
Submitted:
03 April 2024
Posted:
03 April 2024
You are already at the latest version
Abstract
The biological aging, characterized by changing in metabolism and physicochemical properties of cells, has an impact on public health. Environment and lifestyle including factors like diet and physical activity seems to play a key role in healthy ageing. Several studies have shown that regular physical activity can enhance antioxidant defence mechanisms, including the activity of enzymes such as superoxide dismutase (SOD), catalase, and glutathione peroxidase. However, intense or prolonged exercise can also lead to an increase in ROS production temporarily, re-sulting in oxidative stress. This phenomenon is referred as "exercise-induced oxidative stress". The relationship between physical activity and oxidative stress in aging is complex and depends on various factors such as the type, intensity, duration, and frequency of exercise, as well as in-dividual differences in antioxidant capacity and adaptation to exercise. In this review, we ana-lyzed what is reported from several authors regarding the role of physical activity on oxidative stress in aging process as well as the role of hormesis and physical exercise as tools for preven-tion and treatment of sarcopenia, an aging related disease. Finally we reported what has recently been studied in relation to the effect of physical activity and sport on aging in women
Keywords:
aging
; oxidative stress
; sarcopenia
; hormesis
1. Introduction
The improvement of living conditions and advances in medicine lead to an increase of life expectation. According to World Health Organization (WHO) by 2050 people aged 60 years old and older will double from 12% to 22% reaching 2.1 billion while persons aged 80 years or older will triple reaching 426 million [1].
Identify strategies to maintain wellbeing in older age is important since ageing global population is a relatively new problem worldwide. The biological aging is characterized by changing in metabolism and physicochemical properties of cells that manifested with several complex health conditions having an impact on public health [2]. Environment and lifestyle including factors like diet and physical activity seems to play a key role in healthy ageing.
Several studies have shown that regular physical activity can enhance antioxidant defence mechanisms, including the activity of enzymes such as superoxide dismutase (SOD), catalase, and glutathione peroxidase [3]. Exercise has been found to increase the production of endogenous antioxidants and improve the efficiency of mitochondrial function, which can help reduce oxidative stress. However, intense or prolonged exercise can also lead to an increase in ROS production temporarily, resulting in oxidative stress. This phenomenon is often referred to as “exercise-induced oxidative stress”. The relationship between physical activity and oxidative stress in aging is complex and depends on various factors such as the type, intensity, duration, and frequency of exercise, as well as individual differences in antioxidant capacity and adaptation to exercise.
In this review, we investigate the role of oxidative stress in aging process. Further, we analyze the role of hormesis and physical exercise as tools for prevention and treatment of sarcopenia, an aging related disease.
Understanding the interplay between physical activity, oxidative stress, and aging has important clinical implications for the development of interventions aimed at promoting healthy aging and preventing age-related diseases. Strategies such as regular exercise, antioxidant supplementation, and lifestyle modifications can potentially help mitigate the negative effects of oxidative stress and improve overall health and longevity in older adults.
2.1. Aging
Aging is a complex process characterized by a gradual decline in physiological function and an increased vulnerability to diseases. It encompasses various physical, psychological, and social changes that occur as individuals grow older. Biological aging is influenced by genetic factors, environmental factors, lifestyle choices, and other variables. Some common manifestations of aging include wrinkles, reduced muscle mass, decreased bone density, diminished sensory functions, and cognitive decline. Oxidative stress, which results from an imbalance between the production of reactive oxygen species (ROS) and the body’s antioxidant defences, is considered one of the key mechanisms underlying aging. Moreover, biological aging is a complex process characterized by accumulation of DNA damages, cellular senescence, mitochondrial disfunction, reduction of telomere length, loss of proteostasis, imbalanced metabolism, and stem cell exhaustion (Figure 1 panel a) [4]. All of these hallmarks lead a progressive decline in tissue and organ function. Differences in aging between men and women encompass various biological and physiological effect showed in Figure 1 panel b and in several point reported below [5].
Among biological factors, hormonal changes are due to menopause experienced by women that leads to decreased estrogen levels that can influence bone density, skin elasticity, and other physiological functions. On the contrary, men showed a testosterone decline, they experience a gradual decline in testosterone levels with age, which can affect muscle mass, bone density, and sexual function.
Among physiological differences authors reported:
Muscle Mass: Generally, men have greater muscle mass and strength compared to women due to higher testosterone levels, although this difference tends to diminish with age.
Fat Distribution: Women typically have more subcutaneous fat, particularly around the hips and thighs, while men tend to accumulate more visceral fat around the abdomen, which can increase the risk of cardiovascular diseases.
Bone Density: Women are at a higher risk of osteoporosis due to hormonal changes post-menopause, leading to decreased bone density and increased susceptibility to fractures.
Cognitive Decline: While both men and women experience cognitive decline with age, research suggests that women may have a slightly lower risk of developing cognitive impairment and Alzheimer’s disease compared to men.
2.2. Oxidative Stress in Aging
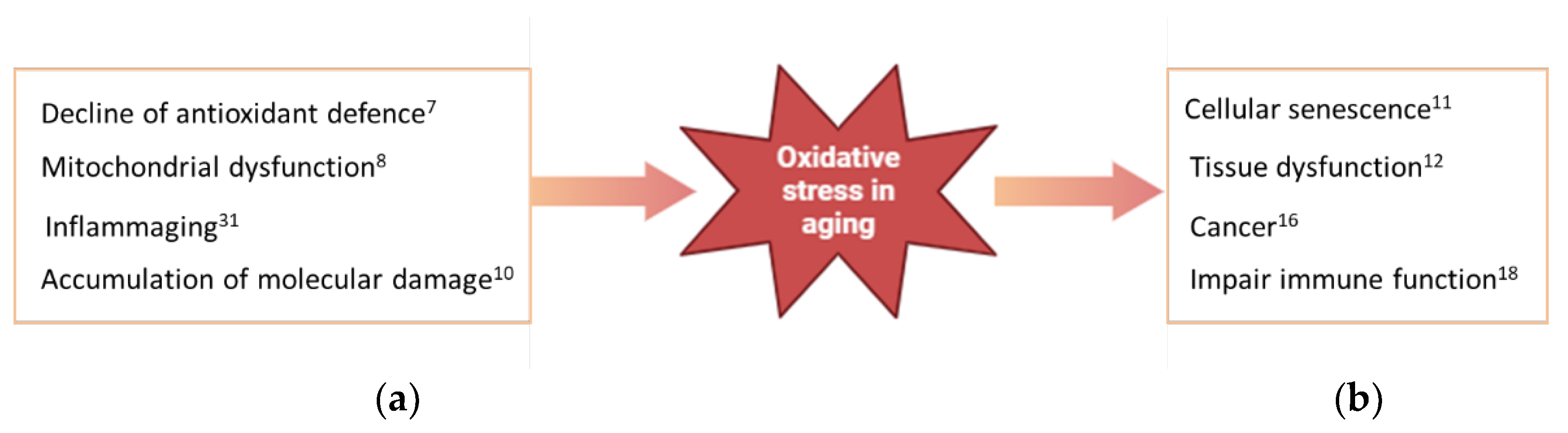
Oxidative stress occurs when there is an imbalance between the production of ROS and the body’s ability to detoxify them or repair the resulting damage. ROS are highly reactive molecules that can damage cellular components such as proteins, lipids, and DNA, leading to cellular dysfunction and contributing to the aging process [6]. In aging, several factors contribute to increased oxidative stress. Several of these are summarized below
Decline in Antioxidant Defences: The body’s antioxidant defences, including enzymes like superoxide dismutase (SOD), catalase, and glutathione peroxidase, decline with age. This reduction in antioxidant capacity makes older individuals more susceptible to oxidative damage [7].
Mitochondrial Dysfunction: Mitochondria, the energy-producing organelles within cells, are a major source of ROS. As mitochondria age, they become less efficient at producing energy and more prone to generating ROS as a by-product of respiration. This contributes to a vicious cycle of oxidative stress and mitochondrial dysfunction [8].
Inflammation: Chronic low-grade inflammation, often termed “inflammaging,” is a hallmark of aging. Inflammatory processes can stimulate the production of ROS and exacerbate oxidative stress. Conversely, oxidative stress can also promote inflammation, creating a feedback loop that contributes to age-related tissue damage [9].
Accumulation of Damage: Over time, cumulative oxidative damage to cellular components like DNA, proteins, and lipids can impair cellular function and contribute to age-related decline in tissue and organ function [10].
The consequences of oxidative stress in aging are wide-ranging and can affect various physiological systems reported here:
Cellular Aging: Oxidative damage contributes to cellular senescence, a state of irreversible growth arrest that limits the replicative capacity of cells and contributes to tissue aging [11].
