
Submitted:
02 April 2024
Posted:
03 April 2024
You are already at the latest version
Abstract
Vaccination, particularly against pneumoccus and influenza, is a low-cost primary prevention, useful to avoid hard complications, particularly among frail older people. In this study, we aimed to assess the effect of a strategy for influenza and pneumococcal vaccination for outpatients, never practiced before, evaluating what could stimulate or demotivate vaccination among older people. This study was conducted during the 2023-2024 influenza season at the outpatient clinics of the Geriatrics section, University Hospital of Palermo (Italy). A total of 101 vaccinations were carried out. Half of the patients could be considered as pre-frail and about 20% frail, according to a comprehensive geriatric evaluation. Among participants, 46.3% received only vaccination against Pneumococcus and 26.8% only anti-influenza or the combination of anti-pneumococcus and anti-influenza. Compared with the previous seasons, a 19.5% increase of influenza and 90.2 % of pneumococcal vaccine uptake was observed. Side effects of vaccination were the main reason of the previous rejections, namely 74.8% for influenza and 29.5% for anti-pneumococcal vaccination. In conclusion, our study indicates how a new vaccination strategy in different settings is possible. Proposing influenza and pneumococcal vaccination for outpatients could be an effective instrument to improve immunization coverage that is still low among older people.
Keywords:
vaccination
; influenza
; pneumococcus
; older people
; outpatients
1. Introduction
The influenza epidemic is a relevant public health challenge affecting thousands of people every year. According to the Italian Ministry of Health, this lead to an important budget increase caused by the management of this pathology, its complications and the rise of control procedures [1]. The European Center for Disease Control showed how in Europe approximately 70,000 people died for reasons strictly connected with influenza every year [2]. Pneumonia associated with influenza virus infection is one of the greatest causes of death in Italy, particularly among frail and older people, immunocompromised and community dwellers, and it is described as one of the top ten causes of death in our country [3].
At the same time, the available microbiological, epidemiological, and modelled data indicate that there is a substantial burden of disease attributable to Streptococcus pneumoniae in adults ≥50 years of age [4]. These infections could cause community-acquired pneumonia and invasive pneumococcal disease such as sepsis and acute meningitis. In the frail population, usually affected by comorbidities, the risk of severe infections, which can be lethal, is particularly high [5].
Vaccination is certainly the best strategy to avoid influenza complications and there is agreement about its reccomendation for frail people [6,7]. The World Health Organization (WHO) guidelines state how a good control of influenza virus and transmission among the general population is a minimum of 75% vaccination coverage for influenza. Among frail people, coverage should be 95% in order to avoid probable negative consequences [1,8]. In Italy, there are extensive vaccination advices to the population and vaccination is administered at no cost. However, the vaccination rate is still low: recent estimates reported that, alson in older people, the vaccination rate is just above 50% [9]. A cross-sectional computer-assisted web interviewing survey of 10,001 Italian citizens, conducted in 2023, underscored the negative impact of a lack of awareness that a person is in a priority group for influenza vaccination and the profound influence of social circles on vaccination decisions [10]; in 2022 among older adults aged 65 years and older only a 58% of vaccination coverage was reached [11].
Low vaccine coverage among frail people or specific risk groups causes higher rates of disease and represents a relevant public health concern since these people are the largest part of those hospitalized and deceased. Vaccinations for adults and frail people are usually delivered through the primary health care system, which represents an important limitation. In fact, increasing evidence shows that vaccination based only on traditional primary care may not guarantee high vaccination adherence among frail people [12]. The main cause of this failure could be the lack of a right vaccine delivery system to provide vaccines properly to persons in need, or even an improper use of vaccines, vaccine ineffectiveness at the time of use, and factors related to patients’ attitudes and knowledge [13]. Another important reason could be trust issues between the population and the healthcare system, due to concerns about vaccine safety [14].The real power of vaccine catch-up instruments in rising vaccination coverage has been proven and several policies could be approved, such as phone calls with a vaccination remind, endorse immunization through informative interventions or attempts to vaccine risk groups in different settings from the primary care [15].
The Italian Ministry of Health, in addition to the usual national vaccination campaings, request each regional administration to improve health strategies for population vaccination coverage [1]. In particular, at the beginning of the 2022-2023 influenza season, the Health Authority of Sicily produced a decree asking all hospitals, community dwelling and health care facilities to vaccinate against influenza virus all patients who were part of at-risk caregroups before discharge [16].
Even if influenza and pneumococcal vaccination are usually at no cost in specifi risk groups, their coverage is strongly influenced by some socio-demographic, physical and cultural obstacles [17,18]. Several barriers are related to influenza vaccine diffidence, including vaccination skepticism, deficient information about negative outcomes of the infection, and low adherence to a healthy lifestyle [17,19,20].
Given this background, we aimed to assess the effect of a new plan for influenza and pneumococcal vaccination coverage dedicated to frail older outpatients and to evaluate what could stimulate or demotivate influenza or pneumococcal vaccine uptake among older outpatients attending our ambulatories for different reasons, such as the evaluation of cognitive profile. This represents a new strategy in the worldwide panorama of vaccination plans, attempting to reach as many persons as possible.
