
Submitted:
08 April 2024
Posted:
09 April 2024
You are already at the latest version
Abstract
Aerobic vaginitis (AV) is a distinct clinical entity characterized by inflammation and abnormal vaginal microflora. Often mistaken for bacterial vaginosis, AV remains relatively unknown and underdiagnosed. AV's understanding is evolving, with some experts suggesting it may primarily be an immunological disorder, the prevalence of which ranges from 7-13% in non-pregnant women and 4.1-8.3% during pregnancy. Pregnancy can affect susceptibility to vaginal infections, leading to adverse outcomes for the woman and the newborn. This review summarizes the correlation between AV and adverse pregnancy outcomes, particularly preterm birth, the leading cause of morbidity and mortality among neonates. Improved understanding of AV's impact on pregnancy outcomes can lead to early recognition, proper management, and effective interventions. While some studies support an association between AV and preterm labor, the existing knowledge of this relationship remains limited. The evidence suggests that AV may contribute to adverse pregnancy outcomes, mainly preterm birth, but further research is needed to establish a definitive link. Further studies are needed to investigate the underlying mechanisms and clarify AV's role in premature labor. A comprehensive understanding of AV's impact on pregnancy outcomes is crucial for early recognition, appropriate management, and effective interventions.
Keywords:
Aerobic vaginitis
; desquamative aerobic vaginitis
; pregnancy outcomes
; preterm labor
Introduction
Aerobic vaginitis (AV) is a distinct vaginal infectious entity characterized by an overgrowth of commensal aerobic microorganisms, mostly of intestinal origin. This condition gives rise to an abnormal (dysbiotic) vaginal microflora consisting of aerobic, enteric bacteria, variable levels of vaginal inflammation, and deficient epithelial maturation [1].
The exact nature of the relationship between AV and its aerobic microflora is still not fully understood. While some consider AV a strict bacterial infection, others propose it is an immunological disorder that influences the vaginal microflora, or a dermatological disease in the vagina [2]. This intriguing perspective highlights the multifaceted nature of AV, warranting further investigation into its underlying mechanisms. In the state of health, the vaginal microbiota comprises a dynamic ecosystem consisting of diverse microbial populations, present in varying proportions, operating to safeguard the vaginal epithelium against different infectious agents.
The symbiotic bacteria, particularly Lactobacillus species, play a crucial role in maintaining vaginal health. These bacteria are responsible for the acidic pH of the vagina, produced through the conversion of glycogen stored in epithelial cells into lactic acid. Lactobacilli form a protective layer on the vaginal mucosa, preventing the adhesion and penetration of pathogens. Furthermore, they produce hydrogen peroxide, bacteriocins, and bacteriocin-like substances, reinforcing the mechanisms against invasion and colonization by opportunistic pathogens [3,4].
Pregnancy induces alterations in the immune response, potentially influencing susceptibility to vaginal infections. Studies have found that, estrogen reduces the resistance of vaginal epithelial cells to pathogens, while progesterone enhances the adhesion of pathogens to the vaginal epithelium [5,6]. Moreover, estrogen and progesterone may increase the virulence of pathogenic strains, potentially leading to severe adverse outcomes. Approximately 25-40% of preterm deliveries are linked to infections, either directly or indirectly through inflammation processes. The pathways leading to preterm labor involve the activation of specific biochemical mechanisms, including increased genital tract prostaglandins and proteases, progesterone withdrawal, and changes in hormone concentrations. Inflammatory responses may also contribute to preterm premature rupture of membranes (PPROM). Inflammation, typically a regulatory mechanism for tissue response, can result in an exaggerated immune response, with increased production of inflammatory cytokines, elastases, and matrix metalloproteinases (MMPs). This heightened inflammation triggers the withdrawal of progesterone, crucial for maintaining pregnancy.
This review aims to explore the correlation between AV and adverse pregnancy outcomes, focusing on preterm birth. Preterm delivery (PTD), defined as delivery before 37 weeks of gestation by the WHO, is a significant global public health issue [7,8]. Neonatal morbidity and mortality present significant challenges, particularly in developed countries, where they serve as primary determinants of adverse outcomes and globally stand as the second leading cause of death among children under five [9]. This study seeks to contribute to the knowledge we have in reproductive health by rigorously examining the potential correlation between AV and adverse pregnancy outcomes. By unraveling the complexities of such interactions, the present study seeks to establish a strong basis for promptly identifying potential risks associated with AV during pregnancy. The knowledge gained from this investigation is intended to guide timely and evidence-based interventions, thereby fostering the development of precise and effective management strategies. Through these efforts, the ultimate goal is to enhance maternal well-being during pregnancy and, consequently, reduce the incidence of neonatal morbidity and mortality.
