
Submitted:
02 April 2024
Posted:
03 April 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The Sars-Cov-2 pandemic led to several needed containing measures that conditioned the onset of depressive, anxiety and post-traumatic stress symptoms in population. These symptoms, espe-cially if not diagnosed and treated, can also occur in patients undergoing surgery with high im-pact on people’s lives, like hysterectomy. To evaluate the post-surgical distress and anx-ious-depressive symptoms following hysterectomy for benign disease focusing on the impact of COVID-19 pandemic. The prospective observational cohort study included patients undergoing hysterectomy for benign disease. Psychologic evaluation through social-demographic question-naires was obtained before surgery (T1), postoperatively (T2), and 3 months after surgery (T3). The HADS (Hospital Anxiety and Depression Scale) was used to evaluate anxious-depressive symptoms and the PCL-5 (Post-traumatic Stress Disorder Checklist for DSM-5) compared the on-set of post-surgical distress and anxiety and depressive symptoms. The pre-COVID-19 pan-demic period was compared to the post-COVID-19 pandemic phase. Patients treated after COVID-19 pandemic showed higher depressive symptoms rate compared to those treated before (p-value=0.02); conversely, pre-COVID-19 patients were more prone to develop a PTSD (p-value=0.04). A significative association between the occurrence PTSD and anxiety-depressive symptoms registered at T2 a (p-value=0.007) and T3 (p-value
Keywords:
post-traumatic stress disorder
; post-surgical traumatic distress
; anxiety
; depression
; hysterecto-my
; COVID-19
1. Introduction
In the last decades the interest in the psychophysical integrity of surgical patients and in the understanding of the postoperative distress in the context of healthcare events has increased [1], and growing interest has been directed to specific cluster of symptoms, usually defined as post-traumatic stress disorder (PTSD), but determined by medical or surgical procedures. The incidence of this disturbance ranges from 12% to 25% among patients who have undergone various medical or surgical treatments [2]. This has been corroborated by a prior study involving patients who underwent surgical intervention for benign gynecological conditions [3]. This form of post-surgical PTSD differs from the conventional PTSD as defined by DSM-5, primarily due to differences in the source of threat, with external factors versus somatic origins, as well as distinctions in the cognitive aspects of threat related to the past, present, or future. Furthermore, there are variations in the avoidance behaviors displayed and the nature and consequences of hyperarousal, which are typically linked to post-surgical pain-induced PTSD. However, both disorders share a key similarity: the fear of death [3]. This specific disorder appears to be associated with unfavorable outcomes, manifested through poor adherence to therapies and follow-up appointments, as well as an elevated risk of complications. Moreover, the literature describes frequent associations between post-surgical PTSD and depressive and anxious symptoms. A previous work evaluated the incidence of post-surgical PTSD after hysterectomy due to benign gynecological disease, since hysterectomy represents the most common gynecological procedure in developed countries [2,3]. It is crucial to underscore that unaddressed and untreated manifestations of anxiety and depression after a hysterectomy for benign conditions can exert detrimental effects on morbidity management, adherence to treatment protocols, disease recovery, and overall quality of life. [4]. On the other hand, the treatment of PTSD can be really tough due to lack of effective pharmacotherapy [5], different from the psychopharmacotherapy for other psychiatric disorders [6]. The previous work showed a PTSD rate of 16.4% at the three months follow-up evaluation, with a significant correlation between post-operative depression (both postoperatively and three months after surgery) and PTSD symptoms, in line with literature. Since 2020, the SARS-CoV-2 (COVID-19) pandemic has had a detrimental impact on people’s mental health. This can be attributed to factors such as being separated from loved ones, loss of personal freedoms, uncertainty surrounding one’s health, and potentially experiencing boredom [8]. These circumstances have significantly influenced and exacerbated the psychological well-being of hospitalized patients. Notably, the most commonly reported psychological conditions during this period include negative emotions, anxiety, depressive symptoms, post-traumatic stress symptoms [9], irritability, panic attacks, phobic symptoms, insomnia, fits of anger, emotional exhaustion [8]. In the most severe cases, individuals may even exhibit suicidal behavior [10]. Assuming SARS COV 2 has worsened post-surgical PTSD and anxious and depressive symptoms, the present study aims to compare data of patients who underwent hysterectomy for benign gynecological disease in a pre-COVID-19 period (January-May 2019) and data collected during COVID-19 pandemic (April-September 2021) in terms of the onset of post-surgical distress and anxiety-depressive symptoms. The study aimed to evaluate post-surgical distress and anxiety and depressive symptoms in post-surgical period (T2) and three months later (T3), highlighting the impact of COVID-19 pandemic on post-surgical traumatic distress and anxiety and depressive symptoms in gynecological patients through a comparison between a group of patients undergone to surgical intervention in the pre-COVID-19 period [2] and a sample of patients of the pandemic period.