2. Materials and Methods
2.1. Patients and Procedures
A cross-sectional study was conducted from 01st December 2023 to 29th February 2024, at the Geriatrics section of the University Hospital “Policlinico P. Giaccone” of Palermo, Italy. Participants included those attending outpatient clinics, mainly dedicated to the management of cognitive disorders and endocrinological conditions, such as diabetes and osteoporosis. The 2023-24 influenza vaccination campaign was conducted in these settings, through the administration of illustrative brochures, posters and direct communications about risks and complications of influenza infection and recommendations of vaccination, with particular focus on frail people. A team of vaccinating physicians from the Geriatrics Section of the Department of Health Promotion, Mother and Child care, Internal Medicine and Medical Specialities of the University of Palermo, Italy, offered vaccination all the days in which the outpatinet clinics were open, from Monday to Friday. Collaboration with the medical and nursing staff of these clinics allowed to identify the possible eligible persons for vaccination.
The study was approved by the Ethical Committee Palermo 1 of the Institution at the meeting of December 12th, 2023 (protocol n. 07/2023 ).
2.2. Technical Characteristics of the Vaccinations Proposed
Sicily region for the season 2023-24 indicated that all the physicians belonging to public health care structures may directly vaccinate the patients (more information at: https://www.vaccinarsinsicilia.org/notizie/2023/09/campagna-vaccinazione-antinfluenzale-2023/2024-in-regione-sicilia#:~:text=Gli%20interessati%20a%20riservare%20un,prima%20per%20tutti%20gli%20altri). Vaccines were formulated according to Food and Drug Administration recommendations. Since High-Dose (HD) Influenza Vaccine is dedicated to frail older patients typical of our outpatient clinics, we only administered this kind of vaccination. IIV4-HD (Efluelda®️, Sanofi Pasteur) contained 60 μg of HA per strain. This vaccine is produced in embryonated chicken eggs, inactivated with formaldehyde, and split with a nonionic detergent.
Similarly, we used a 20-valent pneumococcal conjugate vaccine (PCV20; Prevnar 20®; Apexxnar®), developed by Pfizer for active immunization for the prevention of pneumococcal infections. PCV20 has a similar structure and formulation to 13-valent PCV with the addition of seven capsular polysaccharides to target seven further S. pneumoniae serotypes (8, 10A, 11A, 12F, 15B, 22F and 33F) associated with invasive pneumococcal disease with high mortality rates and antibiotic resistance. PCV20 has been approved for active immunization for the prevention of pneumonia and invasive disease caused by S. pneumoniae in adults since June 2021 in the USA and since February 2022 in the EU.
Both vaccines were provided in ready-to-use 0.5-ml syringes and administered intramuscularly, in the deltoid muscle site.
2.3. Questionnaires
A validated and structured questionnaire, already used in other experiences among inhospital patients, was administered to all eligible patient for vaccination [21]. The questionnaire was addressed to the patients with the aim of identify factors associated with influenza and pneumococcus vaccine uptake. According to previous literature, the following items were investigated: personal and socio-demographic data such as age, gender, education, health habits, and behaviour such as smoking, previous influenza vaccination, and physician recommendations [22,23]. We specifically investigated the characteristics of vaccinations such as if they were suggested or not by general practitioners (GP), if the patients were vaccinated against pneumococcus or influenza and the reasons of not being vaccinated in the past.
Moreover, we collected information about the presence of multidimensional frailty using the brief version of the selfy Multidimensional Prognostic Index (MPI) [24]. Briefly, this version of the MPI has similar multidimensional structure, i.e., collects information about disability, cognitive and health status, nutrition, polypharmacy, social aspects, and risk of pressure sores, giving a score between 0 and 1, higher scores reflecting a more multidimensional impairment [24]. A score less than 0.33 indicates robust patients, between 0.33 and 0.66 pre-frail, and over 0.66 frail [24].
2.4. Statistical Analysis
All collected data were analyzed using SPSS 26.0 statistical software. The normality of the distribution for the quantitative variables was assessed with the Skewness and Kurtosis test. Mean and standard deviation (SD) was chosen for normal distribution of these variables, while median and interquartile range (IQR) was used for non-normal distribution. The absolute and relative frequencies were calculated for the qualitative variables. For all analyses, a P-value of 0.05 was assumed to be statistically significant.
3. Results
Overall, participants comprised a total of 82 older outpatients, including caregivers, during the seasons 2023-24. Figure 1 shows the vaccinations carried out during the season 2023-24: a total of 101 vaccines were administrated, 46.3% received only vaccination against pneumococcus, 26.8% each one received only anti-influenza or the combination of anti-pneumococcus and anti-influenza.