Materials and Methods
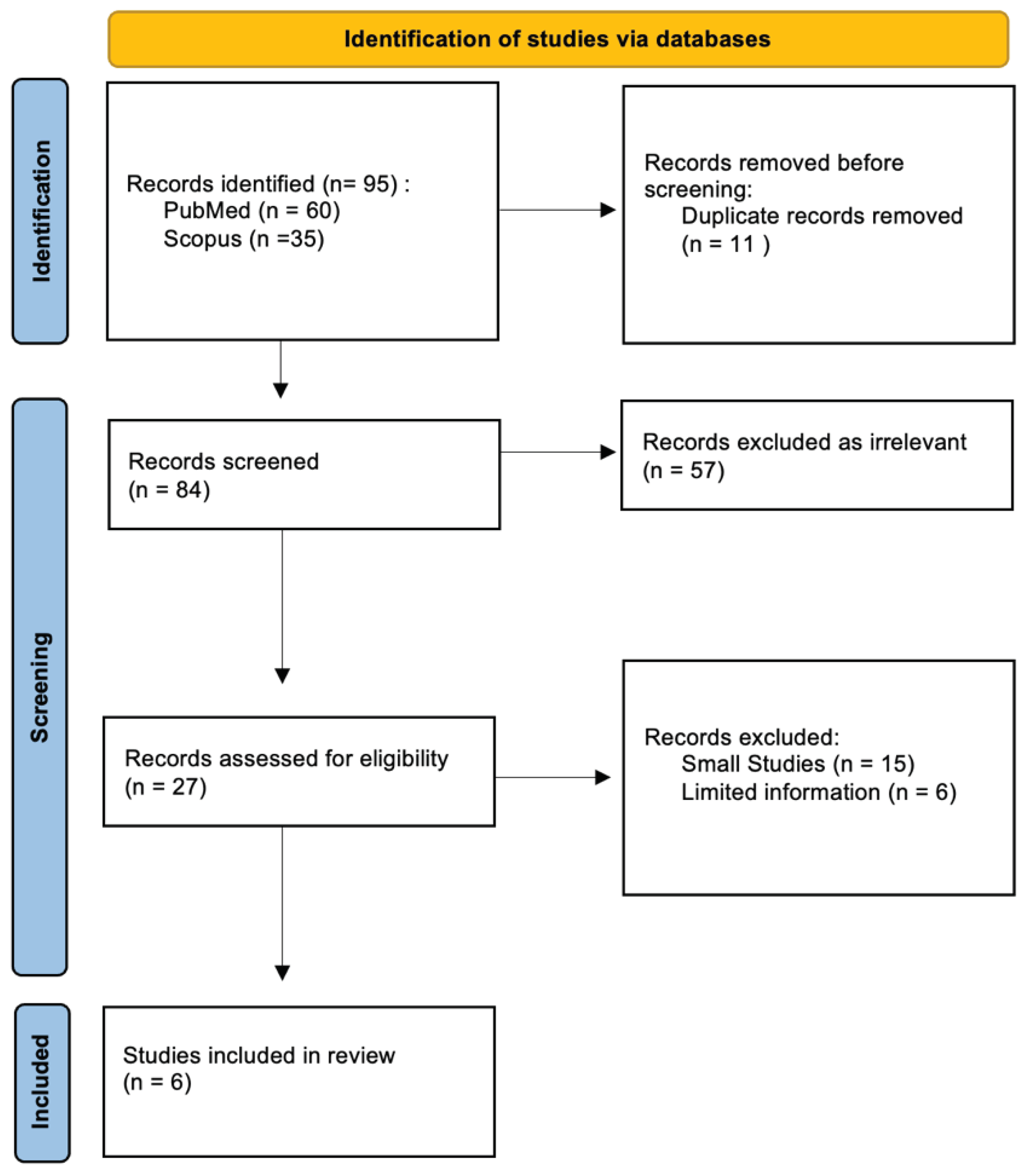
A comprehensive literature review using PubMed and Scopus databases (January 2002 until October 2022) was conducted. The specific query employed was ("aerobic vaginitis" OR “DIV” OR “desquamative inflammatory vaginitis”) AND ("pregnancy outcomes" OR "preterm delivery" OR "preterm birth” OR "preterm labor" OR "premature delivery"), cross- referencing the resulting articles with the query: aerobic vaginitis preterm birth. All studies published in English from 2002 to 2022, based on searched keywords from the databases, were included in our review, including those on human and animal models. Our study excluded non-English studies, conference abstracts, letters to the editor, and ex vivo studies. A total of 95 articles were identified from the databases. Initially, 11 articles were removed as duplicates. The abstracts were screened for relevance, which allowed us to exclude 57 articles that did not discuss any form of AV, but other forms of vaginitis, or did not address pregnancy. After careful analysis and exclusion of 21 more studies, which did not include a sufficient number of participants or did not approach the investigated relationship between av and preterm birth, 6 studies were included in the final review. Three independent researchers reviewed the articles and hand-searched literature. Disagreements were discussed and resolved.
Figure 1.
Process of elimination and inclusion of studies for review. After conducting a Pubmed and Scopus search, a total of 95 articles were reviewed, out of which 11 were removed as duplicates, 57 were deemed irrelevant and 21 were excluded due to limited information and small sample sizes. Finally, 6 studies were deemed suitable and included in the final review. PRISMA Flow Diagram [10].
Figure 1.
Process of elimination and inclusion of studies for review. After conducting a Pubmed and Scopus search, a total of 95 articles were reviewed, out of which 11 were removed as duplicates, 57 were deemed irrelevant and 21 were excluded due to limited information and small sample sizes. Finally, 6 studies were deemed suitable and included in the final review. PRISMA Flow Diagram [10].
Results
In this article, we investigated the correlation between AV and PTB across seven different studies. Among these studies, five provided evidence supporting the correlation between AV and PTB, while two could not prove the claim.
