
Submitted:
11 April 2024
Posted:
14 April 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Almost four years after COVID-19 was declared a global health emergency, equitable distribution of the vaccine remains a challenge, especially among homeless people, the fastest growing population in Brazil. Therefore, we sought to identify the factors associated with completion of the COVID-19 vaccination schedule among homeless people in Brazil. Materials and Methods: We carried out a cross-sectional study in the capital cities of Brazil's Federative Units, considering people living on the streets as the target population. We used a sequential inclusion approach, with individual interviews conducted by trained professionals, using a validated questionnaire. We used descriptive statistics to analyze the data and a binary logistic regression model to identify factors associated with homeless individuals who completed the COVID-19 vaccination schedule. Results: It was identified that the highest density of homeless people and indicators related to COVID-19 is located in the Northeast, Southeast and South regions of Brazil. The primary data sample consisted of 1,392 participants, predominantly male (n: 961; 69.0%), with an average age of 38.3±15.2 years, belonging to the black/brown race/color (n: 1,097; 78.8%), with an elementary school education (n: 1,060; 76.1%). The factors associated with completing the vaccination schedule were: receiving government aid (OR: 1.58; 95%CI: 1.09 - 2.30), visits from Health Agents from the Street Clinic (OR: 3.19; 95%CI: 1.95 - 5.36), history of COVID-19 (OR: 5.77; 95%CI: 3.17 - 11.15), support for mandatory vaccination against COVID-19 (OR: 3.76; 95%CI: 2.48 - 5.76), trust in the efficacy of vaccines (OR: 3.92; 95%CI: 2.63 - 5.89), seeking information from NGOs, street clinics, community leaders (OR: 1.91; 95%CI: 1.01 - 3.88) and trust in the Federal Government's statements on vaccines (OR: 1.57; 95%CI: 1.06 - 2.31).Conclusion: The study advances knowledge by highlighting the completeness of the COVID-19 vaccination schedule among the homeless population. The source of information proved to be one of the determinants of completeness, and the Unified Health System played a leading role in raising awareness among homeless people, notably through its strategy of street clinics, when available. The evidence points to the importance of affirmative and inclusive actions that guarantee access to the vaccine for homeless people.
Keywords:
COVID-19
; vaccines
; vulnerable populations
1. Introduction
The development of vaccines against COVID-19 represents an important advance in science, technology and public health. The approval of safe and effective vaccines by regulatory bodies in record time was a triumph for public health and has marked the history of the country's National Immunization Program, just like the eradication of smallpox in the last century [1].
Although we have succeeded in obtaining this input, the major challenge is the equal distribution and equitable access to vaccines, as well as their acceptance by the population, particularly among homeless people, since structural inequalities represent a barrier to achieving this goal. [2].
There are disparities or gaps that have emerged, especially among individ-uals who lack fully implemented vaccination schedules. One study showed that the more advanced the individual's vaccination schedule, the lower the risk of death from COVID-19 infection, reducing the likelihood of mortality by up to 16 times, depending on age group [3,4].
PSR presents an increased risk for SARS-CoV-2 infection, as well as for clinical progression to severe forms of illness [5]. It is known that the homeless live in conditions of extreme poverty and are more exposed to infectious diseases [5]as well as having great difficulty in accessing health services [6] due to issues related to processes of exclusion, stigma, prejudice, discrimination, among other determinants that can negatively influence the possibility of successfully completing the vaccination schedule [7].
In Brazil, there was a 38% increase in PRS in 2022, according to the Institute for Applied Economic Research (IPEA, 2022). The estimated number of PLWHA exceeded the 281,000 mark compared to 2019, the period before the COVID-19pandemic [8]. This situation makes it imperative to draw up possible plans to respond to the challenge of dealing with this population during the post-pandemic period, as well as in probable future health emergencies.
In the literature, there are several studies under development aimed at understanding the vaccination situation against COVID-19 in PSRs [9,10] with an emphasis on the countries of the Global North [11,12,13,14,15]. A systematic review (SR) identified the pooled proportion of one dose COVID-19 vaccination was 41% (35 to 47%), which was significantly lower than those in the general population [16]. In the review, we can observe a privileging of studies developed in the hemi-sphere, not observing studies in Latin America, including Brazil, revealing a knowledge gap. Thus, this study aimed to analyze the completeness of the COVID-19 vaccination schedule among persons experiencing homelessness in Brazil.
