
Submitted:
10 April 2024
Posted:
11 April 2024
You are already at the latest version
Abstract
Polycystic Ovary Syndrome (PCOS) is the most common endocrine disorder that affects women of reproductive age representing the primary cause of anovulatory infertility. The nonapeptide oxytocin (OT) plays an important role in cognitive, emotional, and reproductive functions in human beings. Oxytocin receptors are expressed in several body parts including the ovaries. Despite this, the possible role played by oxytocin in symptoms of PCOS is not clear. The present systematic review aimed at understanding, the presence of possible oxytocin level alterations in PCOS, the connection between alterations of OT levels and the symptoms of PCOS, and the effect of oxytocin administration in PCOS. After a systematic search in the principal databases, seven studies, five human and two animal, were included. Most of the studies highlighted the role played by oxytocin in fertility issues related to PCOS. Studies that analyzed oxytocin basal levels in PCOS women agreed that PCOS is associated with a reduction in the serum level of oxytocin. Two studies found that in PCOS the serum levels of oxytocin were lower than healthy controls. One human and one animal study agreed about lower levels of PCOS, confirming a possible implication of a dysfunction of OT, in the pathogenesis of PCOS.
Keywords:
Oxytocin
; PCOS
; Systematic Review
; Fertility
1. Introduction
Polycystic Ovary Syndrome (PCOS) is the most common endocrine disorder that affects women of reproductive age [1]. Depending on the diagnostic criteria used its worldwide prevalence goes from 4% up to 20% [2]. PCOS is characterized by polycystic ovary morphology, androgen excess and ovulatory dysfunction [3]. In combination with its typical metabolic, reproductive as well as psychological features, PCOS is a relevant public health concern [4]. In particular, if taken into consideration that about 75% of PCOS cases are estimated to be undiagnosed [5]. PCOS is associated with high levels androgens including dehydroepiandrosterone and androstenedione of adrenal origin as well as androstenedione and testosterone of ovarian origin [6]. PCOS is also usually characterized by increased luteinizing hormone (LH) levels, elevated LH/FSH ratio [6,7,8,9], and low to normal follicle-stimulating hormone (FSH) levels [7,10]. However, other studies suggest there are no significant differences in LH/FSH ratio [11] between PCOS and control groups.
Furthermore, PCOS is the primary cause of anovulatory infertility [12] and accounting for 80% of those cases [13,14]. Pregnant PCOS women, on the other hand have a higher risk of developing gestational diabetes mellitus or suffering a first-trimester spontaneous abortion [15,16]. Interestingly, even though elevated baseline LH/FSH ratio in PCOS was found to be related to poor ovulatory response, PCOS cases with elevated LH/FSH ratio were more likely to achieve a clinical pregnancy and live birth than women with normal LH/FSH [9].
Ovarian function and cycles are regulated by the hypothalamic-pituitary-ovarian (HPO) axis, in particular by GnRH and the Gonadotropins. During the last years, the nonapeptide oxytocin (OT) attracted the attention of the scientific community. OT is synthesized in the paraventricular and supraoptic nuclei of the hypothalamus, along with a few neurons in the accessory nuclei of the hypothalamus, and is transported to the neurohypophysis where it is released in the blood circulation [17,18,19]. OT plays a crucial role in several behavioral and reproductive functions in human beings, such as breastfeeding, pregnancy and parturition but also in other processes like bonding decision-making, prosocial behavior, and physical activity [20]. It is also related to the pleasure associated with orgasm ,both in males and females, being released in elevated quantities during this process. OT receptors (OXTR) are expressed in several body parts including the ovaries and prostate gland. Specifically, OXTR are found to be expressed in the granulosa cells, and in the small follicles in several mammal species including humans [21], and OT takes a still unclear role in steroidogenesis [22]. Despite the growing interest in the role played by oxytocin in several human functions, its possible role in one or more psychological symptoms, such as depression, anxiety, and social cognitive impairments or physical symptoms, such as metabolic dysfunctions or infertility, of PCOS [23] is still not clear or little studied. In the present systematic review, we aimed to disentangle the role played by oxytocin in PCOS, taking into account all animal and human studies. In particular, we aimed to understand (i) the presence of possible alterations of basal plasmatic OT level in PCOS, (ii) in which manner a possible alteration of the OT plasmatic level can be related to the symptoms of PCOS, and (iii) the presence of a possible effect of OT administration in PCOS.
2. Materials and Methods
The present systematic review (PROSPERO reg. n. 531987) followed the procedure recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [24]. We performed a computer-based search in the principal databases, such as PubMed, Web of Science, and Scopus, combining terms related to polycystic ovary syndrome and oxytocin (Figure 1).
Moreover, our research question used the PICO strategy protocol. In particular, our research question was related to the role played by oxytocin (O - Outcome) in women or animal models with polycystic ovary syndrome (P- Population), determining the level of oxytocin in body fluids, such as blood and saliva (I- Intervention) in comparison with healthy women or animals (C- Comparison- Table 1- Appendix A).
In the present systematic review, databases were selected to explore the published studies using the following keywords: "polycystic ovary syndrome" [MeSH Terms] OR ("polycystic" [All Fields] AND "ovary" [All Fields] AND "syndrome"[All Fields]) OR "polycystic ovary syndrome" [All Fields]) AND ("oxytocin"[MeSH Terms] OR "oxytocin"[All Fields] OR "oxytocin s [All Fields] OR "oxytocin [All Fields] OR "oxytocin [All Fields]”, with no time limit, and using the Boolean operators AND and OR. The inclusion and exclusion criteria were determined based on the topic, study design, and population (Table 2).
In the second stage, we removed the duplicates and manually screened both the titles and abstracts to evaluate if they fulfilled the inclusion and/or exclusion criteria. After that, we retrieved the full text of the possibly pertinent studies to verify their eligibility. Two authors independently carried out the literature search, article screening, and methodologic evaluation. Both authors discussed the results and a consensus was reached. However, a third opinion was required when a consensus was not reached.