Table 1 shows the most important descriptive characteristics of the population included. Overall, the 82 patients and caregivers aged a mean of 75.4 years (SD=7.9), with a range between 60 and 96 years. The majority of participants aged between 70 and 80 years (46.3%), followed by 80-90 years (24.4%); 4.9% aged more than 90 years. Participants were prevalently females (68.3%). The large majority of the patients accessed to the outpatient clinic for cognitive disorders (65.9%), followed by endocrinology outpatient clinic (diabetes and osteoporosis) (26.8%). Caregivers represented 7.3% of participants receiving the vaccination during season 2023-24. Half of the patients could be considered as pre-frail according to the BRIEF-SELFY-MPI, about 20% frail and only 29.3% robust. Over half of participants were married (57.3%), 35.4% widow, and 7.3% single. Regarding educational level, 45.1% had elementary school license and 8.5% did not ever attend school, and only 6.1% reached a degree (Table 1). Finally, 52.2% never smoked, 35.4% were former smokers, and 12.2% were actual smokers.
Table 2 shows the most important information about vaccinations received. Overall, 56.1% of the participants interviewed reported that they had influenza signs or symptoms during the five previous years to the vaccination received in 2023-24. The majority reported signs or symptoms typical of influenza for only one season, and 26.7% reported that this symptomatology was present for two seasons. When we asked for the role of GP in improving vaccination coverage, 9.8% of the interviewed participants reported that GPs did not indicate to get vaccination against influenza; similarly, 48.8% of the GPs did not suggest to vaccinate against pneumococcus.
Finally, we also asked about vaccinations received in the past 5 years. It is noteworthy that 19.5% of the patients did not get vaccination against influenza, as well as 90.2% against pneumococcus. When we investigated the main reason for not getting vaccinations, the patients referred in 18.9% of the cases that the vaccination against influenza was not indicated by their GP, 6.3% did not feel that the vaccination against influenza could be efficacious, and 74.8% were worried about side effects. Similarly, when we asked for the same information for pneumococcus, the patients answered in 29.5% of the cases that this vaccination was not indicated by their GPs and almost half of the participants (47.0%) were worried about possible side effects (Table 2).
4. Discussion
The first aim of this study was to assess the effect of a new plan for vaccination coverage in outpatient clinics dedicated to frail older accessing for other reasesons, e.g., the evaluation of cognitive status or bone health. Moreover, we evaluated what could stimulate or demotivate older people for influenza vaccine uptake in an age group commonly considered at higher risk and very vulnerable to infections. As far as we know, this is the first experience considering frail outpatients vaccination.
In our study we reached, for the first time, a very old population, since most participants aged between 70 and 80 years, followed by 80-90 years. Interestingly, caregivers represented 7.3% of people vaccinated in our outpatient settings, showing how it is possible to reach also people who would otherwise never have been vaccinated. Our study proposed a new concept of proactive vaccination: the ideal familiar setting for the older adult would be the GP. However, it is crucial to create a network as widespread as possible of outpatient vaccination clinics for older adults, in order to guarantee the proximity necessary for greater adhesion to the vaccination coverage. This strategy may be applied in territories where there is a shortage of GPs or where the Departments/Districts are not able to meet the needs of older population. Finally, regarding the period in which to vaccinate the older population, a key article strongly emphasises the need to overcome the old concept of seasonal vaccination with a more active intervention, such as that shown in our work [25]. Nowadays, vaccination throughout the year is essential, not concentrating the wide choice of available vaccines, such as anti pneumococcal, anti Herpes Zoster, and anti- Respiratory Syncytial Virus, among others, only in the winter season. The active invitation must always be done, based on a list by birth groups or risk factors. Lastly, as recommended in the Italian National Vaccine Prevention Plan 2023-2025, the active call cannot be successful if it is not supplemented by an operative communication campaign that must go through various networks, including all the figures that orbit around the older population.
Vaccines administration in a hospital setting, including ambulatories, leads to several benefits: chance to catching frail patients who, because of their clinical conditions, often go to the hospital; depth evaluation of the health condition of this older population; elimination of any physical obstacle connected to vaccination facilities; administration of vaccines in a safe setting [26]. The administration of vaccines in hospital settings is a plan encouraged by the WHO to decrease "wasted occasions" in older adult vaccination, increasing the distribution of health services and endorsing a real interaction among healthcare professionals [27,28].
To the best of our knowledge, our experience is one of the few made in an outpatient setting, used as an instrument to develop vaccination coverage in older populations. Previous experiences conducted in hospital settings include an American study where two sequential models were compared in a community hospital for assessing patients' vaccination status and eligibility [29], without improving the vaccination rates; another study among 248 Italian demonstrated that offering influenza vaccination to hospitalised patients could be an effective strategy to increase vaccination coverage [21], but vaccination was only for hospitalised patients, not effective enough to reach the entire susceptible population. There are few experiences of influenza vaccination among outpatinets, such as a South-American study of 465 participants with a median age of 37 years old [30] and without a real definition of frail patients according to geriatrics standards. In an American study of 7182 participants, vaccines were administered only in specific medical reasons such as in allergy, infectious disease, pulmonary, and rheumatology ambulatories, with good results in term of vaccination rates [31]. However, participants were part of different departments, with great difficulties in communicating and managing different professionals, while in our case, different specialists of the various outpatient clinics belonged to the same department. Our work significantly differ from these important experiences since it is remarkable that almost 70% of the vaccinated participants in our ambulatories could be considered as pre-frail or frail from a multidimensional point of view.
