
Submitted:
02 April 2024
Posted:
03 April 2024
You are already at the latest version
Abstract
Keywords: Echocardiographic alterations; left ventricle; dog; Trypanosoma cruzi; flow patterns; dilated cardiomyopathy; Chagas disease
Keywords:
Echocardiographic alterations
; left ventricle
; dog
; Trypanosoma cruzi
; flow patterns
; dilated car-diomyopathy
; Chagas disease
1. Introduction
Chagas disease, also referred as American Trypanosomiasis (AT), is an illness caused by a flagellated protozoan that is transmitted by hematophagous vectors. The etiological agent, Trypanosoma cruzi, is distributed in a large part of the American continent, and it infects several species of wild and domestic mammals and humans [1]. AT is endemic in Latin America, and an increase in the incidences of T. cruzi infection in dogs and humans is noted in Mexico [2]. In Yucatan, Mexico, AT in dogs has been detected in rural and urban areas [3]. In the capital city of Yucatan, Merida, a prevalence of 12.2% has been reported in apparently healthy domiciled dogs [4].
Chronic Chagas disease is presented in humans with myocardial abnormalities ranging from mild forms, such as apical aneurysm and left ventricular (LV) diastolic dysfunction only, to significant cardiac chamber dilatation coupled with severe systolic dysfunction. Dilatation of the left and right ventricles is the most recognizable alteration of the heart in Chagas dogs and humans [1,2,5,6,7,8]. Dogs are important reservoirs of T. cruzi, and due to similar progression of the disease like in humans, canine AT can serve as a surrogate model for studying the course of human Chagas disease.
Electrocardiographic and echocardiographic studies have shown, in experimentally infected dogs, a decrease in the ejection fraction associated with thinning of the LV walls, mural thrombus, hypokinesis and thickening of the septum [9]. More recently, echocardiography examination of 7 animals that were experimentally infected with T. cruzi eight years earlier, identified an inversion of the E/A index indicating a delayed relaxation pattern or mild dysfunction and hypo-motility of the interventricular septum, but cardiomegaly signs were not found [10]. Detailed evaluation of the changes in cardiac structure and function in dogs naturally infected with T. cruzi isolates circulating in Mexico has not been done so far.
In this study, we aimed to characterize the echocardiographic alterations in dogs naturally infected with T. cruzi with an ultrasound equipment normally used in the routine veterinary practice. Our primary objective was to determine if dogs naturally exposed to T. cruzi isolates circulating in the State of Yucatan can develop dilated cardiomyopathy and to describe the cardiac findings before the clinically severe form of the heart disease appears in infected dogs. Our secondary objective was to obtain a comprehensive view of the range of myocardial parameters in dogs and determine if these variabilities are reflective of the human Chagas disease.
2. Materials and Methods
2.1. Study Area
The study was conducted with pet dogs referred by the Veterinary clinics in the area of Merida, Yucatan, Mexico (19°30'' and 21°35'' N; 87°30' 'and 90°24'' W). The climate of the area is tropical sub-humid, with a well-defined rainy season that goes from the months of May-June to October-November.
2.2. Selection of Animals
A cross-sectional study was carried out where 130 dogs with physical symptoms of cardiac involvement were randomly chosen. The inclusion criteria involved dogs that were seropositive for T. cruzi by an ELISA, later confirmed for T. cruzi exposure by Western blotting and/or PCR diagnostic approaches and had not received any treatment. All dogs were owned by people living in the area, of either sex (male or female), older than two years, and of variable size, weight and race. Dogs were considered with a cardiopathy when medical history and physical exam were compatible with heart disease [11]. Electrocardiographic abnormalities, not attributable to electrolyte imbalance, were also recorded [12]. In some cases, radiographic study or determination of blood pressure [13] were also conducted to confirm the cardiopathy. Healthy dogs (n=16) that were seronegative for anti-T. cruzi antibodies, PCR negative for T. cruzi DNA, and exhibited no cardiac pathology were used as controls.
2.3. Blood Samples
From each dog, two blood samples were obtained via cephalic or jugular vein. Half of each blood sample was collected in PAXgene Blood DNA Tube (BD-QIAGEN) to preserve the DNA until purification. A second aliquot of each blood sample was collected in BD Vacutainer and centrifuged at 400 rpm for 15 min at room temperature to obtain the serum.
2.4. Serology
The serological diagnosis of AT was made by the detection of immunoglobulins (IgG) against T. cruzi by using Chagatest ELISA recombinant v.3.0 kit (Wiener, Argentina). The assay was carried out following the manufacturer's recommendations, except that 2nd antibody was replaced with goat anti-dog IgG conjugated with HRP. The details of the protocol were previously described by us [14].
2.5. Western Blotting
Epimastigotes of H4 strain parasites were lysed with Laemmli sample buffer containing protease inhibitor cocktail (Sigma-Aldrich), and protein samples (20 μg) were resolved on 10% polyacrylamide gels and transferred to nitrocellulose membranes. A serum sample was considered positive when it recognized at least five antigenic bands [4,14].
2.6. PCR Detection of T. cruzi
Total DNA was extracted from whole blood samples according to [4]. Alternatively, DNeasy Blood and Tissue Kit (69504, QIAGEN) was used to isolate the genomic DNA from the blood samples by following the manufacturers’ instructions. Total DNA was examined for quality (OD260/OD280 ratio of 1.7–2.0) and quantity ([OD260 –OD320] x 50-μg/ml) by using a DU 800 UV/visible spectrophotometer. To detect the presence of T. cruzi DNA in blood, PCR assay was carried out according to the method used [3].
2.7. Echocardiographic Evaluation of Cardiac Structures and Function
Dogs were prepared, positioned, and scanned according to the conventional technique [15,16,17]. A Mindray M5 real-time ultrasound equipment (Mindray Electronics®, Shenzhen, China) using a sectorial cardiac transducer from 2 to 4 MHz was employed for echocardiography. The parameters of cardiac structure and function were obtained as following: In the right parasternal window, in the short axis of the LV at the level of the papillary muscles, the thickness of the interventricular septum and the free wall, and the diameter of the LV were measured with M-mode in systole and diastole [15,16,17]. To compare these parameters between dogs of variable size, weight, and race, the measurements of the structures were normalized according to the allometric scale formula for cardiac M-mode measurements of adult dogs [18]. Using the Teichholtz method, the software calculated the fractional shortening (FS), ejection fraction (EF), stroke volume (SV) and cardiac output (CO) that together provide an indication of LV systolic function. In the left apical position with a view of four chambers, the trans-mitral flow was measured with a pulse Doppler, placing the sample guide on the tip of the mitral valve [19]. The peaks of the E and A waves were marked, the E/A index (marker of LV diastolic function) was calculated, and the flow patterns were identified as normal, delayed relaxation, and restrictive, as described previously [20]. Where increased flow velocities were observed but with a normal pattern, it was suspected that they may be pseudonormal, because tissue Doppler was not available to confirm.
Dogs were considered positive for DCM according to the ultra-sonographic criteria proposed by the European Society of Veterinary Cardiology (major criteria: Dilatation of the LV in systole or diastole, ventricular spheroid structure, thinning of the septum and reduction of fractional shortening; minor criteria: Increased space between point E and septum, incongruent values of the fractional shortening and left or bilateral atrial dilatation [21]. Reference values were based on prediction interval of 95%, as proposed [18].
