
Submitted:
04 April 2024
Posted:
07 April 2024
You are already at the latest version
Abstract
Spinal cord stimulation (SCS) is a therapeutic modality for the treatment of various chronic pain conditions that has rapidly evolved over the past 50 years. Unfortunately, over time, patients implanted with SCS undergo a habituation phenomenon leading to decreased pain relief. Consequently, discovery of new stimulation waveforms and SCS applications have shown to prolong efficacy and reduce explantation rates. This article explores various SCS waveforms, their applications and proposes a graded approach to habituation mitigation. We suspect the neural habituation phenomenon parallels that seen in pharmacology. Consequently we urge further exploration of early introduction of these stimulation strategies to abate spinal cord stimulation habituation.
Keywords:
spinal cord stimulator
; neuromodulation
; explant
; chronic pain
; waveform
; habituation
1. Introduction
Chronic pain is a debilitating condition that effects the quality of life of approximately 51 million adults in the United States (20.5% of the population). Its economic impact is estimated to range from $560 to $635 billion per a year in healthcare expenditure and lost productivity [1,2,3]. The prevalence of chronic pain - specifically chronic back pain - continues to increase, outpacing the prevalence of cancer, heart disease, and diabetes combined [4]. There are a multitude of treatment options for chronic pain, each with their own associated risks, thus making chronic pain management a complex undertaking. Current options include pharmacological therapy, surgery, minimally invasive procedures, physiotherapy, psychological and behavioral treatments, or multimodal treatment [5]. Specifically, within the past few decades, there has been a rise in the use of spinal cord stimulators (SCS) as a treatment option for chronic pain patients - approximately 34,000 SCS are implanted annually around the world [6].
The first spinal cord stimulator was implanted to alleviate cancer-related pain in 1967 by Shealy and colleagues [7]. In the following years, SCS technology has evolved considerably and is considered a minimally invasive treatment for a wide array of indications. Most commonly implantations are performed for chronic, intractable pain secondary to failed back surgery syndrome (FBSS), complex regional pain syndrome (CRPS) [8], neuropathy [9], and low back pain not amenable to surgery [10,11]. A spinal cord stimulator is composed of a battery and pulse generator system which attaches to spinal epidural electrode arrays known as leads. These leads are snaked up the epidural space to the vertebral level where the nociceptive region receives its neuronal innervation. There, the leads deliver electrical impulses that inhibit the transmission of the pain signals traveling along the spinal cord to the brain [12].
There have been numerous advancements in SCS over the past fifty years such as improvements in device hardware, electrode technology, and stimulation delivery [13]. In addition, novel stimulation waveform paradigms - differing in frequency, duration (pulse width) and amplitude - have improved efficacy [14]. Although there has been tremendous growth in this space, there is a dearth of studies analyzing long-term efficacy of SCS. Specifically, patients have reported diminished pain control over time which is also notably the most common reason for device explantation [15,16,17]. To address this phenomenon, known as habituation, a combination of techniques centering around stimulation waveform modification (deemed salvage therapy) have been proposed [18]. In this review we explore contributors to habituation phenomenon and posit that the early initiation of waveform variability can decrease rate of explantation due to therapeutic failure.
2. Understanding Spinal Cord Stimulation and Waveforms
The initial indication for spinal cord stimulation discovery in the 1960’s was for the treatment of chronic neuropathic pain. Electrical current was delivered as a constant (tonic) to the spinal cord. The efficacy of tonic stimulation is based on the Gate Control Theory of pain transmission proposed by Melzack and Wall. The theory states that stimuli to the brain via neural pathways is modulated via “gates” [19]. Generally, pain signals are conducted on primary small-fiber afferent nerves while other stimuli (eg non-pain sensations) are conducted via large fiber interneurons. If one were to continually stimulate the large-fiber interneurons, there would be a “blockage of the gate” thus preventing small-fiber afferent transmission of pain signals to the brain.
Important parameters to consider in the delivery of energy by SCS are amplitude, frequency and duty cycle. Amplitude indicates current intensity, frequency is the rate at which stimulation is delivered and duty cycle is the ratio of the pulse width to pulse duration. A variation of these variables has enabled the development of different waveforms discussed below.
2.1. Conventional/ Tonic Stimulation
Tonic SCS, also known as conventional SCS, (cSCS) capitalizes on this principle by delivering a constant stream of pulses that are perceived as a paresthesia or tingling carried by large-fiber interneurons. These sensations effectively block pain perception at a targeted vertebral level. Tonic stimulation is characterized by having a high amplitude above sensory threshold (3.6-8.5 mA), low frequency (40-100 Hz), and pulse widths ranging from 300-600 µs [20]. The goal is to obtain fifty-percent reduction in pain or greater with cSCS – a target achieved by nearly half of all patients implanted [23].
One of the challenges of cSCS is the need for accurate coverage of the nociceptive area while accounting for spinal anatomy and neurophysiology [21,22]. Occasionally patients report uncomfortable paresthesia or unpleasant stimulation associated with changes in posture [24,25]. With regard to duration of pain relief, several studies have reported that cSCS provides analgesia in patients with low back and leg pain for six months [15,23] to one year [26]. Similarly, a systematic review published in 1995 reported that 62% of patients had pain relief upwards of one year after implantation. However, a downtrend in pain relief was observed with ratings of 53% relief at five years and 35% relief 10 years after the implant [27]. Similarly, a 2002 prospective study reported significant pain relief as far along as two years after SCS implantation. However, at both 30 month and 48 month follow ups, pain scores were significantly worse [28]. Given decreased pain-relieving effects over time and potential complication of uncomfortable paresthesia, innovative alternatives have evolved to address the shortcomings of tonic SCS.