People with dementia are at a greater risk of complications from respiratory infections [32], therefore vaccinations against influenza and pneumococcal disease can benefit individuals with dementia by reducing both mortality and morbidity [33]. The large majority of the participants in our study accessed the outpatient clinic for cognitive disorders (65.9%). A recent systematic review and meta-analysis showed that influenza vaccination was associated with a significantly lower risk of dementia, suggesting the role of this vaccination in the prevention of dementia [34]. A previous French study of 4682 subjects showed how people with dementia had a slightly nonsignificant lower receipt of influenza vaccine in the year following dementia diagnosis than subjects without dementia [35], showing how it is difficult to reach this part of the older population, because their chronic condition often forces them home.
Another important finding of our work is that, with our experience, we increased by 20% the vaccination against influenza, as well as 90.2% against pneumococcus. The negative consequences of influenza infection in frail patients and those with chronic diseases are well reported in the literature, as are the benefits of vaccination, especially in older people with cardiovascular diseases, diabetes and chronic lung disease [36]. In our setting we administated an high-dose and adjuvanted inactivated influenza vaccination, specifically developed to provide enhanced immune responses in older adults [37], who generally have low responses mainly due to immunosenescence, comorbidities and frailty.
Regarding pneumococcus, growing evidence suggests that pneumococcal vaccine also reduce pneumonia and lower respiratory tract infections more broadly, including protecting against viral-associated respiratory diseases. We administered 20-valent pneumococcal conjugate vaccine, and even a Japanese study showed how in the COVID-19 era, replacing current PPSV23 with a single-dose of PCV20 immunisation programme for 65-year-old adults was highly cost-effective and more favourable in otucomes [38].
In our study 26.8% received the co-administration of anti-pneumococcal and anti influenza vaccination and this could have possible additive effects: a meta-analysis showed how this association was correlated with a significantly lower pneumonia rate than influenza vaccination alone, and with a significantly lower all-cause mortality rate than influenza vaccination alone [39], supporting the role of concomitant anti-pneumococcal and anti-influenza vaccination for older people.
Our study analyzed vaccination coverage in the past 5 years, and a sadly higher percentage of older patients did not get vaccination against influenza or against pneumococcus. The reasons for hesitancy in vaccination are usually complex and include socio-demographic, physical, and psychosocial factors. Gradually, psychosocial factors are being recognised as the first reason why people refuse vaccinations [40]. Usually a population without having experience of the influenza vaccine, has more worries and confusions about security and usefulness of vaccination [41].
Investigating the main reasons for not getting vaccinated about influenza and pneumococcus, more than 70 % reported that they were worried about side effects for the first one, and almost half of the patients for the second one. At the same time, another reason of the vaccination hesitancy is that health care professionals find many problems in communicating with older people about vaccines [42]. A Dutch study showed that the most important reasons for this communication gap were lack of time, due to clinical problems or high number of patients in ambulatorry setting, or clinical problems that were taking precedence over discussing [43]. On the other side, even the patients had sometimes a negative attitude and lack of understanding about the information provided, with a misinformation on vaccines, as well as anti-vax beliefs [42].
The present results were very encouraging for us and testify trust between outpatients and professional in our outpatient clinics, which is a crucial aspect in order to lead to reasonable goals. We observed that numerous patients listened to our reasons to get vaccinated, sometimes more than to the GP, with whom they may not have had a valid relationship, hihlighting the great impact of this new strategy of vacciantion. Our results reported that in 18.9% of the cases, the vaccination against influenza, and in 29.5% of the cases against pneumococcal, were not indicated by the GP. Vaccine hesitancy among GPs could explain these data: a French study of 1712 randomly selected GPs, showed that 16% to 43% of them, sometimes or never recommended at least one specific vaccine to their target patients [44]. This behavior may depend on their small trust in authorities, their perception of the utility and risks of vaccines, and their comfort in explaining the importance of vaccination, particularly in frail older people. At the same time, another French study of 693 GPs demonstrated how they had divergent immunisation attitudes toward their relatives and their patients, especially when considering the newest and most controversial vaccines, with HPV vaccine being the main focus of controversies [45].
The findings of our study must be interpreted within its limitations. The main limitation is the lack of a control group: therefore, no comparison was made between a group receiving vaccinations and a group not receiving it. However, our study is a pilot experience and we did not plan to have a control group. Additionally, information about vaccination and signs or symptoms typical of influenza were self-reported, which may not exlude the possibility of bias. Thirdly, the small population included may not be representative of all frail older people designed for vaccine coverage in the general population, even if our data suggest that the population targeted was frail from different points of view, including comorbidities, polypharmacy, and disability.
