
Submitted:
05 April 2024
Posted:
08 April 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: The Coronavirus Disease 2019 (COVID-19) pandemic presented a new challenge in modern medicine. The development of vaccines was followed by massive population vaccinations. A few reports on post-vaccination allergic reactions have made patients and medical personnel uneasy as to anti-COVID-19 vaccines’ allergising potential. Most of the studies in this area to date have been small, and some that were based on global databases skipped most of the allergic diseases and concentrated only on anaphylaxis. We aimed to analyse the incidence of serious allergic reactions based on the EudraVigilance (EV) database, regardless of the reported symptoms and allergy mechanism. Methods: The total number of administrated vaccine doses was extracted on the 5th October 2023 from Vaccine Tracker and included all administrations since vaccinations began in the European Economic Area (EEA). Data on serious allergic reactions to COVID-19 vaccines was extracted from the EudraVigilance database with the same time point. The code names of 147 allergic symptoms or diseases were used. Results: The frequency of serious allergic reactions per 100,000 administered vaccine doses was 1.53 for Comirnaty, 2.16 for Spikevax, 88.6 for Vaxzevria, 2.11 for Janssen, 7.9 for Novavax, 13.3 for VidPrevtyn Beta and 3.1 for Valneva. The most prevalent reported reactions were oedema (0.46) and anaphylaxis (0.40). Only 6% of these reactions were delayed hypersensitivity-oriented. Conclusions: The overall frequency of potential serious allergic reactions to COVID-19 is very rare. Therefore, COVID-19 vaccines seem to be safe for human use. The lowest frequency of allergic reaction was observed for Comirnaty and the highest for Vaxzevria.
Keywords:
vaccination
; drug allergy
; anaphylaxis
; rash
; side effect
; adverse drug reaction
; COVID-19
1. Introduction
The Coronavirus Disease 2019 (COVID-19) pandemic that started in 2019 generated new challenges in modern medicine [1]. Initially, no effective treatment was available and the medical focus was on disease prevention: 1) passive, with social distancing and personal protection, and 2) active, with vaccinations [2]. The ensuing rapid, one-year-long vaccine development process has made societies uneasy about vaccination safety [3,4,5,6]. Although product characteristics and medical society guidelines, such as the European Academy of Allergy and Clinical Immunology (EAACI), highlighted robust safety and low allergenicity of anti-COVID-19 vaccines, reports on anaphylactic reactions still resulted in vaccination reluctance, especially in patients who had experienced drug-related hypersensitivities in the past [1,7,8]. The available COVID-19 vaccines may cause cutaneous adverse effects, including injection site reactions, urticaria, angioedema, exacerbation of atopic eczema, and even anaphylaxis [9]. The severe hypersensitivity symptoms mostly started within 10–30 min of exposure. The most common symptoms were urticaria, itching, flushing, angioedema, shortness of breath, burning sensation and fainting [10]. As the population vaccination process continued, more data was available and hypersensitivity reactions were estimated at 0.66% of doses, with the majority of these being immediate reactions (0.53%) [11]. Delayed hypersensitivity was observed in 0.1% of doses. With the preventive implementation of Skin Prick Tests and Intradermal tests for vaccines and excipients, it was possible to vaccinate over 99% of patients with a high risk of allergic reactions [12,13,14]. Even in cases of severe delayed allergic reactions, new in vitro tests were developed to enable vaccination, with promising results for the future [15].
EudraVigilance (EV) is a European database supervised by the European Medicines Agency (EMA) that gathers reported suspected side effects of drugs that are authorised for users in the European Economic Area [16]. It is open access for all users. A single adverse event report can be submitted by anyone, though they are categorised by reporter, as 1) Healthcare Professional, 2) Non-Healthcare Professional. Apart from the name of the adverse reaction, they are also categorised by seriousness, as 1) Serious and 2) Non-Serious. By definition, adverse events include all harmful symptoms that may have been caused by drugs, even including overdoses. This freedom of reporting can also be perceived as a flaw that results in the appearance of symptoms that are almost impossible to logically connect to the administered drug. It is also worth noting that EV does not gather reports itself. All adverse events are reported to national medical agencies and then transferred digitally to EV. This may result in discrepancies in methodologies, which may affect the final outcome. On the other hand, the database contains such a great number of cases that those flaws might become irrelevant.
COVID-19 Vaccine Tracker is an open-access tool operated by the European Centre of Disease Control and Prevention [17]. It gathers information on the number of anti-COVID-19 vaccines administrated in the European Economic Area. The doses are categorised by the name of the vaccine and country. The report ends on the 5th October 2023 with a total of 981,454,243 doses administered. The number of administered doses can be used for adverse event incidence calculations.
To date, there have been a few reports on the incidence of hypersensitivity and allergic reactions after COVID-19 vaccines. Most of them concentrated on specific populations, such as children, asthmatics, or patients with mastocytosis, and described thoroughly allergic reactions. These were rather limited to a few thousand patients [18,19,20,21,22,23]. A few reports on large databases such as EV were published, though these concentrated mainly on anaphylaxis or anaphylactic shock as life-threatening reactions, which are easily coded in the database [24,25,26,27,28,29,30,31]. Other reactions, such as oedema, urticaria, and maculopapular rash, are difficult to code and thus to find all instances of in the database. In EV, they might also appear as ‘swelling’, ‘blistering’, ‘rash’, or ‘allergy’, especially when they are reported by someone who is not a healthcare professional. Popiołek et al. successfully created a list of reaction names that correspond to the most likely allergic reactions [32]. The list includes 147 names of reactions that are available for filtering in the EV database. They are presented in the supplementary material and also categorised according to the affected organs and suspected mechanism (for example, type I or IV hypersensitivity according to the EAACI classification) [33]. The study aimed to identify, analyse and evaluate the frequency of hypersensitivity reactions to anti-COVID-19 vaccines available in the European Economic Area based on the EudraVigilance database and vaccination tracker.
2. Materials and Methods
The total number of administrated vaccine doses was extracted on the 5th October 2023 from Vaccine Tracker [17]. Data for all COVID-19 vaccines shown in Table 1 were extracted on the 6th of December from the EudraVigilance database using line listing export for all serious adverse events [16]. Serious adverse events include those: life-threatening, resulting in death, requiring hospitalisation, prolonging hospitalisation, resulting in disability or congenital defect.
To calculate the frequency of each allergic reaction for the given vaccine, the reported number of cases for every allergic reaction was divided by the total number of doses administered in EU/EEA countries.
During the analysed period, a total of 567,203,616 doses of Comirnaty, 132,734,949 doses of Spikevax, 56,007,792 doses of Vaxzevria, 16,056,640 doses of Janssen, 225,312 doses of Novavax, 7,524 doses of VidPrevtyn Beta and 2,257 doses of Valneva were distributed in the EEA region.
Statistical Analysis
Categorical data were summarised with the use of frequencies. The chi-square test was used to check for statistical significance of the differences between the grouping variables. The threshold of statistical significance was set at p<0.05. The analyses were performed in Python 3.10 using the Numpy, Pandas and Scipy libraries.
