
Submitted:
10 April 2024
Posted:
11 April 2024
You are already at the latest version
Abstract
Objective. To evaluate serum neuronal and inflammatory biomarkers in asphyctic newborns treated with hypothermia alone or hypothermia plus melatonin, and whether biomarkers correlate with neurodevelopmental outcomes.
Design. This is a pilot multicentre, randomised, controlled, double blind clinical trial. Neuronal glial fibrillary acidic protein (GFAP), granulocyte-macrophage colony-stimulating factor (GM-CSF), and inflammatory cytokines (interleukin (IL)-1, IL-2, IL-7 and IL-13) were measured in serum samples at hospital admission (T0), 24 hours (T1), 72 hours (T2) and 7-10 days of age (T3). Neurodevelopmental outcomes (Bayley Scales of Infant and Toddler Development-III scales, Gross Motor Function Classification System (GMFCS) and the Tardieu scale) were performed at 6 and 18 months. Setting: Level 3 neonatal intensive care unit. Patients and interventions: 25 newborns were recruited. The treated patients received a daily dose of intravenous melatonin, 5 mg per kg body weight, for 3 days.
Results. After adjusting the data for severity, in the group treated with melatonin, there is a decrease in plasma levels of GM-CSF, IL-2 and IL-13 at T1 compared to placebo, as well as, at T2, in GM-CSF concentrations, as well as IL-7 and IL-13 at T3. Evolutionarily, we found a significant decrease in GM-CSF concentrations in the treatment group compared to placebo, with no differences for the rest of the biomarkers. It is noteworthy that the sustained decrease in GM-CSF and inflammatory cytokines IL-2, IL-7 and IL-13 correlated with better neurodevelopmental outcomes at 6 and 18 months.
Conclusions. In neonates with hypoxic-ischemic encephalopathy, the addition of iv melatonin to hypothermia therapy affects the plasma concentration of biomarkers in the first week of life, with a high correlation with long-term neurological prognosis.
Keywords:
hypoxic-ischaemic encephalopathy
; therapeutic hypothermia
; pro-inflammatory biomarkers
; cytokines
; melatonin
; neurodevelopment
Introduction
Neonatal hypoxic ischemic encephalopathy (HIE) is a major cause of neonatal death and long-term neurologic disability in children [1]. It is well known to be associated with important medical, social, economic and legal implications.
The mechanisms involved in brain injury are not yet fully understood, but they are surely related to inflammatory events, enzymatic activation of proteases, endonucleases and phospholipases, formation of free radicals, effect of excitotoxic amino acids, lipid peroxidation and neuronal apoptosis. Sequential primary, secondary and tertiary energy failures are responsible for the neurological damage [2]. However, there exists a “treatment window” (approximately six hours, according to studies based on animal models) during which a therapeutic intervention can be effective [3]. Among the current neonatal interventions, only moderate hypothermia has been shown to reduce mortality and long term neurological morbidity by reducing inflammatory phenomena and oxidative stress [4,5]. However, even today, despite this cooling therapy, many children continue developing serious neurological sequelae.
Among different molecules investigated, melatonin added to neonatal cooling treatment has obtained promising effects improving long-term neurodevelopmental results (‘hypothermia plus’ effect) [6,7,8,9,10]. This hormone, that readily cross the blood-brain barrier, regulates circadian rhythms and is also considered a highly effective anti-inflammatory, anti-apoptotic, anti-oxidant and free radical scavenger [8,11,12].
Cytokines and brain injury. Brain damage, excitotoxic events and cell death, separately and in combination, triggers neuroinflammation which results in increased extracellular levels of biomarkers. Inflammatory cytokines/chemokines act by binding cell surface receptors and contributing to the initiation, maintenance, and regulation of inflammatory immune responses. These mediators affect the newborn brain through a number of different mechanisms including (1) increasing permeability of blood–brain barrier via activation of vascular endothelial cells, (2) cellular transport across the vascular endothelium (3) recruitment of monocytes to the brain parenchyma, or (4) stimulation of afferent peripheral nerve fibers [13].
Due to the complex multifaceted nature of HIE, a wide range of serum biomarkers are involved in neurological damage pathophysiology. Neuronal glial fibrillary acidic protein (GFAP), circulating proinflammatory cytokines (IL-1, IL-2, IL-7 and IL-13) and granulocyte-macrophage colony-stimulating factor (GM-CSF)], are mechanistically associated in the pathogenesis of brain damage [14,15].
Glial fibrillary acidic protein (GFAP) is a brain-specific protein of astroglia cells, whose production is reactively triggered by acute or chronic adverse brain events. It reaches a serum peak after the first hour of brain insult and has a half-life of 48 h. Transported into the bloodstream through glymphatic drainage, it is a marker of neuronal apoptosis [16,17]. In neonates under hypothermia treatment due to HIE, elevated serum levels of GFAP and IL-1, among other biomarkers, at 6-24 h of life, were also associated with abnormal neurological outcomes [18].
Granulocyte-macrophage colony-stimulating factor (GM-CSF) is a growth factor with proinflammatory effects involved in neuronal hyperexcitability [22], alterations in mitochondrial function that determine neutrophil apoptosis [19], retinopathy, bronchopulmonary dysplasia and age-related memory loss [20,21]. In neonates with perinatal hypoxia, elevated serum levels of GM-CSF and IL-6 after birth are associated with moderate-severe HIE and increased risk of developing cerebral palsy [23].
Cytokines and Melatonin. The administration of melatonin is capable of alleviating the consequences of brain damage by reducing the concentration of proinflammatory cytokines, such as GFAP, IL-1, IL-2, IL-6, TNF-alpha or GM-CSF [24,25,26]. One of its protective effects occurs at the mitochondrial level, preventing calcium overload [19]. Additionally, the administration of melatonin favoured the down-regulation of IL-13[27].
In animal models of brain damage, through trauma or neurotoxins, melatonin addiction showed a decrease in GFAP expression in brain tissue, indicating a lower secondary activation of astroglia [28,29,30,31] and improving learning and memory [32].
Based on the above findings, our hypothesis is that melatonin administered to the asphyctic newborn could contribute to a lower inflammatory response, quantified by plasma biomarkers. We intend to determine whether this decrease in proinflammatory proteins and cytokines has an influence on long-term neurodevelopment.
We addressed two objectives: (1) To evaluate serum neuronal and inflammatory biomarkers in asphyctic newborns treated with hypothermia alone or hypothermia plus melatonin and (2) to determine if levels of these potential biomarkers correlate with abnormal neurodevelopmental outcomes at 6 and 18 months of age.
Material and Methods
Study design. The study was conducted in newborn infants at the Clínico San Cecilio and Virgen de las Nieves universitary hospitals in Granada (Spain) and at the Torrecárdenas hospital in Almería (Spain), after informed consent form were signed. The trial was approved by the Andalusian Regional Ethics Committee and by the corresponding Ethics Committee at each of the participating hospitals. In addition, the mandatory authorisation was obtained from the Spanish Agency for Medicines and Health Products (AEMPS). The study was performed according to the principles outlined by the Helsinki Declaration. Institutional ethics and administrative approvals were granted in 2016. The trial was registered on EudraCT No. 2012- 000184-24). The reporting of the study adhered to the CONSORT statement for pilot studies. An independent data monitoring committee was implemented to monitor the safety of this trial in a vulnerable population.
Patients. 25 newborns were recruited to the trial, between January 2015 and March 2016. All patients, that met international criteria for cooling therapy were randomised into two groups (Figure 1). 13 neonates were assigned to hypothermia+placebo group and 12 to hypothermia+melatonin group. The Pharmacy Unit at the participating hospitals was responsible for treatment randomisation. The intervention was masked to the investigator.
Inclusion criteria were the following:1) Gestational age ≥ 36 weeks; 2) Severe perinatal asphyxia; and 3) Moderate-severe HIE. Severe perinatal asphyxia was considered to be present if at least one of the following conditions was met: 1) Apgar test score ≤5 at five minutes after birth; 2) Need for resuscitation in the delivery room for more than 10 minutes by positive pressure ventilation (bag and mask or endotracheal tube); 3) pH ≤7.00 or base deficit ≤-16 mmol/L within first hour, according to blood gas analyses (cord, arterial, venous or capillary samples). Signs of moderate or severe encephalopathy were quantified by serial assessment using a modified Sarnat and Sarnat scale [33]. A score ≥6 was considered as moderate HIE and ≥13, as severe HIE. Newborns meeting one or more of the following criteria were excluded from the clinical trial: 1) Birth weight <1800 g; 2) Gestational age <36 weeks; 3) Surgical pathology within the first three days of life; 4) Serious congenital malformation located in the central nervous system; 5) Hypoxaemia (preductal oxygen saturation level <90%) with no response to invasive mechanical ventilation, full-oxygen supplement (FiO2=100%) and inhaled nitric oxide therapy; 6) Life-threatening coagulopathy refractory to replacement treatment (plasma and/or platelet transfusion); 7) Chromosomopathy; or 8) Postnatal age >6 hours.
Interventions. The patients in the treatment group received a daily intravenous dose of melatonin, 5 mg per kg of body weight, during the first three days of life. The melatonin, manufactured by Farma Mediterrania SL (Barcelona, Spain), was administered by continuous i.v. infusion for two hours, beginning during the first six hours after birth. The newborns assigned to the placebo group received the same volume of 0.9% normal saline solution, also administered by continuous i.v. infusion for two hours. Propylene glycol and macrogol were the main solvents used for the experimental group (melatonin concentration: 6,5 mg/mL).
The whole body hypothermia neonatal protocol was applied by experienced staff in the hospital’s neonatal intensive care units (NICUs) [34]. This standardised protocol includes a servo-controlled and transient decrease in body temperature to 33-34 ° C (monitored by rectal probe), followed by a subsequent progressive rewarming [35,36,37]. Cooling was achieved with a Tecotherm Neo automatic device (Tecotherm Neo, Inspiration Healthcare Ltd, Leicester, UK) and was maintained for 72 hours. The neonates were then re-warmed at 0.5 ºC per hour until normothermia was reached.
Measurements. 2 mL of blood was collected from each newborn at four different time points: at hospital admission (time zero), 24 hours (time 1), 72 hours (time 2) and within 7-10 days of day of life (time 3). Neuronal and inflammatory biomarkers were assessed in plasma samples, that were centrifuged at 2000 rpm for 15-20 minutes, aliquoted to subsamples and stored at -80 ºC. Immunoassay test was made at Scientific Instrumentation Center of the University of Granada.
