
Submitted:
03 April 2024
Posted:
04 April 2024
You are already at the latest version
Abstract
Background and Objectives: High job strain is worsening the outcome in coronary artery disease, CAD. Severe dissatisfaction on workplace, imbalance between high demands , and low rewards, are affecting the quality of life, and diminishing the duration of life, especially in CAD patients. Our study included two samples : CAD patients (experimental group), and without CAD patients, but with traditional risk factors (control group). The main objective of the study was the role played by high sensitivity C reactive protein, hs CRP, and microalbuminuria, as mediators of job strain and CAD relationship. Secondary objectives were the following: identification of the most vulnerable patients( with significant job strain) and intervention towards this category, for cardiovascular events prevention (primary or secondary). Materials and Methods: The utilized methods were the following : clinical exam; electrocardiogram; echocardiogram; non contrast enhanced computed chest tomography; laboratory findings ( lipid profile, glycemia, hs CRP, microalbuminuria); type D scale, DS 14; depression questionnaire, PHQ-9; and satisfaction with work scale, SWWS. Results: The highest values for hs CRP and microalbuminuria were noticed in patients with the lowest Likert score, for both samples CAD, and without CAD patients. The highest job strain was noticed in females. More than half of CAD patients ,with low Likert scores, revealed myocardial infarction. Conclusions: Microalbuminuria and hs CRP were statistical significant in the study as intercessors, in job strain and CAD relationship. The most vulnerable patients for vascular events were females, in both groups : CAD and “CAD waiting desk”. In CAD sample, the vascular vulnerability was also increased by high job strain.
Keywords:
coronary artery disease
; cardiovascular risk
; job strain
; high sensitivity C reactive protein
; microalbuminuria
1. Introduction
Coronary artery disease, CAD, has an increased prevalence, despite the progresses achieved by medical, interventional, surgical, angiogenesis therapies. According to World Health Organization 2022, 29% of deaths are provoked by this disease. Much more, the onset of this illness can be around 3rd or 4th decade, in socially active persons. 80% of young patients have traditional risk factors, like elderly patients [1,2]; the other 20% of young patients have congenital malformations of coronary arteries; inherited or aquired thrombophilia; spasm of angiographic normal coronaries [3] or are drug abusers (cocaine or amphetamines). Gender and urbanization disparities are noticed in CAD patients : women from rural areas, in United States, register higher mortality rate due to CAD than men [4]. All these factors, traditionals or particulars, are important for CAD promotion and outcome. During last decade, another term is discussed as a major determinant for this illness: job strain. Stressful events repeated on work place; high work demands; short periods for relaxation, during the day or the year, are provoking job strain. The perception of this stress is different from person to person. Mindset towards job strain depends from a lot of factors: emotional intelligence, education, personality type. Type D personality was defined by Denolet in 2000 [5] as an association between negative emotions (repressed anger) and social inhibition (difficulty in expression of personal opinions and thoughts). He named this type of personality ”distressed” and revealed that these persons had a higher risk for CAD, compared with non-D personality subjects. Denolet noticed that there were no gender differences. In 2003, Pederson and Denollet, proved that type D personality had a higher risk of cardiovascular morbidity and mortality, independent by traditional cardiovascular risk factors [6]. They explained these results through vascular overreacting and increased proinflammatory cytokines, in type D persons. In their study, the patients with CAD and type D personality, had a poor life quality( social and personal) and poor answers to medical/interventional/surgical, treatments, comparative with non-D persons. Personality type is essential for social insertion and perception of job strain. Repressed anger (type D) is more distructive for a CAD patient than expressed anger [7]. This type of angers -repressed and expressed- can occur, during job strain; psychotherapy can manage these harmful traits of personality. Steptoe and Malloy affirmed that psychotherapy in CAD patients, had efficient and powerfull effects, as cardiovascular medication [8]. Dahlen et al. defined in 2022, the model of “Big five personality” important in CAD—extraversion, amiability, curiosity, conscientiousness and neuroticism [9]. The Dahlen study included 484,425 participants, with different ethnicity, race ; the study lasted for 7 years. The authors discovered the following interesting results: high scores for neuroticism and extraversion, conducted to a high risk for myocardial infarction; high score for conscientiousness and curiosity, had a protective cardiovascular effect.Also the females revealed interesting results in Dahlen study: those with poor echonomical status and neuroticism,recorded high risk of mortality due to myocardial infarction; if females with important neuroticism, had a high income, this social-echonomical status protected them against myocardial infarction. We can conclude from this large study that between personality traits and CAD is a two-way street, each of them can be “cause” for the other and also “effect”. Job strain alters life quality, among patients with acute coronary syndrome [10] and chronic CAD [11]. Gender disparities, among job strain and CAD incidence/outcome, were noticed in the last years. Wang et al. revealed, in 2021, that women with high job strain, had a 21% increased risk for CAD, compared with women without job strain [12]. Lavigne-Robichaud et al. noticed in 2023, that males with job strain had a 49% increased risk for CAD. Early psychological interventions can reduce CAD burden. The results for females were inconclusive in this study [13]. Modern life is associated with new challenges on work place. Specific questionnaires, can be applied for the employee, at the beginning and during his enrolment. These psychological questionnaires are useful for discovering mental and physical disturbances, induced by job strain. Questionnaires are following job satisfaction and depression. Employees can be help for a better life quality and work effectiveness. Laboratory findings provide accurate assessment of cardiovascular risk. Hs CRP, and microalbuminuria are two accessible and accurate markers for cardiovascular risk. HsCRP, is secreted by the liver in response to inflammatory cytokines, like interleukines, tumor necrosis factor TNF, transforming growth factor, TGF [14]. These cytokines are promoting atherosclerosis. If hs CRP ranges are increased, inflammatory cytokines are increased, and also cardiovascular risk is increased. Much more, hs CRP stimulates the assimilation of low density lipoprotein cholesterol, LDL cholesterol, by macrophages, and diminish nitric oxide production by endothelium. These actions mean the beginning of atherosclerotic plaque [15]. Hs CRP is a reflection of inflammatory status inside atherosclerosis, and also it is an atherosclerosis promoter. HsCRP is a real cardiovascular risk factor, similar to LDL -cholesterol [16]. Hs CRP is considered a ”residual cardiovascular risk factor”. This concept emphasize the importance of hs CRP in promoting and developing atherosclerosis [16,17]. Microalbuminuria is a marker of extensive endothelial dysfunction and an atherosclerotic risk factor, especially in diabetes mellitus and arterial hypertension [18]. Subjects with high grade albuminuria (≥ 25 mg/24 hours) have 50% higher cardiovascular risk than subjects with low grade albuminuria ( < 25 mg/24 hours). These results were collected on a 5- years- study, which included 9580 particiipants, aged ≥40 years, free from cardiovascular disease. The authors concluded that albuminuria-to-creatinine ratio is an important parameter for cardiovascular risk prediction and prevention of cardiovascular events [19]. Our research has the following objectives, illustrated on Table 1 ( objectives are addressed to CAD patients sample and patients without CAD sample, but with cardiovascular risk factors: smoking, obesity, diabetes mellitus, arterial hypertension).
2. Materials and Methods
2.1. Study Design
The research was a descriptive cross-sectional study, conducted between Octomber 2023 and February 2024.The study involved 210 participants, recruited via Promedicanon Cardiology Office. The participants were living and working in 7 counties from Romania: Iasi, Neamt, Botosani, Suceava, Bacau, Galati,Vrancea.
2.2. Research Samples
The participants formed 2 distinct samples: one experimental sample, with CAD( angina pectoris/silent myocardial ischemia/chronic myocardial infarction) had 105 participants; the second sample( control sample) without CAD, had 105 participants, with traditional cardiovascular risk factors (smoking/obesity/hypercholesterolemia/arterial hypertension/diabetes mellitus). Any participant could discontinue at any point, during the research. The data collection ensured patients anonymity. Demographic characteristics of the patients were age, gender, rural/urban environement; also we specified education level: elementary school, secondary(high) school or higher education.The inclusion criteria for both samples are summarized in Table 2.
The exclusion criteria are illustrated in Table 3.
2.3. Methods
We utilized the following methods:
1.complete clinical examination
2. electrocardiogram, made with Heart Screen 80 G
3. transthoracic echocardiogram, made with Fukuda Denshi 850 XTD
4. non contrast enhanced computed chest tomography
5.lipid profile, glycemia, hs CRP, and microalbuminuria, determined by chemistry laboratories
6. DS 14 questionnaire for type D personality diagnosis[20]. DS 14 is a 14-item questionnaire, seven items refer to negative affectivity, and seven items refer to social inhibition; people who score 10 points or more on both dimensions are classified as type D.
7. PHQ-9 questionnaire [21,22]. PHQ-9 is a psychological tool for depression assessment and has nine specific questions; the depression is considered mild if PHQ-9 score is 5-9 and these patients have to repeat the test after 1 month. The same PHQ -9 score after 6 months requires counseling. Moderate( PHQ—9 score =10-14) and moderately severe (PHQ -9 score =15-19) depression, requires counseling and medication. Severe depression (PHQ-9 score) requires immediate and active psychiatric intervention.
8. SWWS questionnaire, according to Blais et al. [23]. SWWS is a psychological questionnaire with 5 items as affirmations. The affirmations are illustrated on Table 4:
These affirmations are receiving a score from 1 to 5. The scores from 1 to 5 compose Likert scale( the worst is 1, with severe dissatisfaction on work place, and the best is 5, with great satisfaction on work place). These scores are figured in Table 5:
Life style changes (diet,physical activity, smoking cessation, weight control) medication, stenting, coronary aortic by pass grafting, were the tools for cardiovascular events prevention (primary or secondary prevention). Betablockers, angiotensine converting enzyme inhibitors, antiplatelet agents, statins, calcium chanel blockers, were the medications for CAD patients. Fixed combination, like angiotensine converting enzyme inhibitors plus diuretic/angiotensine converting enzyme inhibitors plus calcium channel blocker/angiotensine converting enzyme inhibitors plus diuretic and calcium channel blocker, were received by hypertensive patients. For diabetes mellitus, our patients received biguanides/insulin/exenatide/dapagliflozin.
The study was approved by Ethical Comitee for Research, 351/9 October 2023, from“Gr. T. Popa” University of Medicine and Pharmacy, Iasi, Romania, www.umfiasi.ro.
2.4. Statistical Analysis
Characteristics of patients like age, total cholesterol, LDL cholesterol, hs CRP, microalbuminuria, were evaluated via median and interquartile range IQR; the other characteristics, like gender, education, rural/urban, smoking, obesity, arterial hypertension, were evaluated via numbers and percentage. For continuous variables, like age, total cholesterol, LDL cholesterol, hs CRP, and microalbuminuria, statistical analysis was made by Mann Whitney U test (p-value) and for categorical data, like sex, education, rural/urban, smoking, obesity, arterial hypertension, and diabetes mellitus, statistical analysis was performed by Pearson chi square (p-value). We had 5 categories of patients, according to their Likert score (from 1 to 5). For each Likert score, we wanted to find out the connection between job strain, on the one hand, and continuous variables, as age; for each Likert score, we also noticed the connection between job strain, on the other hand, and categorical data as sex, and level of education. Hs CRP, and microalbuminuria were the mediators for this connection. Statistical analysis in Likert score categories was performed by Mann Whitney U test, for continuous variables (p-value) and by Pearson chi square for categorical data(p-value).
3. Results
3.1. Characteristics of the Samples(CAD Patients Sample and without CAD Patients Sample)
Median age of CAD patients was 69 years. Patients without CAD, were younger, with a median age at 52 years. Age had statistical consistency (IQR) and statistical significance (p-value = 0.01) for both samples. In CAD sample, the numbers of females were almost equal with males, 55.2%. The sample without CAD, had a predominance of females, 70.5%. P-value for gender had statistical significance, p = 0.03. About education, we noticed a predominance of high school level for both samples. P-value for education had statistical significance, p = 0.04. Both samples had the predominance of rural patients. P-value was statistically significant, p = 0.032, in rural/urban environement. The variability IQR for total cholesterol was very high for both samples (not sufficient for statistical consistency). Also, p -value for total cholesterol hadn’t statistical significance, p = 0.16. The situation was different in LDL-cholesterol, which had a p-value = 0.03 ( statistical significance). Median value for hs CRP was higher in CAD sample, comparative with the sample without CAD. P-value for hs CRP had a very high statistical significance, p= 0.002. Hs CRP had excellent statistical consistency for both samples (very low values of IQR). Microalbuminuria had good statistical consistency (low values of IQR), and very high statistical significance, p = 0.003. Among traditional cardiovascular risk factors, obesity and arterial hypertension had the highest percentage, for both samples. P-value for obesity had statistical significance, p = 0.04, as well as p-value for hypertension, p = 0.03. Smoking had a lower prevalence than obesity and hypertension, but p-value for smoking had statistical significance, p = 0.032. P-value for diabetes melitus had the best statistical significance, p = 0.02. All traditional cardiovascular risk factor had significant p-values in the study. Table 6 ilustrates these results.