2. Materials and Methods
1.1. Study Design
This is a cross-sectional, analytical study carried out in Brazil.
1.2. Period and Location of the Study
For the study, the capitals of 24 Brazilian states and Brasilia, the capital of the Federal District, were considered. It is worth noting that each state has developed a unique approach in its organization to provide support for PSR. Figure 1 shows a map of Brazil showing the size of the country in territorial terms, as well as its five macro- regions, the states and the country's capital, Brasília.
It is important to mention that Brazil started the national vaccination campaign against COVID-19 in 2021 and, since then, the National Immunization Program (PNI) has been planning the best proposal to complete, start and/or reinforce the population's vaccination schedules. Since 2023, the use of bivalent vaccines with updated strains with a booster dose for specific groups at greater vulnerability, risk of complications and death and greater exposure has been implemented, as well as maintaining the use of monovalent vaccines to start or complete the vaccination schedule for people who are not part of the priority groups (the elderly and immunocompromised people) eligible for bivalent vaccination. According to the Ministry of Health, both vaccines, monovalent and bivalent, act in the same way in the body, stimulating the immune system to produce protective antibodies and defense cells against the SARS-CoV-2 virus. [4].
The current recommendations for immunization against COVID-19 in Brazil are based on age groups, available immunizers, manufacturers' recommendations and the results of national and international studies. The vaccines available to date are: Covid-19 adsorbed vaccine (inactivated) CoronaVac (Butantan), Covid-19-RNAm vaccine Comirnaty® (Pfizer/Wyeth), Covid-19-recombinant vac-cine Oxford/Covishield (Fiocruz and Astrazeneca) and Covid-19-recombinant vaccine Janssen Vaccine (Janssen-Cilag). [4].
1.3. Population or Sample, Inclusion and Exclusion Criteria
The study population was made up of Brazilian citizens or naturalized citizens, aged 18 or over, who had been homeless or in public places/degraded areas (temporarily or permanently) for at least six months, considering the period in which the interviews took place.
The sequential sampling strategy was used to obtain the sample [17,18] which takes into account the restriction of access to populations that are more challenging to reach, with the aim of incorporating, throughout the study, individuals identified during the study and who are readily available to participate when approached. Even so, simple random sampling was used for finite populations, following classic references in opinion studies, epidemiology and surveys:
Where: "z" is the score; "ε" is the margin of error; "N" is the size of the population; "p̂" is the proportion of the population. Through the calculation for finite populations, a minimum sample of 100 people living in situations of social vulnerability per Brazilian capital was adopted, considering a 10% loss rate [17].
It should be noted that the size of the population used in the calculation took into account the survey carried out by IPEA [8] which estimated that ap-proximately 281,472 people were homeless in Brazil in 2022. In total, 1,525 home-less individuals were interviewed and, in the end, after applying the inclusion and exclusion criteria, 1,392 individuals took part in this study.
1.4. Study Instrument
The instrument used in the research was a questionnaire originally created, validated and published in studies conducted by researchers from the National School of Public Health of the New University of Lisbon (ENSP-UNL) [19]. For application in Brazil, the questionnaire underwent cultural adaptation and validation using the Delphi technique [20,21] by researchers from the Sergio Arouca National School of Public Health at the Oswaldo Cruz Foundation (ENSP-Fiocruz) and the Ribeirão Preto School of Nursing at the University of São Paulo (EERP-USP).
The design of the questionnaire was structured using the Redcap platform [22,23] from the University of São Paulo (USP) Ribeirão Preto campus. Redcap is a browser- based, metadata-oriented Electronic Data Capture (EDC) software with a workflow methodology for designing clinical and observational research data-bases.
1.5. Data Collection and Operational Strategies
To administer the questionnaire, a network of contacts was created to recruit participants through professionals linked to research institutions, universities, civil society leaders and social movements (MS). The strategy of mobilizing participants through social movements was also adopted, because they are ex-ponents of the connection to territories and populations in situations of social vulnerability, mainly due to the interlocution created by the various key strategies developed in these places and for these populations.
The questionnaire was administered by field interviewers using cell phones and/or tablets, and the average application time was 20 to 30 minutes. The inter-viewers were also trained to administer the questionnaire in order to avoid measurement bias.