2. Materials and Methods
This is a prospective observational cohort study that involved a comparison of two distinct populations. The first group consisted of 100 subjects who were recruited before the onset of the COVID-19 pandemic, while the second group included 39 subjects who were recruited after the pandemic began (Figure 1). All participants in both groups had a medical indication for hysterectomy due to benign disease and were referred to the Obstetrics and Gynecologic department of the Women’s and Children’s hospital of Varese (Filippo Del Ponte Hospital), where the operations were performed. Prior to their participation, all individuals were duly informed about the study’s objectives and procedures, and they provided written consent for the use and analysis of their data.
Inclusion criteria were: female; age ≥ 18 years old; written consent signed for the use of anonymous data; operated by total hysterectomy for benign disease (fibromatosis; abnormal uterus bleeding; endometriosis/adenomyosis; pelvic/abdominal pain; genital prolapse; uterus (endometrial hyperplasia) and cervical intraepithelial cervical cancer, precancerous lesions).
Exclusion criteria were: no written consent; no Italian language understanding; association of hysterectomy with other non-gynecological interventions; gynecological malignancy or secondary metastasis; patients affected by neuropathic/chronic pain taking anti-inflammatory drugs; enlistment in other studies with pharmacological intake; current diagnosis of major psychiatric disorder (shown in Figure 1).
Patients have been evaluated in 3 different times, first through a social-demographic questionnaire (age, marital status, employment, instruction, pharmacological therapy and parity). To streamline the statistical analysis, we combined “employee” and “retired” into the category “occupied,” while grouping the remaining two categories as “unemployed.” We focused solely on whether psychopharmacological therapy was utilized or not.
The HADS (Hospital Anxiety and Depression Scale) was used to evaluate anxious and depressive symptoms [7] and the PCL-5 (Post-traumatic Stress Disorder Checklist for DSM-5) to investigate PTSD symptomatology. The final score has been calculated adding up the scores of each cluster (a provisory diagnosis of PTSD can be diagnosed with a minimum score of 1 item in clusters B and C, of 2 items in cluster D and E) [7]:
- T1: pre-surgery consulting by a gynecologist, from one month to one week before the interventions. Here patients have been asked to join the study. Those who accepted, had to fill out a social-demographic questionnaire and the HADS scale;
- T2: first post-surgery day. Patients had to fill out HADS and PCL-5 scales;
- T3: 3 months after surgery. Each patient has been called and the HADS and PCL-5 scales were administrated.
The PLC-5 has not been translated into Italian, thus it was administered in English. In instances where the participant faced difficulty in comprehension, the scale was presented through an interview conducted by a specialized operator.
In both populations the following data have also been collected: the primary indication to hysterectomy (symptomatic uterine fibromatosis, abnormal uterus bleeding, endometriosis/adenomyosis, pelvic/abdominal pain, genital prolapse and precancerous lesions), surgical data (surgical approach, removal of the ovaries), pathology report (Division of Pathologic Anatomy and Histology of Circolo and Macchi foundation Hospital of Varese) and postoperative complications (including ER accesses).
Data were analyzed through the software SPSS Inc. (released software 2015, IBM SPSS statistics for Mac) [8]
3. Results
3.1. Sociodemographic Characteristics
The flow-chart of the study population is reported in Figure 1. Overall, the study focused on 139 patients enrolled in the investigation, 100 (71.9%) in the pre-COVID 19 cohort and 39 (28.1%) in the post-COVID 19. Baseline socio-demographic features of both groups are shown in Table 1.
No statistically significant differences emerged in terms of sociodemographic variables between the pre-COVID-19 sample and the post-COVID-19 sample. The median age at the time of surgery did not show a significant difference between the groups; however, the majority of the post-COVID-19 population was slightly younger, albeit not significantly. In both populations, the patients demonstrated a high level of education. Furthermore, the majority of individuals in both samples were employed, married, and most patients had at least one child, lived with family, and did not undergo pharmacotherapy. Surgical-related outcomes of the two groups are reported in Table 2.