The first study [11], conducted by Donders et al. in 2009, involved 759 pregnant women at 9-16 weeks out of 1026 women who were requested to participate in the sampling procedure. The results indicated that coccoid AV was associated with increased risks of extremely preterm birth (OR 3.2; 95% CI 1.2-9.1) and miscarriage (OR 5.2; 95% CI 1.5-17). Similar are the results of the second study by Donders et al. in 2010 [12]. This study referred to the same population of 1026 low-risk pregnant women before the 16th week as the first study conducted by Donders et al. After analysis, it was determined that women with severe AV at 10-14 weeks had shorter cervix lengths at 20-24 and 30-34 weeks, which increased the likelihood of preterm birth. Na Li's study [13], which involved 685 pregnant women at 22.3±8.6 weeks, revealed that the incidences of preterm birth, premature rupture of membranes, neonatal jaundice, and neonatal infection were significantly higher in the AV group compared to the control group (P<0.001, <0.001, =0.007, and =0.025). Additionally, Mahmoud F. Hassan's study et al. [14] with 600 34-36 week pregnant women showed a significant correlation between preterm birth and AV (p=0.001). Cha Han's et al. study [15], which included 624 pregnant women and 365 nonpregnant women in the third trimester, found a correlation between AV and premature rupture of membranes (PROM) (p=0.003), even though the difference was not significant regarding PTB (p=0.236).
On the other hand, two studies did not yield positive results regarding the correlation between AV and PTB. Krauss Silva's et al. study [16], comprising 1199 pregnant women, < 20 weeks gestation, without risk factors, with pH>4.5, did not show an association between moderate AV and spontaneous preterm delivery or abortion. As limitations of the study, we should consider the fact that the analyzed samples were subsamples of Gram-stained vaginal smears with intermediate degree infection and BV, and less than 5% presented moderate AV with no severe cases. The use of Gram staining resulted in the exclusion of the proportion of toxic leukocytes overstimulation of the occurrence of disturbances of the vaginal flora, making the diagnosis questionable.
Furthermore, Thi Cha Nguyen's et al. study [17] with 323 pregnant women in the third trimester, 84% with light and 16% with moderate AV did not find any effect of AV on either PROM or preterm premature rupture of membranes (pPROM). The study revealed that a significant majority of women (84%) displayed a moderate type of asymptomatic BV without any instances of severe AV. Moreover, the occurrence of E. coli and S. agalactiae bacteria was notably lower compared to earlier research. The incidence of preterm births was also minimal in both groups studied. However, the study's weakness lies in its sample size calculation, tailored mainly to identify AV incidence in pregnant women. Consequently, the sample size might be insufficient to highlight differences in outcomes beyond AV incidence effectively.

Table 1.
Studies investigating the correlation between AV (Aerobic Vaginitis) and PTB (Preterm Birth) (* The first two studies refer to the same population, as the population of 759 women is a subset of the group of 1026 women).
Table 1.
Studies investigating the correlation between AV (Aerobic Vaginitis) and PTB (Preterm Birth) (* The first two studies refer to the same population, as the population of 759 women is a subset of the group of 1026 women).
| Study | Patient inclusion criteria | AV diagnostic criteria | Severity | Gestational age at screening | Outcome | OR/ p-value |
|---|---|---|---|---|---|---|
|
*Donders et al 2009 [11] |
759 pregnant women | Donders’ modified score | 9-16 weeks | Coccoid AV associated with increased risks of EPTB and miscarriage |
EPTB OR 3.2; 95% CI 1.2-9.1/ OR 5.2; 95% CI 1.5-17) |
|
| *Donders et al 2010 [12] | 1026 low risk pregnant women | Donders’ modified score | Severe | Before 16w | Severe A V at 10-14 weeks, the cervix appeared shorter at 20-24 and at 30-34 weeks than in other women. |
|
| Na Li et al [13] | 685 pregnant women (control group n=503, AV group n=182) |
Donders’ modified score | 22.3±8.6 weeks, | Incidences of pb, PROM, neonatal jaundice, and neonatal infection significantly higher in the AV group |
<0.001 =0.007, =0.025 |
|
| Mahmoud F. Hassan et al2020 [14] | 600 pregnant women | Composite AV score ≥ 3 determined by saline wet mount microscopy |
34-36 weeks | PTB | 0,001 | |
| Cha Han et al [15] | 624 pregnant women and 365 Non pregnant women |
Score >3 saline wet mount microscopy | 3rd trimester | PROM 0,003 But not PTB 0,236 |
0.003 | |
| Krauss-Silva et al [16] | 1199 pregnant women without risk factors, pH>4.5 | Donders’ modified score (proportion of toxic leukocytes” criterion was not considered in the modified score used) |
< 20 weeks’ gestation | No spontaneous case of PD or abortion was associated with severe or moderate AV. | ||
| Thi Chau Nguyen et al [17] | 323 pregnant women | Donders’ modified score and culture | 84% light , 16% moderate | 3rd trimester | Puerperal sepsis 6%, pb rate low both groups (2% vs 3.3%). without effect of AV on either PROM or pPROM. |
0.02 |
Table 2.