1.5.1. Vaccination Completeness
The complete basic (primary) regimen is defined as the number of doses needed to achieve the immune response sufficient to guarantee protection against the disease, depending on the producing laboratory, 2 doses or 1 single dose [4]. COVID-19 vaccines generally involve two doses to be considered complete, although this may vary depending on the specific vaccine. In addition, in some cases, booster doses may be recommended to maintain or increase the effectiveness of immunization over time. It should be emphasized that having a complete vaccination schedule against COVID-19 is essential to reduce the spread and prevent the occurrence of severe cases of the disease, thus reducing mortality rates [4,24].
1.6. Statistical Analysis
1.6.1. Stage I - Situational Diagnosis
Initially, in order to carry out a situational diagnosis of the homeless population and the indices related to COVID-19 (incidence rate, mortality and per-centage of people who have completed the vaccination schedule against COVID-19), choropleth maps were constructed to verify the spatial distribution and concentration of these indicators.
To do this, data was collected on the estimated number of people living on the streets from the Brazilian Observatory of Public Policies for the Homeless (OBPOPRUA), which is linked to the Federal University of Minas Gerais. [25]data referring to the Brazilian population estimate obtained from the Brazilian Institute of Geography and Statistics (IBGE) [26]data on the number of cases and deaths from COVID-19 obtained from the Coronavirus Panel of the Ministry of Health [27] and data on vaccination against COVID-19 obtained from the Vacinometer, also published by the Ministry of Health [28]. In addition, it is important to mention that data on the number of vaccine doses, cases and deaths from COVID-19 were collected from the first reported case in 2020 until February 29, 2024.
With this data, four indicators were calculated, namely: percentage of homeless population (estimated number of homeless individuals / estimated number of the general population, multiplied by 100 = % homeless population per municipality); COVID-19 incidence rate (number of COVID-19 cases reported / estimated population per municipality, multiplied by 1.000 = incidence rate per 1000 inhabitants, per municipality); COVID-19 mortality rate (number of COVID-19 deaths reported / estimated population per municipality, multiplied by 1.000 = incidence rate per 1000 inhabitants, per municipality).000 = COVID-19 incidence rate per 1000 inhabitants, per municipality); COVID-19 mortality rate (number of COVID-19 deaths reported / estimated population per municipality, multiplied by 100,000 = COVID-19 mortality rate per 100.000 inhabitants, per municipality) and percentage of the population that has completed the COVID-19 vaccination schedule (number of people who have had a booster dose of the COVID-19 vaccine / estimated number of the general population, multiplied by 100 = % of the population with a complete COVID-19 vaccination schedule per municipality). To draw up the choropleth map, ArcGis software was used to check the density of the calculated indices.
1.6.2. Stage II - Primary Data Analysis
After processing the databases, exploratory analyses were carried out to characterize the sociodemographic profile of the study sample. This stage was carried out using descriptive statistics for the quantitative parameters, calculating absolute and relative frequencies for the categorical variables and the mean, median and standard deviation for the continuous variable (age), using SPSS software version 22.
To verify the completeness of the COVID-19 vaccination schedule in the PRS, a binary logistic regression analysis was carried out. To do this, the dependent variable was initially dichotomized into completeness (1) and incompleteness of the COVID-19 vaccination schedule (0). Completeness was defined as when the subject had the required vaccines (booster dose or single dose, depending on the laboratory). Incompleteness was considered to be the situation of individuals who received only one dose of the vaccine, without subsequent booster doses.
To identify the factors associated with completing the COVID-19 vaccination schedule, the following were considered as independent variables: Sex (Male, Female, Other); Race/Color (Black/Brown, White); Marital Status (Single, Divorced or Widowed,
Married or in a Stable Union); Occupation (Unemployed, Retired, Student, Formal Work and Informal Work); Schooling (No schooling, Elementary School, High School, Higher Education or more); Monthly family income (No income, Less than 1 minimum wage, 1 to 5 minimum wages, 5 to 10 minimum wages, Over 10 minimum wages); Receives any government aid (Yes, No); Uses the Unified Health System (Yes, No); Receives a visit from the Community Health Agent (Yes, No); You have a Basic Health Unit in your area (Yes, No); You have been diagnosed with COVID-19 (Yes, No); You agree with the compulsory vaccination against COVID-19 (Yes, No); You feel social pressure to get vaccinated against COVID-19 (Yes, No); You trust the efficacy of the vaccine against COVID-19 (Yes, No); Trusts the government's actions regarding the implementation of vaccination in the country (Yes, No); Seeks information about COVID-19 vaccination from official sources (WHO, MS), unofficial sources (TV, radio, social media), non- governmental organizations, health professionals or does not seek information.