3. Results
Initially, there were 945,909 records in the EudraVigilance database on 6th December related to this study. All records added after the 5th of October 2023 were removed (n=15,489). Next, all records from non-European economic areas were also removed (n=505,958). Thus, the records in the EUDRA database and the COVID-19 Vaccine Tracker database of the European Centre for Disease Control and Prevention referred to the same period and were collected from the same region (European Economic Area). Next, all records that were not considered as an ‘allergic reaction’ were also removed from the database (n=410,793). There were no missing data. In total, there were 13,669 records remaining. These records were further analysed statistically.
3.1. General Characteristics
The dataset included 112 types of allergic reactions (n=13,669). Adverse reactions to the Comirnaty (n=8,734), Spikevax (n=2,857), Vaxzervria (n=1,717), Janssen (n=340), Novavax (n=18), VidPrevtyn Beta (n=1) and Valneva (n=2) vaccine products were analysed. When divided by the total number of doses administered in the EEA region for each vaccine, the frequencies of allergic reactions per 100,000 doses to the analysed vaccines were 1.53 for Comirnaty, 2.16 for Spikevax, 88.6 for Vaxzevria, 2.11 for Janssen, 7.9 for Novavax, 13.3 for VidPrevtyn Beta and 3.1 for Valneva. It must be noted that Novavax, VidPrevtyn Beta and Valneva had much fewer administrations (below 1,000,000), thus the incidence calculations might be uncertain. The results in subgroups according to sex and age are presented in Table 2. In these subgroups, the most reactions occurred in women aged 18–64. In Figure 1, cases are divided according to the year of report, which shows that despite the greatest number of cases being reported in 2021 during the massive, whole-population vaccination, significant numbers were still reported in 2023, probably mostly in people receiving booster doses. In statistical analysis using chi square contingency tables, all comparisons in vaccines, sex and age groups were statistically significant (p<0.001) due to large sample sizes.
3.2. Type of Reaction
All reactions were divided according to time of onset, which also corresponds to the suspected mechanism: 1) Immediate reactions (n=10,853), 2) Delayed reactions (n=830), 3) Unknown time reactions (n=1,986). The proportion is displayed in Figure 2. Unknown time reactions included ‘erythema’, ‘hypersensitivity’, ‘rash’, ‘drug eruption’, ‘injection site reaction’, ‘drug hypersensitivity’, and ‘allergic reaction to excipient’. These code names of reactions were impossible to classify to either immediate or delayed hypersensitivity and due to the construction of the EV database, no additional information is available. The most clinically important reactions according to the number of cases are presented in Figure 3
4. Discussion
The results of our study highlight the safety of COVID-19 vaccines. Serious hypersensitivity events occur in 1.5 cases per 100,000 doses for Comirnaty, up to 88 per 100,000 for Vaxzevria. Our data also highlight the possibly most at-risk population as being adult women <65 years old. The low number of allergic cases reported in the elderly is fortunate, while this group is considered the most vulnerable to COVID [35]. The rationale behind limiting the results to serious events was that the EAACI considers only serious allergic reactions as a potential contraindication for further vaccinations [1]. In addition, non-serious adverse events would include vast numbers of insignificant local reactions and typical side effects, such as increased body temperature [36].
General incidence results are in line with other studies. According to Chu et al.’s meta-analysis of almost 1,400 people who had an adverse reaction to the COVID-19 vaccination’s first dosage, just 6 people (0.4%) had severe reactions after receiving their second dose, while 232 people (17%) only had mild symptoms [37]. In December 2020, the initial US surveillance data revealed a hypersensitivity incidence of 11.1 cases per million doses for the Pfizer-BioNTech COVID-19 vaccine and 2.5 cases per million doses for the Moderna vaccine, with lower rates more recently [38,39]. According to data from Vaccine Safety Datalink Overall, the incidence of COVID-19 mRNA vaccine-associated anaphylaxis is very low, with only 4.8 per million doses for BNT162b2 and 5.1 per million doses for mRNA-1273 [40]. The prevalence of anaphylaxis associated with COVID-19 vaccinations currently appears to be comparable to those observed with other vaccinations.
Before widespread COVID-19 immunisation campaigns started, serious allergic reactions, including anaphylaxis associated with vaccines, were believed to be incredibly unusual events. For instance, between January 2009 and December 2011, the rate of anaphylaxis was 1.31 per million vaccination doses [41].
A commonly known issue is the fact that any adverse reaction experienced in connection with vaccination, such as nausea or subjective oropharyngeal symptoms, which are difficult to evaluate during a physical examination and are frequently psychogenic, is frequently labelled as an allergy. Hourihane et al. reassessed documented cases using the Brighton Collaboration Criteria and criteria by the National Institute of Allergy and Infectious Diseases (NIAID) 2005. They found that 71% of cases previously reported as anaphylaxis were reclassified as not satisfying anaphylaxis criteria [42].
The study by Kyeonghun and colleagues was a large-scale survey based on the WHO database, covering approximately 55 years. They reported that vaccination for DTaP-IPV-Hib is the most common cause of vaccine-associated anaphylaxis and occurs much more frequently [43]. Importantly, despite the extreme rarity of reaction, they found that vaccines presented a relatively high fatality rate once anaphylaxis occurred. The highest fatality rate (15.0%) was associated with the Ad5-vectored COVID-19 vaccine, followed by tuberculosis (9.6%), COVID-19 mRNA (7.2%), cholera (6.3%), influenza (5.8%), encephalitis (3.3%), and hepatitis B (2.4%). In contrast, according to the Vaccine Adverse Event Reporting System in the USA, only 8 (0.97%) of 828 cases of vaccine-related anaphylaxis resulted in death [44]. Such a discrepancy is difficult to explain and might be a result of the great variety of reporting processes around the world. The most important conclusion from this vast analysis is that, among other vaccines, anti-COVID-19 regimens present even fewer hypersensitivity reactions.
Still, it is important to analyse the proportions of each type of reaction, as most of them (73%) are immediate type and respond relatively well to standard treatments [45]. Only 6% (see Figure 1) of all serious reactions were delayed, such as SJS, TEN or maculopapular rash, with difficult treatment and diagnostic processes [15]. These may be patients who cannot undergo standard allergy work-up protocols and thus be disqualified from further vaccinations.
A higher incidence of hypersensitivity to vaccines and other drugs in women has been described before (12,46–49). The reason for this phenomenon remains unclear. Possible explanations include: epigenetics of the X chromosome, higher use of medications in women, longer elimination time, and role of sex hormones. It is also possible that reporting bias contributes to this discrepancy to some extent. However, Watson et al. claim that though women report more drug-related adverse events in general, serious and fatal adverse events are more likely to be reported in men [50].