Samples underwent enzyme-linked immunosorbent assay (ELISA) for GFAP (BioVendor Research and Diagnostic Product, Brno, Czech Republic), GM-CSF and cytokines (MILLIPLEX MAP Human Neurological Disorders Magnetic Bead Panel 3, Luminex, Texas, USA). All samples were assayed in duplicate with the average recorded. Blood samples were also collected to measure routine metabolic parameters, main plasma ion levels and biomarkers of renal, hepatic and haematological function and for coagulation tests.
Infant neurodevelopmental assessment at 6 and 18 months of age was carried out using Bayley Scales of Infant and Toddler Development-III [38]. Long-term Motor milestones were evaluated in two ways: 1) The Gross Motor Function Classification System (GFMCS) which evaluates gross motor skills and overall functional capacity [39,40] and 2) Tardieu scale (also takes into account manual activity and language) [41]. All these validated tests were applied by a psychologist (always the same person, blinded to the interventions) from our Paediatric Neurological Unit.
Statistical analysis. Serum biomarker concentrations resulted in very extreme values, so we have simplified them as median ± interquartile range (p75 - p25). Statistical significance analysis, in both study groups, of biomarker differences and their decrements was performed by Mann-Whitney u test. A multivariate analysis of covariance (MANCOVA) was used to test the statistical significance of the effect, adding as a confounder the variable “severity of HIE” (moderate or severe).
Taking into account the whole sample and independently of the treatment received, we made a comparison study between the decrease of biomarkers after admission (T2-T0 and T3-T0) and long-term neurodevelopment. Connection was performed using Spearman’s correlation coefficient and its significance test, based on a t-test. All differences were considered significant at p<0.05. All data were analysed using SPSS (Statistical Package for the Social Sciences, Chicago, IL, USA) version 20.
Results
Of the 25 newborns recruited initially, two (one in each group) died in the first month of life and another (in the placebo group) did not attend the reviews for neurodevelopmental assessment. Thus, a total of 22 patients (11 in each group) were followed up for 18 months. Of these, 15 were male and 10 were female. At admission, ten presented moderate HIE, and fifteen had severe HIE (Sarnat scale ≥13 points).
The characteristics of the patients are presented in Table 1. There were no significant differences between the groups in the following variables: weight and height at birth, gestational age, cord blood arterial pH, Apgar score at 1 and 5 minutes of life, hours of life on starting hypothermia treatment, severity of HIE, lowest pH in blood gas analyses, or length of stay in the NICU. Likewise, there were no differences between the two groups in terms of blood levels of the inflammatory proteins measured. Accordingly, the groups were considered to be homogeneous.
Table 2 shows the concentrations of the plasma biomarkers studied and their comparison (adjusted for severity of HIE) between the groups studied. In newborns who received melatonin there was an early decrease (first 24 hours) in plasma levels of GM-CSF (p= 0.01), IL-2 (p= 0.01) and IL-13 (p=0.01). The same occurs with GM-CSF concentrations at T2 (p=0.04), as well as IL-7 and IL-13 at T3 (p=0.01 and p= 0.04 respectively) with respect to placebo group.
Table 3 presents the variations in the serum biomarkers from admission to neonatal unit (T0) up to 72 h (T2) and after the first week of life (T3). In both groups, the trends of plasma levels in the first 72 h (T2-T0) and in the first week (T3-T0) are compared. There is a significant decrease in GM-CSF levels in the group treated with melatonin, when comparing birth to the first 72 hours of life (T2-T0). We did not find significant differences in the rest of plasma biomarkers studied.
Relationships between biomarkers and neurodevelopmental parameters (Bayley III scale; GMFCS and Tardieu motor scales) are shown in Table 4. We can observe that a decrease in plasma GM-CSF concentrations in the first 72 h correlates strongly and directly with a higher score on the cognitive scale at 18 months of age (Spearman correlation coefficient, rs=-0.682; p=0.01) (Figure 2). Regarding IL-13, we evidenced a significant inverse correlation between its trend over time and different ace parameters of the Bayley III test. Thus, the greater the plasma decrease, the better the neurodevelopment. In the first 3 days, its decrease correlates strongly with better scores on the language scale at 6 and 18 months (rs=-0.642; p=0.01 and rs=-0.593; p=0.03) and on the cognitive scale at 18 months (rs=-0.638; p=0.01). In cases with confirmed sustained IL-13 drop beyond the first week of life, we evidenced an improvement in language prognosis at 6 months (rs=-0.653; p=0.01) and in motor prognosis (GMFCS at 6 and 18 months) and Tardieu scale at 6 months. (rs=0.577; p=0.04 and rs=0.535; p=0.04 respectively for GMFCS and rs=0.678; p=0.01 in Tardieu scale). Likewise, IL-2 concentrations correlate with neurodevelopment, since its sustained decrease beyond one week (T3-T0) is associated with an improvement in motor skills at 6 months (Tardieu scale (rs=0.584; p=0.03). A better language score was also recognized in patients at 6 and 18 months, inversely to the early decrease (T2-T0) of IL-2 (rs=-0.578; p=0.02 and rs=-0.498; p=0.04) (Figure 3 and Figure 4). Finally, the correlation between IL-7 and gross motor development at 6 months of age is interesting. We have shown that it presents a direct and strong correspondence with lower severity on the Tardieu scale at 6 months (rs=0.728; p=0.01) when its levels keep decreasing beyond the first 7 days (Figure 5).
Discussion
The main objective of the present study is the comparative analysis of cytokine levels in asphyxiated neonates treated with melatonin or placebo. We have found that the serum concentration of three of the biomarkers analysed (IL-2, IL-13 and GM-CSF) show a significant and rapid reduction (24 hours after admission) after intravenous melatonin. However, this decrease is not long-lasting for all of them (more than 3-7 days).
In animal experiments, Bonilla et al. found no changes in IL-2 concentrations, but reached similar conclusions to us regarding GM-CSF levels. In both studies, after an acute proinflammatory event, melatonin seems to achieve a somewhat more sustained decrease in plasma GM-CSF levels, lasting beyond the first 3 days of life [42]. Our results show that GM-CSF experiences the maximum decrease only in the melatonin-exposed group. However, we found no reduction in GM-CSF concentrations in the treated group beyond one week of life.
This rapid impact of melatonin on the aforementioned neuromarkers could mean a potent and rapid direct anti-inflammatory effect of melatonin, which, administered in the window period, would slow down the initial cascade of physiological events immediately after asphyxia. However, the “depletion” of melatonin’s effect over the course of days would mean that the dose or the duration of treatment required would need to be higher, in order to moderate secondary energy failure and achieve greater delayed immunomodulation.
The daily intravenous dose of melatonin we used was 5 mg per kg body weight, administered for 3 days, is considered safe, but could be insufficient. Although lower doses have been used in neonates, preclinical evidence estimates that therapeutic melatonin concentrations are reached with doses of 20-30 mg per kg body weight [43]. Both intravenous and oral administration has been shown to be effective in reducing oxidative stress and inflammatory markers in neonates with other pathologies [44,45]. Oral bioavailability of melatonin in critically ill neonates may, a priori, be questionable due to slowed gastric emptying, higher gastric pH and lower mesenteric arterial flow [46]. Melatonin given orally to preterm neonates results in a large plasma peak and a prolonged half-life (almost 12 hours), much longer than that demonstrated in adults. Its absorption kinetics appear to be non-saturable and therefore concentration-dependent. The high half-life in neonates may be explained by the limited hepatic biotransformation capacity and renal immaturity, so that lower doses can also sustain effective plasma levels [47,48]. However, we believe that administration every 12-24 hours is still necessary to achieve a longer-lasting anti-inflammatory and antioxidant action (the later, not measured here). It is also more useful to maintain the treatment throughout the first week of life, even adapting the doses to the time of day and even to the circadian periodicity.
Clinical trials in human neonates with perinatal asphyxia are very scarce and have a small sample size. In two of them, treatment with hypothermia was supplemented with oral administration of melatonin, at a dose of 10 mg per kg body weight, for 5 days. The authors demonstrate a decrease in oxidative stress and S100B, as a marker of glial damage [49,50]. In the other clinical trial, Ahmad et al. reported a decrease in neonatal mortality after a single oral administration of 10 mg, although none of the enrolled infants underwent simultaneous therapeutic cooling [51].
Dikmen et al. demonstrated that the electrical and microglial damage patterns induced by a 3-day ex vivo exposure to GM-CSF cause severe alterations in long-term cognitive development [22]. Our work is consistent with this pathophysiological hypothesis, already recognised in rats, showing that a greater decrease in GM-CSF in the first 3 days correlates strongly with an improvement in cognitive score at 18 months on the Bayley scale [10].
Regarding GFAP, we have found no differences in serum levels, comparing both treatment groups, nor a relationship between these and long-term motor, cognitive or language abilities. These finding are similar to that found by Zaigham et al, with no correlation in its concentrations in the umbilical cord between controls and asphyxiated newborns, nor with the severity or prognosis of perinatal HIE [52].
We have observed a significant and sustained decrease in serum IL-13 levels in neonates treated with melatonin, in the first 24 hours of life and is maintained after the first week. In addition, long-term neurodevelopment improves directly correlates to the serum decrease maintained over time. The role of IL-13 in brain damage is still unclear and the interpretation of its plasma levels is controversial, since recent animal experimentation attributes to this cytokine: anti-inflammatory and neuroprotective effects [53,54], reactivation of neuronal pyroptosis and increased neurological deficits in models of cerebral hemorrhage [55,56]. In a recent clinical trial in asphyxiated human neonates, Massaro et al. observed that an early plasma increase (24 hours) of cytokines such as IL-1 and IL-13 was related to greater brain injury as seen on magnetic resonance imaging. However, they found no relationship between neurodevelopment at one year of life and serum levels of these two biomarkers at 5 days after birth [57]. In our analysis, the most significant decreases in IL-7 and IL-13 correlated with improvements in the motor domain (GMFCS and Tardieu scale) both at 6 and 18 months of life, and this decrease was independent of the treatment received (hypothermia with/without melatonin).
An increase of the important proinflammatory IL-7, IL-7 in umbilical cord samples showed correlations with an increased risk of retinopathy of prematurity and with internalizing neurological disorders (increased incidence of anxiety-depression, depression) in adults [58,59,60].
Our data shows, that low levels of IL-7 and IL-13 in the first 72 hours (T2-T0) result in better cognitive and language development. These results are in agreement with those of Jenkins et al. who found a better neurological prognosis in neonates with very early (before 36 hours) decreases in IL-6, IL-8 and IL-10 [61], although , in our recruited neonates, when the serum decrease of IL-7 and IL-13 is prolonged until one week of life (T3-T0), the correlation appears mainly associated with an improvement in motor development. To our knowledge, there are no studies that have found that early alteration of inflammatory biomarkers is related to intellectual or language prognosis and later declines are related to motor development.