When constructing the binary logistic regression model for this study, an exploratory analysis was initially carried out to detect multicollinearity between the independent variables, using the Variance Inflation Factor (VIF). Variables with a VIF greater than 10 were excluded from the statistical modeling [29]. The modeling was carried out using the Backward selection method, which starts with a complete model (with all the independent variables) and removes the variables, checking the behavior of the model according to the VIF values. The best model considered was the one with the lowest Akaike Information Criterion (AIC) value [29].
For the final model, the Odds Ratio (OR) was calculated with their respective 95% Confidence Intervals (95%CI). Once all the possibilities for analysis had been exhausted and the final model chosen (based on the criterion of the lowest AIC value), the Hosmer- Lemeshow, likelihood ratio, Cox-Snell, Nagelkerke and McFadden tests were carried out to validate the model. In addition, the model's predictive capacity and accuracy were verified based on the area under the ROC (Receiver Operating Characteristic) curve and their respective 95% CI values (29). The binary logistic regression and validation tests were carried out using the RStudio 4.3.1 software.
1.7. Ethical Aspects
This study was approved by the Research Ethics Committee (CEP) of the Ribeirão Preto School of Nursing at the University of São Paulo (EERP/USP), with Certificate of Submission for Ethical Appraisal (CAAE) No. 57933622.4.1001.5393. The entire investigation was conducted in accordance with Resolution No. 466 of December 12, 2012 of the National Health Council, taking into account the relevant ethical and scientific foundations.
Participants in the study had to sign the Informed Consent Form (ICF), which they read and signed, and only after agreeing and signing did the inter-view begin. The ICF was structured in two lives, in the case of people with no schooling, fingerprints were taken, each party keeping one copy, and the inter-viewer informed the participant of the importance of keeping the document. It should be noted that participation in the research was voluntary.
3. Results
In the exploratory analysis of secondary data, it was possible to verify that the highest percentage of homeless people reside in the Northeast region of Brazil (Figure 1A). As for the indicators related to COVID-19, the highest densities regarding the percentage of complete vaccination schedules and the incidence and mortality rates for COVID-19 were observed in the Northeast, Southeast and South regions of the country (Figure 1B-D).
Regarding the primary data, a total of 1,392 people living on the streets in Brazil answered the questionnaire, with the majority of respondents being male (n: 961; 69.0%), with an average age of 38.3 years ±15.2 years (minimum age: 23; maximum age: 81), black/brown race/color (n: 1.097; 78.8%), single/divorced/widowed marital status (n: 1,247; 89.6%) and with an elementary school education (n: 1,060; 76.1%). In addition, the majority said they were unemployed (n: 669; 48.0%), had an income of between 1 and 5 minimum wages (n: 648; 46.6%) and did not receive any kind of government aid (n: 809; 58.1%), as shown in Table 1.
Of the 1,392 homeless people, 397 (28.5%) had a confirmed diagnosis of COVID- 19, 1,165 (83.7%) had an incomplete basic schedule against COVID-19 and 869 (62.4%) had a complete basic schedule against COVID-19. Also among the results, 70% (n: 975) said they trusted the efficacy of the vaccines and 63.3% (n: 881) did not feel any social pressure to get vaccinated, as shown in Table 2.
As for access to information, 86.6% (n=1205) of the participants said they looked for general information through the official press, such as TV news, radio and printed newspapers. However, specifically about Covid-19, 87.3% (n=1215) did not seek information about COVID-19 from any source (Table 3).
We identified seven factors associated with the likelihood of having a complete COVID-19 vaccination schedule among PRS, which include receiving government assistance (OR: 1.58; 95%CI: 1.09 - 2.30), visits from Street Clinic Health Agents (OR: 3.19; 95%CI: 1.95 - 5.36), history of COVID-19 diagnosis (OR: 5.77; 95%CI: 3.17 - 11.15), support for mandatory vaccination against COVID-19 (OR: 3.76; 95%CI: 2.48 - 5.76), confidence in the effectiveness of vaccines (OR: 3.92; 95%CI: 2.63 - 5.89), seeking information from NGOs, street clinics, community leaders (OR: 1.91; 95%CI: 1.01 - 3.88) and trust in the Federal Government's statements on vaccines (OR: 1.57; 95%CI: 1.06 - 2.31).