2.2. High Frequency Stimulation
High frequency SCS (HF-SCS) is one alternative method used to produce paresthesia-free pain relief. HF-SCS utilizes short duration pulses of stimulation (30 µs) at high frequency (1-10 kHz) and amplitudes (1-5 mA) below the sensory threshold [29]. Since high frequency stimulation is below the sensory threshold, patients do not report feeling paresthesia at target sites. This development broadened the scope of SCS application, specifically for treatment of chronic low back pain which had previously been elusive to treat with SCS [30]. Several randomized controlled trials have reported superiority of HF-SCS compared to conventional/tonic stimulation in measures such as quality of life, pain intensity, functional outcomes and decrease in opioid use [17,31]. For example, patients treated with HF-SCS had a 67% decrease in their mean back pain score (as characterized on Visual Analog Scale for pain intensity) compared to only 44% score decrease in patients treated with cSCS over a twelve month period [17]. Furthermore, HF-SCS has been reported to have clinically significant and sustained pain relief one [32], two [31,33], and three years [34] after implantation.
2.3. Burst Stimulation
Burst stimulation programming was introduced by De Ridder and collogues in 2010. It cycles through a short interval of high frequency (500 Hz) stimulation followed by a pulse-free charge phases and then a rest phase for recharge [35]. The rest phase is thought to mimic the natural neuronal firing pattern involved in pain processing - thus allowing for exogenous control of pain signals free of paresthesia. The clinical efficacy of burst SCS on various pain conditions has been reported in several prospective and cohort-designed studies as noted in Kirketieg et al [36]. Similar to HF-SCS, burst SCS has been reported to be superior in pain relief and preferred by patients compared to cSCS [37,38]. In 2016 De Ridder et al. reported that burst stimulation was able to improve back, limb, and general pain by 51%, 53%, and 55% respectively compared to 30%, 52%, and 31% respectively by tonic stimulation [39]. Small sample observational studies have compared burst stimulation and HF-SCS in reducing pain score in individuals suffering from low back pain. Two studies reported equivalent immediate efficacy in back and leg pain reduction between high frequency and burst waveforms [40,41]. Of note, burst SCS was superior to HF-SCS in reducing leg pain at 3 months [40] and 12 months[41]. Interestingly, burst stimulation was also noted to have positive effects on patient affect and emotions. Researchers post this may be due to neuromodulation of brain regions involved in pain processing [39,42,43].
2.4. Intermittent Dosing Burst Paradigm
The superiority of burst SCS as compared to cSCS has been well established. In an effort to make burst stimulation more efficient, researchers set forth to investigate if limiting the amount of time burst stimulation is active (ON) and inactive (OFF) (duty cycle) can provide a sustained therapeutic effect. The benefit would be twofold: possibly increased time before habituation and decreased energy consumption for stimulation [44]. In 2019, Vesper et al. compared burst SCS to intermittent dosing (also known as microdosing) burst SCS in alternating cycles of five seconds ON and five to ten seconds OFF. They found no significant difference in reported pain relief or quality of life [44]. This was further investigated by Deer et al. who had patients undergo a trial pattern of thirty seconds ON and ninety seconds OFF. Patients were then instructed to select the longest tolerable OFF period that achieved pain control similar to that of the trial period (90, 120, 150, 240, or 360 seconds). After six-months, 45.8% of patients were using the 360 second OFF period and the remainder of the patients were evenly distributed among the shorter OFF periods. Comparing the different prolonged OFF period groups amongst each other and to trial period, patients did not report significant exacerbation of pain, decrease in quality of life, or increased pain catastrophizing [45]. Therefore, this study demonstrates that intermittent burst SCS can be bespoke to provide optimal pain relief and reduce the amount of stimulatory electrical current. Unlike cSCS, the long-term efficacy of intermittent burst SCS has not been thoroughly studied.
3. Closed-Loop Spinal Cord Stimulation
As previously discussed, the electrodes at the end of the leads are fixed in the epidural space, however, the spinal cord is constantly changing position with even the smallest of physical movements (breathing, coughing, sitting, standing) [46]. These movements cause changes in the distance between the electrode and spinal cord resulting in large changes in the amount of current transmitted to neural tissue [47,48]. This is known as an open-loop system; there is no autofeedback mechanism for the stimulator to adapt for positional changes. The risk is delivery of inconsistent therapy with the potential for unwanted side effects or, more significantly, loss of efficacy leading to explantation [49]. To address these limitations, a closed-loop neuromodulation system was developed to continuously measure electrophysiological and postural changes and adjust the stimulation dose [50].
The safety and efficacy of the closed-loop SCS system in patients with leg and low back pain has been reported in several studies [49,50]. Russo et al. reported that at twelve months post-implantation more than seventy-five percent of patients had ≥50% back, leg, and overall pain relief, and more than half of these patients had ≥80% pain relief [51]. Additionally, the superiority of closed-loop to open-loop SCS as measured by improvement in leg and back pain relief has been demonstrated. Mekhail et. al reported that a greater proportion of closed-loop SCS patients had ≥50% relief in overall pain compared to open-loop patients at three months (82.3% vs 60.3% respectively), twelve months (83.1% vs 61.0% respectively), and twenty-four months (79.1% vs 53.7% respectively) post implantation [47,49]. Additionally, closed-loop SCS has demonstrated marked improvements in patient’s health-related quality of life, physical and emotional functioning, and a reduction or complete elimination in opioid use at 24 months [50,52].
4. Habituation and Spinal Cord Stimulator Explantation
Although SCS is an effective therapeutic option for various chronic pain conditions, rates of explantation have noted to increase after the first year of implantation [53,54]. In an observational, nonrandomized, retrospective study of over seventy-nine thousand Medicare beneficiaries who received rechargeable SCS from 2013 to 2020, at one, three, five, and seven years post implantation there was a 5.1%, 12.5%, 17.6%, and 22.0% cumulative incidence of explantation respectively [54]. One of the most frequent reasons for explantation is inadequate pain control. Simopoulos et al. reported that in a sample pool of two hundred fifty-two SCS patients, a total of 30% had their device removed with 28% of those undergoing removal citing ineffective pain control as the reason [55]. Further, Van Buten et al. reported that there was a 7.9% annual explantation rate in a study of nine hundred fifty-five SCS patients. Half of those patients reported inadequate pain relief prior to explantation [56]. More recently, a study by Al-Kaisy et al. performed a retrospective analysis on 182 patients implanted with a neuromodulation device such as SCS and reported explantation rate of 17.8% at 5 years and 25.2% at 10 years. The most common reason for explantation was loss of efficacy (65%) with rates of explantation reported to be 13.3% at 5 years and 17.5% at 10 years regardless of indication [57].
