
Submitted:
03 April 2024
Posted:
04 April 2024
You are already at the latest version
Abstract
Background and Objectives: The purpose of this study was to investigate whether early surfactant administration affects the status of ductus arteriosus (DA) in preterm infants ≤32 weeks of gestational age (GA) within 24 hours of birth. Materials and Methods: It is a prospective study conducted from March 15, 2022, to November 15, 2023, in a tertiary academic center. In-born infants ≤ 32 weeks of gestation (n = 88) were enrolled. The study group was further divided into surfactant (n=44) and non-surfactant (n=44) subgroups. Results: 76% of the preterm infants who received surfactant therapy (RRR = 0.839) recorded an increase in Kindler Score at 24 hours of life (1-RR = 1-0.24 = 76%). Surfactant administration was significantly associated with decreased pre-ductal diastolic pressure (29.9 mmHg vs. 34.8 mmHg, p=0.0231), post-ductal diastolic pressure (28.7 mmHg vs. 32.2 mmHg, p=0.0178) pre-ductal MAP (41.6 mmHg vs. 46.5 mmHg, p=0.0210) post-ductal MAP (41.0 mmHg vs. 45.3 mmHg, p=0.0336). There were no significant changes in ductus arteriosus parameters at 24 hours of life. Conclusions: Early surfactant administration does not affect the status of ductus arteriosus in preterm infants ≤32 weeks of gestational age at 24 hours of life.
Keywords:
surfactant
; ductus arteriosus
; echographic parameters
; preterm infants
1. Introduction
Neonatal respiratory distress syndrome (RDS) is primarily a disease of prematurity caused by surfactant deficiency. It increases morbidity and mortality rates [1,2]. Most early complications of RDS are closely related to prematurity, such as peri/intraventricular hemorrhage (PIVH) and patent ductus arteriosus (PDA). Lung immaturity, invasive mechanical ventilation (MV), and hypo/hyperoxia predispose the very preterm infant to lung injury and inflammation, ultimately leading to bronchopulmonary dysplasia (BPD) [3]. Oxidative stress, fluctuation in cerebral blood flow (CBF) due to respiratory failure, and poor cerebrovascular autoregulation of the immature brain have been linked to neurological complications, neurodevelopmental delays, and cerebral palsy [4,5]. Current management of RDS involves administering prenatal steroids, early uninterrupted non-invasive ventilation (nasal continuous positive airway pressure—nCPAP) of at least 6 cmH2O, and early rescue surfactant treatment [1,6,7,8]. Although exogenous surfactant was previously used as prophylactic therapy for RDS, it is now administered as a rescue therapy as soon as possible after diagnosis. Targeted neonatal echo (TN echo) may be used as a non-invasive diagnostic tool or a guide for surfactant administration, supporting clinical decisions [9,10,11].
According to the latest European Consensus Guidelines, an animal-derived surfactant preparation should be administered at a dose of 200 mg/kg if there is a clinical decline, indicated by a FiO2 level exceeding 30% on nCPAP or if lung LUS reveals bilateral lung consolidations accompanied by air bronchograms [6,12].
The method of administering surfactant to premature infants depends on their clinical status. If intubation is needed in the delivery room for stabilization or the condition worsens, surfactant replacement via endotracheal tube followed by mechanical ventilation (MV) is recommended. The less invasive surfactant administration method (LISA) is considered in spontaneously breathing preterm infants with RDS to avoid intubation and MV [6]. The INSURE technique (INtubation-SURfactant-Extubation) is widely used without ongoing MV and recommended in the 2016 European Consensus Guidelines for managing RDS in infants who fail CPAP [13].
Exogenous surfactant administration improves lung function (lung volume and mechanics, gas exchange) by increasing lung compliance and reducing pulmonary vascular resistance (PVR), leading to shunting augmentations across PDA and variations in cerebral blood flow [14,15,16,17].
Ductus arteriosus (DA) is an essential component of fetal circulation [18] that closes spontaneously after birth, inversely related to gestational age (GA). If in-term newborn DA closes within 24 hours of life, over 50% of preterm infants under 28 weeks of GA still have an open DA after birth, significantly affecting their outcome [19]. PDA can have hemodynamic consequences such as pulmonary over-circulation, systemic hypoperfusion, and decreased perfusion of compromised end-organs due to ductal-steal phenomenon. [17,20,21]. Echocardiography is the gold standard for diagnosing PDA and assessing its hemodynamic significance [22]. Cerebral and abdominal Doppler ultrasound can help evaluate hemodynamic changes during the transition to extrauterine life and the neonatal period, particularly in detecting systolic steal caused by significant PDA [23].
This study investigated whether early surfactant administration affects the status of ductus arteriosus (DA) in preterm infants ≤32 weeks of gestational age (GA) within 24 hours of birth.
2. Materials and Methods
2.1. Study Group. Inclusion and Exclusion Criteria
A prospective study was conducted from March 15, 2022, to November 15, 2023, at a tertiary perinatal center (Targu Mureș County Emergency Hospital, Romania) with onsite pediatric cardiology. This study is part of more comprehensive research on Patent Ductus Arteriosus (PDA) in preterm infants ≤ 32 weeks of gestational age, where the assessments were conducted at 24 and 72 hours after birth, and those who had hemodynamically significant PDA (requiring medical closure) were evaluated at 24 hours after the initiation and completion of the treatment.
In the present study, we hypothesized that early surfactant administration to preterm infants would have a direct hemodynamic impact on PDA, affecting cerebral and splanchnic oxygenation during the transitional period. We consider 24 hours of life to be the time of stabilization after delivery.
The inclusion criteria were as follows: Inborn preterm infants with gestational age (GA) between 22 and 32 weeks survived at least 24 hours after birth. We excluded outborn patients with GA ≥ 32 weeks and those with significant congenital anomalies. The eligible preterm infants were divided into two groups based on the management of RDS: the surfactant group and the non-surfactant group. This study was approved by the hospital’s ethical committee (Nr. 6799/15.03.2022). Written consent of the mother was obtained.
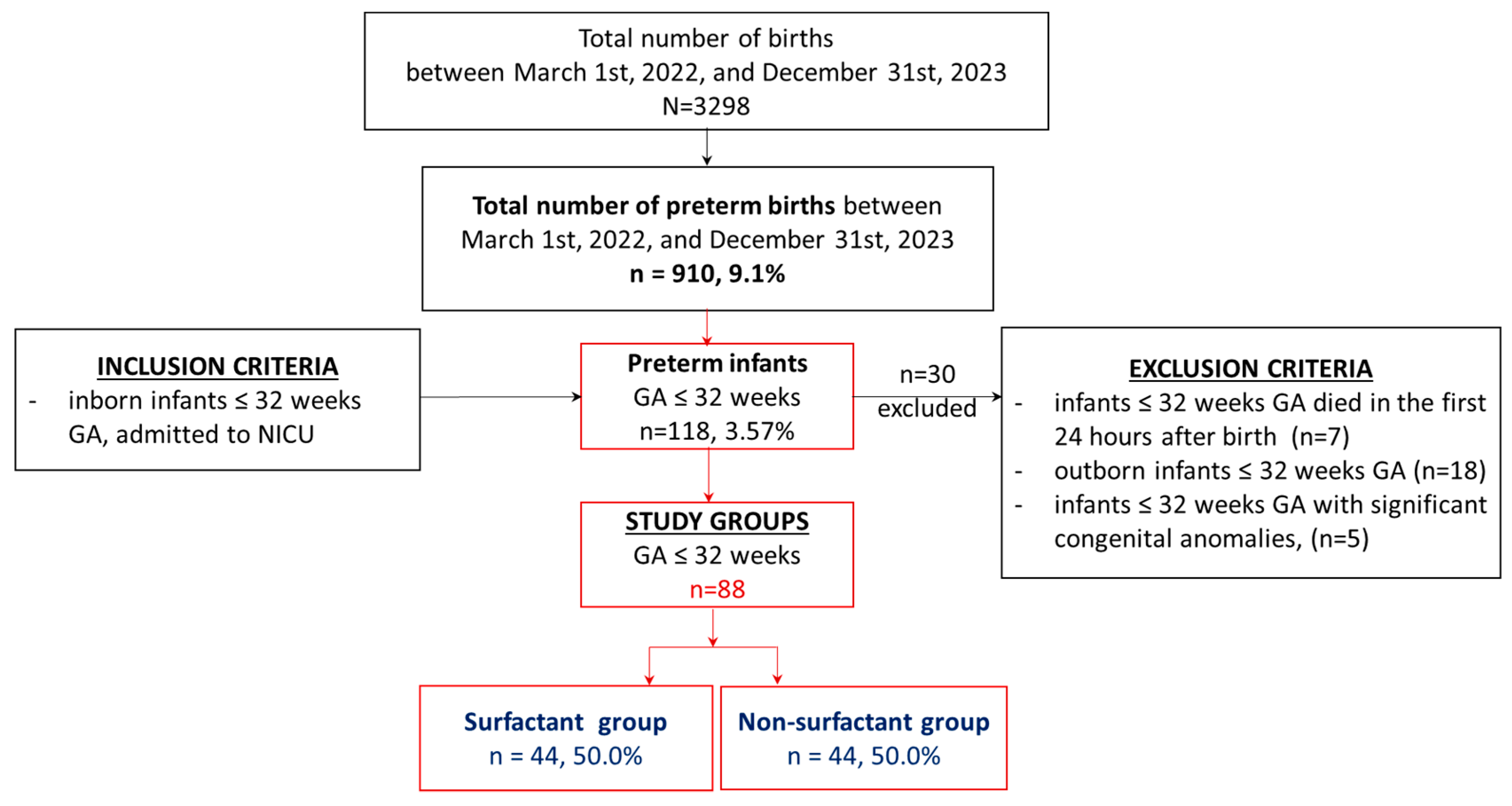
During the study period, a total of 118 preterm infants (3.57% of 3298 births) born between 22—32 weeks of gestation met the inclusion criteria and were admitted to the neonatal intensive care unit (NICU). Therefore, 88 preterm infants out of 118 were enrolled in this study.
Figure 1.
Flow-chart—selection of the study groups.