No substantial disparities were observed in terms of surgical approach; laparoscopy emerged as the predominant surgical method in both groups. Similarly, there were no discernible distinctions in the indications for surgery, with uterine fibroids constituting the most prevalent indication in both cohorts. Furthermore, the majority of treated patients did not undergo oophorectomy beyond hysterectomy. Notably, a majority of the patients did not encounter postoperative complications related to surgery.
3.2. Psychopathological Characteristics
Depressive and anxiety trend evaluation on T1, T2, T3, are shown in Table 3. Differences at the psychopathological evaluation were highlighted at T1 , T2 and T3.
As regards as anxiety score, no statistically significative differences were found between the two groups at T1 or T2 or T3.
In terms of depressive scores, a statistically significant difference in total scores between the two populations was observed at T1 (p-value < 0.001). Specifically, the post-COVID-19 population exhibited higher rates of mild and severe symptoms (p-value = 0.05) and general depressive symptoms (p-value = 0.02). A higher proportion of women displayed depressive symptoms in the post-COVID-19 sample compared to the pre-COVID-19 sample (p-value = 0.02). No statistically significant differences were found between the two groups at T2. However, a statistically significant difference (p-value = 0.01) in mood deflection at T3 favored the pre-COVID-19 population.
As regards PTSD symptoms, a 7% in pre-COVID-19 population and 8% in post-COVID-19 population showed symptoms referable to PTSD with no statistically significative differences at T2 (p-value=1). At T3, PTSD symptoms are statistically significative higher in pre-COVID-19 population, 14 patients (16.4%) vs 1 patient (3%) (p-value =0.04).
A total of 15 patients (were diagnosed as PTSD (14 subjects in pre-COVID-19 period and one woman in post-COVID-19 period), while 15 patients showed post-traumatic symptoms (13 pre-COVID-19 and 2 post-COVID-19). The remaining 109 patients (73 pre-COVID-19, 36 post-COVID-19) had no criteria fulfilling a PTSD diagnosis.
The only significant factor among all the socio demographic and surgical variables associated with PTSD was the recruitment period; specifically, we found a positive association between the pre-COVID-19 period and PTSD (p-value=0.03). PTSD at T3 was identified in 93% during the pre-COVID period (P=14) compared to 7% in the post-COVID period (P= 1)
4. Discussion
The most interesting finding consists in the correlation between depressive symptoms and post-traumatic stress disorder. In fact, 40% of women with post-surgical depression would develop a PTSD in the follow up and 80% of patients with depressive symptoms in T3 had in comorbidity post-traumatic symptoms. For these reasons we encourage the use of psychometric and psycho-diagnostic scales to early identify these risky situations that might evolve in a PTSD, compromising the therapeutic adherence and worsening the outcome with consequent direct and indirect costs [9].
The two populations also differed in terms of depressive symptoms: basal depressive symptoms were higher in post-COVID-19 population in line with many studies published in literature [10,11,12,13], but the same population showed lower depressive symptoms three months away from surgery. Otherwise, with regard to anxious symptomatology, no differences emerged in the two groups which showed a decreasing trend from the pre-operative evaluation to the three months follow-up evaluation.
A relevant reduction of depressive symptoms emerged in the post-COVID-19 population with basal depressive symptoms, in contrast with the literature that has described high levels of depression during pandemic period [13,14]. The reduction of the depression trend, without statistical significance, is probably due to the low numerosity of the sample with such symptoms.
Depressive symptoms in pre-COVID-19 population without basal depressive symptoms show a statistically significative progression. Mood deflection is the only variable predicting PTSD onset. A 40% of the patients with depressive symptoms developed a PTSD at T2, while 30% of them at T3. Three months away from surgery, PTSD rate in population was 3% in post-COVID-19 population and 16% in pre-COVID-19 population.
Unlike the initial hypothesis, the post-Covid 19 sample showed lower post-surgical PTSD rates than the pre-covid population at the three months follow-up evaluation
The association between PTSD and surgical characteristics shows no significance relevance. The only variable statistically significative was the period of recruitment. A 93% of patients in pre-COVID-19 period developed a PTSD three months away from surgery.
This result can be explained by the fact that people in post-pandemic period tend to relocate the subject of concern from the surgery to the pandemic situations and its consequences, experiencing the end of the hospitalization as the end of the extreme distance from family members and benefiting from the idea of being discharged without contracting the COVID-19 infection.