With respect to serum IL-2 concentrations, its down-modulation is shown, in our clinical trial, to be linked to improvement in both the cognitive and motor spheres in the long term. In a small study of 36 neonates, baseline serum elevation of IL-2 and IL-13, among others, was associated with adverse neurological prognosis, but without correlation with concentrations beyond day 1 [62].
To our knowledge, Juul et al conducted the largest multicentre study, which included quantification of cytokines. The authors conclude that no link can be established between serum concentrations of the interleukins analysed and neurodevelopment at two years of age, except for IL-6 at birth and IL-8 at day 4, with a very modest effect. [63]. However, other authors have indicated that alterations in inflammatory biomarkers, such as GM-CSF, persist even at school age in children with neurodevelopmental disorders with a history of perinatal hypoxic-ischemic encephalopathy [64]. In addition, Prasad [65] argues, inhibition of specific human cytokines, such as IL-1, could lead to a reduction in perinatal brain damage.
In human preterm-born infants with evidence of brain injury, elevated concentrations of proinflammatory cytokines (e.g., TNF-α, IL-1β, IL-2, and IL-17) were reported [66,67]. Numerous reports based on very preterm infants have demonstrated the association of elevated proinflammatory cytokines in the cord blood or cerebrospinal fluid with brain injury and adverse neurodevelopmental outcomes. Furthermore, in vitro studies have shown that TNF-alpha and IL-1B can induce neuronal cell death, as well as impair oligodendrocyte and neuronal development [68,69]. Recurrent or persistent elevations of IL-6, IL-1, IL-8, and TNF-a in the first 2-3 weeks of life may be predictors of white matter injury, microcephaly, attention problems and others neurodevelopmental impairment [67,70,71]. Particularly, IL-1B is associated with brain damage and worse neurological prognosis at the cognitive and motor levels in preterm infants. [72]. The greater the brain damage and white matter involvement in extreme preterm infants, the more intense and sustained the elevation of serum IL-1B [73]
In perinatal clinical practice, it’s important to realize clinical trials to evaluate any substance with an anti-inflammatory and neuroprotective effect. Melatonin is a ubiquitous molecule, highly conserved throughout evolution and practically free of side effects, even at very high doses, to the extent that the lethal dose 50 (LD-50) has not been found in animal experiments. Further studies are needed to understand mechanisms of action and effective doses and plasma levels at this very early stage of neurodevelopment. Preclinical studies in humans are needed to systematically address this pathology and, in particular, to include the optimal timing of administration (therapeutic window) to avoid irreversible neurological damage.
Animal models demonstrate that melatonin should be administered as soon as possible after the hypoxic-ischaemic event to achieve effective therapeutic levels [74]. Given that melatonin readily crosses the placental barrier, the relevance of its prenatal administration is being investigated in cases where there is evidence of a high risk of perinatal asphyxia. The inflammatory state induced by lipopolysaccharide inoculation to pregnant rats, was reduced by prenatal melatonin which were associated with decreased placental cytokine concentration and a reduced risk of prematurity. This anti-inflammatory protection by melatonin extends to the immediate postnatal period, with decreased inflammatory biomarkers, less brain damage and better neurodevelopment [75].
In the long-term neurological follow-up (6 and 18 months of age) we have found that improved intellectual and/or motor abilities are associated with an early decrease in most of the biomarkers studied. Specifically, we have evidenced this with blood levels of GM-CSF, IL-1, IL-2, IL-7 and IL-13, a result in agreement with most of the literature, both in humans and in experimental animals.
Since the neonatal hypoxic ischemic encephalopathy has a prevalence of about 1 in every 1,000 births in resource-rich countries, and continues to be as a leading cause of neonatal death and long-term neurologic disability in children, we urgently need more multicentric, well designed clinical trials. We consider it essential that medical research verify the antioxidant and anti-inflammatory effect of intravenous melatonin associated with therapeutic hypothermia and that, at the same time, its safety, the effective therapeutic dose and its pharmacokinetic profile are precisely defined. It will be necessary to overcome all kinds of difficulties (technical, financial, legal, recruitment, etc.) to reach sufficient scientific evidence that can help improve the prognosis of newborns with severe asphyxia. Another aspect to take into account in our recruited neonates is the apparent higher severity of HIE (although not significant) in the placebo group versus the experimental group. To avoid this potential bias, we have adjusted for severity of HIE in the statistical comparisons of biomarkers. Our clinical trial includes a small number of participants, so the results are merely illustrative of the feasibility and safety of melatonin use in neonates. Although there is overwhelming preclinical evidence for the neuroprotective effects of melatonin, very few human trials, although promising, have been conducted in humans [76]. We support that melatonin is a safe and potentially effective treatment to treat perinatal hypoxic-ischaemic encephalopathy.
Conclussions
Our study demonstrates that plasma concentrations of GM-CSF, IL-2, IL-7, and IL-13 are downwardly modified when intravenous melatonin is added to hypothermia treatment in asphyxiated neonates. The greatest decrease with respect to the levels measured at admission was found on the third day for GM-CSF in the treated neonates, compared to placebo. Therefore, we believe that the addition of melatonin could achieve an immediate anti-inflammatory effect by reducing the plasma levels of some proinflammatory markers in newborns with HIE, associated with improved intellectual and/or motor abilities in the long-term follow-up.
Author Contributions
A.J.C. and A.M.C. designed the study. A.J.C., F.C.C., J.A.H.S. and M.F.M.G. undertook the experimental work. H.A. performed the statistical análisis; A.B.F. participated in the neurological follow-up. A.J.C., F.C.C. and A.M.C. wrote the paper, which was edited and approved by all co-authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research project was obtained in a public and competitive call for grant applications, financed through the national programme (Spanish Ministry of Health): Call for Grants for Independent Clinical Research, 2011. Reference Number EC11-222.
Institutional Review Board Statement
The clinical trial was conducted in accordance with the ethical principles set out in the World Medical Association Declaration of Helsinki. The trial was approved by the Andalusian Regional Ethics Committee and by the corresponding Ethics Committee at each of the participating hospitals.
Informed Consent Statement
All parents gave their written informed consent to enrol their newborns
Acknowledgments
Special thanks to all the healthcare professionals caring for neonates in the neonatal intensive care units of the hospitals participating in this clinical trial.
Conflicts of Interest
The authors declare no conflict of interest.
References
- M. E. Dilenge, A. Majnemer, and M. I. Shevell, “Long-term developmental outcome of asphyxiated term neonates.,” J Child Neurol, vol. 16, no. 11, pp. 781–92, Nov. 2001. [CrossRef]
- B. Fleiss and P. Gressens, “Tertiary mechanisms of brain damage: a new hope for treatment of cerebral palsy?,” Lancet Neurol, vol. 11, no. 6, pp. 556–66, Jun. 2012. [CrossRef]
- W. A. Pulsinelli, M. Jacewicz, D. E. Levy, C. K. Petito, and F. Plum, “Ischemic brain injury and the therapeutic window.,” Ann N Y Acad Sci, vol. 835, pp. 187–93, Dec. 1997. [CrossRef]
- S. Perrone et al., “Whole body hypothermia and oxidative stress in babies with hypoxic-ischemic brain injury.,” Pediatr Neurol, vol. 43, no. 4, pp. 236–40, Oct. 2010. [CrossRef]
- E. Ramos et al., “Ischemic brain injury: New insights on the protective role of melatonin.,” Free Radic Biol Med, vol. 104, pp. 32–53, Mar. 2017. [CrossRef]
- J. Nair and V. H. S. Kumar, “Current and Emerging Therapies in the Management of Hypoxic Ischemic Encephalopathy in Neonates.,” Children (Basel), vol. 5, no. 7, Jul. 2018. [CrossRef]
- K. Martinello, A. R. Hart, S. Yap, S. Mitra, and N. J. Robertson, “Management and investigation of neonatal encephalopathy: 2017 update.,” Arch Dis Child Fetal Neonatal Ed, vol. 102, no. 4, pp. F346–F358, Jul. 2017. [CrossRef]
- R. Reiter, L. Tang, J. J. Garcia, and A. Muñoz-Hoyos, “Pharmacological actions of melatonin in oxygen radical pathophysiology.,” Life Sci, vol. 60, no. 25, pp. 2255–71, 1997. [CrossRef]
- A. Muñoz-Hoyos et al., “Melatonin’s role as an anticonvulsant and neuronal protector: experimental and clinical evidence.,” J Child Neurol, vol. 13, no. 10, pp. 501–9, Oct. 1998. [CrossRef]