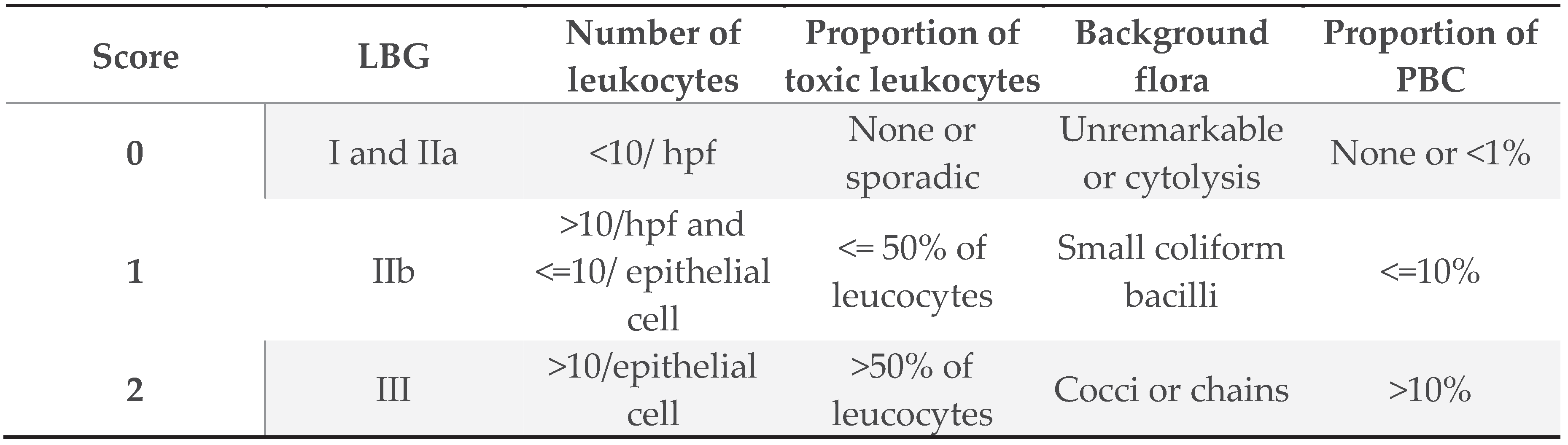
Donders’ modified score: the diagnostic criteria involves the combination of AV (aerobic vaginitis) Gram staining and clinical manifestations.[1] (LBG: Lactobacillary grades, PBC: Parabasal epitheliocytes).
Table 2.
Donders’ modified score: the diagnostic criteria involves the combination of AV (aerobic vaginitis) Gram staining and clinical manifestations.[1] (LBG: Lactobacillary grades, PBC: Parabasal epitheliocytes).
Discussion
Our review provides contradictory evidence found in global literature regarding association of AV and PTB. Even though most studies presented here supported the correlation between abnormal vaginal flora and preterm birth, it's important to note that existing literature also included studies that lack evidence of positive association. These findings emphasize the complexity of this relationship and the need for further research to understand AV's impact on adverse pregnancy outcomes.
AV was initially identified by Belgian scholar Donders and colleagues in 2002, and its prevalence varies across regions. While the prevalence of AV in non-pregnant women ranges from 4,2-25,8%, it is estimated to be 4.1-8.3% during pregnancy. The most frequently encountered pathogens, including E. coli, Klebsiella pneumoniae, Staphylococcus aureus, group B Streptococcus (GBS), and Enterococcus faecalis, appear in varying proportions among several studies [18,19].
Diagnosis of AV relies on wet mount microscopy, performed by a phase-contrast microscope, in order to assess lactobacillus grades and other variables, such as leukocytes, the percentage of toxic leukocytes and parabasal epithelial cells, and the type of background flora. All the parameters mentioned above serve as parts of a composite score that directs to the final diagnosis [1,20].
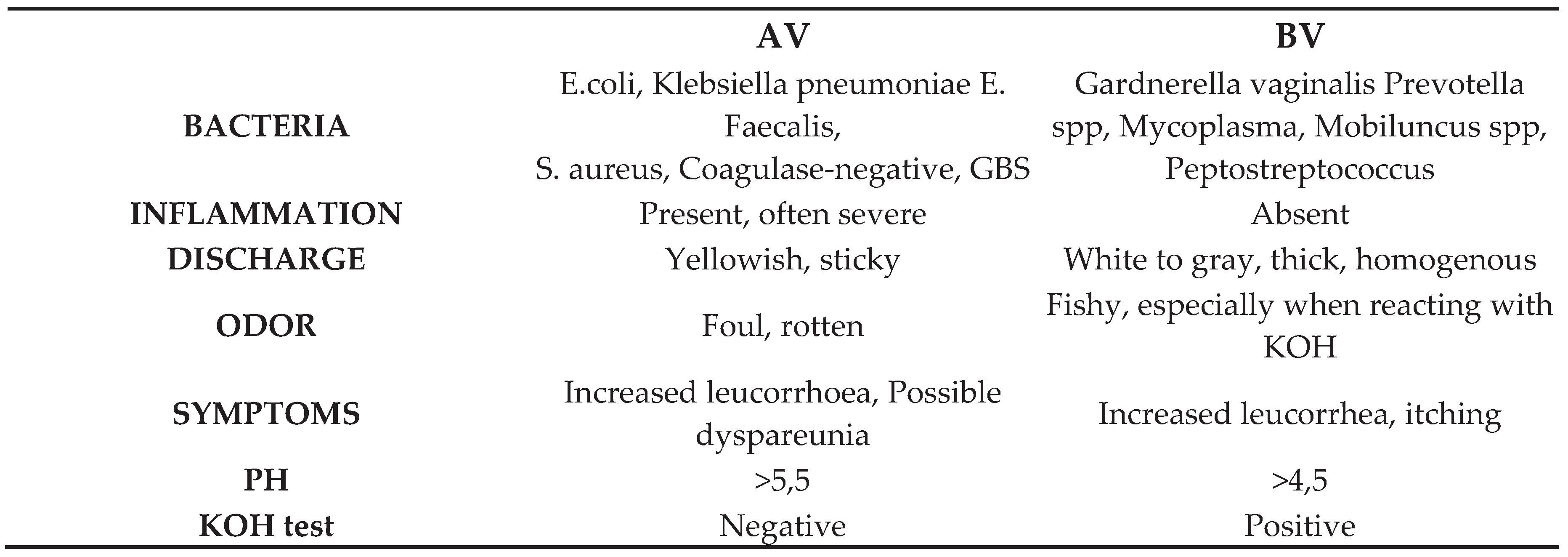
As we stated above, AV is a relatively unknown and underdiagnosed, commonly mistaken for BV (Bacterial Vaginosis). The features that contribute to the differential diagnosis of BV are listed in the table below [3,4].