It is worth comparing the incidence of vaccine allergy with other commonly used drugs. Beta-lactam antibiotics (BL), including penicillins, cephalosporins, monobactams, and carbapenems, are the most widely used antimicrobials because of their effectiveness and safety. Nevertheless, they are also the most prevalent cause of drug-induced hypersensitive reactions [51,52,53]. The penicillin allergy remains the most frequently reported drug allergy. It is estimated that 5–10% of the general public, and up to 19% of hospitalised patients, have a beta-lactam allergy; however, this is confirmed in only 10% of patients [54]. The frequency of beta-lactam allergy reports has grown throughout the years, rising from 1–2% in 1980 to 5–13% in the most recent decades (53,55–57). Patients who receive more health care, particularly women and the elderly, have higher rates [58,59]. The incidence of anaphylaxis caused by penicillin is estimated to be between 0.015% and 0.04%, with fatality rates ranging between 0.0015% and 0.002% [60,61]. It is estimated that 3% of cases of drug-induced anaphylaxis are fatal [62].
Another common cause of antibiotic allergy is sulfonamide antibiotics. Giles et al. pointed out that sulfonamide allergies are reported in approximately 3–8% of patients in the general population [63]. A sulfonamide allergy can present with a wide range of clinical symptoms. These can include delayed cutaneous maculopapular eruptions, which is the most common manifestation of sulfonamide allergy [63,64]. The most prominent known risk factor for a sulfonamide allergy is being persistently HIV positive, especially in those with AIDS [63]. According to Carr et al., 27% of HIV patients treated with trimethoprim/sulfamethoxazole (TMP-SMX) for Pneumocystis Pneumonia experienced hypersensitivity responses [65].
Iodinated contrast media (ICM) generates both immediate and delayed hypersensitivity reactions [66,67]. In a multicentre study of 196,081 patients in Korea, the prevalence of HSR in those who underwent ICM administration was 0.73%, while severe reactions occurred in 0.01%. Regarding severity, 83.2% of the occurrences were categorised as mild HSRs, with a total incidence of 0.61% (1,192 of 196,081), 15.6% as moderate HSRs (0.11%; 224 of 196,081), and 1.2% as severe HSRs [68]. This study showed a comparable, or lower, prevalence of HSR compared to other large studies [69,70].
A large study conducted by Voltolini and colleagues investigated the medical records of patients receiving care in 9 Italian Allergy Centres for experiencing hypersensitivity reactions to ICM and compared them with a control group of 152 subjects that tolerated one or more ICM-enhanced examinations. As described in previous studies, females, and patients under 65 years of age were more likely to experience hypersensitive reactions. Furthermore, potential risk factors for ICM reactions include respiratory allergies and cardiovascular illness, and include a previous reaction, chronic disorders, a history of asthma, adverse drug reactions and food allergy, and a family history of radiologic contrast media reaction [71].
Nonsteroidal anti-inflammatory medications (NSAIDs) belong to the most commonly used medications worldwide [72], which may explain why hypersensitivity reactions to NSAIDs are quite prevalent. NSAID-induced hypersensitivity can range in severity from mild symptoms to severe, potentially life-threatening anaphylaxis [73]. The prevalence of hypersensitivity reactions to NSAIDs in the general population ranges from 0.2% up to 0.6% [74]. However, there are certain patient groups that present much higher hypersensitivity: patients with asthma (21%) or chronic urticaria (20–40%) [75,76,77].
Zhou et al. analysed drug allergy data obtained from the electronic health records of 1,766,328 patients who visited hospitals in Boston from 1990 to 2013. They found that NSAIDs ranked as the 4th most frequently reported drug allergy, with aspirin being the most commonly reported in this group [55,78].
Aspirin has been reported to be the most prevalent NSAID allergy in certain studies, whereas naproxen has been found to be the most common allergy in others [78,79].
In a 6-year study involving almost 4,500 patients by Doña et al., NSAIDs were the drugs most frequently linked to HSRs, with ibuprofen being the most frequent [80].
NSAIDs were the most often reported analgesic allergy until 1993. Opioids, however, are now the allergy that is reported most often. Up to 2006, NSAIDs accounted for just 5–8% of reported drug allergies, while opioids accounted for 10–15% [55].
Local anaesthetics (LAs) are widely used drugs, especially in delivery, dentistry, and surgery. During anaesthesia and surgery, allergic reactions to LAs, particularly anaphylaxis, can be life-threatening. However, numerous studies support the extremely low incidence of IgE-mediated allergic reactions, which are thought to be responsible for less than 1% of all reported reactions (54,81,82). Kvisselgaard et al. claim that various nonallergic mechanisms are usually the main cause of adverse drug reactions to Las [83]. The vasovagal response, which can cause syncope and hypotension, overdose toxicity with paresthaesia, and incorrect medication administration are a few of these [84].
During a period of 10 years, Kvisselgaard and colleagues examined the frequency of IgE-mediated immediate-type perioperative allergic reactions to LAs. They found that out of 162 patients who were suspected of having perioperative allergic reactions and had been exposed to a LA, none of them responded to the relevant LA on subcutaneous provocation. As a result, from 2004 to 2013, no patients in the Danish Anaesthesia Allergy Centre have been diagnosed with LA allergy [85].
Out of 135 events, only two (1.5%) were identified as hypersensitive to a LA in the Harboe et al. study. IgE-mediated allergies to other substances, such as latex, triamcinolone, chlorhexidine, and potentially hexaminolevulinate, were identified in ten reactions (7%) [81].
According to research by Zuo et al., only 6 of 109 patients who were referred to a Chinese anaesthesia allergy clinic and had allergy tests performed with LAs during a ten-year period really had a true allergy to LAs. Out of those patients, the culprit drug was lidocaine in four cases, and ropivacaine in three [86].
The comparison with other drug groups presented above favours COVID-19 vaccines, especially in regards to typically used drugs, such as NSAIDs and beta-lactams. Even among other vaccines, COVID-19 vaccines seem safe and the risk/benefit assessment strongly suggests vaccinations in patients with no post-vaccine allergic reactions.
5. Conclusions
COVID-19 vaccines are safe, especially compared to other vaccines and other groups of pharmaceuticals, as presented above. This information could be supplied to the patient hesitating before vaccination, along with the statement that if a person with no allergic history does not hesitate to take antibiotics, vaccination should also not pose an allergy-related issue. The incidence ranges from 1.5 up to 88 per 100,000 administered doses, with Comirnaty being the safest. The highest number of allergic reactions was reported in adult women <65 years old. Even though the risk of having an allergic reaction is low, given the very large number of administered vaccines, medical personnel, particularly allergologists, need to be prepared to properly handle potential allergic reactions.
Author Contributions
Conceptualisation, J.R. and M.N.; methodology, J.R. and I.P.; software, W.N.; validation, W.N., J.R.; formal analysis, W.N.; investigation, J.R.; resources, M.N.; data curation, W.N.; writing—original draft preparation, J.R. and K.B.; writing—review and editing, W.N. and I.P. and M.N.; visualisation, J.R. and K.B.; supervision, M.N.; project administration, J.R.; funding acquisition, M.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research and APC was funded by the Medical University of Gdansk, Department of Allergology, statutory funding no. 01-10023/0004956/231.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data available upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Barbaud A, Garvey LH, Arcolaci A, Brockow K, Mori F, Mayorga C et al. Allergies and COVID-19 vaccines: An ENDA/EAACI Position paper. Allergy Published Online First: 22. 20 February. [CrossRef]
- Coroiu A, Moran C, Campbell T, Geller AC. Barriers and facilitators of adherence to social distancing recommendations during COVID- 19 among a large international sample of adults. PLoS One 2020;15. [CrossRef]
- Sadoff J, Gray G, Vandebosch A, Cárdenas V, Shukarev G, Grinsztejn B et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N Engl J Med 2021;384:2187–2201.