The included studies were subsequently screened to find further articles in the reference lists related to the topic of interest. Similarly, we screened all the excluded studies to identify additional relevant bibliographic sources. To estimate the quality of the selected studies, when possible, in the current systematic review, it was used the “NOS- Newcastle-Ottawa Scale Quality assessment scale for case-control and cohort studies” (https://www.ohri.ca/programs/clinical_epidemiology/nosgen.pdf- Supplementary material).
Then, information associated with the characteristics of the participants and inclusion and exclusion criteria were extracted from each included article, according to the previously mentioned guidelines. The flowchart in Figure 1 depicts the steps of the selection process.
3. Results
The flowchart depicted in Figure 1 shows the selection process of the studies. We included 6 published studies in the systematic review, after reaching a consensus. Moreover, we calculated Cohen's k with 87.17 % (k = 0.742) indicating substantial agreement (https://idostatistics.com/cohen–kappa–free–calculator/)[25]. The characteristics of the studies are shown in Table 3.
Both human and animal studies were included. However, the selected studies did not show homogeneity in terms of both study design and population. The four human studies included 609 women and were published between 2010 and 2023. Among these, two were randomized or pseudo-randomized clinical trials, one was a case-control study and another one was a population genetics study.
Moreover, the principal focus of the included studies was related to the relationship between fertility and nasal oxytocin administration. Similarly, Ochsenkühn et al. included patients with PCOS as a cause of infertility together with different infertile groups [26]. Conversely, the clinical trial performed by Masrour et al. [27], included only infertile patients with PCOS [27]. During the clinical trial, the patients underwent eight units of OT, but the authors did not observe any significant changes in terms of infertility. Ochsenkühn et al. who did not observe any improvement in the fertility of the PCOS group after OT treatment [26] obtained similar results. Despite the administration of OT, these two above-mentioned studies did not assess the level of blood or salivary oxytocin in the participants [26,27]. However, since the main topic of both RCTs was to assess the effect of 8 IU of intranasal OT on infertility in PCOS, the studies found the treatment not relevant to improving fertility in PCOS patients affected by infertility. As underlined by Ochsenkühn et al., the failure to detect the effect of OT on the pregnancy rate can be the result of inadequacy in dose and or mode of administration [26]. The level of OT in PCOS before a treatment can be relevant, but none of the two RCTs collected such samples in PCOS groups. However, Jahromi et al. compared the level of oxytocin and other hormones (table 3) in both infertile women with or without PCOS [28]. These authors found that in PCOS the mean level of OT was inferior to the non-PCOS, with a mean value of 124.94ng/l compared to 207.42ng/l (p<0.0001). Moreover, since the anti-mullerian hormone usually shows high levels in PCOS, it was negatively correlated with oxytocin and the same occurred with insulin resistance. However, the authors did not observe a significant effect of BMI on oxytocin in both groups. According to the authors, the hormonal imbalances in hypothalamic-pituitary-ovarian (HPO), namely high LH and low FSH in the PCOS group, could be connected to the lower oxytocin levels. These low levels can in turn be implicated in chronic anovulation. Notably, this study was the first that proposed a cut-off value of the oxytocin level in women with PCOS.
Similar results were observed in a case-control study, [29] assessing the hypothalamic-pituitary-ovary axis dysfunction in a sample of 56 infertile PCOS women before the ovarian stimulation, with 2.5 mg of letrozole, and before the human chorionic gonadotropin (hCG) administration. The authors assessed the serum levels of OT, Dopamine(DA), phoenixin-14 (PNX-14), and nesfatin-1(NEF-1) in the group of pregnant and non-pregnant PCOS women. Moreover, FSH, LH, AMH, TSH, and prolactin have been assessed. In the whole sample, they found a weak association of OT with BMI and a stronger one with FSH (p<0.0002). However, in the pregnant group, higher baseline NES-1 and OT levels (+29.2% and +44%) were observed. Similarly, the OT level increase was associated with positive pregnancy rates. After OS in pregnant women the OT levels increase compared to non-pregnant.
Finally, Amin and colleagues [30] assessed the presence of the polymorphisms of the gene responsible for the expression of the receptor of oxytocin (OXTR) in 212 Italian PCOS patients. OXTR is widely expressed in the human body, including the brain and ovary tissue [31]. In their genetic population study, the authors tested the hypothesis whereby the OXTR variants are in linkage disequilibrium with PCOS in Italian families. They found that five variants, out of 22, were significantly (p < 0.05) linked to or were in linkage disequilibrium with PCOS. However, all these variants were not previously related to clinical manifestations of PCOS. Still, three of them (rs60345038, rs35498753, and rs237900) were found to intersect with the repressed chromatin state in the ovaries, with a negative OXTR gene expression.
In the present systematic review, animal studies were included. The two animal studies included 30 female rats and were published in 2018 and 2022, respectively. These two studies were classified as RCTs and both administered OT to PCOS rat models. However, Sajadi et al, [32] also administered carbachol. Despite the use of OT, the main objective of the two studies was different. Sajadi and Colleagues [32] studied the uterine contraction and tone in PCOS and non-PCOS rats after administration of OT or carbachol, while Yamamoto et al. [33] measured the effects of the administration of acute and chronic OT on metabolic disorders as well as the changes in endogenous OT in PCOS model rats.
Sajadi et al, [32] found that PCOS rats showed more irregular uterine contractions than controls and that after being exposed to carbachol their frequency and resting tone were significantly increased compared to controls. However, after the exposure to OT, there were no differences in frequency, resting tone, and amplitude of rhythmic contractions between both groups.
Yamamoto et al. [33] found that PCOS model rats showed lower serum OT levels than control rats. Nonetheless, the two groups did not differ in hypothalamic OT mRNA expression levels. The authors found that there were reductions in body weight gain and food intake only in PCOS model rats after the acute intraperitoneal OT administration during the dark phase, whereas the chronic administration of OT decreased the food intake in both the PCOS model rats and control rats.