To validate the binary logistic regression model shown in Table 4, we used comprehensive statistical tests, including the Hosmer-Lemeshow test (p: 0.14), the likelihood ratio (p: < 0.01), the CoxSnell (0.24), Nagelkerke (0.42) and McFadden (0.32) indices. It should be noted that the model showed an ROC curve with a value of 0.86, which suggests an effective fit of the established model.
4. Discussion
The study aimed to identify the completeness of the COVID-19 vaccination schedule among persons experiencing homelessness in Brazil. The majority of the study participants were male, black/brown, single, unemployed, living mainly on the street, with primary education and a monthly family income of between 1 and 5 minimum wages and not receiving any kind of government aid.
It can be observed that only 62.4% of the PSR who participated in the study have a complete COVID-19 vaccination schedule, which is below the general population, given that 82% of the population has a complete vaccination sched-ule in the country [4,28]. This disparity in relation to the RSH was also evidenced during the first months of the COVID-19 vaccination campaign in the United States in vulnerable populations [30].
In the Democratic Republic of Congo, people living in situations of social vulnerability [31] revealed that having a vaccine against COVID-19 was not a priority, as other conditions affecting basic human needs were more important at the time. This situation underpins the vaccine discrepancy between populations, making the PSR more likely to be vaccine hesitant and consequently more ex-posed to infection.
Conceptually, vaccine hesitancy is the delay in accepting or refusing vaccination despite the availability of the immunizer. Vaccine hesitancy is complex and has a specific context, varying over time and place, according to societies and different vaccines, and is influenced by factors such as complacency, convenience and confidence [32]. Vaccine hesitancy rates among the homeless population out-side Brazil range from 35.7% to 48% [33,34,35,36] and reluctance to be vaccinated in these populations increases the risk of infection and worsening of the disease.
Coronavirus infection among homeless people points to concerns about public health and health care resources, since even the mildest cases of COVID-19 among homeless people require consideration of isolation sites and management. And incomplete schemes are likely to evolve into the severe form of the disease, implying increased hospitalization and mortality from COVID-19 [36]. People experiencing homelessness and other precarious housing conditions are particularly vulnerable to COVID-19 infection, requiring collaboration between health, social care and government agencies to develop services and prevent the spread of infection [37].
In 2022, the Brazilian Ministry of Health presented a plan to guide the vaccination guidelines against COVID-19 to the Federative Units (UF) and municipalities, collaborating in the planning and operationalization of vaccination against the disease, in which homeless people were included as a priority group for vaccination [4]. To date, the homeless have not yet reached the levels of vaccination completeness recommended by the WHO, the conditions of great social vulnerability and the recognized difficulties of access to health systems and social support are some of the factors that influence these figures [7,38].
One strategy for the success of vaccination completeness is access to information, since it influences the decisions of the PSRs in Brazil. According to the findings, only 12.7% of participants sought information about COVID-19. Among them, the sources were non-governmental organizations, street clinics, health professionals and community leaders. The participants who were most likely to be vaccinated against COVID-19 were precisely those who turned to these sources. In contrast, a study carried out in Los Angeles (USA) [33] showed that obtaining in-formation about the COVID-19 vaccine from sources other than official health agencies, including social media, friends and family, increased the chances of completing the vaccination schedule.
There is a need for clear, easy and accurate access to information and for it to reach the most vulnerable populations, since the absence of information or in-adequate search can lead to misconceptions about vaccination [14,33,37]. This is a worrying phenomenon and can negatively influence adherence to the vaccination schedule. This situation represents a significant obstacle to public health, and strategies to raise awareness about vaccination, especially among vulnerable populations, should be the goal of health programs and services. These programs should emphasize the importance and safety of vaccines, addressing myths and misconceptions. Vaccination programs for these urban populations should also be improved by offering financial incentives, education and facilitating access, while addressing barriers to vaccination and planning future guidelines [37].
Building trust in information in a digital and technological age can be seen in both positive and negative ways. Positive when access to information is quick, easy and in real time. However, this access can bring reliable and true information or false, incomplete news, which can encourage and cause non-adherence to vaccination [4,32].