5. Conclusions
Our study demonstrated how a new vaccination strategy in the outpatient clinic setting is possible, especially for frail people. This is the first experience, to the best of our knowledge, of frail outpatients vaccination, representing a unique experience. Proposing influenza and pneumococcal vaccination for outpatients could be an effective instrument to improve immunization coverage. If our new concept of vaccination would be applied in a large scale in every hospital or health care facility, a significant improvement in influenza and pneumococcal vaccines rates for frail people could be reached.
Author Contributions
Conceptualization, N.V., M.B.; methodology, F.S.R., M.R.; formal analysis, N.V., P.M.; data curation, P.T., L.V., G.C., M.R.; writing—original draft preparation, N.V., P.M., G.D.B.; writing—review and editing, L.J.D., M.B., M.P., M.R.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by The study was approved by the Ethical Committee Palermo 1 at the meeting of December 04th, 2023..
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data will be available after to motivated request to corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ministry of Health, I.P.a.C.r.f.t.-s. https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2022&codLeg=87997&parte=1%20&serie=null.
- (ECDC), E.C.f.D.C. Flunewseurope, WHO/Europe weekly Influenza update, available online: https://flunewseurope.org/ (accessed on 30th May).
- Epicenter, H.I.o.H.-. Epidemiology for public health and integrated surveillance report of influenza, available online: https://www.epicentro.iss.it/influenza/flunews (accessed on 30th May).
- Organization, W.H. Considerations for pneumococcal vaccination in older adults. Weekly Epidemiological Record 2021, 23, 217-228.
- Scheen, A.; Louis, R.; Lancellotti, P.; Jouret, F.; Delwaide, J.; Moutschen, M. [Pneumococcal vaccination among at-risk groups with comorbidities : guidelines from the "Belgian Superior Health Council" and reimbursement criteria]. Rev Med Liege 2023, 78, 665-673.
- (WHO), W.H.O. In Global Influenza Programme,, available online: https://www.who.int/teams/global-influenza-programme/vaccines#:~:text=A%20flu%20vaccine%20offers%20the,spread%20of%20flu%20to%20others.&text=The%20constantly%20evolving%20nature%20of,frequent%20reformulation%20of%20influenza%20vaccines, : (accessed on 30th May).
- (CDC), C.o.D.C.a.P. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices — United States, 2022–23 Influenza Season,. In available online: https://www.cdc.gov/mmwr/volumes/71/rr/rr7101a1.htm?s_cid=rr7101a1 (accessed on 30th May).
- 2019), N.V.P.P.P.-. available online: https://www.salute.gov.it/imgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 30th May).
- Bianchi, F.P.; Stefanizzi, P.; Cuscianna, E.; Di Lorenzo, A.; Migliore, G.; Tafuri, S.; Germinario, C.A. Influenza vaccine coverage in 6months-64 years-old patients affected by chronic diseases: A retrospective cohort study in Italy. Human Vaccines & Immunotherapeutics 2023, 19, 2162301.
- Capodici, A.; Salussolia, A.; La Fauci, G.; Di Valerio, Z.; Montalti, M.; Odone, A.; Costantino, C.; Larson, H.J.; Leask, J.; Lenzi, J. Influenza Vaccine Uptake in Italy—The 2022–2023 Seasonal Influenza Vaccination Campaign in Italy: An Update from the OBVIOUS Project. Vaccines 2024, 12, 297.
- Ministry of Health, I.v.-A.v.c. available onlie: https://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=19 (accessed on 30th May).
- Nichol, K.L. Improving influenza vaccination rates for high-risk inpatients. Am J Med. 1991 Dec;91(6):584-8. [CrossRef]
- Hinman, A.R.; Orenstein, W.A.; Mortimer, E.A., Jr. When, where, and how do immunizations fail? Ann Epidemiol 1992, 2, 805-812, . [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Yahaghai, R.; Alimoradi, Z.; Broström, A.; Griffiths, M.D.; Pakpour, A.H. The mediational role of trust in the healthcare system in the association between generalized trust and willingness to get COVID-19 vaccination in Iran. Hum Vaccin Immunother 2022, 18, 1-8, . [CrossRef]
- Thomas RE, L.D. Interventions to increase influenza vaccination rates of those 60 years and older in the community. Cochrane Database Syst Rev. 2018 May 30;5(5):CD005188. [CrossRef]
- Region., H.D.o.t.S. Influenza vaccination campaign 2022/2023-involvement of GPs and PLS, available online: http://www.gurs.regione.sicilia.it/Gazzette/g22-44/g22-44.pdf (accessed on 30th May).
- Schmid, P., Rauber, D., Betsch, C., Lidolt, G., Denker, M.L.,. Barriers of Influenza Vaccination Intention and Behavior - A Systematic Review of Influenza Vaccine Hesitancy, 2005 - 2016. PLoS One. 2017 Jan 26;12(1):e0170550. [CrossRef]
- Veronese, N.; Zambon, N.; Noale, M.; Maggi, S. Poverty and Influenza/Pneumococcus Vaccinations in Older People: Data from The Survey of Health, Ageing and Retirement in Europe (SHARE) Study. Vaccines 2023, 11, 1422.