4. Discussion
Despite the relevant role played by the nonapeptide oxytocin in several functions, such as social cognition, metabolic regulation, and reproduction, only a few recent studies investigated its role in PCOS. However, given the novelty of the topic, the present systematic review took into consideration all the studies that investigated the role played by not only serum oxytocin but also randomized clinical trials with the administration of synthetic oxytocin. The present review took into account also animal studies, since most of the current knowledge about PCOS was obtained by studies on rat models. These played a crucial role for studying and gaining insights into human pathologies during the last two centuries. Despite some similarities between animals and humans, they also showed distinct characteristics. Acknowledging important disparities in OT between animals and humans, the insights from rat studies are nevertheless important for the comprehension of the role played by OT in PCOS.
Most of the studies underestimated the relevance of the levels of OT in women with PCOS, by not reporting a possible OT basal levels difference. Notably, only two studies found that in PCOS the levels of OT were lower than healthy controls. Indeed, one human and one animal study agreed about lower levels of PCOS, confirming a possible implication of OT, in the pathogenesis of the syndrome, which can negatively affect the effect of OT administrations. Despite the complexity of the symptoms of PCOS, anovulatory infertility represents one of the most relevant issues. According to Pirog and colleagues, OT can be considered a predictor of pregnancy before ovarian stimulation therapy [29].
According to Dinsdale and Crespi [34], the relevance of oxytocin and possible alterations in the OT and OTXR system in PCOS is still not well understood. According to their review, PCOS and Autism spectrum disorder share several behavioral features that can induce speculation about a possible common role of OT in the two disorders [34]. However, the focus of the studies that we included was only related to the infertility issues related to PCOS. In different animal models, oxytocin seems to have a role in fertility by promoting the release of PGF2α from endometrial cells. Moreover, OT is involved in the process of luteolysis [35,36]. A similar mechanism is also present in human beings, but a positive role of administration of OT in the folliculogenesis and the increasing pregnancy rate in both humans and animals was reported in a few studies [37,38]. Ochsenkühn and colleagues [26] did not observe any increase in the pregnancy rate in couples affected by PCOS and infertility after 8 IU intranasal OT administration. The role of OT in uterine contractions has been assessed in a recent study [32], which compared PCOS and non-PCOS female rats uteri. After administration of the oxytocin, no significant differences were observed in the amplitude, tone, and frequency in the rhythmic uterine contraction of PCOS rats. However, the increase in the dose of OT stimulated higher levels of tone, with a decrease in the contraction frequency in PCOS rats' uterine tissues. It is well-studied that in the myometrium the number of oxytocin receptors increases, during the pregnancy [39], allowing the uterus to become more sensitive to oxytocin thus affecting the pattern of contraction during the pregnancy and labor. Despite this, Leonhardt et al, [40] did not find uterine morphological differences using magnetic resonance imaging, and less uterine peristaltic movement was found in PCOS assessed with transvaginal ultrasonography.
Despite the increase in the number of receptors, their genetic expression can be different in PCOS. Amin et al., [26] reported five novel genetic variants for the receptor of OT (OXYTR) associated with the risk of developing PCOS in multigenerational Italian families. These variants of the OXTR gene were found to be related to the principal symptoms of PCOS, such as anovulation or oligovulation, hyperandrogenism, polycystic ovaries, and the increased risk for metabolic alterations [41].
Some of the variants found by Amin are considered relevant for vulnerability to different disorders. The variant OXTR rs237902 found by Amin et al., [30] has been associated with schizophrenia vulnerability. Specifically, a significant association between rs237902 and negative symptoms, such as blunted affect, alogia, avolition asociality, and anhedonia, in schizophrenic patients and an overrepresentation in male aggressive children were observed [42,43,44]. Among the variants observed in PCOS, rs60345038 was also found to be relevant for type 2 diabetes [41].
Metabolic alterations were also studied in PCOS rats [33]. Rats to which OT was administered showed a significant decrease in weight and food intake [33]. However, this study did not quantify the lipolysis in the adipose tissue of the rats. Previous findings indicated that OT administration significantly reduced the area of adipocytes, the serum triglyceride, aspartate aminotransferase level alanine aminotransferase, and alkaline phosphatase in ovariectomized rats [46]. The menopausal period is considered to be a risk factor for visceral adiposity and metabolic disorders.
5. Conclusions
PCOS is a multifaceted syndrome involving several symptoms affecting the patients' quality of life at different levels. The present review described the studies that analyzed the levels or the effects of administering OT in PCOS.
The studies reported in the present systematic review took into account only a part of the possible roles played by OT in PCOS. Most of the studies highlighted the role played by OT in fertility issues related to PCOS. Studies that analyzed the basal levels of OT in PCOS women agreed that PCOS is accompanied by a reduction in the serum level of oxytocin.
In what concerns the effects of OT administration it was noticeable that different dosage regimens or patterns of administration were not sufficiently studied. Besides, despite the novelty and relevance of the topic, none of these studies analyzed the effect of OT administration on prosocial behavior, or in couples’ relationships and sexual satisfaction in PCOS. Indeed, OT is not only implied in maternal behavior and reproduction but also in the relationship and importantly in orgasm[53].
6. Future Directions
Several outstanding issues need to be clarified by further studies that could disentangle the role played by OT administration in social behavior and the improvement of psychological symptoms in PCOS. Further studies are needed to clarify if the OT basal serum levels are associated with metabolic disorders in PCOS. Moreover, none of the studies that were included in the present systematic review assessed the relationship between OT and psychiatric comorbidities, such as mood and anxiety disorders, in PCOS.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org., Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, N.C., D.P and J.P.; methodology, N.C and J.P.; investigation, N.C and J.P; resources, N.C and J.P.; data curation, J.P.; writing—original draft preparation, N.C and J.P.; writing—review and editing, N.C and D.P.; visualization, N.C.; supervision, D.P. All authors have read and agreed to the published version of the manuscript.”