Tissue Dysfunction: Oxidative stress plays a role in age-related degenerative diseases such as cardiovascular disease, neurodegenerative diseases (e.g., Alzheimer’s disease, Parkinson’s disease), and age-related macular degeneration [12,13,14,15].
Cancer: While oxidative stress can promote DNA damage and increase the risk of mutations that lead to cancer, paradoxically, cancer cells often exhibit increased antioxidant defences to protect themselves from oxidative damage [16,17].
Immune Function: Oxidative stress can impair immune function, making older individuals more susceptible to infections and less responsive to vaccines [18,19].
Figure 2.
Oxidative stress in aging: (a) factors producing ROS in aging; (b) consequences of oxidative stress in aging.
Figure 2.
Oxidative stress in aging: (a) factors producing ROS in aging; (b) consequences of oxidative stress in aging.
Efforts to mitigate oxidative stress and its effects on aging include lifestyle interventions such as maintaining a balanced diet rich in antioxidants, regular exercise, avoiding tobacco smoke and excessive alcohol consumption, and managing chronic conditions like diabetes and hypertension. More than 300 theories have been proposed to explain the phenomena of ageing but it is clear that a single theory could not explain all the mechanism of ageing [20]. ROS are important for the defence mechanism and signaling transduction [21,22]. These pathways play an important role in various cellular processes such as cell growth, inflammatory response, autophagy or adaptive response for oxidative stress [23]. However, accumulations of ROS has negative effect on health and induce oxidative stress (OS) [24]. The primary endogenous sources for ROS production are mitochondria via oxidative phosphorylation but in mammals cells different protein complexes are responsible of ROS production [25,26].
2.3. Hormesis, Aging and Physical Activity
Southam and Erhlich to indicate the effect of plant extracts on fungi culture [26] used the term hormesis for the first time in scientific literature in 1943. Hormesis is a biological phenomenon where exposure to low doses of a stressor or toxin induces adaptive responses in an organism, resulting in improved health and longevity. This concept suggests that mild stressors can activate cellular mechanisms that enhance resilience and resistance to more severe stressors. Exercise for example, is one of hormetic stressor that has been extensively studied for its beneficial effects on aging. In the context of aging, hormesis has been proposed as a potential mechanism to delay or mitigate age-related decline and promote longevity. Several stressors, such as calorie restriction, exercise, heat shock, and certain phytochemicals, have been studied for their hormetic effects on aging [28]. The hormetic effects of physical activity on aging are thought to involve multiple mechanisms, including the activation of cellular stress response pathways (such as the AMPK and sirtuin pathways) [29], enhanced autophagy [30] and improved mitochondrial function [31]. These adaptations help the body cope with stress more effectively, leading to greater resilience and longevity. Regular physical activity, particularly aerobic and resistance training, induces mild oxidative stress and inflammation, which triggers adaptive responses in muscles, bones, and other tissues, leading to improved function and resilience with age [32]. This stress triggers a cascade of physiological responses aimed at adapting to the demands placed upon it. These adaptations showed in Figure 3 include:
Muscle Growth and Strength: Resistance training, such as weightlifting, places stress on muscles, leading to microscopic damage to muscle fibers. In response, the body repairs and rebuilds these fibers, resulting in increased muscle mass and strength [33].
Cardiovascular Fitness: Aerobic exercise, like jogging or cycling, stresses the cardiovascular system by increasing heart rate and blood flow. Over time, the heart becomes more efficient at pumping blood, and the blood vessels become more elastic, leading to improved cardiovascular fitness and reduced risk of heart disease [34].
Bone Density: Weight-bearing exercises, such as walking or running, stress the bones, stimulating bone remodeling and increasing bone density. This helps prevent osteoporosis and reduces the risk of fractures [35,36].
Metabolic Health: Exercise enhances insulin sensitivity, promotes glucose uptake by muscles, and improves lipid profiles, all of which contribute to better metabolic health and reduced risk of conditions like type 2 diabetes and metabolic syndrome [37,38].
Mood and Cognitive Function: Physical activity triggers the release of endorphins and other neurotransmitters that promote feelings of well-being and reduce stress and anxiety. Regular exercise has also been linked to improved cognitive function and reduced risk of cognitive decline with aging [39,40]. It’s important to note that while moderate exercise provides a beneficial hormetic effect, excessive or overly intense exercise can have the opposite effect, leading to excessive stress, inflammation, and potential injury.
Therefore, finding the right balance and incorporating rest and recovery into exercise routine is crucial for reaping the full benefits of hormesis from physical activity [41,42]. Overall, hormesis provides a theoretical framework for understanding how exposure to mild stressors can stimulate adaptive responses that promote health and longevity. While more research is needed to fully elucidate the mechanisms underlying hormesis and its implications for aging, the concept holds promise for developing interventions to delay age-related decline and extend lifespan.
2.4. Physical Activity in Aging
Regular physical activity has been shown to have numerous benefits for overall health and well-being, including mitigating some of the effects of aging. Exercise helps improve cardiovascular health, maintain muscle mass and strength, enhance cognitive function, and increase overall longevity [43]. Regular physical activity helps to prevent cardiovascular and metabolic disease, obesity, falls, cognitive impairments, osteoporosis and muscular weakness are decreased by regularly completing activities ranging from low intensity walking through to more vigorous sports and resistance exercise. But despite evidence show that is safe for healthy and older people the participation of latter remains low.
In general, the more often a person is physically active, the better their physical capability. This is due to adaptations of physiological systems, most notably within the neuromuscular system to coordinate movements, the cardiopulmonary system to more effectively distribute oxygen and nutrients around the body, and metabolic processes particularly those regulating glucose and fatty acid metabolism, which collectively increase overall aerobic power and physical capability. Thus, the trajectory towards frailty is directly modifiable through physical activity habits [44,45]. Physical activity is extremely important for elderly individuals as it offers a wide range of physical and mental health benefits. Regular physical activity can help improve strength, flexibility, balance, and cardiovascular health, all of which are crucial for maintaining independence and reducing the risk of falls and injuries in older adults [46].
Engaging in physical activity can also help manage chronic conditions such as arthritis, osteoporosis, and diabetes. It can improve mood, reduce symptoms of depression and anxiety, and enhance cognitive function. Additionally, staying physically active promotes social interaction and can contribute to a greater sense of well-being and overall quality of life [47]. It’s important for elderly individuals to choose activities that are appropriate for their fitness level and health status. This might include walking, swimming, cycling, tai chi, yoga, or strength training exercises [48]. It’s also important to consult with a healthcare professional before starting any new exercise program, especially if there are underlying health concerns [49]. Overall, encouraging and supporting elderly individuals to remain physically active can significantly improve their health and vitality as they age [50].
2.5. Sarcopenia in Aging
Sarcopenia refers to the gradual loss of muscle mass, strength, and function that occurs with aging. It is a natural part of the aging process, typically starting around middle age but accelerating after the age of 75. Several factors contribute to sarcopenia, including decreased physical activity [51,52]. It is a multifactorial and complex phenomenon whose underlying mechanisms are not clearly defined. Based on etiological factors sarcopenia is classified in primary when no specific cause other that aging is evident and secondary when other factors like inflammatory and endocrine diseases are evident. Moreover, bad habits like physical inactivity and undernutrition may be a factor that contributes to the development of sarcopenia [53].
The European working group on sarcopenia in older people (EWGSOP) proposed diagnostic criteria based on muscle mass, muscle strength and physical performance [54]. In 2018 EWGSOP revised the parameter of sarcopenia diagnosis giving more importance to muscle strength than muscle mass to predict adverse outcomes [55]. The lack of exercise is one of the major risk factors of sarcopenia and resistance exercise is the main no-pharmacological tool for the management of sarcopenia [56]. In aging muscle there is an imbalance between protein synthesis and degradation that lead a decrease in muscle mass [57]. The consequences of sarcopenia can be significant, as it can lead to decreased mobility, increased risk of falls and fractures, loss of independence, and overall decreased quality of life. It has also associated with increased mortality rates [58].
Preventing and managing sarcopenia involves a multifaceted approach that includes regular physical activity, especially resistance training to maintain muscle mass and strength, adequate protein intake to support muscle repair and growth, and overall good nutrition [59]. Additionally, managing chronic illnesses and addressing hormonal imbalances can help mitigate the effects of sarcopenia [60,61].
Early detection and intervention are crucial in combating sarcopenia. Regular assessments of muscle mass, strength, and function can help identify individuals at risk, allowing timely interventions to preserve muscle health and function as people age [62].
