
Submitted:
28 March 2024
Posted:
09 April 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Throughout the COVID-19 pandemic, masks have been promoted as an important tool for reducing SARS-CoV-2 transmission. However, even though masks are plausible experimental interventions, their mechanistic effectiveness has not been validated by randomized clinical trials (RCTs), with reduction risks of just 1.1-fold (11%) or less. Several meta-analyses have suggested that masks effectively reduce viral transmission, but all of them rely heavily or exclusively on observational data. Indeed, there is a strong inverse correlation between the effectiveness of masks and the number of RCTs included in the meta-analysis. RCTs on alternative therapies often show similar low levels of effectiveness. Thus, masks can be compared with potential new drugs or therapies that failed clinical trials despite showing mechanistic evidence.
Keywords:
COVID-19
; evidence-based medicine
; randomized clinical trials
; masks
; alternative therapies
; condoms
Introduction
In spite of significant progress in biomedical sciences, many health concerns remain unresolved. To ensure the safety and efficacy of new drugs and therapies, researchers have developed efficient, though not bulletproof, methods. Randomized controlled trials (RCTs) are the most rigorous and reliable way to determine the efficacy of new treatments or experimental drugs and are therefore considered the gold standard of clinical trials [1,2]. Drug licensing authorities rarely approve a potential therapeutic molecule without a properly conducted RCT [3,4]. Currently, the FDA (US Food and Drug Administration) and EMA (European Medicines Agency) consider observational studies reliable sources of evidence only when their effects are sufficiently large or dramatic [5].
1. The Mask Issue
1.1. RCTs on Masks
The effectiveness of face masks in curbing viral transmission has been tested in several randomized control trials before and after the onset of the COVID-19 pandemic. Two large RCTs on COVID - the DANMASK [6] and the Bangladeshi [7] trials, have been conducted and published. The DANMASK RCT, carried out between April and May 2020 in Denmark, involved the largest set of participants (almost 5000) in a mask RCT up to that time. The trial results showed a non-significant reduction in the odds ratio of the masked group relative to the non-masked control arm (0.82 [ 0.54 - 1.23]; p = 0.33). The study conclusion was that “the recommendation to wear surgical masks to supplement other public health measures did not reduce the SARS-CoV-2 infection rate among wearers by more than 50% in a community with modest infection rates, some degree of social distancing, and uncommon general mask use.” The reference to a 50% reduction was because the trial was powered to find at least this degree of risk reduction. Despite the fact that the RCT involved a large number of participants and was well-conducted as possible by a pro-mask advocate principal author [8] the mainstream medical-scientific community did not spare efforts to diminish the study impact on the ineffectiveness of masks [9,10,11,12].
The cluster RCT with the largest number of participants in this type of trial (300,000) was carried out in 600 villages in a Bangladesh rural zone. Both cloth and surgical masks were tested, the former showed no reduction in COVID transmission while surgical masks provided a 9.5% reduction in symptomatic SARS-CoV-2 seroprevalence and an 11.6% reduction in the prevalence of COVID-like symptoms (both values significant at the 5% level). In total, there were 1086 cases of symptomatic seropositive infection in the control arm and 1106 in the treatment arm. This small reduction was hailed by some in the mainstream medical-scientific community as a definitive proof of masks’ effectiveness [13,14,15]. However, even this small effect is disputed, since a reanalysis of this RCT found that unblinded staff may have contributed to significant bias in how they approached the treatment and control groups [16]. A surprising finding in this study was that masking effectiveness differed considerably depending on the age of the wearer. While the 50-59 and ≥ 60 years old groups displayed significant reductions in COVID-19 seroprevalence (0.772 [0.595-0.949] and 0.647 [0.448-0.845], respectively), the younger age groups, (< 40 and 40-49 years old), did not show any significant reduction in seroprevalence (0.967 [0.834-1.100] and 1.009 [0.817-1.200], respectively). The authors of the paper provided some hypotheses to explain this discrepancy, but none have been tested. More recently, a randomized trial comparing the effect of medical masks and N95 respirators to prevent COVID-19 in 29 health care facilities in Canada, Israel, Pakistan, and Egypt has been published [17]. No significant difference between the N95 and medical masks arms in the intention to treat analysis was observed. RT-PCR–confirmed COVID-19 occurred in 52 of 497 (10.46%) participants in the medical mask group versus 47 of 507 (9.27%) in the N95 respirator group. The pooled hazard ratio was 1.14 [0.77 - 1.69]). This was the largest RCT on N95 respirators ever performed.