Individuals that report loss of efficacy from SCS are thought to experience habituation, which is described as the progressive loss of pain control despite initial analgesic success and appropriate stimulation that cannot be explained by hardware-related issues [58,59]. Habituation has been reported to effect 13-25.9% of SCS patients [60]. The biological etiology of habituation is not well understood. Many physiological, pathological and psychological factors have been suggested along with neuronal plasticity being a major contributing factor [61,62,63]. The onset of therapy habituation varies by factors such as time, type of SCS device, and patient’s pain condition [64]. For example, Levy et al. reported that tonic SCS demonstrated therapy habituation as early as nine to twelve months in patients with CRPS [63].
In pharmacology, tolerance is defined as a decrease in the drug’s efficacy due to adaptations in the nervous system after prolonged exposure to the drug [65]. Similarly, it is speculated that prolonged exposure of neuronal tissue to stimulation patterns causes a tolerance phenomenon to occur secondary to repetitive driving of electrophysiological and neurochemical mechanisms. If a patient experiences drug tolerance, their physician may increase the dose or recommend a new medication [66]. Therefore, in an attempt to regain pain relief after the habituation of SCS and loss of efficacy, several studies have examined replacing the original stimulation waveform (which has been adapted to) with a new SCS waveform or program.
Interestingly, Rauck et al. reported that 7.6% of a cohort of one thousand two-hundred eighty-nine SCS subjects using custom and variable stim programing required an explant three years post implantation with only 2.5% of these subjects undergoing explanation due to inadequate pain relief [67]. This markedly lower incidence of overall explantation due to habituation compared to other studies could be partially explained by induction of different cellular mechanisms of analgesia controlled by variable stim programming [67]. Further, several studies have demonstrated that patients who had not maintained pain relief with conventional SCS therapy achieved pain improvement when their traditional SCS was replaced with HF-SCS [68,69,70]. Kapural et al. reported that 81% of patients who were switched to HF-SCS due to cSCS habituation received greater than 50% pain relief with 10 kHZ stimulation [68]. Similarly, Cordero Tous et al. demonstrated improvement in analgesia after transitioning from conventional to HF stimulation without replacing existing spinal electrodes. This decreased complications associated with a second procedure [71]. Provenzano et al. studied thirty-one patients on high frequency stimulation with varying duty cycles ranging from 3%, 14%, 50% and 100%. Findings showed that some patients achieved equivalent pain relief with lower duty cycles which reduced device charging time by approximately two-thirds [78]. Improved pain relief has also been reported in patients who were previously implanted with cSCS and then received burst stimulation. Courtney et al. reported that 76% of patients that had been using tonic stimulation for at least 90 days had a reduction in overall daily pain intensity after using burst stimulation for two weeks [72].
Another rescue strategy that has proven to be effective is incorporating a “stimulation holiday” during which SCS therapy is discontinued for a period of time prior to restarting [61]. D’Souza et al. reported that 57.5% of patients that underwent a stimulation holiday (17.3±20.6 days) after experiencing a loss of efficacy with HF-SCS had ≥ 50% relief in pain intensity with maintenance of pain relief for 6 months [61]. Akin to receptor degradation with overexposure of inhibiting medications in pharmacology, allowing for a stim holiday allows the intrinsic responsivity and receptor mediated pathways to reset thus re-establishing sensitivity [73,74,75].
4. Conclusions and Future Directions
Chronic pain affects millions of adults in The United States and disrupts nearly all aspects of an individuals’ life. The field of SCS has evolved tremendously since its first use in 1967, particularly with the addition of several different stimulation waveforms. Given the novelty of the therapy, long-term data on these various SCS waveforms is sparse. Several studies have reported a high incidence of SCS explant, with loss of efficacy being one of the primary reasons for removal. Although several strategies, such as stimulation holidays [61], alternating waveforms [68,71], or SCS microdosing [44], have been proposed to regain pain relief, there has yet to be an established methodology to abate habituation and significant loss of efficacy. In 2023, Mirzakhalili et al. published “An optimization framework for targeted spinal cord stimulation.” They developed computer modeling which allowed for customization of stimulation configurations for targeted SCS. Furthermore, the computational model can be integrated to individual patient variables and allow for more efficient and personalized therapy [76].