2.5. Sarcopenia, Mitochondrial Dysfunction and Physical Activity
Different studies have highlighted the link between mitochondrial disfunction and sarcopenia. In aging muscle are evident mitochondrial alteration like morphological changes and downregulation of PGC1-alpha, the factor that regulate mitochondrial biogenesis [63]. Otherwise, mitochondrial damage induces the accumulation of ROS [64]. Furthermore, PGC-1α expression stimulates the expression of antioxidant genes, including heme oxygenase 1 (HO-1) [65]. The imbalance between the production of ROS, Reactive Nitrogen Species (RNS) and antioxidant defences in the body is an early biomarker of sarcopenia [66]. ROS are produced during muscle contraction by mitochondrial electron transport chain during normal oxidative respiration [67]. With aging skeletal muscle increase the production of ROS which contributes to increase the damage of cell and muscle atrophy [68] because enhancing the ubiquitin-proteasome system, resulting in skeletal muscle atrophy [69]. Progressive resistance training is the most studied method of exercise. Aerobic exercise otherwise contributes to activate mitochondria biogenesis [70] and increase the synthesis of muscle protein like myostatin whose mRNA expression increase [71]. In general, aerobic exercise tend to ameliorate mitochondrial associate problems. In older adult no particular type of exercise satisfies all the needs request for the use of exercise as therapeutic tool in age-related sarcopenia and thus well-rounded aerobic and resistance exercise programs are recommended [72]. Moreover, the vibration therapy in case of inability is able to improve physical measurement [73].
2.6. Aging and Physical Activity in Women
Aging in females involves a complex interplay of physiological, psychological, and social changes that occur, as women grow older. Physical activity plays a crucial role in mitigating many of the physiological and psychological changes associated with aging in females. Overall, aging in females is a multifaceted process influenced by various factors. Here and in Figure 5 are summarized some key aspects of aging in females and how physical activity can positively influence them.
Menopause: characterized by a decline in hormone levels, particularly estrogen and progesterone, that can lead to various symptoms such as hot flashes, mood swings, weight gain, decreased bone density, and increased risk of cardiovascular disease. Regular physical activity can help alleviate many of these symptoms and improve overall well-being during menopause [74].
Bone Health: Women are at a higher risk of osteoporosis compared to men, particularly after menopause. Osteoporosis is characterized by decreased bone density and an increased risk of fractures. Maintaining a regular exercise, is crucial for preserving bone health, weight-bearing and resistance exercises help to maintain bone density and strength, reducing the risk of osteoporosis and fractures. Activities such as walking, jogging, dancing, and weightlifting are beneficial for bone health [75,76]. Moreover, several authors reported that resistance-training exercises help to build and maintain muscle mass, strength, and function, which can decline with age. Strong muscles support joint health, balance, and mobility, reducing the risk of falls and injuries [77].
Weight Management and metabolic changes: Menopause often brings about weight gain, especially around the abdomen. Metabolic rate tends to decrease with age, making weight management more challenging. Regular physical activity helps to maintain a healthy weight, improve insulin sensitivity, and reduce the risk of metabolic conditions such as type 2 diabetes and cardiovascular disease. Both aerobic exercise (e.g., walking, swimming, cycling) and strength training contribute to metabolic health [78,79].
Cardiovascular Health: Post-menopausal women have an increased risk of cardiovascular disease, partly due to changes in hormone levels [80,81]. Managing risk factors such as high blood pressure, high cholesterol, and diabetes through lifestyle modifications and medical treatment is essential for maintaining heart health [82]. Aerobic exercises such as brisk walking, cycling, and swimming are effective for improving cardiovascular fitness, reducing blood pressure, lowering cholesterol levels, and decreasing the risk of heart disease and stroke [83,84].
Cognitive Health, Psychological, and Social Well-being: While cognitive decline can occur with age, women may have a lower risk of developing certain neurodegenerative diseases such as Alzheimer’s disease compared to men [85]. However, they may experience cognitive changes associated with hormonal fluctuations and aging [86]. Moreover, aging can bring about psychological and social changes, including shifts in roles and relationships, retirement, caregiving responsibilities, and coping with loss [87]. Physical activity improves mood, reduces symptoms of anxiety and depression, and enhances cognitive function and brain health in older adults. Engaging in regular exercise can boost self-esteem, promote relaxation, and alleviate stress [88,89].
Moreover, participating in group-based physical activities or exercise classes can provide opportunities for social interaction, connection, and support, which are important for overall well-being and quality of life, particularly as women age [90,91,92]. It’s important for women to choose activities that they enjoy and that fit their individual preferences, abilities, and health goals. Consulting with a healthcare provider or a fitness professional can help in developing a safe and personalized exercise program tailored to individual needs and medical conditions.
2.7. Sport and Elderly Women
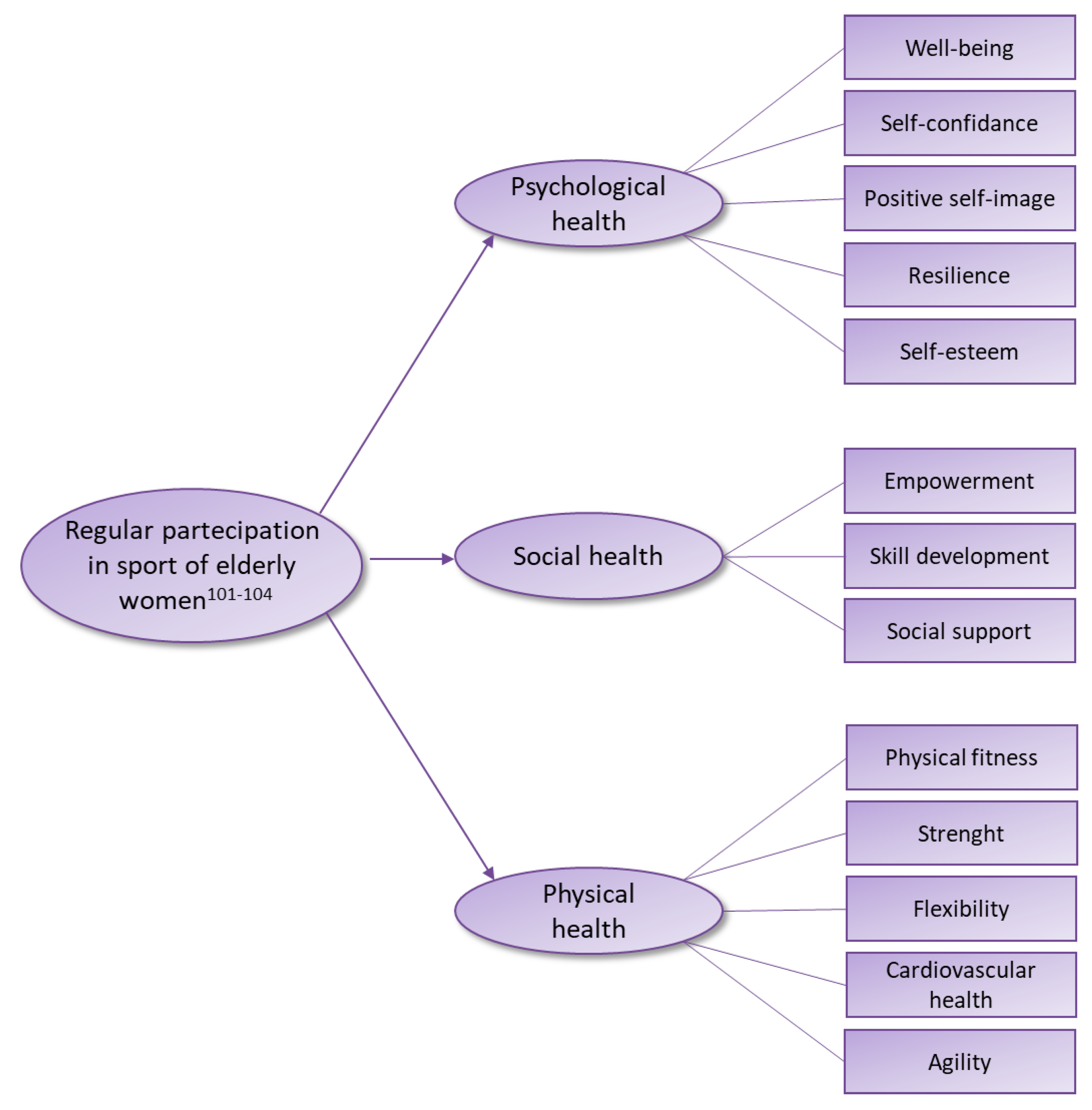
Regular participation in sports helps women maintain physical fitness, strength, flexibility, and cardiovascular health as they age (Figure 6). Activities such as running, swimming, cycling, tennis, and team sports provide opportunities for aerobic exercise, muscle strengthening, and agility training, contributing to overall health and vitality.