- A. Jerez-Calero. et al., “Hypothermia Plus Melatonin in Asphyctic Newborns: A Randomized-Controlled Pilot Study.,” Pediatr Crit Care Med, vol. 21, no. 7, pp. 647–655, Jul. 2020. [CrossRef]
- D. Acuña-Castroviejo et al., “Melatonin, mitochondria, and cellular bioenergetics.,” J Pineal Res, vol. 30, no. 2, pp. 65–74, Mar. 2001. [CrossRef]
- M. Chahbouni et al., “Melatonin Treatment Reduces Oxidative Damage and Normalizes Plasma Pro-Inflammatory Cytokines in Patients Suffering from Charcot-Marie-Tooth Neuropathy: A Pilot Study in Three Children.,” Molecules, vol. 22, no. 10, Oct. 2017. [CrossRef]
- L. Capuron and A. H. Miller, “Immune system to brain signaling: neuropsychopharmacological implications.,” Pharmacol Ther, vol. 130, no. 2, pp. 226–38, May 2011. [CrossRef]
- A. Foster-Barber, B. Dickens, and D. M. Ferriero, “Human perinatal asphyxia: correlation of neonatal cytokines with MRI and outcome.,” Dev Neurosci, vol. 23, no. 3, pp. 213–8, 2001. [CrossRef]
- H. Hagberg et al., “Enhanced expression of interleukin (IL)-1 and IL-6 messenger RNA and bioactive protein after hypoxia-ischemia in neonatal rats.,” Pediatr Res, vol. 40, no. 4, pp. 603–9, Oct. 1996. [CrossRef]
- J. Middeldorp and E. M. Hol, “GFAP in health and disease.,” Prog Neurobiol, vol. 93, no. 3, pp. 421–43, Mar. 2011. [CrossRef]
- L. Papa et al., “Evaluation of Glial and Neuronal Blood Biomarkers Compared With Clinical Decision Rules in Assessing the Need for Computed Tomography in Patients With Mild Traumatic Brain Injury.,” JAMA Netw Open, vol. 5, no. 3, p. e221302, Mar. 2022. [CrossRef]
- L. F. Chalak, P. J. Sánchez, B. Adams-Huet, A. R. Laptook, R. J. Heyne, and C. R. Rosenfeld, “Biomarkers for Severity of Neonatal Hypoxic-Ischemic Encephalopathy and Outcomes in Newborns Receiving Hypothermia Therapy,” J Pediatr, vol. 164, no. 3, pp. 468-474.e1, Mar. 2014. [CrossRef]
- J. Espino et al., “Melatonin is able to delay endoplasmic reticulum stress-induced apoptosis in leukocytes from elderly humans.,” Age (Dordr), vol. 33, no. 4, pp. 497–507, Dec. 2011. [CrossRef]
- L. C. Wickramasinghe et al., “Granulocyte Colony-Stimulating Factor is a Determinant of Severe Bronchopulmonary Dysplasia and Coincident Retinopathy.,” Am J Pathol, vol. 193, no. 12, pp. 2001–2016, Dec. 2023. [CrossRef]
- R. B. Scheinert, A. Asokan, A. Rani, A. Kumar, T. C. Foster, and B. K. Ormerod, “Some hormone, cytokine and chemokine levels that change across lifespan vary by cognitive status in male Fischer 344 rats.,” Brain Behav Immun, vol. 49, pp. 216–32, Oct. 2015. [CrossRef]
- H. O. Dikmen, M. Hemmerich, A. Lewen, J.-O. Hollnagel, B. Chausse, and O. Kann, “GM-CSF induces noninflammatory proliferation of microglia and disturbs electrical neuronal network rhythms in situ.,” J Neuroinflammation, vol. 17, no. 1, p. 235, Aug. 2020. [CrossRef]
- H. Go et al., “Serum cytokine profiling in neonates with hypoxic ischemic encephalopathy.,” J Neonatal Perinatal Med, vol. 14, no. 2, pp. 177–182, 2021. [CrossRef]
- S. D. Paredes et al., “Melatonin Counteracts at a Transcriptional Level the Inflammatory and Apoptotic Response Secondary to Ischemic Brain Injury Induced by Middle Cerebral Artery Blockade in Aging Rats.,” Biores Open Access, vol. 4, no. 1, pp. 407–16, 2015. [CrossRef]
- F. Dehghan et al., “Does the administration of melatonin during post-traumatic brain injury affect cytokine levels?,” Inflammopharmacology, vol. 26, no. 4, pp. 1017–1023, Aug. 2018. [CrossRef]
- M. A. El-Missiry, S. Shabana, S. J. Ghazala, A. I. Othman, and M. E. Amer, “Melatonin exerts a neuroprotective effect against γ-radiation-induced brain injury in the rat through the modulation of neurotransmitters, inflammatory cytokines, oxidative stress, and apoptosis.,” Environ Sci Pollut Res Int, vol. 28, no. 24, pp. 31108–31121, Jun. 2021. [CrossRef]
- L. -L. Zhou, W. Wei, J.-F. Si, and D.-P. Yuan, “Regulatory effect of melatonin on cytokine disturbances in the pristane-induced lupus mice.,” Mediators Inflamm, vol. 2010, 2010. [CrossRef]
- A. Babaee et al., “Melatonin treatment reduces astrogliosis and apoptosis in rats with traumatic brain injury.,” Iran J Basic Med Sci, vol. 18, no. 9, pp. 867–72, Sep. 2015.
- I. Labunets, A. Rodnichenko, S. Savosko, and T. Pivneva, “Reaction of different cell types of the brain on neurotoxin cuprizone and hormone melatonin treatment in young and aging mice.,” Front Cell Neurosci, vol. 17, p. 113 1130, 2023. [Google Scholar] [CrossRef]
- G. Baydas, M. Ozer, A. Yasar, S. T. Koz, and M. Tuzcu, “Melatonin prevents oxidative stress and inhibits reactive gliosis induced by hyperhomocysteinemia in rats.,” Biochemistry (Mosc), vol. 71 Suppl 1, pp. S91-5, 2006. [CrossRef]
- A. Babaee, S. H. E. Vaghefi, S. Dehghani Soltani, M. Asadi Shekaari, N. Shahrokhi, and M. Basiri, “Hippocampal Astrocyte Response to Melatonin Following Neural Damage Induction in Rats.,” Basic Clin Neurosci, vol. 12, no. 2, pp. 177–186, 2021. [CrossRef]
- A. Albazal, A.-A. Delshad, and M. Roghani, “Melatonin reverses cognitive deficits in streptozotocin-induced type 1 diabetes in the rat through attenuation of oxidative stress and inflammation.,” J Chem Neuroanat, vol. 112, p. 101902, Mar. 2021. [Google Scholar] [CrossRef]
- et al. A. Garcia-Alix, et al. “Development, Reliability, and Testing of a New Rating Scale for Neonatal Encephalopathy.,” J Pediatr, vol. 235, pp. 83-91.e7, Aug. 2021. [Google Scholar] [CrossRef]
- P. S. Shah, “Hypothermia: a systematic review and meta-analysis of clinical trials.,” Semin Fetal Neonatal Med, vol. 15, no. 5, pp. 238–46, Oct. 2010. [CrossRef]
- A. D. Edwards et al., “Neurological outcomes at 18 months of age after moderate hypothermia for perinatal hypoxic ischaemic encephalopathy: synthesis and meta-analysis of trial data.,” BMJ, vol. 340, p. c363, Feb. 2010. [CrossRef]
- S. E. Jacobs, M. Berg, R. Hunt, W. O. Tarnow-Mordi, T. E. Inder, and P. G. Davis, “Cooling for newborns with hypoxic ischaemic encephalopathy.,” Cochrane Database Syst Rev, vol. 2013, no. 1, p. CD003311, Jan. 2013. [CrossRef]
- E. Shepherd et al., “Neonatal interventions for preventing cerebral palsy: an overview of Cochrane Systematic Reviews.,” Cochrane Database Syst Rev, vol. 6, no. 6, p. CD012409, Jun. 2018. [CrossRef]
- C. A. Albers and A. J. Grieve, “Test Review: Bayley, N. (2006). Bayley Scales of Infant and Toddler Development– Third Edition. San Antonio, TX: Harcourt Assessment,” J Psychoeduc Assess, vol. 25, no. 2, pp. 180–190, Jun. 2007. [CrossRef]
- R. Palisano, P. Rosenbaum, S. Walter, D. Russell, E. Wood, and B. Galuppi, “Development and reliability of a system to classify gross motor function in children with cerebral palsy.,” Dev Med Child Neurol, vol. 39, no. 4, pp. 214–23, Apr. 1997. [CrossRef]
- M. Voorman, A. J. Dallmeijer, D. L. Knol, G. J. Lankhorst, and J. G. Becher, “Prospective longitudinal study of gross motor function in children with cerebral palsy.,” Arch Phys Med Rehabil, vol. 88, no. 7, pp. 871–6, Jul. 2007. [CrossRef]
- Tardieu, G. , Le dossier clinique de l’infirmité motrice cérébrale. Méthodes d’Évaluation et Applications Thérapeutiques., Third. Paris, 1984.
- E. Bonilla et al., “Melatonin prolongs survival of immunodepressed mice infected with the Venezuelan equine encephalomyelitis virus.,” Trans R Soc Trop Med Hyg, vol. 95, no. 2, pp. 207–10, 2001. [CrossRef]
- S. Victor, E. Rocha-Ferreira, A. Rahim, H. Hagberg, and D. Edwards, “New possibilities for neuroprotection in neonatal hypoxic-ischemic encephalopathy.,” Eur J Pediatr, vol. 181, no. 3, pp. 875–887, Mar. 2022. [CrossRef]
- E. Gitto et al., “Melatonin reduces oxidative stress in surgical neonates.,” J Pediatr Surg, vol. 39, no. 2, pp. 184–9; discussion 184-9, Feb. 2004. [CrossRef]
- E. Gitto et al., “Oxidative and inflammatory parameters in respiratory distress syndrome of preterm newborns: beneficial effects of melatonin.,” Am J Perinatol, vol. 21, no. 4, pp. 209–16, May 2004. [CrossRef]
- M. Korf, L. D. McCullough, and V. Caretti, “A narrative review on treatment strategies for neonatal hypoxic ischemic encephalopathy.,” Transl Pediatr, vol. 12, no. 8, pp. 1552–1571, Aug. 2023. [CrossRef]
- S. Carloni et al., “Melatonin Pharmacokinetics Following Oral Administration in Preterm Neonates.,” Molecules, vol. 22, no. 12, Dec. 2017. [CrossRef]
- N. M. Merchant et al., “Pharmacokinetics of melatonin in preterm infants.,” Br J Clin Pharmacol, vol. 76, no. 5, pp. 725–33, Nov. 2013. [CrossRef]
- M. S. El Farargy and N. A. Soliman, “A randomized controlled trial on the use of magnesium sulfate and melatonin in neonatal hypoxic ischemic encephalopathy.,” J Neonatal Perinatal Med, vol. 12, no. 4, pp. 379–384, 2019. [CrossRef]
- H. Aly et al., “Melatonin use for neuroprotection in perinatal asphyxia: a randomized controlled pilot study.,” J Perinatol, vol. 35, no. 3, pp. 186–91, Mar. 2015. [CrossRef]
- Q. M. Ahmad, A. L. Chishti, and N. Waseem, “Role of melatonin in management of hypoxic ischaemic encephalopathy in newborns: A randomized control trial.,” J Pak Med Assoc, vol. 68, no. 8, pp. 1233–1237, Aug. 2018.
