Submitted:
04 April 2024
Posted:
05 April 2024
You are already at the latest version
Abstract
Childhood obesity has become a global epidemic, with significant increases in prevalence over recent decades. While excessive calorie consumption and physical inactivity are known factors, emerging research highlights the role of Endocrine-Disrupting Chemicals (EDCs), particularly obesogens, in obesity's pathogenesis. This review explores the historical context of the environmental obesogens hypothesis, their sources, mechanism of action, impact on prenatal and postnatal development and epigenetics. Additionally, it discusses the long-term consequences of childhood obesity and proposes prevention strategies that will mitigate the negative health effects. Obesogens were found to disrupt hormonal balance and metabolic processes through various mechanisms such as altering gene expression, hormonal interference, and inflammation. Especially significant, was exposure during critical windows of development which correlates with increased risk of obesity in childhood or adolescence. Long-term effects of childhood obesity include chronic health conditions and psychosocial issues. A comprehensive approach is necessary to address childhood obesity, encompassing genetic, environmental, and lifestyle factors. Prevention strategies should focus on reducing obesogens exposure, promoting healthy lifestyles, and implementing regulatory policies. Future research should investigate obesogens-diet interactions, microbiome impacts, and combined obesogens effects. Long-term human studies are also crucial for validating findings from animal models and allow for inform decision-making to combat the obesity pandemic.
Keywords:
endocrine disrupting chemicals
; obesogens
; obesity
; children
; adolescents
; prevention strategies
Introduction
Childhood obesity is defined by the Centers for Disease Control and Prevention (CDC) as a Body Mass Index (BMI) at or above the 95th percentile, or +2 SDS for age and sex. For children younger than 5 years, it is defined as weight for height above +3 SDS. Overweight is defined by a BMI above the 85th percentile or +1 SDS, but less than the 95th percentile, similarly, for children younger than 5 years is defined as weight for height above +2 SDS. Obesity has increased dramatically over the last fifty years, giving rise to a pervasive and harmful public health crisis, frequently denoted as an epidemic [1,2]. According to NCD Risk Factor Collaboration (NCD-RisC), between 1975 and 2016, the worldwide age-standardized prevalence of obesity in children and adolescents aged 5–19 years rose from 0.9% to 7.8% for boys and from 0.7% to 5.6% for girls [3]. Furthermore, in 2019, the World Obesity Federation estimated that by 2025, around 390 million children and adolescents would be overweight and 206 million would be obese, with an expected increase to 254 million by 2030 [4]. As childhood obesity becomes more prevalent worldwide, so does the burden of comorbidities associated with it. It is not just a matter of body image and cosmetic concerns, but it is strongly correlated with increased risk for type 2 diabetes, heart diseases and other metabolic diseases [5]. While numerous theories tried to explain this spreading rise in obesity worldwide, there remains considerable uncertainty. Although non-lifestyle factors such as genetic predispositions were known to be associated with obesity, a recent analysis of 97 BMI-associated loci found that these only account for ~2.7% of BMI variation [6]. Thus, it can be reasonably concluded that abrupt changes in the gene pool, of a magnitude required to be the primary cause of the current issue, are unlikely factors. The prevailing medical explanation continues to be that obesity is due to a combination of excessive caloric consumption and insufficient energy expenditure [7]. Despite a well-recognised global rise in the consumption of fat and sugar rich food as well as a surge in physical inactivity secondary to sedentary lifestyles, this dramatic increase in obesity rates over a relatively short period of time cannot be explained by energy imbalances alone.[7] Consequently, additional mechanisms have been proposed to be contributing to the modern obesity epidemic, one of which is the exposure to Endocrine-Disrupting Chemicals (EDCs). The Endocrine Society defines EDCs as external chemicals that can mimic, block, or interfere with the way body’s hormones work [8]. A subset of these chemicals, known as “obesogens” have been found to play an important role in the pathogenesis of obesity, especially if exposure occurs during critical windows of development [9]. Identifying the sources of obesogens and understanding their pathophysiology will allow us to implement more effective prevention strategies and better treatment approaches. This could provide a possible solution to the problem and help improve the challenges in obesity management faced by today’s paediatric care professionals.
History of Obesogens and the Environmental Obesogens Hypothesis
The relationship between EDCs and obesity first gained attention in the early twenty-first century and more specifically in 2002, when Dr. Paula Baillie-Hamilton authored the first review paper on environmental chemicals and their effect on obesity [10]. She proposed a correlation between the actual obesity epidemic and the increased production of exogenous chemicals following World War II. This link was particularly evident by a figure in her review, illustrating an increase in obesity with an increase in production of chemicals throughout the course of several decades [10]. In 2006, Felix Grun and Bruce Blumberg introduced the idea of environmental disruptors and published a paper revealing that tributyltin (TBT), a xenobiotic compound utilised in marine paints, wood preservation, and industrial water systems, induced weight gain in a population of mice [11,12]. This reinforced the concept that these chemicals could potentially lead to obesity by interfering with normal development and homeostatic control of processes like adipogenesis and energy balance and coined the term “obesogens” to categorize such chemicals. More specifically, the obesogens hypothesis suggests that exposure to obesogens during development could dysregulate pathways responsible for the development of adipose tissue, alter the metabolic balance and hormonal control of appetite and satiety, and impact insulin sensitivity and lipid metabolism, ultimately resulting in obesity. This hypothesis ignited the field and in 2011, the National Institute of Environmental Health Sciences (NIEHS) initiated the first funding dedicated to obesogens [13]. In the ensuing years, several workshops, reviews, and new research has led to the growth and prominence of this field with trends continuing to this day.
Sources of Obesogens
In recent times, humans are exposed to a vast amount of obesogens present in their everyday lives. According to Endocrine Society, around 1,000 synthetic chemicals are known to be EDCs and interfere with physiological hormonal processes [14]. The most common and well-studied EDCs with obesogenic properties are summarised in table 1. Exposure can be in the form of plastics and plasticisers, pesticides, personal care products, construction materials, food additives and packaging, as well as from industrial pollutants found in the air, water, and soil [15]. While many of these sources were initially developed to improve our quality of life and provide modern conveniences, they have become ubiquitous in our daily lives, making exposure to obesogens almost impossible to avoid.
Exposure among children is of greater concern as they are in a critical window of susceptibility and adverse effects can be long-lasting. They also have a much greater exposure to obesogens when compared to adults as they breath, eat and drink more per body surface area, spend more time inside the house where ECDs are more likely to be found, and engage more frequently in object-to-mouth activities [16].

Table 1.
List of most common obesogens. This table analyses few of the most important obesogens, their source and route of exposure.
Table 1.
