
Submitted:
05 April 2024
Posted:
08 April 2024
You are already at the latest version
Abstract
Sarcopenia is associated with clinical complications, which increase mortality. Effective sarcopenia risk screening in the elderly should be grounded in a comprehensive assessment, encompassing both nutritional status and medication use. Current screening tools, while emphasizing muscular per-formance, exhibit limited sensitivity in identifying elderly individuals at risk of sarcopenia. This cross-sectional study aimed to develop a sarcopenia risk screening tool, named Sarc-Global, with enhanced sensitivity, incorporating factors pertinent to the overall health of the elderly. Utilizing the criteria established by EWGSOP2 for diagnosing sarcopenia, we evaluated 395 communi-ty-dwelling elderly individuals. This evaluation served as a reference for assessing the efficacy of two validated questionnaires, Sarc-F and Sarc-CalF, and our newly developed Sarc-Global. Con-structed through multiple logistic regression, Sarc-Global integrates variables such as sex, age, medication use, body mass index, arm circumference, and handgrip strength – all significantly associated with sarcopenia (p
Keywords:
sarcopenia
; older adults
; sarcopenia screening
; Sarc-F
; Sarc-CalF
; Sarc-Global
1. Introduction
Sarcopenia, a geriatric syndrome characterized by the progressive and generalized loss of skeletal muscle, has a reported prevalence of 11.5% to 22.6% [1,2,3,4,5,6,7,8,9,10]. Timely diagnosis is imperative as it aids in identifying risks tied to clinical complications such as prolonged hospitalization, extended bedrest, increased incidents of falls and fractures, physical disability, functional deterioration, diminished quality of life, and heightened mortality risk [6,11,12,13,14,15,16,17].
The European Working Group on Sarcopenia in Older People (EWGSOP2) advocates for the routine screening of older individuals for risk of sarcopenia, recommending tools like Sarc-F or Sarc-CalF [1]. Following screening, confirming a sarcopenia diagnosis requires identifying reduced muscle strength and muscle mass. Muscle mass evaluation is often done by calculating the Appendicular Skeletal Mass Index (ASMI) using diagnostic tools like dual-energy x-ray absorptiometry (DXA) or bioelectrical impedance (BIA). However, these tools are not always accessible due to their high costs and limited availability in healthcare facilities [18].
Sarc-F, a validated screening tool, has been used to detect sarcopenia across various populations [19,20,21,22,23,24]. Positive Sarc-F results correlate with adverse health outcomes [22,25]. However, Sarc-F doesn't evaluate muscle mass, a key sarcopenia indicator, limiting its diagnostic scope. Its sensitivity is also relatively low, making it more effective for ruling out sarcopenia than confirming it [26]. To address these issues, Sarc-CalF was introduced as a Brazilian adaptation of Sarc-F, incorporating calf measurement as a significant muscle mass measure [27]. Yet, Sarc-CalF's sensitivity in identifying at-risk older adults remains limited [25,27].
Voelker et al. [28] argue that neither Sarc-F nor Sarc-CalF effectively screen for risk of sarcopenia and don't fully align with EWGSOP2 recommendations. This discrepancy underscores concerns about their suitability as standalone sarcopenia screening tools, especially given their known limitations. Hence, there's a pressing need for more sensitive and accurate screening tools for this prevalent geriatric condition.
The World Health Organization (WHO) emphasizes comprehensive assessments for older individuals [29], indicating that muscle mass loss isn't the only health risk. For instance, polypharmacy, defined by the regular use of five or more medications, is a notable risk factor for adverse outcomes in the elderly, including sarcopenia and increased fall likelihood [30,31,32,33,34]. This highlights the importance of a holistic approach in evaluating the health of older adults.
Understanding the critical need for precise diagnosis of sarcopenia in older populations, our study is designed to tackle the shortcomings in the sensitivity of existing screening tools and to delve into the broader impact of various factors contributing to muscle degeneration. Our objective is to forge a more nuanced and sensitive sarcopenia risk assessment tool that considers a broader spectrum of factors influencing muscle wasting in the elderly. This endeavor aims to provide a more comprehensive and effective alternative to the current screening methodologies, potentially enhancing the accuracy and efficacy of sarcopenia diagnosis in geriatric care.
2. Materials and Methods
2.1. Study Design, Participants and Ethical Issues
This is a cross-sectional study aimed at developing and validating a novel screening risk tool for sarcopenia in older adults. The study participants were selected from both the community and the geriatric outpatient clinic of the Hospital das Clinicas at the University of São Paulo, Brazil. A total of 395 volunteers were recruited between February 2016 and December 2019. The inclusion criteria for the study were as follows: age ≥ 60 years, living independently, and capable of providing conscious responses to the questions asked during the anamnesis, cognitive questionnaire, and sarcopenia screening questionnaires. The study also had specific exclusion criteria, including being less than 60 years old, having a physical disability, or having dementia. All study assessments were conducted by a single trained technician, following the ethical standards outlined in the Declaration of Helsinki by the World Medical Association. Prior to the protocol beginning, each participant provided informed consent by signing a consent form. The study protocol received approval from the Institutional Ethics Review Board (1.905.072) and was registered at www.clinicalTrials.gov (NCT04451005).
2.2. Data Collection
Demographic information, lifestyle variables, and personal disease history of the participants were recorded. The collected variables encompassed age, gender, and any history of prior illnesses. Participants were also instructed to bring their medical prescriptions or a list of medications they were currently taking to facilitate the assessment of polypharmacy.
2.3. Anthropometric Measurements
The anthropometric parameters assessed in this study were height, weight, calf circumference (CC), arm circumference (AC) and skinfold thickness. Height and weight were measured while the participants were barefoot and wearing light clothing. A height and weight measuring scale was used, providing measurements to the nearest 0.1 cm and 0.1 kg, respectively. Body mass index (BMI) was then calculated by dividing the weight in kilograms by the square of the height in meters. CC was measured at the greatest circumference of the lower right leg while the participants were in a standing position, and the calf perpendicular to the thigh. The measurements were recorded in centimeters (cm) and accurate to one decimal place. To ensure accuracy, all measurements were performed twice, and the means of the duplicate measurements were calculated for subsequent analysis. The AC was measured with the right arm extended along the body and the palm of the hand towards the thigh, placing the tape at a reference point previously marked from the midpoint between the acromion and the olecranon, coming from the arm flexed at a 90º angle. Biceps (BSFT), triceps (TSFT), subscapularis (SSFT) and suprailiac (SISFT) skinfold thickness were measured using an adipometer (Lange®, Beta Technology Incorporated, Cambridge, USA). The average value of 3 measurements was recorded. Handgrip strength (HGS) was also assessed by using an analog dynamometer (JAMAR®). During the analysis, participants remained seated on a height-adjustable chair with their legs upright and feet flat on the floor, ensuring a right angle in the hip, knee, and ankle joints. The test arm was kept close to the body, with the elbow flexed at a 90º angle, the palm facing inward, and the thumb pointing upward. The non-evaluated arm was supported and relaxed on the participant's thigh [34,35].