- M. Zaigham, F. Lundberg, R. Hayes, J. Undén, and P. Olofsson, “Umbilical cord blood concentrations of ubiquitin carboxy-terminal hydrolase L1 (UCH-L1) and glial fibrillary acidic protein (GFAP) in neonates developing hypoxic-ischemic encephalopathy.,” J Matern Fetal Neonatal Med, vol. 29, no. 11, pp. 1822–8, 2016. [CrossRef]
- D. Chen et al., “Interleukin 13 promotes long-term recovery after ischemic stroke by inhibiting the activation of STAT3.,” J Neuroinflammation, vol. 19, no. 1, p. 112, May 2022. [CrossRef]
- J. Van Broeckhoven et al., “Macrophage-based delivery of interleukin-13 improves functional and histopathological outcomes following spinal cord injury.,” J Neuroinflammation, vol. 19, no. 1, p. 102, Apr. 2022. [CrossRef]
- Y. Yan et al., “Interleukin-13 Affects the Recovery Processes in a Mouse Model of Hemorrhagic Stroke with Bilateral Tibial Fracture.,” Mol Neurobiol, vol. 59, no. 5, pp. 3040–3051, May 2022. [CrossRef]
- G. Chen et al., “Inhibiting ER Stress Weakens Neuronal Pyroptosis in a Mouse Acute Hemorrhagic Stroke Model.,” Mol Neurobiol, vol. 57, no. 12, pp. 5324–5335, Dec. 2020. [CrossRef]
- A. N. Massaro et al., “Plasma Biomarkers of Brain Injury in Neonatal Hypoxic-Ischemic Encephalopathy.,” J Pediatr, vol. 194, pp. 67-75.e1, Mar. 2018. [CrossRef]
- N. M. Simon et al., “A detailed examination of cytokine abnormalities in Major Depressive Disorder.,” Eur Neuropsychopharmacol, vol. 18, no. 3, pp. 230–3, Mar. 2008. [CrossRef]
- C. Galera et al., “Cord Serum Cytokines at Birth and Children’s Anxiety-Depression Trajectories From 3 to 8 Years: The EDEN Mother-Child Cohort.,” Biol Psychiatry, vol. 89, no. 6, pp. 541–549, Mar. 2021. [CrossRef]
- H. Yu et al., “Serum concentrations of cytokines in infants with retinopathy of prematurity.,” APMIS, vol. 122, no. 9, pp. 818–23, Sep. 2014. [CrossRef]
- D. D. Jenkins et al., “Serum cytokines in a clinical trial of hypothermia for neonatal hypoxic-ischemic encephalopathy.,” J Cereb Blood Flow Metab, vol. 32, no. 10, pp. 1888–96, Oct. 2012. [CrossRef]
- J. E. Orrock et al., “Association of brain injury and neonatal cytokine response during therapeutic hypothermia in newborns with hypoxic-ischemic encephalopathy.,” Pediatr Res, vol. 79, no. 5, pp. 742–7, May 2016. [CrossRef]
- S. E. Juul et al., “Association of High-Dose Erythropoietin With Circulating Biomarkers and Neurodevelopmental Outcomes Among Neonates With Hypoxic Ischemic Encephalopathy: A Secondary Analysis of the HEAL Randomized Clinical Trial.,” JAMA Netw Open, vol. 6, no. 7, p. e2322131, Jul. 2023. [CrossRef]
- Z. Zareen et al., “Cytokine dysregulation persists in childhood post Neonatal Encephalopathy.,” BMC Neurol, vol. 20, no. 1, p. 115, Mar. 2020. [CrossRef]
- J. D. Prasad et al., “Anti-Inflammatory Therapies for Treatment of Inflammation-Related Preterm Brain Injury,” Int J Mol Sci, vol. 22, no. 8, p. 4008, Apr. 2021. [CrossRef]
- K. Sävman, M. K. Sävman, M. Blennow, H. Hagberg, E. Tarkowski, M. Thoresen, and A. Whitelaw, “Cytokine response in cerebrospinal fluid from preterm infants with posthaemorrhagic ventricular dilatation.,” Acta Paediatr, vol. 91, no. 12, pp. 1357–63, 2002. [CrossRef]
- A. Leviton et al., “The relationship between early concentrations of 25 blood proteins and cerebral white matter injury in preterm newborns: the ELGAN study.,” J Pediatr, vol. 158, no. 6, pp. 897-903.e1–5, Jun. 2011. [CrossRef]
- J. H. Gilmore, L. Fredrik Jarskog, S. Vadlamudi, and J. M. Lauder, “Prenatal infection and risk for schizophrenia: IL-1beta, IL-6, and TNFalpha inhibit cortical neuron dendrite development.,” Neuropsychopharmacology, vol. 29, no. 7, pp. 1221–9, Jul. 2004. [CrossRef]
- et al. N. Kuzumaki, et al. “Enhanced IL-1beta production in response to the activation of hippocampal glial cells impairs neurogenesis in aged mice.,” Synapse, vol. 64, no. 9, pp. 721–8, Sep. 2010. [Google Scholar] [CrossRef]
- T. M. O’Shea et al., “Elevated blood levels of inflammation-related proteins are associated with an attention problem at age 24 mo in extremely preterm infants.,” Pediatr Res, vol. 75, no. 6, pp. 781–7, Jun. 2014. [CrossRef]
- R. S. Procianoy and R. C. Silveira, “Association between high cytokine levels with white matter injury in preterm infants with sepsis.,” Pediatr Crit Care Med, vol. 13, no. 2, pp. 183–7, Mar. 2012. [CrossRef]
- M. D. Nist and R. H. Pickler, “An Integrative Review of Cytokine/Chemokine Predictors of Neurodevelopment in Preterm Infants.,” Biol Res Nurs, vol. 21, no. 4, pp. 366–376, Jul. 2019. [CrossRef]
- A. Leviton et al., “Systemic inflammation, intraventricular hemorrhage, and white matter injury.,” J Child Neurol, vol. 28, no. 12, pp. 1637–45, Dec. 2013. [CrossRef]
- N. J. Robertson et al., “Melatonin as an adjunct to therapeutic hypothermia in a piglet model of neonatal encephalopathy: A translational study.,” Neurobiol Dis, vol. 121, pp. 240–251, Jan. 2019. [CrossRef]
- J. Y. Lee et al., “Administration of melatonin for prevention of preterm birth and fetal brain injury associated with premature birth in a mouse model.,” Am J Reprod Immunol, vol. 82, no. 3, p. e13151, Sep. 2019. [CrossRef]
- J. Ahmed, A. K. Pullattayil S, N. J. Robertson, and K. More, “Melatonin for neuroprotection in neonatal encephalopathy: A systematic review & meta-analysis of clinical trials.,” Eur J Paediatr Neurol, vol. 31, pp. 38–45, Mar. 2021. [CrossRef]
Figure 1.
Flow Diagram of the study.
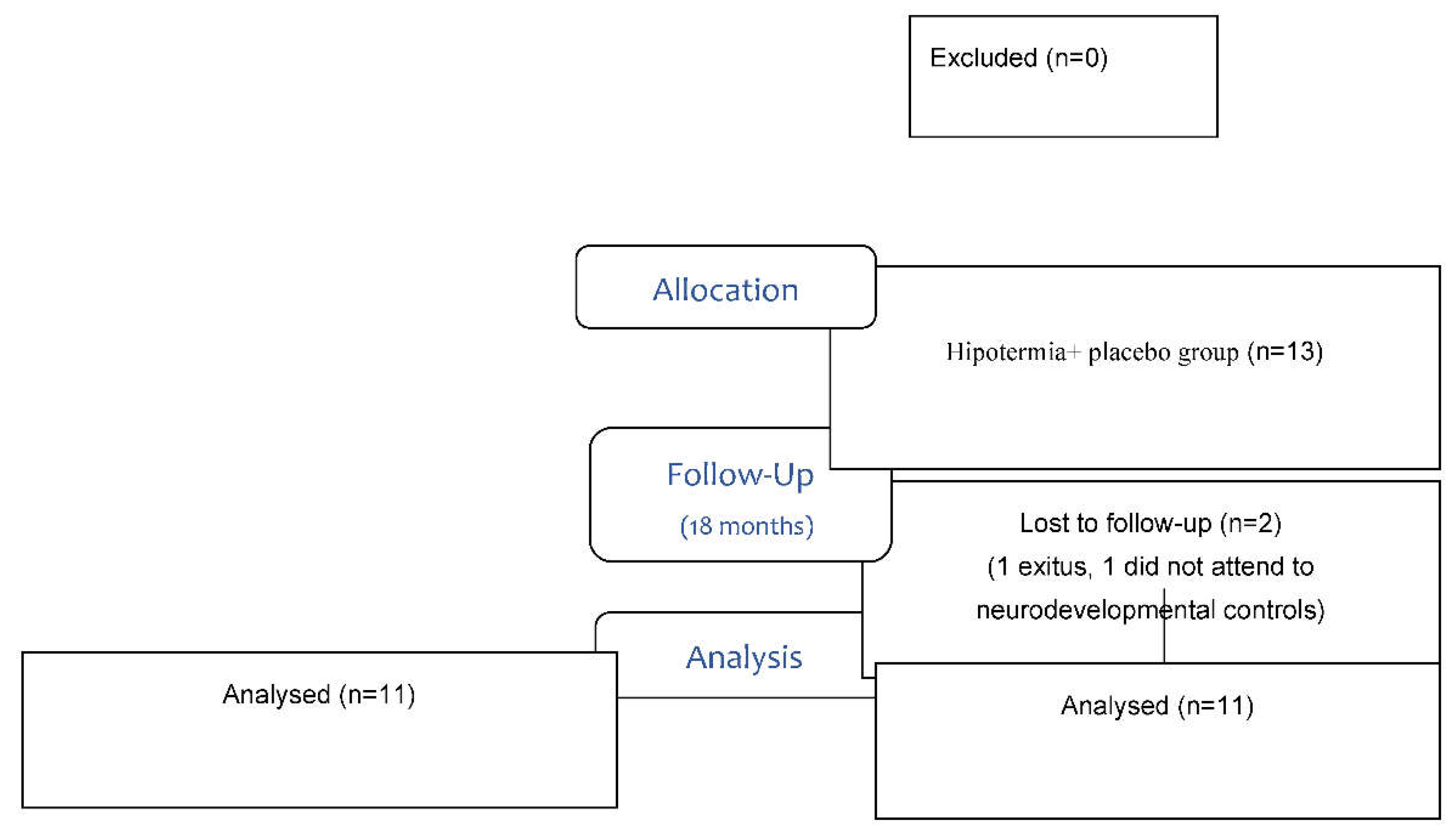
Figure 2.
Correlation between the decrease in serum GM-CSF level and the score on the Bayley III scale. GM-CSF= granulocyte-macrophage colony-stimulating factor; decT2-T0= decrease when comparing levels from T0 to T2 (values on logarithmic scale); Cog CS18 = Cognitive Composite Score at 18 month of age.
Figure 2.
Correlation between the decrease in serum GM-CSF level and the score on the Bayley III scale. GM-CSF= granulocyte-macrophage colony-stimulating factor; decT2-T0= decrease when comparing levels from T0 to T2 (values on logarithmic scale); Cog CS18 = Cognitive Composite Score at 18 month of age.