- Voysey M, Clemens SAC, Madhi SA, Weckx LY, Folegatti PM, Aley PK et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021;397:99–111.
- Baden LR, El Sahly HM, Essink B, Kotloff K, Frey S, Novak R et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N Engl J Med 2021;384:403–416.
- Polack FP, Thomas SJ, Kitchin N, Absalon J, Gurtman A, Lockhart S et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. New England Journal of Medicine 2020;383:2603–2615.
- Smout, A. UK issues anaphylaxis warning on Pfizer vaccine after adverse reactions. Reuters. 2020.https://www.reuters.
- Kruszewski J, Cichocka-Jarosz E, Czarnobilska E, Jutel M, Kulus M, Kuna P et al. Rekomendacje Polskiego Towarzystwa Alergologicznego dotyczące kwalifikacji osób z alergią i anafilaksją do szczepienia przeciw COVID-19. Alergologia Polska - Polish Journal of Allergology 2021;8:1–8.
- Bogdanov G, Bogdanov I, Kazandjieva J, Tsankov N. Cutaneous adverse effects of the available COVID-19 vaccines: Effects of COVID-19 vaccines. Clin Dermatol 2021;39. [CrossRef]
- Gold MS, Amarasinghe A, Greenhawt M, Kelso JM, Kochhar S, Yu-Hor Thong B et al. Anaphylaxis: Revision of the Brighton collaboration case definition. Vaccine 2023;41. [CrossRef]
- Xu J, Vanijcharoenkarn K, Sexton ME, Martin L, Lee FEH, Kuruvilla ME. Delayed Hypersensitivity Reactions Following First Dose of the SARS-CoV2 mRNA Vaccines. J Gen Intern Med. 2021;36. [CrossRef]
- Romantowski J, Kruszewski J, Solarski O, Bant A, Chciałowski A, Pietrzyk I et al. Protocol of safe vaccination against COVID-19 in patients with high risk of allergic reactions. Clin Transl Allergy 2022;12:e12152.
- Mortz CG, Kjaer HF, Rasmussen TH, Rasmussen HM, Garvey LH, Bindslev-Jensen C. Allergy to polyethylene glycol and polysorbates in a patient cohort: Diagnostic work-up and decision points for vaccination during the COVID-19 pandemic. Clin Transl Allergy 2022;12:e12111.
- Nilsson L, Csuth Á, Storsaeter J, Garvey LH, Jenmalm MC. Vaccine allergy: evidence to consider for COVID-19 vaccines. Curr Opin Allergy Clin Immunol 2021;21:401–409.
- Romantowski J, Górska A, Zieliński M, Trzonkowski P, Rucka K, Niedoszytko M. Clinical Application of In Vitro Tests for COVID-19 Vaccine Delayed Hypersensitivity Diagnostics. Int J Mol Sci 2023;24. [CrossRef]
- European Medicines Agency 2017 Annual Report on EudraVigilance for the European Parliament, the Council and the Commission. https://www.ema.europa.eu/en/news/ema-annual-report-2022-published (accessed 29 Dec2023).
- European Centre for Disease Prevention and Control (ECDC). Covid19 Vaccine Tracker. 2023.https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html#uptake-tab (accessed 5 Oct2023).
- Takano T, Hirose M, Yamasaki Y, Hara M, Okada T, Kunishima H. Investigation of the incidence of immunisation stress-related response following COVID-19 vaccination in healthcare workers. Journal of Infection and Chemotherapy 2022;28. [CrossRef]
- Luxi N, Giovanazzi A, Arcolaci A, Bonadonna P, Crivellaro MA, Cutroneo PM et al. Allergic Reactions to COVID-19 Vaccines: Risk Factors, Frequency, Mechanisms and Management. BioDrugs. 2022;36. [CrossRef]
- Marković I, Božan M, Perković T, Paušek K, Nedeljković V, Perković M et al. Incidence of immediate allergic reactions to mRNA COVID-19 vaccines in adults with drug allergies and other allergic disorders. Medicine (United States) 2022;101. [CrossRef]
- Yuksel Bulut H, Ulusoy Severcan E, Ertugrul A. COVID-19 Vaccines Are Safely Tolerated in Adolescents with Cutaneous Mastocytosis. Int Arch Allergy Immunol 2023;184. [CrossRef]
- Ali SB, Perkins G, Ryoo D, Lee M, Tunbridge M, Yuson C et al. AstraZeneca ChAdOx1-S COVID-19 vaccine can be safely administered in patients with EDTA allergy. Allergy, Asthma and Clinical Immunology 2022;18. [CrossRef]
- Novembre E, Tosca M, Caffarelli C, Calvani M, Cardinale F, Castagnoli R et al. Management of BNT162b2 mRNA COVID-19 vaccine in children aged 5–11 years with allergies, asthma, and immunodeficiency: consensus of the Italian Society of Pediatric Allergy and Immunology (SIAIP). Ital J Pediatr. 2022;48. [CrossRef]
- Maltezou HC, Hatziantoniou S, Theodoridou K, Vasileiou K, Anastassopoulou C, Tsakris A. Anaphylaxis rates following mRNA COVID-19 vaccination in children and adolescents: Analysis of data reported to EudraVigilance. Vaccine 2023;41. [CrossRef]
- Yoon D, Jeon HL, Noh Y, Choe YJ, Choe SA, Jung J et al. A Nationwide Survey of mRNA COVID-19 Vaccinee’s Experiences on Adverse Events and Its Associated Factors. J Korean Med Sci 2023;38. [CrossRef]
- Jaggers J, Samarakoon U, Fu X, Gonzalez-Estrada A, Anvari S, Chong HJ et al. Anaphylaxis after COVID-19 vaccination: A registry-based study. Journal of Allergy and Clinical Immunology: In Practice 2022;10. [CrossRef]
- Toledo-Salinas C, Scheffler-Mendoza SC, Castano-Jaramillo LM, Ortega-Martell JA, Del Rio-Navarro BE, Santibáñez-Copado AM et al. Anaphylaxis to SARS-CoV-2 Vaccines in the Setting of a Nationwide Passive Epidemiological Surveillance Program. J Clin Immunol 2022;42. [CrossRef]
- Macy E, Pandya S, Sheikh J, Burnette A, Shi JM, Chung J et al. Population-Based Incidence, Severity, and Risk Factors Associated with Treated Acute-Onset COVID-19 mRNA Vaccination–Associated Hypersensitivity Reactions. Journal of Allergy and Clinical Immunology: In Practice 2022;10. [CrossRef]
- Hatziantoniou S, Anastassopoulou C, Lampropoulou V, Maltezou HC, Andreakos E, Poland GA et al. Comparative assessment of allergic reactions to COVID-19 vaccines in Europe and the United States. Allergy: European Journal of Allergy and Clinical Immunology. 2022;77. [CrossRef]
- Montano, D. Frequency and Associations of Adverse Reactions of COVID-19 Vaccines Reported to Pharmacovigilance Systems in the European Union and the United States. Front Public Health 2022;9. [CrossRef]
- Boufidou F, Hatziantoniou S, Theodoridou K, Maltezou HC, Vasileiou K, Anastassopoulou C et al. Anaphylactic Reactions to COVID-19 Vaccines: An Updated Assessment Based on Pharmacovigilance Data. Vaccines (Basel) 2023;11. [CrossRef]
- Popiołek I, Piotrowicz-Wójcik K, Porebski G. Hypersensitivity Reactions in Serious Adverse Events Reported for Paracetamol in the EudraVigilance Database, 2007–2018. Pharmacy 2019;7. [CrossRef]
- Jutel M, Agache I, Zemelka-Wiacek M, Akdis M, Chivato T, del Giacco S et al. Nomenclature of allergic diseases and hypersensitivity reactions: Adapted to modern needs: An EAACI position paper. Allergy 2023;78:2851–2874.