2.4. Sarcopenia Screening
Sarcopenia screening was conducted using the Sarc-F and Sarc-CalF tools. These two questionnaires were administered by a single trained evaluator through face-to-face interviews. The Sarc-F questionnaire consists of five items: strength, assistance in walking, getting up from a chair, climbing stairs, and falls. In addition to these items, the Sarc-CalF questionnaire includes the CC measurement using a millimeter tape. A total Sarc-F score of 4 or higher, as well as a total Sarc-CalF score of 11 or higher, indicate the possibility of sarcopenia [20,27].
2.5. Sarcopenia Diagnosis
For reference, the diagnosis of sarcopenia was established according to the criteria of the EWGSOP, which defines sarcopenia as the combination of loss of lean mass, strength, and performance [1]. Lean mass and strength are applied to diagnose sarcopenia, while the performance is applied to determine the grade of this condition. To diagnose sarcopenia, we calculated the ASMI as a marker of skeletal muscle mass, following the method described elsewhere [36]. Briefly, we first determined the lean mass of the four limbs using a DXA device (Lunar iDXA GE Medical Systems Lunar, Maidson, USA) and then applied the following equation to obtain the ASMI: ASMI = appendicular skeletal mass / height² (kg/m²) [36]. The HGS measure served as an indicator of skeletal muscle strength. To ensure accurate assessments, participants were instructed to fast for 4 hours and refrain from engaging in physical activity (except light walking), using diuretics, and consuming alcohol for 24 hours prior to these evaluations.
2.6. Creation of the New Sarcopenia Risk Screening Tool
We first assessed the performance of Sarc-F and Sarc-CalF in screening risk of sarcopenia. Subsequently, the new toll was designed from the most effective questionnaire by incorporating additional variables that have the potential to enhance its sensitivity in detecting the risk of sarcopenia. To accomplish this objective, we utilized the R version 4.0.2 software program to conduct statistical analyses and develop a novel screening tool for risk of sarcopenia in older adults. The significance level chosen for the tests was 0.05, and we constructed 95% confidence intervals. Initially, we performed univariate logistic regression analysis on the relevant data, including clinical information, anthropometric measurements, and sarcopenia screening questionnaires, in order to generate inputs for the new tool. Categorical variables were analyzed using Fisher's exact test, while continuous variables were analyzed using Student's t-test, Mann-Whitney test, or Brunner-Munzel test. Continuous variables were presented as summary measures, including mean, median, standard deviation, and quartiles. Categorical variables were presented as frequencies and percentages. The new tool was developed using a multiple logistic regression model. A random sample comprising 70% (n=277) of the participants was selected as the creation group (CG). The aim was to identify sarcopenia risk according to the EWGSOP2 criteria. The odds ratio (OR) of each variable was used to determine the weights assigned to the items in the questionnaire. The original weights for the Sarc-F items were retained. As no established national cut-off point existed, the median value of the arm circumference (AC) variable was chosen as the cut-off point. To identify the appropriate cut-off point for the new tool, an ROC curve analysis was performed. This new sarcopenia risk screening tool was named Sarc-Global.
2.7. Validation of the New Sarcopenia Screening Tool
The accuracy of the new screening tool for risk of sarcopenia in older adults was evaluated by comparing it to the diagnosis of sarcopenia using the reference method (EWGSOP2). This analysis involved assessing the accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of the new tool in relation to the established gold standard. The validation stage of the tool involved utilizing 30% of the sample (n=118), which was designated as the validation group (VG).
3. Results
3.1. Descriptive Data
Table 1 presents the demographic and anthropometric characteristics of the patients enrolled in the study, categorized into SARC-global creation (SGC) (n=277), SARC-global validation (SGV) (n=118), and the total sample (n=395). The majority of participants in the sample were female (81%), ranging in age from 60 to 93 years. Additionally, 48.6% of the patients had a BMI greater than 27 kg/m², indicating that they were overweight.
According to the diagnosis proposed by the EWGSOP2, the prevalence of sarcopenia in the total population was 21.5% (n=85). Specifically, sarcopenia affected 20.9% (n=58) of the SGC group and 22.9% (n=27) of the SGV group. Assessments conducted using the Sarc-F and Sarc-CalF questionnaires revealed that 18% (n=71) and 13.4% (n=53) of older adults in the overall population were found to be at risk of sarcopenia, respectively. Moreover, within our sample, 53.92% displayed low muscle strength, while low muscle mass, as determined by the IMMA, was observed in only 24.55% of the older adults. Notably, the use of four or more medications was prominent among the clinical data, with 50.37% of older adults taking four or more medications daily.
3.2. Creation of the New Sarcopenia Risk Screening Tool—Sarc-Global
Sarc-CalF (p < 0.001), but not Sarc-F (p = 0.425), demonstrated a significant performance in identify risk of sarcopenia using the EWGSOP criteria as the reference. As a result, Sarc-CalF was selected for the development of the new tool, with the incorporation of additional variables aimed at enhancing its sensitivity in identifying the risk of sarcopenia. Among the variables tested, univariate logistic regression analysis revealed a significant association between sarcopenia diagnosis and gender (p < 0.001), age (p < 0.001), number of medications in use (p < 0.001), HGS (p < 0.001), BMI (p < 0.001), CC (p < 0.001), AC (p < 0.001), TSFT (p < 0.001), BSFT (p < 0.001), SSFT (p < 0.001), and SISFT (p < 0.001). Based on this analysis, gender, age, number of medications, HGS, BMI, CC, and AC were selected as variables for the multiple logistic regression analysis, forming the foundation of the new tool. The weights assigned to each variable was determined by the odds ratio (OR), with rounded values being used to facilitate the final calculation (Table 2).
The conclusive questionnaire, along with the assigned score for each response, is presented in Figure 1. Through an analysis of the receiver operating characteristic (ROC), the optimal threshold for the questionnaire in identifying individuals in risk of sarcopenia was determined. Consequently, a cut-off point of 11, representing the cumulative score of the Sarc-Global questionnaire ≥ 11, was established to indicate a potential diagnosis of sarcopenia. The corresponding area under the curve (AUC) for this particular threshold was found to be 0.8 (0.75-0.85) (Figure 2).
3.3. Validation of the New Sarcopenia Risk Screening Tool—The Sarc-Global
The new sarcopenia risk screening tool, SARC-global, showed an accuracy of 0.74, sensitivity of 0.74, specificity of 0.74, PPV of 0.44 and NPV of 0.91. In contrast, within the same population, the Sarc-F exhibited a sensitivity of 0.21 and a specificity of 0.83, while the Sarc-CalF displayed a sensitivity of 0.34 and a specificity of 0.92, as indicated in Table 3. It was found that out of the 85 older adults diagnosed with sarcopenia based on the EWGSOP2 criteria, 63 individuals were also identified as in risk of sarcopenia when using the Sarc-Global assessment tool. On the other hand, the Sarc-CalF and Sarc-F tools identified only 29 and 18 individuals, respectively, as having risk of sarcopenia. These findings suggest a greater level of agreement between the Sarc-Global tool and the EWGSOP2 criteria.
4. Discussion
Our study sheds light on the advantages of integrating anthropometric and clinical data in a questionnaire for screening risk of sarcopenia in the elderly. By adopting this comprehensive approach, we were able to develop a novel sarcopenia screening tool that exhibits enhanced sensitivity in identifying patients, along with a superior NPV, when compared to the currently available instruments. Moreover, our new tool excels in its practicality, making it suitable for implementation in a diverse range of healthcare services.