1.2. The Cochrane Review on Mask RCTs
All randomized trials conducted before the COVID pandemic have reported null to low effect of masks and no difference between masks and respirators. The best RCTs of this kind were systematically reviewed by Cochrane researchers. The fifth and most recent review of this kind was published in January 2023 [18]. Cochrane is an international network whose mission is to analyze and summarize the best evidence from biomedical research providing authoritative and reliable information, unconstrained by commercial and financial interests, being the leading global advocate for evidence-informed health and care (https://www.cochrane.org/). Cochrane reviews are internationally recognized as the benchmark for high-quality information about the effectiveness of health care. Over 7,500 reviews have hitherto been published, they are freely available from the Cochrane library (http://www.cochranelibrary.com/). In the 2023 review on masks and other interventions the authors analyzed 13 RCTs on medical or surgical masks, of which 11 were in the community and 2 in healthcare workers. In addition, five studies on N95/P2 respirators (4 in hospital or outpatient settings and one in the community) were also evaluated. All of these trials studied the spread of influenza or influenza-like illnesses (ILI). Medical or surgical masks were compared to no-masks and respirators were compared to medical or surgical masks. The most reliable outcomes were from studies that used laboratory-confirmed viral illness, which provided a “moderate certainty of evidence”. These studies showed no significant risk reduction by medical/surgical mask or P2/N95 wearers. The total number of participants in the RCTs on medical/surgical masks versus no mask was 290,000, with approximately half this number in each arm. The pooled risk ratio (RR) for laboratory-confirmed influenza was 1.01 [0.72, 1.42], while the pooled RR for influenza-like illness was 0.95 [0.84, 1.09]. A pooled RR of 1.10 [0.90-1.34] was observed when N95 respirators were compared with medical/surgical masks in laboratory-confirmed influenza, a result that favors surgical/medical masks, though not statistically significant. Interestingly, the two other viral illness outcomes – clinical respiratory illness and influenza-like illness, which provided less certainty of evidence, also showed statistically non-significant results, but with pooled risk ratios favoring N95 masks (0.70 [0.45, 1.10] and 0.82 [0.66, 1.03], respectively). In general, there is an inverse correlation between mask study quality (or quality of evidence) and mask effectiveness, i.e., the better the study or the quality of evidence, the lower the effectiveness of masks. This becomes evident while comparing more rigorous and less rigorous studies (randomized vs. observational for example) or different endpoints – clinical respiratory and influenza-like illnesses (less reliable endpoint) vs. laboratory-confirmed influenza (more reliable endpoint) in a single study as in the case of N95 vs. surgical/medical masks mentioned above. The Cochrane review on mask RCTs [18] concluded that “The pooled results of RCTs did not show a clear reduction in respiratory viral infection with the use of medical/surgical masks. There were no clear differences between the use of medical/surgical masks compared with N95/P2 respirators in healthcare workers when used in routine care to reduce respiratory viral infection”. There are no qualitative differences between the current and previous Cochrane review [19]. If anything, the effectiveness of masks decreased with the addition of three recent randomized trials to the 2023 review studies [6,7,20], two of them on SARS-CoV-2 transmission. It should be noted that all but one N95 trial, including the most recent international multicenter RCT [17] were conducted with healthcare workers who had been trained on how to fit and wear respirators. Considering the failure of these trials to demonstrate a reduction in viral transmission compared to surgical/medical masks, it makes one wonder if the recommendations for wearing respirators and the calls for their distribution to the general public (https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/types-of-masks.html, https://www.ama-assn.org/delivering-care/public-health/what-doctors-wish-patients-knew-about-wearing-n95-masks, https://edition.cnn.com/2022/01/19/politics/n95-masks-biden-administration-covid-19/index.html), who are not trained to wear these type of masks, will be of any benefit.
1.3. Meta-Analyses that Support Masking
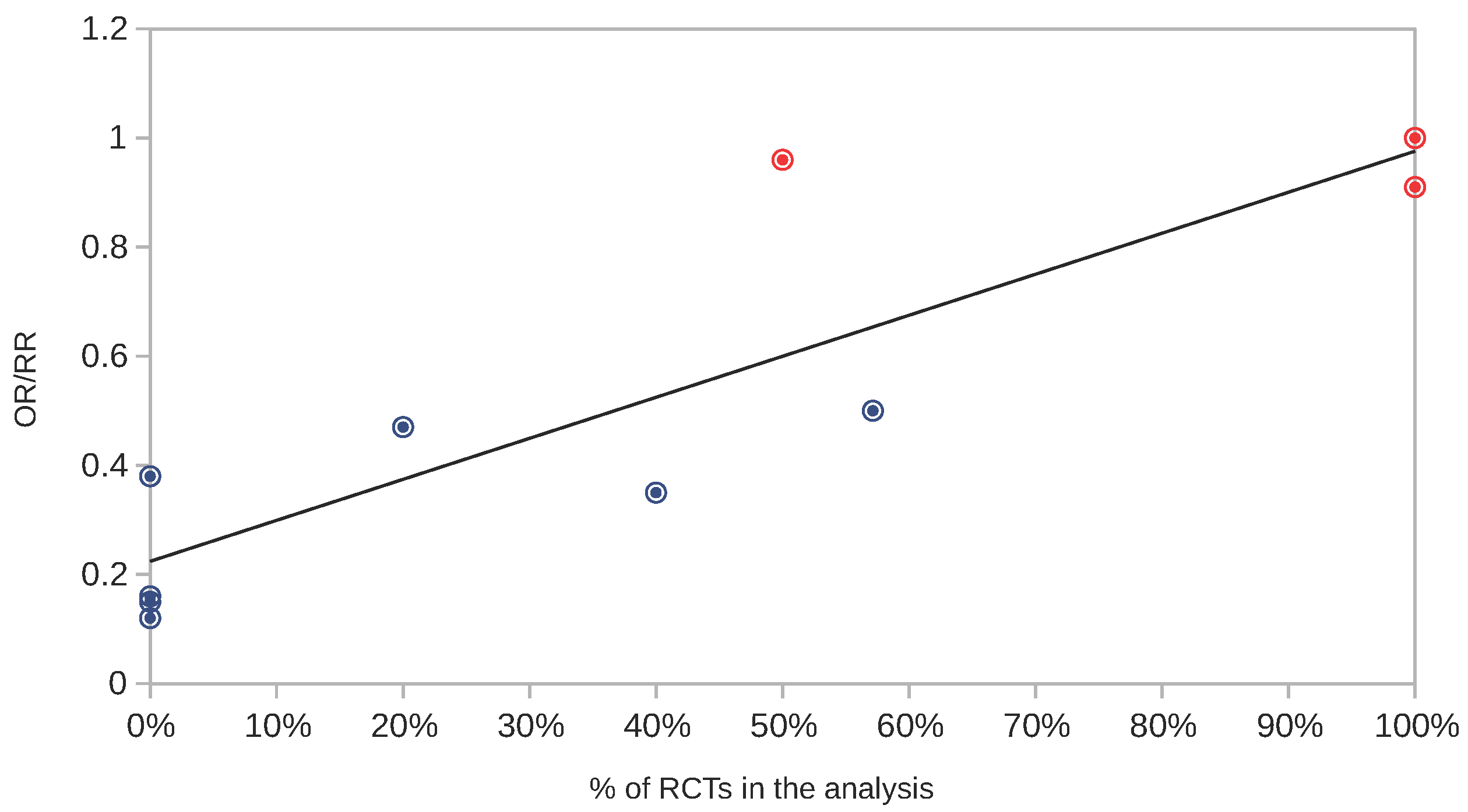
Several reviews and meta-analyses have evaluated the data from mask studies since the beginning of the COVID pandemic and concluded that mask wearing may be associated with a significant reduction in viral transmission [21,22,23,24,25,26,27,28]. We will look at two of these reviews in more detail. A meta-analysis published at the same time as the Cochrane review - December 2020 - examined 12 randomized trials and 21 observational studies on the effectiveness of masks in preventing the transmission of respiratory viruses [29]. According to this review, face masks reduced the risk of primary respiratory infections by 6 - 15%. The authors justified the inclusion of observational studies because "the conclusions of RCTs and observational studies differ widely and both are prone to significant bias". However, since randomized trials are designed to minimize bias and confounders, their inherent bias is considerably lower than that of observational studies [2]. Additionally, the risk reduction calculated in this meta-analysis (6-15%) for mask wearers is too low to justify a mask recommendation, let alone mandates (see section below “on masks and condoms” for a comparison of mask and condom effectiveness). An exception to the pro-masking chorus of meta-analyses that reviewed observational studies is Wang et al. who, by analyzing 5 randomized and 10 observational studies estimated a non-significant pooled odds ratio of 0.96 [0.8–1.15] for surgical mask