2.2. Study Design
The study groups underwent a Doppler echocardiography 24 hours after birth to evaluate the status of the Ductus Arteriosus. At the same time, Doppler investigation was used to record systolic and diastolic velocities of the Anterior Cerebral Artery (ACA), Celiac Trunk (CT), and Superior Mesenteric Artery (SMA) to assess cerebral and splanchnic perfusion. Oxygenation levels in the same areas were evaluated using near-infrared spectroscopy (NIRS). Pre- and post-ductal peripheral saturations (SpO2) and pre- and post-ductal blood pressure were simultaneously monitored. Blood gases, troponin, and NT-proBNP samples were collected for laboratory testing.
2.3. Demographic and Clinical Data
The demographic data collected included: maternal age, maternal pathology (diabetes, hypertension, chorioamnionitis, thrombophilia), antenatal care, antenatal steroids, premature rupture of membranes (PROM—hours), mode of delivery, gender, gestational age (GA), birth weight (BW), small for gestational age (SGA) status (defined as BW below the 10th centile on Fenton’s growth chart), Apgar score at 1 and 5 minutes, cord blood gases (pH, pO2, pCO2, BE, Lactate), initial hematocrit (Hct).
The clinical data variables collected included: Silverman-Anderson score for RDS, need for surfactant, mode of surfactant administration (conventional, INSURE, LISA), need for MV, clinical Kindler score for PDA, pre- and post-ductal blood pressure (systolic, diastolic, mean (MAP)), FiO2, pre- and post-ductal peripheric oxygen saturation (SpO2), cerebral regional oxygen saturation (CrSO2), mesenteric regional tissue oxygenation (MrSO2) at 24 hours after birth.
2.4. Diagnosis and Surfactant Treatment of RDS
Respiratory distress syndrome (RDS) was diagnosed based on clinical signs (Silverman-Anderson Scoring: score 0–3: mild; score 4–6: moderate; and score > 6: severe RDS), oxygen requirement (FiO2 > 30% to maintain SpO2 between 88–94%) [6], reticulogranular pattern with air bronchogram on chest radiograph and/or bilateral lung consolidations and air bronchograms on LUS [6,10].
Based on our unit’s protocol, it is recommended to administer early rescue surfactant within the first 2 hours of birth for preterm infants who are unresponsive to nCPAP (PEEP 6-8 cm H2O), have a FiO2 requirement higher than 40% and have a Silverman-Anderson score above 4. Additionally, chest radiograph/LUS characteristics for RDS should be observed.
A dose of 200 mg/kg of surfactant (poractant alpha, Curosurf, Chiesi Pharmaceuticals, Parma, Italy) was administered to all treated patients, regardless of the method. In cases where preterm infants required intubation at birth or soon after delivery, conventional surfactant administration through a catheter inserted into the endotracheal tube followed by MV was performed. In preterm infants breathing spontaneously, the LISA method (without premedication, using a 5-6 Fr. feeding tube) was used as the first intention for surfactant administration, followed by non-invasive ventilation. If the LISA technique failed twice, the INSURE method was used.
2.5. Evaluation of DA at 24 Hours after Birth
2.5.1. Clinical Evaluation of DA
For DA clinical evaluation, we used the Kindler score composed of eight criteria scored with one point each: presence of heart murmur (systolic or continuous); persistent tachycardia (heart rate >160/min); hyperactive precordial pulsation; bounding pulses; apnea or need of mechanical ventilation; pulmonary deterioration; hepatomegaly; acidosis [24].
2.5.2. Echocardiographic Assessment of DA
Echocardiography was performed using a LOGIQ e9 ultrasound machine with a 12 MHz transducer 24 hours after birth, using two-dimensional pulsed and continuous wave color Doppler ultrasonography. After congenital heart defects (CHD) were excluded, all measurements were taken repeatedly over three consecutive cardiac cycles by one pediatric cardiologist according to a standardized protocol.
The protocol included:
1. measurement of trans-ductal diameter (mm) at its narrowest point in high left parasternal short axis view (“ductal” view)
2. interrogation of DA shunt direction in “ductal” view: left to right (L-R), right to left (R-L), bidirectional shunt
3. interrogation velocity of blood flow across DA by measuring systolic max flow velocity (DAVsmax in m/s) and diastolic max flow velocity (DAVdmax in m/s) on pulse or continuous wave Doppler in “ductal” view
4. measurement of the left atrium to aortic root ratio (LA: Ao ratio) in parasternal long axis view (LAX) using M-mode
2.5.3. Head Ultrasound
Standard and Doppler’s cranial echography were performed and recorded with LOGIQ e9 ultrasound machine (GE Medical Systems Co.) by trained neonatologists in ultrasound examination using a 7.5-12 MHz transducer 24-36 hours after birth. The infants were in a supine position and quiet state. Images were obtained through the anterior fontanel, anterior to the genu corporis callosi in sagittal view. A pulsed Doppler sample volume gate was placed at ACA with the insonation angle close to 0. Recorded values for ACA include peak systolic velocity (PSV in cm/s), end-diastolic velocity (EDV in cm/s), and automatically calculated resistive index (RI/Pourcelot index).
2.5.4. Abdominal Ultrasounds
The transducer was positioned in a sagittal plane in the epigastric area, just below the xiphoid process. The first branch of the abdominal aorta, the celiac trunk (CT), was identified. The superior mesenteric artery (SMA), originating just below the celiac artery, was also identified. The sample volume was placed 2-3 mm distally above the origin of arteries from the aorta. An angle correction of ≤ 30º was used when necessary. Flow velocities and resistive index in the celiac trunk (CT) and superior mesenteric artery (SMA) were performed through two cycles of at least three consecutive waves using duplex-pulsed Doppler ultrasound.
2.5.5. Cerebral and Mesenteric Oxygenation Monitoring
NIRS is a non-invasive method for monitoring cerebral oxygenation and perfusion [25]. Cerebral and mesenteric oxygenation was monitored simultaneously by measuring regional cerebral oxygen saturation (crSaO2) and regional mesenteric oxygen saturation (mrSaO2) one hour before and one hour after ultrasound examinations with an INVOS 5100C monitor (Somanetics Corporation, Troy, MI).
Neonatal NIRS sensors were placed on the forehead and in the supraumbilical region of the infants. Arterial oxygen saturation (SpO2) was measured simultaneously using Nellcor (Medtronic) sensors. Cerebral fractional tissue oxygen extraction (cFTOE) was calculated as (SpO2-rcSO2)/SpO2. Mesenteric fractional tissue oxygen extraction (mFTOE) was calculated as (SpO2-rmSO2)/SpO2 [26].
2.5.6. Blood Sample Collection (Laboratory Data)
Samples of umbilical cord artery blood gases were taken at birth and before ultrasound examinations. pH, base excess (BE), and lactate levels were recorded. In addition, at 24 hours of life, serum protein inflammatory markers such as N-terminal pro-BNP (NT-proBNP) and troponin T (cTnT) were assessed.
2.6. Statistical Analysis
The statistical analysis of data was performed using SPSS v.29 (IBM Ireland Product Distribution Limited, IBM House, Shelbourne Road, Ballsbridge, Dublin 4, Ireland) and the STATA 16 software (StataCorp LLC, 4905 Lakeway Drive, College Station, Texas 77845-4512, USA). Continuous variable types were reported as mean values and standard deviation (SD) or median with 25th–75th percentiles (range), depending on the normality and homogeneity of the data series. The Kolmogorov–Smirnov test was applied to verify the normal distribution of the variables. The comparisons between the analyzed groups were performed using Student’s t-test or Mann-Whitney U Test for continuous variables, depending on the homogeneity of data-series, based on Levene’s test. The qualitative variables were presented as absolute (n) and relative (%) frequencies and the comparison among the groups was based on the results of Pearson Chi-square test.
The accuracy of predictive power was evaluated based on the ROC curve, taking into account the area under the curve (AUC). In order to comparatively evaluate the impact of surfactant administration on the clinical and ultrasound parameters of the ductus arteriosus, we applied a linear regression model with adjustment for gestational age. The significance level calculated in utilized tests (p-value) was considered significant for the values of p<0.05.
3. Results
We have conducted a prospective (observational) study on a cohort of 88 preterm infants with gestational ages ranging from 22 to 32 weeks. We calculated the relative risk or risk ratio (RR) values that are appropriate for prospective studies. It is important to note that the odd ratio (OR) values are specific to retrospective studies, and they tend to overestimate the risk.
The objective of the univariate analysis (Table 1) was to estimate the probability of requiring surfactant administration based on maternal-neonatal parameters at delivery. The study involved a dichotomous dependent variable: the administration or non-administration of surfactant.
Generalized linear models (GLM) regression analysis was applied to calculate RR. For the Odd Ratio (OR) calculation, the binary outcome variable has been modeled using logistic regression.
Study group 1 consisted of preterm infants with lower GA who experienced significant RDS. Most of them required intubation during the transition from intrauterine to extrauterine life. Consequently, mechanical ventilation was required for 63.6% of newborns in this group, compared to 11.4% in study group 2.
Research has shown that surfactant administration has a positive impact on critically ill preterm infants by significantly reducing the probability of requiring mechanical ventilation (OR = 0.179, p < 0.001).
This means that preterm infants who received surfactant had a 5.58 times (1/OR = 5.58) lower chance of requiring MV. Moreover, after surfactant administration, the need for mechanical ventilation decreases by 40.1% (Relative Risk Reduction = 0.401; RRR = 1-RR). Considering these findings, the frequency of MV observed in study group 1 (63.6%) would have been even higher if surfactant had not been administered.
The prevalence of critically ill preterm infants requiring a long period of MV (duration of MV, hours; cut off > 114 h) was significantly reduced with the administration of surfactant (AUC (95%CI): 0.783 (0.684–0.882), p<0.01). Surfactant reduced MV duration by 16.94 times (OR = 0.059, p = 0.002; 1/OR = 16.94). Thus, 83.9% of critically ill newborns who received surfactant (RRR = 0.839) had a shorter ventilation duration.