2.8. Statistical Analysis
The normal distribution of the variables of interest was confirmed by the Shapiro-Wilk test. Evaluated animals were first grouped according to the results of the serologic and molecular tests and the presence and absence of DCM as following: group A, serology negative, PCR positive, DCM negative; Group Aw, serology negative, PCR positive, DCM positive; group B, serology positive, PCR negative, DCM negative; group Bw, serology positive, PCR negative, DCM positive; group C, serology positive, PCR positive, DCM negative; and group Cw, serology positive, PCR positive, DCM positive. Control group included seronegative, PCR negative, DCM negative, healthy dogs (n=16).
Echocardiographic, age and body size data showing normal distribution were compared using ANOVA procedures. Non normally distributed data were tested with Kruskal-Wallis test with Bonferroni correction, and the frequencies of the alterations of each indicator of cardiac structure and function were determined. Binary data were analyzed by Chi2 test or exact Fisher test to establish the association between the transmitral flow patterns and the DCM positive vs. DCM negative disease status. All statistical analyses were run with Statgraphics v.19.0 software.
3. Results
3.1. Characteristics of T. cruzi Infection
All dogs enrolled in the study were in an age range of 6.94 to 9.83 years old, and of small to medium size (weight range: 8.41-13.06 kg). PCR detection of T. cruzi DNA is indicative of circulating parasites, and mostly noted in response to acute infection. Seropositivity for anti-T. cruzi antibodies is generally noted in all infected cases irrespective of the stages of disease development. Thus, a lack of anti-T. cruzi IgGs would indicate very early stage of acute infection before adaptive humoral immunity has been elicited by the host. Our data showed that most of the dogs enrolled in the study were positive for both diagnostic tests, i.e. anti-T. cruzi antibodies by ELISA and Western blotting and parasite DNA detection by PCR (group C: 97 out of 130 dogs, 75% of total). Some dogs were PCR positive only (group A: 26 out of 130, 20% of total) indicating the first, early phase of acute infection, and fewest dogs were in chronic phase (group B: 7 out of 130, 5% of total), indicated by their seropositive only status (Table 1).
3.2. Echocardiographic Findings
Dogs were analyzed by echocardiography to measure the changes in left ventricular (LV) structure and function and characterize the presence and absence of DCM. Figure 1 shows a representative image in B mode of the cardiac characteristics of DCM in a dog positive for anti-T. cruzi antibodies. Note the dilatation of the LV (ventricular sphericity) with thinning of the septum and it’s bowing towards the right ventricle. A greater diameter of the right atrium compared to the left is also noticeable.
3.3. M-Mode Ultrasonographic Findings
Representative M-mode ultrasonographic images and measurements of the LV structure from normal and infected dogs are shown in Figure 2. In comparison to non-infected, seronegative dogs (Figure 2A), infected dogs with DCM (Figure 2C) and advanced DCM (Figure 2D) exhibited highest values of LV diameter indicating the dilatation of the LV. Dogs that were infected but without DCM exhibited minor-to-no changes in LV diameter. Based on these structural features, we noted that 3, 1, and 12 dogs within groups A, B, and C, respectively, exhibited the features of DCM, while remaining 114 infected dogs were not presenting DCM (Table 1). Thus, overall, a total of 16 of the infected dogs (i.e. 12% of total) exhibited DCM.
Next, we performed a Kruskall-Wallis analysis to determine if the infection and seropositivity status were significantly correlated with any of the echocardiographic parameters of LV structure in dogs (Table 2A). On an average level, we did not observe major changes in the IVS thickness at diastole (IVS-d) and systole (IVS-s) between any of the infected groups and non-infected, healthy controls. Dogs exhibited an average IVS thickness of 0.4-0.5 at diastole and 0.64-0.70 at systole. The mean values of internal diameter of LV at diastole (LVID-d) and systole (LVID-s) were also not significantly changed in groups A, B, and C (without DCM) compared to the healthy controls. However, Aw (acute infection) and Cw (chronic and parasitemic dogs) groups with DCM exhibited 23-40% increase in LVID-d and 30-43% increase in LVID-s in comparison to the infected groups without DCM and healthy controls. The mean LV posterior wall thickness at diastole (LVPW-d) was decreased by 14.9-17% in Aw and Cw (vs. control) groups. Dogs in group B (chronic infection) exhibited 22-28% decline in LVPW-d and LVPW-s values (p<0.05). Together, these results suggest that increase in LVID and thinning of LVPW were major features of DCM in infected dogs, and the risk of LVPW thinning was increased with chronic infection (group B).
Echocardiographic parameters of global LV function were also measured in all enrolled dogs (Table 2B). These results showed that the mean values for LV systolic function, including stroke volume (SV), heart rate (HR) and cardiac output (CO) were increased by 39-80%, 11.2-21.4%, and 62-110%, respectively, in Aw and Cw groups compared to that noted in normal controls and infected groups (A, B, C) without DCM. Maximal increase in SV, HR, and CO values was noted in Cw group (chronic and parasitemic dogs). Despite increased SV, dogs in Cw group exhibited 15.9% decline in ejection fraction (EF). Fractional shortening (FS) was decreased by 15% in Cw group. These findings indicate an early stage of DCM in a majority of dogs in Aw and Cw groups, as was also noted in echocardiography imaging (Figure 2C).
3.4. Pulse Doppler Ultrasonographic Findings
Transmitral flow and calculation of the E/A index was carried out by ultrasonic recording with pulse Doppler. Representative images of the four chambers in left apical window view of a seronegative healthy dog and infected dogs are presented in Figure 3, and mean E/A values for each group are presented in Table 2. Most of the infected dogs without DCM exhibited normal transmitral flow pattern (Figure 3B). A pattern of delayed relaxation (E<A) was also observed in some of the infected dogs without DCM or in dogs with early signs of DCM (Figure 3C).
An increase in E and A values in T. cruzi positive dogs with DCM (Figure 3D), could correspond to pseudonormal, pattern of blood flow but tissue Doppler (TDI) is required to confirm. At a population level, 18.75% of the dogs with DCM (i.e. 3 out of 16) exhibited restrictive pattern, while normal were 62.5% and delayed relaxation flows were observed in 18.75% of the infected, DCM positive animals. Among the infected, DCM negative dogs, 75.44% had a normal pattern,4.39% exhibited delayed relaxation pattern, 5.26% recorded as suspicious of a pseudo normal pattern, and 14.91% exhibited the restrictive flow pattern. On an average, all infected dogs exhibited an increase in E/A ratio, the maximal increase being noted in group A (acutely infected), yet the average E/A values in infected dogs were within the normal range of 0.98-1.7, and no association of the flow patterns with infection and disease status was noted by Chi2 test (probability of association between type of flows and groups: 0.82). These results suggest that flow patterns are not directly correlated with infection and/or disease status.
We examined the frequency of alterations in the heart structure and function of the LV in infected dogs without DCM to determine if status of infection is associated with particular features of LV dysfunction (Table 3). In group A (acute infection), 26.09% (6 out of 23) of dogs exhibited an increase in E/A ratio and a reduction of the LVID in both stages of the cardiac cycle (each in 21.74% of dogs). In group B (chronic infection), 33.3% of the cases showed thinning of LVPW at systole. In group C, the most frequent alterations were in LVID-s and LVID-d, that were a decreased in 42.3% and 38.8% of dogs, respectively. These results suggest that changes in LVID-s, LVID-d, and a E/A ratio increased are important indicators of risk of DCM development in dogs that were acutely infected (group A) or repeatedly exposed to T. cruzi infection (group C) and were positive for T. cruzi by PCR. In comparison, thinning of the LV posterior wall was the most defining feature of risk of DCM development in chronically infected dogs (group B).