3.2. Detailed Results
3.2.1. Complete clinical examination
Anamnesis revealed clinical description of angina pectoris in 42 patients with chronic myocardial infarction, and in 29 patients with angina pectoris (80% of CAD patients). Atrial fibrillation was diagnosed in 11% of CAD patients, and heart failure in 27% of 105 CAD patients.
3.2.2. Electrocardiogram
CAD patients
Rest electrocardiogram revealed specific alterations for all 52 patients with chronic myocardial infarction, 49% of CAD patients (Q waves, ST segment depression/elevation, negative T waves); for all 17 patients with silent myocardial ischemia, 16% of CAD patients (ST segment depression and/or negative T waves), and for 27 of 29 patients with angina pectoris, 25% of CAD patients (ST segment depression and/or negative T waves). Figure 1 ilustrates an example from the study, with chronic inferior and anterior myocardial infarctions.
Exercise test was necessary for 9 patients ( 8.5% of CAD patients) with clinical description of angina pectoris, and normal rest electrocardiogram. Left ventricular hypertrophy was noticed in 21, 20% of CAD patients,who also had arterial hypertension. Atrial fibrillation was confirmed through electrocardiogram in 115 of CAD patients.
Patients without CAD
Left ventricular hypertrophy was noticed in 26 patients, 24.7% of patients without CAD.
3.2.2. Echocardiogram
Specific alterations of segments and ventricular walls motility were noticed in CAD patients: hypokinesia 32%, akinesia 26%, and dyskinesia 22%. Normokinesia was noticed in 20% of CAD patients. Figure 2 ilustrates an example of akinesia from our study.
Figure 3 ilustrates an example, from our study, with chronic septal myocardial infarction and its expression on echocardiography(diminished transversal dimension in myocardial necrosis area).
Echocardiogram revealed preserved ejection fraction heart failure in 23% of 105 patients without CAD (they had arterial hypertension and diastolic dysfunction on echocardiogram) and in 28% of 105 patients with CAD. Reduced ejection fraction heart failure was noticed in 36% of 105 CAD patients.
3.2.3. Non Contrast Enhanced Computed Chest Tomography, NCECCT
We calculated Agatston calcium coronary scoring, ACCS, for all CAD patients [24].

Table 7.
The severity of coronary artery calcification [24].
Table 7.
The severity of coronary artery calcification [24].
| Scoring | Interpretation |
| 0 | no measurable calcified plaque |
| 1-10 | Minimal |
| 11-100 | Mild |
| 100-400 | Moderate |
| > 400 | Extensive |
An example of NCECCT from our study, with extensive calcification, ACCS =1513, can be seen in Figure 4.
Severity of coronary arteries calcification, in our CAD patients, was the following: 56.1% extensive, 25.7% moderate, 5.7% mild and 12.3% minimal.
3.2.4. Biochemistry Results
They are illustrated in Table 6, page 6 (total and LDL cholesterol, hs CRP, microalbuminuria).
3.2.5. DS-14 Results
Type D personality was noticed in 72% of CAD patients. The sample without CAD registered a lower prevalence of type D personality ( 34%).
3.2.6. PHQ-9 Results
CAD patients and depression
More than half CAD patients with Likert score 1 and Likert score 2, with sever dissatisfaction on workplace, had moderately severe or severe depression (grey and yellow columns in Figure 5). Much more, all the CAD Likert score 1 and 2 patients, had depression. Severe dissatisfaction on workplace was accompanied by depression in CAD patients. CAD patients with Likert score 4 and 5( with satisfaction on workplace) had mild depression( blue columns in Figure 5) and moderate depression (orange columns in Figure 5). None of CAD patients with Likert score 4 and 5, had moderately severe or severe depression. Satisfaction on workplace was protective against moderately severe and severedepression, in CAD patients. All these results can be seen in Figure 5.
Patients without CAD and depression
The sample without CAD had a similar situation as CAD patients, for depression prevalence and severity. Moderately severe and severe depression (grey and yellow columns in Figure 6) affected more than half without CAD patients, with severe dissatisfaction on workplace ( Likert 1 and 2, at SWWS test). All the patients with Likert 1 and 2, had depression. The patients with satisfaction on workplace, had mild depression (blue columns in Figure 6) or moderate depression (orange columns in Figure 6). Only one patient with Likert 5 suffered by moderately severe depression. All these results can be noticed in Figure 6.
3.2.7. SWWS Results
According to SWWS questionnaire, we had 5 groups of patients. For each Likert score, we compared the following continuous variables: age, hs CRP, microalbuminuria,
and the following categorical data: sex, and education level. The comparison was between CAD patients with a Likert score, and the patients without CAD, with the same Likert score. CAD patients were older than without CAD patients, in Likert 1. P-value for age in Likert 1 patients had a very high statistical significance, p = 0.007. There was a predominance of females, with Likert 1, for both samples. P-value for gender was statistical significant, p = 0.03. Almost half of the CAD patients and Likert 1, had high school education ; only a few of CAD patients and Likert 1, had higher education. The percentages were different for patients without CAD, and Likert 1: the majority had high school education, almost 1/3 had higher education and only a few, had elementary school education. P-value had statistical significance for each level of education, but the most significant value, was recorded in the group with elementary school education, p = 0.03. hs CRP and microalbuminuria, in Likert 1, had statistical consistency(IQR) and statistical significance (P-value), for CAD and without CAD patients. Table 8 ilustrates these results.
For Likert score 2 (“partially disagree”), CAD patients were older than without CAD patients. P-value for age had statistical significance, p = 0.008, in Likert score 2 patients. In CAD sample, and Likert score 2, females and males numbers were comparable; in sample without CAD, and Likert score 2, the females had a higher percentage than males. P-value for gender had statistical significance, p = 0.032. More than half of CAD patients, and Likert score 2, had high school education; the percentage of elementary school education, and Likert score 2, was lower than in Likert 1. Patients without CAD and Likert score 2, had a majority with high school education. P-value was significant for all levels of education, in Likert score 2 patients, but the most relevant was p-value for elementary school education, p = 0.025. Continuous variables, like hs CRP and microalbuminuria, had significant p-values in Likert score 2 patients. Table 9 presents these results.
In Likert score 3 (“almost agree”), CAD patients were older than patients without CAD. P-value for age was very significant in Likert 3, p = 0.004. The patients with CAD, had equal percenttages for females and males; in sample without CAD, females were the majority, in Likert score 3. P-value for gender, in Likert score 3, had statistical significance, p = 0.04. Education level revealed the predominance of high school education in CAD patients. The patients without CAD had also a predominance of high school education. P-value was significant for each level of education, but the most significant p-value, in Likert score 3, was revealed by the patients with higher education, p = 0.036. The situation for hs CRP and microalbuminuria was as same as in Likert score 1 and 2. These results are ilustrated in Table 10.
The highest median value for age was noticed in CAD patients, with Likert score 4 (71 years). P-value for age in Likert score 4 had a high statistical significance, p = 0.009. Males were predominant in CAD sample. Females were predominant in sample without CAD. P-value for gender in Likert score 4 had statistical significance, p = 0.03. Almost half of the CAD patients with Likert score 4, had higher education. More than half of the patients without CAD and Likert score 4, had high school education. The most significant p-value for education in Likert score 4 sample, was registered for higher education, p = 0.024. Microalbuminuria and hs CRP had similar statistical results in Likert score 4, as in previous Likert samples. Table 11 summarizes these results.
Likert 5 group revealed close median ages in CAD patients, and without CAD patients. In previous Likert groups (scale 1, 2,3, 4) the difference between median age in CAD and without CAD was higher than in Likert 5 sample. P-value for age in Likert score 5 had a very high statistical significance, p = 0.008. Females had equal numbers with males, both for CAD patients and patients without CAD. P-value for gender, in Likert score 5, had statistical significance, p = 0.04. Half of the CAD patients, and half of patients without CAD, in Likert score 5, had high school education. The most significant p-value for education in Likert score 5 was obtained for higher education, p = 0.033. Endothelial dysfunction markers revealed the same results in Likert score 5, as in Likert scores 1, 2, 3, 4. All these results are summarized in Table 12.
3.2.8. The study Objectives
First study objective
We achieved the first objective of our study: the relationship between job strain and outcome of CAD patients, and without CAD patients. Significant job strain (low Likert scores) was identified especially in CAD patients; their outcome would be unfavorable if active interventions weren’t applied ; diminished job strain and satisfaction on workplace (high Likert scores) were noticed especially in patients without CAD. Figure 7 ilustrates these results: Likert scores 1 and 2, at SWWS questionnaire, were common for CAD patients; Likert score 4 at SWWS questionnaire was common for patients without CAD.
Second study objective
The second objective of our study was to find out the role of hs CRP, and microalbuminuria, as mediators in the relationship between job strain, and outcome of CAD, and without CAD patients. A hs CRP ≥ 0.3 mg/dl is associated with high cardiovascular risk, as well as a microalbuminuria ≥ 25 mg/24 hours.Figure 8 ilustrates the reverse correlation between hsCRP median value and Likert score. The highest values for hsCRP were recorded for the lowest Likert score, in CAD and without CAD patients.
Figure 9 illustrates the reverse correlation between microalbuminuria and Likert score. The lowest scores for job satisfaction were associated with the highest value for microalbuminuria in CAD, and without CAD patients.
The third study objective
The third objective of our study was the identification of the most vulnerable CAD patients: Likert scores 1 and 2 (severe dissatisfaction on work place). More than half of CAD patients with Likert 1 and 2 were diagnosed with chronic myocardial infarction. Lower prevalence of myocardial infarction was noticed in CAD patients with job satisfaction, Likert 3, 4, 5. These results are illustrated in Figure 10.
The fourth study objective
The fourth objective of our study was the implementation of active interventions. Life style changes; medication; stenting; coronary aortic by pass grafting, CABG, were the tools for CAD patients. Medication was administered for all 3 categories of CAD patients. The other interventions were applied as can be seen in Figure 11.
All the patients without CAD, received medical advices, about physical activity and diet; weight control and smoking cessation were recommended in selected patients, who required these life style changes; CAD and without CAD patients, with arterial hyperten- sion/diabetes melitus received medication. These results are ilustrated in Figure 12.
Psychoterapy and anxiolytics were addressed for CAD and without CAD patients, with PHQ -9 above 10: moderate, moderately severe and severe depression.
Discussion
4.1. Age
The predominance of elderly patients in CAD sample was due to a better compliance of geriatrics, than middle age or young patients. P-value for age had a statistical significance in the study, p = 0.01, better than p-values for gender, education, rural/urban environement. In our country, elderly patients are retired, they don’t have job strain, and they learned to take care about their health. Middle age and young patients are usually coming to the cardiologist in advanced stages of CAD, in Romania. Much more, middle age and young patients, are recording a premature cardiovascular mortality, because the majority of them have 2 or 3 jobs, they don’t have time for relaxation and they considere that regular check up is not necessary for themselves. Family support and religiosity also contributed to a higher compliance of elderly patients in the study. In our country, religiosity is often practiced by elderly people, especially if they suffere by cardiac diseases. Wantiyah et al. noticed a direct correlation, between religiosity and self efficacy in CAD patients [25]. Family support was presented in our study, because taking care of your parents is a deep-rooted tradition in Romania. The majority of our elderly patients were brought by their family to the cardiologist, and their family was implicated in treatment monitoring. We had a permanent communication via cell phones, not only with our elderly patients, but also with their family. Li et al. observed that elderly CAD patients had angina stabilization, treatment satisfaction, and positive social perceptions, if they benefitted by family support—active implication of family through medical education, internet base mobile terminal monitoring in elderly patients [26]. In our study, mean age for the group without CAD, was around middle age. More explanations are available for this predominance of middle age patients in this group. Firstly, we selected active subjects, with cardiovascular risk factors, to participate in the study. These patients had obesity, diabetes mellitus, arterial hypertension, hypercholesterolemia, or they were smokers. They didn’t have symptoms or evidence for CAD, so they were selected by us, to be without CAD. Secondly, the elderly patients were coming to us, because they already had specific symptoms for CAD. Thirdly, unhealthy social behaviours, like smoking, were more frequent in middle age group, without CAD, than in elderly patients with CAD. Elderly patients, with CAD in their past medical history, and smoking as an unhealthy behaviour, were more compliant in smoking cessation, than middle age patients. And this was happening because the elderly with CAD, had symptoms and/or medical confirmation of a life-threatening disease; middle age patients had no CAD symptoms, so the motivation for smoking cessation was diminished. Much more, smoking is utilized by middle age/young people, as a ‘’necessary” behaviour, for social acceptance, inside work community. This is a social problem, with important consequences towards health. In our study, middle age patients without CAD, combined unhealthy social behaviours with job strain. Kivimaki et al. included a large cohort of patients (102,128) with job strain, and traditional atherosclerotic risk factors; the authors observed that the highest risk for CAD was registered by people who associated job strain with unhealthy life style [27].