- EUDRA. Vigilance database. 2023.https://www.adrreports.eu/ (accessed 6 Dec2023).
- Gao Y, Ding M, Dong X, Zhang J, Kursat Azkur A, Azkur D et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021;76:428–455.
- Kricorian K, Civen R, Equils O. COVID-19 vaccine hesitancy: misinformation and perceptions of vaccine safety. Hum Vaccin Immunother 2022;18. [CrossRef]
- Chu DK, Abrams EM, Golden DBK, Blumenthal KG, Wolfson AR, Stone CA et al. Risk of Second Allergic Reaction to SARS-CoV-2 Vaccines A Systematic Review and Meta-analysis. JAMA Intern Med. 2022;182. [CrossRef]
- Shimabukuro T, Nair N. Allergic Reactions including Anaphylaxis after Receipt of the First Dose of Pfizer-BioNTech COVID-19 Vaccine. JAMA - Journal of the American Medical Association. 2021;325. [CrossRef]
- Shimabukuro TT, Cole M, Su JR. Reports of Anaphylaxis after Receipt of mRNA COVID-19 Vaccines in the US-, 2020-January 18, 2021. JAMA - Journal of the American Medical Association. 2021;325. 14 December. [CrossRef]
- Klein NP, Lewis N, Goddard K, Fireman B, Zerbo O, Hanson KE et al. Surveillance for Adverse Events after COVID-19 mRNA Vaccination. JAMA - Journal of the American Medical Association 2021;326. [CrossRef]
- McNeil MM, Weintraub ES, Duffy J, Sukumaran L, Jacobsen SJ, Klein NP et al. Risk of anaphylaxis after vaccination in children and adults. Journal of Allergy and Clinical Immunology 2016;137. [CrossRef]
- Hourihane JOB, Byrne AM, Blümchen K, Turner PJ, Greenhawt M. Ascertainment Bias in Anaphylaxis Safety Data of COVID-19 Vaccines. Journal of Allergy and Clinical Immunology: In Practice. 2021;9. [CrossRef]
- Lee K, Lee H, Kwon R, Shin YH, Yeo SG, Lee YJ et al. Global burden of vaccine-associated anaphylaxis and their related vaccines, 1967–2023: A comprehensive analysis of the international pharmacovigilance database. Allergy: European Journal of Allergy and Clinical Immunology Published Online First: 2023. [CrossRef]
- McNeil, MM. Vaccine-Associated Anaphylaxis. Curr Treat Options Allergy. 2019;6:297–308.
- Stone SF, Phillips EJ, Wiese MD, Heddle RJ, Brown SGA. Immediate-type hypersensitivity drug reactions. Br J Clin Pharmacol. 2014;78. [CrossRef]
- Macy E, Ho NJ. Multiple drug intolerance syndrome: prevalence, clinical characteristics, and management. Ann Allergy Asthma Immunol 2012;108:88–93.
- Eaddy Norton A, Broyles AD. Drug allergy in children and adults: Is it the double X chromosome? Annals of Allergy, Asthma & Immunology 2019;122:148–155.
- Zucker I, Prendergast BJ. Sex differences in pharmacokinetics predict adverse drug reactions in women. Biol Sex Differ 2020;11. [CrossRef]
- Tharpe, N. Adverse Drug Reactions in Women’s Health Care. J Midwifery Womens Health. 2011;56. [CrossRef]
- Watson S, Caster O, Rochon PA, den Ruijter H. Reported adverse drug reactions in women and men: Aggregated evidence from globally collected individual case reports during half a century. EClinicalMedicine 2019;17. [CrossRef]
- Torres MJ, Blanca M, Fernandez J, Romano A, De Weck A, Aberer W et al. Diagnosis of immediate allergic reactions to beta-lactam antibiotics. Allergy: European Journal of Allergy and Clinical Immunology 2003;58. [CrossRef]
- Pumphrey RSH. Lessons for management of anaphylaxis from a study of fatal reactions. Clinical and Experimental Allergy 2000;30. [CrossRef]
- Blumenthal KG, Peter JG, Trubiano JA, Phillips EJ. Antibiotic allergy. The Lancet. 2019;393. [CrossRef]
- Drug allergy: An updated practice parameter. Annals of Allergy, Asthma and Immunology 2010;105. [CrossRef]
- Zhou L, Dhopeshwarkar N, Blumenthal KG, Goss F, Topaz M, Slight SP et al. Drug allergies documented in electronic health records of a large healthcare system. Allergy: European Journal of Allergy and Clinical Immunology 2016;71. [CrossRef]
- International Rheumatic Fever Study Group. Allergic reactions to long-term benzathine penicillin prophylaxis for rheumatic fever. The Lancet 1991;337. [CrossRef]
- Apter AJ, Kinman JL, Bilker WB, Herlim M, Margolis DJ, Lautenbach E et al. Represcription of penicillin after allergic-like events. Journal of Allergy and Clinical Immunology 2004;113. [CrossRef]
- MacY E, Ho NJ. Multiple drug intolerance syndrome: Prevalence, clinical characteristics, and management. Annals of Allergy, Asthma and Immunology 2012;108. [CrossRef]
- Macy E, Poon K-Y T. Self-reported Antibiotic Allergy Incidence and Prevalence: Age and Sex Effects. American Journal of Medicine 2009;122. [CrossRef]
- Dhopeshwarkar N, Sheikh A, Doan R, Topaz M, Bates DW, Blumenthal KG et al. Drug-Induced Anaphylaxis Documented in Electronic Health Records. Journal of Allergy and Clinical Immunology: In Practice 2019;7. [CrossRef]
- Idsoe O, Guthe T, Willcox RR, de Weck AL. Nature and extent of penicillin side-reactions, with particular reference to fatalities from anaphylactic shock. Bull World Health Organ 1968;38.