effectiveness against acute respiratory illness among individuals in non-healthcare settings [30], concluding that surgical mask wearing among individuals in the community is not significantly associated with a reduction in acute respiratory illnesses. Meta-analyses that concluded that masks do have a substantial impact on viral transmission relied only or almost exclusively on observational studies. This is exactly what the very influential paper by Chu et al. has done [21]. The pooled effect of 29 observational trials (26 in healthcare settings and 3 in the community) and not a single RCT reached a significant adjusted odds ratio of 0.15 [0.07 – 0.34]. There were other recent meta-analyses on masks that included only or mostly observational studies [22,24,25,26,27,28]. Figure 1 shows the correlation plot between the proportion of RCTs in ten mask meta-analyses and their respective pooled odds ratio or risk reduction ratio. The lower the proportion of RCTs, the greater the effect of masks (lower OR or RR). In fact, there is a strong association between these two variables (Pearson correlation coefficient = 0.88). It should be noted that two systematic reviews [18,23] that included only RCTs in their analysis and the meta-analysis conducted by Wang et al 2020 that contained both RCTs and observational studies [30] found no statistically significant effects.
Additionally, real-world (ecological) observations greatly contradict the overoptimistic assessments made by meta-analyses based on observational studies [21,22,23,24,25,26,27,28], whose combined OR was 0.28. To illustrate this point consider Spain and Italy, which had, respectively, 95% and 91% of their population reporting always wearing a mask while leaving home, the highest levels of mask compliance during the COVID-19 second wave (October 2020 - March 2021) in Europe [31].As of that period, Italy and Spain ranked 20th and 18th in terms of COVID-19 cases among 35 European countries. If the actual OR of masks had been 0.23, the Spanish and Italian population should have been among the countries with the lowest COVID-19 infection rates. While western countries saw a rise in COVID-19 cases, Japan, known for high mask adherence, saw far fewer as early in the pandemic [32,33]. However, between January 1st and December 31st of 2022 Japan underwent a 15-fold increase in COVID-19 cases (from 1.73 million to 29.23 million cases), even though mask compliance was still above 85% [34]. While these uncontrolled observations do not prove that masks do not contribute to viral transmission, they do indicate that most observational studies reported unrealistically high effectiveness levels.
1.4. Randomised Trials with Positive Results of Masks and Their Statistical Significance
Two RCTs showed statistically significant results in favor of masks. The Bangladeshi study, which showed a small positive effect of surgical masks on SARS-CoV-2 transmission, did not provide exact p values, but stated that the overall effect of surgical masks (11% RR) was statistically significant at the 5% level. Among the 9 RCTs reviewed by [18], only one showed a significant level of confidence (p = 0.0238) in one of the analyzed interventions - medical masks were found to reduce clinical respiratory illness (but not ILI or lab-confirmed viral illness) [35]. Nonetheless, it is worth reminding that a p value just below 0.05 indicates that there is a 26% chance that the result is a false positive [36].
1.5. On Masks and Condoms
In both popular and scientific literature, masks are frequently referred to as physical barriers against respiratory viruses, much like condoms act as physical barriers against sexually transmitted diseases ([37,38,39];https://time.com/6232830/why-masks-still-matter-covid-19/). However, despite the widespread belief in this analogy, condoms and masks are not comparable, mainly because these two protection tools provide completely different levels of protection. In the cRCT with the most positive results [7], masks significantly reduced the prevalence of COVID-like symptoms by 11.6% (a 1.13 risk reduction). On the other hand, a Cochrane review on condom efficacy concluded that condoms are effective to a degree of 80%, i.e., a 5-fold risk reduction [40]. Condom effectiveness was estimated from observational studies, in which information about individuals inadvertently exposed to HIV while using or not using condoms was collected. As a consequence, obtaining clear evidence of effectiveness, that can be provided by randomized trials, is not possible due to ethical considerations (especially in cases of incurable diseases). As an appropriate proxy for STD (sexually-transmitted diseases) transmission, randomized trials have been conducted on condoms as a means of preventing pregnancy. According to the pooled estimate of a Cochrane review [41] on the effectiveness of non-latex versus latex male condoms for contraception, latex condoms were 97.8% effective against pregnancy, a failure rate of 2.2%, in 11 separate studies. Since the non-latex condom test group was always compared to a latex condom control group, these randomized trials did not pose any ethical concerns. Participants in these trials reported incidents of condom breakage and slippage, which are considered bona fide indicators of condom failure [42]. In contrast to mask trials against respiratory viruses, which use definitive endpoints, such as seroprevalence or viral nucleic acid detection, this alternative condom efficacy endpoint is less stringent, since not all broken or slipped condoms cause pregnancy. Therefore, the overall effectiveness of condoms in preventing pregnancy is likely to be higher than 98%, further exacerbating the difference between masks and condoms. In light of the overwhelming difference between the effectiveness of masks and condoms, which, in the case of masks, results in very low risk reduction (11.6% or 1.13-fold according to the most favorable cRCT [7], the argument that masks are comparable to condoms is disproportionate given that condoms result in a risk reduction > 50-fold (>98%).