Funding
“This research received no external funding”
Institutional Review Board Statement
“Not applicable”
Informed Consent Statement
“Not applicable.”
Data Availability Statement
All the data are shown in the full text.
Conflicts of Interest
“The authors declare no conflicts of interest.”
Appendix A
PICO Worksheet and Search Strategy Protocol
1. Define your question using PICO by identifying the patient/Problem, Intervention, Comparison group, and outcome:
Patient/Problem: Patients with Polycystic Ovary Syndrome (PCOS)/ PCOS Animal Models
Intervention: Hormonal level measurement/ pharmacological treatment
Comparison: comparison of the patients/animals with healthy controls
Outcome: Treatment effects and /or difference in oxytocin levels
Write out your question
2. Type of question/problem: The role of oxytocin in PCOS.
Circle one: x Therapy/Prevention/Diagnosis/Etiology/Prognosis
3. Type of studies/publications to include in the search:
Check all that apply:
□ x Meta-analysis □ x Systematic review
□ Clinical practice guidelines □ x Randomized controlled trial
□ x Research studies or articles □ Case report or series
□ Research report or other grey literature
4. List main topics and alternate terms from your PICO question that can be used for your search: “experimental studies”; “women”; “PCOS”; “rats”; “Oxytocin”.
5. Write out your search strategy: "polycystic ovary syndrome"[MeSH Terms] OR ("polycystic"[All Fields] AND "ovary"[All Fields] AND "syndrome"[All Fields]) OR "polycystic ovary syndrome"[All Fields]) AND ("oxytocin"[MeSH Terms] OR "oxytocin"[All Fields] OR "oxytocin s [All Fields] OR "oxytocin [All Fields] OR "oxytocin [All Fields]”
Boolean search operators (AND) and (OR).
6. List any limits that may apply to your search:
Gender: Female;
Age: Adults;
Year(s) of publication: no limits; Language(s): English
7. List the databases you will search: PubMed, Scopus, and Web of Science.
References
- Witchel, S.F.; Teede, H.J.; Peña, A.S. Curtailing PCOS. Pediatr. Res. 2019, 87, 353–361. [Google Scholar] [CrossRef]
- Pundir, C.S.; Deswal, R.; Narwal, V.; Dang, A. The Prevalence of Polycystic Ovary Syndrome: A Brief Systematic Review. J. Hum. Reprod. Sci. 2020, 13, 261–271. [Google Scholar] [CrossRef]
- Chiaffarino, F.; Cipriani, S.; Dalmartello, M.; Ricci, E.; Esposito, G.; Fedele, F.; La Vecchia, C.; Negri, E.; Parazzini, F. Prevalence of polycystic ovary syndrome in European countries and USA: A systematic review and meta-analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 279, 159–170. [Google Scholar] [CrossRef]
- Azziz, R.; Carmina, E.; Chen, Z.; Dunaif, A.; Laven, J.S.; Legro, R.S.; Lizneva, D.; Natterson-Horowtiz, B.; Teede, H.J.; Yildiz, B.O. Polycystic ovary syndrome. Nat. Rev. Dis. Primers 2016, 2, 16057. [Google Scholar] [CrossRef]
- Carmina, E. Diagnosis of polycystic ovary syndrome: from NIH criteria to ESHRE-ASRM guidelines. 2004, 56, 1–6. [Google Scholar]
- Blank, S.K.; McCartney, C.R.; Chhabra, S.; Helm, K.D.; Eagleson, C.A.; Chang, R.J.; Marshall, J.C. Modulation of Gonadotropin-Releasing Hormone Pulse Generator Sensitivity to Progesterone Inhibition in Hyperandrogenic Adolescent Girls—Implications for Regulation of Pubertal Maturation. J. Clin. Endocrinol. Metab. 2009, 94, 2360–2366. [Google Scholar] [CrossRef]
- Haqq, L.; McFarlane, J.; Dieberg, G.; Smart, N. Effect of lifestyle intervention on the reproductive endocrine profile in women with polycystic ovarian syndrome: a systematic review and meta-analysis. Endocr. Connect. 2014, 3, 36–46. [Google Scholar] [CrossRef]
- Malini, N.; George, K.R. Evaluation of different ranges of LH:FSH ratios in polycystic ovarian syndrome (PCOS) – Clinical based case control study. Gen. Comp. Endocrinol. 2018, 260, 51–57. [Google Scholar] [CrossRef]
- Xia, Q.; Xie, L.; Wu, Q.; Cong, J.; Ma, H.; Li, J.; Cai, W.; Wu, X. Elevated baseline LH/FSH ratio is associated with poor ovulatory response but better clinical pregnancy and live birth in Chinese women with PCOS after ovulation induction. Heliyon 2023, 9, e13024. [Google Scholar] [CrossRef]
- Kriedt, K.J.; Alchami, A.; Davies, M.C. PCOS: diagnosis and management of related infertility. Obstet. Gynaecol. Reprod. Med. 2018, 29, 1–5. [Google Scholar] [CrossRef]
- Cho, L.W.; Jayagopal, V.; Kilpatrick, E.S.; Holding, S.; Atkin, S.L. The LH/FSH ratio has little use in diagnosing polycystic ovarian syndrome. Ann. Clin. Biochem. Int. J. Biochem. Lab. Med. 2006, 43, 217–219. [Google Scholar] [CrossRef]
- E Joham, A.; Norman, R.J.; Stener-Victorin, E.; Legro, R.S.; Franks, S.; Moran, L.J.; Boyle, J.; Teede, H.J. Polycystic ovary syndrome. Lancet Diabetes Endocrinol. 2022, 10, 668–680. [Google Scholar] [CrossRef]
- Balen, A.H.; Morley, L.C.; Misso, M.; Franks, S.; Legro, R.S.; Wijeyaratne, C.N.; Stener-Victorin, E.; Fauser, B.C.; Norman, R.J.; Teede, H. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum. Reprod. Update 2016, 22, 687–708. [Google Scholar] [CrossRef]
- Melo, A.S.; Ferriani, R.A.; Navarro, P.A. Treatment of infertility in women with polycystic ovary syndrome: approach to clinical practice. Clinics 2015, 70, 765–769. [Google Scholar] [CrossRef]
- Sirmans, S.; Pate, K. Epidemiology, diagnosis, and management of polycystic ovary syndrome. Clin. Epidemiology 2013, 6, 1–13. [Google Scholar] [CrossRef]
- Salley, K.E.S.; Wickham, E.P.; Cheang, K.I.; Essah, P.A.; Karjane, N.W.; Nestler, J.E. POSITION STATEMENT: Glucose Intolerance in Polycystic Ovary Syndrome—A Position Statement of the Androgen Excess Society. J. Clin. Endocrinol. Metab. 2007, 92, 4546–4556. [Google Scholar] [CrossRef]
- Carter, C.S. Oxytocin Pathways and the Evolution of Human Behavior. Annu. Rev. Psychol. 2014, 65, 17–39. [Google Scholar] [CrossRef]
- Freda, S. N. , Priest, M. F., Badong, D., Xiao, L., Liu, Y.; Kozorovitskiy, Y. Brainwide input-output architecture of paraventricular oxytocin and vasopressin neurons. bioRxiv, 2022, 2022-01.