Moreover, sports participation can enhance self-esteem, self-confidence, and a sense of empowerment in women of all ages [102]. Achieving personal fitness goals, mastering new skills, and overcoming challenges in sports can build resilience and a positive self-image, particularly as societal attitudes toward aging continue to evolve. Engaging in sports offers opportunities for continuous learning, skill development, and personal growth throughout the aging process [103]. Women can explore new sports, adapt their training routines, and set new goals to stay active and motivated as they navigate different life stages [104]. It’s important for women to choose sports and physical activities that align with their interests, abilities, and health goals, and to consult with healthcare professionals or fitness experts as needed to ensure safety and appropriate exercise programming. With the right support and resources, sports participation can enrich the lives of women as they age, promoting health, vitality, and overall well-being.
5. Conclusions
What is reported in this review suggests that normal daily activity in elderly subjects preserves the independence of the elderly and keeps their oxidative state at low levels. Moreover, encouraging physical activity and sports practice among elderly, regardless of gender, should be a priority in healthcare and community settings. Tailored exercise programs, accessibility to suitable facilities, social support networks, and education on the importance of staying active can all contribute to improving the physical and mental well-being of elderly men and women. Additionally, addressing specific barriers faced by each gender group can help in promoting inclusivity and participation in physical activities among the elderly population.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable
Conflicts of Interest
The authors declare no conflicts of interest
References
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 2020, 139, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Dziechciaż, M.; Filip, R. Biological psychological and social determinants of old age: bio-psycho-social aspects of human aging. Ann Agric Environ Med. 2014, 21, 835–8. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Bustamante-Sanchez, Á.; Mielgo-Ayuso, J.; Martínez-Guardado, I.; Martín-Rodríguez, A.; Tornero-Aguilera, J.F. Antioxidants and Sports Performance. Nutrients. 2023, 15, 2371. [Google Scholar] [CrossRef]
- Ferrucci, L.; Gonzalez-Freire, M.; Fabbri, E.; Simonsick, E.; Tanaka, T.; Moore, Z.; Salimi, S.; Sierra, F.; de Cabo, R. Measuring biological aging in humans: A quest. Aging Cell. 2020, 19, e13080. [Google Scholar] [CrossRef] [PubMed]
- Hägg, S.; Jylhävä, J. Sex differences in biological aging with a focus on human studies. Elife. 2021, 10, e63425. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Mills, K.; le Cessie, S.; Noordam, R.; van Heemst, D. Ageing, age-related diseases and oxidative stress: What to do next? Ageing Res Rev. 2020, 57, 100982. [Google Scholar] [CrossRef]
- Viña, J.; Olaso-Gonzalez, G.; Arc-Chagnaud, C.; De la Rosa, A.; Gomez-Cabrera, M.C. Modulating Oxidant Levels to Promote Healthy Aging. Antioxid Redox Signal. 2020, 33, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Miller, B.; Kumagai, H.; Silverstein, A.R.; Flores, M.; Yen, K. Mitochondrial-derived peptides in aging and age-related diseases. Geroscience. 2021, 43, 1113–1121. [Google Scholar] [CrossRef] [PubMed]
- Vatic, M.; von Haehling, S.; Ebner, N. Inflammatory biomarkers of frailty. Exp Gerontol. 2020, 133, 110858. [Google Scholar] [CrossRef] [PubMed]
- Schaum, N.; Lehallier, B.; Hahn, O.; Pálovics, R.; Hosseinzadeh, S.; Lee, S.E.; Sit, R.; Lee, D.P.; Losada, P.M.; Zardeneta, M.E.; Fehlmann, T.; Webber, J.T.; McGeever, A.; Calcuttawala, K.; Zhang, H.; Berdnik, D.; Mathur, V.; Tan, W.; Zee, A.; Tan, M.; Tabula Muris Consortium; Pisco, A. O.; Karkanias, J.; Neff, N.F.; Keller, A.; Darmanis, S.; Quake, S.R.; Wyss-Coray, T. Ageing hallmarks exhibit organ-specific temporal signatures. Nature. 2020, 583, 596–602. [Google Scholar] [CrossRef]
- Finkel, T.; Holbrook, N.J. Oxidants, oxidative stress and the biology of ageing. Nature. 2000, 408, 239–47. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.C.; Bennett, M. Aging and atherosclerosis: mechanisms, functional consequences, and potential therapeutics for cellular senescence. Circ Res. 2012, 111, 245–59. [Google Scholar] [CrossRef] [PubMed]
- Hajam, Y.A.; Rani, R.; Ganie, S.Y.; Sheikh, T.A.; Javaid, D.; Qadri, S.S.; Pramodh, S.; Alsulimani, A.; Alkhanani, M.F.; Harakeh, S.; Hussain, A.; Haque, S.; Reshi, M.S. Oxidative Stress in Human Pathology and Aging: Molecular Mechanisms and Perspectives. Cells. 2022, 11, 552. [Google Scholar] [CrossRef] [PubMed]
- Ionescu-Tucker, A.; Cotman, C.W. Emerging roles of oxidative stress in brain aging and Alzheimer’s disease. Neurobiol Aging. 2021, 107, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Trist, B.G.; Hare, D.J.; Double, K.L. Oxidative stress in the aging substantia nigra and the etiology of Parkinson’s disease. Aging Cell. 2019, 18, e13031. [Google Scholar] [CrossRef]
- Jelic, M.D.; Mandic, A.D.; Maricic, S.M.; Srdjenovic, B.U. Oxidative stress and its role in cancer. J Cancer Res Ther. 2021, 17, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Klaunig, J.E. Oxidative Stress and Cancer. Curr Pharm Des. 2018, 24, 4771–4778. [Google Scholar] [CrossRef] [PubMed]
- Martínez de Toda, I.; Vida, C.; Sanz San Miguel, L.; De la Fuente, M. Function, Oxidative, and Inflammatory Stress Parameters in Immune Cells as Predictive Markers of Lifespan throughout Aging. Oxid Med Cell Longev. 2019, 2019, 4574276. [Google Scholar] [CrossRef] [PubMed]
- Frasca, D.; Blomberg, B.B. Adipose tissue, immune aging, and cellular senescence. Semin Immunopathol. 2020, 42, 573–587. [Google Scholar] [CrossRef] [PubMed]
- Harman, D. Aging: a theory based on free radical and radiation chemistry. J Gerontol. 1956, 11, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Finkel, T.; Holbrook, N.J. Oxidative stress and aging: Catalase is a longevity determinant enzyme. Nature. 2000, 408, 239. [Google Scholar] [CrossRef]
- Evans, J.L.; Goldfine, I.D.; Maddux, B.A.; Grodsky, G.M. Are oxidative stress-activated signaling pathways mediators of insulin resistance and β-cell dysfunction? Diabetes. 2003, 52, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, X.; Vikash, V.; Ye, Q.; Wu, D.; Liu, Y.; Dong, W. ROS and ROS-Mediated Cellular Signaling. Oxid. Med. Cell. Longev. 2016, 2016, 4350965. [Google Scholar] [CrossRef] [PubMed]
- Dröge, W. Free radicals in the physiological control of cell function. Physiol. Rev. 2002, 82, 47–95. [Google Scholar] [CrossRef] [PubMed]