1.6. Masking as an “Alternative Therapy”
As a general rule, the better the quality of the study (e.g., observational vs. randomised trials), the lower the reported efficacy of masks. This rule also applies to clinical trials of "alternative therapies." One example is homeopathy, a widely known and controversial alternative therapy that is used by thousands of doctors around the world and that had a market size valued at US$ 6.2 billion in 2020 (https://www.precedenceresearch.com/homeopathic-products-market). Homeopathy is based on two principles: (1) “simila similibus curentur” – “like cures like”, which holds that substances that cause similar symptoms in healthy individuals can cure diseases, and (2) the law of infinitesimals, which states that a drug’s curative power can be increased by succussion, a sequential process of ultra dilutions. Consequently, the second premise of the homeopathic canon violates fundamental principles of chemistry and pharmacology, rendering it highly unlikely to be valid. The field of homeopathy has, however, seen hundreds of clinical trials over the years. Shang et al. examined 110 homeopathy randomized or quasi-randomized control trials and 110 matched conventional medicine trials [43]. They found out an average odds ratio of 0.88 [0.65–1.19] in the eight higher quality homeopathy trials, while in their conventional counterparts the odds ratio was 0.58 [0.39–0.85]. When looking at the lower quality trials the odds ratio of both homeopathic and conventional treatments improved (became smaller), but more predictably so in the former. For instance, when not double-blind were confronted with double-blind studies, the reduction in OR were higher and significant for homeopathy (0.44 [0.22–0.87]) but not so for conventional drugs (0.63 [0.36–1.11]). It is evident thus that there is an inverse correlation between study quality and positive effects in placebo-controlled trials of homeopathy. Clinical trials showing positive results for homeopathy also had a small quantitative impact and a wide confidence interval. Why did some RCTs show a positive effect for homeopathic interventions? Those might be the result of a combination of methodological deficiencies and biased reporting. A similar pattern emerges when mask trials are examined, with observational studies showing better outcomes for masks than higher quality RCTs and cluster-RCTs, as well as when comparing laboratory-confirmed viral infection with the less well-defined clinical illnesses. Even when supported by randomized trials with statistical significance, small effects in conventional or alternative therapies are dangerously susceptible to biases. They should not be taken as evidence of causality, and certainly should not shape public health policy. In contrast, effective interventions such as condoms for the prevention of pregnancy and STDs, and vaccines and antibiotics for the prevention and treatment of infectious diseases, usually provide robust conclusive results. Take, for example, two Cochrane meta-analyses that examined the use of antibiotics. One of them analysed the effectiveness of oral or parenteral treatments with co-trimoxazole, penicillin and ampicillin for severe pneumonia in children, where the success rates were of 80-90% [44]. The other meta-analysis reviewed the use of doxycycline, tetracycline or rifampicin against scrub typhus with success rates of 95-100% [45]. Many other randomized controlled trials of antibiotics have been hitherto performed, with similar success rates. In contrast, homeopathic treatments have no success rates even remotely similar to antibiotics. Even though not all antibiotics are effective against all bacterial infections, there is no doubt that they have revolutionized medicine by providing fast and effective chemotherapy against deadly bacteria.
1.7. Masking Priors
It is true that, from a Bayesian perspective, masking should be viewed differently from homeopathy. Since homeopathy was built on an unlikely theoretical framework, particularly the infinitesimal rule of ultra-dilutions, homeopathic drugs have a very low prior probability. Conversely, intuition, common sense, and most importantly, laboratory experiments provide masks with a relatively high prior probability. It is undeniable that masks are capable of filtering particulates, even if the actual filtration effectiveness of different mask types varies widely across studies (in large part due to variation in experimental design and particle sizes analysed) (https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/masking-science-sars-cov2.html). Surgical or cloth masks, which are used by the vast majority of people, provide only 10-12% filtration efficiency. Respirators (P2/N95) are more efficient, but none of them achieve more than 60% filtration, even under optimized laboratory conditions [46]. In addition, a small fractional leak area of 2% can severely reduce mask filtration efficiency by 75%, especially for particles smaller than 5 mm in diameter [47]. Even before 2020, several credible randomized controlled trials demonstrated that masks do not perform as well in practice as in the laboratory [18]. By utilizing meta-analyses of randomized trials as a prior instead of mechanistic evidence, the prior probability of masks comes close to zero, not so different from other alternative therapies. In other words, masks are plausible interventions based on laboratory experiments, but their continued failure in clinical trials to reduce viral infections in healthcare settings and in the community undermines their usefulness, making them similarly ineffective as alternative therapies. In this regard, the main differences between masking and classical alternative therapies is that the former has been widely supported by the mainstream medical and academic establishment and that alternative therapies have never been mandated by law.