Moreover, the results showed that the COVID-19 pandemic has impacted negatively on mental health of patients evaluated, giving especially a worsening of their mood. This result is confirmed by other studies in professional literature[11,15]. Post-surgery distress has decreased in pandemic era (p-value=0.04), maybe due to the fear of getting COVID-19 in the hospital that lead to desert clinical checks up [16,17,18].
Some limitations need to be addressed. First, the study includes a relatively small sample size, particularly in the post-COVID-19 group.
Secondly, we employed a self-administered psychometric scale that indicates the presence of symptoms but does not enable a diagnostic determination. Third, all the operations were performed via a minimally invasive surgery, specifically laparoscopy, which did not allow to evaluate the impact of other surgical approaches on PTSD. The assessment of the level of education faced the same limitation, as all the patients reported having a high level of education.
5. Conclusions
In conclusion, this study reveals a noteworthy link between depressive symptoms and post-traumatic stress disorder (PTSD). Our findings underscore the importance of early identification using psychometric and psycho-diagnostic scales, as untreated cases may compromise therapeutic adherence and lead to adverse outcomes with associated direct and indirect costs. The results of this investigation might contribute to a more comprehensive understanding of the observed correlations and facilitate the development of targeted interventions for at-risk individual.
Informed Consent Statement
Informed consent was obtained from every participants (or their parent/legal guardian/next of kin) before to participate in the study. .
Conflicts of Interest
There are no conflicts of interest.
References
- R. El-Gabalawy et al., «Post-traumatic stress in the postoperative period: current status and future directions», Can. J. Anesth. Can. Anesth., vol. 66, fasc. 11, pp. 1385–1395, nov. 2019. [CrossRef]
- J. Casarin et al., «Post-traumatic stress following total hysterectomy for benign disease: an observational prospective study», J. Psychosom. Obstet. Gynecol., vol. 43, fasc. 1, pp. 11–17, gen. 2022. [CrossRef]
- C. L. Liu, L. C. L. Liu, L. Liu, Y. Zhang, X. Z. Dai, e H. Wu, «Prevalence and its associated psychological variables of symptoms of depression and anxiety among ovarian cancer patients in China: a cross-sectional study», Health Qual. Life Outcomes, vol. 15, fasc. 1, p. 161, dic. 2017. [Google Scholar] [CrossRef]
- C. Brennan, A. C. Brennan, A. Worrall-Davies, D. McMillan, S. Gilbody, e A. House, «The Hospital Anxiety and Depression Scale: A diagnostic meta-analysis of case-finding ability», J. Psychosom. Res., vol. 69, fasc. 4, pp. 371–378, ott. 2010. [Google Scholar] [CrossRef]
- M. Hoskins et al., «Pharmacotherapy for post-traumatic stress disorder: Systematic review and meta-analysis», Br. J. Psychiatry, vol. 206, fasc. 2, pp. 93–100, feb. 2015. [CrossRef]
- N. Poloni et al., «Oral Antipsychotic Versus Long-Acting Injections Antipsychotic in Schizophrenia Spectrum Disorder: a Mirror Analysis in a Real-World Clinical Setting», Psychopharmacol. Bull., vol. 49, fasc. 2, pp. 17–27, giu. 2019.
- Weathers, F. W. , Palmieri, P. A, Marx, B. P., Schnurr, P. P, Litz, B., e Keane, T. M., «The PTSD Checklist for DSM-5 (PCL-5) – Standard [Measurement instrument].» 2013.
- «SPSS Inc. (released software 2015, IBM SPSS statistics for Mac)».
- C. Callegari et al., «Paroxetine versus Vortioxetine for Depressive Symptoms in Postmenopausal Transition: A Preliminary Study», Psychopharmacol. Bull., vol. 49, fasc. 1, pp. 28–43, feb. 2019.