4. Discussion
The presence of circulating DNA in seropositive dogs (group C) may indicate a low but persistent parasitemia in chronic Chagas disease. This trend is similar to the observation in seropositive people from endemic areas that exhibit circulating T. cruzi detected by PCR [22,23]. Yucatan state, the site of this study, is a T. cruzi endemic zone with abundance of the vector Triatoma dimidiata [24] and vector borne transmission. Curtis-Robles et al. [25] have found 25% of dogs included in their study were PCR positive/seropositive. In the present study, a larger number of cases were positive to both tests (97 from 130 dogs), which cannot be justified just by the presence of low, occasional parasitemia. Thus, we surmise that repeat exposure to infection contributed to detection of circulating parasites in the seropositive dogs.
The published literature has not addressed the prevalence of DCM and heart failure in dogs. Our in-depth analysis of changes in LV structure and function in infected dogs in this study identified the prevalence of DCM in 12.3% of the infected dogs, and DCM features in dogs were consistent with the clinical characterization of chronic AT made by other authors [10,26]. A majority of dogs included in the study were without DCM or in the process of DCM development. These observations do not mean that DCM is uncommon in dogs with AT, but that it is a terminal feature of the disease [1,2,7,27]. It rather suggests that most animals have not presented this clinical condition and perhaps many die due to arrhythmias, blockages, endocarditis, valvular endocardiosis, congestive heart failure and other conditions that can be manifested before developing DCM [8,27]. In this study, it was also found that three dogs with DCM were negative to the serological tests, but positive to PCR, which indicates that acute T. cruzi infection can also result in the DCM and heart failure as is noted in 5% of the acutely infected human patients. Another possibility is that these dogs were exposed to T. cruzi infection after they have already developed DCM.
Ventricular dilatation is the main feature of DCM [21] and is referred to as one of the most well-known alterations of AT in dogs and humans [1,2,5,6,7,27]. As expected, groups of dogs with DCM showed the higher mean value of LVID-s and LVID-d, and these values were statistically different when compared to other groups (Table 2). In comparison, many of the PCR positive dogs in group A and group C exhibited a reduction of the LVID-s and LVD-d values (Table 3). This pattern is similar to that reported [28] in puppies during the acute stage of the disease.
Chetboul [21] has documented thinning of the IVS and/or LVPW in dogs with DCM. In this study, we either observed no significant changes in the IVS thickness in Chagas dogs (Table 2 and Table 3) or it was noted at a very low frequency in infected/seropostive dogs without DCM. Instead, infected dogs exhibited increased thickening of IVS, especially at systole (Table 3). Barr et al [9] have also documented a septal thickening during systole in Chagas dogs, which exceeded the maximum reference value of septal thickness. The reduction in LVPWs seen in group B is consistent with the decrease in size of the cardiac wall in dogs with AT as reported in other studies [9].
The frequency of reduction of LVID at systole and diastole, along with the observation of thickening of IVS and LVPW at systole, particularly in the PCR positive dogs (group A and group C) suggest progressive tendency of a decline in the ventricular diameter. This condition has been reported in patients with acute AT [9,10,26,28,29], but not in the chronic phase of Chagas disease in experimental models and human patients. This acute like ventricular diameter reduction and septum/wall thickening of seropositive/PCR positive animals, is possibly due to an increase in ventricular mass as reported in mice with myocarditis [30], which in turn is produced by the persistent parasitemia [23,31]. In chronic stages, fibrosis caused by the loss of myocardial cells and their replacement by collagen fibers [32,33,34], may be contributing to this reduction, before the DCM develops over time due to compensatory cardiovascular mechanisms [5,23]. It is also possible that there is a difference in the DTU of T. cruzi with respect to previous studies [9,10,26], since the DTU (TcI) circulating in this study area [35] is cardiotropic and highly virulent [36,37].
Although the Teichholtz method is not optimal for determining EF, SV, and CO, it allows obtaining values that can be obtained even with low-end ultrasound machines without specific software and by operators with little experience in echocardiography, which offers a great advantage when working in small veterinary clinics.
As in other studies [9,26], a systolic dysfunction (decreased FS and EF) was found in some of the infected animals without DCM (Table 3), though the average values for these parameters in infected dogs (groups A, B, C) were not significantly different from that observed in healthy controls (Table 2). This observation indicates that though identified as DCM negative with normal myocardial contractility, some of the infected dogs were progressing towards clinical development of DCM. The EF in animals with DCM was less efficient than in animals without DCM despite the observation that SV and CO were significantly greater due to the dilated ventricular space. Yet, there is a possibility that the increase in systolic function parameters seen in PCR positive groups, specialty in group C (Table 2), is the result of stress effect when the ultrasonographic procedure was accomplished without anesthesia, since it could increase the heart rate and the ventricular contractibility transiently [38]. Further, studies comparing LV function in sedated and non-sedated dogs will be needed to address this.
The mean diastolic function (E/A index) was found within the reference ranges [39] in all groups (Table 2), though E/A ration tended to be on higher side in all infected groups. The flow patterns do not seem to be associated with AT or its severity (with or without DCM) because in both groups there were similar number of cases with delayed relaxation, restrictive and normal patterns with no predominance of any. The pattern of delayed relaxation in dogs has already been reported by Pascon et al., [10] in dogs without DCM and positive to T. cruzi, but it has not been described in T. cruzi positive dogs with DCM, although this and the other patterns found are consistent with the pathophysiology of DCM [21].
It is particularly important to consider those indicators that were statistically different between DCM positive and negative groups (i.e. IVS-s, LVID-d, LVID-s, LVPW-d and EF), because they allow an approximation to the evaluation of these variables in dogs that are at risk of developing DCM. It should be noted that the alterations found here, when proceeding in an uncontrolled (open) population, may be associated not only with T. cruzi, since it is possible that there are other diseases or chronic-degenerative processes present in the patients studied.
5. Conclusions
The changes of the heart structure were more evident in infected dogs with DCM, but before the onset of it, there is a tendency to reduced left chamber when the wall thickening is present. Transmitral flow patterns do not seem to be associated with the severity of cardiac damage in cardiopathic dogs with AT. The results of the present study can also suggest that changes in LVID at systole and diastole is a major indicator of cardiac involvement in largest number of the infected dogs, and observation of changes in thickness of IVS and LVPW at systole or diastole, fractional shortening, and E/A ratio above and below the normal range will provide high predictive efficacy in determining the risk of DCM progression.
Author Contributions
EEAB and AOP conceived the study and analyzed the data; EEAB and CMAA carried out the echocardiography; MJC provided reagents for serology and PCR experiments; JCSC formal analysis and data curation; AOP and MJC wrote the manuscript; NJG provided intellectual input, conceptualization and edited the manuscript. All authors have read and approved the manuscript to be published.
Funding
This research received no external funding. NJG is supported by grants from National Institute of Allergy and Infectious Diseases (R01AI054578; R01AI136031) of the National Institutes of Health.
Institutional Review Board Statement
The study was conducted in accordance with the the bioethics committee (CB-CCBA-I-2017-003) at the Facultad de Medicina Veterinaria y Zootecnia, Universidad Autónoma de Yucatán.
Informed Consent Statement
An informed consent was obtained from dog owners before dogs were enrolled in the study.