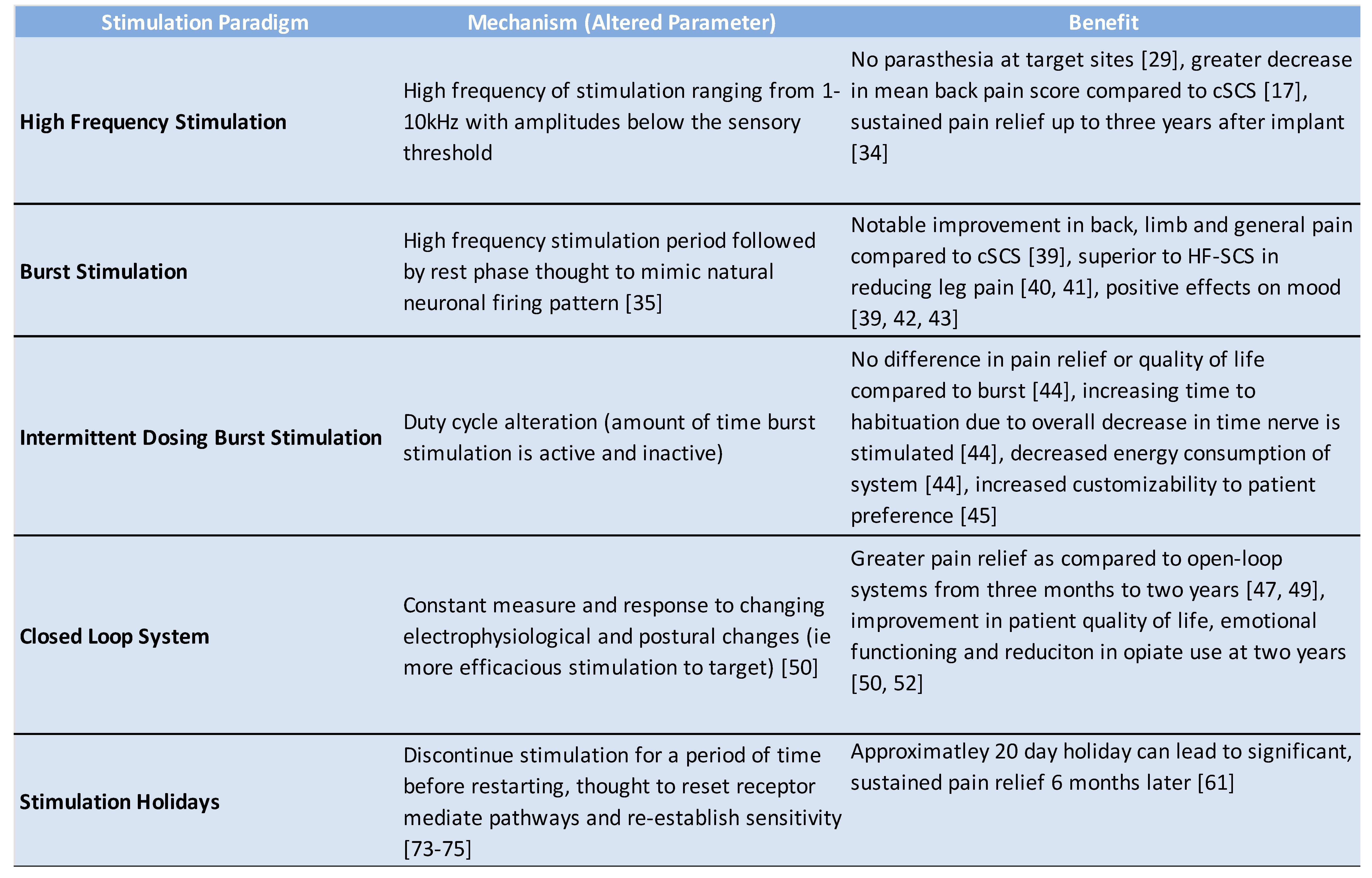
The MULTIWAVE study, a prospective, randomized, controlled, crossover, double-blind trial showed that allowing switching or waveforms and/or combining waveforms increased the rate of SCS responders by 25%. The study also found waveform versatility had a positive and sustained response in patients who had been salvaged from cSCS loss of efficacy [77]. Given the current evidence implicating the individual effectiveness of SCS microdosing [44], turning stimulation off for a designated period [61], pulse dosing, and cycling between different stimulation waveforms [44,45] we hypothesize that implementing all three strategies immediately after SCS implantation will prolong device efficacy and pain relief. A summary of these technologies and their benefits can be appreciated in Table 1. These stimulations strategies can be viewed as steps of habituation mitigation which work in tandem to ultimately extend significant pain relief duration post SCS implantation.
In Figure 1 we propose a graded approach to limiting habituation. Changes in stimulation programming are compared to equivalent approaches in opioid therapy as we suspect electrostimulation habituation mirrors the habituation phenomenon appreciated in pharmacology. Specifically, more exploration is needed in deployment timeline of each paradigm and its utility on responder longevity or use as salvage therapy. Therefore, we encourage providers to investigate further strategies of incorporating diverse stimulation paradigms to abate stimulation habituation.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Nahin RL, Feinberg T, Kapos FP, Terman GW. (2023) Estimated Rates of Incident and Persistent Chronic Pain Among US Adults, 2019-2020. JAMA Network Open.6(5):e2313563-e.
- Yong RJ, Mullins PM, Bhattacharyya N. (2022) Prevalence of chronic pain among adults in the United States. Pain.163(2):e328-e32. [PubMed]
- Gaskin DJ, Richard P. (2012) The economic costs of pain in the United States. The journal of pain.13(8):715-24.
- Gatchel RJ, McGeary DD, McGeary CA, Lippe B. (2014) Interdisciplinary chronic pain management: past, present, and future. Am Psychol.69(2):119-30. [PubMed]
- Dale R, Stacey B. (2016) Multimodal treatment of chronic pain. Medical Clinics.100(1):55-64.
- Vakkala M, Järvimäki V, Kautiainen H, Haanpää M, Alahuhta S. (2017) Incidence and predictive factors of spinal cord stimulation treatment after lumbar spine surgery. J Pain Res.10:2405-11. PMCID: PMC5634380. [PubMed]
- Shealy CN, Mortimer JT, Reswick JB. (1967) Electrical inhibition of pain by stimulation of the dorsal columns: preliminary clinical report. Anesth Analg.46(4):489-91. [PubMed]
- Knotkova H, Hamani C, Sivanesan E, Le Beuffe MFE, Moon JY, Cohen SP, Huntoon MA. (2021) Neuromodulation for chronic pain. The Lancet.397(10289):2111-24.
- Duarte RV, Nevitt S, Maden M, Meier K, Taylor RS, Eldabe S, de Vos CC. (2021) Spinal cord stimulation for the management of painful diabetic neuropathy: a systematic review and meta-analysis of individual patient and aggregate data. Pain.162(11):2635-43.