List of most common obesogens. This table analyses few of the most important obesogens, their source and route of exposure.
| EDCs | Source | Route of Exposure |
|---|---|---|
| Bisphenol A (BPA) | Use in the manufacturing of various plastics such as food packaging, water bottles, water supply pipes, children’s toys, and electronic appliances [17]. | Inhalation, ingestion, or dermal contact [17]. |
| Phthalates | Belongs to the group of plasticizers used to make plastics more flexible and durable. Found in plastic packaging, children’s toys, personal care products, vinyl flooring materials, clothing, and medical devices [18]. | Inhalation, ingestion, or dermal contact [18]. |
| Dioxins | Unwanted by-products of industrial or (production of herbicides, smelting or bleaching of paper) natural processes (forest fires and volcanic eruptions) [19]. | Highest level of exposure is through food, especially dairy and meat products, shellfish and fish. They are mainly stored in the fat tissue of animals, thus accumulate in the food chain [19]. |
| Tributyltin (TBT) | Biocide used to control a broad spectrum of organisms and used in marine paints, wood preservation and industrial water systems [12]. | Most common contaminant of marine and freshwater ecosystems. Humans exposed through inhalation or consumption of contaminated seafood or water [20]. |
| Atrazine (ATZ) | One of the most widely used herbicides in the world, used to control grasses and broadleaf weeds in corn, sugarcane, and sorghum crops [21]. | Eating or drinking contaminated products, through inhalation or dermal contact [21]. |
| Perchlorate | Manufactured for use in fireworks, explosives, rocket fuel and road flares or naturally occurring in the environment in small amounts [22]. | Inhalation, ingestion, or dermal contact [22]. |
| Per- and polyfluoroalkyl substances (PFAS) | Man-made chemicals resisting heat, water, oil, and grease. Therefore, they are widely used in fire-fighting foams, non-stick cooking pans, food packaging, textile coatings and household products [23]. | PFAS are known to persist in the environment longer than any other man-made chemicals as they break down very slowly. Humans are exposed by consuming PFAS contaminated food or water, through inhalation of contaminated air or by direct exposure with PFASs products [23]. |
| Polybrominated diphenyl ethers (PBDEs) and Polybrominated biphenyls (PBBs) | Chemicals used as flame retardants in wire insulation, electronic devices, upholstery, draperies, rugs, and furniture [24]. | Ingestion (particularly of food high in fat content), inhalation or dermal contact [24]. |
| Triclosan | Used as antibacterial in products such as soaps, toothpaste, body washes and cosmetics [25]. | Ingestion and dermal absorption [25]. |
| Parabens | Chemicals used as preservatives in food, cosmetics, and pharmaceuticals [26]. | Ingestion and dermal absorption [26]. |
| Polycyclic aromatic hydrocarbons (PAH) | Occur naturally in most fossil fuels (coal, gasoline, and crude oil) and are also by-products of incomplete combustion processes [27]. | Inhalation of contaminated air (motor vehicle exhaust, cigarette smoke etc), ingestion (grilled or charred meats or contaminated food) and in some cases dermal absorption [27]. |
Pathophysiology
Mechanism of Action
Obesogens contribute to the development of obesity through various mechanisms. Although there is high heterogeneity amongst mechanisms of action, they all share key characteristics. They are recognised for their ability to mimic the function of natural hormones and interfere with the hormonal balance by binding to cellular or nuclear receptors, altering signalling pathways, cellular responses, and gene expression [28]. Their ability to do so depends on the fact that they possess similar chemical features to natural hormones including a low molecular weight, lipophilicity, and long half-lives. These three properties enable them to diffuse into cells more easily, accumulating in the body and competing with the endocrine system [15].
One of the most well-studied mechanisms through which obesogens exert their effects is that of peroxisome proliferator activated receptor γ (PPARγ) activation. PPARγ is a type of ligand-activated nuclear receptor that plays a crucial role in regulation cellular functions, particularly those related to metabolism and inflammation. It is predominantly found in adipose tissue and regulates the expression of various genes that control adipocyte proliferation and differentiation, glucose metabolism, energy storage, and insulin sensitisation [29]. Activation of PPARγ occurs when endogenous ligands, EDCs, or pharmaceutical drugs bind to it causing it to form a heterodimer with the nuclear receptor 9-cis retinoic acid receptor (RXR). The PPARγ: RXR heterodimer then binds to specific regions on the DNA of target genes called the peroxisome proliferator hormone response elements (PPREs) which cause recruitment of co-transcription factors and subsequent mRNA expression of the target gene [28]. Given its involvement in these metabolic pathways, PPARγ has been an important target for drug development, especially for managing type 2 diabetes and other metabolic conditions. Thiazolidinedione is an example of such drug whose mechanism of PPARγ activation became evident in the mid-1990s [30]. It is an anti-diabetic drug that works by increasing insulin sensitivity with the expense of inducing adipogenesis and weight gain thus supporting the proposed mechanism of obesogens contributing to obesity [30].
Furthermore, obesogens do not contribute to obesity only through the proliferation of adipose tissue but also through the formation of ‘unhealthy’ adipocytes, hormone interference, and increasing inflammatory responses. Healthy white adipocytes are characterised by their preserved insulin sensitivity which facilitates glucose uptake from the circulation and their ability to maintain a balanced inflammatory response, preventing excessive inflammation that can lead to insulin resistance and subsequent metabolic dysfunction. At the same time, healthy adipocytes secrete adipokines such as leptin and adiponectin in appropriate amounts which play a significant role in maintaining metabolic homeostasis. Leptin was first discovered in 1994 by Y Zhang et al and is a hormone responsible for appetite regulation, glucose uptake in the periphery, and thermogenesis in brown adipose tissue [31]. Similarly, adiponectin was first discovered in 1995 by Scherer PE et al, two of its key functions are enhancing insulin sensitivity and having anti-inflammatory properties [32]. It has been found that adipocytes produced under the influence of obesogens have an effect on these hormones thus affecting the hormonal control of satiety and hunger. For example, TBT was found to increase leptin levels and decrease adiponectin levels [33] while di-2-ethylhexyl phthalate (DEHP), the most common type of phthalate, decreased both adiponectin and leptin levels in mice [34]. Similarly, BPA exposure to 3T3-L1 adipocytes in early life was found to increase the levels of leptin mRNA and disrupt the hypothalamic circuit involved in feeding behaviour and energy homeostasis [35]. All the above compound the negative effects of obesogens in dysregulating metabolic processes.