Supporters of the anti-vaccine movement question the safety of immuno-biologicals and their possible side effects [6]and supporters of the individual freedom movement encourage the right to choose whether or not to be vaccinated. When taken into the context of the PRS, these problems are exacerbated by the economic, social and structural conditions and access to information [4]. Ac-cording to Lin et al. (2020) [39]in addition to vaccination campaigns, permanent health education campaigns should be implemented in a language accessible to all classes, with the participation and involvement of social actors, with the aim of strengthening health actions and programs. Another aspect that deserves attention is trust, both in the efficacy and safety of vaccines and in government actions. It is important to note that people who believed in the efficacy of COVID-19 vaccines were more likely to complete the COVID-19 vaccination schedule and less likely to be incomplete. This finding corroborates the study by Lin et. al. (2020) [39] which found that peo-ple who trusted the efficacy of the vaccine were more likely to agree to take the COVID-19 vaccine.
Another important finding is that homeless people who trusted the federal government when it came to COVID-19 vaccination were more likely to complete the vaccination schedule and less likely to be incomplete. Trust in the actions proposed by the federal government or its health agencies implies trust in collective and social actions to mitigate the impacts suffered by the population, especially in the critical period of the pandemic, where research and production of immunobiologicals were taking place concurrently with the health crisis in the country, such trust had a positive impact on vaccination adherence, albeit late, reaching levels of vaccination coverage in the general population recommended by the World Health Organization. [4].
Research that addressed the themes of collective action, government intervention and the importance of trust showed that a key factor in tackling the spread of COVID-19 is mutual trust, both horizontal trust, between people and the community, and vertical trust, between people and their governments [38,40].
Several studies have been carried out to verify the acceptance of a possible vaccine against COVID-19 in the pandemic period [41] other studies to find out about adherence and/or vaccine hesitancy [39] in the general population. However, few studies have focused on the PRS. Among the studies [39,41]it is clear that the population that is theoretically more exposed to the risk of falling ill is more likely to accept the vaccine than other parts of the population.
It is notorious that the population's health situation is positively linked to self-care, as seen in this study with the greater chance of completing the vaccination schedule against COVID-19 among PIH who were diagnosed with COVID-19. These data corroborate a study carried out in Mozambique in 2021 [34] which showed that the perception of risk of COVID-19 is directly linked to health behavior, and that worrying about (re)infection is recognized as a protective factor that modifies the attitude at the time of vaccination acceptance. Thus, a person who feels at great risk of getting sick may have a more protective behavior and more positive attitudes towards vaccination in general.
Homelessness leads to great social vulnerability, with recognized difficulties in accessing the Brazilian health system and social support. The condition of homeless people deserves special consideration, since this population is naturally susceptible to infection and may be at greater risk of exposure related to the conditions in which they find themselves [7,38]. Homeless people under the age of 65 have an all-cause mortality rate 5 to 10 times higher than that of the general population [42]. COVID-19 infection can increase this disparity, which is alarming to say the least.
Data from this study show that only 33.8% of the homeless who answered the questionnaire reported that they receive visits from health workers and 41.9% receive social assistance. In Brazil, receiving social aid for this population is still a major challenge. The homeless are unaware of their rights, they don't recognize themselves as subjects of rights, there are difficulties in accessing it, mainly due to a lack of documentation, and all of these factors affect the health of this population [43,44]. In this study, people who received government assistance and a visit from a health worker were more likely to complete their vaccination schedule, which highlights the need for integrated strategies that combine social and health support. Receiving visits from health workers and having a Basic Health Unit (BHU) to refer to increase the chances of PSR completing their vaccination schedule. In this sense, we can highlight the power of PHC and the importance of street clinics as a PHC policy for this population.
Including community organizations and local leaders in the actions of health workers can significantly improve the effectiveness of interventions. This community approach can strengthen bonds of trust and facilitate access to health services, thus contributing to improved vaccination coverage and the well-being of this population [45].
It is also important to mention that another factor was associated with the decision to complete the vaccination schedule: the mandatory nature of the vac-cine. In this study, 58.2% of the population agreed that the COVID-19 vaccine should be mandatory. People who agreed that COVID-19 vaccines were mandatory were more likely to complete the vaccination and less likely to incomplete it. Despite being an infectious and contagious disease, with a high morbidity and mortality rate, in Brazil it is not legally possible to vaccinate compulsorily, even in the face of such a health crisis [1].
The study's limitations include the fact that the sample was non-probabilistic, which limits the generalizability of the results. However, snowballing is the most appropriate strategy for reaching vulnerable and/or stigmatized populations, especially since we don't know where they are or how they can be located. It is also important to note that the study was only carried out in Brazil's capitals and Federal District, and did not go into the countryside. This may not fully represent the reality of homeless people throughout the coun-try, although it does provide a relevant overview of the situation of homeless people in terms of the completeness of vaccinations. In addition, the cross- sectional nature of the study prevents the inference of causality between the variables analyzed.