- W. Li et al., «The Prevalence of Psychological Status During the COVID-19 Epidemic in China: A Systemic Review and Meta-Analysis», Front. Psychol., vol. 12, p. 614964, mag. 2021. [CrossRef]
- Y.-J. Zhao et al., «The prevalence of psychiatric comorbidities during the SARS and COVID-19 epidemics: a systematic review and meta-analysis of observational studies», J. Affect. Disord., vol. 287, pp. 145–157, mag. 2021. [CrossRef]
- M. Necho, M. M. Necho, M. Tsehay, M. Birkie, G. Biset, e E. Tadesse, «Prevalence of anxiety, depression, and psychological distress among the general population during the COVID-19 pandemic: A systematic review and meta-analysis», Int. J. Soc. Psychiatry, vol. 67, fasc. 7, pp. 892–906, nov. 2021. [Google Scholar] [CrossRef]
- J. Deng et al., «The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis», Ann. N. Y. Acad. Sci., vol. 1486, fasc. 1, pp. 90–111, feb. 2021. [CrossRef]
- R. Lakhan, A. R. Lakhan, A. Agrawal, e M. Sharma, «Prevalence of Depression, Anxiety, and Stress during COVID-19 Pandemic», J. Neurosci. Rural Pract., vol. 11, pp. 519–525, set. 2020. [Google Scholar] [CrossRef]
- M. Gultekin et al., «Perspectives, fears and expectations of patients with gynaecological cancers during the COVID-19 pandemic: A Pan-European study of the European Network of Gynaecological Cancer Advocacy Groups (ENGAGe)», Cancer Med., vol. 10, fasc. 1, pp. 208–219, gen. 2021. [CrossRef]
- M. R. Kibbe, «Surgery and COVID-19», JAMA, vol. 324, fasc. 12, p. 1151, set. 2020. [CrossRef]
- D. W. Franco et al., «Medical adherence in the time of social distancing: a brief report on the impact of the COVID-19 pandemic on adherence to treatment in patients with diabetes», Arch. Endocrinol. Metab., apr. 2021. [CrossRef]
- C. López-Medina et al., «Treatment adherence during the COVID-19 pandemic and the impact of confinement on disease activity and emotional status: A survey in 644 rheumatic patients», Joint Bone Spine, vol. 88, fasc. 2, p. 105085, mar. 2021. [CrossRef]
Figure 1.
populations flow chart.
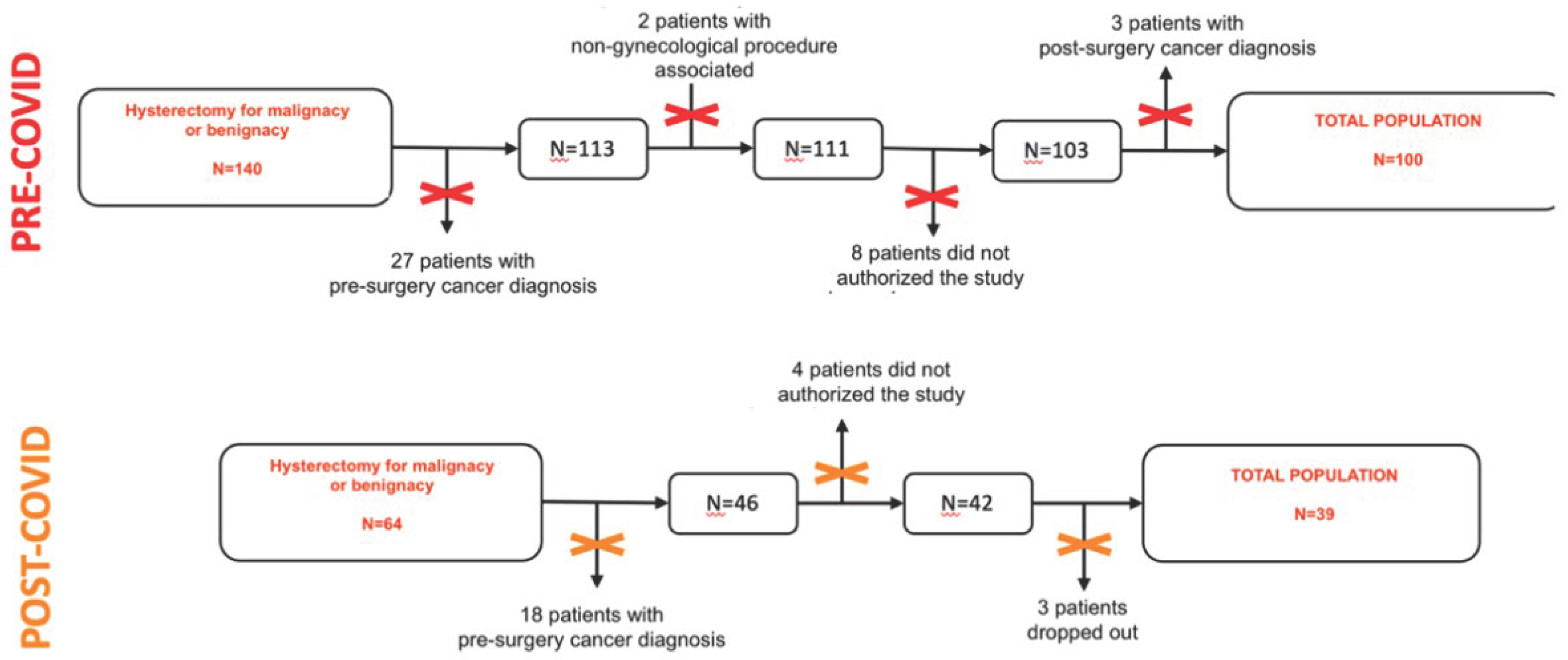

Table 1.