Cohesively, chronic inflammation is a common finding in obesity and obesogens can play a role. Apart from the disruption of adipokine balance mentioned earlier, obesogens like DEHP and BPA have been found to promote inflammation in adipose tissue by increasing the production of reactive oxygen species (ROS) and impairing antioxidant defence mechanisms [36]. It has been suggested that when mesenchymal stem cells are exposed to large numbers of ROS, they have a preference to differentiate into adipocytes thus leading to adipose tissue proliferation [37]. In addition, the imbalance in production of ROS and their detoxification results in oxidative stress which can activate inflammatory signalling pathways and damage cellular structures [36]. Moreover, obesogens can induce inflammation by activating and increasing the number of immune cells in adipose tissues such as lymphocytes and macrophages. These in turn secrete pro-inflammatory cytokines, like interleukin-6 (IL-6) and tumour necrosis factor-alpha (TNF-a), which initiate and sustain an inflammatory response [15,38].
Aside the obesogenic interference with leptin and adiponectin, other hormones are also involved. This includes androgens and oestrogens, which beyond their reproductive functions, play a crucial role in energy homeostasis and adipose tissue function. The exact mechanisms of action of sex steroids, especially oestrogens on metabolism and energy balance are complicated and are out of the scope of this review. In summary, certain obesogens, have the ability to bind to oestrogen and androgen receptors to disrupt their cellular activities and subsequent endocrine system. For example, studies have shown that perinatal exposure of mice to either BPA or DDE led to heavier offspring and rapid weight gain in infants respectively, suggesting their xenoestrogenic properties [39,40]. In addition, other studies found that thyroid receptors may also be unintended targets of obesogens. PBDEs, BPA and phthalates are some of those chemicals with antithyroid properties that can potentially bind to thyroid receptors and interfere with their function. Being a key regulator of metabolism, any alteration in thyroid levels could dysregulate the basal metabolic rate and lead to BMI changes [36,40,41]. The proposed mechanisms are illustrated in figure 1 below.
Pre and Postnatal Effects
Both prenatal and early postnatal life are a pivotal period for child development. Any environmental, maternal, or foetal stressors during this critical window can have profound effects later in life [42]. David Barker proposed a hypothesis that adverse nutrition in early life can increase the risk of metabolic syndrome in adult life. Specifically, he argued that undernutrition during intrauterine life predisposes individuals to conserve calories later in life and increase the likelihood of obesity, when exposed to a calorie-rich postnatal environment [43]. Numerus later studies proved the hypothesis on the role of foetal programming in later life. However, the dramatic rise in paediatric obesity cannot be explained by Baker’s hypothesis alone. Exposure to environmental pollutants during these sensitive periods also comes into play. Numerous animal and epidemiological studies provide evidence supporting the obesogenic impact of early-life exposure to EDCs. One of these is a prospective cohort study involving 412 mother-child pairs from Sweden and Norway, whereby a positive correlation between maternal serum concentrations of perfluoroalkyl substances (PFAS) and higher child BMI was evident at a 5-year follow-up [44]. Similar obesogenic effects have been observed with prenatal exposure to TBT in mice. Offspring of mice exposed to TBT had higher adiposity when compared to those not exposed with similar effects observed in zebrafish, rats, and goldfish [45]. Additionally, another study revealed that higher levels of phthalates detected in maternal urine during pregnancy were associated with a twofold increase in the probability of the offspring being obese [36]. Likewise, maternal exposure to BPA and DDT during pregnancy has been correlated with higher BMI, waist circumference, and risk of obesity in offspring [46,47]. All of the above highlight the dangerous effect of environmental chemicals as obesogens and their impact on human health, particularly during critical periods of development.
Epigenetics
The term epigenetics was first introduced in 1940s by Conrad Waddington and is currently referred to as the study of changes in gene expression that occur without alterations in the underlying DNA sequence i.e. not the result of mutations [48]. These changes can be influenced by various factors, including exposure to EDCs or obesogens during pregnancy or during the early postnatal period. Multiple mechanisms of epigenetic change have been proposed which include DNA methylation, histone modification, and altered microRNA expression [49]. DNA methylation is the most commonly studied mechanism and involves the addition of a methyl group to a specific region of DNA, thereby impacting gene expression. Exposure to obesogens during critical windows of development can lead to changes in expression of genes related to adipogenesis and metabolism [50]. For example, a recent study found that methylation of the cg11531579 island site (CHFR) is associated with accelerated weight gain in early life and the development of obesity [51]. In addition, exposure of obesogens can disrupt histone modifications, which regulate the structure of chromatin and gene expression. If genes involved in metabolic regulation are targeted, the risk of obesity later in life increases [50]. TBT is an example of obesogen found to induce changes to histone methylation in vitro [50]. Similarly, exposure to obesogens can change the expression of miRNAs that are important for lipid metabolism, insulin signalling, and adipocyte differentiation, all of which can lead to the development of obesity [49].
The changes in phenotype that occur secondary to epigenetic modifications can manifest soon after exposure to EDCs or later on. The timing of exposure is particularly important in determining the extent of these changes. On the one hand, if exposure and epigenetic changes occur during early development, an irreversible change occurs in the germline’s epigenome potentially passing on the modified epigenome to future generations. To truly exhibit transgenerational effects, these phenotypes should be evident in the F3 generation as this would be the first generation which was not directly involved to EDC exposure. On the other hand, if epigenetic changes secondary to EDC exposure arise in adulthood, they usually affect the individual’s somatic cells and are neither hereditary nor permanent. Moreover, it is crucial that both the specific tissue and dose of EDCs are taken into consideration before drawing definite conclusions regarding their epigenetic effects [49]. Overall, epigenetic mechanisms provide a framework for understanding how obesogens influence gene expression and metabolic processes to promote obesity. However, further studies are needed to better understand the mechanisms so as to be able to develop strategies and mitigate the impact of obesogens on human health.