1.8. Mask in the Lab – Filtering Efficacy as a Secondary Outcome
The ability of masks and respirators to filter viral particles in laboratory conditions has been examined in a great number of in vitro mechanistic studies. Many of these studies were published during the COVID pandemic, after masks were mandated worldwide (see [46,47,48,49,50] for a few examples). In addition, pictures and remarks taken from or based on such studies have been widely used to promote masking in the public. The enthusiasm on the apparent efficacy of mask filtration resulted in calls for disregarding RCTs (Muller 2021) in favor of what some call EBM+ (evidence based medicine+) where the ‘+’ refers to the addition of non-clinical evidence such as in vitro experimentation (mechanistic evidence) [51]. Their argument goes as follows: “the complex nature of the pandemic, characterized by multiple variables interacting dynamically with a high degree of uncertainty, urgency and threat to public health, requires the use of mechanistic evidence once randomized trials are difficult or impossible to conduct”. There is no evidence to support the assertion that randomized trials are difficult or impossible to carry out. Mask RCTs can be conducted without any hindrance from an operational perspective, as they have been conducted in the past, even during epidemics. On the allegation that conducting mask RCTs during a pandemic is unethical, we should remember that all previous randomized trials have consistently shown no effect of masks in reducing viral transmission, thus performing new RCTs would not involve any ethical concerns, as the control group would most certainly not be at risk. Additionally, the preoccupation with the severity and uncertainty of the pandemic should reinforce, rather than undermine, the need for good and reliable data. This is not the time to disregard the best tool available to the biomedical sciences, the RCT, to distinguish between working therapies and bogus or ineffective ones. The conflict between low quality data, supported by observation and common sense, and high quality data permeates the medical literature as shown by Fanaroff et al. who describe 31 heart-related conditions in which common sense or observational evidence predicted positive outcomes, only to be contradicted by robust clinical trials [2].
Whether a specific therapy or intervention should be implemented cannot be determined solely by mechanistic evidence. The best that laboratory results can do is provide the theoretical foundation for a successful clinical trial. Furthermore, the biomedical sciences is currently experiencing a reproducibility crisis, especially in pre-clinical research, where high-impact journals publish studies that yield false positives that could not be replicated [52,53]. Therefore, it is unwise to use pre-clinical research that is prone to false-positive results to justify mask use. The fact that a particular drug or therapy is successful in the laboratory does not necessarily indicate that it will be successful in the clinical trial. Many promising drugs with state-of-the-art mechanistic explanations have been withdrawn after failing randomized trials. In reality, less than 14% of pre-clinical potential drugs make it to the market [54]. Different therapeutic groups have varying success rates. Oncology-related drugs, that account for the majority of clinical trials, have a success rate, i.e. the percentage of drugs that are eventually approved by the regulatory authority, of 3.4%. In contrast, biologics such as vaccines are approved at a rate of 33.4% [54]. Some particular therapeutic fields are plagued by an overabundance of failures. Until 2008, there were over 200 failed Alzheimer’s drugs and candidates [55] and their number keeps increasing. The same is true for other therapeutic areas such as obesity [56] and most other medical fields [54]. All of these potential drugs passed pre-clinical trials with flying colors, but failed at one or other stage of the clinical trials. Similarly, mask testing under laboratory conditions may have shown filtration efficacy (although the degree of efficacy is unclear), but clinical trials (RCTs and cRCTs) have repeatedly demonstrated that they are not effective in reducing viral transmission in the community and among healthcare workers. Real-world situations are often considerably more complex than mechanistic experiments conducted under controlled conditions in laboratories, especially since we do not fully understand how respiratory virus transmission works.
Throughout the COVID-19 pandemic masks have been promoted as an important tool to reduce or even halt the spread of SARS-CoV-2 in the population. Many governments mandated the use of masks in public by law. However, even before the pandemic, the best evidence available - randomized trials, were already showing that masks are likely ineffective in curbing respiratory viral transmission. Additional high-quality data produced throughout the pandemic reinforced that conclusion. In spite of that, with a few exceptions [57], most critical reviews or opinion articles have never questioned the effectiveness of masks in the COVID-19 pandemic. While intuition and laboratory experiments suggest that masks are plausible interventions, their continued failure in randomized clinical trials undermines their effectiveness.
References
- Ernst, E.; Smith, K. Research Fundamentals. In More Harm than Good? Springer International Publishing: Cham, 2018; pp. 25–60. [Google Scholar] [CrossRef]
- Fanaroff, A.C.; Califf, R.M.; Harrington, R.A.; Granger, C.B.; McMurray, J.J.; Patel, M.R.; Bhatt, D.L.; Windecker, S.; Hernandez, A.F.; Gibson, C.M.; Alexander, J.H.; Lopes, R.D. Randomized Trials Versus Common Sense and Clinical Observation. Journal of the American College of Cardiology 2020, 76, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Montori, V.; Vist, G.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Djulbegovic, B.; Atkins, D.; Falck-Ytter, Y.; Williams, J.W.; Meerpohl, J.; Norris, S.L.; Akl, E.A.; Schünemann, H.J. GRADE guidelines: 5. Rating the quality of evidence—publication bias. Journal of Clinical Epidemiology 2011, 64, 1277–1282. [Google Scholar] [CrossRef] [PubMed]
- Razavi, M.; Glasziou, P.; Klocksieben, F.A.; Ioannidis, J.P.A.; Chalmers, I.; Djulbegovic, B. US Food and Drug Administration Approvals of Drugs and Devices Based on Nonrandomized Clinical Trials: A Systematic Review and Meta-analysis. JAMA Netw Open 2019, 2, e1911111. [Google Scholar] [CrossRef] [PubMed]
- Djulbegovic, B.; Glasziou, P.; Klocksieben, F.A.; Reljic, T.; VanDenBergh, M.; Mhaskar, R.; Ioannidis, J.P.; Chalmers, I. Larger effect sizes in nonrandomized studies are associated with higher rates of EMA licensing approval. Journal of Clinical Epidemiology 2018, 98, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Bundgaard, H.; Bundgaard, J.S.; Raaschou-Pedersen, D.E.T.; von Buchwald, C.; Todsen, T.; Norsk, J.B.; Pries-Heje, M.M.; Vissing, C.R.; Nielsen, P.B.; Winsløw, U.C. Effectiveness of adding a mask recommendation to other public health measures to prevent SARS-CoV-2 infection in Danish mask wearers: a randomized controlled trial. Annals of internal medicine 2021, 174, 335–343, Publisher: American College of Physicians. [Google Scholar] [CrossRef] [PubMed]
- Abaluck, J.; Kwong, L.H.; Styczynski, A.; Haque, A.; Kabir, M.A.; Bates-Jefferys, E.; Crawford, E.; Benjamin-Chung, J.; Raihan, S.; Rahman, S. Impact of community masking on COVID-19: A cluster-randomized trial in Bangladesh. Science 2021. p. eabi9069. Publisher: American Association for the Advancement of Science. [Google Scholar]
- Unherd. danish-mask-study-professor-protective-effect-may-be-small-but-masks-are-worthwhile, 2020.