Sociodemographic variables in both populations.
| Socio-demographic | Pre COVID-19 (N=100) |
Post COVID-19 (N=39) |
P-value |
|---|---|---|---|
|
Age <40 40-50 >50 |
51 (36-77) 4 (4%) 45 (45%) 51 (51%) |
47 (36-71) 4 (10%) 24 (62%) 11 (28%) |
0.10 |
|
Menopause Yes No |
27 (27%) 73 (73%) |
14 (36%) 25 (64%) |
0.44 |
|
Education Primary Secondary High school Degree |
0 (0%) 33 (33%) 50 (50%) 17 (17%) |
2 (5%) 10 (26%) 20 (51%) 7 (18%) |
0.14 |
|
Employment Employee Unemployed Housewife Retiree |
73 (73%) 16 (16%) 9 (9%) 2 (2%) |
29 (74%) 5 (13%) 3 (8%) 2 (5%) |
0.75 |
|
Marital status Married Unmarried Divorced Widowed |
64 (64%) 22(22%) 12 (12%) 2 (2%) |
28 (72%) 7 (18%) 4 (10%) 0 (0%) |
0,72 |
|
Parity 0 1 >1 |
29 (29%) 22 (22%) 49 (49%) |
6 (16%) 13 (33%) 20 (51%) |
0.11 |
|
Living with Alone Family Parents Other |
15 (15%) 77 (77%) 3 (3%) 5 (5%) |
3 (8%) 34 (87%) 1 (2,5%) 1 (2,5%) |
0.59 |
|
Pharmacological therapy No therapy Therapy Antidepressants Anxiolytics/hypnotic Combined |
80 (80%) 20 (20%) 4 (4%) 14 (14%) 2 (2%) |
34 (87%) 5 (13%) 0 (0%) 5 (13%) 0 (0%) |
0.46 |
Table 2.
Surgical gynecological variables in both populations.
| Surgery |
Pre COVID-19 (N=100) |
Post COVID-19 (N=39) |
P-value |
|---|---|---|---|
|
Surgical indication Fibromatosis Endometriosis Genital prolapse Abnormal bleeding uterus Endometrial hyperplasia Other |
71 (71%) 10 (10%) 14 (14%) 3 (3%) 2 (2%) 0 (0%) |
28 (72%) 5 (13%) 2 (5%) 1 (2.5%) 1 (2.5%) 2 (5%) |
0.20 |
|
Surgical approach Laparoscopic Laparotomy Others |
90 (90%) 1 (1%) 9 (9%) |
37 (95%) 2 (5%) 0 (0%) |
0.06 |
|
Oophorectomy Yes No |
25 (25%) 75 (75%) |
14 (36%) 25 (64%) |
0.21 |
|
Post-surgery complications Yes No |
10 (10%) 90 (90%) |
7 (18%) 32 (82%) |
0.25 |
Table 3.
Depressive and anxiety trend evaluation on T1, T2, T3.
| Pre-COVID-19 | Post-COVID-19 | |||
|---|---|---|---|---|
| Median (range) | P-value | Median (range) | P-value | |
|
HADS ANXIETY SCORE T1 T2 T3 |
7 (0-21) 6 (0-18) 4 (0-20) |
0.01 |
6 (0-16) 5 (0-18) 5 (0-12) |
0.02 |
|
HADS DEPRESSION SCORE T1 T2 T3 |
3 (0-14) 3 (0-15) 2 (0-17) |
0.20 |
5 (0-16) 4 (0-16) 4 (0-14) |
0.66 |
|
HADS DEPRESSION SCORE Negative T1 cut-off T1 T2 T3 |
3 (0-7) 3 (0-12) 4 (0-15) |
<0.001 |
4 (0-8) 3 (0-9) 3 (0-8) |
0.56 |
|
HADS DEPRESSION SCORE Positive T1 cut-off T1 T2 T3 |
13 (8-21) 11 (5-18) 7 (0-20) |
0.10 |
10 (8-12) 7 (2-16) 7 (0-14) |
0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