Long-Term Effects of Childhood Obesity
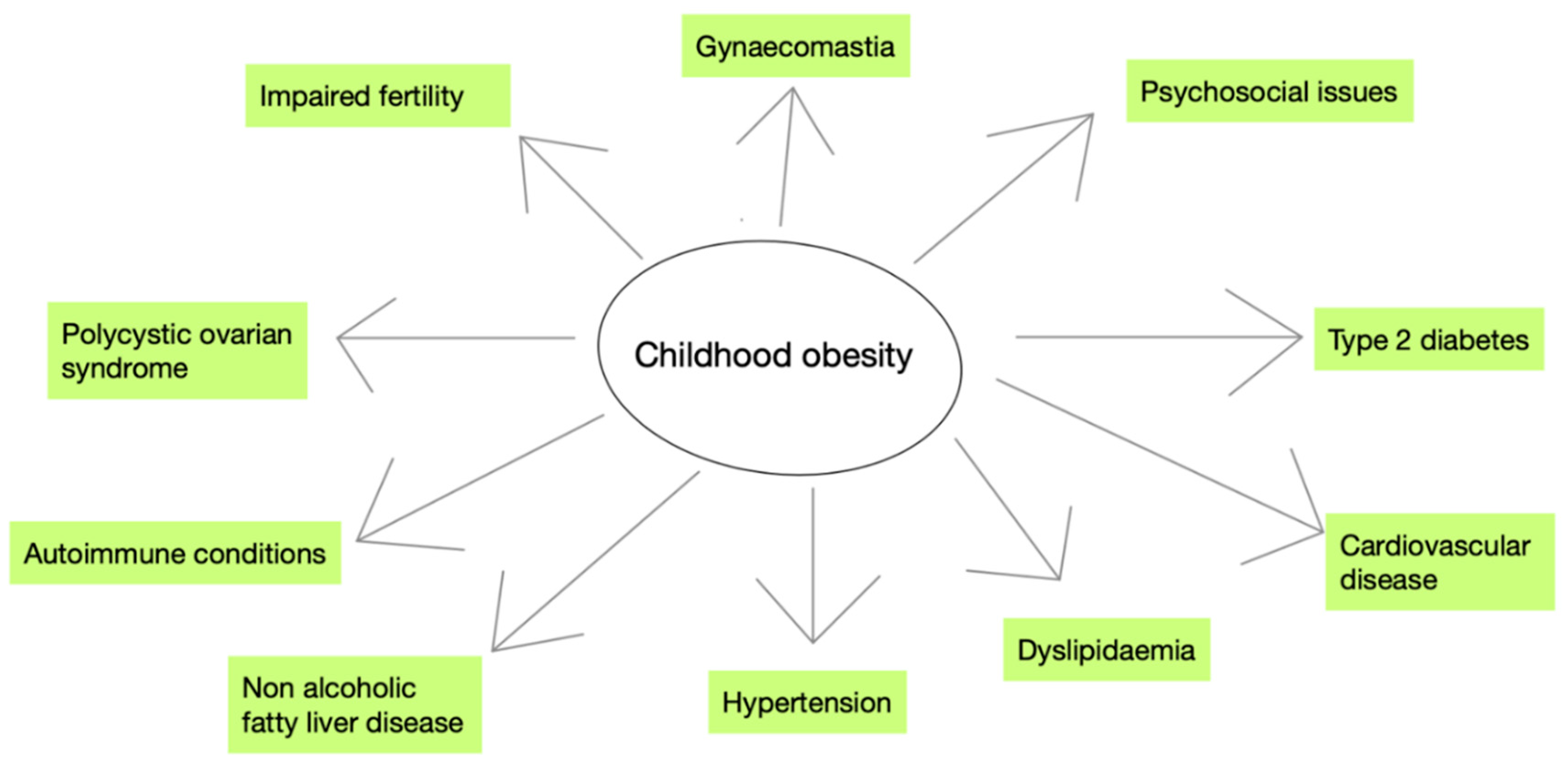
According to the WHO, childhood obesity is one of the most serious public health issues in the 21st century. A wide range of variables interact and nearly every organ system is affected. Irrespective of the underlying causes, childhood obesity can have significant and enduring consequences throughout an individual's life. Long-term consequences include an increased risk of developing chronic health conditions such as type 2 diabetes, cardiovascular disease, dyslipidaemia, and hypertension. Specifically, research shows that at the time of diagnosis, more than 85% of children with type 2 diabetes are overweight or obese [52] and 30-50% of obese adults were also obese during childhood suggesting that the cardiovascular risk factors usually persist in adulthood [53]. Furthermore, 28-41% of obese children and adolescents are found to have non-alcoholic fatty liver disease (NAFLD), making it the most common liver condition in childhood [54]. Additionally, childhood obesity has been associated with increased prevalence and worse prognosis of certain autoimmune conditions such as type 1 diabetes, inflammatory bowel disease, rheumatoid arthritis, psoriasis, and systemic lupus erythematosus [55]. Moreover, obesity increase the risk of polycystic ovarian syndrome (PCOS) in females, gynecomastia in males and reduced fertility in both [55]. Despite the numerous adverse effects in physical health, the psychosocial issues that can arise with childhood obesity should not be underestimated. Children and adolescents who are overweight or obese often encounter challenges with self-esteem and may experience feelings of depression [55]. They are vulnerable to bullying at school with a study confirming that around 45-50% of obese adolescents experience frequent bullying [56]. Additionally, academic performance may be adversely affected, with overweight or obese children typically achieving lower grades and attaining a lower level of education compared to theirpeers of normal weight [55,57]. The aforementioned long-term effects of childhood obesity summarised in figure 2 below.
Prevention Strategies
Preventing obesity nowadays is a great challenge, as Hippocrates said, “preventing is better than cure.” The World Health Organization has caused alarm by recently releasing a new obesity prevention framework which endorses the WHO acceleration Plan to Stop Obesity [58]. The key aim of this strategy is to recognize obesity as a chronic disease and to replace models of obesity comorbidities management with models of obesity prevention starting from early childhood. The framework supports the integration of primary health carers to play a pivotal role in obesity prevention as the frontline health care providers. This is important as prevention must start in infancy or in early childhood, but also much earlier with prenatal programming.
Preventing and managing obesity is no easy task due to previous neglect of the disease individually or/and globally for many years. Multi-sectoral and multi-thematic actions are needed in order to overcome the task; governmental, societal, and individual measures must be adopted. The recognized environmental impact of obesogens on the development and progression of obesity led to the incorporation of specific actions and policies regarding the control of the EDCs that act as obesogens. Nevertheless, years ago Hippocrates recognized that the quality of food has a has a reflective impact on human health by saying ‘let food be thy medicine and medicine be thy food’.
Individual Actions
Individuals and families must follow a balanced diet and include physical activity in their everyday life, where canned and packaged food consumption must be reduced at the minimum. The use of cosmetics containing triclosan, dioxins, parabens and other EDCs also be avoided [59]. Plastic material in general and plastic food containers must be evaded especially prenatally and during neonatal life as plastics can affect not only child’s metabolism but also neurodevelopment [60]. Specifically, families must focus on purchasing labelled phthalate-free products and avoid microwaving or heating food in plastic containers. The US food and Drug administration (FDA) also acclaims that all damaged plastic bottles be discarded, as they may harbour bacteria and lead to more release of BPA. In February 2024, the FDA announced the removal of the EDCs per- and polyfluoroalkyl substances (PFAS) from food packaging [61]. Individuals must read the food container codes in order to avoid such substances. Finally, all individuals must consume organic fruit, vegetables, and grains.