Data Availability Statement
The data in the present study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Taylor, M.A.; Coop, R.L.; Wall, R.L. Veterinary Parasitology, 3rd ed.; Wiley-Blackwell: New Delhi, India, 2016; pp. 356–358. [Google Scholar]
- Weese, J.S.; Peregrine, A.S.; Anderson, M.E.C.; Fulford, M.B. Parasitic Diseases. In Companion Animal Zoonoses; Weese, J.S., Fulfords, M.B., Eds.; Wiley-Blackwell: Iowa, 2011; pp. 3–108. [Google Scholar]
- Jiménez-Coello, M.; Poot-Cob, M.; Ortega-Pacheco, A.; Guzma-Marin, E.; Ramos-Ligonio, A.; Sauri-Arceo, C.H.; Acosta-Viana, K.Y. American trypanosomiasis in dogs from an urban and rural area of Yucatan, Mexico. Vector Borne Zoonotic Dis. 2008, 8, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Coello, M.; Acosta-Viana, K.Y.; Guzmán-Marín, E.; Bárcenas-Irabién, A.; Ortega-Pacheco, A. American trypanosomiasis and associated risk factors in owned dogs from the major city of Yucatan, Mexico. J. Venom Anim. Toxins Incl. Trop. Dis. 2015, 21, 37. [Google Scholar] [CrossRef] [PubMed]
- Camacho, A.A. Miocardiopatía chagásica en caninos. In Afecciones Cardiovasculares en Pequeños Animales, Belerenian G.C.; Mucha, C.J., Camacho, A.A., Eds.; Inter-Médica: Buenos Aires, 2007; pp. 180–183. [Google Scholar]
- Guedes, P.M.M.; Veloso, V.M.; Alfonso, L.C.C.; Caliari, M.V.; Carneiro, C.M.; Diniz, L.F.; Marques-da-Silva, E.A.; Caldas, I.S.; do Valle Mata, M.A.; Souza, S.M.; Lana, M.; Chiari, E.; Galvao, L.M.C.; Bahia, M.T. Development of chronic cardiomyopathy in canine chagas disease correlates whith high IFN-gamma, TN-alpha, and low IL-10 production during the acute infection phase. Vet. Immunol. Immunopathol. 2009, 130, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Rassi, A. Jr.; Rassi, A.; Marin-Neto, J.A. Chagas disease. The Lancet 2010, 375, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Pereira-Nunes, M.C.; Dones, W.; Morillo, C.A.; Justiniano-Encina, J.; Ribeir, A.L. Chagas disease an overview of clinical and epidemiological aspects. J. Am. Coll. Cardiol. 2013, 62, 767–776. [Google Scholar]
- Barr, S.C.; Holmes, R.A.; Klei, T.R. Electrocardiographic and echocardiographic features of trypanosomiasis in dogs inoculated with North American Trypanosoma cruzi isolates. Am. J. Vet. Res. 1992, 53, 521–527. [Google Scholar] [CrossRef]
- Pascon, J.P.D.; Neto, G.B.P.; Sousa, M.G.; Sousa, M.G.; Paulino, D.; Camacho, A.A. Clinical characterization of chronic chagasic cardiomyopathy in dogs. Pesq. Vet. Bras. 2010, 30, 115–120. [Google Scholar] [CrossRef]
- Gompf, R.E. History and physical examination. In Manual of Canine and Feline Cardiology 5th ed.; Smith, F.W.K.; Tilley, L.P.; Oyama, M.; Sleeper, M.M. Eds.; Elsevier, St. Louis 2016. pp. 3–25.
- Tilley, L; Burtnick, N. ECG for the small animal practitioner. Teton New Media, Jackson Wyoming, 2009. pp. 64–84.
- Kittleson, M.D.; Kienle, R.D. Pulmonary arterial and systemic arterial hypertension. In: Small Animal Cardiovascular Medicine; Kittleson, M.D.; Kienle, R.D. Eds; Mosby, St. Louis, 1998. pp.1472-1845.
- Torres-Vargas, J.; Jimenez-Coello, M.; Guzman-Marin, E.; Acosta-Viana, K.Y.; Yadon, Z.E.; Gutierrez-Blanco, E.; Guillermo-Cordero, J.L.; Garg, N.J.; Ortega-Pacheco, A. Quantitative and histological assessment of maternal-fetal transmission of Trypanosoma cruzi in guinea pigs: An experimental model of congenital Chagas disease. PLOS Negl. Trop. Dis. 2018, 12, e0006222. [Google Scholar] [CrossRef] [PubMed]
- Boon, J.A. Veterinary Echocardiography, 2nd ed.; Wiley-Blackwell: USA, 2011; pp. 50–132. [Google Scholar]
- de Madron, E. Normal views: 2D, TM, spectral and color doppler, In: Clinical Echocardography of the Dog and Cat; de Madron, E., Chetboul, V., Bussadori, C., Eds.; Elsevier: St Luis, 2015. [Google Scholar]
- Boon, J.A. Two-dimensional and M-mode echocardiography for the small animal practitioner, 2nd ed.; Wiley-Blackwell: Iowa, 2016; pp. 75–83. [Google Scholar]
- Cornell, C.C.; Kittleson, M.D.; Della Torre, P.; Häggström, J.; Lombard, C.W.; Pedersen, H.D.; Vollmar, A.; Wey, A. Allometric scaling of M-mode cardiac measurements in normal adult dogs. J. Vet. Int. Med. 2004, 18, 311–321. [Google Scholar]
- Gallay-Lepoutre, J.; Bélanger, M.C.; Nadeau, M.E. Prospective evaluation of Doppler echocardiography, tissue Doppler imaging and biomarkers measurement for the detection of doxorubicin-induced cardiotoxicity in dogs: A pilot study. Res. Vet. Sci. 2016, 105, 153–159. [Google Scholar] [CrossRef]
- de Madron, E. Assessment of distolic function. In Clinical Echocardography of the Dog and Cat; de Madron, E., Chetboul, V., Bussadori, C., Eds.; Elsevier: St Louis, 2015; pp. 3–19. [Google Scholar]
- Chetboul, V. Dilated cardiomyopathy and other cardiomyopathies in dogs In Clinical Echocardiography of the Dog and Cat; de Madron, E., Chetboul, V., Bussadori, C., Eds.; Elsevier Masson: St Luis, 2016; pp 181–205.
- Salomone, O.A.; Juri, D.; Omelianiuk, M.O.; Sembaj, A.; Afiguerri, A.M.; Carriazo, C.; Barral, J.M.; Madoery, R. Prevalence of circulating Trypanosoma cruzi detected by polymerase chain reaction in patients with Chagas cardiomyopathy. Am. J. Cardiol. 2000, 85, 1274–1276. [Google Scholar] [CrossRef] [PubMed]
- Marin-Neto, J.A.; Cunha-Neto, E.; Maciel, B.C.; Simões, M.V. Pathogenesis of chronic Chagas heart disease. Circulation 2007, 115, 1109–1123. [Google Scholar] [CrossRef] [PubMed]
- Dumonteil, E.; Ramirez-Sierra, M.J.; Ferral, J.; Euan-Garcia, M.E.; Chavez-Nuñez, L. Usefulness of community participation for the fine temporal monitoring of house infestation by non-domiciliated triatomines. J. Parasitol. 2009, 95, 469–471. [Google Scholar] [CrossRef] [PubMed]
- Curtis-Robles, R.; Snowden, K.F.; Dominguez, B.; Dinges, L.; Rodgers, S.; Mays, G.; Hamer, S.A. Epidemiology and molecular typing of Trypanosoma cruzi in naturally-infected hound dogs and associated triatomine vectors in Texas, USA. PLOS Negl. Trop. Dis. 2017, 11, e0005298. [Google Scholar] [CrossRef]
- Meurs, K.M.; Anthony, M.A.; Slater, M.; Miller, M.W. Chronic Trypanosoma cruzi infection in dogs: 11 cases (1987-1996). J. Am. Vet. Med. Assoc. 1998, 213, 497–500. [Google Scholar] [CrossRef] [PubMed]
- Graiff, D.S. Relación entre perros seropositivos a Trypanosoma cruzi y alteraciones electrocardiográficas compatibles con miocardiopatía chagásica canina en la localidad de La Para (Córdoba-Argentina). MSc Thesis, Universidad Nacional del Litoral, Argentina. 2010.