Table 3.
Differential Diagnosis between Aerobic Vaginitis (AV) and Bacterial Vaginosis (BV).
While some studies support an association between aerobic vaginitis (AV) and preterm labor, the existing knowledge of this relationship remains limited. The available evidence, from the limited number of concrete studies included in our review, suggests that AV may contribute to adverse pregnancy outcomes, particularly preterm birth, but further research is needed to establish a definitive link.
A significant percentage (25-40%) of preterm deliveries can be attributed to various pathogens causing infections directly (overt or subclinical) and indirectly via the inflammation process elicited by such infections [21]. The pathological processes that lead to preterm labor involve the activation of one or more components of a specific biochemical pathway, such as the increased production of prostaglandins and proteases in the genital tract, the functional withdrawal of progesterone and changes in hormone concentrations such as corticotropin-releasing factor (CRF) and cortisol [22,23,24]. These inflammatory processes may also lead to preterm premature rupture of membranes (PPROM) [25].
Inflammation can be considered as a regulative mechanism by which the tissues respond to injurious stimuli in order to control and repair possible damage. More specifically, inflammation induces an exaggerated immune response that increases the production of inflammatory cytokines, elastases, and matrix metalloproteinases (MMPs) and triggers the functional withdrawal of progesterone, a vital hormone for pregnancy’s maintenance [26,27].
Regarding infections, bacteria are found in the fetal circulation in 30% of intra-amniotic infections, leading to a systemic inflammatory response in the fetus [25]. The most common route of infection is ascending [28], while there is also a possibility of hematogenous dispersion with transplacental passage [29]. Most likely, pathways for infection-induced PTB include decidual stimulation and the fetal immunological response, both as innate immune system reactions [21,30]. Moreover, a fetal response takes place as the infection promotes the release of corticotropin-releasing hormone and, subsequently, the release of fetal corticotropin and fetal cortisol from both the placenta and the fetal hypothalamus, resulting in prostaglandin production [31].
As supporting evidence, it is worth considering two more studies which suggest a correlation between abnormal vaginal flora and PB. Szubert [3] examined 396 pregnant women with abundant growth of aerobic bacteria and fungi while 413 with physiologic vaginal biocenosis and found a significantly higher percentage of PB among patients infected with GBS than those not infected, while there was no statistical correlation between PTB and Klebsiella spp., S. aureus or Candida spp. infection. In the meanwhile, Hocevar [32] suggested that preterm relative to term pregnancies have higher richness and diversity of the vaginal microbiome, along with reduced Lactobacillus species.
Supporting our case, is also the existing body of knowledge regarding the influence of vaginal infections on pregnancy outcomes, and specifically the impact of the extensively studied BV. In a comprehensive systematic review conducted by Josiane Kenfack-Zanguim in 2022, after an exhaustive search extending from January 2002 until December 2022, 26 articles met the inclusion criteria. This review served as a vital compendium of contemporary knowledge pertaining to the impact of Bacterial Vaginosis (BV) on maternal and neonatal outcomes.
Among the findings, it was revealed that PTB exhibited the highest prevalence at 17.9%, with a 95% confidence interval ranging from 13% to 23.3% across the various studies. Moreover, the study unveiled a significant association between BV and PTB, with an odds ratio (OR) of 1.76 and a 95% confidence interval of 1.32 to 2.35. Additionally, BV was also linked to Premature Rupture of Membranes (PROM) with an OR of 2.59 and a 95% confidence interval of 1.39 to 4.82 [33].
Similarly, Mohanty [34] conducted a meta-analysis, including 20 articles, which produced strikingly consistent results. This meta-analysis also proves a significant association between bacterial vaginosis and preterm birth, with an overall odds ratio (OR) of 1.79 and a 95% Confidence Interval of 1.32 to 2.43.
Considering the shared pathophysiological mechanisms between BV and AV and the inflammatory factors associated with AV, this entity may be a more potential candidate to cause pregnancy complications. Specifically, dysbiosis occurs in both AV and BV, leading to a decrease in lactobacillus-dominated microflora, disrupting the healthy vaginal ecosystem. However, AV presents a unique profile, marked by a more pronounced increase in interleukin 1β (IL-1β) compared to BV, combined with elevated levels of interleukin 6 (IL-6) and interleukin 8 (IL-8), which are not commonly seen in BV cases [35,36,37]. Both AV and BV involve the production of sialidases, enzymes that diminish the local immune response [36,38]. Additionally, AV frequently presents with lower local estrogen levels, a prevalent characteristic, whereas in BV, this is not consistently implicated as an etiological factor. [39] The presence of aerobic bacteria contributes to the pathophysiological pathways in different ways, depending on the particular characteristics of each bacterium [1,40].
E. coli is the most frequently cultured Gram (-) microorganism in AV, principally as the only isolated microorganism. Its role is controversial, but it is still one of the most frequent causes of neonatal sepsis and chorioamnionitis [41]. In the study conducted by Lobos et al, 46 cases of E. coli was described as the only microorganism isolated in cultures, taken from 425 women with vaginal infection. The genetic subtypes of E. coli were the same subgroup in 98% of the cases. The authors suggested that these strains probably constitute a subpopulation within the other species specifically found in vaginal secretions. Although the finding's clinical implications remain unclear, one can assume that specific subtypes deriving from the vagina maybe are associated with adverse pregnancy outcomes. The fact that the specific E. coli strain is an uropathogen, also supports the above-described hypothesis [42].