Healthcare Providers’ Actions
Health care providers have a leading role as the frontline carers of children and families. They need to teach families about the importance of a healthy lifestyle throughout life, even starting as early as the prenatal period [62]. Additionally, obstetricians must guide future mothers to avoid contact with EDC lotions, cosmetics, and hair care products, further advising them to eliminate their contact with food in plastics, as well as processed food. Paediatricians must underline the importance of lifestyle modifications including balanced food consumption and physical exercise as early as possible to all children. Paediatricians should especially emphasize the aforementioned to families at a high risk for obesity and its complications due to genetic predispositions [63]. Cohesively, researchers can help by developing models of early recognition of chemical exposure using genomic studies in order to enhance prevention strategies [64].
Community Actions
Societies and governments must firstly recognize the relationship between the obesity pandemic and its associated risks with the early exposure of EDCs in childhood, as environmental obesogens such as thiazolidinediones, organotins, perfluorooctanoic acid, diisobutyl phthalate, and bisphenol A, are still being used worldwide. Urgent development of policies to ban these substances and remove them from the environment must adopted. Actions on a regulatory level are also important for industries that use of EDCs in their products to be banned from the market. Labelling food products, cosmetics and plastics with the ingredients including EDCs shall inform and warn the consumers. European countries have started a practice of becoming ‘greener’ by banning BPA in food packing materials in schools and eliminating the use of obesogenic chemical substances in their industries [65].
Discussion
This literature review delves into the complex issue of childhood obesity, highlighting its significant rise globally and the multitude of factors contributing to its prevalence. The identification of endocrine-disrupting chemicals acting as obesogens and their potential contribution to the obesity epidemic, beyond the prevailing medical explanation of energy imbalances, represents a significant paradigm shift in understanding the aetiology of this multifactorial condition. In contemporary society, approximately 1,000 synthetic compounds were identified as EDCs, 50 of which are obesogens [66]. After analysing some of the most important obesogens, looking into their source and exposure route, we can confidently say that exposure is widespread. They are found in various everyday items such as plastics, pesticides, personal care products, and food additives which makes them hard to avoid given the ubiquity of these sources. To reiterate, children are particularly vulnerable as they are in a critical developmental stage, the issue is further compounded given their higher levels of exposure; due to behaviours such as mouthing objects, and the fact that they spend more time indoors where EDCs are more prevalent.
Obesogens contribute to obesity through various mechanisms, all characterized by their ability to mimic natural hormones and disrupt hormonal balance. The fact that they share similar chemical properties to hormones, enables them to interfere with cellular receptors and signalling pathways, thus altering gene expression. On most well-studied mechanisms discussed in this review involves the activation of the PPARγ nuclear receptor, which is crucial for metabolic regulation; its activation can lead to adipogenesis and subsequent weight gain. Different mechanisms such as adipose tissue dysfunction, hormonal interference and inflammation were also examined. Obesogens are able to disrupt the balance of adipokines like leptin and adiponectin, affecting satiety control and metabolic homeostasis and at the same time promote inflammation in adipose tissue by increasing reactive oxygen species production and activation of immune cells. Furthermore, they can interfere with other hormones like androgens, oestrogens, and thyroid hormones, affecting energy homeostasis and metabolic function, thus increasing vulnerability to obesity. However, our understanding on these mechanisms is not absolute and a more comprehensive understanding is required. This will allow us to establish effective management plans in the future and mitigate their adverse effects on human health.
In addition, the review underscores the importance of considering both prenatal and postnatal exposure to obesogens in shaping long-term health outcomes. Evidence from both animal and epidemiological studies suggests that maternal exposure to EDCs during pregnancy correlates with increased adiposity in offspring and can dysregulate metabolic pathways and hormonal control systems in the foetus or infant, ultimately predisposing them to obesity [36,44,45,46,47]. Epigenetic mechanisms were also discussed, elucidating how exposure to obesogens during critical periods of development can induce lasting changes in gene expression, contributing to the intergenerational transmission of obesity-related traits.
The myriad long-term consequences of childhood obesity were highlighted, emphasizing its multifaceted impact on various organ systems. It can lead to enduring health consequences, including an increased risk of developing chronic conditions like type 2 diabetes, cardiovascular disease, dyslipidaemia, and hypertension. Current literature indicates a strong association between childhood obesity and the persistence of cardiovascular risk factors into adulthood which creates a vicious cycle of metabolic and other diseases. Non-alcoholic fatty liver disease (NAFLD) was also found to be prevalent among obese children, while obesity exacerbates autoimmune conditions and increases the risk of reproductive problems in both males and females. Importantly, this review highlights the psychosocial ramifications of obesity, including diminished self-esteem, depression, and academic underachievement, underscoring the need for comprehensive interventions that address both the physical and emotional well-being of affected individuals; adopting a biopsychosocial approach in treatment and management.
In light of these findings, we advocated for a multi-faceted approach to obesity prevention, encompassing individual, healthcare provider, and community-level strategies. Individual actions, such as adopting a balanced diet, reducing exposure to EDCs, and promoting physical activity, are essential components of obesity prevention from an early age. Healthcare providers play a crucial role in educating families about the importance of lifestyle modifications and early intervention, particularly in high-risk populations. Moreover, community-wide initiatives, including regulatory policies to restrict the use of obesogenic chemicals, labelling of products containing EDCs, and promoting sustainable and environmentally friendly practices, are imperative for reducing the obesity epidemic at a population level.
Conclusions
In conclusion, this literature review underscores the urgent need for a holistic approach to combat childhood obesity, acknowledging the multifactorial nature of the condition and the critical role of environmental factors such as obesogens. By addressing the complex interplay between genetic predisposition, environmental exposures, and lifestyle factors, stakeholders can work towards implementing effective prevention strategies and mitigating the long-term health consequences associated with obesity.
Future Directions
While there have been significant advancements in understanding the different types, numbers, and mechanisms of action of obesogens, there still remains a considerable amount to discover regarding their overall impact on obesity vulnerability. One area in which current literature is lacking is how obesogens may interact with nutrients in the diet to promote obesity. In addition, the influence of obesogens on the gut’s microbiome composition and its contribution to obesity is not well-understood and may potentially offer innovative approaches for treating obesity. Another challenge is comprehending the effects of exposure to a combination of obesogens—whether they produce additive or synergistic effects, or hinder each other's actions. In essence, all these important questions need to be addressed as this knowledge will be instrumental in devising strategies to prevent or minimize exposure to these harmful substances. The European Union made an important effort by funding eight international consortia through its Horizon 2020 grant program to examine EDCs, three of which specifically focus on developing techniques to identify obesogens [50,67]. These efforts are expected to yield fruitful results as they aim to identify the complete range of obesogens and understand their mechanisms of action. Moreover, although the use of animal models and screening assays so far has been fundamental, results cannot be extrapolated confidently in relation to humans. Thus, in the future, it would be beneficial to aim for longitudinal studies on humans which will provide a more robust data set with more valid results. Ultimately, all of the aforementioned initiatives seek to provide healthcare professionals and the public with a thorough understanding of the dangers associated with obesogens exposure. This will enable them to make informed decisions and implement changes that will minimize exposure and mitigate health risks, combating the obesity pandemic.