4.2. Gender
CAD had similar prevalence in females and males, but in the sample without CAD, females had the majority. These results were signaling us that females have similar cardiovascular risk as males. Much more, on the ‘’CAD waiting desk ‘’, males are exceeded by females. Increased social implication, unhealthy social behaviours, specific mindset, special demands, family care, are overwhelming for females. We had to insist with anamnesis, because females were describing a lot of symptoms connected to their emotional perceptions. In the study, we had to “navigate’’ through females medical informations. We had to find out the true severity of CAD females, or cardiovascular risk stratification for females without CAD. Special attention was addressed to females in the study, as it was required in recent papers. Vogel et al. declared in 2021 that ‘’cardiovascular disease in women remains understudied, under-recognised, underdiagnosed, and undertreated’’. Dr. Vogel and her team formed an international commission with experts in the field; its objectives were the following: to connect the experts, to realize sex-related disparities, and to reduce global cardiovascular morbidity and mortality in women by 2030 [28]. Martinho et al. noticed in 2023 that ‘’females are more than twice as likely to die after a heart attack than men’’[29]. Hosseini and Kaier affirmed that gender disparity is still present in CAD assessment and usually in cardiovascular diseases ”in the era of precision medicine”[30].
4.3. Education
Education level has a relevant impact, influencing patient ‘s attitude towards health. The education situated around middle level (high school) for more than half of our patients, permitted us to build a strong relationship cardiologist—patient. The patients with high school education were more compliant than patients with lower level of education. They understood the utility of life style changes, sustained treatment, and regular follow- up. Income and education level influenced the outcome of CAD patients in a large study addressed to Eastern Europe [31] and Romania is located in this region. Much more, the experts from this study noticed important disparities in mortality rates for CAD patients. North-Eastern Europe had 399.2 CAD deaths per 100,000 inhabitants, and Central-Eastern Europe had 71 CAD deaths per 100,000 inhabitants. Inside the regions of Eastern Europe, different areas and countries, recorded disparities in mortality rates. These CAD mortality rate disparities were explained by income and education level disparities.
4.4. Rural/Urban Environment
The predominance of rural patients in CAD group, and in the group without CAD, could ignite the following discussions. The first explanation for our study is that life style in rural Romanian CAD patients, became similar with urban patients. Rural patients adopted harmful habbits ( western diet, sedentariness, smoking). Secondly, rural inhabitants had a lower access to education, and to healthcare, comparative with urban inhabitants. Thirdly, in our study, rural patients had lower incomes than urban patients. Rural-urban disparities in outcomes of cardiovascular health is due to multiple factors worldwide: economic, educational factors, and healthcare access [32,33].
4.5. LDL-Cholesterol
LDL-cholesterol was an important parameter for cardiovascular risk, in our study,with statistical significance. A large meta-analysis, with 1,055,309 participants, diagnosed with cardiovascular diseases, was published by Yung et al. in 2022 [34]. The authors noticed that LDL cholesterol registrered a hazard ratio HR = 1.21(95% CI,1.09-1.35). Pathological ranges for LDL cholesterol increased cardiovascular mortality rate, in this large population.
4.6. Hs CRP and Microalbuminuria
In our study, hs CRP was the most sensitive parameter, with statistical consistency. P- value for hs CRP was the most significant, between the other characteristics of our patients: age, gender, education, LDL cholesterol, rural/urban environment, and traditional cardiovascular risk factors. Bienstock et al. noticed in 2024, that atherosclerotic plaque progression is strongly correlated with hsCRP level [35]. In our study, microalbuminuria had statistical consistency in CAD patients and in patients without CAD. P-value for microalbuminuria was comparable with p-value for hs CRP. Barzilay et al. noticed in 2024 that albuminuria is an underappreciated risk factor for CAD and other vascular diseases [36]. The authors considered that high risk patients as diabetes mellitus and arterial hypertension, must be screened for albuminuria rates. We considere that these two parameters, hs CRP and microalbuminuria, have great importance in cardiovascular risk stratification. They are affordable, non-invasive and simple.
4.7. Traditional Cardiovascular Risk Factors
Obesity and arterial hypertension were observed in more than half of the patients, among CAD group, with statistical significance. These two traditional cardiovascular factors had also the first place, among patients without CAD. The second place was taken by diabetes mellitus and the third place was taken by smoking- with statistical significance, for CAD and without CAD patients. The diminishing numbers of smokers in our study can be explained by medical education. Our city, Iași, is the second large city from our country, with a prestigious University of Medicine. Many doctors are trained here to educate large population, about cardiovascular risk factors. Life style changes are easier as regarding smoking, in our city and region, and heavier when we discuss about gain control and hypertension. Many doctors are overwhelmed by time pression, multiple tasks, patients requierements. Future direction will include nurses, clinical pharmacists, and nutritionists training, for medical education in cardiovascular risk factors control, as it is sugested by Brown et al. [37].
4.8. Depression
Depression prevalence was higher for the patients with dissatisfaction on workplace in our study. Patients satisfied by their professional achievements registered good mental health. The relationship between depression and job strain was like a circle. It was difficult to establish if affective disorder was previously to dissatisfaction on workplace, or after it. We applied counseling and medication for moderate, moderately severe and severe depression. Patients with mild depression were invited to repeat PHQ—9 test after 6 months, as we can take a decision about depression severity. Strudwick et al. noticed, in a large systematic review, that screening and active interventions are improving mental health of employees [38]. Deady et al. explored the direct relationship between depression and workplace satisfaction [39].
4.9. SWWS Questionnaire Results
SWWS questionnaire permitted us to express the following discussions.
4.9.1. Age
CAD patients with Likert score 4 were the oldest (median 71 years). Likert score 4 means that the patients answered with “agree” for all 5 questions addressed to job satisfaction. These patients presented an emotional flexibility, during their social and work activities; they continuously adapted to job strain, and selected opportunities. Their quality of life was increased, as well as their duration of life. The most significant p-values for age were registered in Likert score 4 and 5 patients, so for the most patients with job satisfaction. The patients without CAD had median ages around 50 years, for all 5 Likert scores.
4.9.2. Gender
The majority of CAD patients with Likert score 4 were males and we explain these results via psychological gender disparities. The males were more satisfied by their job than females, because in our country males are frequently educated to have a decent income, as they must be providers. Much more, the males from our study followed the worldwide rules: even they don’t have the experience and knowledge to advance in a job, they will act to obtain that job. And that job will give them satisfaction. The percentage of males was also significant in without CAD sample and Likert score 4. Females were the majority in Likert score 1, for both CAD patients and without CAD patients. The females were more unsatisfied by their job than males, because they applied to a job interview only if they felt competent in that job. Many females were wasting job opportunities, and they were unsatisfied with their jobs. They didn’t act like males. They were acting when they were prepared, after a long period of training. These gender disparities on work engagement, and career aspirations were similar with the observations of Hartman and Barber [40].
4.9.3. Education
Job satisfaction was influenced by education level in our study. Patients with higher education, registered the most significant p-value in Likert score 4 and 5. Patients with elementary school education, registered the most significant p-value in Likert score 1 and 2. In our study, higher education permitted higher job satisfaction (Likert score 4 and 5); elementary school education, the lowest level of education, was associated to severe job insatisfaction (Likert score 1 and 2).
4. Conclusions
We can conclude that especially elderly people, rather than middle age or young people, were affected by CAD, in our study. As regarding patients without CAD, middle age patients were predominant. Medical education must be enhanced for this category, as prevention is a keyword in modern medicine. We identified more females than males with traditional risk factors, like obesity, smoking, arterial hypertension, diabetes melitus. Our efforts must be concerned especially towards women, with atherosclerotic risk factor, and we have to increase our active interventions. The predominance of rural patients in both groups lead us to the following conclusion- life style in rural CAD patients became similar with urban patients, rural patients adopted harmful habbits( western diet, sedentariness, smoking). Medical education must be addressed especially to countryside communities for primary and secondary CAD prevention. LDL-cholesterol was keeping its position as a major cardiovascular risk factor. Diet and medication were important tools in controlling LDL cholesterol levels. Hs CRP was suggestive for high cardiovascular risk, both in CAD patients and in group without CAD (hsCRP ≥ 0.300 mg/dl). Preventive cardiology must identify and evaluate patients at high cardiovascular risk. Hs CRP can be very usefull for an adequate selection of this category, as its p-value was very significant in our study. Microalbuminuria could be utilized as an excellent endothelial dysfunction marker, like hs CRP, due to its very high statistical significance. Hs CRP was more sensitive than microalbuminuria( different IQR—high consistency for hsCRP and only good consistency for microalbuminuria). Obesity and arterial hypertension were noticed among more than half of study patients. Our efforts would be strongly addressed against weight and arterial hypertension control. That doesn’t mean we could neglect smoking and diabetes melitus, when we discussed to our patients about life style changes. Job strain was higher in females than in males in the study. This affirmation was sustained by females predominance, on the worst score about job satisfaction. Enhanced efforts are necessary in women education: encouraging their skills, sustaining their aspirations, and suporting their achievements. Depression had a direct correlation with job strain. Active interventions were undertaken in all the patients with more than mild depression. Future research directions will include couple satisfaction and its implications in CAD patients outcome.
Author Contributions
All authors have equal contribution as first author.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of “Gr.T.Popa” University of Medicine and Pharmacy, Iasi, Romania, no. 351/9.10.2023; www.umfiasi.ro
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from all the patients to publish this paper.