Undoubtedly, conducting a thorough exploration of treatment options aimed at preventing preterm birth stands as a pivotal endeavor in mitigating the associated complications. The most effective way to treat AV in both pregnant and non-pregnant women remains uncertain. Over the years, several therapeutic approaches have been suggested. Antibiotics, like metronidazole, have been commonly used, but their effectiveness is unclear. Studies show that metronidazole may not decrease the risk of preterm birth in women with AV, and, in some cases, it might even increase the risk. Furthermore, research conducted by Odendaal [43] and Klebanoff [44], focusing on the treatment of trichomoniasis or bacterial vaginosis (BV), revealed a higher likelihood of preterm birth following metronidazole treatment. This finding has led several experts to a strong consensus that using metronidazole during pregnancy to mitigate the risk of preterm birth should be avoided.
On the other side, when researchers employed antibiotics with a broader spectrum, capable of targeting Gram-positive cocci and E. coli, they achieved a decrease in the incidence of preterm birth in the majority of placebo-controlled studies, such as oral clindamycin [45]. Although not all of them showed the same positive results, for example the use of vaginal clindamycin in the treatment of bacterial vaginosis (BV) by Kekki et al [46], which indicated that that vaginal clindamycin did not lead to a reduction in the rate of preterm deliveries or peripartum infections when compared to the placebo group.
In a study by Tempera et al [47], local kanamycin was evaluated in non-pregnant women with AV. Through a thorough analysis of culture results, the researchers suggested that this topical treatment could be an effective method for addressing Enterobacteriaceae in the context of AV. Although some of these options for the use of antibiotics seem to be very promising, testing during pregnancy with such agents has not been conducted in a systematic way in order to provide us with robust data.
The use of probiotics has also been reported, mainly to treat abnormal vaginal flora during pregnancy, and not specifically as a regime for AV. A Cochrane review of all randomized controlled trials assessing the prevention of preterm birth through the use of antibiotics, showed that while probiotics seem to be effective in treating vaginal infections during pregnancy, there is currently a lack of adequate trial data to evaluate their impact on preterm birth and its associated complications [48]. We should also consider the fact that AV can co-occur with other genital tract infections, such as BV, candidiasis and sexually transmitted infections, therefore the therapy must be tailored to each patient. In the studies analyzed, no therapeutic agent was used, so the development of research to clarify the appropriate treatment regimen seems of utmost importance.
Our review bears a number of limitations including, the heterogeneity of the studies reviewed, in terms of the population under study, the gestational age, the diagnosis criteria, and further particular characteristics of each research. To address this limitation, future research endeavors should be meticulously designed, ensuring an adequate number of participants and adopting a standardized methodology. This approach will facilitate meta-analysis, allowing for a comprehensive synthesis of findings across studies and enabling more robust conclusions to be drawn.
Additional studies are necessary to define the contours of AV’s impact on adverse pregnancy outcomes, focusing on preterm labor. Gaining a thorough comprehension of how AV influences the outcome of pregnancy holds significant importance for early recognition, suitable care, and successful interventions. Comprehensive exploration into the impact of Aerobic Vaginitis (AV) on adverse pregnancy outcomes, particularly its association with preterm labor, necessitates further studies. The complex effects of AV on pregnancy need further exploration as current knowledge is insufficient. Understanding the nuanced interactions between AV and pregnancy outcomes holds paramount importance for various reasons. Firstly, it facilitates early recognition of potential risks, enabling healthcare professionals to intervene promptly. Secondly, it paves the way for the development of suitable care strategies tailored to address the specific challenges posed by AV during pregnancy. Additionally, a thorough comprehension of how AV affects pregnancy outcomes is crucial for the implementation of successful interventions that can positively impact maternal and neonatal health. By advancing our insights in this domain, we are ready to achieve improved reproductive health results, with a particular focus on mitigating the impact of preterm birth. Ultimately, these endeavors contribute to enhancing the overall well-being of both women and neonates, underscoring the importance of continued research in this critical area of maternal and child health. Progressing our insights in this domain will inevitably result in improved reproductive health results, lessening the impact of preterm birth and enhancing the well-being of both women and neonates.