It was also found that the administration of surfactant significantly reduces the prevalence of cases (AUC (95%CI): 0.882 (0.604–0.902), p<0.01) that require prolonged continuous positive airway pressure (CPAP) treatment (duration of CPAP, hours; cut off > 72h). The duration of CPAP treatment decreases by 3.14 times (1/OR = 3.14; OR = 0.318, p = 0.007). Based on these findings, we can conclude that for nearly half (46.8%) of preterm infants who receive surfactant therapy, there will be a significant decrease in the period (hours) they require CPAP treatment (1–RR = 0.468).
Administration of surfactant significantly decreases the chance of an extended NICU stay (OR = 0.226, p < 0.001). Preterm infants who received surfactant had 4.42 times fewer NICU days (1/OR = 4.424) than infants who did not receive it. The relative risk reduction (RRR: Relative Risk Reduction = 0.599) indicates that 59.9% of newborns who received surfactant spent less than ten days (AUC (95%CI): 0.730 (0.625–0.836), p<0.01) in the NICU.
The cutoff values for MV and CPAP duration (hours), and NICU stay (days) were determined using surfactant administration as the independent variable.
Based on the study, there was no significant difference in the survival rate between the two groups of preterm infants who received surfactant and those who did not (p = 0.0785). However, the study results indicated that administering surfactant to neonates with pulmonary immaturity and small gestational age could increase their survival rate, making it similar to infants who did not require surfactant. The study also revealed a 3.96-fold decrease in the death rate in cases where surfactant was administered (1/OR = 3.96).
Evaluation of the Clinical Parameters of the DUCTUS arteriosus
The clinical parameters of the two groups of preterm infants were compared, and the probability of their change with surfactant administration was evaluated.
Surfactant administration increased Kindler Score by 1/OR=2.46 times. The study’s results indicated that 76% of the preterm infants who received surfactant therapy (RRR = 0.839) recorded an increase in Kindler Score at 24 hours of life (1-RR = 1-0.24 = 76). The frequency of tachycardia was significantly higher in the surfactant-treated group (40.9% vs. 15.9%, p=0.0084).
Surfactant administration was significantly associated with decreased pre-ductal diastolic pressure (29.9 mmHg vs. 34.8 mmHg, p=0.0231), post-ductal diastolic pressure (28.7 mmHg vs. 32.2 mmHg, p=0.0178) pre-ductal MAP (41.6 mmHg vs. 46.5 mmHg, p=0.0210) post-ductal MAP (41.0 mmHg vs. 45.3 mmHg, p=0.0336), pH (7.31 vs. 7.35, p=0.0165) and BE (-5.61 vs. -3.96, p=0.0125) at 24 hours of life.
At 24 hours of life, the surfactant group had significantly lower saturation levels in both cerebral (CrSO2) and mesenteric (MrSO2) regions compared to the non-surfactant group (73.14% vs. 78.59%, p=0.0024; 73.8% vs. 78.9%, p=0.0055, respectively). Moreover, the fractional tissue oxygen extraction of both cerebral (cFTOE) and mesenteric (mFTOE) regions increased in the surfactant group (0.22 vs. 0.17, p=0.0024; 0.18 vs. 0.15, p=0.0345, respectively). Levels of N-terminal pro-BNP (NT-proBNP) were significantly higher in the surfactant group compared to the non-surfactant group (12.962.6 pg/mL vs. 9.621.6 pg/mL, p=0.0247).
Predictive Analysis: The Influence of Surfactant Administration on Clinical Parameters of the Ductus Arteriosus
The predictive analysis aimed to assess the effect of early surfactant administration on ductus arteriosus (DA) status in preterm neonates ≤32 weeks gestational age within 24 hours of birth. Clinical parameters that showed significant changes according to surfactant administration were included in the prediction analysis (Table 2).
The study results showed that administering surfactant had a significant predictive power on the clinical parameters of assessing the ductus arteriosus, as presented in Table 3. The cutoff values of the clinical parameters for the evaluation of the ductus arteriosus at 24 hours after surfactant administration, as shown in Figure 2, indicate the predicted reference thresholds (cutoff), which can classify newborns according to surfactant administration. These values can be used as references in the clinical evaluation of the ductus arteriosus.
To quantify the impact of surfactant administration on ductus arteriosus clinical characteristics, we performed the univariate analysis using a linear regression model with continuous numerical variables as dependent variables.
We analyzed the coefficient values corresponding to the standardized statistic. Thus, the interpretation of the results does not change if we change the measurement scales of the variables. In non-standardized statistics, the resulting statistical coefficients are dependent on the measurement scales of the analyzed variables.
Considering that GA can influence the clinical and ultrasound parameters of the ductus arteriosus, we adjusted the regression model according to GA.
This adjustment eliminated the possible influence that gestational age (GA) may have on modifying the parameters. Adjusting for GA eliminates any potential impact it has on changing the parameters of the ductus arteriosus. Therefore, the interpretation of the coefficients in Table 4 solely refers to the influence of the surfactant on these parameters. Based on these coefficients, we can evaluate which clinical parameter is the most sensitive to surfactant administration.
According to our findings displayed in Table 4, the use of surfactant led to the most significant changes in Kindler Score (Beta=0.406), CrSO2 (Beta=-0.315), cFTOE (Beta=0.309), and NT-proBNP (Beta=0.303). Under surfactant administration conditions, we observed a significant increase in Kindler Score, frequency of tachycardia, cFTOE, mFTOE, and NT-proBNP values (Table 4). Conversely, significant decreases were found for pre-ductal diastolic pressure, post-ductal diastolic pressure, pre-ductal MAP, post-ductal MAP, pH, BE, CrSO2, and MrSO2 (Table 4).
Evaluation of Echographic Parameters of the Arterial Duct
Echographic parameters were evaluated for significant changes after surfactant administration, like the evaluation for clinical parameters of the ductus arteriosus. The results did not show any significant changes in these parameters (Table 5).
Predictive Analysis: The Effect of Surfactant on Echographic Parameters for Ductus Arteriosus Assessment.
The results of the evaluation of the predictive power of surfactant on echographic parameters did not reveal a significant accuracy. Echographic parameters are not significantly influenced by surfactant administration, and in this context, the predictive power of surfactant on them also decreases (Table 6).
Figure 3.
Paired histogram for estimating cut-off values predictive of the ultrasound parameters for evaluation of the ductus arteriosus.
Figure 3.
Paired histogram for estimating cut-off values predictive of the ultrasound parameters for evaluation of the ductus arteriosus.
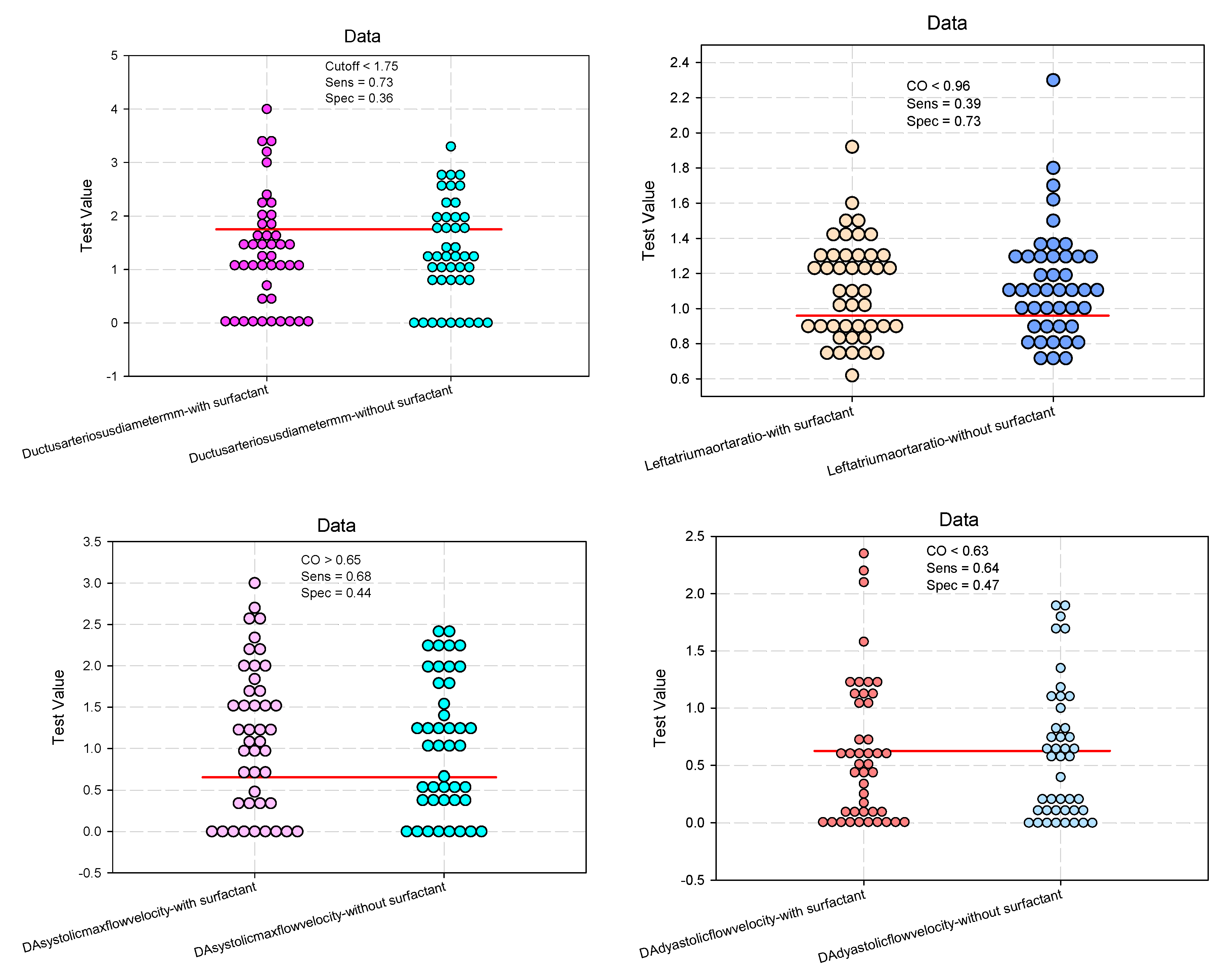
We used a linear regression analysis model adjusted for gestational age to classify the ultrasound parameters of DA based on their response to surfactant administration. However, the standardized coefficients showed that these parameters did not change significantly with surfactant administration, as shown in Table 7.