- Al-Kaisy A, Van Buyten J, Kapural L, Amirdelfan K, Gliner B, Caraway D, Subbaroyan J, Edgar D, Rotte A. (2020) 10 kHz spinal cord stimulation for the treatment of non-surgical refractory back pain: subanalysis of pooled data from two prospective studies. Anaesthesia.75(6):775-84.
- Eckermann JM, Pilitsis JG, Vannaboutathong C, Wagner BJ, Province-Azalde R, Bendel MA. (2022) Systematic literature review of spinal cord stimulation in patients with chronic back pain without prior spine surgery. Neuromodulation: Technology at the Neural Interface.25(5):648-56.
- Vannemreddy P, Slavin KV. (2011) Spinal cord stimulation: Current applications for treatment of chronic pain. Anesth Essays Res.5(1):20-7. PMCID: PMC4173369. [PubMed]
- Lam CM, Latif U, Sack A, Govindan S, Sanderson M, Vu DT, Smith G, Sayed D, Khan T. (2023) Advances in Spinal Cord Stimulation. Bioengineering (Basel).10(2). PMCID: PMC9951889. [PubMed]
- Miller JP, Eldabe S, Buchser E, Johanek LM, Guan Y, Linderoth B. (2016) Parameters of spinal cord stimulation and their role in electrical charge delivery: a review. Neuromodulation: Technology at the Neural Interface.19(4):373-84.
- Brill S, Defrin R, Aryeh IG, Zusman AM, Benyamini Y. (2022) Short-and long-term effects of conventional spinal cord stimulation on chronic pain and health perceptions: A longitudinal controlled trial. European Journal of Pain.26(9):1849-62.
- Hayek SM, Veizi E, Hanes M. (2015) Treatment-Limiting Complications of Percutaneous Spinal Cord Stimulator Implants: A Review of Eight Years of Experience From an Academic Center Database. Neuromodulation.18(7):603-8; discussion 8-9. [PubMed]
- Kapural L, Yu C, Doust MW, Gliner BE, Vallejo R, Sitzman BT, Amirdelfan K, Morgan DM, Brown LL, Yearwood TL. (2015) Novel 10-kHz high-frequency therapy (HF10 therapy) is superior to traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: the SENZA-RCT randomized controlled trial. Anesthesiology.123(4):851-60.
- Reddy RD, Moheimani R, Yu GG, Chakravarthy KV. (2020) A Review of Clinical Data on Salvage Therapy in Spinal Cord Stimulation. Neuromodulation.23(5):562-71. PMCID: PMC7202967. [PubMed]
- Melzack R, Wall PD. (1965) Pain mechanisms: a new theory. Science.150(3699):971-9. [PubMed]
- Linderoth B, Meyerson BA. (2010) Spinal cord stimulation: exploration of the physiological basis of a widely used therapy. The Journal of the American Society of Anesthesiologists.113(6):1265-7.
- Jeon, YH. (2012) Spinal cord stimulation in pain management: a review. Korean J Pain.25(3):143-50. PMCID: PMC3389317. [PubMed]
- Barolat G, Massaro F, He J, Zeme S, Ketcik B. (1993) Mapping of sensory responses to epidural stimulation of the intraspinal neural structures in man. J Neurosurg.78(2):233-9. [PubMed]
- Kumar K, North R, Taylor R, Sculpher M, Van den Abeele C, Gehring M, Jacques L, Eldabe S, Meglio M, Molet J. (2005) Spinal cord stimulation vs. conventional medical management: a prospective, randomized, controlled, multicenter study of patients with failed back surgery syndrome (PROCESS study). Neuromodulation: Technology at the Neural Interface.8(4):213-8.
- Levy RM. (2014) Anatomic considerations for spinal cord stimulation. Neuromodulation: Technology at the Neural Interface.17:2-11.
- Schultz DM, Webster LR, Kosek P, Dar U, Tan Y, Sun M. (2012) Sensor-driven position-adaptive spinal cord stimulation for chronic pain. Pain physician.15(1):1.
- Barolat G, Oakley JC, Law JD, North RB, Ketcik B, Sharan A. (2001) Epidural spinal cord stimulation with a multiple electrode paddle lead is effective in treating intractable low back pain. Neuromodulation: Technology at the Neural Interface.4(2):59-66.
- Turner JA, Loeser JD, Bell KG. (1995) Spinal cord stimulation for chronic low back pain: a systematic literature synthesis. Neurosurgery.37(6):1088-95; discussion 95-6. [PubMed]
- Aló KM, Redko V, Charnov J. (2002) Four Year Follow-up of Dual Electrode Spinal Cord Stimulation for Chronic Pain. Neuromodulation.5(2):79-88. [PubMed]
- Caylor J, Reddy R, Yin S, Cui C, Huang M, Huang C, Rao R, Baker DG, Simmons A, Souza D. (2019) Spinal cord stimulation in chronic pain: evidence and theory for mechanisms of action. Bioelectronic medicine.5:1-41.
- Kumar K, Taylor RS, Jacques L, Eldabe S, Meglio M, Molet J, Thomson S, O'Callaghan J, Eisenberg E, Milbouw G. (2008) The effects of spinal cord stimulation in neuropathic pain are sustained: a 24-month follow-up of the prospective randomized controlled multicenter trial of the effectiveness of spinal cord stimulation. Neurosurgery.63(4):762-70.