- Kaludercic, N.; Mialet-Perez, J.; Paolocci, N.; Parini, A.; Di Lisa, F. Monoamine oxidases as sources of oxidants in the heart. J. Mol. Cell. Cardiol. 2014, 73, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Yasui, H.; Hayashi, S.; Sakurai, H. Possible involvement of singlet oxygen species as multiple oxidants in p450 catalytic reactions. Drug Metab. Pharmacokinet. 2005, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Southam, C.M.; Erhlich, J. Effects of extracts of western red-cedar heartwood on certain wood-decaying fungi in culture. Phytophathology 1943, 33, 517–524. [Google Scholar]
- Rattan, S.I. Hormesis in aging. Ageing Res Rev. 2008, 7, 63–78. [Google Scholar] [CrossRef] [PubMed]
- Bayod, S.; Del Valle, J.; Lalanza, J.F.; Sanchez-Roige, S.; de Luxán-Delgado, B.; Coto-Montes, A.; Canudas, A.M.; Camins, A.; Escorihuela, R.M.; Pallàs, M. Long-term physical exercise induces changes in sirtuin 1 pathway and oxidative parameters in adult rat tissues. Exp Gerontol. 2012, 47, 925–35. [Google Scholar] [CrossRef] [PubMed]
- Martel, J.; Ojcius, D.M.; Ko, Y.F.; Ke, P.Y.; Wu, C.Y.; Peng, H.H.; Young, J.D. Hormetic Effects of Phytochemicals on Health and Longevity. Trends Endocrinol Metab. 2019, 30, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Ristow, M.; Zarse, K. How increased oxidative stress promotes longevity and metabolic health: The concept of mitochondrial hormesis (mitohormesis). Exp Gerontol. 2010, 45, 410–8. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Martucci, M.; Conte, M.; Capri, M.; Franceschi, C.; Salvioli, S. Inflammaging, hormesis and the rationale for anti-aging strategies. Ageing Res Rev. 2020, 64, 101142. [Google Scholar] [CrossRef] [PubMed]
- Ji, L.L.; Kang, C.; Zhang, Y. Exercise-induced hormesis and skeletal muscle health. Free Radic Biol Med. 2016, 98, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Di Raimondo, D.; Rizzo, G.; Musiari, G.; Tuttolomondo, A.; Pinto, A. Role of Regular Physical Activity in Neuroprotection against Acute Ischemia. Int J Mol Sci. 2020, 21, 9086. [Google Scholar] [CrossRef]
- Ashe, M.C.; Santos, I.K.D.; Edward, N.Y.; Burnett, L.A.; Barnes, R.; Fleig, L.; Puyat, J.H.; Sale, J.E.M.; McKay, H.A.; Giangregorio, L.M. Physical Activity and Bone Health in Men: A Systematic Review and Meta-Analysis. J Bone Metab. 2021, 28, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.A.; Scott, D.; Seibel, M.J.; Cumming, R.G.; Naganathan, V.; Blyth, F.M.; Le Couteur, D.G.; Waite, L.M.; Handelsman, D.J.; Hirani, V. Higher-Impact Physical Activity Is Associated With Maintenance of Bone Mineral Density But Not Reduced Incident Falls or Fractures in Older Men: The Concord Health and Aging in Men Project. J Bone Miner Res. 2021, 36, 662–672. [Google Scholar] [CrossRef] [PubMed]
- Amanat, S.; Ghahri, S.; Dianatinasab, A.; Fararouei, M.; Dianatinasab, M. Exercise and Type 2 Diabetes. Adv Exp Med Biol. 2020, 1228, 91–105. [Google Scholar] [CrossRef] [PubMed]
- Tamura, Y.; Omura, T.; Toyoshima, K.; Araki, A. Nutrition Management in Older Adults with Diabetes: A Review on the Importance of Shifting Prevention Strategies from Metabolic Syndrome to Frailty. Nutrients. 2020, 12, 3367. [Google Scholar] [CrossRef] [PubMed]
- Nuzum, H.; Stickel, A.; Corona, M.; Zeller, M.; Melrose, R.J.; Wilkins, S.S. Potential Benefits of Physical Activity in MCI and Dementia. Behav Neurol. 2020, 2020, 7807856. [Google Scholar] [CrossRef] [PubMed]
- Nuzum, H.; Stickel, A.; Corona, M.; Zeller, M.; Melrose, R.J.; Wilkins, S.S. Potential Benefits of Physical Activity in MCI and Dementia. Behav Neurol. 2020, 2020, 7807856. [Google Scholar] [CrossRef] [PubMed]
- Fiorenza, M.; Gliemann, L.; Brandt, N.; Bangsbo, J. Hormetic modulation of angiogenic factors by exercise-induced mechanical and metabolic stress in human skeletal muscle. Am J Physiol Heart Circ Physiol. 2020, 319, H824–H834. [Google Scholar] [CrossRef] [PubMed]
- Santoro, A.; Martucci, M.; Conte, M.; Capri, M.; Franceschi, C.; Salvioli, S. Inflammaging, hormesis and the rationale for anti-aging strategies. Ageing Res Rev. 2020, 64, 101142. [Google Scholar] [CrossRef] [PubMed]
- Eckstrom, E.; Neukam, S.; Kalin, L.; Wright, J. Physical Activity and Healthy Aging. Clin Geriatr Med. 2020, 36, 671–683. [Google Scholar] [CrossRef] [PubMed]
- Nystoriak, M.A.; Bhatnagar, A. Cardiovascular Effects and Benefits of Exercise. Front Cardiovasc Med. 2018, 5, 135. [Google Scholar] [CrossRef] [PubMed]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: perspectives for healthy ageing and frailty. Biogerontology. 2016, 17, 567–80. [Google Scholar] [CrossRef] [PubMed]
- Wanigatunga, A.A.; Tudor-Locke, C.; Axtell, R.S.; Glynn, N.W.; King, A.C.; McDermott, M.M.; Fielding, R.A.; Lu, X.; Pahor, M.; Manini, T.M. Effects of a Long-Term Physical Activity Program on Activity Patterns in Older Adults. Med Sci Sports Exerc. 2017, 49, 2167–2175. [Google Scholar] [CrossRef] [PubMed]
- Merom, D.; Stanaway, F.; Gebel, K.; Sweeting, J.; Tiedemann, A.; Mumu, S.; Ding, D. Supporting active ageing before retirement: a systematic review and meta-analysis of workplace physical activity interventions targeting older employees. BMJ Open. 2021, 11, e045818. [Google Scholar] [CrossRef] [PubMed]
- Gamberi, T.; Gorini, G.; Fiaschi, T.; Morucci, G.; Pratesi, S.; et al. Effect of Functional Fitness on Plasma Oxidation Level in Elders: Reduction of the Plasma Oxidants and Improvement of the Antioxidant Barrier. American Journal of Sports Science 2018, 6, 55–64. [Google Scholar] [CrossRef]
- Morucci, G.; Ryskalin, L.; Pratesi, S.; Branca, J.J.V.; Modesti, A.; Modesti, P.A.; Gulisano, M.; Gesi, M. Effects of a 24-Week Exercise Program on Functional Fitness, Oxidative Stress, and Salivary Cortisol Levels in Elderly Subjects. Medicina 2022, 58, 1341. [Google Scholar] [CrossRef] [PubMed]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical activity and exercise: Strategies to manage frailty. Redox Biol. 2020, 35, 101513. [Google Scholar] [CrossRef] [PubMed]
- Billot, M.; Calvani, R.; Urtamo, A.; Sánchez-Sánchez, J.L.; Ciccolari-Micaldi, C.; Chang, M.; Roller-Wirnsberger, R.; Wirnsberger, G.; Sinclair, A.; Vaquero-Pinto, N.; Jyväkorpi, S.; Öhman, H.; Strandberg, T.; Schols, J.M.G.A.; Schols, A.M.W.J.; Smeets, N.; Topinkova, E.; Michalkova, H.; Bonfigli, A.R.; Lattanzio, F.; Rodríguez-Mañas, L.; Coelho-Júnior, H.; Broccatelli, M.; D’Elia, M.E.; Biscotti, D.; Marzetti, E.; Freiberger, E. Preserving Mobility in Older Adults with Physical Frailty and Sarcopenia: Opportunities, Challenges, and Recommendations for Physical Activity Interventions. Clin Interv Aging. 2020, 15, 1675–1690. [Google Scholar] [CrossRef] [PubMed]
- Barajas-Galindo, D.E.; González Arnáiz, E.; Ferrero Vicente, P.; Ballesteros-Pomar, M.D. Effects of physical exercise in sarcopenia. A systematic review. Endocrinol Diabetes Nutr (Engl Ed). 2021, 68, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Rosenburg, I. Summary comments: epidemiological and methodological problems in determining nutritional status of older persons. Am J Clin Nutr. 1989, 50, 1231–1233. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Buckinx, F.; Landi, F.; Cesari, M.; Fielding, R.A.; Visser, M.; Engelke, K.; et al. Pitfalls in the measurement of muscle mass: a need for a reference standard. J Cachexia Sarcopenia Muscle. 2018, 9, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, T. Efficacy of progressive resistance training interventions in older adults in nursing homes: a systematic review. J Am Med Dir Assoc. 2012, 13, 418–428. [Google Scholar] [CrossRef] [PubMed]