- Manjila, S.B.; Betty, R.; Kim, Y. Missing pieces in decoding the brain oxytocin puzzle: Functional insights from mouse brain wiring diagrams. Front. Neurosci. 2022, 16, 1044736. [Google Scholar] [CrossRef]
- Heinrichs, M. , von Dawans, B. ; Domes, G. Oxytocin, vasopressin, and human social behavior. Frontiers in neuroendocrinology, 2009, 30, 548–557. [Google Scholar]
- Yamamoto, K.; Nakano, Y.; Iwata, N.; Soejima, Y.; Suyama, A.; Hasegawa, T.; Otsuka, F. Oxytocin enhances progesterone production with upregulation of BMP-15 activity by granulosa cells. Biochem. Biophys. Res. Commun. 2023, 646, 103–109. [Google Scholar] [CrossRef]
- Saller, S.; Kunz, L.; Dissen, G.; Stouffer, R.; Ojeda, S.; Berg, D.; Berg, U.; Mayerhofer, A. Oxytocin receptors in the primate ovary: molecular identity and link to apoptosis in human granulosa cells. Hum. Reprod. 2010, 25, 969–976. [Google Scholar] [CrossRef]
- Pinto, J.; Cera, N.; Pignatelli, D. Psychological symptoms and brain activity alterations in women with PCOS and their relation to the reduced quality of life: a narrative review. J. Endocrinol. Investig. 2024, 1–22. [Google Scholar] [CrossRef]
- Knobloch, K.; Yoon, U.; Vogt, P.M. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and publication bias. J. Cranio-Maxillofacial Surg. 2010, 39, 91–92. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. An Application of Hierarchical Kappa-type Statistics in the Assessment of Majority Agreement among Multiple Observers. Biometrics 1977, 33, 363–74. [Google Scholar] [CrossRef]
- Ochsenkühn, R.; Pavlik, R.; Hecht, S.; von Schönfeldt, V.; Rogenhofer, N.; Thaler, C.J. The effect of nasal oxytocin on pregnancy rates following intrauterine insemination: double-blind, randomized, clinical pilot study. Arch. Gynecol. Obstet. 2009, 281, 753–759. [Google Scholar] [CrossRef]
- Masrour, M. J.; Azad, Z. A comparison of the effects of human chorionic gonadotropin and oxytocin on ovulation in PCOS patients from 2015 until 2018. Acta Medica Mediterranea, 2018, 34, 1757–1763. [Google Scholar]
- Jahromi, B.N.; Dabbaghmanesh, M.H.; Bakhshaie, P.; Parsanezhad, M.E.; Anvar, Z.; Alborzi, M.; Zarei, A.; Bakhshaei, M. Assessment of oxytocin level, glucose metabolism components and cutoff values for oxytocin and anti-mullerian hormone in infertile PCOS women. Taiwan. J. Obstet. Gynecol. 2018, 57, 555–559. [Google Scholar] [CrossRef]
- Piróg, M.; Jach, R.; Ząbczyk, M.; Natorska, J. Increased Serum Levels of Phoenixin-14, Nesfatin-1 and Dopamine Are Associated with Positive Pregnancy Rate after Ovarian Stimulation. J. Clin. Med. 2023, 12, 6991. [Google Scholar] [CrossRef]
- Amin, M.; Horst, N.; Wu, R.; Gragnoli, C. Oxytocin receptor (OXTR) is a risk gene for polycystic ovarian syndrome. 2023, 27, 2634–2638. [CrossRef]
- Gimpl, G.; Fahrenholz, F.; Srinivasa, S.; Aulinas, A.; O’malley, T.; Maehler, P.; Adler, G.K.; Grinspoon, S.K.; Lawson, E.A.; Santoso, P.; et al. The Oxytocin Receptor System: Structure, Function, and Regulation. Physiol. Rev. 2001, 81, 629–683. [Google Scholar] [CrossRef]
- Sajadi, M.; Noroozzadeh, M.; Bagheripour, F.; Tehrani, F.R. Contractions in the Isolated Uterus of a Rat Model of Polycystic Ovary Syndrome Compared to Controls in Adulthood. Int. J. Endocrinol. Metab. 2018, 16, e63135. [Google Scholar] [CrossRef]
- Yamamoto, S.; Noguchi, H.; Takeda, A.; Arakaki, R.; Uchishiba, M.; Imaizumi, J.; Minato, S.; Kamada, S.; Kagawa, T.; Yoshida, A.; et al. Changes in Endogenous Oxytocin Levels and the Effects of Exogenous Oxytocin Administration on Body Weight Changes and Food Intake in Polycystic Ovary Syndrome Model Rats. Int. J. Mol. Sci. 2022, 23, 8207. [Google Scholar] [CrossRef] [PubMed]
- Dinsdale, N.L.; Crespi, B.J. Revisiting the wandering womb: Oxytocin in endometriosis and bipolar disorder. Horm. Behav. 2017, 96, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Burns, P. D. , Mendes Jr, J. O., Yemm, R. S., Clay, C. M., Nelson, S. E., Hayes, S. H.; Silvia, W. J. Cellular mechanisms by which oxytocin mediates ovine endometrial prostaglandin F2α synthesis: role of Gi proteins and mitogen-activated protein kinases. Biology of reproduction, 2001, 65, 1150–1155. [Google Scholar]
- Mechsner, S.; Bartley, J.; Loddenkemper, C.; Salomon, D.S.; Starzinski-Powitz, A.; Ebert, A.D. Oxytocin receptor expression in smooth muscle cells of peritoneal endometriotic lesions and ovarian endometriotic cysts. Fertil. Steril. 2005, 83, 1220–1231. [Google Scholar] [CrossRef] [PubMed]
- Roushangar L, Soleimani Rad J, Nikpou P, Sayahmeli M. Effect of oxytocin injection on folliculogenesis, ovulation and endometrial growth in mice. Int J Reprod Biomed 2009, 7, 91e5.