Sarcopenia risk screening tools have proven to be highly valuable in clinical practice due to their ease of use in different settings [26,28,37]. Particularly, the Sarc-F is a user-friendly tool that can be effectively employed across diverse populations, consisting of a short scoring questionnaire in which a cumulative score of four or more points indicates a high likelihood of sarcopenia [1,19,38,39,40,41,42,43]. However, the Sarc-F has shown high specificity but low sensitivity in its performance, suggesting it better suited for identifying individuals without risk of sarcopenia rather than its presence [26,44,45]. In our study, the Sarc-F demonstrated a sensitivity of only 21% and a specificity of 82% in diagnosing sarcopenia. These findings are consistent with those reported by Bahat et al. [26], where the Sarc-F exhibited a sensitivity of 25% and a specificity of 81.4% in community-dwelling older adults. These observations further support the notion that the Sarc-F is primarily a screening tool that is more effective at ruling out sarcopenia.
The Sarc-CalF was designed to attend the pressing need for more sensitive sarcopenia risk screening tool. This tool not only encompasses the Sarc-F's questions but also includes Calf Circumference (CC) as an evaluative measure of muscle mass [23]. This modified tool has been tested across various populations and demonstrated a sensitivity of 60.7% in a Chinese cohort study, significantly (p=0.003) higher than that achieved by Sarc-F within this particular community [46,47]. In our study, the Sarc-CalF displayed a higher specificity (92%) and slightly higher sensitivity (34%), when compared to Sarc-F. Accordingly, the Sarc-CalF outperformed the Sarc-F in terms of specificity and diagnostic accuracy when assessed among a Turkish community-dwelling older adult population, but both tools showed an equal sensitivity of 25% [48]. These observations suggest that the sensibility of Sarc-CalF may not improve the screening risk of sarcopenia according to the population analyzed.
Given the criticisms regarding the low sensitivity of both Sarc-F and Sarc-CalF, our study aimed to address the need for a new screening tool that effectively identifies the potential presence of sarcopenia. The newly designed tool, Sarc-Global, demonstrated an accuracy of 74.12%, which was quite comparable to the accuracies of Sarc-F (69.62%) and Sarc-CalF (79.75%). However, Sarc-Global exhibited superior sensitivity (74.12%) compared to Sarc-F (21.18%) and Sarc-CalF (34.12%), indicating its enhanced performance in identifying older adults at risk of sarcopenia [49]. Our findings support the potential to improve the performance of a tool for screening risk of sarcopenia by incorporating variables related to the syndrome. As Sarc-CalF may enhance the sensitivity of Sarc-F by incorporating calf measurements, Sarc-Global appears to further enhance the sensitivity of Sarc-CalF by combining additional sarcopenia-related anthropometric measurements and clinical data.
The new anthropometric data added to Sarc-Global included BMI, CC, and AC, all objective variables that reflect an individual's nutritional status. Indeed, malnutrition and underweight status have been recognized as independent predictors of an elevated risk of sarcopenia [50,51,52,53]. In our sample, a heightened risk for sarcopenia was identified among older adults, particularly those with lower BMI. These findings are consistent with data from other studies conducted with community-dwelling older adults and underscore the importance of age as a clinical variable in sarcopenia, which was also included in the composition of the new tool [52,53].
Sarc-Global also incorporated HGS, which is a convenient anthropometric measure that can be easily conducted in diverse settings. Lower HGS has been linked to adverse health outcomes such as compromised limb function, increased risk of falls and fractures, multimorbidity, diminished quality of life, and increased mortality from various causes [54]. A significant relationship between decreased HGS and elevated mortality rates was observed in a prospective study analyzing 502,293 individuals aged between 40 and 69 years over an average of seven years [55]. Specifically, a reduction of 5kg in HGS was significantly associated with increased mortality from cardiovascular disease, respiratory disease, chronic obstructive pulmonary disease, and all types of cancer. In the hospital setting, low HGS in older adults undergoing surgery for hip fractures was also associated with high mortality [56].
In addition to age, Sarc-Global incorporated gender and polypharmacy as clinical variables. In our study, sarcopenia was found to be more prevalent in men compared to women (26.66% versus 20.31%, respectively). This finding aligns with the research conducted by Zhong et al. [57], who reported sarcopenia prevalence of 26.2% in men and 25.2% in women among a population of 1,040 older adults. Similarly, Chew et al. [58] demonstrated a significantly lower risk of sarcopenia in women than in men in a sample of 811 community-dwelling older adults. These observations may explain why gender had a predictive value within the new sarcopenia screening tool.
In terms of polypharmacy, over half (50.37%) of our study population demonstrated the consumption of four or more medications per day. Furthermore, in our study, the number of medications being taken enhanced the predictive capability of the Sarc-Global tool when used in combination with other variables. Konig et al. [59] emphasize that polypharmacy can significantly impact the diagnosis of sarcopenia, as it has been associated with lower ASMI, a crucial variable in diagnosing the syndrome. The prevalence of polypharmacy increases with age and has significant implications for the health of older adults. It heightens the risk of falls, fractures, cognitive impairment, decline in physical function, mortality, frailty, hospitalization, and hospital readmission. These effects emphasize the importance of including polypharmacy as a fundamental aspect in a comprehensive assessment of older adults [60,61,62,63,64,65,66].
New sarcopenia screening tools have also been developed by other authors, including the Mini Sarcopenia Risk Assessment (MSRA) and its two variants: MSRA-7 and MSRA-5. These tools have demonstrated improved sensitivity in identifying sarcopenia among older Chinese adults [67]. However, when the Asian Working Group for Sarcopenia (AWGS) criteria were used to diagnose sarcopenia, the researchers observed that 15.9% of older adults had sarcopenia, whereas Sarc-F identified 12%, MSRA-7 identified 34.4%, and MSRA-5 identified 39.99% [67]. Similar to Sarc-F, MSRA is a screening tool that consists of subjective questions based on a theoretical framework of risk factors for sarcopenia, such as hospitalization, physical activity level, dietary habits, and weight loss [68]. In contrast, the Sarc-Global supplements the Sarc-CalF questionnaire with objective measurements derived from rigorous statistical tests. Indeed, our robust methodology for variables selection and test can enhance the reliability of Sarc-Global as a sarcopenia risk screening tool.
In our study, when the EWGSOP criteria were used to diagnose sarcopenia, we observed 21.5% of sarcopenia, a finding that aligns closely with another Brazilian study also utilizing the EWGSOP criteria, which reported a prevalence rate of 18% [34]. In the same cohort, the Sarc-Global identified 35,9% of risk of the syndrome. Importantly, 63 from the 85 older adults with sarcopenia (EWGSOP2) were effectively identified as in risk of sarcopenic when using the Sarc-Global assessment tool, whereas Sarc-CalF and Sarc-F tools identified only 29 and 18 of these individuals, respectively.
Our study shares certain limitations with similar studies, which are worth highlighting. Firstly, our study population predominantly comprised women, reflecting the broader context in Brazil, where 76% of all primary care consultations between 2016 and 2018 involved women [69]. Furthermore, our study focused exclusively on community-dwelling older adults. Therefore, further research is needed to validate the applicability of Sarc-Global within institutionalized or hospitalized older adults.