Acknowledgments
The authors thank the technical support provided by Andreea Beatrice Manea, Handshake Company, San Francisco, California, United States of America and Eduard Moisii, Iasi, Romania.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Aggarwal, A.; Srivastava, S.; Velmurugan, M. Newer perspectives of coronary artery disease in young. World. J. Cardiol. 2016, 8, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.X.; Yang, Z.; Wu, Y.J.; Qiao, S.B.; Yang, Y.J.; Chen, J.L. Factors associated with coronary artery disease in young population (age ≤ 40): Analysis with 217 cases. Chin. Med. Sci. J. 2014, 29, 38–42. [Google Scholar] [CrossRef] [PubMed]
- Klein, L.W. Acute coronary syndromes in young patients with angiographically normal coronary arteries. Am. Heart. J. 2006, 152, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Bossard, M.; Latifi, Y.; Fabbri, M.; Kurman, R.; Brinkert, M.; Wolfrum, M.; Berte, B.; Cuculi, F.; Toggweiler, F.; Kobza, R.; et al. Increasing mortality from premature coronary artery disease in women in the rural United States. JAHA 2020, 9, e–015334. [Google Scholar] [CrossRef] [PubMed]
- Denollet, J. Type D personality. A potential risk factor refined. J. Psychosom. Res. 2000, 49, 256–266. [Google Scholar] [CrossRef]
- Pedersen, S.; Denollet, J. Type D personality, cardiac events and impaired quality of life: A review. Eur. J. Prev. Cardiol. 2003, 10, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Denollet, J.; Gidron, Y.; Vrints, C.; Conraads, V.M. Anger,suppressed anger and risk of adverse events in patients with coronary artery disease. Am. J. Card. 2011, 105, 1555–1560. [Google Scholar] [CrossRef] [PubMed]
- Steptoe, A.; Malloy, G.J. Personality and heart disease. Heart 2007, 93, 783–784. [Google Scholar] [CrossRef] [PubMed]
- Dahlen, A.D.; Miguet, M.; Schioth, H.B.; Rukh, G. The influence of personality on the risk of myocardial infarction in UK Biobank cohort. Sci. Rep. 2022, 12, 6706. [Google Scholar] [CrossRef]
- Wang, L.; Shi, W.; Li, Y.; Ang, Y.; Jing, P.; Zhang, B.; Cao, X.; Loerbroks, A.; Zhang, M. Longitudinal associations of work stress with changes in quality of life among patients after acute coronary syndromes -a hospital based study. IJERPH 2022, 19, 17018. [Google Scholar] [CrossRef]
- Jaskanval, D.S.; Prasad, M.; Mackram, F.E.; Zhang, M.; Widmer, R.J. Association between work related stress and coronary heart disease: A review of prospective studies through the job strain, effort-reward balance and organizational justice models. JAHA 2018, 7, e0008073. [Google Scholar]
- Wang, C.; Le-Scherban, F.; Taylor, J.; Blotcher, E.; Allison, M.; Michael, Y.L. Associations of job strain,stresfull life events and social strain with coronary heart disease in the Women’s health initiative observational study. JAHA 2021, 10, e017780. [Google Scholar] [CrossRef] [PubMed]
- Lavigne-Robichaud, M.; Trudel, X.; Talbot, D.; Milot, A.; Gilbert-Ouimet, M.; Vézina, M.; Laurin, D.; Dionne, C.E.; Pearce, N.; Dagenais, G.R.; et al. Psychosocial Stressors at Work and Coronary Heart Disease Risk in Men and Women: 18-Year Prospective Cohort Study of Combined Exposures. Circ. Cardiovasc. Qual. Outcomes. 2023, 16, e009700. [Google Scholar] [CrossRef] [PubMed]
- Della Corte, V.; Todaro, F.; Cataldi, M.; Tuttolomondo, A. Atherosclerosis and Its Related Laboratory Biomarkers. Int. J. Mol. Sci. 2023, 24, 15546. [Google Scholar] [CrossRef]
- Braig, D.; Nero, T.L.; Koch, H.-G.; Kaiser, B.; Wang, X.; Thiele, J.R.; Morton, C.J.; Zeller, J.; Kiefer, J.; Potempa, L.A. Transitional changes in the CRP structure lead to the exposure of pro-inflammatory binding sites. Nat. Commun. 2017, 8, 14188. [Google Scholar] [CrossRef]
- Zhang, W.; Speiser, J.L.; Ye, F.; Tsai, M.Y.; Cainzos-Achirica, M.; Nasir, K.; Herrington, D.M.; Shapiro, M.D. High-sensitivity C-Reactive Protein Modifies the Cardiovascular Risk of Lipoprotein(a): Multi-Ethnic Study of Atherosclerosis. JACC 2021, 78, 1083–1094. [Google Scholar] [CrossRef] [PubMed]
- Denegri, A.; Boriani, G. High sensitivity C reactive protein (hsCRP)and its implications in cardiovascular outcomes Curr. Farm. Des. 2021, 27, 263–275. [Google Scholar] [CrossRef]
- Naidoo, D.P. The link between microalbuminuria, endothelial dysfunction and cardiovascular disease in diabetes. Cardiovasc. J. S. Afr. 2002, 13, 194–199. [Google Scholar] [PubMed]
- Liu, S.; Niu, J.; Wu, S. Urinary albumin-to-creatinine ratio levels are associated with subclinical atherosclerosis and predict CVD events and all-cause deaths: A prospective analysis. BMJ Open 2021, 11. [Google Scholar] [CrossRef]
- Denollet, J. DS14: Standard assessment of negative affectivity, social inhibition, and Type D personality. Psychosom. Med. 2005, 67, 89–97. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–13. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The Patient Health Questionnaire-2: Validity of a Two-Item Depression Screener. Med. Care. 2003, 41, 1284–1292. [Google Scholar] [CrossRef]
- Blais, M.R.; Lachance, L.; Forget, J.; Richer, S.; Dulude, D.M. L’eschelle de satisfaction globale au travail. In Proceedings of the Annual Congress of the Society Quebecoise for Research in Psychology, Trois Riviers, Quebec, Canada; 1991. [Google Scholar]
- Rumberger, J.A. Using noncontrast cardiac CT and coronary artery calcification measurements for cardiovascular risk assessment and management in asymptomatic adults. Vasc. Health. Risk. Manag. 2010, 6, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Wantiyah, W.; Rivani, F.R.P.; Hakam, M. The correlation between religiosity and self-efficacy in patients with coronary heart disease. Belitung Nurs J. 2020, 6. [Google Scholar] [CrossRef]
- Li, X.; Zheng, W.; Li, J.; Lin, Q.; Yang, J.; Huang, S.; Wang, D.; Wang, B. Primary exploration of efficacy of community-family management mode under internet -based mobile terminal monitoring in elderly patients with stable coronary heart disease. J. Health. Eng. 2022, 704. [Google Scholar] [CrossRef] [PubMed]
- Kivimaki, K.; Nyberg, S.T.; Fransson, I.; Heikkila, K.; Alfredsson, L.; Sasini, A.; Clays, E.; De Bquer, D.; Dragano, N.; Ferrie, J.E.; et al. Associations of job strain and lifestyle risk factors with risk of coronarynartery disease: A meta-analysis of individual participant data. CMAJ 2013, 185, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Vogel, B.; Acevedo, M.; Appelman, Y.; Bairey Merz, C.N.; Chieffo, A.; Figtree, G.A.; Guerrero, M.; Kunadian, V.; Lam, C.S.P.; Maas, A.H.E.M.; et al. The Lancet women and cardiovascular disease Commission: Reducing the global burden by 2030. Lancet 2021, 397, 2385–2438. [Google Scholar] [CrossRef]
- Martinho, M. Women more likely to die after heart attack than men.In Proceedings in Heart Failure, Congress of European Society of Cardiology. Topics Heart Failure, Prague, Czechia. 22 May 2023.
- Hosseini, N.; Kaier, T. Gender Disparity in Cardiovascular Disease in the Era of Precision Medicine. JACC Case Rep. 2023, 23. [Google Scholar] [CrossRef] [PubMed]
- Cenko, E.; Manfrini, O.; Fabin, N.; Dorobantu, M.; Milicic, D. Clinical determinants of ischemic heart disease in Eastern Europe. Lancet 2023, 33. [Google Scholar] [CrossRef]
- Schopfer, D. Rural health disparities in chronic heart disease. Prev. Med. 2021, 152, 106782. [Google Scholar] [CrossRef]
- Loccoh, E.C.; Maddox, J.; Wang, Y.; Kazi, D.S.; Yah, R.W.; Wadhera, R.K. Rural-urban disparities in outcome of myocardial infarction, heart failure abd stroke in United States. JACC 2022, 79, 267–279. [Google Scholar] [CrossRef]
- Yung, E.; Kong, S.Y.; Ro, Y.S.; Shin, S.D. Serum Cholesterol Levels and Risk of Cardiovascular Death: A Systematic Review and a Dose-Response Meta-Analysis of Prospective Cohort Studies, Int. J. Environ. Res. Public Health 2022, 19, 8272. [Google Scholar] [CrossRef]
- Bienstock, S.; Lee, S.E.; Blankstein, R.; Leipsic, J.; Patel, K.; Narula, J.; Chandrashekhar, Y.S.; Fuster, V.; Shaw, L.J. Systemic inflammation and high sensitivity C reactive protein and atherosclerotic plaque progression. JACC 2024, 17, 212–213. [Google Scholar] [CrossRef]
- Barzilay, J.I.; Farag, Y.M.K.; Durthaler, J. Albuminuria-an underappreciated risk factor for cardiovascular disease. JAHA 2024, 13. [Google Scholar] [CrossRef]
- Brown, J.C.; Gerhardt, T.E.; Kwon, E. Risk Factors for Coronary Artery Disease. [Updated 2023 Jan 23]. In: StatPearls [Internet]. Stat Pearls Publishing, Treasure Island, Finland. 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554410/.
- Strudwick, J.; Gayed, M.; Deady, M.; Haffar, S.; Mobbs, S.; Malik, A.; Akhtar, A.; Braund, T.; Bryant, R.A.; Harvey, S.B. Workplace mental health screening: A systematic review and meta-analysis. Occup. Environ. Med. BMJ 2023, 0, 1–16. [Google Scholar] [CrossRef]
- Deady, M.; Collins, D.A.J.; Johnston, D.A.; Glozier, N.; Calvo, R.A.; Christensen, H.; Harvey, M. The impact of depression, anxiety and comorbidity on occupational outcomes. Occup. Med. 2022, 72, 17–24. [Google Scholar] [CrossRef]
- Hartman, R.; Barber, E. Women in the workforce. The effect of gender on occupational self-efficacy, work engagement and career aspirations. Gend 2020. [Google Scholar] [CrossRef]
Figure 1.
Q waves in DIII, aVF, V1, V2,V3; ST elevation on all thoracic leads(‘’frozen aspect in chronic myocardial infarction”).
Figure 1.
Q waves in DIII, aVF, V1, V2,V3; ST elevation on all thoracic leads(‘’frozen aspect in chronic myocardial infarction”).
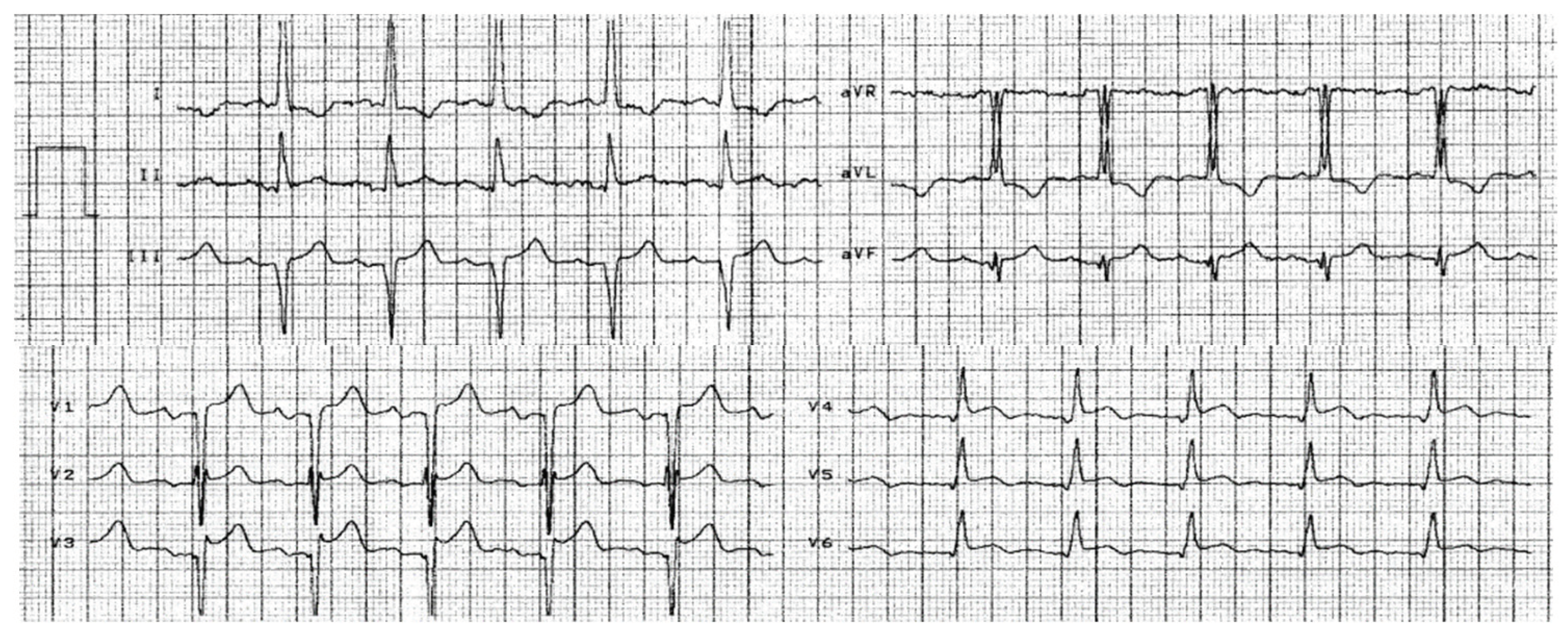
Figure 2.
Echocardiogram, long axis parasternal view Akinesia of antero-septal wall.