- Sayyah-Melli M, Ouladsahebmadarek E, Tagavi S, Mostafa-Garabaghi P, Alizadeh M, Ghojazadeh M, et al. Effect of oxytocin (OT) and OT plus human chorionic gonadotropin (hCG), in cycles induced by letrozole or clomiphene citrate (CC). Afr J Pharm 2012, 6, 2112e8.
- Soloff MS, Alexandrova M, Fernstrom MJ. Oxytocin receptors: triggers for parturition and lactation? Science. 1979, 204, 1313–5.
- Leonhardt, H.; Gull, B.; Kishimoto, K.; Kataoka, M.; Nilsson, L.; O Janson, P.; Stener-Victorin, E.; Hellström, M. Uterine Morphology and Peristalsis in Women with Polycystic Ovary Syndrome. Acta Radiol. 2012, 53, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.H.; Chang, W.H.; Chi, M.H.; Peng, Y.C.; Huang, C.-C.; Yang, Y.K.; Chen, P.S. The OXTR Polymorphism Stratified the Correlation of Oxytocin and Glucose Homeostasis in Non-Diabetic Subjects. Diabetes, Metab. Syndr. Obesity: Targets Ther. 2707; 12. [Google Scholar] [CrossRef]
- Malik, A.I.; Zai, C.C.; Abu, Z.; Nowrouzi, B.; Beitchman, J.H. The role of oxytocin and oxytocin receptor gene variants in childhood-onset aggression. Genes, Brain Behav. 2012, 11, 545–551. [Google Scholar] [CrossRef]
- Montag, C.; Brockmann, E.-M.; Bayerl, M.; Rujescu, D.; Müller, D.J.; Gallinat, J. Oxytocin and oxytocin receptor gene polymorphisms and risk for schizophrenia: A case–control study. World J. Biol. Psychiatry 2012, 14, 500–508. [Google Scholar] [CrossRef]
- Correll, C.U.; Schooler, N.R. Negative Symptoms in Schizophrenia: A Review and Clinical Guide for Recognition, Assessment, and Treatment. Neuropsychiatr. Dis. Treat. 2020, 16, 519–534. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.; Wu, R.; Gragnoli, C. Novel Risk Variants in the Oxytocin Receptor Gene (OXTR) Possibly Linked to and Associated with Familial Type 2 Diabetes. Int. J. Mol. Sci. 2023, 24, 6282. [Google Scholar] [CrossRef] [PubMed]
- Iwasa, T.; Matsuzaki, T.; Mayila, Y.; Yanagihara, R.; Yamamoto, Y.; Kawakita, T.; Kuwahara, A.; Irahara, M. Oxytocin treatment reduced food intake and body fat and ameliorated obesity in ovariectomized female rats. Neuropeptides 2019, 75, 49–57. [Google Scholar] [CrossRef]
- Carr, D.B.; Utzschneider, K.M.; Hull, R.L.; Kodama, K.; Retzlaff, B.M.; Brunzell, J.D.; Shofer, J.B.; Fish, B.E.; Knopp, R.H.; Kahn, S.E. Intra-Abdominal Fat Is a Major Determinant of the National Cholesterol Education Program Adult Treatment Panel III Criteria for the Metabolic Syndrome. Diabetes 2004, 53, 2087–2094. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, C.M.; Lynch, N.A.; Nicklas, B.J.; Ryan, A.S.; Berman, D.M. Differences in Adipose Tissue Metabolism between Postmenopausal and Perimenopausal Women. J. Clin. Endocrinol. Metab. 2002, 87, 4166–4170. [Google Scholar] [CrossRef] [PubMed]
- Iwasa, T.; Matsuzaki, T.; Yano, K.; Yanagihara, R.; Tungalagsuvd, A.; Munkhzaya, M.; Mayila, Y.; Kuwahara, A.; Irahara, M. The effects of chronic testosterone administration on body weight, food intake, and adipose tissue are changed by estrogen treatment in female rats. Horm. Behav. 2017, 93, 53–61. [Google Scholar] [CrossRef]
- Liang, Y.-Q.; Akishita, M.; Kim, S.; Ako, J.; Hashimoto, M.; Iijima, K.; Ohike, Y.; Watanabe, T.; Sudoh, N.; Toba, K.; et al. Estrogen receptor ß is involved in the anorectic action of estrogen. Int. J. Obes. 2002, 26, 1103–1109. [Google Scholar] [CrossRef]
- Meli, R.; Pacilio, M.; Raso, G.M.; Esposito, E.; Coppola, A.; Nasti, A.; Di Carlo, C.; Nappi, C.; Di Carlo, R. Estrogen and Raloxifene Modulate Leptin and Its Receptor in Hypothalamus and Adipose Tissue from Ovariectomized Rats. Endocrinology 2004, 145, 3115–3121. [Google Scholar] [CrossRef]
- Palmisano, B.T.; Zhu, L.; Stafford, J.M. Role of Estrogens in the Regulation of Liver Lipid Metabolism. Sex and Gender Factors Affecting Metabolic Homeostasis, Diabetes and Obesity, 2017, 1043, 227–256. [Google Scholar] [CrossRef]
- Cera, N.; Vargas-Cáceres, S.; Oliveira, C.; Monteiro, J.; Branco, D.; Pignatelli, D.; Rebelo, S. How Relevant is the Systemic Oxytocin Concentration for Human Sexual Behavior? A Systematic Review. Sex. Med. 2021, 9, 100370–100370. [Google Scholar] [CrossRef]
Figure 1.