On the other hand, our study design demonstrates robustness, which is a significant strength. Additionally, the number of participants in our sample aligns with similar studies investigating sarcopenia in older adults. All participants were recruited from the same community, thereby being exposed to similar environmental factors that may influence sarcopenia. This aspect enhances the coherence of our dataset. Furthermore, the population of São Paulo city exhibits significant ethnic diversity, which suggests the potential applicability of Sarc-Global across various populations. Our data collection was performed by a single evaluator, ensuring consistency. Moreover, our protocol for diagnosing sarcopenia strictly adhered to the criteria outlined by the EWGSOP2, establishing a rigorous and reliable diagnostic framework.
5. Conclusions
In conclusion, the Sarc-Global, a novel user-friendly sarcopenia risk screening tool developed in our study, exhibited a good specificity and superior sensitivity in identifying individuals at risk of sarcopenia compared to existing tools. We recommend further research to evaluate its prognostic value in relation to adverse outcomes associated with sarcopenia, with the aim of expanding its application in clinical practice.
Author Contributions
NCL: Conceptualization, Methodology, Investigation, Formal analysis, Data curation, Visualization, Writing of the initial draft. DLW: Conceptualization, Methodology, Project administration, Writing of the initial draf; ACCV: Investigation, Formal analysis; NVM: Investigation, Formal analysis; WJ: Resources, Investigation; AB: Resources, Investigation; DF: Resources, Investigation; RT: final review and final writing; GB: Conceptualization, Methodology, Data curation, Supervision, Writing of the initial draft. All the authors critically revised the manuscript, approved its final version and are fully accountable for ensuring the integrity and accuracy its data.
Funding
This research received no external funding of Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) (process number 88887.511605/2020-00).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of NAME OF INSTITUTE (CAPEPesq n 15359, February 02, 2017).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors thank the patients, the ambulatory of the Geriatric Service at the Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HC-FMUSP), the Department of Research Laboratory in Rheumatology (LIM-17), in particular Lilian Takayama for their technical assistance during the study, the Danilo Alves, and Leandro Ferreira (Smart Statistical Analysis) for the statistical analysis of the data. The authors thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for funding this project (process number 88887.511605/2020-00).
Conflicts of Interest
No conflict of interest to declare.
References
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F. et al. European Working Group on Sarcopenia in Older People. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing, 2010; 39, 412-23. [Google Scholar]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol 1998, 147, 755-63. [Google Scholar] [CrossRef]
- Alexandre, T.S.; Duarte, Y.A.; Santos, J.L.; Wong, R.; Lebrão, M.L. Prevalence and associated factors of sarcopenia among elderly in Brazil: findings from the SABE study. J Nutr Health Aging, 2014; 18, 284-90. [Google Scholar]
- Arango-Lopera, V.E.; Arroyo, P.; Gutiérrez-Robledo, L.M.; Pérez-Zepeda, M.U. Prevalence of sarcopenia in Mexico City. European Geriatric Medicine, 2012; 3, 157-160. [Google Scholar]
- Beaudart, C.; Reginster, J.Y.; Petermans, J.; Gillain, S.; Quabron, A.; Locquet, M.; Slomian, J.; Buckinx, F.; Bruyère, O. Quality of life and physical components linked to sarcopenia: The SarcoPhAge study. Exp Gerontol, 2015; 69, 103-10. [Google Scholar]
- Landi, F.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.; Bernabei, R.; Onder, G. Sarcopenia as a risk factor for falls in elderly individuals: results from the ilSIRENTE study. Clin Nutr, 2012; 31, 652-658. [Google Scholar]
- Barbosa-Silva, T.G.; Bielemann, R.M.; Gonzalez, M.C.; Menezes, A.M. Prevalence of sarcopenia among community-dwelling elderly of a medium-sized South American city: results of the COMO VAI? study. J Cachexia Sarcopenia Muscle. 2016, 7, 136–143. [Google Scholar] [CrossRef]
- Kitamura, A.; Seino, S.; Abe, T.; Nofuji, Y.; Yokoyama, Y.; Amano, H.; Nishi, M.; Taniguchi, Y.; Narita, M.; Fujiwara, Y.; Shinkai, S. Sarcopenia: prevalence, associated factors, and the risk of mortality and disability in Japanese older adults. J Cachexia Sarcopenia Muscle, 2021; 12, 30-38. [Google Scholar]
- Bertschi, D.; Kiss, C.M.; Beerli, N.; Kressig, R.W. Sarcopenia in hospitalized geriatric patients: insights into prevalence and associated parameters using new EWGSOP2 guidelines. Eur J Clin Nutr, 2021; 75, 653-660. [Google Scholar]
- Pérez-Sousa, M.Á.; Pozo-Cruz, J.D.; Cano-Gutiérrez, C.A.; Izquierdo, M.; Ramírez-Vélez, R. High Prevalence of Probable Sarcopenia in a Representative Sample From Colombia: Implications for Geriatrics in Latin America. J Am Med Dir Assoc, 2021; 22, 859-864.e1. [Google Scholar]
- Laviano, A.; Gori, C.; Rianda, S. Sarcopenia and nutrition. Adv Food Nutr Res, 2014; 71, 101-136. [Google Scholar]
- Edwards, M.H.; Buehring, B. Novel Approaches to the Diagnosis of Sarcopenia. J Clin Densitom, 2015; 18, 472-477. [Google Scholar]
- Visser, M.; Schaap, L.A. Consequences of sarcopenia. Clin Geriatr Med. 2011; 27, 387-399. [Google Scholar]
- Makiura, D.; Ono, R.; Inoue, J.; Fukuta, A.; Kashiwa, M.; Miura, Y.; Oshikiri, T.; Nakamura, T.; Kakeji, Y.; Sakai, Y. Impact of Sarcopenia on Unplanned Readmission and Survival After Esophagectomy in Patients with Esophageal Cancer. Ann Surg Oncol, 2018; 25, 456-464. [Google Scholar]
- Bouchard, D.R.; Dionne, I.J.; Brochu, M. Sarcopenic/obesity and physical capacity in older men and women: data from the Nutrition as a Determinant of Successful Aging (NuAge)-the Quebec longitudinal Study. Obesity, 2009; 17, 2082-2088. [Google Scholar]
- Li, C.W.; Yu, K.; Shyh-Chang, N.; Li, G.X.; Jiang, L.J.; Yu, S.L.; Xu, L.Y.; Liu, R.J.; Guo, Z.J.; Xie, H.Y.; Li, R.R.; Ying, J.; Li, K.; Li, D.J. Circulating factors associated with sarcopenia during ageing and after intensive lifestyle intervention. J Cachexia Sarcopenia Muscle, 2019; 10, 586-600. [Google Scholar]