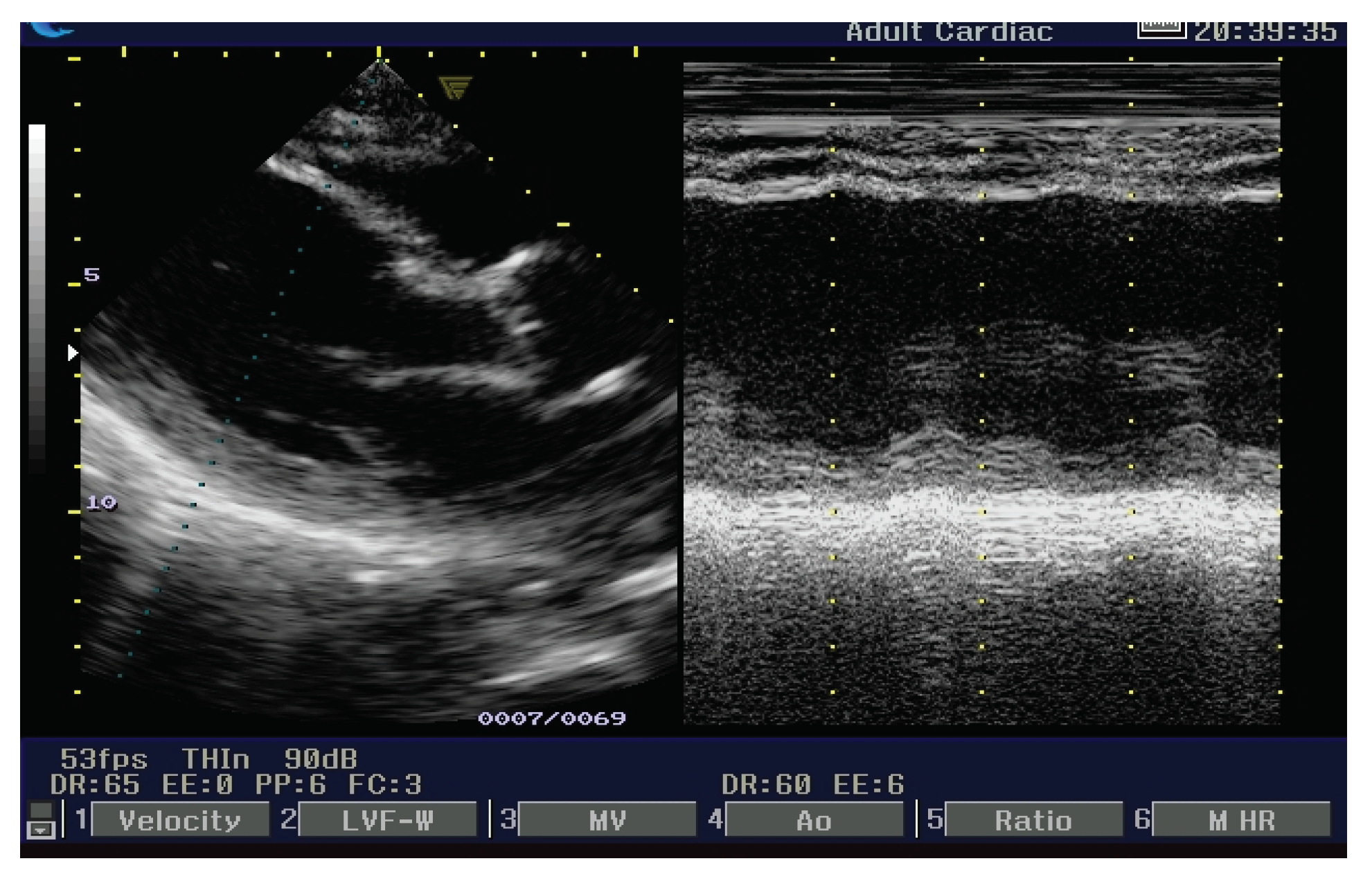
Figure 3.
Apical 4-chambers view: median segment of the postero-septal wall is 6.5 mm, comparative with transversal dimension of basal segment: 13.9 mm.
Figure 3.
Apical 4-chambers view: median segment of the postero-septal wall is 6.5 mm, comparative with transversal dimension of basal segment: 13.9 mm.
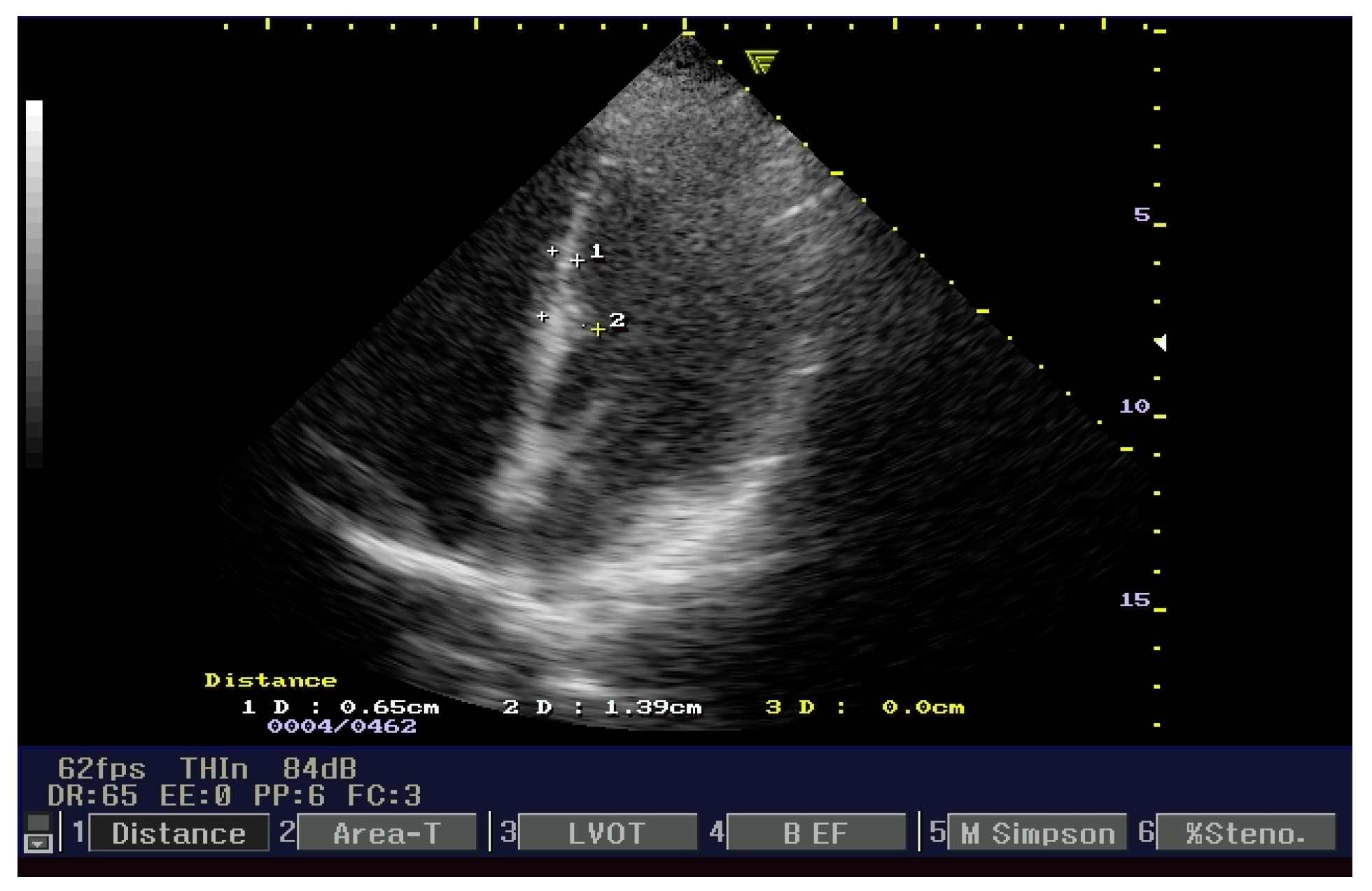
Figure 4.
NCECCT CT calcium score—region of interest (ROI) on right coronary artery (RCA) and left main coronary artery (Lmain) (arrows).
Figure 4.
NCECCT CT calcium score—region of interest (ROI) on right coronary artery (RCA) and left main coronary artery (Lmain) (arrows).
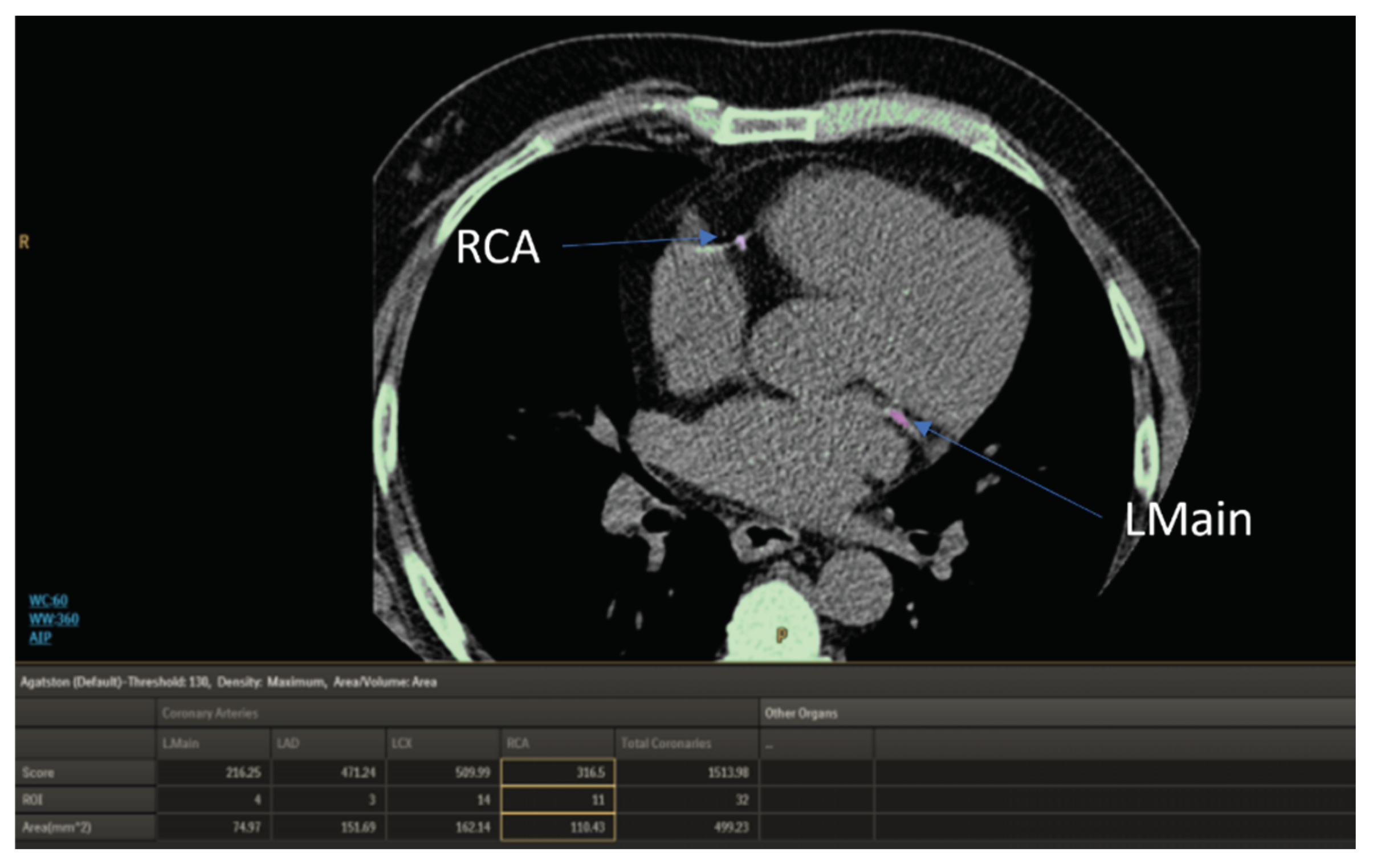
Figure 5.
Prevalence and severity depression in CAD patients.