- Ribeiro-Vaz I, Marques J, Demoly P, Polónia J, Gomes ER. Drug-induced anaphylaxis: A decade review of reporting to the Portuguese Pharmacovigilance Authority. Eur J Clin Pharmacol 2013;69. [CrossRef]
- Giles A, Foushee J, Lantz E, Gumina G. Sulfonamide Allergies. Pharmacy 2019;7. [CrossRef]
- Dorn JM, Alpern M, McNulty C, Volcheck GW. Sulfonamide Drug Allergy. Curr Allergy Asthma Rep. 2018;18. [CrossRef]
- Carr A, Swanson C, Penny R, Cooper DA. Clinical and laboratory markers of hypersensitivity to trimethoprim-sulfamethoxazole in patients with pneumocystis carinii pneumonia and AIDS. Journal of Infectious Diseases 1993;167. [CrossRef]
- Schönmann C, Brockow K. Adverse reactions during procedures: Hypersensitivity to contrast agents and dyes. Annals of Allergy, Asthma and Immunology. 2020;124. [CrossRef]
- Brockow K, Christiansen C, Kanny G, Clément O, Barbaud A, Bircher A et al. Management of hypersensitivity reactions to iodinated contrast media. Allergy: European Journal of Allergy and Clinical Immunology. 2005;60. [CrossRef]
- Cha MJ, Kang DY, Lee W, Yoon SH, Choi YH, Byun JS et al. Hypersensitivity reactions to iodinated contrast media: A multicenter study of 196 081 patients. Radiology 2019;293. [CrossRef]
- Motosugi U, Ichikawa T, Sano K, Onishi H. Acute adverse reactions to nonionic iodinated contrast media for CT: Prospective randomized evaluation of the effects of dehydration, oral rehydration, and patient risk factors. American Journal of Roentgenology 2016;207. [CrossRef]
- Wang CL, Cohan RH, Ellis JH, Caoili EM, Wang G, Francis IR. Frequency, outcome, and appropriateness of treatment of nonionic iodinated contrast media reactions. American Journal of Roentgenology 2008;191. [CrossRef]
- Bilò MB, Bignardi D. Iodinated contrast media hypersensitivity reactions: is it time to re-evaluate risk factors? Eur Ann Allergy Clin Immunol. 2022;54. [CrossRef]
- Meek IL, van de Laar MAFJ, Vonkeman HE. Non-steroidal anti-inflammatory drugs: An overview of cardiovascular risks. Pharmaceuticals. 2010;3. [CrossRef]
- Blanca-Lopez N, Soriano V, Garcia-Martin E, Canto G, Blanca M. Nsaid-induced reactions: Classification, prevalence, impact, and management strategies. J Asthma Allergy. 2019;12. [CrossRef]
- Kasper L, Sladek K, Duplaga M, Bochenek G, Liebhart J, Gladysz U et al. Prevalence of asthma with aspirin hypersensitivity in the adult population of Poland. Allergy: European Journal of Allergy and Clinical Immunology 2003;58. [CrossRef]
- Zembowicz A, Mastalerz L, Setkowicz M, Radziszewski W, Szczeklik A. Safety of Cyclooxygenase 2 Inhibitors and Increased Leukotriene Synthesis in Chronic Idiopathic Urticaria with Sensitivity to Nonsteroidal Anti-inflammatory Drugs. Arch Dermatol 2003;139. [CrossRef]
- McDonald JR, Mathison DA, Stevenson DD. Aspirin intolerance in asthma. Detection by oral challenge. J Allergy Clin Immunol 1972;50. [CrossRef]
- Jenkins C, Costello J, Hodge L. Systematic review of prevalence of aspirin induced asthma and its implications for clinical practice. Br Med J. 2004;328. [CrossRef]
- Caimmi S, Caimmi D, Bousquet PJ, Demoly P. How can we better classify NSAID hypersensitivity reactions? - Validation from a large database. Int Arch Allergy Immunol 2012;159. [CrossRef]
- Hernandez-Salazar A, de Leon-Rosales SP, Rangel-Frausto S, Criollo E, Archer-Dubon C, Orozco-Topete R. Epidemiology of Adverse Cutaneous Drug Reactions. A Prospective Study in Hospitalized Patients. Arch Med Res 2006;37. [CrossRef]
- Doña I, Blanca-López N, Torres MJ, García-Campos J, García-Núñez I, Gómez F et al. Drug hypersensitivity reactions: Response patterns, drug involved, and temporal variations in a large series of patients. J Investig Allergol Clin Immunol 2012;22.
- Harboe T, Guttormsen AB, Aarebrot S, Dybendal T, Irgens Å, Florvaag E. Suspected allergy to local anaesthetics: Follow-up in 135 cases. Acta Anaesthesiol Scand 2010;54. [CrossRef]
- Schatz M, Fung DL. Anaphylactic and anaphylactoid reactions due to anesthetic agents. Clin Rev Allergy 1986;4. [CrossRef]
- Kvisselgaard AD, Mosbech HF, Fransson S, Garvey LH. Risk of Immediate-Type Allergy to Local Anesthetics Is Overestimated—Results from 5 Years of Provocation Testing in a Danish Allergy Clinic. Journal of Allergy and Clinical Immunology: In Practice 2018;6. [CrossRef]
- Saff, RR. Immediate Local Anesthetic Reactions: Too Quick to Point the Finger? Journal of Allergy and Clinical Immunology: In Practice. 2018;6. [CrossRef]
- Kvisselgaard AD, Krøigaard M, Mosbech HF, Garvey LH. No cases of perioperative allergy to local anaesthetics in the Danish Anaesthesia Allergy Centre. Acta Anaesthesiol Scand 2017;61. [CrossRef]
- Zuo J, Gong R, Liu X, Zhao J. Risk of true allergy to local anesthetics: 10-year experience from an anesthesia allergy clinic in china. Ther Clin Risk Manag 2020;16. [CrossRef]
Figure 1.
Number of cases according to year of occurrence in each age and sex group.