- Ohtsubo, T.; Nozoe, M.; Kanai, M.; Yasumoto, U.K. Association of sarcopenia and physical activity with functional outcome in older Asian patients hospitalized for rehabilitation. Aging Clin Exp Res. 2021. [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T. et al. Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing, 2019; 48, 16-31. [Google Scholar]
- Malmstrom, T.K.; Morley, J.E. SARC-F: a simple questionnaire to rapidly diagnose sarcopenia. J Am Med Dir Assoc, 2013; 14, 531-532. [Google Scholar]
- Woo, J.; Leung, J.; Morley, J.E. Validating the SARC-F: a suitable community screening tool for sarcopenia? J Am Med Dir Assoc, 2014; 15, 630-634. [Google Scholar]
- Sánchez-Rodríguez, D.; Marco, E.; Dávalos-Yerovi, V.; López-Escobar, J.; Messaggi-Sartor, M.; Barrera, C. et al. Translation and Validation of the Spanish Version of the SARC-F Questionnaire to Assess Sarcopenia in Older People. J Nutr Health Aging, 2019; 23, 518-524. [Google Scholar]
- Li, M.; Kong, Y.; Chen, H.; Chu, A.; Song, G.; Cui, Y. Accuracy and prognostic ability of the SARC-F questionnaire and Ishii's score in the screening of sarcopenia in geriatric inpatients. Braz J Med Biol Res. 2019; 52, e8204. [Google Scholar]
- Zasadzka, E.; Pieczyńska, A.; Trzmiel, T.; Pawlaczyk, M. Polish Translation and Validation of the SARC-F Tool for the Assessment of Sarcopenia. Clin Interv Aging, 2020; 22, 567-574. [Google Scholar]
- Kim, S.; Kim, M.; Won, C.W. Validation of the Korean Version of the SARC-F Questionnaire to Assess Sarcopenia: Korean Frailty and Aging Cohort Study. J Am Med Dir Assoc, 2018; 19, 40-45. [Google Scholar]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: a symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J Cachexia Sarcopenia Muscle, 2016; 7, 28-36. [Google Scholar]
- Bahat, G.; Yilmaz, O.; Kılıç, C.; Oren, M.M.; Karan, M.A. Performance of SARC-F in Regard to Sarcopenia Definitions, Muscle Mass and Functional Measures. J Nutr Health Aging, 2018; 22, 898-903. [Google Scholar]
- Barbosa-Silva, T.G.; Menezes, A.M.; Bielemann, R.M.; Malmstrom, T.K.; Gonzalez, M.C. Enhancing SARC-F: Improving Sarcopenia Screening in the Clinical Practice. J Am Med Dir Assoc, 2016; 17, 1136-1141. [Google Scholar]
- Voelker, S.N.; Michalopoulos, N.; Maier, A.B.; Reijnierse, E.M. Reliability and Concurrent Validity of the SARC-F and Its Modified Versions: A Systematic Review and Meta-Analysis. J Am Med Dir Assoc, 2021; 16. [Google Scholar]
- Dovjak, P. Polypharmacy in elderly people. Wien Med Wochenschr, 2022; 172, 109-113. [Google Scholar]
- Schenker, Y.; Park, S.Y.; Jeong, K.; Pruskowski, J.; Kavalieratos, D.; Resick, J.; Abernethy, A.; Kutner, J.S. Associations Between Polypharmacy, Symptom Burden, and Quality of Life in Patients with Advanced, Life-Limiting Illness. J Gen Intern Med, 2019; 34, 559-566. [Google Scholar]
- Abe, N.; Kakamu, T.; Kumagai, T.; Hidaka, T.; Masuishi, Y.; Endo, S.; Kasuga, H.; Fukushima, T. Polypharmacy at admission prolongs length of hospitalization in gastrointestinal surgery patients. Geriatr Gerontol Int, 2020; 20, 1085-1090. [Google Scholar]
- Salinas-Rodríguez, A.; Manrique-Espinoza, B.; Rivera-Almaraz, A.; Ávila-Funes, J.A. Polypharmacy is associated with multiplem health-related outcomes in Mexican community-dwelling older adults. Salud Publica Mex, 2020; 62, 246-254. [Google Scholar]
- Romano-Lieber, N.S.; Corona, L.P.; Marques, L.F.G.; Secoli, S.R. Survival of the elderly and exposition to polypharmacy in the city of São Paulo, Brazil: SABE Study. Rev Bras Epidemiol, 2019; 21. [Google Scholar]
- Moreira, V.G.; Perez, M.; Lourenço, R.A. Prevalence of sarcopenia and its associated factors: the impact of muscle mass, gait speed, and handgrip strength reference values on reported frequencies. Clinics, 2019; 8. [Google Scholar]
- Roberts, H.C.; Denison, H.J.; Martin, H.J. et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing, 2011; 40, 423-429. [Google Scholar]
- Carnevale, V.; Castriotta, V.; Piscitelli, P.A.; Nieddu, L.; Mattera, M.; Guglielmi, G.; Scillitani, A. Assessment of Skeletal Muscle Mass in Older People: Comparison Between 2 Anthropometry-Based Methods and Dual-Energy X-ray Absorptiometry. J Am Med Dir Assoc, 2018; 19, 793-796. [Google Scholar]
- Bauer, J.; Morley, J.E.; Schols, A.M.W.J.; Ferrucci, L.; Cruz-Jentoft, A.J.; Dent, E.; Baracos, V.E.; Crawford, J.A.; Doehner, W.; Heymsfield, S.B.; Jatoi, A.; Kalantar-Zadeh, K.; Lainscak, M.; Landi, F.; Laviano, A.; Mancuso, M.; Muscaritoli, M.; Prado, C.M.; Strasser, F.; von Haehling, S.; Coats, A.J.S.; Anker, S.D. Sarcopenia: A Time for Action. An SCWD Position Paper. J Cachexia Sarcopenia Muscle, 2019; 10, 956-961. [Google Scholar]
- da Luz, M.C.L.; Pinho, C.P.S.; Bezerra, G.K.A. et al. SARC-F and SARC-CalF in screening for sarcopenia in older adults with Parkinson's disease. Experimental Gerontology. 2021. [Google Scholar] [CrossRef]
- Williams, G.R.; Al-Obaidi, M.; Dai, C.; Bhatia, S.; Giri, S. SARC-F for screening of sarcopenia among older adults with cancer. Cancer, 2021; 127, 1469-1475. [Google Scholar]
- Ushiro, K.; Nishikawa, H.; Matsui, M.; Ogura, T.; Takeuchi, T.; Goto, M. et al. Comparison of SARC-F Score among Gastrointestinal Diseases. Journal of Clinical Medicine, 2021; 10, 4099. [Google Scholar]
- Fu, X.; Tian, Z.; Thapa, S.; Sun, H.; Wen, S.; Xiong, H.; Yu, S. Comparing SARC-F with SARC-CalF for screening sarcopenia in advanced cancer patients. Clin Nutr, 2020; 39, 3337-3345. [Google Scholar]
- Ishida, Y.; Maeda, K.; Ueshima, J. et al. The SARC-F Score on Admission Predicts Falls during Hospitalization in Older Adults. J Nutr Health Aging. 2021, v.25, p399–404. [Google Scholar] [CrossRef]
- Malas, F.Ü.; Kara, M.; Özçakar, L. SARC-F as a case-finding tool in sarcopenia: valid or unnecessary? Aging Clin Exp Res 2021, 33, 2305–2306. [Google Scholar] [CrossRef]
- Piotrowicz, K.; Głuszewska, A.; Czesak, J.; Fedyk-Łukasik, M.; Klimek, E.; Sánchez-Rodríguez, D.; Skalska, A.; Gryglewska, B.; Grodzicki, T.; Gąsowski, J. SARC-F as a case-finding tool for sarcopenia according to the EWGSOP2. National validation and comparison with other diagnostic standards. Aging Clin Exp Res. 2021, v.33, p1821–1829. [Google Scholar] [CrossRef]