References
- Jebeile H, Kelly AS, O’Malley G, Baur LA. Obesity in children and adolescents: Epidemiology, causes, assessment, and Management. The Lancet Diabetes & Endocrinology. 2022 May;10(5):351–65. [CrossRef]
- Defining child BMI categories [Internet]. Centers for Disease Control and Prevention; 2023 [cited 2023 Dec 13]. Available from: https://www.cdc.gov/obesity/basics/childhood-defining.html.
- Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. The Lancet. 2017 Dec;390(10113):2627–42. [CrossRef]
- Global atlas on childhood obesity [Internet]. [cited 2023 Dec 14]. Available from: https://www.worldobesity.org/membersarea/global-atlas-on-childhood-obesity.
- Pulgarón, ER. Childhood obesity: A review of increased risk for physical and psychological comorbidities. Clinical Therapeutics. 2013 Jan;35(1). [CrossRef]
- Locke AE, Kahali B, Berndt SI, Justice AE, Pers TH, Day FR, et al. Genetic studies of body mass index yield new insights for Obesity Biology. Nature. 2015 Feb 11;518(7538):197–206. [CrossRef]
- Obesity and overweight [Internet]. World Health Organization; [cited 2023 Dec 16]. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- Endocrine Society. Endocrine-disrupting chemicals (edcs) [Internet]. Endocrine Society; 2022 [cited 2023 Dec 16]. Available from: https://www.endocrine.org/patient-engagement/endocrine-library/edcs.
- Grün F, Blumberg B. Environmental obesogens: Organotins and endocrine disruption via nuclear receptor signaling. Endocrinology. 2006 Jun 1;147(6). [CrossRef]
- Baillie-Hamilton, PF. Chemical toxins: A hypothesis to explain the global obesity epidemic. The Journal of Alternative and Complementary Medicine. 2002 Apr;8(2):185–92. [CrossRef]
- Grün F, Blumberg B. Endocrine disrupters as obesogens. Molecular and Cellular Endocrinology. 2009 May 25;304(1–2):19–29. [CrossRef]
- PubChem [Internet]. Bethesda (MD): National Library of Medicine (US), National Center for Biotechnology Information; 2004-. PubChem Compound Summary for CID 3032732, Tributyltin; [cited 2023 Dec. 16]. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Tributyltin.
- PAR-11-171: Role of Environmental Chemical Exposures in the development of obesity, type 2 diabetes and metabolic syndrome (R21) [Internet]. U.S. Department of Health and Human Services; [cited 2023 Dec 20]. Available from: https://grants.nih.gov/grants/guide/pa-files/PAR-11-171.html.
- Endocrine Society. Common edcs and where they are found [Internet]. Endocrine Society; 2019 [cited 2023 Dec 20]. Available from: https://www.endocrine.org/topics/edc/what-edcs-are/common-edcs.html.
- Micic, D. Endocrine disrupting chemicals and obesity: The evolving story of obesogens. Acta Endocrinologica (Bucharest). 2021;17(4):503–8. [CrossRef]
- Di Pietro G, Forcucci F, Chiarelli F. Endocrine disruptor chemicals and children’s health. International Journal of Molecular Sciences. 2023 Jan 31;24(3):2671. [CrossRef]
- Bisphenol A (BPA) [Internet]. U.S. Department of Health and Human Services; [cited 2023 Dec 20]. Available from: https://www.niehs.nih.gov/health/topics/agents/sya-bpa.
- Phthalates factsheet [Internet]. Centers for Disease Control and Prevention; 2021 [cited 2023 Dec 21]. Available from: https://www.cdc.gov/biomonitoring/Phthalates_FactSheet.html.
- Dioxins [Internet]. World Health Organization; [cited 2023 Dec 22]. Available from: https://www.who.int/news-room/fact-sheets/detail/dioxins-and-their-effects-on-human-health.
- Bandara KRV, Chinthaka SDM, Yasawardene SG, Manage PM. Modified, optimized method of determination of tributyltin (TBT) contamination in coastal water, sediment and biota in Sri Lanka. Marine Pollution Bulletin. 2021 May;166:112202. [CrossRef]
- Atrazine [Internet]. Environmental Protection Agency; [cited 2023 Dec 23]. Available from: https://www.epa.gov/ingredients-used-pesticide-products/atrazine.
- Niziński P, Błażewicz A, Kończyk J, Michalski R. Perchlorate – properties, toxicity and human health effects: An updated review. Reviews on Environmental Health. 2020 Sept 4;36(2):199–222. [CrossRef]
- Perfluoroalkyl and Polyfluoroalkyl Substances (PFAS) [Internet]. U.S. Department of Health and Human Services; [cited 2023 Dec 23]. Available from: https://www.niehs.nih.gov/health/topics/agents/pfc.
- Polybrominated diphenyl ethers (pbdes) and polybrominated biphenyls (pbbs) factsheet [Internet]. Centers for Disease Control and Prevention; 2017 [cited 2024 Jan 3]. Available from: https://www.cdc.gov/biomonitoring/PBDEs_FactSheet.html.
- Commissioner O of the. 5 things to know about triclosan [Internet]. FDA; 2019 [cited 2024 Jan 3]. Available from: https://www.fda.gov/consumers/consumer-updates/5-things-know-about-triclosan.
- Parabens factsheet [Internet]. Centers for Disease Control and Prevention; 2023 [cited 2024 Jan 3]. Available from: https://www.cdc.gov/biomonitoring/Parabens_FactSheet.html.
- Polycyclic aromatic hydrocarbons (pahs): Where are pahs found? [Internet]. Centers for Disease Control and Prevention; 2023 [cited 2024 Jan 3]. Available from: https://www.atsdr.cdc.gov/csem/polycyclicaromatic-hydrocarbons/where_are_pahs_found.html.