4. Discussion
Administering surfactant and nCPAP as a primary mode of respiratory support is widely recognized as the gold standard for treating respiratory distress syndrome in preterm infants. Administration of exogenous surfactant via minimally invasive methods is associated with shorter duration of respiratory support, hospitalization, and lower risks of death [27]. In our study, administering surfactant to critically ill preterm infants less than 32 weeks of gestational age had a positive impact. It significantly reduced the need for mechanical ventilation, decreased the duration of mechanical ventilation, and shortened the NICU hospital stay.
There are many controversies regarding the effects of surfactant administration on hemodynamic changes and extrapulmonary effects. Surfactant therapy in preterm neonates may impact their hemodynamics and cardiopulmonary interactions, influencing the pattern and magnitude of PDA flow. This can be quite challenging to recognize, especially during the transitional period. Surfactant administration can cause rapid changes in pulmonary vascular resistance (PVR), which can result in systemic to pulmonary circulatory shifts through the ductus arteriosus, affecting cerebral and mesenteric flows [17].
We found that early surfactant administration did not significantly change the size of ductus arteriosus and DA systolic/diastolic flow velocities. At 24 hours of age, these parameters were similar in both surfactant and non-surfactant groups. Echographic parameters were not significantly influenced by surfactant administration. However, 76% of preterm infants who received surfactant therapy showed an increase in Kindler Score at 24 hours of life. They also had a significantly higher frequency of tachycardia, as well as decreased pre-ductal diastolic pressure, post-ductal diastolic pressure, pre-ductal MAP, post-ductal MAP, and pH at 24 hours of life. It is important to note that these clinical signs can be impacted by factors other than PDA, such as mechanical ventilation and surfactant treatment. This is particularly relevant for preterm infants who receive surfactant treatment, as they tend to experience more severe respiratory distress and require ventilation more frequently than those who do not need surfactant. After the administration of surfactant, the mean arterial blood pressure tends to decrease due to systemic vasodilation. This effect can be partially offset by an increase in cardiac output, which can be achieved by increasing the heart rate [28]. Sehgal found that surfactant treatment was associated with decreased diastolic arterial pressure [29].
In a study on very premature infants between 24 and 29 weeks of gestation, conducted by Fujii et al., no direct effect of surfactant on PDA hemodynamics was observed. In the poractant alfa-treated infants, the PDA size was 1.9±0.8 mm (48% of infants had a DA size > 1.5 mm), and the mean blood flow velocity was 1.0±0.8 m/s at 48 hours after birth [15]. In the present study, among the surfactant-treated preterm infants, 43.20% had a ductus arteriosus size of more than 1.5 mm, and 15.9% revealed spontaneous closure of ductus arteriosus at 24 hours of life.
Conversely, Sehgal et al. found that surfactant administration can cause changes in ductal diameter, left atrium: aortic ratio, shunt direction, and magnitude [29]. Similarly, Kumar et al. discovered that preterm infants who undergo surfactant treatment are more likely to have a larger diameter of the ductus arteriosus (DA), hemodynamically significant DA, and require therapeutic interventions to close the ductus [30,31].
Our study found lower cerebral and mesenteric oxygenation values with decreased CrSO2 and MrSO2 but no significant modification of cerebral and mesenteric ultrasound parameters in surfactant-treated preterm infants. The cerebral blood flow response to surfactant decreased cerebral blood flow in a study conducted by Fuji [15]. Mechanical ventilation has been associated with decreased cerebral blood flow, and variation in cerebral oxygen saturation [33].
We acknowledge the limitations of our study, including the small sample size. We chose to evaluate ductus arteriosus at 24 hours of life, but further studies will be needed to confirm our observation and clarify the relationship between surfactant and ductus arteriosus hemodynamics.
5. Conclusions
Administration of surfactant to preterm infants with gestational age less than 32 weeks resulted in decreased pre-ductal and post-ductal diastolic pressure and mean arterial pressure without significant changes on ductus arteriosus at 24 hours of life.
Author Contributions
Conceptualization, M.C., M.M., R.M. and M.S.; methodology, M.C., M.M., M.-L.O., A.F., D.T., R.M. and M.S.; software, M.M., M.A.-C., A.R., Z.G.; validation, M.C., M.M., M.-L.O. and M.S.; formal analysis, M.C., M.M., M.-L.O., R.M. and Z.G.; investigation, M.C., A.F., D.T., R.M., M.A-C., A.R., Z.G. and M.S.; resources, M.C., M.M., A.F., D.T., R.M., M.A-C., A.R., Z.G. and M.S.; data curation, M.C., M.M., M.-L.O., R.M., M.A-C., A.R. and M.S.; writing—original draft preparation, M.C. and M.M.; writing—review and editing, M.C., M.M., M.-L.O., A.F., D.T., R.M., M.A-C., A.R., Z.G. and M.S.; visualization, M.-L.O., A.F., D.T., R.M., M.A-C., A.R., Z.G. and M.S.; supervision, M.C. and M.M.; project administration, M.C. and M.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the University of Medicine, Pharmacy, Sciences and Technology George Emil Palade of Targu Mureș, grant number 10126/3, 17.12.2020.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Targu Mures County Emergency Hospital, Romania (No. Ad. 6799/15.03.2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- De Luca, D. Respiratory distress syndrome in preterm neonates in the era of precision medicine: A modern critical care-based approach. Pediatr Neonatol. 2021, 62 (Suppl. S1), S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Tana, M.; Tirone, C.; Aurilia, C.; Lio, A.; Paladini, A.; Fattore, S.; Esposito, A.; De Tomaso, D.; Vento, G. Respiratory Management of the Preterm Infant: Supporting Evidence-Based Practice at the Bedside. Children 2023, 10, 535. [Google Scholar] [CrossRef] [PubMed]