Flow chart of the selection process for PCOS and Oxytocin. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. http://www.prisma-statement.org/.
Figure 1.
Flow chart of the selection process for PCOS and Oxytocin. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021;372:n71. doi: 10.1136/bmj.n71. http://www.prisma-statement.org/.
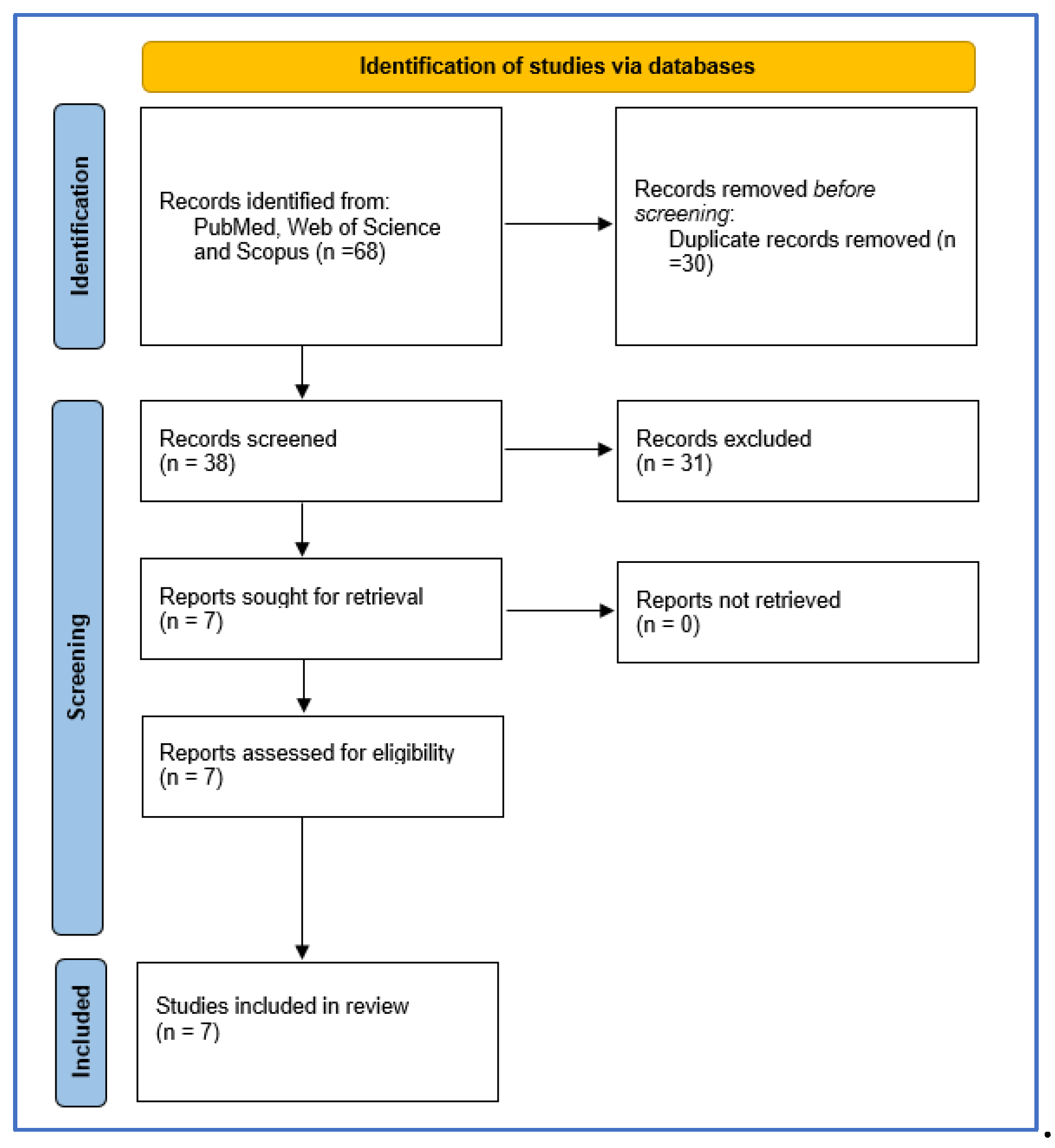

Table 1.
The search strategy used in the present systematic review.
|
Polycystic ovary syndrome 1. Polycystic ovary syndrome [MeSHTerms] 2. Polycystic [All Fields] 3. Ovary [All Fields] 4. Syndrome [All Fields] 5. Polycystic ovary syndrome [All Fields] OR/ 1-2; 4-1 AND/ 3-4; 1-10 |
|
Oxytocin 6. Oxytocin [MeSH Terms] 7. Oxytocin [All Fields] 8. Oxytocin s [All Fields] 9. Oxytocin [All Fields] 10. Oxytocins [All Fields] OR/ 6-10 |
Table 2.