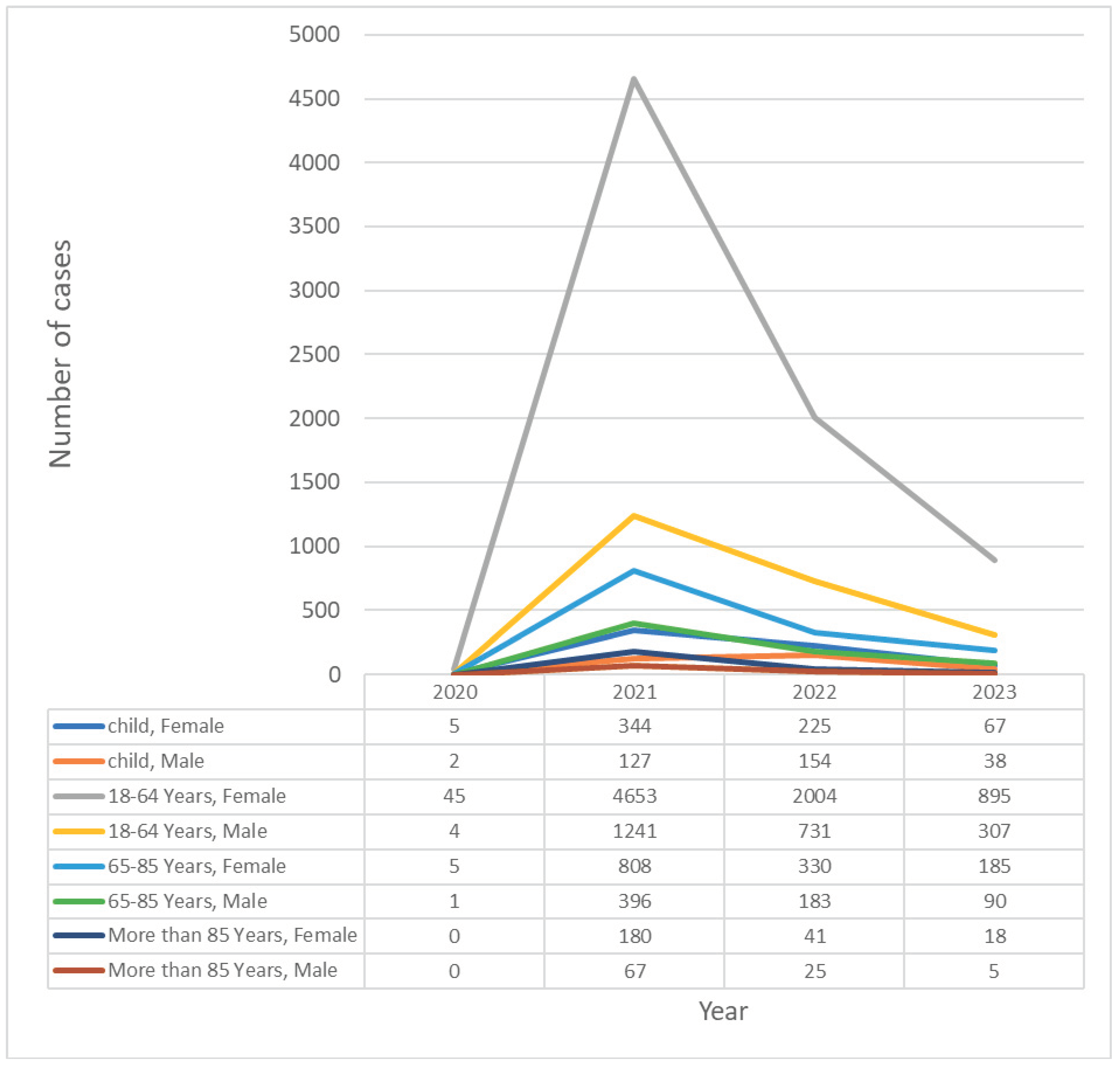
Figure 2.
Proportion of type of allergic reaction post-COVID-19 vaccination.
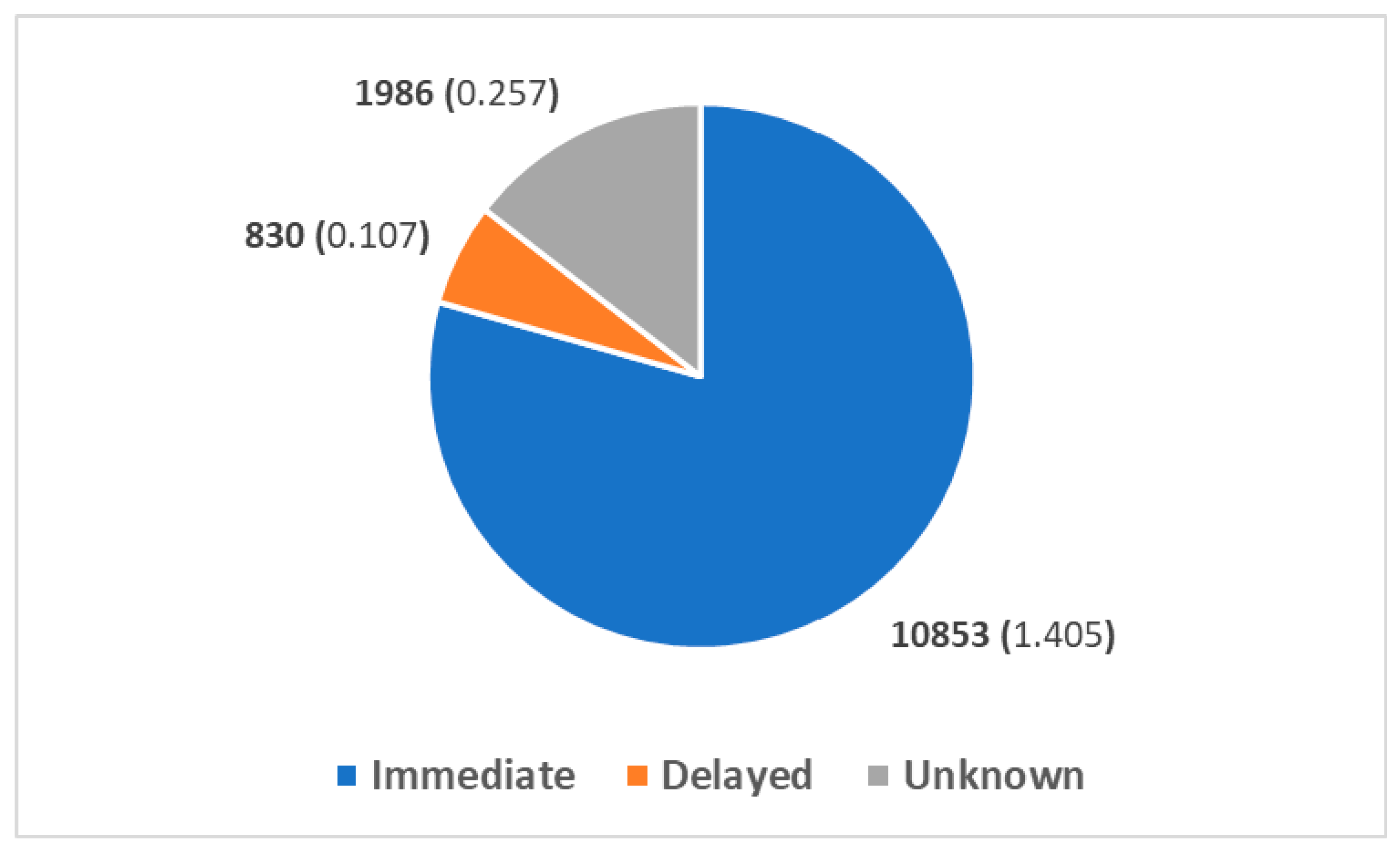
Figure 3.
Examples of allergic reactions post-COVID-19 vaccination.