- Kapural L, Yu C, Doust MW, Gliner BE, Vallejo R, Sitzman BT, Amirdelfan K, Morgan DM, Yearwood TL, Bundschu R, Yang T, Benyamin R, Burgher AH. (2016) Comparison of 10-kHz High-Frequency and Traditional Low-Frequency Spinal Cord Stimulation for the Treatment of Chronic Back and Leg Pain: 24-Month Results From a Multicenter, Randomized, Controlled Pivotal Trial. Neurosurgery.79(5):667-77. PMCID: PMC5058646. [PubMed]
- Al-Kaisy A, Palmisani S, Smith TE, Pang D, Lam K, Burgoyne W, Houghton R, Hudson E, Lucas J. (2017) 10 kHz High-Frequency Spinal Cord Stimulation for Chronic Axial Low Back Pain in Patients With No History of Spinal Surgery: A Preliminary, Prospective, Open Label and Proof-of-Concept Study. Neuromodulation.20(1):63-70. [PubMed]
- Al-Kaisy A, Van Buyten JP, Smet I, Palmisani S, Pang D, Smith T. (2014) Sustained effectiveness of 10 kHz high-frequency spinal cord stimulation for patients with chronic, low back pain: 24-month results of a prospective multicenter study. Pain Med.15(3):347-54. PMCID: PMC4282782. [PubMed]
- Al-Kaisy A, Palmisani S, Smith TE, Carganillo R, Houghton R, Pang D, Burgoyne W, Lam K, Lucas J. (2018) Long-Term Improvements in Chronic Axial Low Back Pain Patients Without Previous Spinal Surgery: A Cohort Analysis of 10-kHz High-Frequency Spinal Cord Stimulation over 36 Months. Pain Med.19(6):1219-26. [PubMed]
- De Ridder D, Vanneste S, Plazier M, van der Loo E, Menovsky T. (2010) Burst spinal cord stimulation: toward paresthesia-free pain suppression. Neurosurgery.66(5):986-90.
- Kirketeig T, Schultheis C, Zuidema X, Hunter CW, Deer T. (2019) Burst Spinal Cord Stimulation: A Clinical Review. Pain Med.20(Suppl 1):S31-s40. PMCID: PMC6544556. [PubMed]
- de Vos CC, Bom MJ, Vanneste S, Lenders MW, De Ridder D. (2014) Burst spinal cord stimulation evaluated in patients with failed back surgery syndrome and painful diabetic neuropathy. Neuromodulation: Technology at the Neural Interface.17(2):152-9.
- Schu S, Slotty PJ, Bara G, von Knop M, Edgar D, Vesper J. (2014) A prospective, randomised, double-blind, placebo-controlled study to examine the effectiveness of burst spinal cord stimulation patterns for the treatment of failed back surgery syndrome. Neuromodulation: Technology at the Neural Interface.17(5):443-50.
- De Ridder D, Vanneste S. (2016) Burst and Tonic Spinal Cord Stimulation: Different and Common Brain Mechanisms. Neuromodulation.19(1):47-59. [PubMed]
- Kinfe TM, Pintea B, Link C, Roeske S, Güresir E, Güresir Á, Vatter H. (2016) High frequency (10 kHz) or burst spinal cord stimulation in failed back surgery syndrome patients with predominant back pain: preliminary data from a prospective observational study. Neuromodulation: Technology at the Neural Interface.19(3):268-75.
- Muhammad S, Roeske S, Chaudhry SR, Kinfe TM. (2017) Burst or high-frequency (10 kHz) spinal cord stimulation in failed back surgery syndrome patients with predominant back pain: one year comparative data. Neuromodulation: Technology at the Neural Interface.20(7):661-7.
- De Ridder D, Plazier M, Kamerling N, Menovsky T, Vanneste S. (2013) Burst spinal cord stimulation for limb and back pain. World neurosurgery.80(5):642-9. e1.
- Yearwood T, De Ridder D, Yoo HB, Falowski S, Venkatesan L, Ting To W, Vanneste S. (2020) Comparison of Neural Activity in Chronic Pain Patients During Tonic and Burst Spinal Cord Stimulation Using Fluorodeoxyglucose Positron Emission Tomography. Neuromodulation.23(1):56-63. [PubMed]
- Vesper J, Slotty P, Schu S, Poeggel-Kraemer K, Littges H, Van Looy P, Agnesi F, Venkatesan L, Van Havenbergh T. (2019) Burst SCS microdosing is as efficacious as standard burst SCS in treating chronic back and leg pain: results from a randomized controlled trial. Neuromodulation: Technology at the Neural Interface.22(2):190-3.
- Deer TR, Patterson DG, Baksh J, Pope JE, Mehta P, Raza A, Agnesi F, Chakravarthy KV. (2021) Novel intermittent dosing burst paradigm in spinal cord stimulation. Neuromodulation: Technology at the Neural Interface.24(3):566-73.
- Ranger M, Irwin G, Bunbury K, Peutrell J. (2008) Changing body position alters the location of the spinal cord within the vertebral canal: a magnetic resonance imaging study. British journal of anaesthesia.101(6):804-9.
- Parker JL, Karantonis DM, Single PS, Obradovic M, Cousins MJ. (2012) Compound action potentials recorded in the human spinal cord during neurostimulation for pain relief. Pain.153(3):593-601.
- Russo M, Brooker C, Cousins MJ, Taylor N, Boesel T, Sullivan R, Holford L, Hanson E, Gmel GE, Shariati NH, Poree L, Parker J. (2020) Sustained Long-Term Outcomes With Closed-Loop Spinal Cord Stimulation: 12-Month Results of the Prospective, Multicenter, Open-Label Avalon Study. Neurosurgery.87(4):E485-e95. PMCID: PMC8184296. [PubMed]
- Deer TR, Jain S, Hunter C, Chakravarthy K. (2019) Neurostimulation for Intractable Chronic Pain. Brain Sci.9(2). PMCID: PMC6406470. [PubMed]
- Mekhail N, Levy RM, Deer TR, Kapural L, Li S, Amirdelfan K, Hunter CW, Rosen SM, Costandi SJ, Falowski SM. (2020) Long-term safety and efficacy of closed-loop spinal cord stimulation to treat chronic back and leg pain (Evoke): a double-blind, randomised, controlled trial. The Lancet Neurology.19(2):123-34.