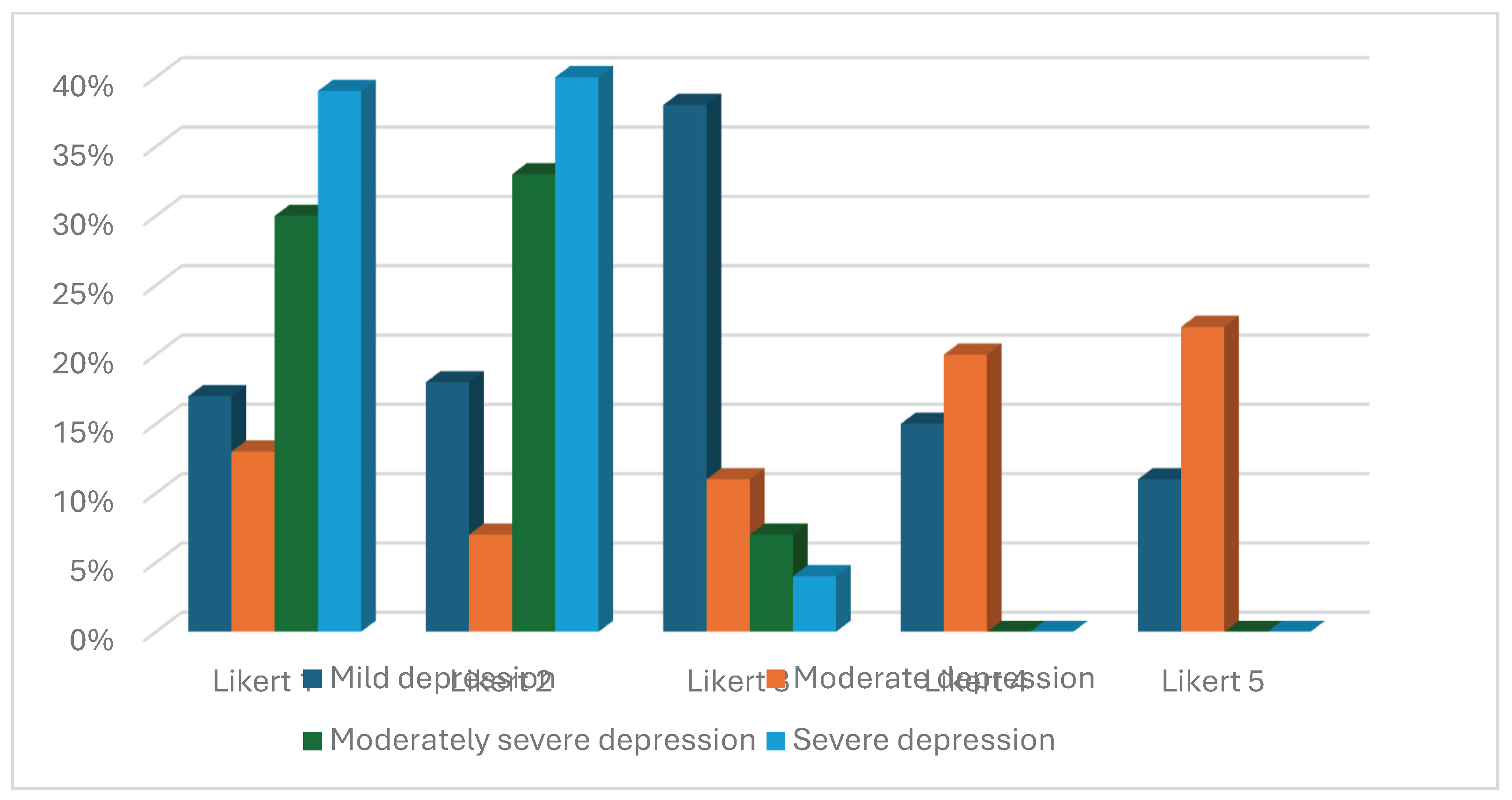
Figure 6.
Prevalence and severity depression in patients without CAD.
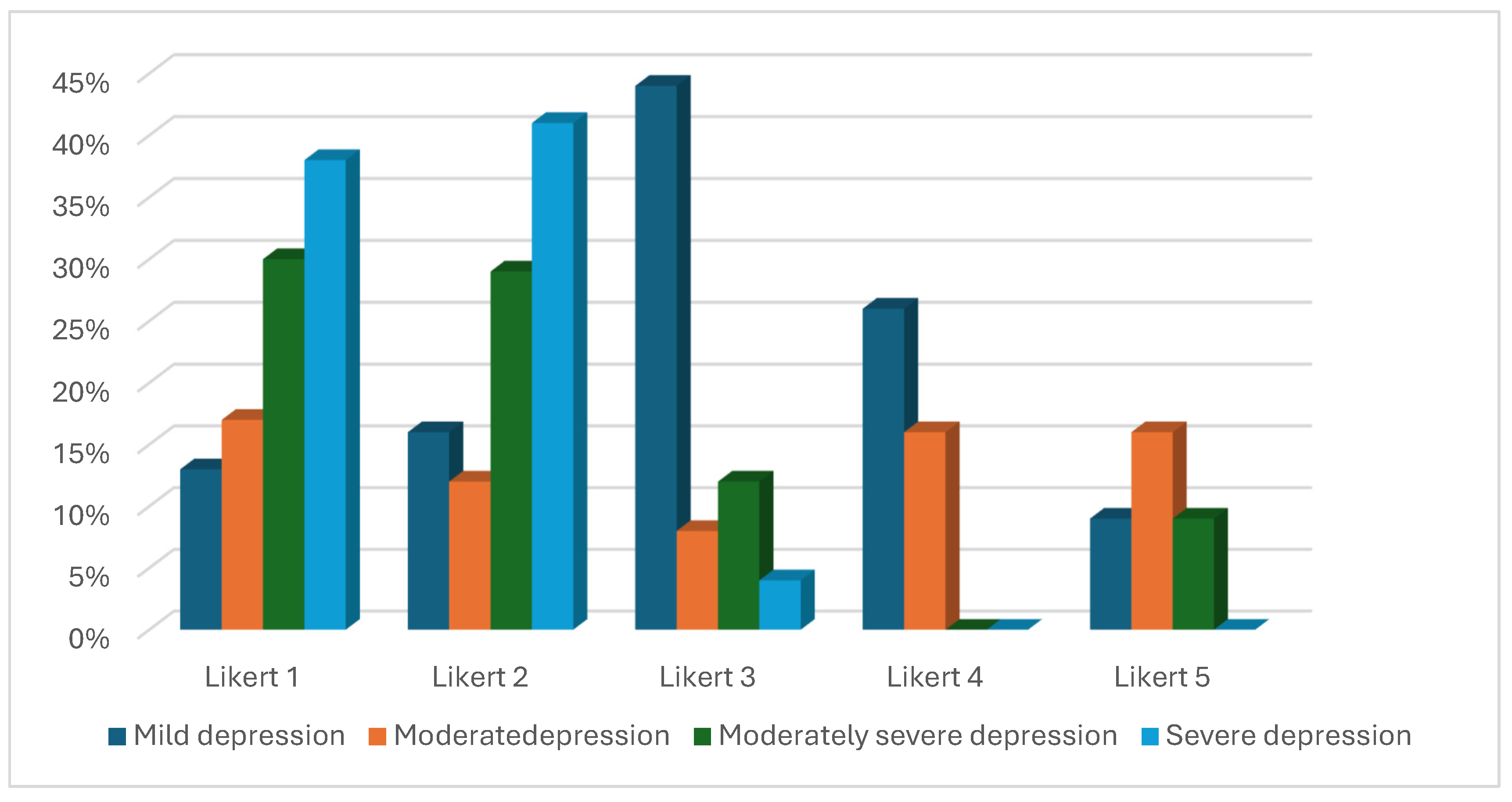
Figure 7.
Chart with satisfaction on workplace (Likert scores) in CAD and without CAD.
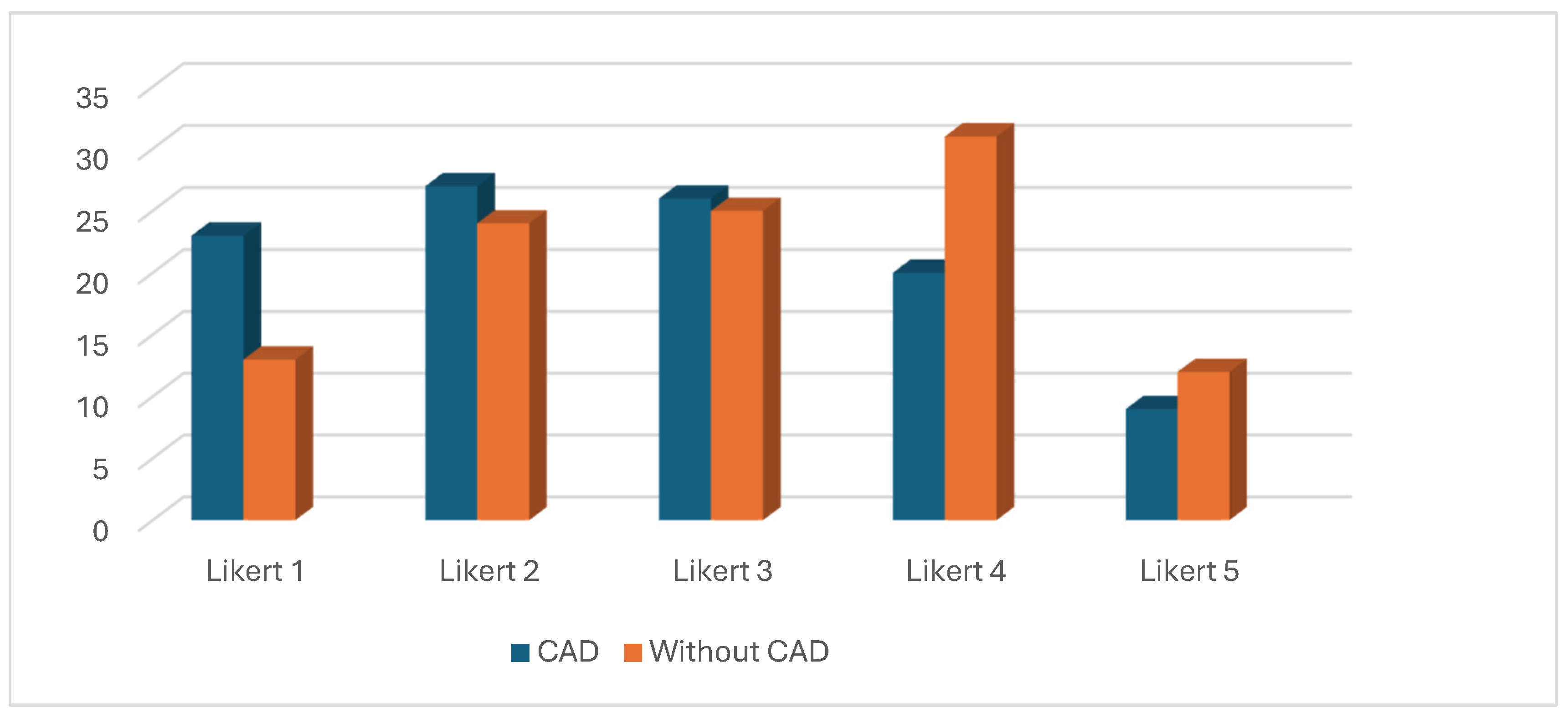
Figure 8.
Chart with hsCRP value and Likert scores.
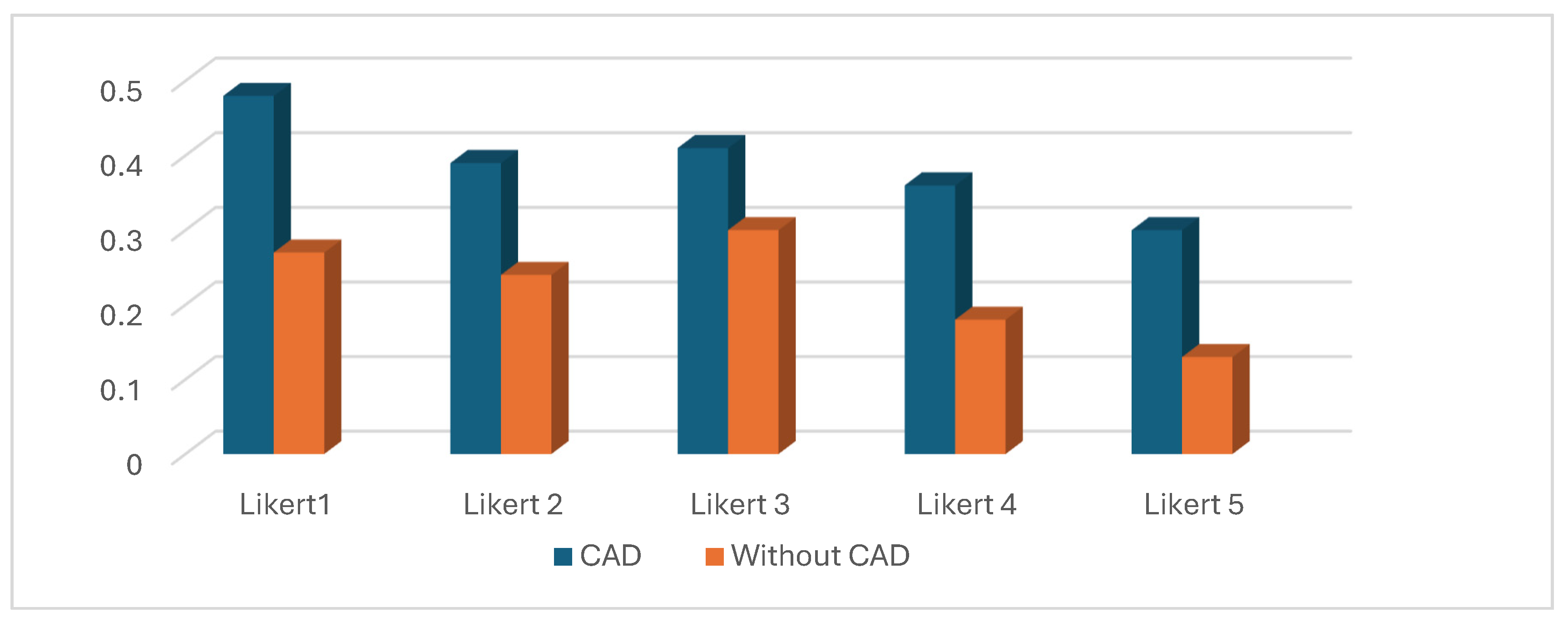
Figure 9.