- Mo, Y.H.; Zhong, J.; Dong, X.; Su, Y.D.; Deng, W.Y.; Yao, X.M.; Liu, B.B.; Wang, X.Q.; Wang, X.H. Comparison of Three Screening Methods for Sarcopenia in Community-Dwelling Older Persons. J Am Med Dir Assoc 2021, 22, 746-750. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Hu, X.; Xie, L.; Zhang, L.; Zhou, J.; Lin, J. et al. Screening Sarcopenia in Community-Dwelling Older Adults: SARC-F vs SARC-F Combined with CalF Circumference (SARC-CalF). J Am Med Dir Assoc 2018, 19, 277.e1-277.e8. [Google Scholar] [CrossRef] [PubMed]
- Bahat, G.; Oren, M.M.; Yilmaz, O.; Kılıç, C.; Aydin, K.; Karan, M.A. Comparing SARC-F with SARC-CalF to Screen Sarcopenia in Community Living Older Adults. J Nutr Health Aging 2018, 22, 1034-1038. [Google Scholar] [CrossRef]
- Rodrigues, F.W.; Burgel, C.F.; Brito, J.E.; Baumgardt, E.; de Araújo, B.E.; Silva, F.M. SARC-CalF tool has no significant prognostic value in hospitalized patients: a prospective cohort study. Nutr. Clin. Pract 2021, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Chaiwat, O.; Wongyingsinn, M.; Muangpaisan, W.; Chalermsri, C.; Siriussawakul, A.; Pramyothin, P.; Thitisakulchai, P.; Limpawattana, P.; Thanakiattiwibun, C. A simpler screening tool for sarcopenia in surgical patients. PLoS One 2021, 16. [Google Scholar] [CrossRef] [PubMed]
- Simsek, H.; Meseri, R.; Sahin, S.; Kilavuz, A.; Bicakli, D.H.; Uyar, M. ; Savas. S.; Sarac, F.; Akcicek, F. Prevalence of sarcopenia and related factors in community-dwelling elderly individuals. Saudi Med J 2019, 40, 568-574. [Google Scholar] [CrossRef] [PubMed]
- Swan, L.; Warters, A.; O'Sullivan, M. Socioeconomic Disadvantage is Associated with Probable Sarcopenia in Community-Dwelling Older Adults: Findings from the English Longitudinal Study of Ageing. J Frailty Aging 2022, 11, 398-406. [Google Scholar] [CrossRef]
- Wu, C.H.; Chen, K.T.; Hou, M.T.; Chang, Y.F.; Chang, C.S.; Liu, P.Y.; Wu, J.; Chiu, C.J.; Jou, I.M.; Chen, C.Y. Prevalence and associated factors of sarcopenia and severe sarcopenia in older Taiwanese living in rural community: the Tianliao Old People study 04. Geriatr Gerontol Int 2014, 14, 69-75. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Grip Strength: An Indispensable Biomarker For Older Adults. Clin Interv Aging 2019, 14, 1681–1691. [Google Scholar] [CrossRef] [PubMed]
- Celis-Morales, C.A.; Welsh, P.; Lyall, D.M.; Steell, L.; Petermann, F.; Anderson, J.; Iliodromiti, S.; Sillars, A.; Graham, N.; Mackay, D.F.; Pell, J.P.; Gill, J.M.R.; Sattar, N.; Gray, S.R. Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: prospective cohort study of half a million UK Biobank participants. BMJ 2018, 8. [Google Scholar] [CrossRef]
- Gutiérrez-Hermosillo, H.; de León-González, E.D.; Medina-Chávez, J.H.; Torres-Naranjo, F.; Martínez-Cordero, C. , Ferrari, S. Hand grip strength and early mortality after hip fracture. Arch Osteoporos 2020, 15, 185. [Google Scholar] [CrossRef] [PubMed]
- König, M.; Spira, D.; Demuth, I.; Steinhagen-Thiessen, E.; Norman, K. Polypharmacy as a Risk Factor for Clinically Relevant Sarcopenia: Results From the Berlin Aging Study II. J Gerontol A Biol Sci Med Sci 2017, 73, 117-122. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Xie, W.; Wang, X.; Dong, X.; Mo, Y.; Liu, D. et al. The Prevalence of Sarcopenia among Hunan Province Community-Dwelling Adults Aged 60 Years and Older and Its Relationship with Lifestyle: Diagnostic Criteria from the Asian Working Group for Sarcopenia 2019 Update. Medicina 2022, 58, 1562. [Google Scholar] [CrossRef]
- Chew, S.T.H.; Tey, S.L.; Yalawar, M. et al. Prevalence and associated factors of sarcopenia in community-dwelling older adults at risk of malnutrition. BMC Geriatr 2022, 22, 997. [Google Scholar] [CrossRef] [PubMed]
- König, M.; Spira, D.; Demuth, I.; Steinhagen-Thiessen, E.; Norman, K. Polypharmacy as a Risk Factor for Clinically Relevant Sarcopenia: Results From the Berlin Aging Study II. J Gerontol A Biol Sci Med Sci 2017, 73, 117-122. [Google Scholar] [CrossRef] [PubMed]
- Pana, A.; Sourtzi, P.; Kalokairinou, A.; Velonaki, V.S. Sarcopenia and polypharmacy among older adults: A scoping review of the literature. Arch Gerontol Geriatr 2022, 98, 104520. [Google Scholar] [CrossRef] [PubMed]
- Mabuchi, T.; Hosomi, K.; Yokoyama, S.; Takada, M. Polypharmacy in elderly patients in Japan: Analysis of Japanese real-world databases. J Clin Pharm Ther. 2020; 45, 991-996. [Google Scholar]
- Ambrose, A.F.; Cruz, L.; Paul, G. Falls and Fractures: A systematic approach to screening and prevention. Maturitas, 2015; 82, 85-93. [Google Scholar]
- Kojima, T.; Akishita, M.; Nakamura, T.; Nomura, K.; Ogawa, S.; Iijima, K.; Eto, M.; Ouchi, Y. Polypharmacy as a risk for fall occurrence in geriatric outpatients. Geriatr Gerontol Int, 2012; 12, 425-30. [Google Scholar]
- Helgadóttir, B.; Laflamme, L.; Monárrez-Espino, J.; Möller, J. Medication and fall injury in the elderly population; do individual demographics, health status and lifestyle matter? BMC Geriatr, 9: v.23, p.14, 2014; 14, 92. [Google Scholar]
- Veronese, N.; Stubbs, B.; Noale, M.; Solmi, M.; Pilotto, A.; Vaona, A.; Demurtas, J.; Mueller, C.; Huntley, J.; Crepaldi, G.; Maggi, S. Polypharmacy Is Associated With Higher Frailty Risk in Older People: An 8-Year Longitudinal Cohort Study. J Am Med Dir Assoc, 2017; 18, 624-628. [Google Scholar]
- Saum, K.U.; Schöttker, B.; Meid, A.D.; Holleczek, B.; Haefeli, W.E.; Hauer, K.; Brenner, H. Is Polypharmacy Associated with Frailty in Older People? Results From the ESTHER Cohort Study. J Am Geriatr Soc, 2017; 65, e27-e32. [Google Scholar]
- Yang, M.; Hu, X.; Xie, L.; Zhang, L.; Zhou, J.; Lin, J.; Wang, Y.; Li, Y.; Han, Z.; Zhang, D.; Zuo, Y.; Li, Y. Comparing Mini Sarcopenia Risk Assessment With SARC-F for Screening Sarcopenia in Community-Dwelling Older Adults. J Am Med Dir Assoc. 2019, 20, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.P.; Micciolo, R.; Rubele, S.; Fantin, F.; Caliari, C.; Zoico, E.; Mazzali, G.; Ferrari, E.; Volpato, S.; Zamboni, M. Assessing the Risk of Sarcopenia in the Elderly: The Mini Sarcopenia Risk Assessment (MSRA) Questionnaire. J Nutr Health Aging 2017, 21, 743-749. [Google Scholar] [CrossRef]
- Brasil. Ministério da Saúde. Plano Nacional de Saúde 2020-2023. Brasília/DF, Fevereiro de 2020.