- Russo M, Cousins MJ, Brooker C, Taylor N, Boesel T, Sullivan R, Poree L, Shariati NH, Hanson E, Parker J. (2018) Effective Relief of Pain and Associated Symptoms With Closed-Loop Spinal Cord Stimulation System: Preliminary Results of the Avalon Study. Neuromodulation.21(1):38-47. [PubMed]
- Mekhail N, Levy RM, Deer TR, Kapural L, Li S, Amirdelfan K, Hunter CW, Rosen SM, Costandi SJ, Falowski SM. (2022) Durability of clinical and quality-of-life outcomes of closed-loop spinal cord stimulation for chronic back and leg pain: a secondary analysis of the evoke randomized clinical trial. JAMA neurology.79(3):251-60.
- Dupré DA, Tomycz N, Whiting D, Oh M. (2018) Spinal Cord Stimulator Explantation: Motives for Removal of Surgically Placed Paddle Systems. Pain Pract.18(4):500-4. [PubMed]
- Deer TR, Pope JE, Falowski SM, Pilitsis JG, Hunter CW, Burton AW, Connolly AT, Verrills P. (2023) Clinical Longevity of 106,462 Rechargeable and Primary Cell Spinal Cord Stimulators: Real World Study in the Medicare Population. Neuromodulation.26(1):131-8. [PubMed]
- Simopoulos T, Aner M, Sharma S, Ghosh P, Gill JS. (2019) Explantation of Percutaneous Spinal Cord Stimulator Devices: A Retrospective Descriptive Analysis of a Single-Center 15-Year Experience. Pain Med.20(7):1355-61. [PubMed]
- Van Buyten JP, Wille F, Smet I, Wensing C, Breel J, Karst E, Devos M, Pöggel-Krämer K, Vesper J. (2017) Therapy-Related Explants After Spinal Cord Stimulation: Results of an International Retrospective Chart Review Study. Neuromodulation.20(7):642-9. PMCID: PMC5656934. [PubMed]
- Al-Kaisy A, Royds J, Al-Kaisy O, Palmisani S, Pang D, Smith T, Padfield N, Harris S, Wesley S, Yearwood TL, Ward S. (2020) Explant rates of electrical neuromodulation devices in 1177 patients in a single center over an 11-year period. Reg Anesth Pain Med.45(11):883-90. [PubMed]
- Kumar K, Hunter G, Demeria D. (2006) Spinal cord stimulation in treatment of chronic benign pain: challenges in treatment planning and present status, a 22-year experience. Neurosurgery.58(3):481-96.
- Hayek SM, Veizi E, Hanes M. (2015) Treatment-limiting complications of percutaneous spinal cord stimulator implants: a review of eight years of experience from an academic center database. Neuromodulation: Technology at the Neural Interface.18(7):603-9.
- Hagedorn JM, Layno-Moses A, Sanders DT, Pak DJ, Bailey-Classen A, Sowder T. (2020) Overview of HF10 spinal cord stimulation for the treatment of chronic pain and an introduction to the Senza Omnia™ system. Pain management.10(6):367-76.
- D'Souza RS, Her YF. (2022) Stimulation holiday rescues analgesia after habituation and loss of efficacy from 10-kilohertz dorsal column spinal cord stimulation. Regional Anesthesia & Pain Medicine.47(12):722-7.
- Reddy RD, Moheimani R, Gregory GY, Chakravarthy KV. (2020) A review of clinical data on salvage therapy in spinal cord stimulation. Neuromodulation: Technology at the Neural Interface.23(5):562-71.
- Levy RM, Mekhail N, Kramer J, Poree L, Amirdelfan K, Grigsby E, Staats P, Burton AW, Burgher AH, Scowcroft J, Golovac S, Kapural L, Paicius R, Pope J, Samuel S, McRoberts WP, Schaufele M, Kent AR, Raza A, Deer TR. (2020) Therapy Habituation at 12 Months: Spinal Cord Stimulation Versus Dorsal Root Ganglion Stimulation for Complex Regional Pain Syndrome Type I and II. J Pain.21(3-4):399-408. [PubMed]
- Chapman KB, Spiegel MA, van Helmond N, Patel KV, Yang A, Yousef TA, Mandelberg N, Deer T, Mogilner AY. (2022) Dorsal Root Ganglion Stimulation as a Salvage Therapy Following Failed Spinal Cord Stimulation. Neuromodulation: Technology at the Neural Interface.25(7):1024-32.
- Bateson, A. (2002) Basic pharmacologic mechanisms involved in benzodiazepine tolerance and withdrawal. Current pharmaceutical design.8(1):5-21.
- Glajchen, M. (2001) Chronic pain: treatment barriers and strategies for clinical practice. The Journal of the American Board of Family Practice.14(3):211-8.
- Rauck RL, Loudermilk E, Thomson SJ, Paz-Solis JF, Bojrab L, Noles J, Vesper J, Atallah J, Roth D, Hegarty J. (2023) Long-term safety of spinal cord stimulation systems in a prospective, global registry of patients with chronic pain. Pain management.13(2):115-27.
- Kapural L, Sayed D, Kim B, Harstroem C, Deering J. (2020) Retrospective assessment of salvage to 10 kHz spinal cord stimulation (SCS) in patients who failed traditional SCS therapy: RESCUE study. Journal of Pain Research.2861-7.
- Andrade P, Heiden P, Visser-Vandewalle V, Matis G. (2021) 1.2 kHz high-frequency stimulation as a rescue therapy in patients with chronic pain refractory to conventional spinal cord stimulation. Neuromodulation: Technology at the Neural Interface.24(3):540-5.
- Kumar V, Prusik J, Lin Y, Hwang R, Feustel P, Pilitsis JG. (2018) Efficacy of alternating conventional stimulation and high frequency stimulation in improving spinal cord stimulation outcomes: a pilot study. Neuromodulation: Technology at the Neural Interface.21(5):466-71.