- Vitt, J.P.; Saunders, A.B.; O'Brien, M.T.; Mansell, J.; Ajithdoss, D.K.; Hamer, S.A. Diagnostic features of acute Chagas myocarditis with sudden death in a family of boxer dogs. J. Vet. Intern. Med. 2016, 30, 1210–1215. [Google Scholar] [CrossRef] [PubMed]
- Rassi, A.; de Rezende, A.J.M. American trypanosomiasis (Chagas disease). Infect. Dis. Clin. North. Am. 2012, 26, 275–291. [Google Scholar] [CrossRef]
- Steinl, D.C.; Xu, L.; Khanicheh, E.; Ellertsdottir, E.; Ochoa-Espinosa, A.; Mitterhuber, M.; Glatz, K.; Kuster, G.M.; Kaufmann, B.A. Noninvasive contrast-enhanced ultrasound molecular imaging detects myocardial inflammatory response in autoimmune myocarditis. Circ. Cardiovasc. Imaging, 2016, 9, e004720. [Google Scholar]
- Gironès, N.; Fresno, M. Etiology of Chagas disease myocarditis: autoimmunity, parasite persistence, or both? Trends. Parasitol. 2003, 19, 19–22. [Google Scholar] [CrossRef]
- Guedes, P.M.M.; Veloso, V.M.; Caliari, M.V.; Carneiro, C.M.; Souza, S.M.; de Lana, M.; Chiari, E.; Bahia, M.T.; Galvao, L.M.C. Trypanosoma cruzi high infectivity in vitro is related to cardiac lesions during long-term infection in Beagle dogs. Mem. Inst. Oswaldo Cruz, 2007, 102, 141–147. [Google Scholar] [CrossRef]
- Garzoni, L.R.; Adesse, D.; Soares, M.J.; Rossi, M.I.D.; Borojevic, R.; de Meirelles, M.D.L. Fibrosis and hypertrophy induced by Trypanosoma cruzi in a three-dimensional cardiomyocyte-culture system. J. Infect. Dis. 2008, 197, 906–915. [Google Scholar] [CrossRef] [PubMed]
- Cunha-Neto, E.; Teixeira, P.C.; Nogueira, L.G.; Kalil. J. Autoimmunity. In Advances in Parasitology, Chagas Disease; Weiss, L.M., Tanowitz, H.B., Eds.; Elsevier Academic Press Inc.: San Diego, 2011; Volume 76, pp. 129–152.
- Jiménez-Coello, M.; Shelite, T.; Castellanos-Gonzalez, A.; Saldarriaga, O.; Rivero, R.; Ortega-Pacheco, A.; Acevedo-Arcique, C.; Amaya-Guardia, K.; Garg, N.; Melby, P.; Travi, B.L. Efficacy of recombinase polymerase amplification to diagnose Trypanosoma cruzi infection in dogs with cardiac alterations from an endemic area of Mexico. Vector Borne Zoonotic Dis. 2018, 18, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Miles, M.A.; Llewellyn, M.S.; Lewis, M.D.; Yeo, M.; Baleela, R.; Fitzpatrick, S.; Gaunt, M.W.; Mauricio, I.L. The molecular epidemiology and phylogeography of Trypanosoma cruzi and parallel research on Leishmania: looking back and to the future. Parasitology 2009, 136, 1509–1528. [Google Scholar] [CrossRef] [PubMed]
- Espinoza, B.; Rico, T.; Sosa, S.; Oaxaca, E.; Vizcaino-Castillo, A.; Caballero, M.L.; Martínez, I. Mexican Trypanosoma cruzi Tc I strains with different degrees of virulence induce diverse humoral and cellular immune responses in a murine experimental infection model. J. Biomed. Biotechnol. 2010, 890672. [Google Scholar] [CrossRef]
- Sisson, D.D. Patophysiology of heart failure. In Textbook of Veterinary Internal Medicine, 7th ed.; Ettinger, S.J., Feldman, E.C., Eds.; Saunders; Elsevier: St Luis, 2010; pp. 1143–1158. [Google Scholar]
- Schober, K.E.; Fuentes, V.L. Effects of age, body weight, and heart rate on transmitral and pulmonary venous flow in clinically normal dogs. Am. J. Ve.t Res. 2001, 62, 1447–54. [Google Scholar] [CrossRef]
Figure 1.
B-mode ultrasound image of the heart of a dog with dilated cardiomyopathy (DCM) and seropositive for anti-T. cruzi antibodies. Shown is a right parasternal window with long axis view of the four chambers. Dilatation of the left ventricle (spheroid shape) can be seen with thinning of the septum and its bowing to the right ventricle. A greater diameter of the right atrium with respect to the left atrium is also noticeable. Abbreviations: RA = Right atrium, LA = Left atrium, RV= Right ventricle, LV = Left ventricle, Ao = Aorta artery, IVS= Interventricular septum.
Figure 1.
B-mode ultrasound image of the heart of a dog with dilated cardiomyopathy (DCM) and seropositive for anti-T. cruzi antibodies. Shown is a right parasternal window with long axis view of the four chambers. Dilatation of the left ventricle (spheroid shape) can be seen with thinning of the septum and its bowing to the right ventricle. A greater diameter of the right atrium with respect to the left atrium is also noticeable. Abbreviations: RA = Right atrium, LA = Left atrium, RV= Right ventricle, LV = Left ventricle, Ao = Aorta artery, IVS= Interventricular septum.
