Left lower | None |
| Hofland, et al. [86] | 2000 | Case report | 1 | 49 | Adeno | 9 | 1 | Asymptomatic | Surgical resection | Lost to follow-up | 10 | CXR, Chest CT | Solitary | Left lower | L.N |
| Kume, et al. [66] | 1999 | Case report | 2 | 56 | N/A | N/A | N/A | N/A | Bilateral orchiectomy, ADT | Survived | 88, 32 | CXR, Chest CT | Multiple | Bilateral | None, Bone |
| Smith, et al. [96] | 1999 | Case report | 1 | 70 | Adeno | 9 | 2.1 | Asymptomatic | Surgical resection | Survived | 12 | CXR, Chest CT | Solitary | Right lower | None |
| Behrakis, et al. [62] | 1997 | Case report | 1 | 71 | N/A | N/A | N/A | N/A | ADT | Survived | 8 | CXR | Multiple | N/A | N/A |
| Allen, et al. [37] | 1996 | Case report | 1 | 59 | Adeno | N/A | N/A | N/A | Bilateral orchiectomy | Survived | 3 | CXR | Multiple | Bilateral | None |
| Harris, et al. [40] | 1996 | Case report | 1 | 76 | Adeno | N/A | 42.6 | Asymptomatic | ADT | Survived | 60 | CXR | Multiple | Bilateral | None |
| Leibman, et al. [67] | 1995 | Case report | 1 | 78 | Adeno | 7 | 0.4 | Asymptomatic | ADT, Chemo | Died | 20 | CXR, Chest CT | 3 | 2 Right, 1 Left | Brain |
| Fabozzi, et al. [39] | 1995 | Retrospective | 47 | N/A | Adeno | 6,7,8,9 | N/A | N/A | ADT, Orchiectomy, Chemotherapy | N/A | HSPC: 25, CRPC: 13 | CXR | N/A | N/A | N/A |
| Cusan, et al. [93] | 1994 | Case report | 1 | 60 | Adeno | N/A | N/A | Asymptomatic | Flutamide, thoracotomy | Survived | 25 | CXR, Chest CT | Multiple | Bilateral | None |
| Eastham, et al. [38] | 1993 | Case report | 1 | 69 | Adeno | 7 | N/A | Asymptomatic | Bilateral orchiectomy | Survived | N/A | CXR | Multiple | Bilateral | None |
| Rockey, et al. [72] | 1990 | Case report | 1 | 83 | Adeno | N/A | N/A | N/A | ADT | N/A | N/A | Chest CT | Solitary | Left | None |
| Bromberg, et al. [92] | 1989 | Case report | 1 | N/A | N/A | 6 | N/A | N/A | Bilateral orchiectomy, Wedge resection | Survived | 13 | N/A | N/A | N/A | N/A |
| Petras, et al. [26] | 1983 | Case report | 1 | 59 | N/A | N/A | N/A | Cough | Bilateral orchiectomy | Survived | N/A | CXR, Bone scan | Multiple | Bilateral | Bone |
| Panella, et al. [41] | 1980 | Case report | 1 | 76 | Adeno | N/A | N/A | N/A | RT, bilateral orchiectomy, chemo | N/A | N/A | CXR, transthoracic needle biopsy | Multiple | Bilateral | N/A |
| Varkarakis, et al. [73] | 1974 | Retrospective | 26 | 64 | N/A | N/A | N/A | N/A | ADT, RT | Died | 14.9 | CXR | N/A | N/A | Bone |
| Abbreviations: PSA: Prostate Specific Antigen, Met: Metastasis, Adeno: Adenocarcinoma, N/A: Not Available, ADT: Androgen Deprivation Therapy, PET: Positron Emission Tomography, CT: Computed Tomography, SCC: Small Cell Carcinoma, L.N: Lymph Node, PSMA: Prostate-Specific Membrane Antigen, ARPI: Androgen Receptor Pathway Inhibitors, VATS: Video-Assisted Thoracic Surgery, SBRT: Stereotactic Body Radiation Therapy, RT: Radiotherapy, CXR: Chest X-ray, HSPC: Hormone Sensitive Prostate Cancer, CRPC: Castrate-Resistant Prostate Cancer. | |||||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