Chart with microalbuminuria levels and Likert scores.
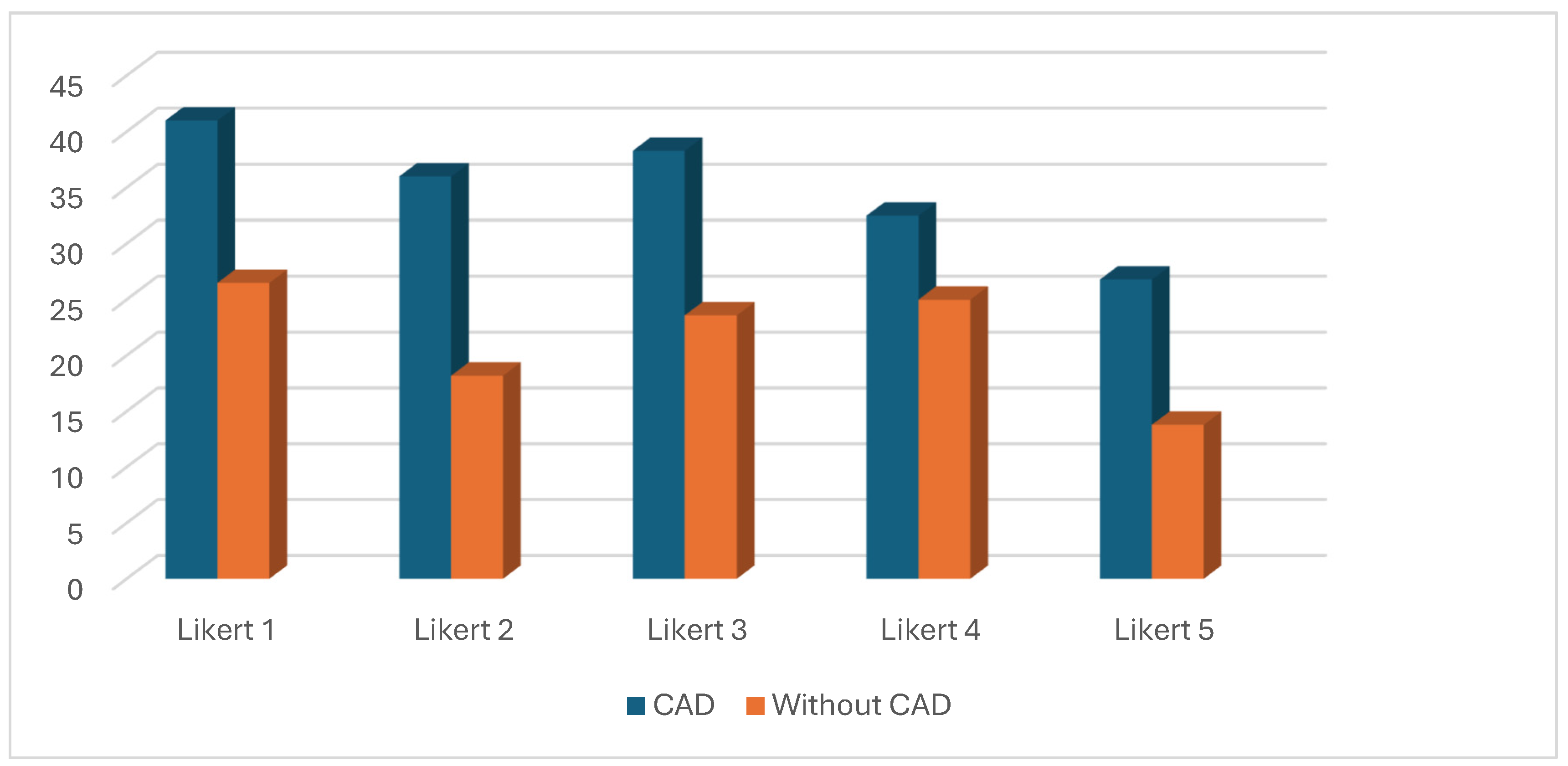
Figure 10.
Distribution of different expressions of CAD for all Likert scores.
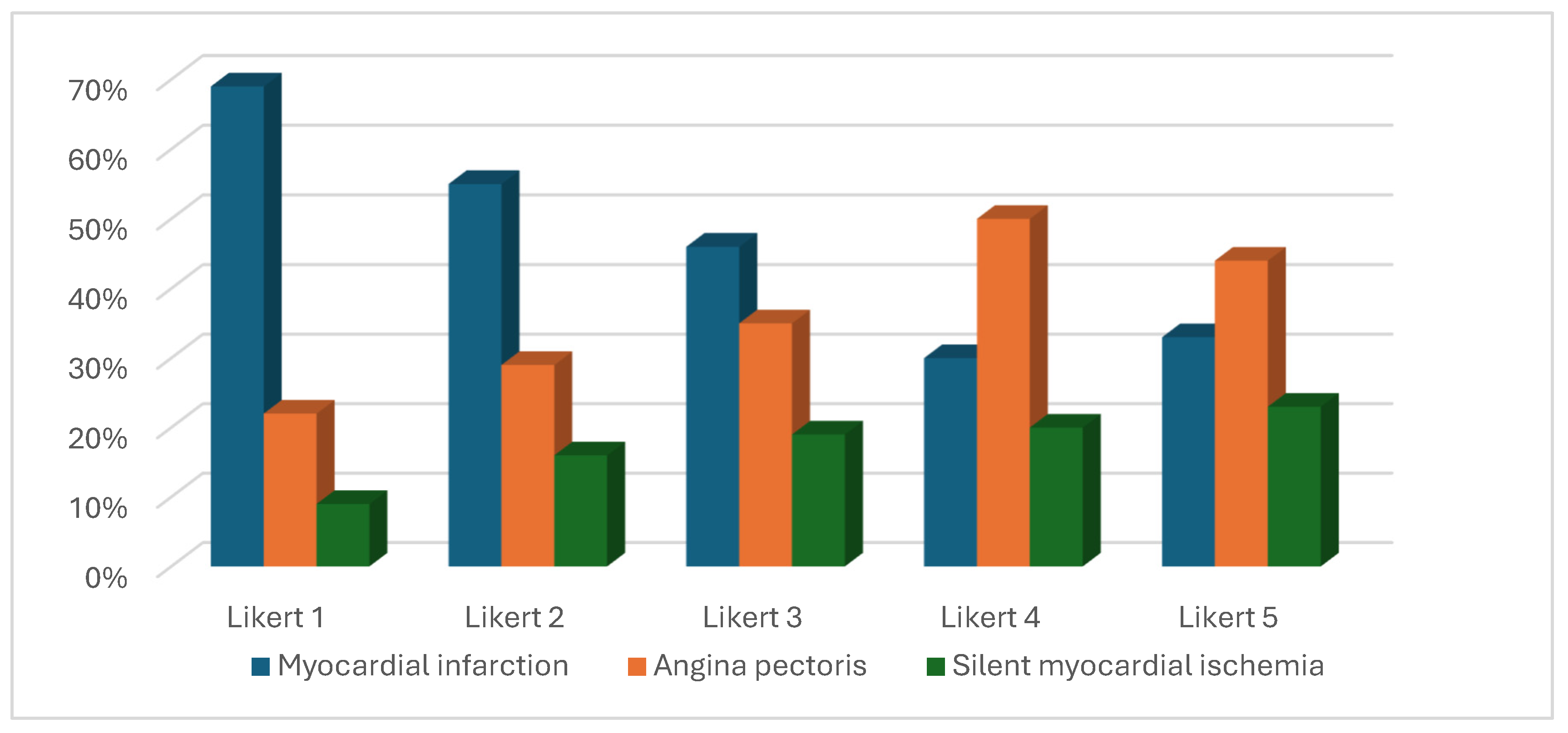
Figure 11.
Active interventions for CAD patients.
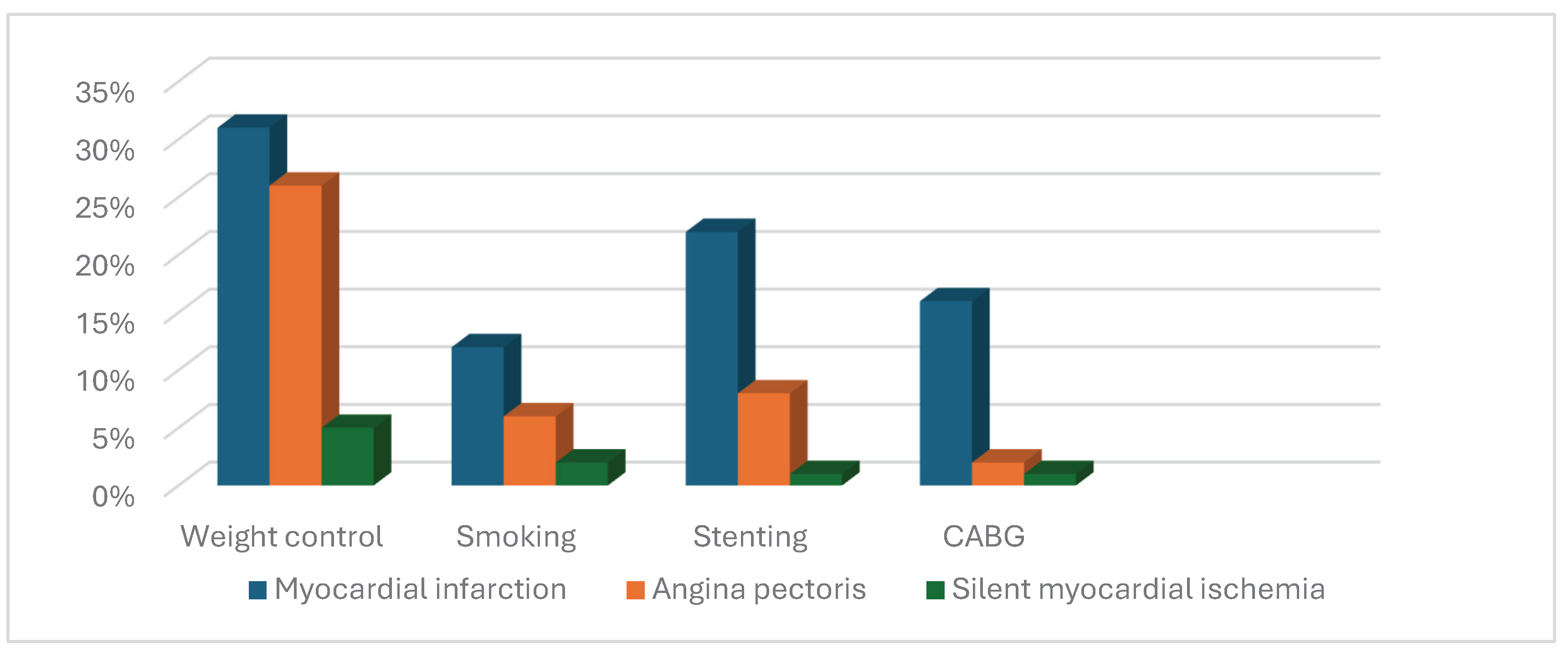
Figure 12.