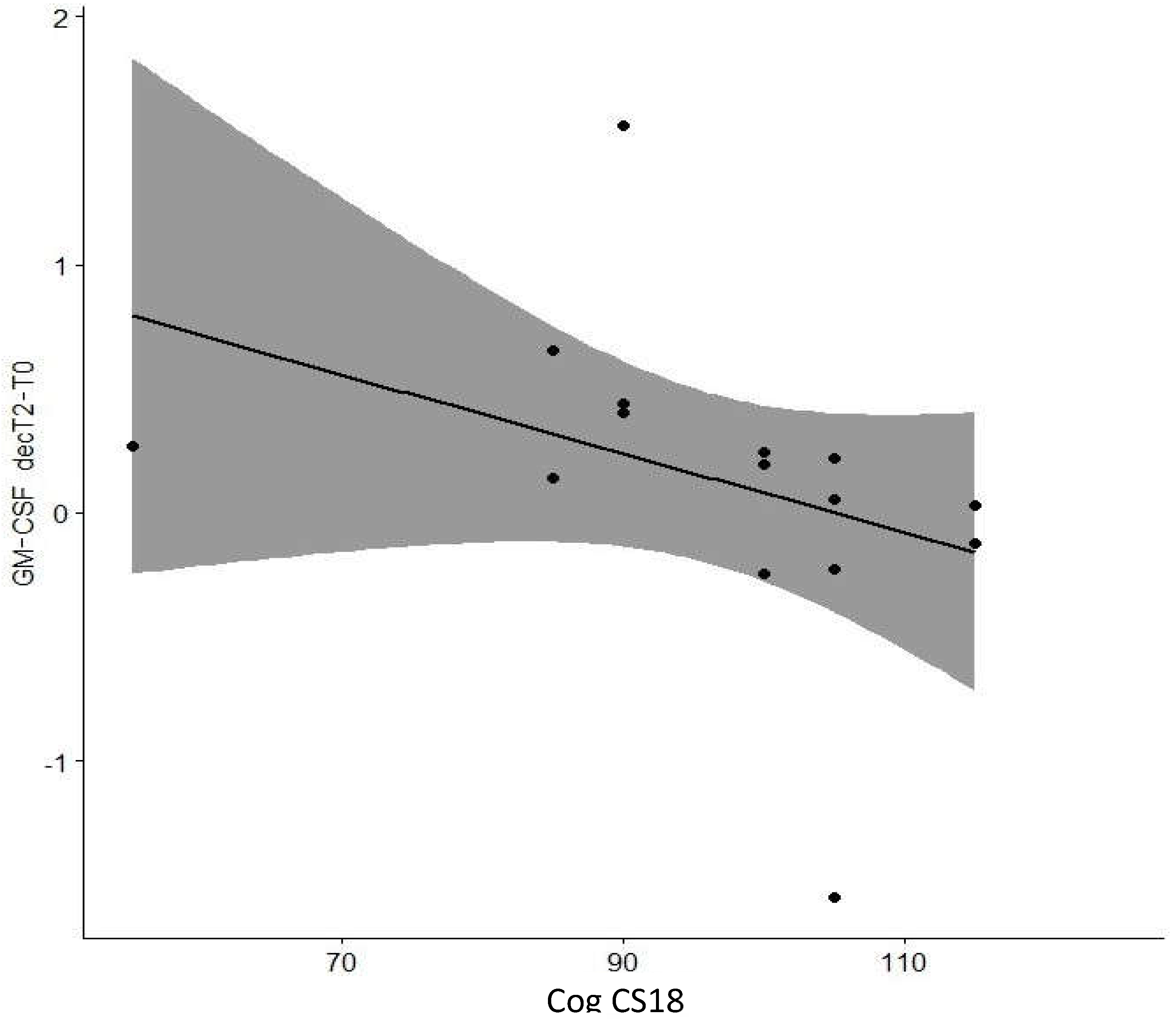
Figure 3.
Correlation between the decrease in serum IL-2 level and the score on the Bayley III scale. IL-2= interleukin 2; decT2-T0= decrease when comparing levels from T0 to T2 (values on logarithmic scale); L CS6 = Language Composite Score at 6 month of age.
Figure 3.
Correlation between the decrease in serum IL-2 level and the score on the Bayley III scale. IL-2= interleukin 2; decT2-T0= decrease when comparing levels from T0 to T2 (values on logarithmic scale); L CS6 = Language Composite Score at 6 month of age.
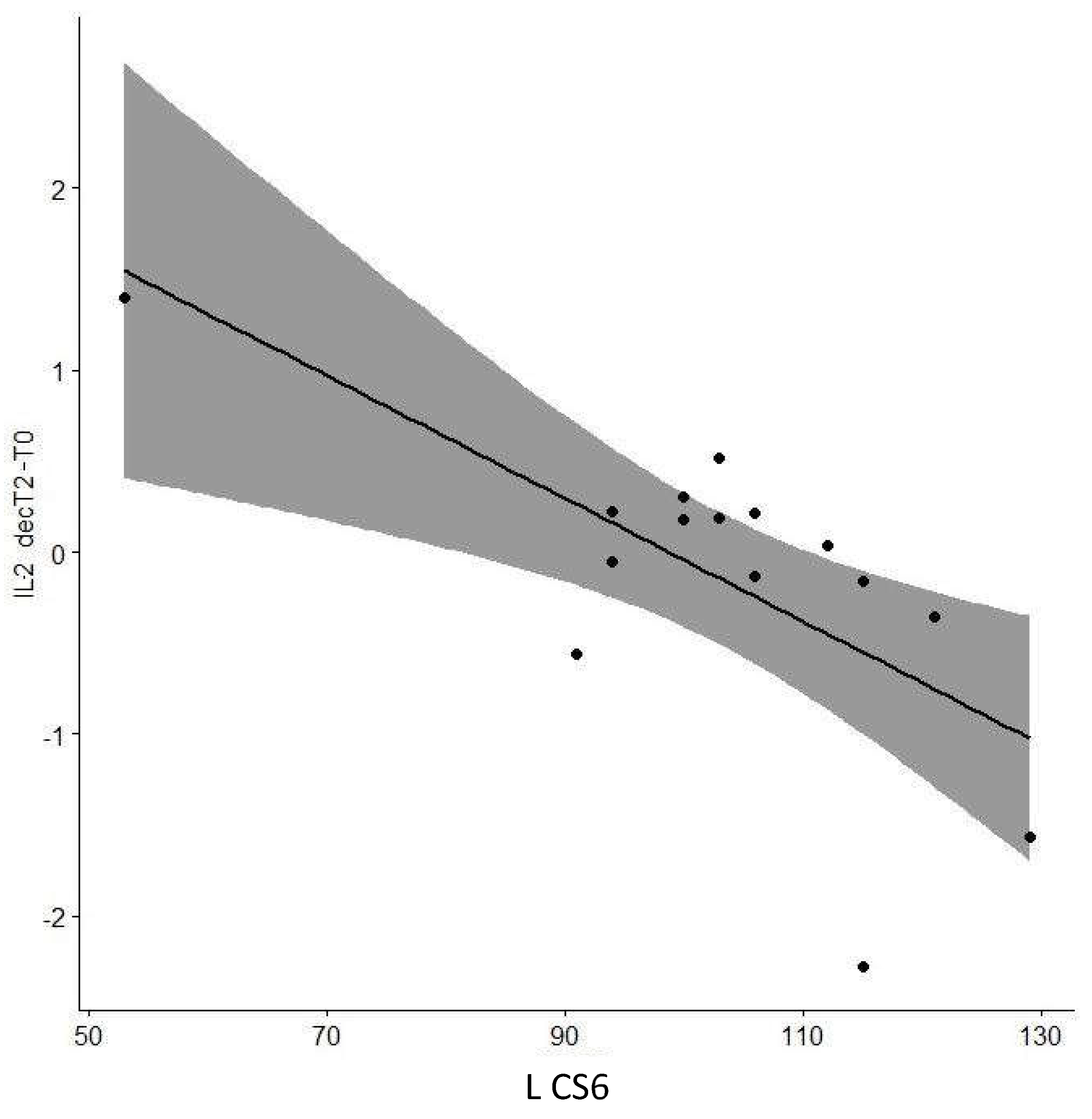
Figure 4.
Correlation between the decrease in serum IL-2 level and the score on the Bayley III scale. IL-2= interleukin 2; decT2-T0= decrease when comparing levels from T0 to T2 (values on logarithmic scale); L CS18 = Language Composite Score at 18 month of age.
Figure 4.
Correlation between the decrease in serum IL-2 level and the score on the Bayley III scale. IL-2= interleukin 2; decT2-T0= decrease when comparing levels from T0 to T2 (values on logarithmic scale); L CS18 = Language Composite Score at 18 month of age.
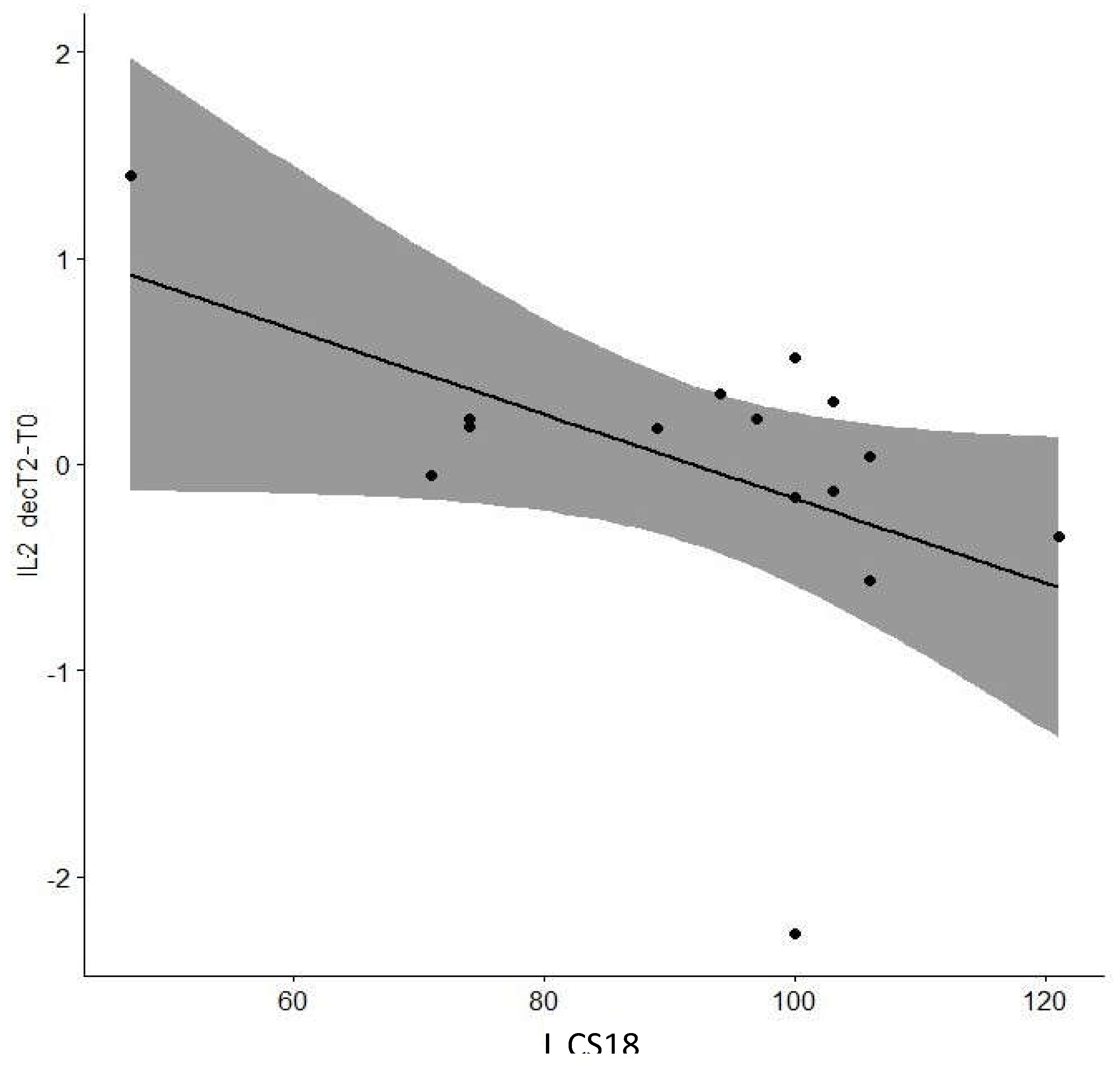
Figure 5.