With regard to the exploratory analysis carried out for the situational diagnosis, it is important to mention the limitation of using secondary data, which may contain unavailable or incomplete information and could affect the accuracy of the results obtained. In addition, the population data was derived from projections based on the last official Demographic Census carried out in 2010. Due to this time gap, the demographic data may not fully reflect the reality of the population during the research period, as well as the estimation of PSR, which is based on the CadÚnico registry, which may also not reflect reality, which could influence the analyses carried out.
Another important aspect to note is that in the analysis of secondary data, this study only considered reported COVID-19 cases and deaths, and this notification was based on the diagnosis of COVID-19, which was only carried out on symptomatic individuals tested for the disease. This may not fully represent the real epidemiological scenario in the state. In this respect, it is also important to mention that the COVID-19 testing process has varied across the country and has fluctuated over time. In other words, there have been periods of greater and lesser testing, as well as places that have tested more than others, and this fact can cause a bias in the temporal analyses, not reflecting the real epidemiological scenario at that time.
Future longitudinal studies are recommended to add to the literature on the completeness of the COVID-19 vaccination schedule in the homeless. These studies can explore the influence of various factors on adherence to vaccination over time and identify the barriers faced by homeless people in seeking health information. These insights are key to developing more effective strategies for promoting health and meeting the specific needs of this population.
5. Conclusions
The study highlights the complexity of the factors that influence adherence to vaccination among homeless people in Brazil. These results contribute to the development of public health education strategies in order to increase adherence to individual immunization, favoring collective protection in the homeless population. Although Brazil is a country where vaccine uptake is significant, vaccine hesitancy is already recognized as a public health problem, and this study aims to point out the related factors in order to mitigate the impacts of the pandemic on the homeless population.
Increasing vaccination coverage in homeless populations requires a set of uninterrupted strategic actions that meet the specific needs of this population. In this context, the end of the pandemic emergency points to the risk of a decline in the wide range of actions carried out to mitigate the disease, which could make it even more difficult for this population to access health services and, consequent-ly, restrict access to vaccination if this input is henceforth offered only in non-ambulatory health services. Therefore, it is imperative to make a collective effort for inter-institutional movements that transcend the health sector, guaran-teeing the wide availability of vaccination against COVID-19 for homeless populations, with the aim of reducing the risks of illness and mortality related to the disease in this specific context.
Ultimately, collaboration between different sectors of society becomes cru-cial to address the unique challenges faced by these populations, ensuring equi-table access to protection against the disease for all.
Author Contributions
I declare that the authors JSTA, TZB, HSDM, LPF, ACVR, MCN, GLF e RAA participated in Conceptualization; methodology, formal analysis and writing—review and editing, TZB, LPF, ACVR, MCR participated in data curation; JSTA, TZB, HSDM, LPF, ACVR, MCN, GLF e RAA, YMA, RJR, AFT, RCF and DAS participated in writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the Coordination for the Improvement of Higher Education Personnel—Brazil (CAPES) — Financial Code 001 and Process: 88887.657730/2021-00 - Programa Impactos CAPES and by the São Paulo State Research Support Foundation (FAPESP) number grant 2021/08263 -7; CNPQ (Research Productivity Grant - Process Process: 307014/2022-3).
Institutional Review Board Statement
The study was approved by the Research Ethics Committee of the School of Nursing of Ribeirão Preto at the University of São Paulo, under protocol number CAAE: 57933622.4.1001.5393.
Informed Consent Statement
Written informed consent has been obtained from the participants to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Vilhena A, Bardanachvili E. National Immunization Program (PNI) and Covid-19: challenges to a history of almost half a century of success. Fiocruz Antonio Ivo de Carvalho Center for Strategic Studies. 2021. https://cee.fiocruz.br/?q=Programa- Nacional-de-Imunizacoes-PNI-e-Covid-19 (accessed April 7, 2024).
- Souza LEPF de, Buss PM. Global challenges for equitable access to COVID-19 vaccination. Cad Saúde Pública 2021;37:e00056521. [CrossRef]
- Brazil. Recommendations for the prevention and control of COVID-19 due to the increase in cases of the disease and the circulation of new subvariants of Omicron (VOC). Information Note. State Health Surveillance Center. Rio Grande do Sul Health Department. 2022.