- Cannataro, R.; Carbone, L.; Petro, J.L.; Cione, E.; Vargas, S.; Angulo, H.; Forero, D.A.; Odriozola-Martínez, A.; Kreider, R.B.; Bonilla, D.A. Sarcopenia: Etiology, Nutritional Approaches, and Mirnas. Int. J. Mol. Sci. 2021, 22, 9724. [Google Scholar] [CrossRef] [PubMed]
- Martin, F.C.; Ranhoff, A.H. Frailty and Sarcopenia. 2020 Aug 21. In: Falaschi P, Marsh D, editors. Orthogeriatrics: The Management of Older Patients with Fragility Fractures [Internet]. 2nd ed. Cham (CH): Springer; [PubMed]
- Bao, W.; Sun, Y.; Zhang, T.; Zou, L.; Wu, X.; Wang, D.; Chen, Z. Exercise Programs for Muscle Mass, Muscle Strength and Physical Performance in Older Adults with Sarcopenia: A Systematic Review and Meta-Analysis. Aging Dis. 2020, 11, 863–873. [Google Scholar] [CrossRef] [PubMed]
- Mende, E.; Moeinnia, N.; Schaller, N.; Weiß, M.; Haller, B.; Halle, M.; Siegrist, M. Progressive machine-based resistance training for prevention and treatment of sarcopenia in the oldest old: A systematic review and meta-analysis. Exp Gerontol. 2022, 163, 111767. [Google Scholar] [CrossRef] [PubMed]
- Marcos-Pardo, P.J.; González-Gálvez, N.; López-Vivancos, A.; Espeso-García, A.; Martínez-Aranda, L.M.; Gea-García, G.M.; Orquín-Castrillón, F.J.; Carbonell-Baeza, A.; Jiménez-García, J.D.; Velázquez-Díaz, D.; Cadenas-Sanchez, C.; Isidori, E.; Fossati, C.; Pigozzi, F.; Rum, L.; Norton, C.; Tierney, A.; Äbelkalns, I.; Klempere-Sipjagina, A.; Porozovs, J.; Hannola, H.; Niemisalo, N.; Hokka, L.; Jiménez-Pavón, D.; Vaquero-Cristóbal, R. Sarcopenia, Diet, Physical Activity and Obesity in European Middle-Aged and Older Adults: The LifeAge Study. Nutrients. 2020, 13, 8. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.J.; Lim, Y.H.; Yun, J.M.; Yoon, H.J.; Park, M. Sex- and age-specific effects of energy intake and physical activity on sarcopenia. Sci Rep. 2020, 10, 9822. [Google Scholar] [CrossRef] [PubMed]
- Fukunaga, T.; Mori, S.; Omura, T.; Noda, Y.; Fujita, Y.; Ohsawa, I.; Shigemoto, K. Muscle Fiber Type Specific Alterations of Mitochondrial Respiratory Function and Morphology in Aged Female Mice. Biochem. Biophys. Res. Commun. 2021, 540, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Mankhong, S.; Kim, S.; Moon, S.; Kwak, H.B.; Park, D.H.; Kang, J.H. Experimental Models of Sarcopenia: Bridging Molecular Mechanism and Therapeutic Strategy. Cells. 2020, 9, 1385. [Google Scholar] [CrossRef] [PubMed]
- Shen, S.-H.; Singh, S.P.; Raffaele, M.; Waldman, M.; Hochhauser, E.; Ospino, J.; Arad, M.; Peterson, S.J. Adipocyte-Specific Expression of PGC1α Promotes Adipocyte Browning and Alleviates Obesity-Induced Metabolic Dysfunction in an HO-1-Dependent Fashion. Antioxidants. 2022, 11, 1147. [Google Scholar] [CrossRef] [PubMed]
- Delrieu, L.; Martin, A.; Touillaud, M.; Pérol, O.; Morelle, M.; Febvey-Combes, O.; Freyssenet, D.; Friedenreich, C.; Dufresne, A.; Bachelot, T.; et al. Sarcopenia and Serum Biomarkers of Oxidative Stress after a 6-Month Physical Activity Intervention in Women with Metastatic Breast Cancer: Results from the ABLE Feasibility Trial. Breast Cancer Res. Treat. 2021, 188, 601. [Google Scholar] [CrossRef]
- Luo, J.; Mills, K.; le Cessie, S.; Noordam, R.; van Heemst, D. Ageing, Age-Related Diseases and Oxidative Stress: What to Do Next? Ageing Res. Rev. 2020, 57, 100982. [Google Scholar] [CrossRef] [PubMed]
- Kadoguchi, T.; Shimada, K.; Miyazaki, T.; Kitamura, K.; Kunimoto, M.; Aikawa, T.; Sugita, Y.; Ouchi, S.; Shiozawa, T.; Yokoyama-Nishitani, M.; et al. Promotion of Oxidative Stress Is Associated with Mitochondrial Dysfunction and Muscle Atrophy in Aging Mice. Geriatr. Gerontol. Int. 2020, 20, 78–84. [Google Scholar] [CrossRef]
- Tang, H.; Inoki, K.; Brooks, S.V.; Okazawa, H.; Lee, M.; Wang, J.; Kim, M.; Kennedy, C.L.; Macpherson, P.C.D.; Ji, X.; et al. MTORC1 Underlies Age-related Muscle Fiber Damage and Loss by Inducing Oxidative Stress and Catabolism. Aging Cell. 2019, 18, e12943. [Google Scholar] [CrossRef] [PubMed]
- Erlich, A.T.; Tryon, L.D.; Crilly, M.J.; Memme, J.M.; Moosavi, Z.S.M.; Oliveira, A.N.; Beyfuss, K.; Hood, D.A. Function of specialized regulatory proteins and signaling pathways in exercise-induced muscle mitochondrial biogenesis. Integr. Med. Res. 2016, 5, 187–197. [Google Scholar] [CrossRef] [PubMed]
- Ko, I.G.; Jeong, J.W.; Kim, Y.H.; Jee, Y.S.; Kim, S.E.; Kim, S.H.; Jin, J.J.; Kim, C.J.; Chung, K.J. Aerobic exercise affects myostatin expression in aged rat skeletal muscles: A possibility of antiaging effects of aerobic exercise related with pelvic floor muscle and urethral rhabdosphincter. Int. Neurourol. J. 2014, 18, 77. [Google Scholar] [CrossRef] [PubMed]
- Takeshima, N.; Rogers, M.E.; Islam, M.M.; Yamauchi, T.; Watanabe, E.; Okada, A. Effect of concurrent aerobic and resistance circuit exercise training on fitness in older adults. Eur. J. Appl. Physiol. 2004, 93, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Reginster, J.-Y.Y.; Slomian, J.; Buckinx, F.; Quabron, A.; Dardenne, N.; Bruyère, O.; Locquet, M.; Bruyère, O. Prevalence of sarcopenia: The impact of different diagnostic cut-off limits. J. Musculoskelet. Neuronal Interact. 2014, 14, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Witkowski, S.; Evard, R.; Rickson, J.J.; White, Q.; Sievert, L.L. Physical activity and exercise for hot flashes: trigger or treatment? Menopause. 2023, 30, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.W.; Bass, M.A.; Ting, L.; Brown, B. Influence of yard work and weight training on bone mineral density among older U. S. women. J Women Aging. 2002, 14, 139–48. [Google Scholar] [CrossRef] [PubMed]
- O’Bryan, S.J.; Giuliano, C.; Woessner, M.N.; Vogrin, S.; Smith, C.; Duque, G.; Levinger, I. Progressive Resistance Training for Concomitant Increases in Muscle Strength and Bone Mineral Density in Older Adults: A Systematic Review and Meta-Analysis. Sports Med. 2022, 52, 1939–1960. [Google Scholar] [CrossRef]
- Kim, S.W.; Park, H.Y.; Jung, W.S.; Lim, K. Effects of Twenty-Four Weeks of Resistance Exercise Training on Body Composition, Bone Mineral Density, Functional Fitness and Isokinetic Muscle Strength in Obese Older Women: A Randomized Controlled Trial. Int J Environ Res Public Health. 2022, 19, 14554. [Google Scholar] [CrossRef] [PubMed]