- Thekkeveedu, R.K.; El-Saie, A.; Prakash, V.; Katakam, L.; Shivanna, B. Ventilation-Induced Lung Injury (VILI) in Neonates: Evidence-Based Concepts and Lung-Protective Strategies. J. Clin. Med. 2022, 11, 557. [Google Scholar] [CrossRef] [PubMed]
- Polglase, G.R.; Miller, S.L.; Barton, S.K.; Kluckow, M.; Gill, A.W.; Hooper, S.B.; Tolcos, M. Respiratory support for premature neonates in the delivery room: effects on cardiovascular function and the development of brain injury. Pediatr. Res. 2014, 75, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.Y.Y.; Miller, S.L.; Schmölzer, G.M.; Stojanovska, V.; Polglase, G.R. Respiratory Support of the Preterm Neonate: Lessons About Ventilation-Induced Brain Injury From Large Animal Models. Front. Neurol. 2020, 11, 862. [Google Scholar] [CrossRef]
- Sweet, D.G.; Carnielli, V.P.; Greisen, G.; Hallman, M.; Klebermass-Schrehof, K.; Ozek, E.; Pas, A.T.; Plavka, R.; Roehr, C.C.; Saugstad, O.D.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome: 2022 Update. Neonatology 2023, 120, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Course, C.; Chakraborty, M. Management of Respiratory Distress Syndrome in Preterm Infants In Wales: A Full Audit Cycle of a Quality Improvement Project. Sci. Rep. 2020, 10, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Balázs, G.; Balajthy, A.; Seri, I.; Hegyi, T.; Ertl, T.; Szabó, T.; Röszer, T.; Papp, Á.; Balla, J.; Gáll, T.; et al. Prevention of Chronic Morbidities in Extremely Premature Newborns with LISA-nCPAP Respiratory Therapy and Adjuvant Perinatal Strategies. Antioxidants 2023, 12, 1149. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, F.; de Winter, J.P.; De Luca, D. Lung ultrasound-guided surfactant administration: time for a personalized, physiology-driven therapy. Eur. J. Pediatr. 2020, 179, 1909–1911. [Google Scholar] [CrossRef]
- Raschetti, R.; Yousef, N.; Vigo, G.; Marseglia, G.; Centorrino, R.; Ben-Ammar, R.; Shankar-Aguilera, S.; De Luca, D. Echography-Guided Surfactant Therapy to Improve Timeliness of Surfactant Replacement: A Quality Improvement Project. J. Pediatr. 2019, 212, 137–143.e1. [Google Scholar] [CrossRef]
- Raimondi, F.; Yousef, N.; Migliaro, F.; Capasso, L.; De Luca, D. Point-of-care lung ultrasound in neonatology: classification into descriptive and functional applications. Pediatr. Res. 2018, 90, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.-B.; Pang, L.; Yang, B.; Zhang, C.; Chen, X.-Y.; OuYang, J.-B.; Wu, C.-J. Lung Ultrasound for the Diagnosis and Management of Neonatal Respiratory Distress Syndrome: A Minireview. Front. Pediatr. 2022, 10, 864911. [Google Scholar] [CrossRef] [PubMed]
- Sweet, D.G.; Carnielli, V.; Greisen, G.; Hallman, M.; Ozek, E.; Plavka, R.; Saugstad, O.D.; Simeoni, U.; Speer, C.P.; Vento, M.; et al. European Consensus Guidelines on the Management of Respiratory Distress Syndrome - 2016 Update. Neonatology 2016, 111, 107–125. [Google Scholar] [CrossRef] [PubMed]
- Behrman, R.E.; Clyman, R.I.; Jobe, A.; Heymann, M.; Ikegami, M.; Roman, C.; Payne, B.; Mauray, F. Increased shunt through the patent ductus arteriosus after surfactant replacement therapy. J. Pediatr. 1982, 100, 101–107. [Google Scholar] [CrossRef]
- Fujii, A.; Allen, R.; Doros, G.; O'Brien, S. Patent ductus arteriosus hemodynamics in very premature infants treated with poractant alfa or beractant for respiratory distress syndrome. J. Perinatol. 2010, 30, 671–676. [Google Scholar] [CrossRef]
- Vitali, F.; Galletti, S.; Aceti, A.; Aquilano, G.; Fabi, M.; Balducci, A.; Faldella, G. Pilot observational study on haemodynamic changes after surfactant administration in preterm newborns with respiratory distress syndrome. Ital. J. Pediatr. 2014, 40, 26–26. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, A.; Ruoss, J.L.; Stanford, A.H.; Lakshminrusimha, S.; McNamara, P.J. Hemodynamic consequences of respiratory interventions in preterm infants. J. Perinatol. 2022, 42, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, S.G.; McBrien, A. Ductus arteriosus and fetal echocardiography: Implications for practice. Semin. Fetal Neonatal Med. 2018, 23, 285–291. [Google Scholar] [CrossRef]
- Sung, S.I.; Chang, Y.S.; Kim, J.; Choi, J.H.; Ahn, S.Y.; Park, W.S. Natural evolution of ductus arteriosus with noninterventional conservative management in extremely preterm infants born at 23-28 weeks of gestation. PLOS ONE 2019, 14, e0212256. [Google Scholar] [CrossRef]
- McNamara, P.J.; Sehgal, A. Towards rational management of the patent ductus arteriosus: the need for disease staging. Arch. Dis. Child. - Fetal Neonatal Ed. 2007, 92, F424–F427. [Google Scholar] [CrossRef]
- Rios, D.R.; Bhattacharya, S.; Levy, P.T.; McNamara, P.J. Circulatory Insufficiency and Hypotension Related to the Ductus Arteriosus in Neonates. Front. Pediatr. 2018, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Singh, Y. Echocardiographic Evaluation of Hemodynamics in Neonates and Children. Front. Pediatr. 2017, 5, 201. [Google Scholar] [CrossRef] [PubMed]
- Keusters, L.; Purna, J.; Deshpande, P.; Mertens, L.; Shah, P.; McNamara, P.J.; Weisz, D.E.; Jain, A. Clinical validity of systemic arterial steal among extremely preterm infants with persistent patent ductus arteriosus. J. Perinatol. 2020, 41, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Kindler, A.; Seipolt, B.; Heilmann, A.; Range, U.; Rüdiger, M.; Hofmann, S.R. Development of a Diagnostic Clinical Score for Hemodynamically Significant Patent Ductus Arteriosus. Front. Pediatr. 2017, 5, 280. [Google Scholar] [CrossRef] [PubMed]
- Martini, S.; Thewissen, L.; Austin, T.; da Costa, C.S.; de Boode, W.P.; Dempsey, E.; Kooi, E.; Pellicer, A.; Rhee, C.J.; Riera, J.; et al. Near-infrared spectroscopy monitoring of neonatal cerebrovascular reactivity: where are we now? Pediatr. Res. 2023. [CrossRef]