Correlation between the decrease in serum IL-7 level and motor development. IL-7= interleukin 7; decT3-T0= decrease when comparing levels from T0 to T3 (values on logarithmic scale); Tardieu6= Tardieu Scale at 6 month of age.
Figure 5.
Correlation between the decrease in serum IL-7 level and motor development. IL-7= interleukin 7; decT3-T0= decrease when comparing levels from T0 to T3 (values on logarithmic scale); Tardieu6= Tardieu Scale at 6 month of age.
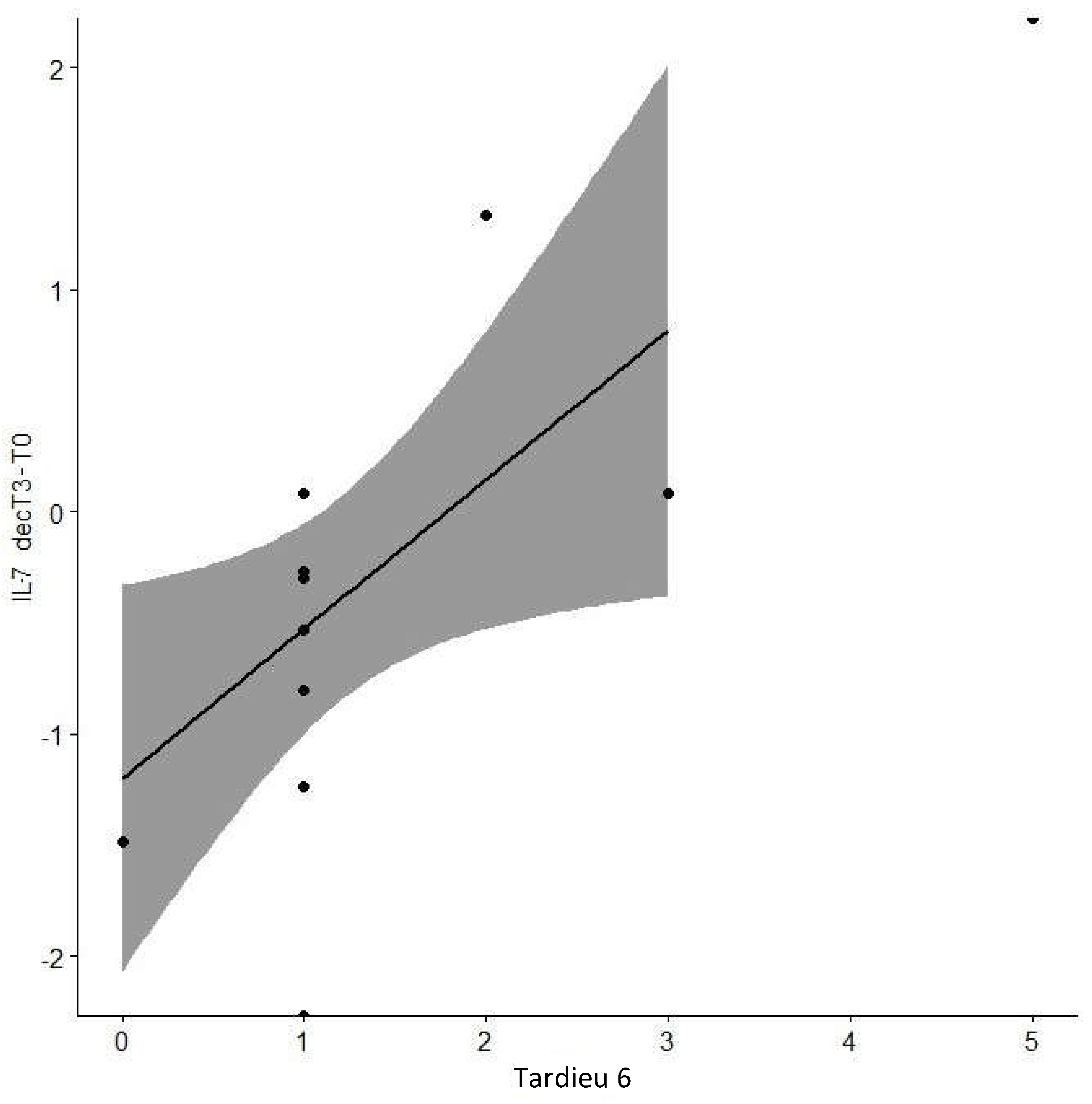

Table 1.
Clinical characteristics of the neonates.
| Clinical characteristics | Placebo Group (n = 13) (Mean ± SD) | Melatonin Group (n = 12) (Mean ± SD) | p |
|---|---|---|---|
| Birth weight (grams) | 2973 +/- 660 | 3.057+/-514 | 0.86 |
| Gestational age (weeks) | 39.45+/-1.72 | 38.49+/-1.71 | 0.22 |
| Height (centimeters) | 49.96+/-2.39 | 50.73+/-2.05 | 0.56 |
| pH cord blood | 6.96+/-0.14 | 6.98+/-0.15 | 0.63 |
| Apgar score at 1 minute of life | 3.77+/-2.52 | 3.55+/-2.46 | 0.69 |
| Apgar score at 5 minutes of life | 5.42+/-2.39 | 5.91+/-1.97 | 0.78 |
| Start hypothermia therapy from birth (hours) | 4.92+/-2.56 | 3.95+/-2.49 | 0.25 |
| Sarnat-Sarnat score | 20.69+/-10.67 | 12.72+/-7.57 | 0.09 |
| Lower blood pH at NICU admittance | 7.15+/-0.16 | 7.17 +/-0.13 | 0.31 |
| Arterial Pressure (mm Hg) | 48.42 +/-15.22 | 51.7+/-11.24 | 0.41 |
| Length of stay in the NICU (days) | 11.08+/-4.25 | 11.35+/-4.37 | 0.53 |
Both groups were subjected to therapeutic hypothermia. SD: standard deviation; p= p value less than 0.05 was considered significant.
Table 2.
Plasma biomarkers concentrations measured within the first week of life.
| Plasma biomarker | n | Placebo Group | Melatonin Group | n | p |
|---|---|---|---|---|---|
| GFAP T0 | 11 | 0.096 ± 0.015 | 0.118 ± 0.122 | 10 | 0.35 |
| GFAP T1 | 10 | 0.079 ± 0.07 | 0.036 ± 0.061 | 10 | 0.48 |
| GFAP T2 | 10 | 0.086 ± 0.095 | 0.061 ± 0.111 | 9 | 0.99 |
| GFAP T3 | 11 | 0.079 ± 0.057 | 0 ± 0.082 | 9 | 0.26 |
| GM-CSF T0 | 10 | 13.28 ± 4 | 14.77 ± 4.717 | 13 | 0.60 |
| GM-CSF T1 | 10 | 15.76 ± 11.25 | 11.77 ± 11.177 | 13 | 0.01* |
| GM-CSF T2 | 10 | 17.485 ± 8.008 | 12.275 ± 7.688 | 12 | 0.04* |
| GM-CSF T3 | 11 | 16.75 ± 6.057 | 12.78 ± 3.02 | 10 | 0.08 |
| IL1 T0 | 10 | 59.79 ± 86.88 | 32.52 ± 63.12 | 13 | 0.32 |
| IL1 T1 | 10 | 69.48 ± 108.53 | 13.28 ± 39.81 | 13 | 0.20 |
| IL1 T2 | 10 | 32.52 ± 64.455 | 36.93 ± 18.225 | 12 | 0.39 |
| IL1 T3 | 11 | 59.67 ± 32.55 | 29.9 ± 43.025 | 10 | 0.87 |
| IL2 T0 | 10 | 6.71 ± 2.46 | 6.245 ± 5.595 | 13 | 0.67 |
| IL2 T1 | 10 | 7.31 ± 5.5 | 5.27 ± 4.828 | 13 | 0.01* |
| IL2 T2 | 10 | 7.605 ± 4.608 | 5.44 ± 4.543 | 12 | 0.09 |
| IL2 T3 | 11 | 8.875 ± 3.643 | 6.09 ± 1.495 | 10 | 0.07 |
| IL7 T0 | 10 | 8.74 ± 9.61 | 11.14 ± 8.67 | 13 | 0.56 |
| IL7 T1 | 10 | 11.32 ± 14.61 | 6.635 ± 5.247 | 13 | 0.32 |
| IL7 T2 | 10 | 7.7 ± 16.438 | 7.12 ± 5.81 | 12 | 0.61 |
| IL7 T3 | 11 | 14.21 ± 11.213 | 4.95 ± 2.73 | 10 | 0.01* |
| IL13 T0 | 10 | 8.67 ± 5.47 | 8.24 ± 4.47 | 13 | 0.71 |
| IL13 T1 | 10 | 9.51 ± 7.99 | 6.015 ± 8.455 | 13 | 0.01* |
| IL13 T2 | 10 | 8.24 ± 5.037 | 7.37 ± 10.515 | 12 | 0.41 |
| IL13 T3 | 11 | 11.95 ± 3.663 | 7.81 ± 3.46 | 10 | 0.04* |
Both groups were subjected to therapeutic hypothermia. GFAP= Glial fibrillary acidic protein, GM-CSF= granulocyte-macrophage colony-stimulating factor, IL= Interleukin, T0= hospital admission, T1=24 hours of life, T2=72 hours of life, T3=7-10 days of age, n= number of subjects included. p= p value (adjusted by severity of HIE). * p < 0.05. Results expressed as median ±Interquartile range. GFAP and GM-CSF values are expressed as ng/mL. Interleukins values are expressed as pg/mL.