- Thornley, S.; Jackson, M.D.; Sundborn, G. Danish mask study: masks, media, fact checkers, and the interpretation of scientific evidence. BMJ 2020. p. m4919. Publisher: BMJ. [Google Scholar] [CrossRef]
- O’Grady, C. ‘It’s misinformation at worst.’ Weak health studies can do more harm than good, scientists say, 2021.
- Head, M.; Gill, J. expert reaction to paper using an RCT to assess mask use as a public health measure to help control SARS-CoV-2 spread (DANMASK-19), 2020.
- Ontario, P.H. Review of “Effectiveness of Adding a MaskRecommendation to Other Public HealthMeasures to Prevent SARS-CoV-2 Infection inDanish Mask Wearers”, 2020.
- Leech, G.; Rogers-Smith, C.; Monrad, J.T.; Sandbrink, J.B.; Snodin, B.; Zinkov, R.; Rader, B.; Brownstein, J.S.; Gal, Y.; Bhatt, S.; Sharma, M.; Mindermann, S.; Brauner, J.M.; Aitchison, L. Mask wearing in community settings reduces SARS-CoV-2 transmission. Proceedings of the National Academy of Sciences 2022, 119. Publisher: Proceedings of the National Academy of Sciences. [Google Scholar] [CrossRef] [PubMed]
- Peeples, L. Face masks for COVID pass their largest test yet, 2021.
- Conger, K. Surgical masks reduce COVID-19 spread, large-scale study shows, 2021.
- Chikina, M.; Pegden, W.; Recht, B. Re-analysis on the statistical sampling biases of a mask promotion trial in Bangladesh: a statistical replication. Trials 2022, 23. Publisher: Springer Science and Business Media LLC. [Google Scholar] [CrossRef] [PubMed]
- Loeb, M.; Bartholomew, A.; Hashmi, M.; Tarhuni, W.; Hassany, M.; Youngster, I.; Somayaji, R.; Larios, O.; Kim, J.; Missaghi, B.; others. Medical masks versus N95 respirators for preventing COVID-19 among health care workers: a randomized trial. Annals of Internal Medicine 2022, 175, 1629–1638, Publisher: American College of Physicians. [CrossRef] [PubMed]
- Jefferson, T.; Dooley, L.; Ferroni, E.; Al-Ansary, L.A.; van Driel, M.L.; Bawazeer, G.A.; Jones, M.A.; Hoffmann, T.C.; Clark, J.; Beller, E.M.; Glasziou, P.P.; Conly, J.M. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database of Systematic Reviews 2023, 2023. [Google Scholar] [CrossRef]
- Jefferson, T.; Mar, C.B.D.; Dooley, L.; Ferroni, E.; Al-Ansary, L.A.; Bawazeer, G.A.; Driel, M.L.v.; Jones, M.A.; Thorning, S.; Beller, E.M.; Clark, J.; Hoffmann, T.C.; Glasziou, P.P.; Conly, J.M. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database of Systematic Reviews 2020, 2020. Publisher: Wiley. [Google Scholar] [CrossRef]
- Alfelali, M.; Haworth, E.A.; Barasheed, O.; Badahdah, A.M.; Bokhary, H.; Tashani, M.; Azeem, M.I.; Kok, J.; Taylor, J.; Barnes, E.H.; El Bashir, H.; Khandaker, G.; Holmes, E.C.; Dwyer, D.E.; Heron, L.G.; Wilson, G.J.; Booy, R.; Rashid, H.; on behalf of the Hajj Research Team. Facemask against viral respiratory infections among Hajj pilgrims: A challenging cluster-randomized trial. PLoS ONE 2020, 15, e0240287. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; Chu, D.K.; Akl, E.A.; El-harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; Hajizadeh, A.; Bak, A.; Izcovich, A.; Cuello-Garcia, C.A.; Chen, C.; Harris, D.J.; Borowiack, E.; Chamseddine, F.; Schünemann, F.; Morgano, G.P.; Schünemann, G.E.U.M.; Chen, G.; Zhao, H.; Neumann, I.; Chan, J.; Khabsa, J.; Hneiny, L.; Harrison, L.; Smith, M.; Rizk, N.; Rossi, P.G.; AbiHanna, P.; El-khoury, R.; Stalteri, R.; Baldeh, T.; Piggott, T.; Zhang, Y.; Saad, Z.; Khamis, A.; Reinap, M.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. The Lancet 2020, 395, 1973–1987, Publisher: Elsevier BV. [Google Scholar] [CrossRef]