- Binder, C.; Urlesberger, B.; Avian, A.; Pocivalnik, M.; Müller, W.; Pichler, G. Cerebral and Peripheral Regional Oxygen Saturation during Postnatal Transition in Preterm Neonates. J. Pediatr. 2013, 163, 394–399. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Lim, J.; Shim, G.-H. Comparison of mortality and short-term outcomes between classic, intubation-surfactant-extubation, and less invasive surfactant administration methods of surfactant replacement therapy. Front. Pediatr. 2023, 11, 1197607. [Google Scholar] [CrossRef] [PubMed]
- Hentschel, R.; Bohlin, K.; van Kaam, A.; Fuchs, H.; Danhaive, O. Surfactant replacement therapy: from biological basis to current clinical practice. Pediatr. Res. 2020, 88, 176–183. [Google Scholar] [CrossRef]
- Sehgal, A.; Mak, W.; Dunn, M.; Kelly, E.; Whyte, H.; McCrindle, B.; McNamara, P.J. Haemodynamic changes after delivery room surfactant administration to very low birth weight infants. Arch. Dis. Child. - Fetal Neonatal Ed. 2010, 95, F345–F351. [Google Scholar] [CrossRef]
- Kumar, A.; Lakkundi, A.; McNamara, P.J.; Sehgal, A. Surfactant and patent ductus arteriosus. Indian J. Pediatr. 2010, 77, 51–55. [Google Scholar] [CrossRef]
- Canpolat, F.E.; Şimşek, G.K.; Webbe, J.; Büyüktiryaki, M.; Karaçağlar, N.B.; Elbayiyev, S.; Kutman, H.G.K. Late Administration of Surfactant May Increase the Risk of Patent Ductus Arteriosus. Front. Pediatr. 2020, 8, 130. [Google Scholar] [CrossRef] [PubMed]
- Hentschel, R.; Bohlin, K.; van Kaam, A.; Fuchs, H.; Danhaive, O. Surfactant replacement therapy: from biological basis to current clinical practice. Pediatr. Res. 2020, 88, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Bugiera, M.; Szczapa, T.; Sowińska, A.; Roehr, C.C.R.; Szymankiewicz-Bręborowicz, M. Cerebral oxygenation and circulatory parameters during pressure-controlled vs volume-targeted mechanical ventilation in extremely preterm infants. Adv. Clin. Exp. Med. 2020, 29, 1325–1329. [Google Scholar] [CrossRef] [PubMed]
Figure 2.
Paired histogram for estimating cut-off values predictive of the parameters for evaluation of the ductus arteriosus.
Figure 2.
Paired histogram for estimating cut-off values predictive of the parameters for evaluation of the ductus arteriosus.
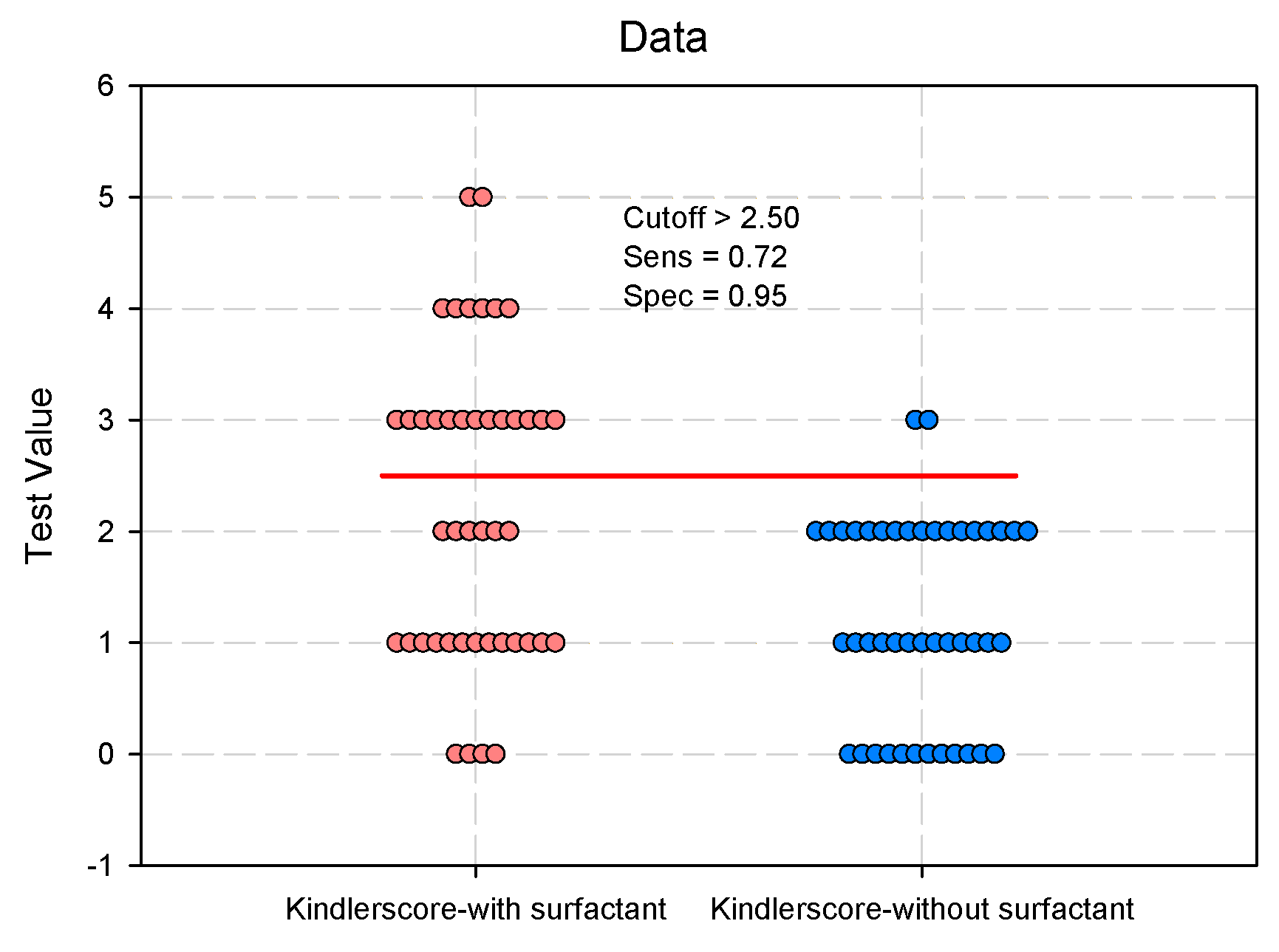
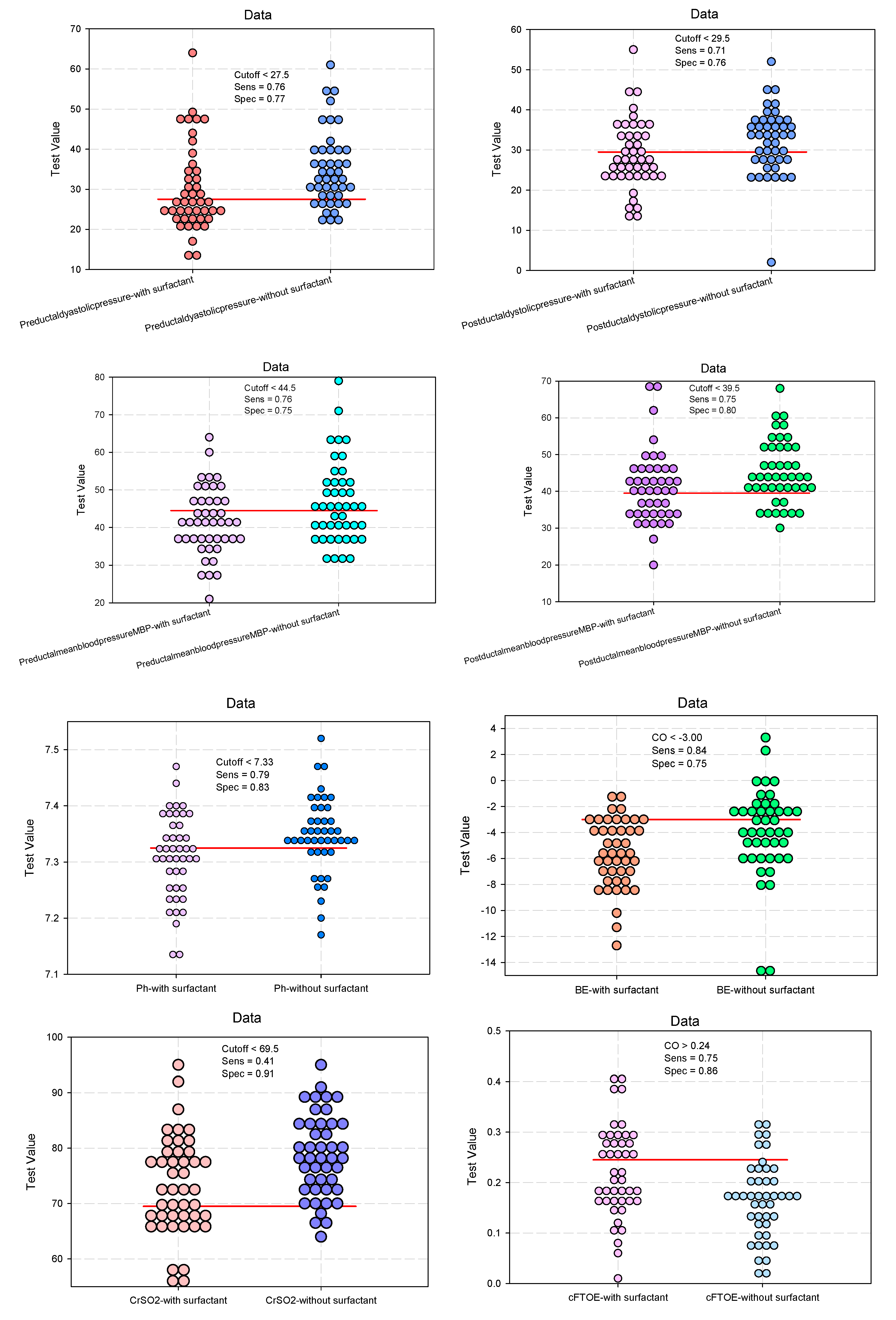
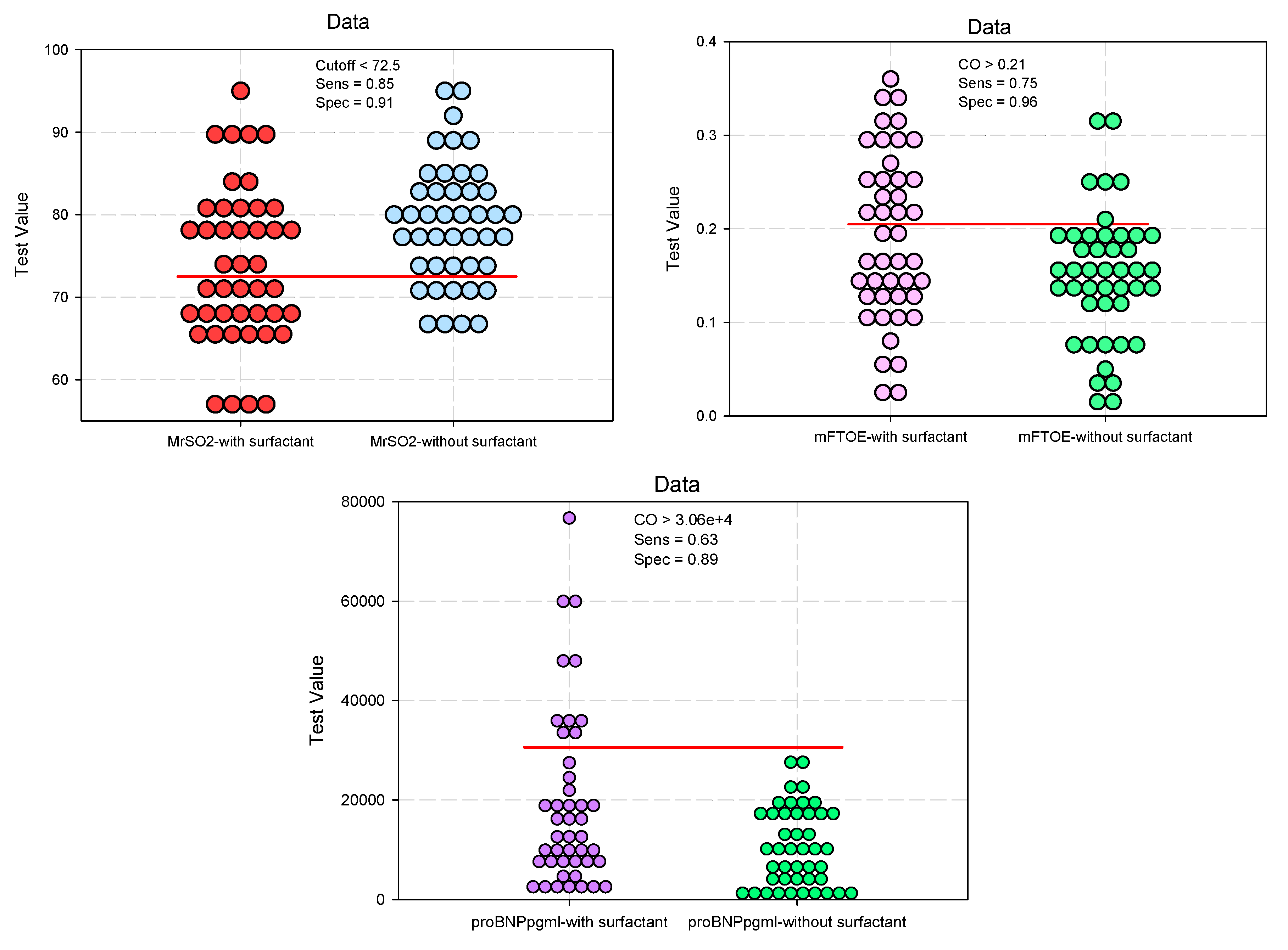

Table 1.
Baseline characteristics.
| Study Group (n = 88) | Odd Ratio (OR) / Risk ratio (RR) | ||||
|---|---|---|---|---|---|
| Group 1 (Surfactant) (n = 44) |
Group 2 (Non- Surfactant) (n = 44) |
p-value | OR (95%CI) RR (95%CI) |
p-value | |
| Dependent variable: Surfactant. Independent variable: Maternal age, GA, BW, gender, SGA, PROM, ACT, vaginal delivery Apgar score, pH, BE, pO2, lactate, Need of intubation at birth, RDS | |||||
| Maternal age #, mean (SD) |
30.2 (7.7) | 27.3 (6.9) | 0.075 | 1.055 (0.994–1.119) 1.000 (0.658–1.519) |
0.078 |
| GA §, (weeks), median (IQR) |
28 (25–29) | 30 (29–31) | <0.001* | 0.539 (0.405–0.716) 0.991 (0.571–0.993) |
<0.001* |
| BW §, (g) median (IQR) |
875.0 (700-1195) | 1260 (1100–1400) | <0.001* | 0.997 (0.995–0.998) 0.631 (0.000–0.947) |
<0.001* |
| Male gender ‡, n (%) male (n=53) / female (n=35) |
29 / 15 (54.7 / 42.9) |
24 / 20 (45.3 / 57.1) |
0.275 |
1.611 (0.681–3.810) 1.262 (0.836–1.906) |
0.277 |
| SGA ‡, n (%) SGA (Yes n=22 / No n=66) |
13 / 31 (59.1 / 46.9) | 9 / 35 (40.9 / 53.1) | 0.332 | 1.631 (0.613–4.336) 1.296 (0.747–2.249) |
0.325 |
| PROM # (hours) mean (SD) |
42.2 (92.51) | 32.6 (100.63) | 0.639 | 1.001 (0.997–1.006) 0.999 (0.994–1.003) |
0.638 |
| ACT ‡, n (%) Yes n=59 / No n=29 |
23 / 12 (54.2 / 41.4) | 27 / 17 (45.8 / 58.6) | 0.256 | 1.679 (0.683–4.126) 1.281 (0.847–1.936) |
0.259 |
| Vaginal delivery ‡, n (%) Yes n=36 / C-section n=52 |
15 / 29 (41.7 / 55.8) | 21 / 23 (58.3 / 44.2) | 0.192 | 1.765 (0.747–4.169) 1.319 (0.874–1.990) |
0.192 |
| Apgar score 1 min § median (IQR) |
6.0 (3–7) | 7.0 (6–8) | <0.001* | 0.663 (0.521–0.844) 0.411 (0.121–0.700) |
<0.001* |
| Apgar score 5 min § median (IQR) |
7.0 (5–8) | 8.0 (8–9) | 0.003* | 0.705 (0.535–0.927) 0.510 (0.163–0.935) |
0.012* |
| Cord blood gases | |||||
| pH # mean (SD) |
7.06 (1.05) | 7.31 (0.10) | 0.001* | 0.472 (0.259–0.863) 0.368 (0.201–0.672) |
0.014* |
| BE # mean (SD) |
-6.36 (4.58) | -4.83 (3.44) | 0.079 | 0.907 (0.812–1.014) 0.854 (0.741–1.002) |
0.085 |
| pO2 # mean (SD) |
35.3 (17.73) | 39.9 (15.7) | 0.203 | 0.983 (0.958–1.009) 0.936 (0.990–1.002) |
0.195 |
| Lactate § median (IQR) |
3.60 (1.60–6.40) | 2.15 (1.65–3.35) | 0.0592 | 1.004 (0.951–1.060) 1.001 (0.987–1.015) |
0.893 |
| Need of intubation at birth‡, n (%) (Yes n=25 / No n=63) |
22/22 (88/34.9) | 3/41 (12/65.1) | <0.001* | 13.67 (3.67–50.79) 13.66 (4.16–62.38) |
0.001* |
| RDS (Silverman) § median (IQR) |
5.5 (5–6) | 3 (2–4) | <0.001* | 2.872 (1.858–4.440) 2.348 (2.216–3.560) |
<0.001* |
|
Group 1 (Surfactant) (n = 44) |
Group 2 (Non- Surfactant) (n = 44) |
p-value |
OR (95%CI) RR (95%CI) |
p-value | |
| Dependent variable: Need of MV, Duration of MV, Duration of CPAP, NICU days, Deaths. Independent variables: surfactant | |||||
| Need of MV ‡ (after 72h), n (%) Yes / No |
28/16 (63.6/36.4) | 5/39 (11.4 / 88.6) | <0.001* | 0.179 (0.076–0.420) 0.593 (0.500–0.703) |
<0.001* |
| Duration of MV §, (hours) median (IQR) |
240 (154–396) | 108 (100–160) | 0.0327* | 0.059 (0.008–0.423) 0.161 (0.030–0.852) |
0.002* |
| Duration of CPAP §, (hours) median (IQR) |
160 (72–243) | 72 (24–160) | 0.007* | 0.318 (0.139–0.729) 0.532 (0.332–0.854 |
0.007* |
| NICU days § median (IQR) |
24.5 (13–34) | 14.5 (8.25–19) | <0.001* | 0.226 (0.104–0.492) 0.401 (0.257–0.625) |
<0.001* |
| Deaths ‡, n (%) | 7 / 37 (15.9 / 84.1) | 2 / 42 (4.5 / 95.5) | 0.0785 | 0.252 (0.049–1.288) 0.286 (0.063–1.300) |
0.098 |
Continuous variables were expressed as †median (quartile); the variables did not have a normal distribution (data not normally distributed); mean ± standard deviation, the variables did have a normal distribution. Categorical variables: number (%); GA: gestational age; BW: birth weight; SGA: small for gestational age; PROM: premature rupture of membranes; ACT: antenatal corticosteroids; RDS: respiratory distress syndrome; MV: mechanical ventilation; CPAP: continuous positive airway pressure; NICU: neonatal intensive care unit. # t-test; § Mann-Whitney U Test. ‡ Pearson Chi-square test.