Inclusion and exclusion criteria.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
Table 3.
Demographics, design, assessment, and principal results as shown in the included studies.
| Source | Country | Subjects | Age | Design | Assessment | Treatment | Results |
|---|---|---|---|---|---|---|---|
| Amin et al., 2023 | Italy | 212 women | - | Population genetics study | Single nucleotide polymorphisms (SNPs) within OXTR | - | Out of 22 OXTR-risk variants tested, 5 independent variants were significantly linked to/in LD with PCOS. Three intronic variants were linked to PCOS. One intronic variant and a synonymous variant were both linked and associated with PCOS. All variants are novel and have not been previously associated with PCOS or any PCOS-related phenotype. Three of the variants were found to confer risk for PCOS intersected with a repressed chromatin state in the ovaries. |
| Jahromi et al., 2018 | Iran | 161 women (PCOS = 80; Non-PCOS = 81) |
20-35 years | Case-control | OT, AMH, BMI, LH, T, FSH, TSH, Prolactin, DHEAS. Fasting Blood Sugar, Fasting Insulin, Blood sugar 2 h after 75 gr glucose, Insulin 2h after 75g glucose, HOMA-IR | - | The mean OT level was lower in the case group. The mean BMI, AMH, HOMA-IR, fasting insulin and insulin 2-h after 75-g glucose were higher in the PCOS group. OT was negatively correlated to AMH when evaluated for all participants or only among controls. OT was also negatively correlated to HOMA-IR among all participants. There was not a significant relationship between OT and BMI. The calculated cutoff value for OT was 125 ng/L and for AMH was 3.6 ng/mL in the PCOS group. |
| Piróg et al., 2023 | Poland | 56 infertile women with PCOS18 pregnant | 31.89 ±4.59 years | Case-control | Assessment before ovarian stimulation (OS) and before hCG administration. Assessments of PNX-14, NES-1, DA, and OT serum levels were performed. Other Tests: LH, FSH, Estradiol, PRL, AMH, BMI |
In the whole cohort of patients, OT levels were weakly associated with BMI (r = 0.26, p = 0.048), and FSH (r = 0.47, p = 0.0002). Pregnant group: positive correlations between baseline OT and PRL (r = 0.47; p = 0.04), as well as OT and NES-1 (r = 0.55; p = 0.02). The OT level increase was associated with positive pregnancy rates. In the post-OS, in pregnant PCOS, OT was 2.7 times lower than non-pregnant. |
|
| Masrour et al., 2018 | Iran | 150 women | 19-39 (29 ± 4.48) years |
Clinical Trial | OT, HCG, FSH, Prolactin, Follicle number, Progesterone. | The three groups at random received: 100 mg clomiphene-citrate + 8 units of OT; 100mg clomiphene-citrate + 10000 units of HCG; 100 mg clomiphene citrate + 8 units of OT + 10000 units of HCG. |
There was no major difference among the groups regarding the ovulation rate or the number of follicles, nor were there any significant side effects observed in any groups. |
| Ochsenkühn et al., 2010 | Germany | 86 women | 18-42 (34.2 ± 4.3) years | Randomized, Double-blind, Placebo-controlled Clinical Pilot-Study | Follicle number, Double endometrial width, Estradiol, LH, Progesterone, To assess male fertility: Semen parameters (native sperm concentration, progressive motility, normal sperm morphology, semen volume, total progressive motile sperm count). | 132 homologous IUI cycles with nasal application of placebo or 8 IU OT following IUI | In 132 IUI cycles of 86 women, 17 pregnancies were achieved, accounting for a pregnancy rate of 12.9% per IUI cycle. The pregnancy rates were 13.4% per IUI cycle in the placebo group, and 12.3% per IUI cycle in the OT group. So, the difference was not statistically significant. No relevant side effects were observed in both groups. |
| Sajadi et al., 2018 | Iran | 14 female rats (PCOS = 7; Control = 7) | 75-95 days | Randomized Clinical Trial | CCh; OT. | Rats in the experimental group were subcutaneously injected with 5m/g of free testosterone on gestational day 20; controls received solvent. The contractions of isolated uterus in offspring of both groups were recorded by the power lab system, after exposure to CCh and OT. | Uterine contractions were more irregular in PCOS rats than controls, after exposure to both contractile agonists. |
| Yamamoto et al., 2022 | Japan | 16 female rats (PCOSChronic = 8; ControlCronic = 8; PCOSAcute = 8; ControlAcute =8) |
28 days | Randomized Clinical Trial | OT. | At 10 weeks after the surgical day, all rats were injected with saline for 7 consecutive days, then injected with OT (1200 µg/kg, 0.4 to 0.5 mL injection volume) for the following 7 consecutive days. | The serum OT level was lower in PCOS model rats than in control rats, whereas the hypothalamic OT mRNA expression level did not differ between them. Acute intraperitoneal administration of OT during the dark phase reduced the body weight gain and food intake in PCOS model rats. However, these effects were not observed in control rats. In contrast, chronic administration of OT decreased the food intake in both the PCOS model rats and control rats. |
Abbreviations: OXTR, Oxytocin receptor; LD, linkage disequilibrium; PCOS, Polycystic Ovary Syndrome; OT, Oxytocin; AMH, Anti-mullerian hormone; BMI, Body Mass Index; LH, Luteinizing hormone; T, total Testosterone; FSH, Follicle stimulating hormone; TSH, Thyroid stimulating hormone; DHEAS, Dehydroepiandrosterone sulfate; HOMA-IR, Insulin resistance index; HCG, Chorionic gonadotropin; IUI, intrauterine insemination; CCh, Carbachol. PNX-14, phoenixin-14; NES-1, nesfatin-1; body mass index; DA, dopamine; PRL, Prolactin.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