- Cordero Tous N, Sanchez Corral C, Ortiz Garcia IM, Jover Vidal A, Galvez Mateos R, Olivares Granados G. (2021) High-frequency spinal cord stimulation as rescue therapy for chronic pain patients with failure of conventional spinal cord stimulation. European Journal of Pain.25(7):1603-11.
- Courtney P, Espinet A, Mitchell B, Russo M, Muir A, Verrills P, Davis K. (2015) Improved pain relief with burst spinal cord stimulation for two weeks in patients using tonic stimulation: results from a small clinical study. Neuromodulation: Technology at the Neural Interface.18(5):361-6.
- Breitfeld C, Eikermann M, Kienbaum P, Peters J. (2003) Opioid “holiday” following antagonist supported detoxification during general anesthesia improves opioid agonist response in a cancer patient with opioid addiction. The Journal of the American Society of Anesthesiologists.98(2):571-3.
- Howland, RH. (2009) Medication holidays. Journal of psychosocial nursing and mental health services.47(9):15-8.
- Corona T, Rivera C, Otero E, Stopp L. (1995) A longitudinal study of the effects of an L-dopa drug holiday on the course of Parkinson's disease. Clinical neuropharmacology.18(4):325-32.
- Mirzakhalili E, Rogers ER, Lempka SF. An optimization framework for targeted spinal cord stimulation. J Neural Eng. 2023;20(5):056026. Published 2023 Sep 28. [CrossRef]
- Rigoard P, Ounajim A, Moens M, et al. Should we Oppose or Combine Waveforms for Spinal Cord Stimulation in PSPS-T2 Patients? A Prospective Randomized Crossover Trial (MULTIWAVE Study). J Pain. 2023;24(12):2319-2339. [CrossRef]
- Provenzano D, Tate J, Gupta M, et al. Pulse Dosing of 10-kHz Paresthesia-Independent Spinal Cord Stimulation Provides the Same Efficacy with Substantial Reduction of Device Recharge Time. Pain Med. 2022;23(1):152-163. [CrossRef]
Figure 1.
Graded approach to pharmacological and stimulation habituation mitigation.
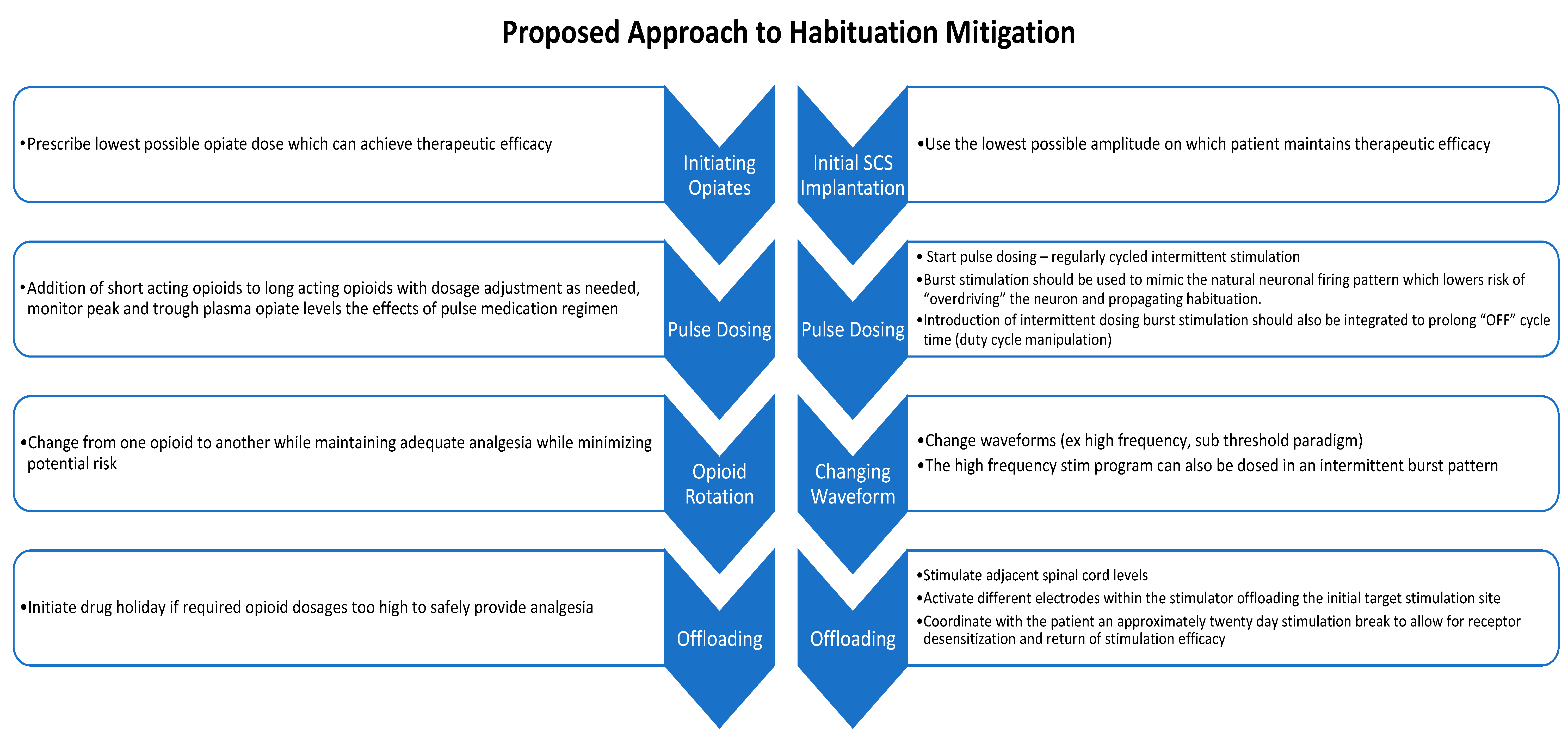

Table 1.
Stimulation paradigms summarized.
 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