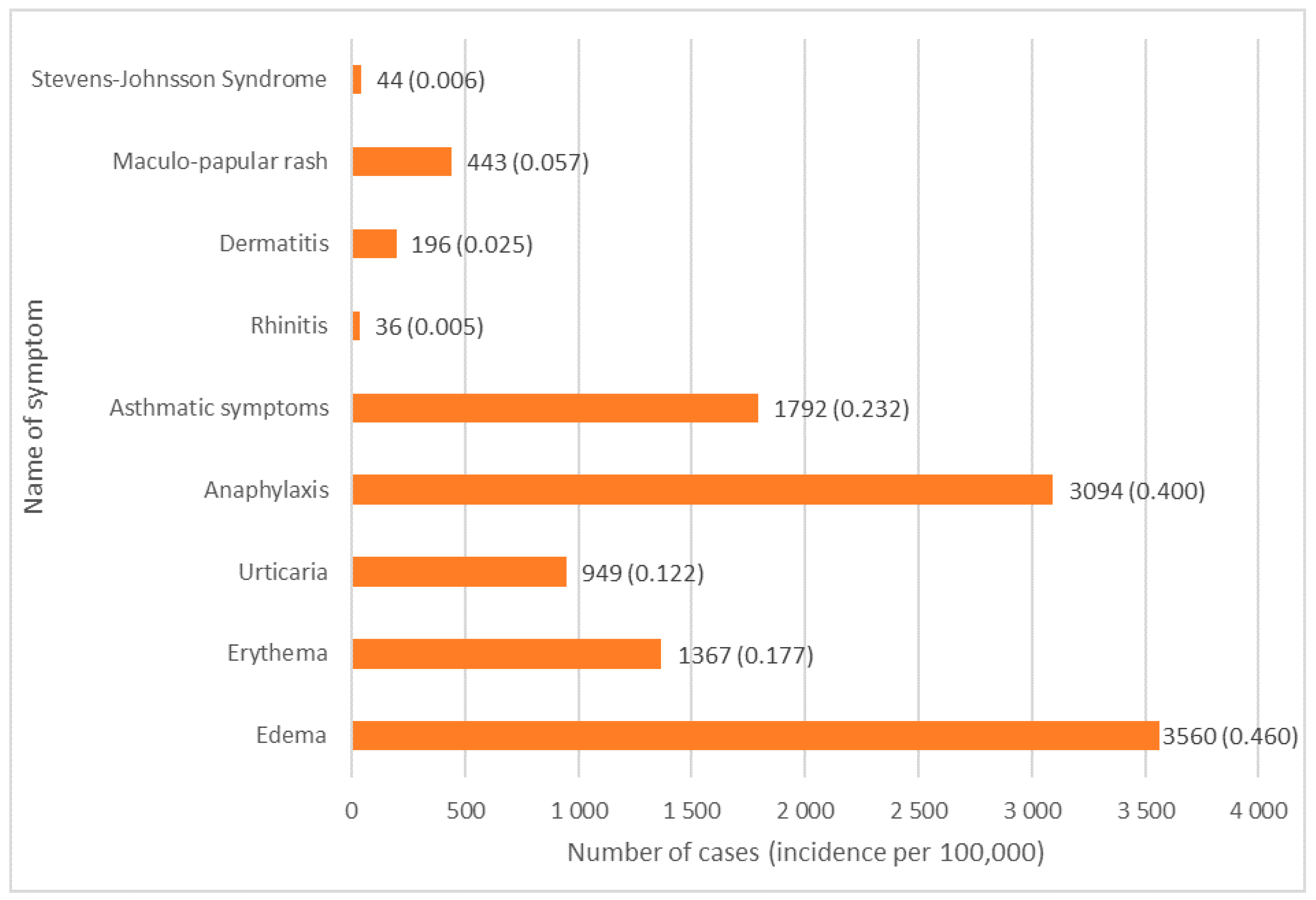

Table 1.
Investigated vaccines by substance name as they appear in the EudraVigilance database [34].
Table 1.
Investigated vaccines by substance name as they appear in the EudraVigilance database [34].
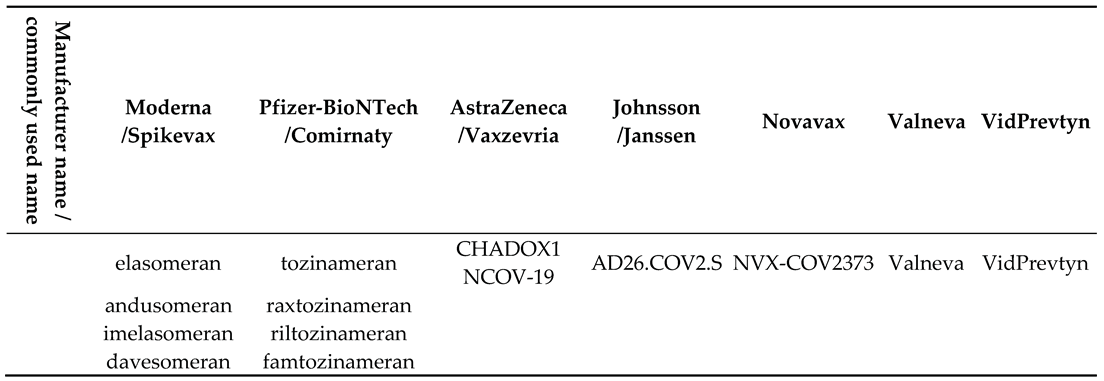 |
Table 2.
Comparison of number of allergic reactions according to vaccine, age and sex. Due to reporting discrepancies, general population cases might not be the sum of the subgroups, such as Female and Male, as it is possible that some patients’ characteristics were not specified in some reports. p value was calculated using chi square. All comparisons in vaccines and age groups were statistically significant due to large sample sizes.
Table 2.
Comparison of number of allergic reactions according to vaccine, age and sex. Due to reporting discrepancies, general population cases might not be the sum of the subgroups, such as Female and Male, as it is possible that some patients’ characteristics were not specified in some reports. p value was calculated using chi square. All comparisons in vaccines and age groups were statistically significant due to large sample sizes.
| Number of cases | Spikevax | Comirnaty | Vaxzevria | Janssen | Novavax | Valneva | VidPrevtyn Beta | P value |
|---|---|---|---|---|---|---|---|---|
| General population | 2,857 | 8,734 | 1,717 | 340 | 18 | 2 | 1 | <0.001 |
| Female | 2,052 | 6,363 | 1,216 | 157 | 15 | 1 | 1 | <0.001 |
| Male | 753 | 2,064 | 409 | 141 | 3 | 1 | 0 | |
| Female, child | 89 | 479 | 65 | 6 | 1 | 0 | 1 | <0.001 |
| Male, child | 61 | 236 | 14 | 9 | 1 | 0 | 0 | |
| Male, Adult 18–64 years old | 572 | 1322 | 263 | 123 | 2 | 1 | 0 | <0.001 |
| Female, Adult 18–64 years old | 1,647 | 4,870 | 928 | 137 | 14 | 1 | 0 | |
| Female, elderly>85 | 27 | 202 | 10 | 0 | 0 | 0 | 0 | <0.001 |
| Male, elderly>85 | 14 | 78 | 3 | 2 | 0 | 0 | 0 | |
| Female Adult 65–85 years old | 289 | 812 | 213 | 14 | 0 | 0 | 0 | <0.001 |
| Male Adult 65–85 years old | 106 | 428 | 129 | 7 | 0 | 0 | 0 | |
| Incidence per 100,000 | Spikevax | Comirnaty | Vaxzevria | Janssen | Novavax | Valneva | VidPrevtyn Beta | |
| General population | 2,162 | 1,538 | 88,614 | 2,115 | 7,989 | 3,07 | 13,291 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