Table 2.
Clinical and paraclinical diagnosis of ductus arteriosus at 24 hours of life.
| Study group (n = 88) | Odd Ratio (OR) / Risk ratio (RR) |
||||
|---|---|---|---|---|---|
| Group 1 (Surfactant) (n = 44) |
Group 2 (Non-Surfactant) (n = 44) |
p-value | OR (95%CI) RR (95%CI) |
p-value | |
| Independent variable: surfactant. | |||||
| Kindler Score § 0/1/2/3/4/5, n(%) median (IQR) |
4/13/6/13/6/2 (9.1/29.6/13.6/29.5/13.6/4.6) 2 (1–3) |
12/13/17/2/0/0 (27.3/29.6/38.6/4.6/0/0) 1 (0–2) |
<0.001* | 0.406 (0.256–0.643) 0.240 (0.108–0.532) |
<0.001* |
| Cardiac murmur ‡, n(%) Yes / No |
9 / 35 (20.5 / 79.5) | 6 / 38 (13.6 / 86.4) | 0.3937 | 0.667 (0.259–1.715) 0.614 (0.198–1.902) |
0.398 |
| Tachycardia>160/min ‡, n (%) Yes / No |
18 / 26 (40.9 / 59.1) | 7 / 37 (15.9 / 84.1) | 0.0084* | 0.389 (0.181–0.837) 0.273 (0.100–0.748) |
0.012* |
| Blood pressure #, mean (SD) | |||||
| Pre-ductal systolic pressure | 59.8 (11.9) | 64.2 (11.6) | 0.0783 | 0.593 (0.416–0.844) 0.605 (0.341–1.074) |
0.086 |
| Post-ductal systolic pressure | 58.1 (11.0) | 62.7 (12.0) | 0.0656 | 0.642 (0.455–1.907) 0.748 (0.427–1.310) |
0.231 |
| Pre-ductal diastolic pressure | 29.9 (10.6) | 34.8 (9.3) | 0.0231* | 0.443 (0.307–0.640) 0.505 (0.283–0.900) |
0.021* |
| Post-ductal diastolic pressure | 28.7 (8.6) | 32.2 (8.1) | 0.0178* | 0.293 (0.192–0.448) 0.389 (0.214–0.709) |
0.002* |
| Pre-ductal MAP | 41.6 (8.9) | 46.5 (10.7) | 0.0210* | 0.437 (0.300–0.637) 0.555 (0.312–0.987) |
0.001* |
| Post-ductal MAP | 41 (9.8) | 45.3 (8.6) | 0.0336* | 0.393 (0.266–0.580) 0.692 (0.393–0.841) |
0.001* |
| Blood gases | |||||
| pH #, mean (SD) | 7.31 (0.08) | 7.35 (0.07) | 0.0165* | 0.422 (0.289–0.616) 0.677 (0.480–0.955) |
0.005* |
| pH<7.25 ‡, n (%) | 12 / 32 (27.3 / 72.7) | 7 / 37 (15.9 / 84.1) | 0.1951 | 0.505 (0.177–1.435) 0.583 (0.254–1.342) |
0.195 |
| pO2 #, mean (SD) | 47.5 (13.2) | 47.8 (9.1) | 0.9031 | 0.594 (0.420–1.140) 0.766 (0.544–1.077) |
0.125 |
| pCO2 #, mean (SD) | 42.2 (11.4) | 40.1 (10) | 0.3544 | 1.368 (0.970–1.930) 1.211 (0.861–1.704) |
0.074 |
| BE #, mean (SD) | -5.61 (2.64) | -3.96 (3.41) | 0.0125* | 0.578 (0.406–0.823) 0.678 (0.480–0.958) |
0.028* |
| Lactate §, median (IQR) | 1.65 (1.30–2.55) | 1.70 (1.25–2.00) | 0.3247 | 0.713 (0.505–1.007) 0.823 (0.583–1.161) |
0.055 |
| SpO2 #, mean (SD) | |||||
| Pre-ductal | 94.2 (3.01) | 94.8 (2.45) | 0.3155 | 0.486 (0.336–1.102) 0.713 (0.504–1.008) |
0.056 |
| Post-ductal | 94.0 (3.00) | 94.9 (2.60) | 0.1329 | 0.622 (0.420–1.085) 0.802 (0.569–1.130) |
0.207 |
| FiO2 #, mean (SD) | 30.5 (13.29) | 26.3 (6.39) | 0.0618 | 0.667 (0.471–1.146) 0.944 (0.667–1.335) |
0.745 |
| CrSO2 #, mean (SD) | 73.14 (8.89) | 78.59 (7.42) | 0.0024* | 0.636 (0.447–0.905) 0.690 (0.485–0.980) |
0.012* |
| cFTOE #, mean (SD) | 0.22 (0.09) | 0.17 (0.08) | 0.0024* | 2.454 (1.670–3.605) 1.997 (1.387–2.874) |
<0.001* |
| MrSO2 #, mean (SD) | 73.8 (9.52) | 78.9 (7.35) | 0.0055* | 0.430 (0.294–0.629) 0.502 (0.348–0.725) |
<0.001* |
| mFTOE §, median (IQR) | 0.18 (0.13–0.26) | 0.15 (0.12–0.19) | 0.0345* | 2.305 (1.586–3.350) 1.749 (1.225–2.495) |
0.002* |
| Troponin #, mean (SD) | 34.37 (34.6) | 33.07 (29.4) | 0.8496 | 1.170 (0.508–3.124) 1.020 (0.457–3.007) |
0.069 |
| NT-proBNP §, median (IQR) | 12962.6 (7333.7–25934.8) | 9621.6 (3463.2–17381.8) |
0.0247* | 2.995 (1.973–4.545) 3.250 (2.114–4.996) |
<0.001* |
Continuous variables were expressed as: median (quartile) if they did not have a normal distribution; mean ± standard deviation (SD) if the variables had a normal distribution; categorical variables: number (%); MAP: mean blood pressure; CrSO2: Cerebral regional oxygen saturation; cFTOE: cerebral fractional tissue oxygen extraction; MrSO2: Mesenteric regional tissue oxygenation; mFTOE: Mesenteric fractional tissue oxygen extraction. # t-test; § Mann-Whitney U Test, ‡ Pearson Chi-square test.
Table 3.
Predictive value (accuracy in prediction) of clinical parameters for assessment of ductus arteriosus under surfactant administration.
Table 3.
Predictive value (accuracy in prediction) of clinical parameters for assessment of ductus arteriosus under surfactant administration.
| Clinical parameters: evaluation of the ductus arteriosus Independent variable: surfactant |
Area under the Curve (AUC) |
Std. Error |
p-Value | 95%Confidence Interval for AUC |
||
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| Kindler Score | 0.780 | 0.052 | 0.0001* | 0.678 | 0.882 | |
| Tachycardia | 0.654 | 0.064 | 0.0161* | 0.528 | 0.779 | |
| Blood pressure | Pre-ductal diastolic pressure | 0.679 | 0.058 | 0.0037* | 0.565 | 0.793 |
| Post-ductal diastolic pressure | 0.645 | 0.059 | 0.0183* | 0.529 | 0.761 | |
| Pre-ductal MAP | 0.617 | 0.059 | 0.0376* | 0.501 | 0.734 | |
| Post-ductal MAP | 0.646 | 0.058 | 0.0179* | 0.531 | 0.761 | |
| Blood gases | pH | 0.654 | 0.059 | 0.0122* | 0.539 | 0.770 |
| BE | 0.682 | 0.056 | 0.0032* | 0.571 | 0.793 | |
| CrSO2 | 0.682 | 0.056 | 0.0031* | 0.571 | 0.793 | |
| cFTOE | 0.672 | 0.057 | 0.0052* | 0.560 | 0.785 | |
| MrSO2 | 0.668 | 0.058 | 0.0064* | 0.555 | 0.782 | |
| mFTOE | 0.630 | 0.059 | 0.0347* | 0.513 | 0.748 | |
| NT-proBNP | 0.638 | 0.058 | 0.0247* | 0.523 | 0.754 | |
(*) Marked effects are significant at p < 0.05.