- Maréchal, R.; Ghachem, A.; Prud’homme, D.; Rabasa-Lhoret, R.; Dionne, I.J.; Brochu, M. Physical activity energy expenditure and fat-free mass: relationship with metabolic syndrome in overweight or obese postmenopausal women. Appl Physiol Nutr Metab. 2021, 46, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Wasserfurth, P.; Nebl, J.; Schuchardt, J.P.; Müller, M.; Boßlau, T.K.; Krüger, K.; Hahn, A. Effects of Exercise Combined with a Healthy Diet or Calanus finmarchicus Oil Supplementation on Body Composition and Metabolic Markers-A Pilot Study. Nutrients. 2020, 12, 2139. [Google Scholar] [CrossRef] [PubMed]
- El Khoudary, S.R.; Aggarwal, B.; Beckie, T.M.; Hodis, H.N.; Johnson, A.E.; Langer, R.D.; Limacher, M.C.; Manson, J.E.; Stefanick, M.L.; Allison, M.A.; American Heart Association Prevention Science Committee of the Council on Epidemiology and Prevention; and Council on Cardiovascular and Stroke Nursing. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association. Circulation. 2020, 142, e506–e532. [Google Scholar] [CrossRef] [PubMed]
- Giardina, E.G. Heart disease in women. Int J Fertil Womens Med. 2000, 45, 350–7. [Google Scholar] [CrossRef] [PubMed]
- LaMonte, M.J.; Manson, J.E.; Chomistek, A.K.; Larson, J.C.; Lewis, C.E.; Bea, J.W.; Johnson, K.C.; Li, W.; Klein, L.; LaCroix, A.Z.; Stefanick, M.L.; Wactawski-Wende, J.; Eaton, C.B. Physical Activity and Incidence of Heart Failure in Postmenopausal Women. JACC Heart Fail. 2018, 6, 983–995. [Google Scholar] [CrossRef]
- Trachsel, L.D.; Boidin, M.; Henri, C.; Fortier, A.; Lalongé, J.; Juneau, M.; Nigam, A.; Gayda, M. Women and men with coronary heart disease respond similarly to different aerobic exercise training modalities: a pooled analysis of prospective randomized trials. Appl Physiol Nutr Metab. 2021, 46, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Glassberg, H.; Balady, G.J. Exercise and heart disease in women: why, how, and how much? Cardiol Rev. 1999, 7, 301–8. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, N.T.; Mielke, M.M. Sex Differences in Alzheimer’s Disease. Neurol Clin. 2023, 41, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Scheyer, O.; Rahman, A.; Hristov, H.; Berkowitz, C.; Isaacson, R.S.; Diaz Brinton, R.; Mosconi, L. Female Sex and Alzheimer’s Risk: The Menopause Connection. J Prev Alzheimers Dis. 2018, 5, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Faravelli, C.; Alessandra Scarpato, M.; Castellini, G.; Lo Sauro, C. Gender differences in depression and anxiety: the role of age. Psychiatry Res. 2013, 210, 1301–3. [Google Scholar] [CrossRef] [PubMed]
- Aibar-Almazán, A.; Hita-Contreras, F.; Cruz-Díaz, D.; de la Torre-Cruz, M.; Jiménez-García, J.D.; Martínez-Amat, A. Effects of Pilates training on sleep quality, anxiety, depression and fatigue in postmenopausal women: A randomized controlled trial. Maturitas. 2019, 124, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Cunha, P.M.; Werneck, A.O.; Nunes, J.P.; Stubbs, B.; Schuch, F.B.; Kunevaliki, G.; Zou, L.; Cyrino, E.S. Resistance training reduces depressive and anxiety symptoms in older women: a pilot study. Aging Ment Health. 2022, 26, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Haskell, W.L.; Taylor, C.B.; Kraemer, H.C.; DeBusk, R.F. Group- vs home-based exercise training in healthy older men and women. A community-based clinical trial. JAMA. 1991, 266, 1535–42. [Google Scholar] [CrossRef] [PubMed]
- Eyigor, S.; Karapolat, H.; Durmaz, B. Effects of a group-based exercise program on the physical performance, muscle strength and quality of life in older women. Arch Gerontol Geriatr. 2007, 45, 259–71. [Google Scholar] [CrossRef] [PubMed]
- Gulli, G.; Cevese, A.; Cappelletto, P.; Gasparini, G.; Schena, F. Moderate aerobic training improves autonomic cardiovascular control in older women. Clin Auton Res. 2003, 13, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Arnold, C.M.; Dal Bello-Haas, V.P.; Farthing, J.P.; Crockett, K.L.; Haver, C.R.; Johnston, G.; Basran, J. Falls and Wrist Fracture: Relationship to Women’s Functional Status after Age 50. Can J Aging. 2016, 35, 361–71. [Google Scholar] [CrossRef] [PubMed]
- Pinkas, J.; Gujski, M.; Humeniuk, E.; Raczkiewicz, D.; Bejga, P.; Owoc, A.; Bojar, I. State of Health and Quality of Life of Women at Advanced Age. Med Sci Monit. 2016, 22, 3095–105. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, L.; Leng, X.; La Monte, M.J.; Tindle, H.A.; Cochrane, B.B.; Shumaker, S.A. Functional Independence in Late-Life: Maintaining Physical Functioning in Older Adulthood Predicts Daily Life Function after Age 80. J Gerontol A Biol Sci Med Sci. 2016, 71 (Suppl 1), S79–86. [Google Scholar] [CrossRef] [PubMed]
- Parra-Rizo, M.A.; Sanchís-Soler, G. Physical Activity and the Improvement of Autonomy, Functional Ability, Subjective Health, and Social Relationships in Women over the Age of 60. Int J Environ Res Public Health. 2021, 18, 6926. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Ahn, N.; Park, J.; Kim, K. 12-Week Exercise Training of Knee Joint and Squat Movement Improves Gait Ability in Older Women. Int J Environ Res Public Health. 2021, 18, 1515. [Google Scholar] [CrossRef] [PubMed]
- Lauche, R.; Schumann, D.; Sibbritt, D.; Adams, J.; Cramer, H. Associations between yoga practice and joint problems: a cross-sectional survey among 9151 Australian women. Rheumatol Int. 2017, 37, 1145–1148. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, L.C.; Oliveira, R.G.; Pires-Oliveira, D.A. Comparison between static stretching and the Pilates method on the flexibility of older women. J Bodyw Mov Ther. 2016, 20, 800–806. [Google Scholar] [CrossRef] [PubMed]
- de Resende-Neto, A.G.; do Nascimento, M.A.; de Sá, C.A.; Ribeiro, A.S.; Desantana, J.M.; da Silva-Grigoletto, M.E. Comparison between functional and traditional training exercises on joint mobility, determinants of walking and muscle strength in older women. J Sports Med Phys Fitness. 2019, 59, 1659–1668. [Google Scholar] [CrossRef] [PubMed]
- Dunsky, A.; Netz, Y. Physical activity and sport in advanced age: is it risky? a summary of data from articles published between 2000-2009. Curr Aging Sci. 2012, 5, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Kirby, J.B.; Kluge, M.A. For the Love of the Game: An Exploration of the Experiences and Psychosocial Development of Women 70 Years of Age and Older Who Play Volleyball. J Aging Phys Act. 2022, 30, 445–454. [Google Scholar] [CrossRef] [PubMed]
- Deck, S.; Doherty, A.; Hall, C.; Schneider, A.; Patil, S.; Belfry, G. “Older, Faster, Stronger”: The Multiple Benefits of Masters Sport Participation. J Aging Phys Act. 2023, 31, 786–797. [Google Scholar] [CrossRef] [PubMed]
- Huebner, M.; Meltzer, D.; Ma, W.; Arrow, H. The Masters athlete in Olympic weightlifting: Training, lifestyle, health challenges, and gender differences. PLoS One. 2020, 15, e0243652. [Google Scholar] [CrossRef] [PubMed]
- Kolt, G.S.; Driver, R.P.; Giles, L.C. Why older Australians participate in exercise and sport. J Aging Phys Act. 2004, 12, 185–98. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Biological aging. (a) Different factors influencing aging [4]; (b) Differences in aging between men and women [5].
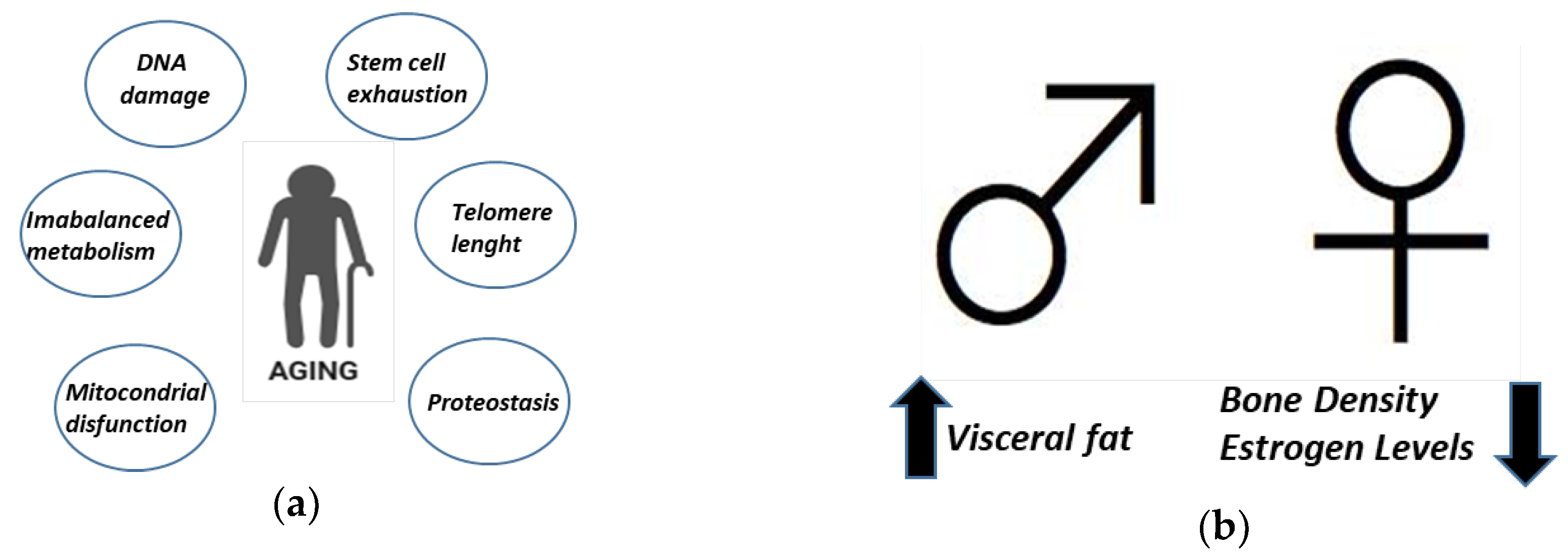
Figure 3.