Table 3.
Trend of plasma inflammatory biomarkers from newborns admission.
| Plasma biomarker | n | Placebo Group | n | Melatonin Group | p |
|---|---|---|---|---|---|
| GFAP decT2-T0 | 9 | -0.01 ± 0.06 | 10 | -0.01 ± 0.05 | 0.32 |
| GFAP decT3-T0 | 9 | -0.02 ± 0.06 | 11 | -0.03 ± 0.14 | 0.16 |
| GM-CSF decT2-T0 | 12 | 3.71 ± 4.78 | 9 | -2.44 ± 4 | 0.02* |
| GM-CSF decT3-T0 | 10 | 0 ± 8.55 | 9 | -2.01 ± 8.48 | 0.12 |
| IL1 decT2-T0 | 12 | 0 ± 35.83 | 9 | 15.16 ± 62.87 | 0.45 |
| IL1 decT3-T0 | 10 | -23.37 ± 96.65 | 9 | 0 ± 35.22 | 0.91 |
| IL2 decT2-T0 | 12 | 0.76 ± 1.69 | 9 | -1.38 ± 3.65 | 0.19 |
| IL2 decT3-T0 | 10 | -0.15 ± 3.37 | 9 | -1.34 ± 6.62 | 0.31 |
| IL7 decT2-T0 | 12 | 0 ± 4.24 | 9 | -0.82 ± 4.37 | 0.36 |
| IL7 decT3-T0 | 10 | -0.41 ± 12.05 | 9 | -8.22 ± 7.03 | 0.09 |
| IL13 decT2-T0 | 12 | 0 ± 3.02 | 9 | -2.24 ± 6.03 | 0.21 |
| IL13 decT3-T0 | 10 | 0 ± 4.11 | 9 | -1.74 ± 2.32 | 0.10 |
Both groups were subjected to therapeutic hypothermia. Data are expressed as Interquartile range ± standard deviation. GFAP= Glial fibrillary acidic protein, GM-CSF= granulocyte-macrophage colony-stimulating factor, IL= Interleukin, T0= hospital admission, T2=72 hours of life, T3=7-10 days of age , decT2-T0= decrease when comparing levels from T0 to T2, decT3-T0= decrease when comparing levels from T0 to T3, n= number of subjects included. p= p value (adjusted by severity of HIE). p= p value (adjusted by severity of HIE). * p < 0.05.
Table 4.
Relationships between plasma biomarker decline and long-term neurodevelopment.
| Plasma biomarker | Neurodevelopment test | Spearman’s correlation coefficient | p |
|---|---|---|---|
| GFAP decT2-T0 | Cog CS6 | -0.052 | 0.85 |
| L CS6 | -0.089 | 0.75 | |
| Mot CS6 | 0.057 | 0.84 | |
| Cog CS18 | 0.255 | 0.36 | |
| L CS18 | 0.326 | 0.24 | |
| Mot CS18 | 0.009 | 0.97 | |
| GMFCS6 | -0.182 | 0.52 | |
| GMFCS18 | -0.014 | 0.96 | |
| Tardieu6 | 0.134 | 0.63 | |
| Tardieu18 | 0.023 | 0.93 | |
| GFAP decT3-T0 | Cog CS6 | -0.120 | 0.65 |
| L CS6 | -0.397 | 0.11 | |
| Mot CS6 | -0.424 | 0.09 | |
| Cog CS18 | -0.043 | 0.88 | |
| L CS18 | 0.201 | 0.47 | |
| Mot CS18 | -0.133 | 0.64 | |
| GMFCS6 | 0.243 | 0.38 | |
| GMFCS18 | 0.331 | 0.23 | |
| Tardieu6 | 0.359 | 0.19 | |
| Tardieu18 | 0.290 | 0.29 | |
| GM-CSF decT2-T0 | Cog CS6 | -0.047 | 0.87 |
| L CS6 | -0.257 | 0.36 | |
| Mot CS6 | 0.052 | 0.85 | |
| Cog CS18 | -0.682 | 0.01* | |
| L CS18 | -0.185 | 0.51 | |
| Mot CS18 | 0.014 | 0.99 | |
| GMFCS6 | 0.187 | 0.50 | |
| GMFCS18 | 0.214 | 0.44 | |
| Tardieu6 | 0.252 | 0.36 | |
| Tardieu18 | 0.235 | 0.40 | |
| GM-CSF decT3-T0 | Cog CS6 | 0.042 | 0.89 |
| L CS6 | -0.013 | 0.96 | |
| Mot CS6 | -0.091 | 0.76 | |
| Cog CS18 | -0.189 | 0.54 | |
| L CS18 | -0.194 | 0.52 | |
| Mot CS18 | -0.150 | 0.63 | |
| GMFCS6 | 0.289 | 0.34 | |
| GMFCS18 | 0.350 | 0.24 | |
| Tardieu6 | 0.524 | 0.07 | |
| Tardieu18 | 0.510 | 0.08 | |
| IL13 decT2-T0 | Cog CS6 | 0.016 | 0.96 |
| L CS6 | -0.642 | 0.01* | |
| Mot CS6 | 0.003 | 0.99 | |
| Cog CS18 | -0.638 | 0.01* | |
| L CS18 | -0.593 | 0.03* | |
| Mot CS18 | -0.155 | 0.60 | |
| GMFCS6 | 0.563 | 0.09 | |
| GMFCS18 | 0.462 | 0.10 | |
| Tardieu6 | 0.400 | 0.16 | |
| Tardieu18 | 0.456 | 0.10 | |
| IL13 decT3-T0 | Cog CS6 | -0.281 | 0.33 |
| L CS6 | -0.653 | 0.01* | |
| Mot CS6 | -0.163 | 0.58 | |
| Cog CS18 | -0.287 | 0.34 | |
| L CS18 | -0.388 | 0.19 | |
| Mot CS18 | -0.496 | 0.08 | |
| GMFCS6 | 0.577 | 0.04* | |
| GMFCS18 | 0.535 | 0.04* | |
| Tardieu6 | 0.678 | 0.01* | |
| Tardieu18 | 0.732 | 0.10 | |
| IL1 decT2-T0 | Cog CS6 | -0.121 | 0.68 |
| L CS6 | -0.311 | 0.28 | |
| Mot CS6 | 0.420 | 0.13 | |
| Cog CS18 | -0.579 | 0.17 | |
| L CS18 | -0.538 | 0.24 | |
| Mot CS18 | -0.040 | 0.89 | |
| GMFCS6 | 0.299 | 0.30 | |
| GMFCS18 | 0.292 | 0.31 | |
| Tardieu6 | 0.292 | 0.31 | |
| Tardieu18 | 0.299 | 0.30 | |
| IL1 decT3-T0 | Cog CS6 | -0.036 | 0.91 |
| L CS6 | -0.157 | 0.63 | |
| Mot CS6 | 0.041 | 0.90 | |
| Cog CS18 | -0.188 | 0.56 | |
| L CS18 | -0.398 | 0.20 | |
| Mot CS18 | -0.248 | 0.44 | |
| GMFCS6 | 0.261 | 0.41 | |
| GMFCS18 | 0.230 | 0.47 | |
| Tardieu6 | 0.408 | 0.19 | |
| Tardieu18 | 0.469 | 0.12 | |
| IL2 decT2-T0 | Cog CS6 | -0.249 | 0.37 |
| L CS6 | -0.578 | 0.02* | |
| Mot CS6 | -0.014 | 0.96 | |
| Cog CS18 | -0.484 | 0.07 | |
| L CS18 | -0.498 | 0.04* | |
| Mot CS18 | -0.188 | 0.50 | |
| GMFCS6 | 0.465 | 0.08 | |
| GMFCS18 | 0.500 | 0.35 | |
| Tardieu6 | 0.490 | 0.06 | |
| Tardieu18 | 0.452 | 0.09 | |
| IL2 decT3-T0 | Cog CS6 | -0.180 | 0.54 |
| L CS6 | -0.126 | 0.67 | |
| Mot CS6 | 0.055 | 0.85 | |
| Cog CS18 | -0.056 | 0.86 | |
| L CS18 | -0.227 | 0.46 | |
| Mot CS18 | 0.058 | 0.85 | |
| GMFCS6 | 0.367 | 0.22 | |
| GMFCS18 | 0.494 | 0.09 | |
| Tardieu6 | 0.584 | 0.03* | |
| Tardieu18 | 0.498 | 0.08 | |
| IL7 decT2-T0 | Cog CS6 | -0.070 | 0.82 |
| L CS6 | 0.202 | 0.50 | |
| Mot CS6 | 0.114 | 0.71 | |
| Cog CS18 | -0.403 | 0.17 | |
| L CS18 | -0.266 | 0.38 | |
| Mot CS18 | -0.010 | 0.97 | |
| GMFCS6 | 0.464 | 0.11 | |
| GMFCS18 | 0.367 | 0.22 | |
| Tardieu6 | 0.086 | 0.78 | |
| Tardieu18 | 0.052 | 0.86 | |
| IL7 decT3-T0 | Cog CS6 | -0.258 | 0.39 |
| L CS6 | -0.338 | 0.26 | |
| Mot CS6 | -0.204 | 0.50 | |
| Cog CS18 | -0.141 | 0.65 | |
| L CS18 | -0.145 | 0.64 | |
| Mot CS18 | -0.380 | 0.20 | |
| GMFCS6 | 0.553 | 0.55 | |
| GMFCS18 | 0.599 | 0.43 | |
| Tardieu6 | 0.728 | 0.01* | |
| Tardieu18 | 0.711 | 0.31 |
GFAP= Glial fibrillary acidic protein, GM-CSF= granulocyte-macrophage colony-stimulating factor, IL= Interleukin, T0= hospital admission, T2=72 hours of life, T3=7-10 days of age, decT2-T0= decrease when comparing levels from T0 to T2, decT3-T0= decrease when comparing levels from T0 to T3, n= number of subjects included. Cog CS6 = Cognitive Composite Score at 6 mo, Cog CS18 = Cognitive Composite Score at 18 mo, L CS6 = Language Composite Score at 6 mo, L CS18 = Language Composite Score at 18 mo, Mot CS6 = Motor Composite Score at 6 mo, Mot CS18=Motor Composite Score at 18 mo, GMFCS6 = Gross Motor Function Classification System at 6 mo, GMFCS18 = Gross Motor Function Classification System at 18 mo, Tardieu6= Tardieu Scale at 6 mo, Tardieu18= Tardieu Scale at 18 mo. *p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