- Liang, M.; Gao, L.; Cheng, C.; Zhou, Q.; Uy, J.P.; Heiner, K.; Sun, C. Efficacy of face mask in preventing respiratory virus transmission: A systematic review and meta-analysis. Travel Medicine and Infectious Disease 2020, 36, 101751, Publisher: Elsevier BV. [Google Scholar] [CrossRef]
- Nanda, A.; Hung, I.; Kwong, A.; Man, V.C.; Roy, P.; Davies, L.; Douek, M. Efficacy of surgical masks or cloth masks in the prevention of viral transmission: Systematic review, meta-analysis, and proposal for future trial. J Evid Based Med. 2021, 14, 97–111. [Google Scholar] [CrossRef]
- Li, Y.; Liang, M.; Gao, L.; Ahmed, M.A.; Uy, J.P.; Cheng, C.; Zhou, Q.; Sun, C. Face masks to prevent transmission of COVID-19: A systematic review and meta-analysis. American Journal of Infection Control 2021, 49, 900–906, Publisher: Elsevier BV. [Google Scholar] [CrossRef] [PubMed]
- Talic, S.; Shah, S.; Wild, H.; Gasevic, D.; Maharaj, A.; Ademi, Z.; Li, X.; Xu, W.; Mesa-Eguiagaray, I.; Rostron, J.; Theodoratou, E.; Zhang, X.; Motee, A.; Liew, D.; Ilic, D. Effectiveness of public health measures in reducing the incidence of covid-19, SARS-CoV-2 transmission, and covid-19 mortality: systematic review and meta-analysis. BMJ, 2021; p. e068302. [Google Scholar] [CrossRef]
- Tabatabaeizadeh, S.A. Airborne transmission of COVID-19 and the role of face mask to prevent it: a systematic review and meta-analysis. Eur J Med Res 2021, 26, 1. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Seong, D.; Li, H.; Chung, S.K.; Park, Y.; Lee, M.; Lee, S.W.; Yon, D.K.; Kim, J.H.; Lee, K.H.; Solmi, M.; Dragioti, E.; Koyanagi, A.; Jacob, L.; Kronbichler, A.; Tizaoui, K.; Cargnin, S.; Terrazzino, S.; Hong, S.H.; Abou Ghayda, R.; Radua, J.; Oh, H.; Kostev, K.; Ogino, S.; Lee, I.; Giovannucci, E.; Barnett, Y.; Butler, L.; McDermott, D.; Ilie, P.; Shin, J.I.; Smith, L. Comparative effectiveness of N95, surgical or medical, and non-medical facemasks in protection against respiratory virus infection: A systematic review and network meta-analysis. Reviews in Medical Virology 2022, 32. [Google Scholar] [CrossRef]
- Schoberer, D.; Osmancevic, S.; Reiter, L.; Thonhofer, N.; Hoedl, M. Rapid review and meta-analysis of the effectiveness of personal protective equipment for healthcare workers during the COVID-19 pandemic. Public Health in Practice 2022, 4, 100280. [Google Scholar] [CrossRef]
- Brainard, J.; Jones, N.R.; Lake, I.R.; Hooper, L.; Hunter, P.R. Community use of face masks and similar barriers to prevent respiratory illness such as COVID-19: a rapid scoping review. Eurosurveillance 2020, 25. Publisher: European Centre for Disease Control and Prevention (ECDC). [Google Scholar] [CrossRef]
- Wang, M.X.; Gwee, S.X.W.; Chua, P.E.Y.; Pang, J. Effectiveness of Surgical Face Masks in Reducing Acute Respiratory Infections in Non-Healthcare Settings: A Systematic Review and Meta-Analysis. Frontiers in Medicine 2020, 7. Publisher: Frontiers Media SA. [Google Scholar] [CrossRef]
- Spira, B. Correlation Between Mask Compliance and COVID-19 Outcomes in Europe. Cureus 2022. [Google Scholar] [CrossRef]
- Iwasaki, A.; Grubaugh, N.D. Why does Japan have so few cases of COVID-19? EMBO Mol Med 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Konishi, Y.; Saito, T.; Ishikawa, T.; Kanai, H.; Igei, N. How Did Japan Cope with COVID-19? Big Data and Purchasing Behavior*. Asian Economic Papers 2021, 20, 146–167. [Google Scholar] [CrossRef]
- IHME. Institute for Health Metrics and Evaluation. University of Washington, 2022.