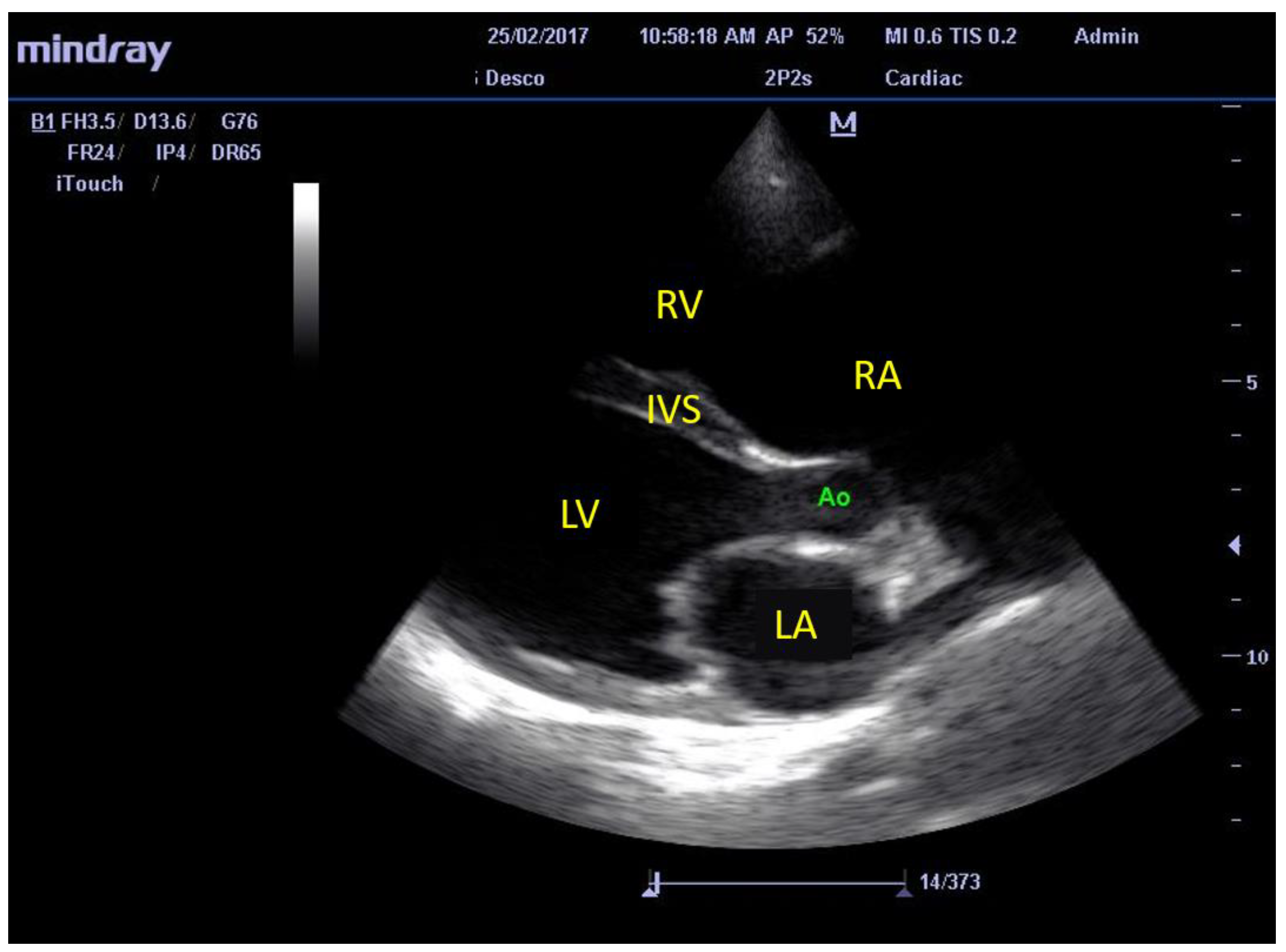
Figure 2.
Representative images of the M-mode ultrasonographic measurement of the structures of the left ventricle in right parasternal window, short axis, at the level of the papillary muscles in dogs. A. Healthy, non-infected, B. Seropositive for anti-T. cruzi antibodies and no DCM, C. Seropositive with incipient DCM, and D. Seropositive with advanced DCM. Abbreviations: IVS = intraventricular septum, LVID = left ventricle inner diameter, LVPW = left ventricle posterior wall, d = diastole, s = systole, FS = fractional shortening, EDV= end diastolic volume, ESV= end systolic volume, SV= stroke volume, EF= ejection fraction, SI= stroke index, CO= cardiac output, CI= cardiac index, HR= heart rate.
Figure 2.
Representative images of the M-mode ultrasonographic measurement of the structures of the left ventricle in right parasternal window, short axis, at the level of the papillary muscles in dogs. A. Healthy, non-infected, B. Seropositive for anti-T. cruzi antibodies and no DCM, C. Seropositive with incipient DCM, and D. Seropositive with advanced DCM. Abbreviations: IVS = intraventricular septum, LVID = left ventricle inner diameter, LVPW = left ventricle posterior wall, d = diastole, s = systole, FS = fractional shortening, EDV= end diastolic volume, ESV= end systolic volume, SV= stroke volume, EF= ejection fraction, SI= stroke index, CO= cardiac output, CI= cardiac index, HR= heart rate.
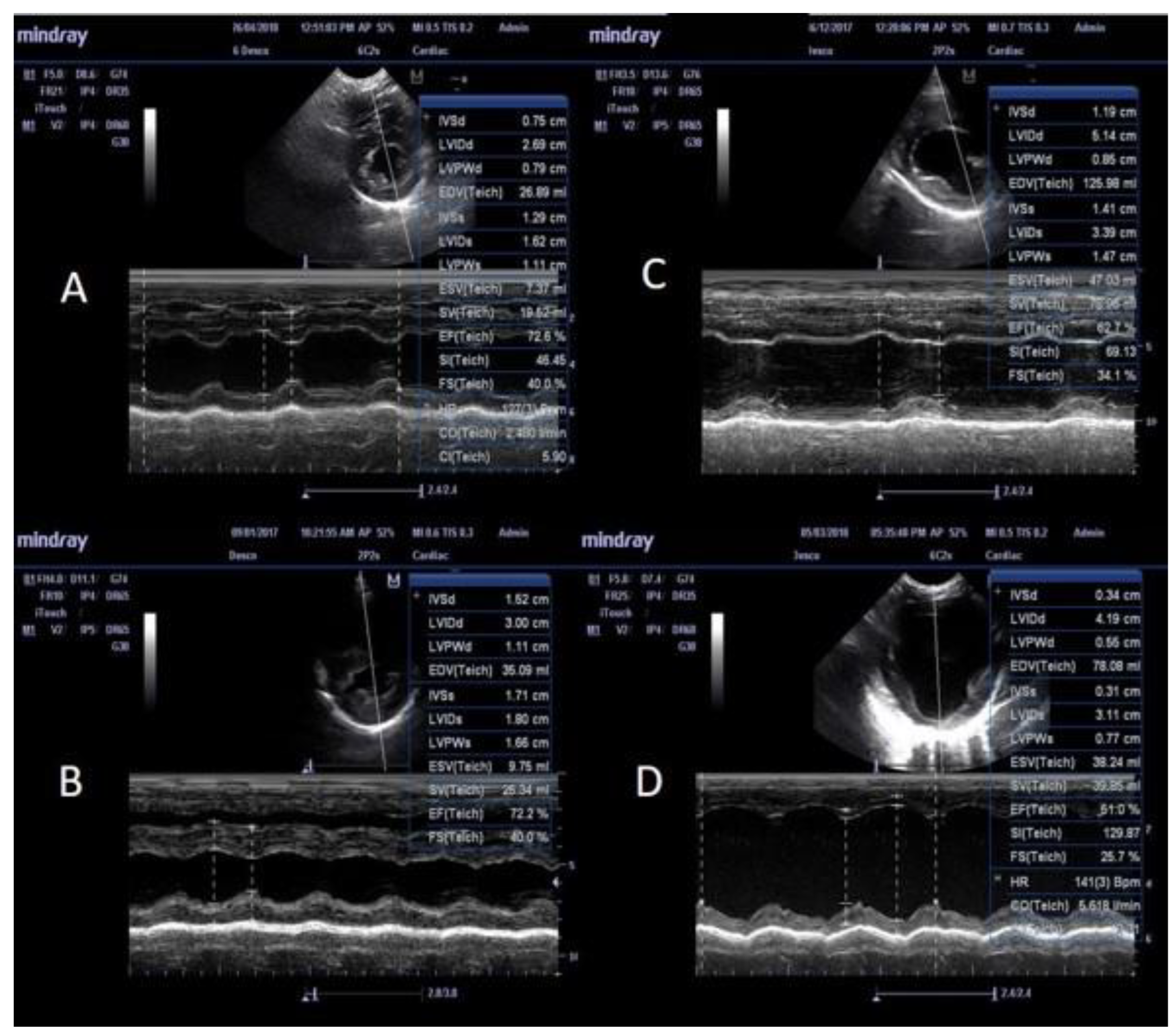
Figure 3.