- Griffin MD, Pereira SR, DeBari MK, Abbott RD. Mechanisms of action, chemical characteristics, and model systems of obesogens. BMC Biomedical Engineering. 2020 Apr 30;2(1). [CrossRef]
- Tyagi S, Sharma S, Gupta P, Saini A, Kaushal C. The peroxisome proliferator-activated receptor: A family of nuclear receptors role in various diseases. Journal of Advanced Pharmaceutical Technology & Research. 2011;2(4):236. [CrossRef]
- Soccio RE, Chen ER, Lazar MA. Thiazolidinediones and the promise of insulin sensitization in type 2 diabetes. Cell Metabolism. 2014 Oct;20(4):573–91. [CrossRef]
- Zhang Y, Proenca R, Maffei M, Barone M, Leopold L, Friedman JM. Positional cloning of the mouse obese gene and its human homologue. Nature. 1994 Dec;372(6505):425–32. [CrossRef]
- Scherer PE, Williams S, Fogliano M, Baldini G, Lodish HF. A novel serum protein similar to C1Q, produced exclusively in adipocytes. Journal of Biological Chemistry. 1995 Nov;270(45):26746–9. [CrossRef]
- Yan H, Guo H, Cheng D, Kou R, Zhang C, Si J. Tributyltin reduces the levels of serum adiponectin and activity of Akt and induces metabolic syndrome in male mice. Environmental Toxicology. 2018 Apr 20;33(7):752–8. [CrossRef]
- Schmidt J-S, Schaedlich K, Fiandanese N, Pocar P, Fischer B. Effects of di(2-ethylhexyl) Phthalate (DEHP) on female fertility and adipogenesis in C3H/N mice. Environmental Health Perspectives. 2012 Aug;120(8):1123–9. [CrossRef]
- MacKay H, Patterson ZR, Abizaid A. Perinatal exposure to low-dose bisphenol-a disrupts the structural and functional development of the hypothalamic feeding circuitry. Endocrinology. 2017 Feb 7;158(4):768–77. [CrossRef]
- Shahnazaryan U, Wójcik M, Bednarczuk T, Kuryłowicz A. Role of obesogens in the pathogenesis of obesity. Medicina. 2019 Aug 21;55(9):515. [CrossRef]
- Bateman ME, Strong AL, McLachlan JA, Burow ME, Bunnell BA. The effects of endocrine disruptors on adipogenesis and osteogenesis in Mesenchymal Stem Cells: A Review. Frontiers in Endocrinology. 2017 Jan 9;7. [CrossRef]
- Ricote M, Li AC, Willson TM, Kelly CJ, Glass CK. The peroxisome proliferator-activated receptor-γ is a negative regulator of macrophage activation. Nature. 1998 Jan;391(6662):79–82. [CrossRef]
- Heindel JJ, Blumberg B, Cave M, Machtinger R, Mantovani A, Mendez MA, et al. Metabolism disrupting chemicals and metabolic disorders. Reproductive Toxicology. 2017 Mar;68:3–33. [CrossRef]
- Griffin MD, Pereira SR, DeBari MK, Abbott RD. Mechanisms of action, chemical characteristics, and model systems of obesogens. BMC Biomedical Engineering. 2020 Apr 30;2(1). [CrossRef]
- Knudsen N, Laurberg P, Rasmussen LB, Bülow I, Perrild H, Ovesen L, et al. Small differences in thyroid function may be important for body mass index and the occurrence of obesity in the population. The Journal of Clinical Endocrinology & Metabolism. 2005 Jul;90(7):4019–24. [CrossRef]
- Heindel JJ, Blumberg B. Environmental obesogens: Mechanisms and controversies. Annual Review of Pharmacology and Toxicology. 2019 Jan 6;59(1):89–106. [CrossRef]
- Barker DJ, Gluckman PD, Godfrey KM, Harding JE, Owens JA, Robinson JS. Fetal nutrition and cardiovascular disease in adult life. Lancet. 1993 Apr 10;341(8850):938-41. [CrossRef] [PubMed]
- Lauritzen HB, Larose TL, Øien T, Sandanger TM, Odland J, van de Bor M, et al. Prenatal exposure to persistent organic pollutants and child overweight/obesity at 5-year follow-up: A prospective cohort study. Environmental Health. 2018 Jan 18;17(1). [CrossRef]
- Egusquiza, Riann & Blumberg, Bruce. (2020). Environmental Obesogens and Their Impact on Susceptibility to Obesity: New Mechanisms and Chemicals. Endocrinology. 161. 10.1210/endocr/bqaa024.
- Valvi D, Casas M, Mendez MA, Ballesteros-Gómez A, Luque N, Rubio S, et al. Prenatal bisphenol A urine concentrations and early rapid growth and overweight risk in The offspring. Epidemiology. 2013 Nov;24(6):791–9. [CrossRef]
- Cano-Sancho G, Salmon AG, La Merrill MA. Association between exposure to p,p′-DDT and its metabolite p,p′-DDE with obesity: Integrated systematic review and meta-analysis. Environmental Health Perspectives. 2017 Sept 22;125(9). [CrossRef]
- Dupont C, Armant D, Brenner C. Epigenetics: Definition, mechanisms, and clinical perspective. Seminars in Reproductive Medicine. 2009 Aug 26;27(05):351–7. [CrossRef]
- Gore AC, Chappell VA, Fenton SE, Flaws JA, Nadal A, Prins GS, et al. EDC-2: The endocrine society’s second scientific statement on endocrine-disrupting chemicals. Endocrine Reviews. 2015 Dec 1;36(6). [CrossRef]
- Egusquiza RJ, Blumberg B. Environmental obesogens and their impact on susceptibility to obesity: New mechanisms and chemicals. Endocrinology. 2020 Feb 18;161(3). [CrossRef]
- Robinson N, Brown H, Antoun E, Godfrey KM, Hanson MA, Lillycrop KA, et al. Childhood DNA methylation as a marker of early life rapid weight gain and subsequent overweight. Clinical Epigenetics. 2021 Jan 12;13(1). [CrossRef]
- Type 2 diabetes in children and adolescents. American Diabetes Association. Diabetes Care. 2000 Mar 1;23(3):381–9. [CrossRef]
- Simmonds M, Llewellyn A, Owen CG, Woolacott N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obesity Reviews. 2015 Dec 23;17(2):95–107. [CrossRef]
- Anderson EL, Howe LD, Jones HE, Higgins JP, Lawlor DA, Fraser A. The prevalence of non-alcoholic fatty liver disease in children and adolescents: A systematic review and meta-analysis. PLOS ONE. 2015 Oct 29;10(10). [CrossRef]
- Marcus C, Danielsson P, Hagman E. Pediatric obesity—long-term consequences and effect of weight loss. Journal of Internal Medicine. 2022 Aug 5;292(6):870–91. [CrossRef]
- Neumark-Sztainer D, Falkner N, Story M, Perry C, Hannan P, Mulert S. Weight-teasing among adolescents: Correlations with weight status and disordered eating behaviors. International Journal of Obesity. 2002 Jan;26(1):123–31. [CrossRef]
- Karnehed N, Rasmussen F, Hemmingsson T, Tynelius P. Obesity and attained education: Cohort Study of more than 700,000 Swedish men. Obesity. 2006 Aug;14(8):1421–8. [CrossRef]
- Health service delivery framework for prevention and management of obesity. Geneva: World Health Organization; 2023.