Table 4.
Linear regression coefficients regarding the impact of surfactant administration on changes in the clinical characteristics of the ductus arteriosus after adjusting for gestational age.
Table 4.
Linear regression coefficients regarding the impact of surfactant administration on changes in the clinical characteristics of the ductus arteriosus after adjusting for gestational age.
| Linear Regression: adjustment for gestational age (GA) |
Unstandardized Coefficients | Standardized Coefficients | t | p-Value | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| Kindler Score | 1.023 | 0.249 | 0.406 | 4.115 | <.001* |
| Tachycardia | 0.236 | 0.093 | 0.265 | 2.546 | 0.013* |
| Blood pressure | |||||
| Pre-ductal diastolic pressure | -4.800 | 2.134 | -0.236 | -2.250 | 0.027* |
| Post-ductal diastolic pressure | -3.568 | 1.782 | -0.211 | -2.002 | 0.041* |
| Pre-ductal MAP | -4.784 | 2.109 | -0.238 | -2.268 | 0.026* |
| Post-ductal MAP | -4.227 | 1.958 | -0.227 | -2.159 | 0.034* |
| Blood gases | |||||
| pH | -0.037 | 0.015 | -0.251 | -2.400 | 0.019* |
| BE | -1.676 | 0.657 | -0.265 | -2.548 | 0.013* |
| CrSO2 | -5.320 | 1.731 | -0.315 | -3.073 | 0.003* |
| cFTOE | 0.054 | 0.018 | 0.309 | 3.016 | 0.003* |
| MrSO2 | -5.043 | 1.802 | -0.289 | -2.799 | 0.006* |
| mFTOE | 0.040 | 0.017 | 0.243 | 2.323 | 0.023* |
| NT-proBNP | 8515.645 | 2893.041 | 0.303 | 2.943 | 0.004* |
Weighted Least Squares Regression—Weighted by GA. (*) Marked effects are significant at p < 0.05.
Table 5.
Echographic parameters of ductus arteriosus at 24 hours of life.
| Study Group (n = 88) | Odd Ratio (OR) / Risk ratio (RR) |
||||
|---|---|---|---|---|---|
| Group 1 (Surfactant) (n = 44) |
Group 2 (Non-Surfactant) (n = 44) |
p-value | OR (95%CI) RR (95%CI) |
p-value | |
| Independent variable: surfactant; dependent variable: diameter, direction of shunt, LA/Ao ratio, DA flow velocity, DA treated after 72 h | |||||
| Diameter (mm) #, mean (SD) | 1.32 (1.04) | 1.32 (0.92) | 0.983 | 1.092 (0.779–1.531) 1.002 (0.715–1.406) |
0.990 |
| Small <1.5 mm ‡, n (%) | 18 (40.9) | 18 (40.9) | 0.828 | - | - |
| Moderate 1.5-3 mm ‡, n (%) | 14 (31.8) | 16 (36.4) | 0.652 | - | - |
| Large > 3 mm ‡, n (%) | 5 (11.4) | 1 (2.3) | 0.204 | - | - |
| Closed ‡, n (%) | 7 (15.9) | 9 (20.5) | 0.580 | 0.736 (0.247–2.189) | 0.814 |
| Direction of shunt‡, n (%) | |||||
| L-R: Left to right shunt | 34 (77.3) | 34 (77.3) | 0.799 | 1.0 (0.797–1.254) 1.0 (0.369–2.210) |
0.921 |
| Bidirectional | 2 (4.5) | 2 (4.5) | 0.691 | 1.0 (0.135–7.434) 1.0 (0.147–6.786) |
0.934 |
| No shunt | 7 (15.9) | 10 (22.7) | 0.416 | 0.643 (0.220–1.880) 0.919 (0.748–1.128) |
0.722 |
| LA/Ao ratio #, mean (SD) | 1.12 (0.28) | 1.14 (0.31) | 0.664 | 0.790 (0.446–1.398) 0.827 (0.467–1.463) |
0.418 |
| <1.5 ‡, n (%) | 40 (90.9) | 39 (88.6) | 0.724 | - | - |
| 1/5-2.1 ‡, n (%) | 4 (9.1) | 4 (9.1) | 0.710 | - | - |
| >2 | 0 (0) | 1 (2.3) | 0.237 | - | - |
| DA flow velocity | |||||
| Systolic #, mean (SD) | 1.14 (0.88) | 1.05 (0.81) | 0.597 | 1.318 (0.750–2.314) 1.257 (0.716–2.205) |
0.426 |
| restrictive DA ‡, n (%) | 10 (22.7) | 9 (20.5) | 0.795 | 1.144 (0.414–3.162) 1.029 (0.827–1.282) |
0.818 |
| unrestrictive DA ‡, n (%) | 25 (56.8) | 27 (61.4) | 0.828 | 0.828 (0.354–1.940) 0.895 (0.541–1.480) |
0.739 |
| Diastolic #, mean (SD) | 0.62 (0.63) | 0.61 (0.58) | 0.911 | 1.167 (0.669–2.036) 1.064 (0.611–1.854) |
0.587 |
| DA treated after 72 h ‡, n (%) | 12 (27.3) | 9 (20.9) | 0.489 | 1.417 (0.526–3.812) 1.087 (0.857–1.379) |
0.805 |
Continuous variables were expressed as: †median (quartile), the variables did not have a normal distribution; categorical variables: number (%); L-R: Left to right shunt; LA/Ao: Left atrium: aorta ratio; restrictive DA: Systolic max flow velocity > 2m/s; unrestrictive DA: Systolic max flow velocity < 2m/s; MAP: mean blood pressure; CrSO2: Cerebral regional oxygen saturation; cFTOE: cerebral fractional tissue oxygen extraction; MrSO2: Mesenteric regional tissue oxygenation; mFTOE: Mesenteric fractional tissue oxygen extraction. § Mann-Whitney U Test. ‡ Pearson Chi-square test.
Table 6.
Predictive value (accuracy in prediction) of echographic parameters for evaluating the ductus arteriosus under surfactant administration conditions.
Table 6.
Predictive value (accuracy in prediction) of echographic parameters for evaluating the ductus arteriosus under surfactant administration conditions.
| Clinical parameters: evaluation of the ductus arteriosus Independent variable: surfactant |
Area under the Curve AUC (95%CI) |
Std. Error |
p-Value | 95%Confidence Interval | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Diameter (mm) | 0.501291 | 0.062204 | 0.983355 | 0.3794 | 0.6232 |
| LA/Ao ratio | 0.51188 | 0.062329 | 0.847787 | 0.3897 | 0.6340 |
| DA flow velocity | |||||
| Systolic | 0.523784 | 0.062364 | 0.702437 | 0.4016 | 0.6460 |
| Diastolic | 0.512949 | 0.062504 | 0.835232 | 0.3904 To | 0.6355 |
(*) Marked effects are significant at p < 0.05.
Table 7.
Linear regression coefficients regarding the impact of surfactant administration on changes in the ultrasound parameters of the ductus arteriosus after adjusting for gestational age.
Table 7.
Linear regression coefficients regarding the impact of surfactant administration on changes in the ultrasound parameters of the ductus arteriosus after adjusting for gestational age.
| Linear Regression: adjustment for gestational age (GA) |
Unstandardized Coefficients |
Standardized Coefficients |
t | p-Value | |
|---|---|---|---|---|---|
| B | Std. Error | Beta | |||
| Diameter (mm) | 0.028 | 0.210 | 0.014 | 0.134 | 0.894 |
| LA/Ao ratio | -0.026 | 0.064 | -0.043 | -0.401 | 0.689 |
| DA flow velocity | |||||
| Systolic | 0.101 | 0.181 | 0.060 | 0.558 | 0.578 |
| Diastolic | 0.019 | 0.131 | 0.016 | 0.149 | 0.882 |
Weighted Least Squares Regression—Weighted by GA (*) Marked effects are significant at p < 0.05.
Table 8.
Descriptive evaluation of surfactant influence on cerebral and mesenteric circulation at 24 hours of life.
Table 8.
Descriptive evaluation of surfactant influence on cerebral and mesenteric circulation at 24 hours of life.
| Study Group (n = 88) | |||
|---|---|---|---|
| Group 1 (Surfactant) (n = 44) |
Group 2 (Non-Surfactant) (n = 44) |
p-value | |
| HEAD ULTRASOUNDS | |||
|
ACA PSV §, median (IQR) EDV §, median (IQR) RI #, mean (SD) |
24.7 (19.2-31.15) 7.60 (4.6-8.3) 0.73 (0.12) |
23.75 (20.65-26.65) 7.10 (5.55-8.20) 0.71 (0.09) |
0.603 0.717 0.329 |
| ABDOMINAL ULTRASOUNDS | |||
|
CT PSV #, mean (SD) EDV #, mean (SD) RI #, mean (SD) |
44.8 (21.1) 12.1 (8.38) 0.73 (0.1) |
46.1 (16.1) 13.8 (7.31) 0.70 (0.08) |
0.743 0.312 0.246 |
|
SMA PSV #, mean (SD) EDV §, median (IQR) RI #, mean (SD) |
35.7 (16.92) 9.8 (6.45–11.7)) 0.71 (0.64-0.75) |
33.9 (10.05) 9.15 (7.85–10.7) 0.70 (0.67-0.77) |
0.547 0.485 0.628 |
Continuous variables were expressed as median (quartile) if they did not have a normal distribution; mean ± standard deviation (SD) if the variables had a normal distribution; categorical variables: number (%); ACA: Anterior cerebral artery; PSV: Peak systolic velocity; EDV: End-diastolic velocity; RI: Resistance index; CT: Celiac trunk; SMA: superior mesenteric artery; # t-test; § Mann-Whitney U Test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