Ultrasonic recording with pulse Doppler of the transmitral flow and calculation of the E/A index in dogs positive for T. cruzi exposure. Shown is the left apical window view of four chambers. A. Normal healthy, seronegative for anti-T. cruzi antibodies, B. Normal pattern in a seropositive dog without DCM, C. Pattern of delayed relaxation in a seropositive dog without DCM, D. Flow of a pseudo normal pattern in a T. cruzi positive dog with DCM. LA= left atrium, LV= left ventricle, RA= right atrium, RV= right ventricle, MV= mitral valve. MV E vel = velocity of peak E, MV A vel = velocity of peak A, MV E/A = index E/A.
Figure 3.
Ultrasonic recording with pulse Doppler of the transmitral flow and calculation of the E/A index in dogs positive for T. cruzi exposure. Shown is the left apical window view of four chambers. A. Normal healthy, seronegative for anti-T. cruzi antibodies, B. Normal pattern in a seropositive dog without DCM, C. Pattern of delayed relaxation in a seropositive dog without DCM, D. Flow of a pseudo normal pattern in a T. cruzi positive dog with DCM. LA= left atrium, LV= left ventricle, RA= right atrium, RV= right ventricle, MV= mitral valve. MV E vel = velocity of peak E, MV A vel = velocity of peak A, MV E/A = index E/A.
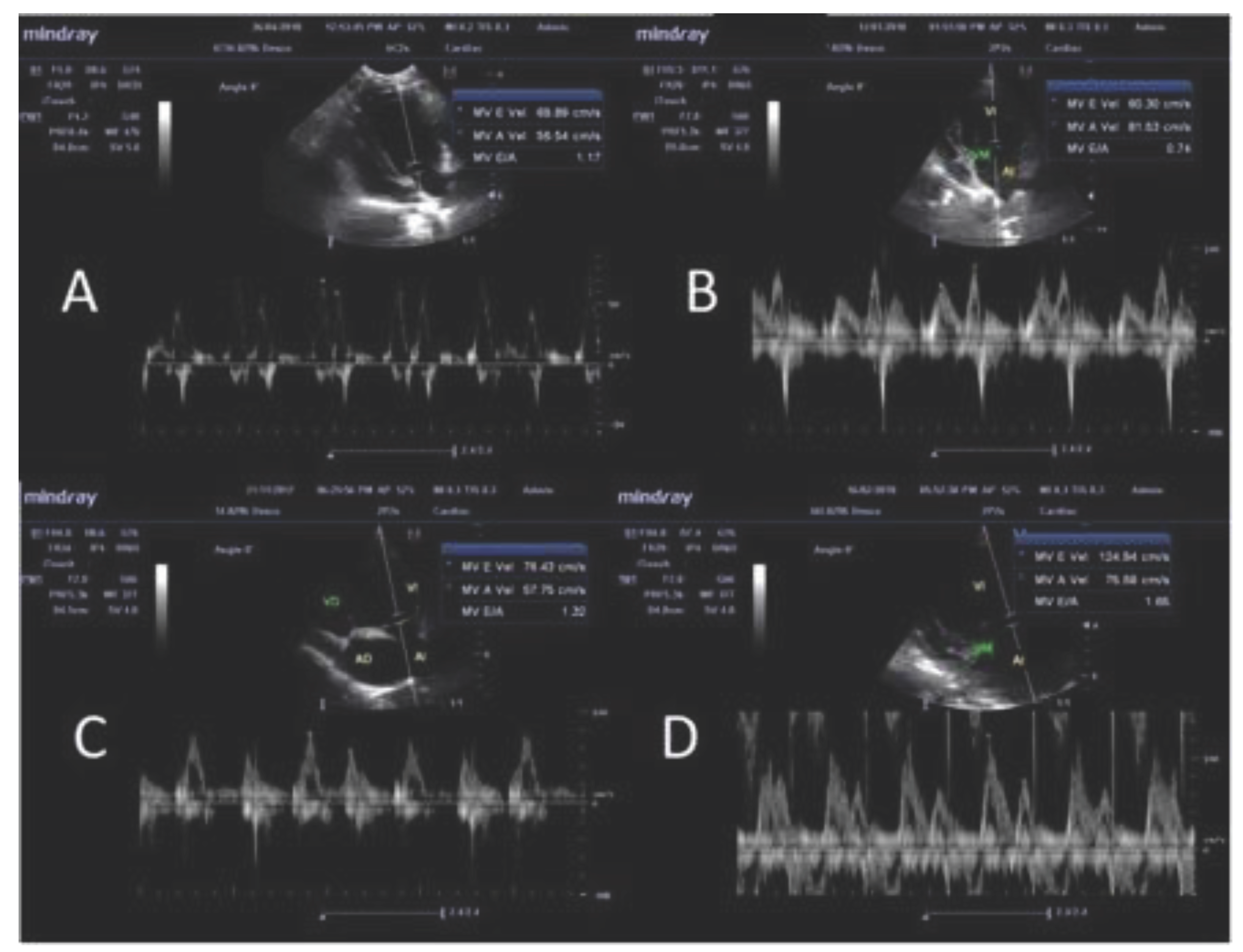

Table 1.
Categorization of 130 dogs based on serological and molecular tests for Trypanosoma cruzi infection and the presence of dilated cardiomyopathy.
Table 1.
Categorization of 130 dogs based on serological and molecular tests for Trypanosoma cruzi infection and the presence of dilated cardiomyopathy.
| Dilated cardiomyopathy | Group A Seronegative PCR positive |
Group B Seropositive PCR negative |
Group C Seropositive PCR positive |
Total |
| Absent | 23 | 6 | 86 | 115 |
| Present | 3 | - | 12 | 15 |
| Total | 26 | 6 | 98 | 130 |
Dogs were screened for anti-T. cruzi antibodies by two serological tests, including enzyme-linked immunosorbent assay (ELISA) and Western blotting; and for circulating parasites by T. cruzi-specific PCR, as described in Materials and Methods. Echocardiography was performed to measure the changes in cardiac structure and function, and animals in each group were further identified to be with or without dilated cardiomyopathy.
Table 2.