- Sammon, C.J., McGrogan, A., Snowball, J., de Vries, C.S. Factors associated with uptake of seasonal and pandemic influenza vaccine among clinical risk groups in the UK: an analysis using the General Practice Research Database. Vaccine. 2012 Mar 23;30(14):2483-9. [CrossRef]
- Malosh, R., Ohmit, S.E., Petrie, J.G., Thompson, M.G., Aiello, A.E., Monto, A.S.,. Factors associated with influenza vaccine receipt in community dwelling adults and their children. Vaccine. 2014 Apr 1;32(16):1841-7. [CrossRef]
- Fallucca, A.; Ferro, P.; Mazzeo, L.; Zagra, L.; Cocciola, E.; Oliveri, R.; Tuttolomondo, A.; Benfante, A.; Battaglia, S.; Scichilone, N. Impact of Actively Offering Influenza Vaccination to Frail People during Hospitalisation: A Pilot Study in Italy. Vaccines 2023, 11, 1829.
- Chen H, L.Q., Zhang M, Gu Z, Zhou X, Cao H, Wu F, Liang M, Zheng L, Xian J, Chen Q, Lin Q. Factors associated with influenza vaccination coverage and willingness in the elderly with chronic diseases in Shenzhen, China. Hum Vaccin Immunother. 2022 Nov 30;18(6):2133912. [CrossRef]
- Minardi V, G.R., Possenti V, Contoli B, Di Fonzo D, D'Andrea E, Masocco M. Influenza Vaccination Uptake and Prognostic Factors among Health Professionals in Italy: Results from the Nationwide Surveillance PASSI 2015-2018. Vaccines (Basel). 2023 Jul 10;11(7):1223. [CrossRef]
- Morganti, W.; Veronese, N.; Barbagelata, M.; Castagna, A.; Custodero, C.; Solimando, L.; Burgio, M.I.; Montana Lampo, S.E.; Seminerio, E.; Puleo, G. Validation of a Brief Form of the Self-Administered Multidimensional Prognostic Index: The SELFY-BRIEF-MPI Project. Journal of Clinical Medicine 2023, 12, 6026.
- Szilagyi, P.G.; Bordley, C.; Vann, J.C.; Chelminski, A.; Kraus, R.M.; Margolis, P.A.; Rodewald, L.E. Effect of patient reminder/recall interventions on immunization rates: a review. Jama 2000, 284, 1820-1827.
- McFadden, K., Seale, H.,. A review of hospital-based interventions to improve inpatient influenza vaccination uptake for high-risk adults, 2021 Jan 22;39(4):658-666. [CrossRef]
- Organization, W.H. Essential Immunization Program - Reducing Lost Opportunities to Immunize (MOV);. In available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization/implementation/reducing-missed-opportunities-for-vaccination-(mov) (accessed on 30th May).
- Measles Immunization Status of Health Care Workers: A Cross-Sectional Study Exploring Factors Associated with Lack of Immunization According to the Health Belief Model. Vaccines (Basel) 2023;11(3):618. [CrossRef]
- Bakare, M.; Shrivastava, R.; Jeevanantham, V.; Navaneethan, S.D. Impact of two different models on influenza and pneumococcal vaccination in hospitalized patients. Southern medical journal 2007, 100, 140-145.
- Macias, L.M.; Sabato, S.; Obed, M.; Nannini, E.; Crinejo, A.; Losso, M. Effectiveness of influenza vaccination in an ambulatory cohort of patients with flu-like symptoms. International Journal of Infectious Diseases 2018, 73, 359.
- Pennant, K.N.; Costa, J.J.; Fuhlbrigge, A.L.; Sax, P.E.; Szent-Gyorgyi, L.E.; Coblyn, J.; Desai, S.P. Improving Influenza and Pneumococcal Vaccination Rates in Ambulatory Specialty Practices. Open Forum Infectious Diseases 2015, 2, . [CrossRef]
- Manabe, T.; Fujikura, Y.; Mizukami, K.; Akatsu, H.; Kudo, K. Pneumonia-associated death in patients with dementia: A systematic review and meta-analysis. PLoS One 2019, 14, e0213825, . [CrossRef]
- Ridda, I.; Dastouri, F.; King, C.; Yin, J.K.; Tashani, M.; Rashid, H. Vaccination of Older Adults with Dementia Against Respiratory Infections. Infect Disord Drug Targets 2014, 14, 133-139, . [CrossRef]
- Veronese, N.; Demurtas, J.; Smith, L.; Michel, J.P.; Barbagallo, M.; Bolzetta, F.; Noale, M.; Maggi, S. Influenza vaccination reduces dementia risk: A systematic review and meta-analysis. Ageing Res Rev 2022, 73, 101534, . [CrossRef]
- Gallini, A.; Coley, N.; Andrieu, S.; Lapeyre-Mestre, M.; Gardette, V. Effect of dementia on receipt of influenza vaccine: a cohort study in French older adults using administrative data: 2007-2012. Fundam Clin Pharmacol 2017, 31, 471-480, . [CrossRef]
- Antonelli Incalzi, R.; Consoli, A.; Lopalco, P.; Maggi, S.; Sesti, G.; Veronese, N.; Volpe, M. Influenza vaccination for elderly, vulnerable and high-risk subjects: a narrative review and expert opinion. Intern Emerg Med 2023, 10.1007/s11739-023-03456-9, . [CrossRef]
- Lee, J.K.; Lam, G.K.; Yin, J.K.; Loiacono, M.M.; Samson, S.I. High-dose influenza vaccine in older adults by age and seasonal characteristics: Systematic review and meta-analysis update. Vaccine: X 2023, 100327.