Figure 1.
Sarc-Global – new sarcopenia screening questionnaire.
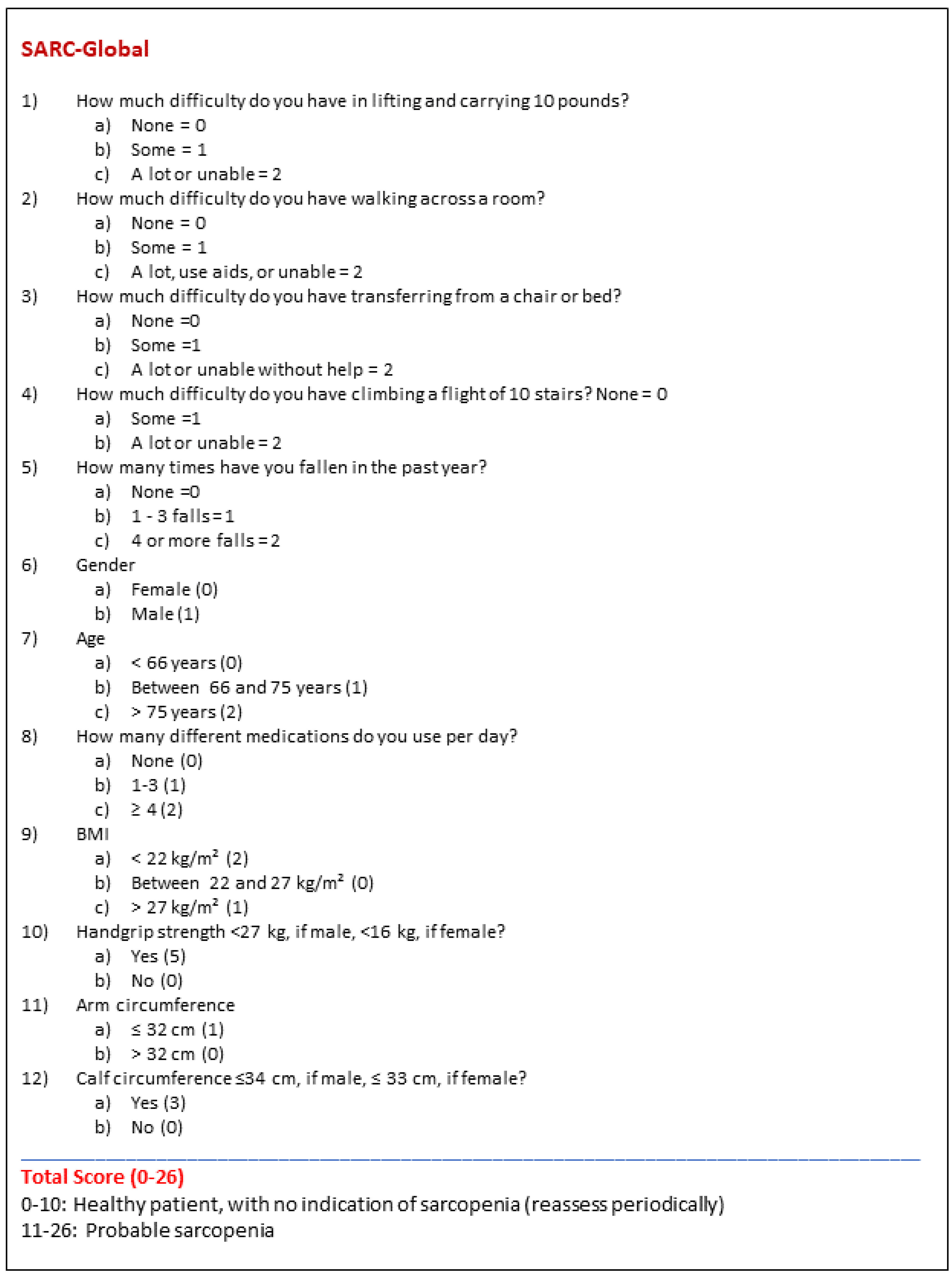
Figure 2.
Area under the curve (AUC) to identify cut-off accuracy of the new sarcopenia screening tool.
Figure 2.
Area under the curve (AUC) to identify cut-off accuracy of the new sarcopenia screening tool.
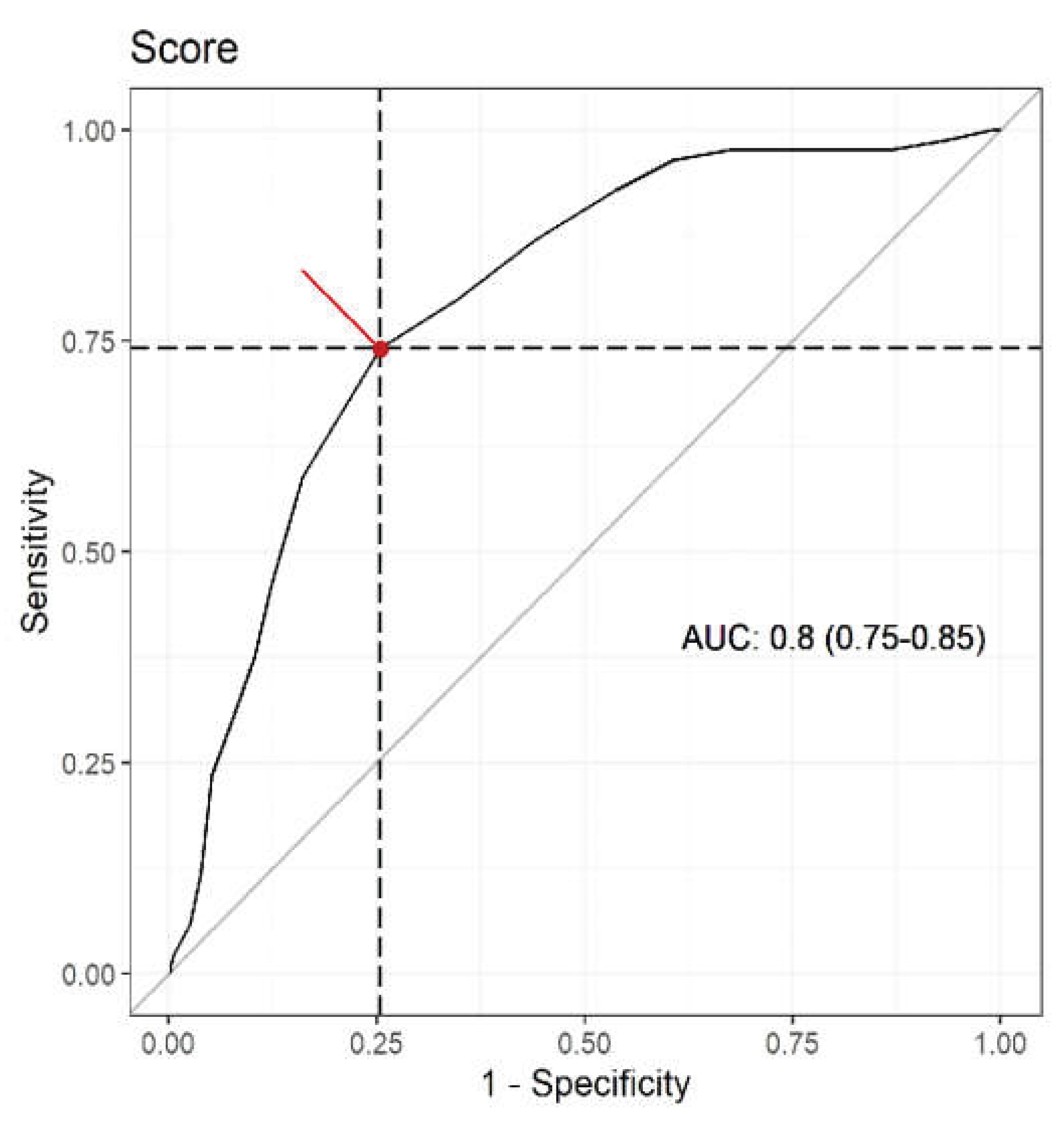

Table 1.