Echocardiographic, age and body size parameters in Trypanosoma cruzi positive dogs.
| Parameters | Mode | A (n= 23) | Aw (n= 3) | B (n= 6) | C (n= 86) | Cw (n= 12) | Controls (n=16) |
| A: Structural features | |||||||
| IVS diastole (IVS-d)* 1 | M mode | 0.5 ± 0.07 a | 0.51 ± 0.05 | 0.4 ± 0.08 | 0.49 ± 0.08 b | 0.4 ± 0.08 a, b | 0.44 ± 0.07 |
| IVS systole (IVS-s)* 1 | M mode | 0.69 ± 0.01 | 0.66 ± 0.05 | 0.67 ± 0.17 | 0.7 ± 0.15 | 0.64 ± 0.18 | 0.64 ± 0.09 |
| LVID diastole (LVID-d)* 2 | M mode | 1.44 ± 0.24 a, | 2.02 ± 0.16 a, b | 1.57 ± 0.20 b, c | 1.35 ± 0.25 b, c, d | 2.05 ± 0.15a ,c ,d, e | 1.55 ± 0.1 b, d, e |
| LVID systole (LVID-s)* 2 | M mode | 0.83 ± 0.18 a | 1.15 ± 0.10 a, b | 0.91 ± 0.13 c | 0.76 ± 0.2 b | 1.23 ± 0.19 a, c | 0.86 ± 0.1 b |
| LVPW diastole (LVPW-d)* 2 | M mode | 0.51 ± 0.09 a | 0.39 ± 0.16 a | 0.34 ± 0.03 a, b | 0.49 ± 0.1 b, c, d | 0.4 ± 0.09 a, c, d, e | 0.47 ± 0.06 b, d, e |
| LVPW systole (LVPW-s)*2 | M mode | 0.71 ± 0.09 a | 0.62 ± 0.18 | 0.53 ± 0.11 a, b | 0.73 ± 0.12 b | 0.69 ± 0.19 b | 0.68 ± 0.08 b |
| EPSS 1 | M mode | 0.39 ± 0.21a | 0.93 ± 0.13 b | 0.5 ± 0.2 | 0.31 ± 0.21 b, c | 0.96 ± 0.09 a, c, d | 0.27 ± 0.11 b, d |
| LA/Ao 1 | B mode | 1.39 ± 0.51 a | 1.69 ± 0.51 | 1.38 ± 0.17 | 1.25 ± 0.24 b | 1.86 ± 0.43 a, b, c | 1.19 ± 0.14 c |
| SI 1 | B & M mode | 1.99 ± 0.21 a | 1.54 ± 0.1 b | 1.87 ± 0.19 | 1.97 ± 0.24 b, c | 1.53 ± 0.08 a, c | 1.75 ± 0.07 a, c |
| B: Functional features | |||||||
| Fractional shortening (FS), %** 1 | M mode | 40.35 ± 6.66 | 40.33 ± 5.69 | 38.83 ± 5.03 | 41.39 ± 11.2 | 37 ± 10.72 | 41.75 ± 5.36 |
| Ejection fraction (EF), %** 1 | M mode | 72.61 ± 7.69 | 71.2 ± 7.30 | 68.33 ± 7.51 | 72.75 ± 12.58 | 64.17 ± 14.1 | 74.09 ± 6.68 |
| Stroke volume (SV), mL** 1 | M mode | 20.85 ± 14.37 a | 33.52 ± 14.77 | 27.49 ± 26.35 | 22.17 ± 15.5 b | 51.18 ± 28.4 a, b | 24.01 ± 10.97 |
| Heart rate 1 | M mode | 102.43 ± 17.98 | 121 ± 8.54 | 95.33 ± 8.71 | 102.5 ± 31.57 | 121.25 ± 41.29 | 108.75 ± 23.95 |
| Cardiac output (CO), L/min** 1 | M mode | 2.1 ± 1.31 a | 4 ± 1.53 | 2.63 ± 2.52 | 2.22 ± 1.55 b | 6.6 ± 5.13 a, b | 2.46 ± 0.81 |
| E/A ratio 1 | PW Doppler | 1.53 ± 0.34 a | 1.24 ± 0.24 | 1.35 ± 0.26 | 1.37 ± 0.34 | 1.41 ± 0.61 | 1.1 ± 0.29 a |
| Age, years 1 | ….. | 9.83 ± 3.46 a | 7.33 ± 3.78 | 7.33 ± 3.33 | 8.52 ± 4.01 | 9.83 ± 2.25 | 5.94 ± 3.23 a |
| Weight, kg 1 | ….. | 8.41 ± 6.31 | 9.53 ± 7.33 | 13.06 ± 11.86 | 12.77 ± 10.03 | 16.03 ± 18.61 | 9.56 ± 6.84 |
Mindray© M5 ultrasound system was used to perform transthoracic echocardiography in B and M modes and pulse wave Doppler echocardiography to assess the changes in left ventricular diastolic function. Group A: seronegative by ELISA and Western blotting and PCR positive indicative of acute infection; group Aw: seronegative and PCR positive with DCM; group B: seropositive and PCR negative indicative of chronic infection; group C: seropositive and PCR positive indicative of chronic stage and repeat infections; group Cw: seropositive and PCR positive with DCM. Controls included seronegative and PCR negative dogs with no indication of cardiac involvement. Data are presented as mean value ± standard deviation, determined by using Stat graphics software. Significance (p<0.05) is plotted with superscript letters, where equal letters indicate statistical difference; * Values calculated as defined in Cornell et al, 2004. ** Values calculated with Teichholz formula. 1 Compared by Kruskal-Wallis test with Bonferroni correction. 2. Compared by ANOVA and Fisher test; Abbreviations: IVS, interventricular septum; LVID, left ventricular (LV) internal diameter; LVPW, LV posterior wall; EPSS, E point septal separation; LA/Ao, left atrium/Aorta; SI, sphericity index; ELISA, enzyme-linked immunosorbent assay; PCR, polymerase chain reaction; DCM, dilated cardiomyopathy.
Table 3.
Frequency of alterations in dogs positive to Trypanosoma cruzi without dilated cardiomyopathy.
Table 3.
Frequency of alterations in dogs positive to Trypanosoma cruzi without dilated cardiomyopathy.
| Parameters | Mode | A (n=23) | B (n=6) | C (n=85) | Reference value | |||
| Increase (%) | Decrease (%) | Increase (%) | Decrease (%) | Increase (%) | Decrease (%) | |||
| IVS at diastole (IVS-d) | M mode | 4.35 | … | … | … | 8.24 | 1.18 | 0.29 - 0.59 1 |
| IVS at systole (IVS-s) | M mode | 13.04 | … | 16.67 | … | 22.35 | 2.35 | 0.43 - 0.79 1 |
| LVID at diastole (LVID-d) | M mode | … | 21.74 | … | 16.67 | … | 38.82 | 1.27 - 1.85 1 |
| LVID at systole (LVID-s) | M mode | … | 21.74 | … | … | … | 42.35 | 0.71 - 1.26 1 |
| LVPW at diastole (LVPW-d) | M mode | 13.04 | … | … | … | 10.59 | 1.18 | 0.29 - 0.60 1 |
| LVPW at systole (LVPW-s) | M mode | … | … | … | 33.33 | 9.41 | 1.18 | 0.48 - 0.87 1 |
| Fractional shortening (FS) | M mode | 8.70 | 13.04 | … | 16.67 | 22.35 | 20.00 | 33.6 - 49.9 2 |
| Ejection fraction (EF) | M mode | 8.70 | 4.35 | … | 16.67 | 22.35 | 12.94 | 58.9 - 82.9 3 |
| E/A ratio | PW Doppler | 26.09 | 8.70 | 16.67 | … | 11.76 | 3.53 | 0.98 - 1.7 4 |
Mindray© M5 ultrasound system was used to perform transthoracic echocardiography in B and M modes and pulse wave Doppler echocardiography to assess the left ventricular diastolic function. Please see Table 2 for units of measurement for each parameter; Group A: seronegative by ELISA and Western blotting and PCR positive indicative of acute infection; group B: seropositive and PCR negative indicative of chronic infection; group C: seropositive and PCR positive indicative of chronic and repeat infections; Group A: seronegative by ELISA and Western blotting and PCR positive indicative of acute infection; group B: seropositive and PCR negative indicative of chronic infection; group C: seropositive and PCR positive indicative of chronic and repeat infections.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