- MacIntyre, C.R.; Wang, Q.; Seale, H.; Yang, P.; Shi, W.; Gao, Z.; Rahman, B.; Zhang, Y.; Wang, X.; Newall, A.T.; Heywood, A.; Dwyer, D.E. A Randomized Clinical Trial of Three Options for N95 Respirators and Medical Masks in Health Workers. Am J Respir Crit Care Med 2013, 187, 960–966. [Google Scholar] [CrossRef] [PubMed]
- Colquhoun, D. The reproducibility of research and the misinterpretation of p -values. R. Soc. open sci. 2017, 4, 171085. [Google Scholar] [CrossRef]
- Syed, Q. Behind the mask. Journey through an epidemic: some observations of contrasting public health responses to SARS. Journal of Epidemiology & Community Health 2003, 57, 855–856. [Google Scholar] [CrossRef]
- Valdiserri, R.O.; Holtgrave, D.R.; Kalichman, S.C. Barrier Methods for the Prevention of Infectious Diseases: Decades of Condom Research can Inform the Promotion of Face Mask Use. AIDS Behav 2020, 24, 3283–3287. [Google Scholar] [CrossRef]
- Yan, Y.; Bayham, J.; Richter, A.; Fenichel, E.P. Risk compensation and face mask mandates during the COVID-19 pandemic. Sci Rep 2021, 11, 3174. [Google Scholar] [CrossRef]
- Weller, S.C.; Davis-Beaty, K. Condom effectiveness in reducing heterosexual HIV transmission. Cochrane Database of Systematic Reviews 2002, 2012. [Google Scholar] [CrossRef]
- Gallo, M.F.; Grimes, D.A.; Lopez, L.M.; Schulz, K.F. Nonlatex versus latex male condoms for contraception. Cochrane Database of Systematic Reviews 2006. [Google Scholar] [CrossRef]
- Steiner, M.; Trussell, J.; Glover, L.; Joanis, C.; Spruyt, A.; Dorflinger, L. Standardized protocols for condom breakage and slippage trials: a proposal. Am J Public Health 1994, 84, 1897–1900. [Google Scholar] [CrossRef] [PubMed]
- Shang, A.; Huwiler-Müntener, K.; Nartey, L.; Jüni, P.; Dörig, S.; Sterne, J.A.; Pewsner, D.; Egger, M. Are the clinical effects of homoeopathy placebo effects? Comparative study of placebo-controlled trials of homoeopathy and allopathy. The Lancet 2005, 366, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Rojas-Reyes, M.X.; Granados Rugeles, C. Oral antibiotics versus parenteral antibiotics for severe pneumonia in children. Cochrane Database of Systematic Reviews 2006. [Google Scholar] [CrossRef] [PubMed]
- El Sayed, I.; Liu, Q.; Wee, I.; Hine, P. Antibiotics for treating scrub typhus. Cochrane Database of Systematic Reviews 2018, 2018. [Google Scholar] [CrossRef] [PubMed]
- Shah, Y.; Kurelek, J.W.; Peterson, S.D.; Yarusevych, S. Experimental investigation of indoor aerosol dispersion and accumulation in the context of COVID-19: Effects of masks and ventilation. Physics of Fluids 2021, 33, 073315. [Google Scholar] [CrossRef]
- Drewnick, F.; Pikmann, J.; Fachinger, F.; Moormann, L.; Sprang, F.; Borrmann, S. Aerosol filtration efficiency of household materials for homemade face masks: Influence of material properties, particle size, particle electrical charge, face velocity, and leaks. Aerosol Science and Technology 2021, 55, 63–79. [Google Scholar] [CrossRef]
- Sankhyan, S.; Heinselman, K.N.; Ciesielski, P.N.; Barnes, T.; Himmel, M.E.; Teed, H.; Patel, S.; Vance, M.E. Filtration Performance of Layering Masks and Face Coverings and the Reusability of Cotton Masks after Repeated Washing and Drying. Aerosol Air Qual. Res. 2021, 21, 210117. [Google Scholar] [CrossRef]
- Kwong, L.H.; Wilson, R.; Kumar, S.; Crider, Y.S.; Reyes Sanchez, Y.; Rempel, D.; Pillarisetti, A. Review of the Breathability and Filtration Efficiency of Common Household Materials for Face Masks. ACS Nano 2021, 15, 5904–5924. [Google Scholar] [CrossRef] [PubMed]
- Joo, T.; Takeuchi, M.; Liu, F.; Rivera, M.P.; Barr, J.; Blum, E.S.; Parker, E.; Tipton, J.H.; Varnedoe, J.; Dutta, B.; Lively, R.P.; Ng, N.L. Evaluation of particle filtration efficiency of commercially available materials for homemade face mask usage. Aerosol Science and Technology 2021, 55, 930–942. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Fisman, D.; Cane, D.J.; Oliver, M.; Macintyre, C.R. Adapt or die: how the pandemic made the shift from EBM to EBM+ more urgent. BMJ EBM 2022, 27, 253–260. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A. Why Science Is Not Necessarily Self-Correcting. Perspect Psychol Sci 2012, 7, 645–654. [Google Scholar] [CrossRef]
- Gall, T.; Ioannidis, J.P.A.; Maniadis, Z. The credibility crisis in research: Can economics tools help? PLoS Biol 2017, 15, e2001846. [Google Scholar] [CrossRef]
- Wong, C.H.; Siah, K.W.; Lo, A.W. Estimation of clinical trial success rates and related parameters. Biostatistics 2019, 20, 273–286. [Google Scholar] [CrossRef]
- Becker, R.E.; Greig, N.H. Fire in the ashes: Can failed Alzheimer’s disease drugs succeed with second chances? Alzheimer’s & Dementia 2013, 9, 50–57. [Google Scholar] [CrossRef]
- Müller, T.D.; Blüher, M.; Tschöp, M.H.; DiMarchi, R.D. Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov 2022, 21, 201–223. [Google Scholar] [CrossRef]
- Beauchamp, J.D.; Mayhew, C.A. Revisiting the rationale of mandatory masking. Journal of Breath Research 2023, 17, 042001. [Google Scholar] [CrossRef]
Figure 1.
Correlation between the proportion of RCTs in 10 different mask meta-analyses and the respective pooled odds ratio (OR) or risk reduction ratio (RR). The results of ten meta-analyses on masks and respiratory viral illnesses, all published since 2020 [18,21,22,23,24,25,26,27,28,30], were analysed for ORs or RRs and the proportion of RCTs or cRCTs included in the analysis. An individual meta-analysis is represented by a bullseye symbol. The red symbols indicate no statistically significant reduction in the primary outcome (lab-confirmed illness or influenza-like illness).
Figure 1.
Correlation between the proportion of RCTs in 10 different mask meta-analyses and the respective pooled odds ratio (OR) or risk reduction ratio (RR). The results of ten meta-analyses on masks and respiratory viral illnesses, all published since 2020 [18,21,22,23,24,25,26,27,28,30], were analysed for ORs or RRs and the proportion of RCTs or cRCTs included in the analysis. An individual meta-analysis is represented by a bullseye symbol. The red symbols indicate no statistically significant reduction in the primary outcome (lab-confirmed illness or influenza-like illness).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