Author Contributions
Conceptualization: Alexandros Psarris and Panagiota Zarmakoupi; methodology: Alexandros Psarris; validation: Michael Syndos and Georgios Daskalakis; formal analysis: Panagiota Zarmakoupi and Christina Karasmani; investigation: Panagiota Zarmakoupi; resources: Andreas Pampanos, Kalliopi I. Pappa and Ekaterini Domali, writing - original draft preparation: Panagiota Zarmakoupi; writing – review and editing: Christina Karasmani; visualization: Christina Karasmani, Nikolaos Thomakos; supervision: Alexandros Psarris, Panagiotis Antsaklis, Marianna Theodora, Kalliopi I. Pappa, Michael Syndos, Ekaterini Domali, Aristotelis Tsiakalos, Karolina Akinosoglou and Georgios Daskalakis; project administration: Panagiotis Antsaklis and Marianna Theodora. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
The data used to support the findings of this study are included within the article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- G. G. G. Donders, G. Bellen, S. Grinceviciene, K. Ruban, and P. Vieira-Baptista, “Aerobic vaginitis: no longer a stranger,” Res Microbiol, vol. 168, no. 9–10, 2017. [CrossRef]
- L. Edwards, “Dermatologic causes of vaginitis: A clinical review,” Dermatologic Clinics, vol. 28, no. 4. 2010. [CrossRef]
- M. Szubert et al., “The Association Between Imbalances In Vaginal Microflora And Duration Of Pregnancy As Well As Selected Maternal And Neonatal Parameters,” Ginekol Pol, vol. 92, no. 9, pp. 624–630, 2021. [CrossRef]
- D. Pacha-Herrera, G. Vasco, C. Cruz-Betancourt, J. M. Galarza, V. Barragán, and A. Machado, “Vaginal Microbiota Evaluation and Lactobacilli Quantification by qPCR in Pregnant and Non-pregnant Women: A Pilot Study,” Front Cell Infect Microbiol, vol. 10, 2020. [CrossRef]
- L. Salinas-Muñoz et al., “Estrogen receptor-alpha (ESR1) governs the lower female reproductive tract vulnerability to Candida albicans,” Front Immunol, vol. 9, no. MAY, 2018. [CrossRef]
- P. L. Fidel, J. Cutright, and C. Steele, “Effects of reproductive hormones on experimental vaginal candidiasis,” Infect Immun, vol. 68, no. 2, 2000. [CrossRef]
- J. Perin et al., “Global, regional, and national causes of under-5 mortality in 2000–19: an updated systematic analysis with implications for the Sustainable Development Goals,” Lancet Child Adolesc Health, vol. 6, no. 2, 2022. [CrossRef]
- E. O. Ohuma et al., “National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis,” Lancet, 2023.
- Z. Ou et al., “Global trends in incidence and death of neonatal disorders and its specific causes in 204 countries/territories during 1990–2019,” BMC Public Health, vol. 22, no. 1, pp. 1–13, Dec. 2022. [CrossRef]
- M. J. Page et al., “The PRISMA 2020 statement: an updated guideline for reporting systematic reviews,” BMJ, vol. 372, Mar. 2021. [CrossRef]
- G. G. Donders et al., “Predictive value for preterm birth of abnormal vaginal flora, bacterial vaginosis and aerobic vaginitis during the first trimester of pregnancy,” BJOG, vol. 116, no. 10, pp. 1315–1324, Sep. 2009. [CrossRef]
- G. G. Donders et al., “Association between abnormal vaginal flora and cervical length as risk factors for preterm birth,” Ultrasound in Obstetrics & Gynecology, Aug. 2010. [CrossRef]
- N. Li, Y. Yue, and Q. Chen, “Pathogen profile and risk factors of aerobic vaginitis in pregnant women: A retrospective cohort study,” Ann Palliat Med, vol. 10, no. 8, pp. 8881–8888, Aug. 2021. [CrossRef]
- M. F. Hassan et al., “Does aerobic vaginitis have adverse pregnancy outcomes? Prospective observational study,” Infect Dis Obstet Gynecol, vol. 2020, 2020. [CrossRef]
- C. Han et al., “Aerobic vaginitis in late pregnancy and outcomes of pregnancy,” European Journal of Clinical Microbiology and Infectious Diseases, vol. 38, no. 2, pp. 233–239, Feb. 2019. [CrossRef]
- L. Krauss-Silva, A. Almada-Horta, M. B. Alves, K. G. Camacho, M. E. L. Moreira, and A. Braga, “Basic vaginal pH, bacterial vaginosis and aerobic vaginitis: Prevalence in early pregnancy and risk of spontaneous preterm delivery, a prospective study in a low socioeconomic and multiethnic South American population,” BMC Pregnancy Childbirth, vol. 14, no. 1, 2014. [CrossRef]
- T. C. Nguyen et al., “Aerobic vaginitis in the third trimester and its impact on pregnancy outcomes,” BMC Pregnancy Childbirth, vol. 22, no. 1, Dec. 2022. [CrossRef]
- X. Ma et al., “The pathogenesis of prevalent aerobic bacteria in aerobic vaginitis and adverse pregnancy outcomes: a narrative review,” Reproductive Health, vol. 19, no. 1. 2022. [CrossRef]
- E. Serretiello et al., “Prevalence and antibiotic resistance profile of bacterial pathogens in aerobic vaginitis: A retrospective study in italy,” Antibiotics, vol. 10, no. 9, 2021. [CrossRef]
- M. Dong et al., “Aerobic Vaginitis Diagnosis Criteria Combining Gram Stain with Clinical Features: An Establishment and Prospective Validation Study,” Diagnostics, vol. 12, no. 1, 2022. [CrossRef]
- R. L. Goldenberg, J. F. Culhane, J. D. Iams, and R. Romero, “Epidemiology and causes of preterm birth,” The Lancet, vol. 371, no. 9606. 2008. [CrossRef]
- R. Romero et al., “The preterm parturition syndrome,” BJOG: An International Journal of Obstetrics and Gynaecology, vol. 113, no. SUPPL. 3. 2006. [CrossRef]
- V. Khandre, J. Potdar, and A. Keerti, “Preterm Birth: An Overview,” Cureus, 2022. [CrossRef]
- E. J. Hodgson and C. J. Lockwood, “Preterm Birth: A Complex Disease,” in Preterm Birth: Prevention and Management, 2010. [CrossRef]
- G. Daskalakis et al., “Maternal Infection and Preterm Birth: From Molecular Basis to Clinical Implications,” Children, vol. 10, no. 5. 2023. [CrossRef]
- N. Gomez-Lopez et al., “Cellular immune responses in amniotic fluid of women with preterm labor and intra-amniotic infection or intra-amniotic inflammation,” American Journal of Reproductive Immunology, vol. 82, no. 5, 2019. [CrossRef]
- R. Goepfert et al., “Periodontal disease and upper genital tract inflammation in early spontaneous preterm birth,” Obstetrics and Gynecology, vol. 104, no. 4, 2004. [CrossRef]
- R. Romero, S. K. Dey, and S. J. Fisher, “Preterm labor: One syndrome, many causes,” Science, vol. 345, no. 6198. 2014. [CrossRef]
- P. Parthiban and J. Mahendra, “Toll-like receptors: A key marker for periodontal disease and preterm birth – A contemporary review,” Journal of Clinical and Diagnostic Research, vol. 9, no. 9. 2015. [CrossRef]
- M. V. Pararas, C. L. Skevaki, and D. A. Kafetzis, “Preterm birth due to maternal infection: Causative pathogens and modes of prevention,” European Journal of Clinical Microbiology and Infectious Diseases, vol. 25, no. 9. 2006. [CrossRef]
- R. Romero et al., “A fetal systemic inflammatory response is followed by the spontaneous onset of preterm parturition,” Am J Obstet Gynecol, vol. 179, no. 1, 1998. [CrossRef]
- K. Hočevar et al., “Vaginal Microbiome Signature Is Associated With Spontaneous Preterm Delivery,” Front Med (Lausanne), vol. 6, Sep. 2019. [CrossRef]
- J. Kenfack-Zanguim and et al., “Systematic review and meta-analysis of maternal and fetal outcomes among pregnant women with bacterial vaginosis,” Eur J Obstet Gynecol Reprod Biol, vol. 289, no. (2023): 9-18., Oct. 2023.