Demographic and anthropometric data of the study participants.
| Characteristicsa | Total (n=395) | Sarc-Global Creation | Sarc-Global validation |
|---|---|---|---|
| N = 395 | N = 277 | N = 118 | |
| Age, years | 70.7 ± 7.54 | 70.87 ± 7.75 | 70.28 ± 7.05 |
| Females, N (%) | 320 (81) | 225 (81.2) | 95 (80.5) |
| Males, N (%) | 75 (19) | 52 (18.8) | 23 (19.5) |
| Number of medications in use | |||
| None, N (%) | 47 (11.9) | 31 (11.2) | 16 (13.6) |
| One, N (%) | 57 (14.4) | 39 (14.1) | 18 (15.3) |
| Two, N (%) | 53 (13.4) | 36 (13) | 17 (14.4) |
| Three, N (%) | 39 (9.9) | 32 (11.5) | 7 (5.9) |
| Four or more, N (%) | 199 (50.4) | 139 (50.2) | 60 (50.8) |
| Weight, kg | 67.82 ± 14.24 | 67.55 ± 14.24 | 68.47 ± 14.27 |
| Height, m | 1.57 ± 0.08 | 1.57 ± 0.08 | 1.57 ± 0.08 |
| BMI, kg/m² | 27.57 ± 5.29 | 27.48 ± 5.35 | 27.77 ± 5.16 |
| AC, cm | 32.11 ± 4.49 | 31.97 ± 4.47 | 32,42 ± 4.55 |
| CC, cm | 35.91 ± 3.53 | 35.83 ± 3.60 | 36.11 ± 3.38 |
| TSFT, mm | 23.25 ± 8.85 | 23.15 ± 8.76 | 23,49 ± 9.11 |
| BSFT, mm | 15.15 ± 7.96 | 14.93 ± 7.87 | 15.67 ± 8.20 |
| SSFT, mm | 21.89 ± 9.03 | 21.69 ± 9.20 | 22.35 ± 8.63 |
| SISFT, mm | 22.67 ± 9.37 | 22.48 ± 9.19 | 23.09 ± 9.80 |
| HGS, kg | 17.13 ± 7.16 | 16.82 ± 7.0 | 17.86 ± 7.50 |
Abbreviations: BMI, body mass index; AC, arm circumference; CC, calf circumference; TSFT, triceps skinfold thickness; BSFT, biceps skinfold thickness; SSFT, subscapular skinfold thickness; SISFT, suprailiac skinfold thickness; HGS, handgrip strength. a Data are presented as weighted percentage and unweighted frequency % (N) for categorical variables and weighted mean (standard errors, SE) for continuous variables.
Table 2.
Multiple logistic regression analysis to determine the score of each variable in the Sarc-Global questionnaire.
Table 2.
Multiple logistic regression analysis to determine the score of each variable in the Sarc-Global questionnaire.
| Variable | Category | Reference | Coefficient | OR | 95%CI (OR) | p-value |
|---|---|---|---|---|---|---|
| Medication in use | 1-3 | None | 0.686 | 1.985 | 1.278;3.084 | <0.001 |
| ≥4 | 1.107 | 3.027 | 2.055;4.459 | <0.001 | ||
| BMI (kg/m²) | >27 | 22-27 | 0.743 | 2.102 | 1.186;3.726 | <0.001 |
| <22 | 1.063 | 2.895 | 1.436;5.857 | <0.001 | ||
| Gender | Male | Female | 0.637 | 1.890 | 0.997;3.584 | 0.058 |
| Age (years) | 66-75 | <66 | 0.790 | 2.203 | 1.229;3.948 | <0.001 |
| >75 | 1.143 | 3.137 | 1.330;7.396 | <0.001 | ||
| HGS (kg) | Low (M<27; F<16) |
Normal (M≥27; F≥16) |
1.801 | 6.057 | 2.772;13.236 | <0.001 |
| AC (cm) | ≤32 | >32 | 0.738 | 2.092 | 1.423;3.076 | <0.001 |
| CC (cm) | Low (M ≤ 34; F ≤ 33) |
Normal (M >34; F>33) | 1.368 | 3.927 | 2.173;7.096 | <0.001 |
Abbreviations: OR, odds ratio; CI, confidence interval; BMI, body mass index; AC, arm circumference; CC, calf circumference; HGS, handgrip strength.
Table 3.
Analysis of accuracy, sensitivity and specificity of the Sarc-Global, Sarc-F and Sarc-CalF instruments in relation to the sarcopenia diagnosis by the EWGSOP.
Table 3.
Analysis of accuracy, sensitivity and specificity of the Sarc-Global, Sarc-F and Sarc-CalF instruments in relation to the sarcopenia diagnosis by the EWGSOP.
| Measure | Sarc-Global | Sarc-F | Sarc-CalF |
|---|---|---|---|
| Accuracy | 0.744 (0.699 – 0.785) | 0.696 (0.649 – 0.740) | 0.798 (0.755 – 0.834) |
| Sensitivity | 0.741 (0.639 – 0.823) | 0.212 (0.138 – 0.311) | 0.341 (0.249 – 0.447) |
| Specificity | 0.745 (0.694 – 0.791) | 0.829 (0.783 – 0.867) | 0.923 (0.887 – 0.948) |
| PPV | 0.443 (0.365 – 0.526) | 0.254 (0.166 – 0.366) | 0.547 (0.415 – 0.674) |
| NPV | 0.913 (0.871 – 0.942) | 0.793 (0.746 – 0.834) | 0.836 (0.793 – 0.872) |
Abbreviations: PPV, positive predictive value (PPV); NPV, negative predictive value.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