Exercise as hormetic stressor and its beneficial effects on aging.
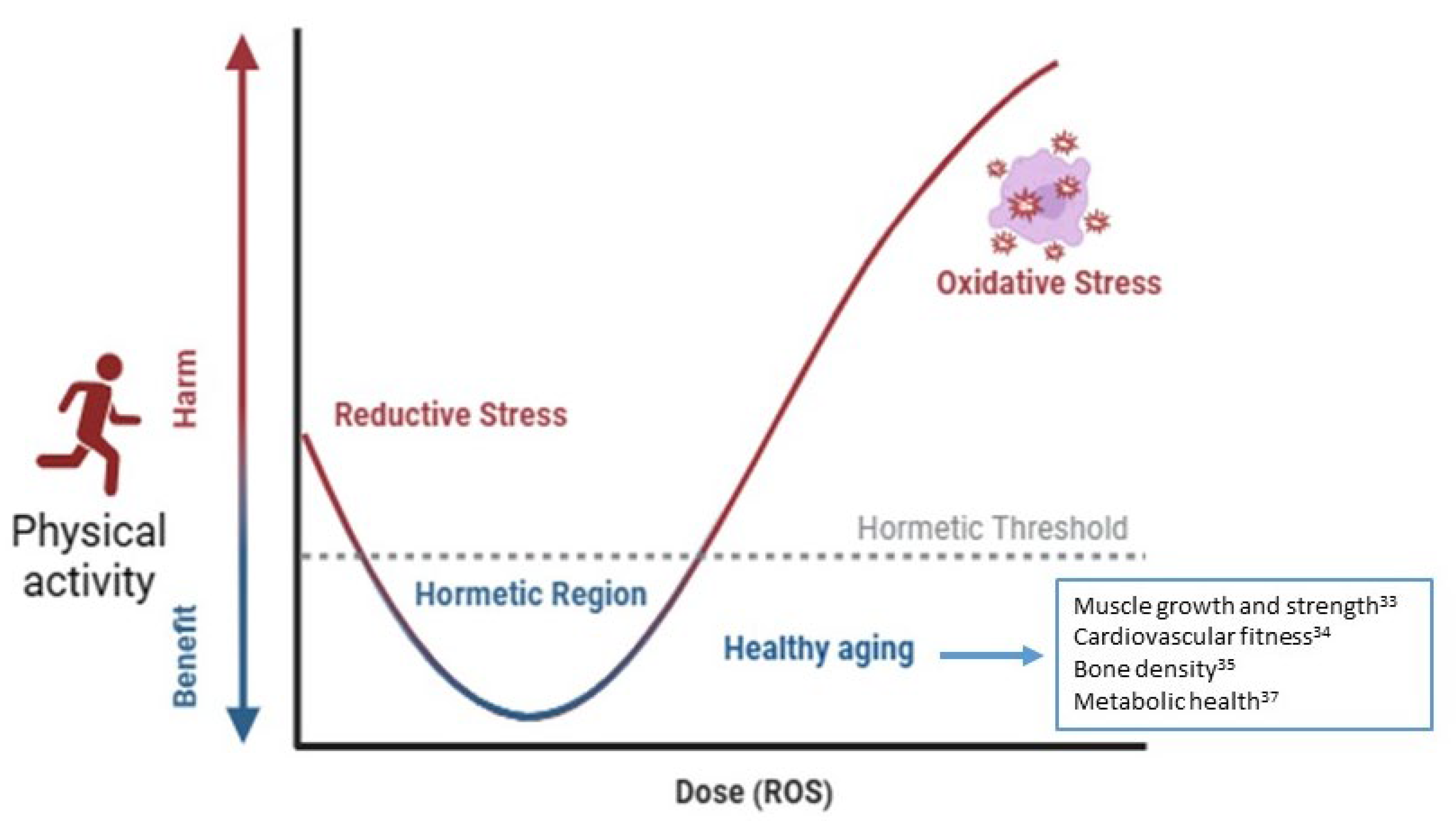
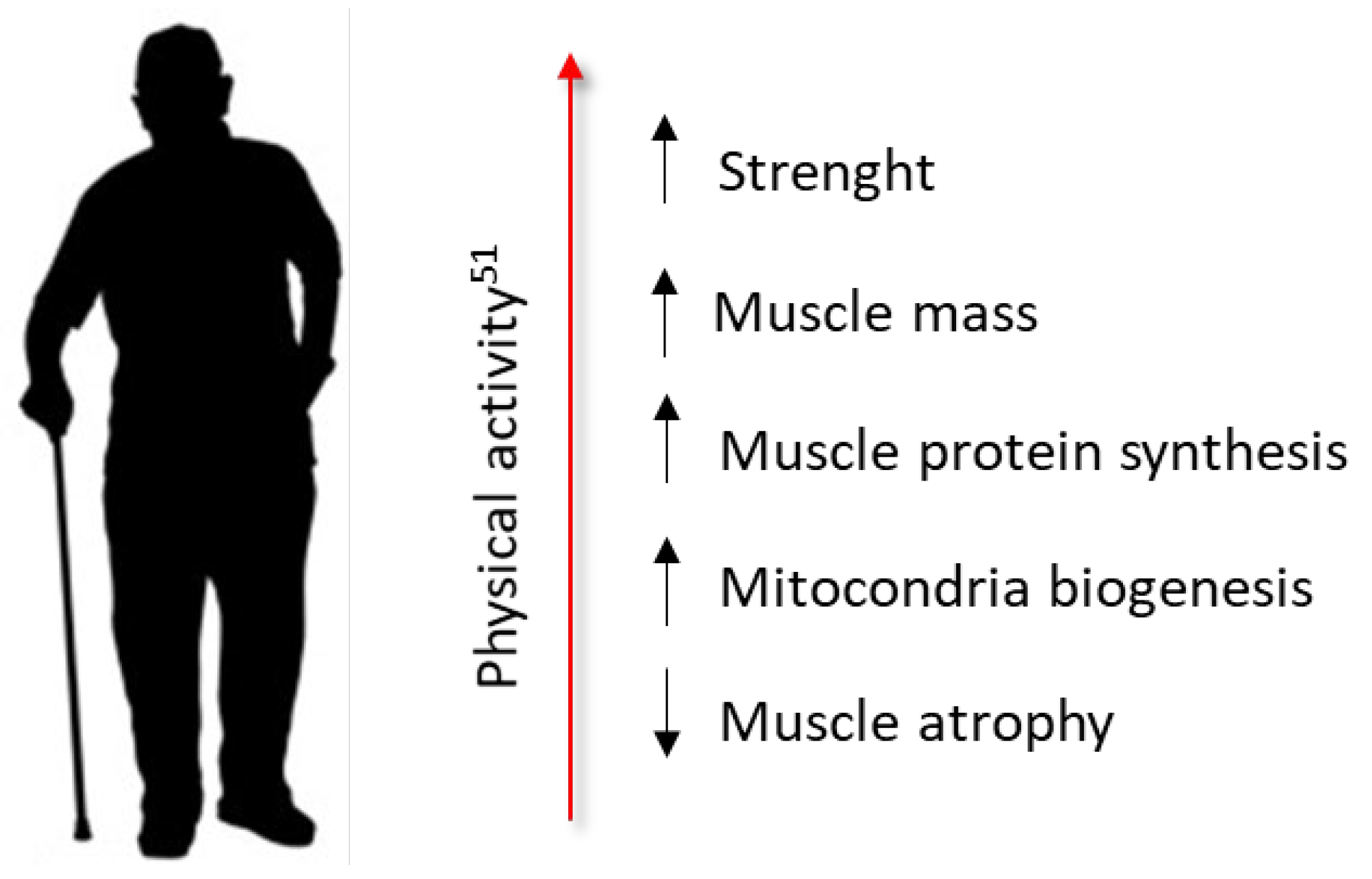
Figure 5.
Aging in females and positive influence of physical activity [74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100].

Figure 6.
Effects of participation in sports on physical fitness, strength, flexibility, and cardiovascular health in aged women.
Figure 6.
Effects of participation in sports on physical fitness, strength, flexibility, and cardiovascular health in aged women.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