- Lobstein T, Brownell KD. Endocrine-disrupting chemicals and obesity risk: A review of recommendations for obesity prevention policies. Obesity Reviews. 2021; 22(11):e13332. [CrossRef]
- Braun, JM. Early-life exposure to EDCs: role in childhood obesity and neurodevelopment. Nat Rev Endocrinol. 2017;13(3):161-173. [CrossRef]
- FDA Removes Harmful Chemicals From Food Packaging - Medscape - February 29, 2024.
- Fernandez-Twinn DS, Hjort L, Novakovic B, Ozanne SE, Saffery R. Intrauterine programming of obesity and type 2 diabetes. Diabetologia. 2019;62(10):1789-1801. [CrossRef]
- Russ K, Howard S. Developmental exposure to environmental chemicals and metabolic changes in children. Curr Probl Pediatr Adolesc Health Care. 2016;46(8):255-285. [CrossRef]
- Heindel JJ, Howard S, Agay-Shay K, Arrebola JP, Audouze K, Babin PJ, et al. Obesity II: Establishing causal links between chemical exposures and Obesity. Biochemical Pharmacology. 2022 May; 199:115015. [CrossRef]
- World Health Organization. Action Plan for the Prevention and Control of Noncommunicable Diseases in the WHO European Region 2016– 2025. Copenhagen: WHO Regional Office for Europe; 2016.
- Heindel JJ, Blumberg B. Environmental obesogens: Mechanisms and controversies. Annual Review of Pharmacology and Toxicology. 2019 Jan 6;59(1):89–106. [CrossRef]
- Horizon 2020 [Internet]. European Commission; [cited 2024 Mar 28]. Available from: https://research-and-innovation.ec.europa.eu/funding/funding-opportunities/funding-programmes-and-open-calls/horizon-2020_en.
Figure 1.
Mechanism of action of obesogens. Diagram depicting established mechanisms and impacts of exposure to obesogens. This includes the activation of PPARγ nuclear receptor, hormonal interference, increase in inflammation and dysregulation of the endocrine
Figure 1.
Mechanism of action of obesogens. Diagram depicting established mechanisms and impacts of exposure to obesogens. This includes the activation of PPARγ nuclear receptor, hormonal interference, increase in inflammation and dysregulation of the endocrine
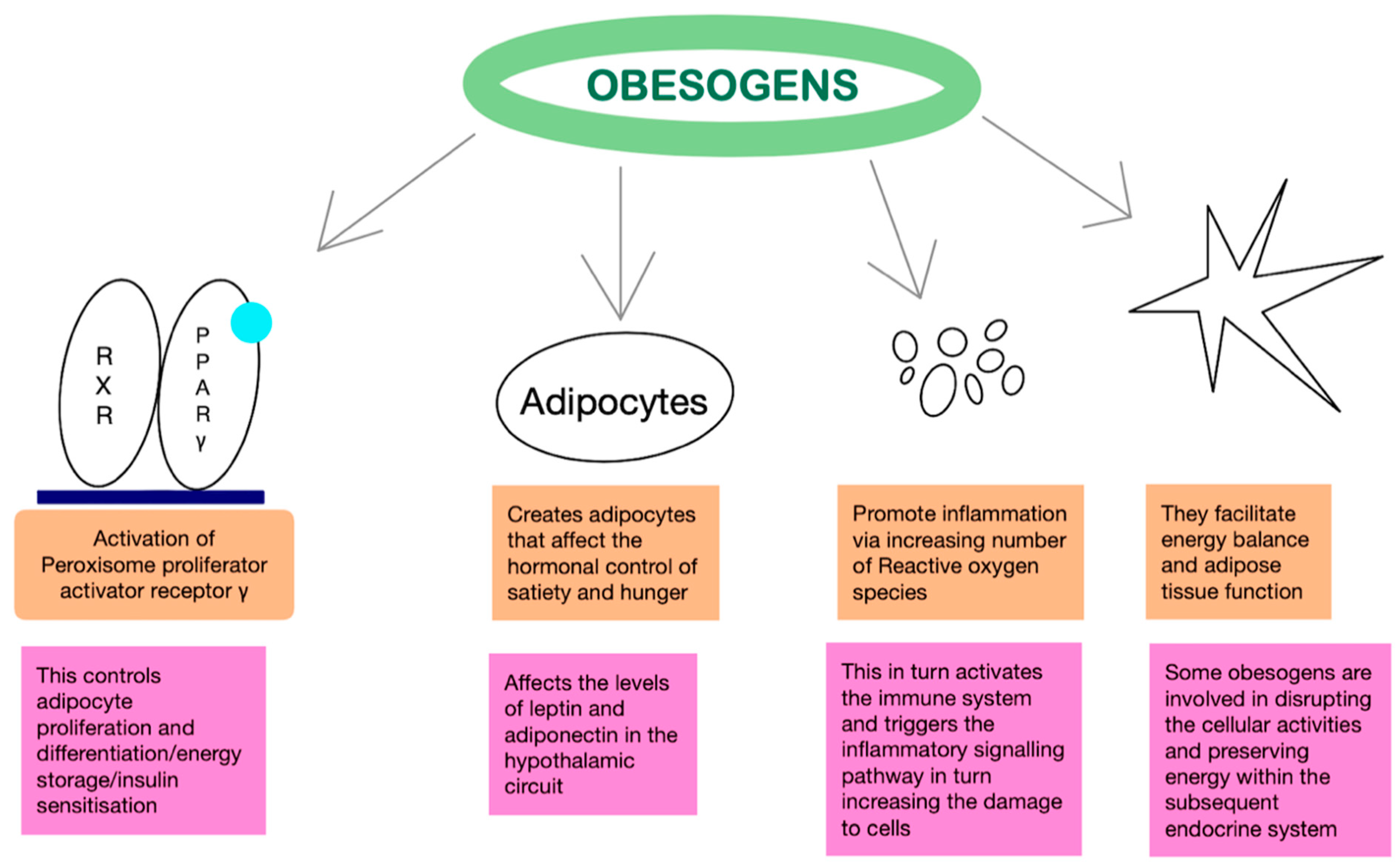
Figure 2.
Long-term effects of childhood obesity. This figure summarises the most important implications of childhood obesity both on the physical and psychosocial.
Figure 2.
Long-term effects of childhood obesity. This figure summarises the most important implications of childhood obesity both on the physical and psychosocial.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