- Hoshi, S.-l.; Shono, A.; Seposo, X.; Okubo, R.; Kondo, M. Cost-effectiveness analyses of 15-and 20-valent pneumococcal conjugate vaccines for Japanese elderly. Vaccine 2022, 40, 7057-7064.
- Zhang, Y.-Y.; Tang, X.-F.; Du, C.-H.; Wang, B.-B.; Bi, Z.-W.; Dong, B.-R. Comparison of dual influenza and pneumococcal polysaccharide vaccination with influenza vaccination alone for preventing pneumonia and reducing mortality among the elderly: A meta-analysis. Human Vaccines & Immunotherapeutics 2016, 12, 3056-3064.
- Capasso, M.; Bianchi, M.; Caso, D. Psychosocial Factors Influencing Parents’ Acceptance of COVID-19 Vaccination for Their Children: An Italian Cross-Sectional Study. Vaccines 2024, 12, 317.
- Rao, S., Fischman, V., Moss, A., Ziniel, S.I., Torok, M.R., McNeely, H., Hyman, D., Wilson, K.M., Dempsey, A.F.,. Exploring provider and parental perceptions to influenza vaccination in the inpatient setting. Influenza Other Respir Viruses. 2018 May;12(3):416-420. [CrossRef]
- Wennekes, M.; Eilers, R.; Caputo, A.; Gagneux-Brunon, A.; Gavioli, R.; Nicoli, F.; Quatrehomme, M.; Vokó, Z.; Timen, A. Vaccines for older adults; the low-hanging fruit of disease prevention. European Journal of Public Health 2022, 32, ckac131. 407.
- Vermeir, P.; Vandijck, D.; Degroote, S.; Peleman, R.; Verhaeghe, R.; Mortier, E.; Hallaert, G.; Van Daele, S.; Buylaert, W.; Vogelaers, D. Communication in healthcare: a narrative review of the literature and practical recommendations. International journal of clinical practice 2015, 69, 1257-1267.
- Verger, P.; Fressard, L.; Collange, F.; Gautier, A.; Jestin, C.; Launay, O.; Raude, J.; Pulcini, C.; Peretti-Watel, P. Vaccine hesitancy among general practitioners and its determinants during controversies: a national cross-sectional survey in France. EBioMedicine 2015, 2, 891-897.
- Killian, M.; Detoc, M.; Berthelot, P.; Charles, R.; Gagneux-Brunon, A.; Lucht, F.; Pulcini, C.; Barbois, S.; Botelho-Nevers, E. Vaccine hesitancy among general practitioners: evaluation and comparison of their immunisation practice for themselves, their patients and their children. European Journal of Clinical Microbiology & Infectious Diseases 2016, 35, 1837-1843.
Figure 1.
Prevalence of vaccinations done during season 2023-24.