- T. Mohanty, P. P. Doke, and S. R. Khuroo, “Effect of bacterial vaginosis on preterm birth: a meta-analysis,” Arch Gynecol Obstet, vol. 308, no. 4, 2023. [CrossRef]
- C. Mitchell and J. Marrazzo, “Bacterial Vaginosis and the Cervicovaginal Immune Response,” American Journal of Reproductive Immunology, vol. 71, no. 6, 2014. [CrossRef]
- C. Marconi, G. G. G. Donders, G. Bellen, D. R. Brown, C. M. G. L. Parada, and M. G. Silva, “Sialidase activity in aerobic vaginitis is equal to levels during bacterial vaginosis,” European Journal of Obstetrics and Gynecology and Reproductive Biology, vol. 167, no. 2, 2013. [CrossRef]
- G. G. G. Donders, A. Vereecken, E. Bosmans, and B. Spitz, “Vaginal cytokines in normal pregnancy,” Am J Obstet Gynecol, vol. 189, no. 5, 2003. [CrossRef]
- S. Cauci et al., “Vaginal hydrolytic enzymes, immunoglobulin A against Gardnerella vaginalis toxin, and risk of early preterm birth among women in preterm labor with bacterial vaginosis or intermediate flora,” in American Journal of Obstetrics and Gynecology, 2002. [CrossRef]
- D. G.G.G., R. K., and B. G., “Selecting Anti-Microbial Treatment of Aerobic Vaginitis,” Curr Infect Dis Rep, vol. 17, no. 5, 2015.
- J. D. Sobel, “Desquamative inflammatory vaginitis: A new subgroup of purulent vaginitis responsive to topical 2% clindamycin therapy,” Am J Obstet Gynecol, vol. 171, no. 5, 1994. [CrossRef]
- L. Surgers et al., “Escherichia coli bacteraemia in pregnant women is life-threatening for foetuses,” Clinical Microbiology and Infection, vol. 20, no. 12, 2014. [CrossRef]
- Lobos and C. Padilla, “Phenotypic characterization and genomic DNA polymorphisms of Escherichia coli strains isolated as the sole micro-organism from vaginal infections,” Microbiology (N Y), vol. 155, no. 3, 2009. [CrossRef]
- H. Odendaal, “Preterm labour--is bacterial vaginosis involved?,” S Afr Med J, Jan. 2002, Accessed: Jan. 21, 2024. [Online]. Available: https://www.academia.edu/81395928/Preterm_labour_is_bacterial_vaginosis_involved.
- M. A. Klebanoff et al., “Failure of metronidazole to prevent preterm delivery among pregnant women with asymptomatic Trichomonas vaginalis infection,” N Engl J Med, vol. 345, no. 7, pp. 487–493, Aug. 2001. [CrossRef]
- Ugwumadu, I. Manyonda, F. Reid, and P. Hay, “Effect of early oral clindamycin on late miscarriage and preterm delivery in asymptomatic women with abnormal vaginal flora and bacterial vaginosis: A randomised controlled trial,” Lancet, vol. 361, no. 9362, pp. 983–988, Mar. 2003. [CrossRef]
- K. M, K. T, P. J, K.-R. M, C. B, and P. J, “Vaginal clindamycin in preventing preterm birth and peripartal infections in asymptomatic women with bacterial vaginosis: a randomized, controlled trial.,” Obstetrics and Gynecology, vol. 97, no. 5 Pt 1, pp. 643–648, May 2001. [CrossRef]
- G. Tempera, G. Bonfiglio, E. Cammarata, S. Corsello, and A. Cianci, “Microbiological/clinical characteristics and validation of topical therapy with kanamycin in aerobic vaginitis: A pilot study,” Int J Antimicrob Agents, vol. 24, no. 1, pp. 85–88, Jul. 2004. [CrossRef]
- M. Othman, J. P. Neilson, and Z. Alfirevic, “Probiotics for preventing preterm labour,” Cochrane Database Syst Rev, vol. 2007, no. 1, 2007. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