Cardiovascular risk factors in CAD and without CAD patients.
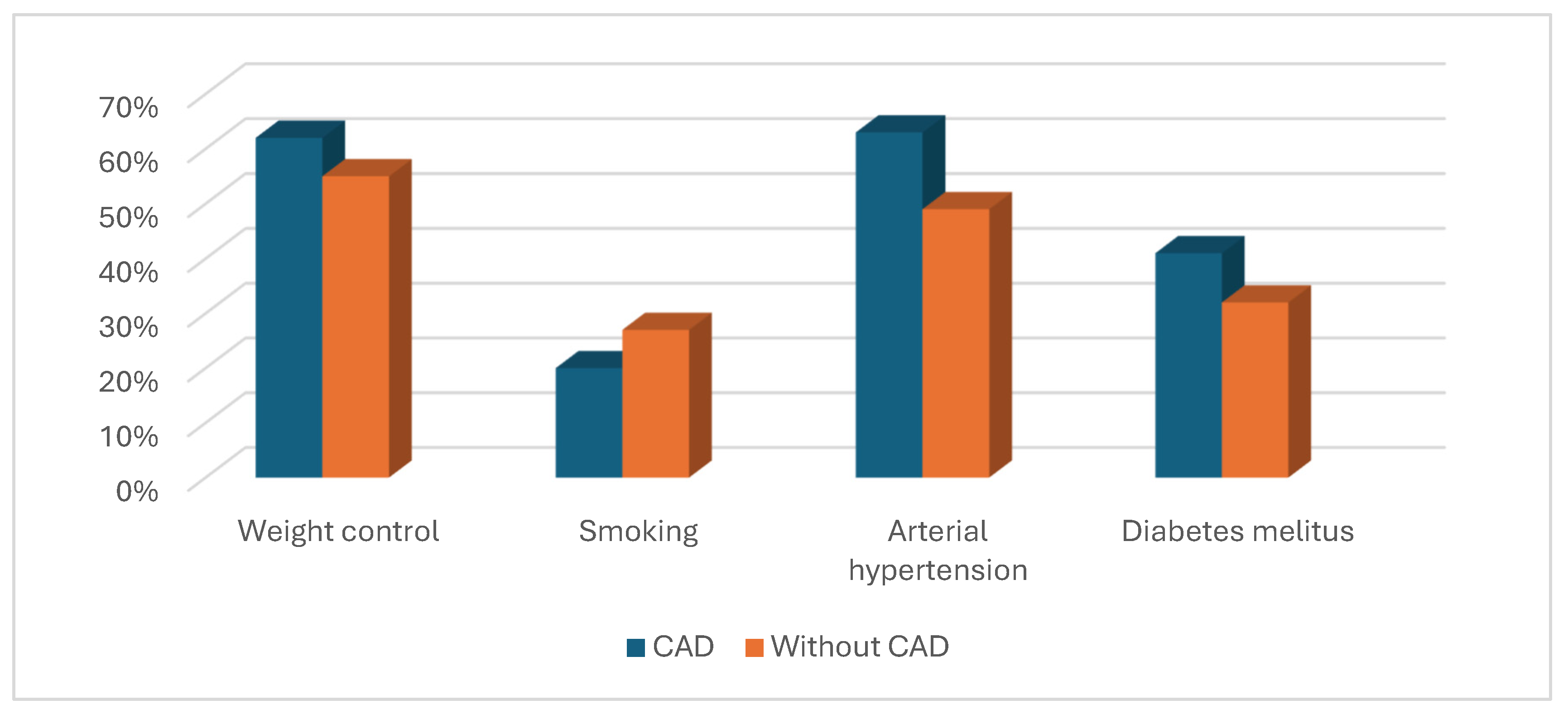
Table 1.
The study objectives.
| Objectives | Objectives description |
|---|---|
| 1 | establish the relationship between job strain and outcome of CAD patients/without CAD patients |
| 2 | discover the role of hs CRP and microalbuminuria, as mediators in this relationship |
| 3 | find out the vulnerable CAD patients ( significant scores at job strain assessment) |
| 4 | active interventions for cardiovascular events prevention |
Table 2.
Inclusion criteria.
| Inclusion criteria | |
|---|---|
| 1 | Age ≥ 18 years |
| 2 | Informed consent and consent for publication |
| 3 | Adherence to medical recommendations |
Table 3.
Exclusion criteria.
| Exclusion criteria | |
|---|---|
| 1 | Evolutive cancer |
| 2 | Autoimmune disorder |
| 3 | Pregnancy |
| 4 | Difficult transportation to Cardiology Office |
| 5 | Acute myocardial infarction |
| 6 | Unstable angina pectoris(de novo/worsened) |
Table 4.
Satisfaction with work scale SWWS—affirmations [23].
Table 4.
Satisfaction with work scale SWWS—affirmations [23].
| Affirmation |
|---|
| a. ‘’generally speaking, my work corresponds with what I want in my life” |
| b. “work conditions are excellent” |
| c. “I am satisfied by my work” |
| d. “I achieved important things wanted by me at work, till now” |
| e. “if I could change something at work place, I woudn’t change anything”. |
Table 5.
Likert scores in SWWS questionnaire[23].
Table 5.
Likert scores in SWWS questionnaire[23].
| Likert score | Patient’s answer |
|---|---|
| 1 | “ totally disagree” |
| 2 | “ partially disagree” |
| 3 | “ almost agree” |
| 4 | “ agree” |
| 5 | “ totally agree” |
Table 6.
Characteristics of the samples.
| Continuos variables and categorical data | Total (210) | With CAD (105) | Without CAD (105) | p-Value |
|---|---|---|---|---|
| Age, years, median (IQR) | 60 (22) | 69 (16) | 52 (18) | 0.01 |
| Sex Female, n (%) | 130 (61.9) | 58 (55.2) | 74 (70.5) | 0.03 |
| Education n (%) | 1. Elementary school 42 (20) 2.High school 128 (61) 3. Higher education 40 (19) |
1. Elementary school 28 (26.6) 2. High school 59 (56.2) 3. Higher education 18 (17.2) |
1. Elementary school 14 (13.3) 2. High school 69 (65.7) 3.Higher education 22 (21) |
0.04 |
|
Rural n (%) Urban n (%) |
126 (60) 84 (40) |
62 (59) 43 (41) |
64 (61) 41 (39) |
0.032 |
| Total cholesterol (mg/dl) median (IQR) | 248 (55) | 260 (59) | 246 (52) | 0.16 |
| LDL cholesterol (mg/dl) median (IQR) | 182 (61) | 186 (52) | 177.5 (59.75) | 0.03 |
| hsCRP (mg/dl) median (IQR) | 0.48 (0.27) | 0.38 (0.25) | 0.22 (0.26) | 0.002 |
| Microalbuminuria/24 hours(mg/dl) median (IQR) | 29 (19) | 36.5 (20) | 21.4 (14.3) | 0.003 |
| Smoking n (%) | 50 (23.8) | 21 (20) | 29 (27.6) | 0.032 |
| Obesity n (%) | 124 (59) | 66 (62.8) | 58 (55.2) | 0.04 |
| Arterial hypertension n (%) | 119 (56.6) | 67 (63.8) | 52 (49.5) | 0.03 |
| Diabetes mellitus n (%) | 77 (36.6) | 43 (41) | 34 (32.4) | 0.02 |
Table 8.
Likert score 1 (SWWS) and its connection with continuos variables and categorical data.
| Likert 1 | Total (36) | With CAD (23) | Without CAD (13) | p-Value |
|---|---|---|---|---|
| Age median (IQR) | 59 (21) | 66 (18) | 50 (12.75) | 0.007 |
| Sex F n (%) | 26 (72.2) | 16 (69.5) | 10 (76.9) | 0.03 |
| Elementary school n (%) | 11 (30.5) | 10 (43.4) | 1 (7.7) | 0.03 |
| High school n (%) | 20 (55.5) | 11 (47.8) | 9 (69.2) | 0.042 |
| Higher education n (%) | 5 (13.8) | 2 (8.7) | 3 (23) | 0.045 |
| hsCRP (mg/dl) median (IQR) | 0.41 (0.47) | 0.48(0.29) | 0.27 (0.14) | 0.002 |
|
Microalbuminuria/24hours (mg/dl) median (IQR) |
29 (22.57) | 41 (18) | 26.5 (9.1) | 0.003 |
Table 9.
Likert scale 2 (SWWS) and its connection with continuos variable and categorical data.
| Likert 2 | Total (51) | With coronary heart disease (27) | Without coronary heart disease (24) | p-Value |
|---|---|---|---|---|
| Age median (IQR) | 58 (22) | 67 (17) | 53 (26.75) | 0.008 |
| Sex F n (%) | 31 (60.7) | 15 (55.5) | 16 (66.6) | 0.032 |
| Elementary school n (%) | 12 (23.5) | 9 (33.3) | 3 (12.5) | 0.025 |
| High school n (%) | 33 (64.7) | 15 (55.5) | 18 (75) | 0.031 |
| Higher education n (%) | 6 (11.7) | 3 (11.1) | 3 (12.5) | 0.04 |
| hsCRP (mg/dl) median (IQR) | 0.29 (0.42) | 0.39 (0.24) | 0.24 (0.14) | 0.003 |
|
Microalbuminuria/24hours (mg/dl) median (IQR) |
26 (14.2) | 36 (18.3) | 18.2 (15.6) | 0.006 |
Table 10.
Likert score 3 (SWWS) and its connection with continuos variables and categorical data.
| Likert 3 | Total (51) | With CAD (26) | Without CAD (25) | p-Value |
|---|---|---|---|---|
| Age median (IQR) | 64 (19.7) | 69.5 (11) | 52 (16.2) | 0.004 |
| Sex F n (%) | 32 (62.7) | 14 (53.8) | 18 (72) | 0.04 |
| Elementary school n (%) | 11 (21.5) | 6 (23) | 5 (20) | 0.045 |
| High school n (%) | 33 (64.5) | 18 (69.2) | 15 (60) | 0.041 |
| Higher education n (%) | 7 (13.7) | 2 (7.7) | 5 (20) | 0.036 |
| hsCRP (mg/dl) median (IQR) | 0.37 (0.31) | 0.41 (0.15) | 0.3 (0.1) | 0.004 |
|
Microalbuminuria/24hours (mg/dl) median (IQR) |
34 (17.35) | 38.3 (14.5) | 23.6 (7.6) | 0.005 |
Table 11.
Likert score 4 (SWWS) and its connection with continuos variables and categorical data.
| Likert 4 | Total (51) | With CAD (20) | Without CAD (31) | p-Value |
|---|---|---|---|---|
| Age median (IQR) | 59 (25.5) | 71 (15.5) | 51 (17) | 0.009 |
| Sex F n (%) | 32 (62.7) | 8 (40) | 24 (77.4) | 0.03 |
| Elementary school n (%) | 5 ( 9.8) | 1 (5) | 4 (12.9) | 0.041 |
| High school n (%) | 31 (60.7) | 10 (50) | 21 (67.7) | 0.036 |
| Higher education n (%) | 15 (29.4) | 9 (45) | 6 (19.3) | 0.024 |
| hsCRP (mg/dl) median (IQR) | 0.27 (0.28) | 0.36 (0.17) | 0.18 (0.09) | 0.004 |
|
Microalbuminuria/24hours (mg/dl) median (IQR) |
24.6 (16.5) | 32.5 (20.7) | 25 (14.8) | 0.005 |
Table 12.
Likert scale 5 (SWWS) and its connection with continuos variable and categorical data.
| Likert 5 | Total (21) | With CAD (9) | Without CAD (12) | p-Value |
|---|---|---|---|---|
| Age median (IQR) | 63 (17.75) | 67 (18) | 59 (30.75) | 0.008 |
| Sex F n (%) | 11 (52.3) | 5 (55.5) | 6 (50) | 0.04 |
| Elementary school n (%) | 3 (14.3) | 2 (22.2) | 1(8.3) | 0.042 |
| High school n (%) | 11 (52.3) | 5 (55.5) | 6 (50) | 0.04 |
| Higher education n (%) | 7 (33.3) | 2 (22.2) | 5 (41.6) | 0.033 |
| hsCRP (mg/dl) median (IQR) | 0.22 (0.16) | 0.3 (0.09) | 0.13 (0.1) | 0.005 |
|
Microalbuminuria/24hours (mg/dl) median (IQR) |
21.5 (14.2) | 26.8 (25.4) | 13.85 (11.17) | 0.006 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