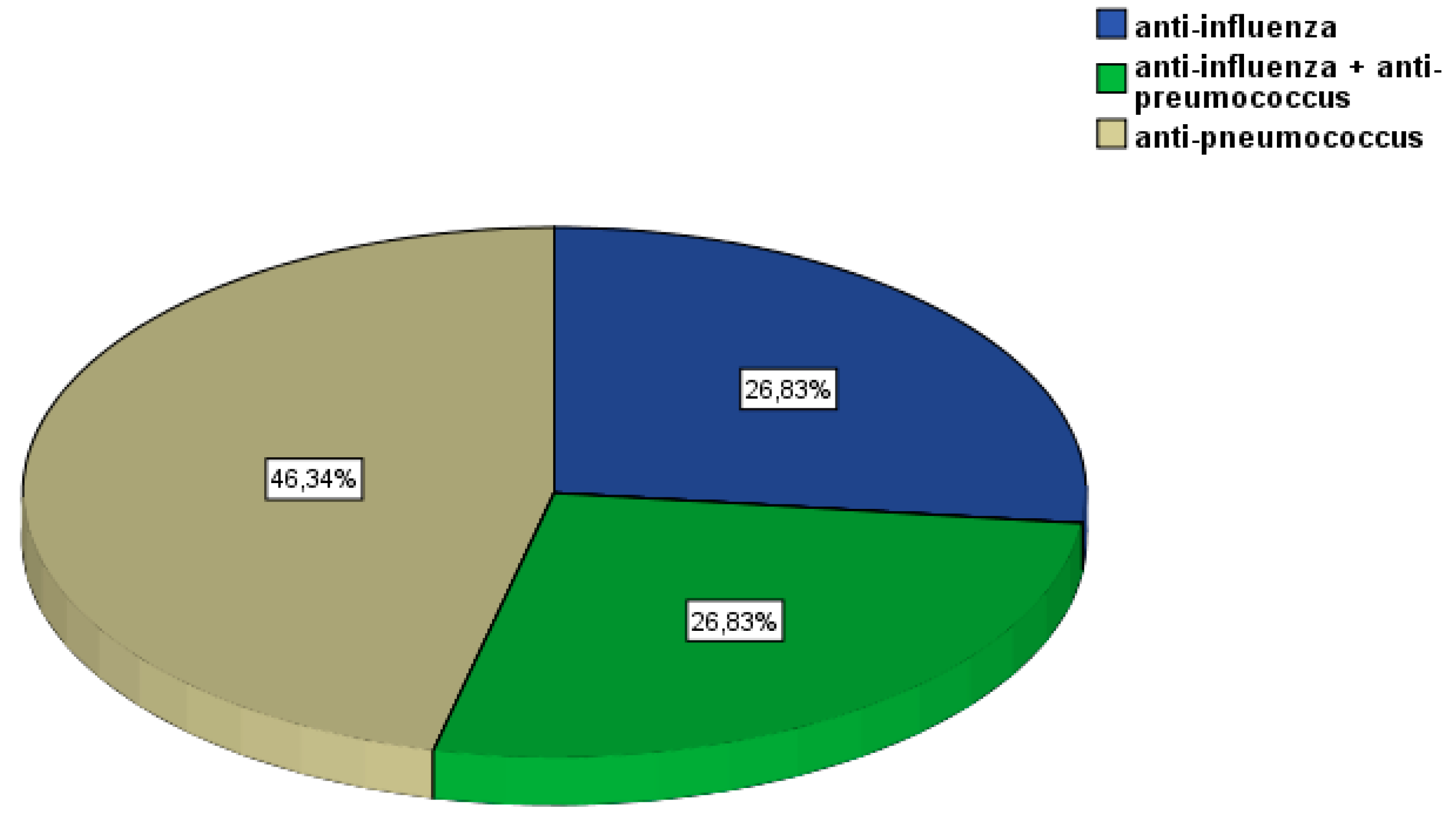

Table 1.
Descriptive characteristics of the older outpatients vaccinated for influenza and/or pneumococcus.
Table 1.
Descriptive characteristics of the older outpatients vaccinated for influenza and/or pneumococcus.
| Variable | Values | Mean values or frequency |
|---|---|---|
| Age | ||
| Mean age (SD) | 75.4 (7.9) (range: 60-96) | |
| 60-70 years | 24.4 | |
| 70-80 years | 46.3 | |
| 80-90 years | 24.4 | |
| >90 years | 4.9 | |
| Gender | ||
| F | 68.3 | |
| M | 31.7 | |
| Frailty status | ||
| Robust | 29.3 | |
| Pre-frailty | 50.0 | |
| Frailty | 19.5 | |
| Missing | 1.2 | |
| Ambulatory | ||
| Cognitive disorders | 65.9 | |
| Endocrinology | 26.8 | |
| Caregivers | 7.3 | |
| Civil status | ||
| Married | 57.3 | |
| Widow | 35.4 | |
| Single | 7.3 | |
| Educational level | ||
| Elementary | 45.1 | |
| Medium school | 26.8 | |
| High school | 12.2 | |
| Degree | 6.1 | |
| No scholarity | 8.5 | |
| Smoking status | ||
| Actual | 12.2 | |
| Former | 35.4 | |
| Never | 52.2 |
Table 2.
Characteristics about vaccinations for influenza and pneumococcus.
| Variable | Values | Influenza | Pneumococcus |
|---|---|---|---|
| Influenza last 5 years | |||
| Yes | 56.1 | - | |
| Number of seasons with influenza symptoms | - | ||
| 1 | 48.9 | ||
| 2 | 26.7 | ||
| 3 | 13.3 | ||
| 4 | 11.1 | ||
| Suggested by GP | |||
| Yes | 82.9 | 13.4 | |
| No | 9.8 | 48.8 | |
| Don’t know/remember | 7.3 | 37.8 | |
| Vaccination in the past | |||
| Yes | 78.0 | 7.3 | |
| No | 19.5 | 90.2 | |
| Don’t know/remember | 2.4 | 2.4 | |
| If no, what’s the reason | |||
| Not suggested by GP | 18.9 | 29.5 | |
| Felt not efficacious | 6.3 | 5.9 | |
| Fear of adverse events | 74.8 | 47.0 | |
| Other reasons | - | 17.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