- Brazil. Operational Technical Report on Vaccination Against Covid-19. Ministry of Health. 2023. https://www.gov.br/saude/pt-br/assuntos/covid-19/informes- tecnicos/2023/informe-tecnico-operacional-de-vacinacao-contra-a-covid-19/view (accessed April 7, 2024).
- Brito, C.; da Silva, L.N.; Xavier, C.C.L.; Antunes, V.H.; Costa, M.S.; Filgueiras, S.L. The way of life of the unhoused people as an enhance for COVID-19 care. Rev. Bras. de Enferm. 2021, 74, e20200832. [Google Scholar] [CrossRef]
- Melo, L.J.F.; Aragão, F.B.A.; Cunha, J.H.D.S.; Carneiro, T.G.; Fiorati, R.C. Accessibility and quality of life of homeless people and primary care. Revista Família, Ciclos de Vida e Saúde no Contexto Social 2022, 10, 57–67. [Google Scholar] [CrossRef]
- Honorato, B.E.F.; Oliveira, A.C.S. Homeless people and COVID-19. Rev Adm Pública 2020, 54, 1064–1078. [Google Scholar] [CrossRef]
- Natalino M. Nota Técnica no 103. Estimativa da Populacão em Situação de Rua no Brasil (2012-2022). Directorate of Social Studies and Policies (Disoc) 2023.
- Meehan, A.A.; Yeh, M.; Gardner, A.; DeFoe, T.L.; Garcia, A.; Kelen, P.V.; Montgomery, M.P.; Tippins, A.E.; Carmichael, A.E.; Gibbs, C.R.; et al. COVID-19 Vaccine Acceptability Among Clients and Staff of Homeless Shelters in Detroit, Michigan, February 2021. Heal. Promot. Pr. 2021, 23, 35–41. [Google Scholar] [CrossRef]
- Ahillan, T.; Emmerson, M.; Swift, B.; Golamgouse, H.; Song, K.; Roxas, A.; Mendha, S.B.; Avramović, E.; Rastogi, J.; Sultan, B. COVID-19 in the homeless population: a scoping review and meta-analysis examining differences in prevalence, presentation, vaccine hesitancy and government response in the first year of the pandemic. BMC Infect. Dis. 2023, 23, 1–16. [Google Scholar] [CrossRef]
- Abramovich, A.; Pang, N.; Kunasekaran, S.; Moss, A.; Kiran, T.; Pinto, A.D. Examining COVID-19 vaccine uptake and attitudes among 2SLGBTQ+ youth experiencing homelessness. BMC Public Heal. 2022, 22, 1–12. [Google Scholar] [CrossRef]
- Iacoella, C.; Ralli, M.; Maggiolini, A.; Arcangeli, A.; Ercoli, L. Acceptance of COVID-19 vaccine among persons experiencing homelessness in the City of Rome, Italy. Eur Rev. Med. Pharmacol. Sci 2021, 25, 3132–3135. [Google Scholar]
- Goode, J.-V.R.; Cook, P.; Cuttino, S.; Gatewood, S.B.S. Early experience with COVID-19 vaccine in a Federally-Qualified Healthcare Center for the homeless. Vaccine 2021, 39, 7131–7134. [Google Scholar] [CrossRef]
- Nguyen, D.A.; Alagbo, H.O.; Hassan, T.A.; Mera-Lojano, L.D.; Abdelaziz, E.O.; The, N.P.N.; Makram, A.M.; Makram, O.M.; Elsheikh, R.; Huy, N.T. Vaccine acceptance, determinants, and attitudes toward vaccine among people experiencing homelessness: a systematic review and meta-analysis. BMC Infect. Dis. 2023, 23, 1–21. [Google Scholar] [CrossRef]
- Roederer, T.; Mollo, B.; Vincent, C.; Leduc, G.; Sayyad-Hilario, J.; Mosnier, M.; Vandentorren, S. Estimating COVID-19 vaccine uptake and its drivers among migrants, homeless and precariously housed people in France. Commun. Med. 2023, 3, 30. [Google Scholar] [CrossRef]
- Liang, Y.; Sun, Q.; Liu, Q.; Pang, Y.; Tang, S. SARS-CoV-2 incidence, seroprevalence, and COVID-19 vaccination coverage in the homeless population: a systematic review and meta-analysis. Front. Public Heal. 2023, 11, 1044788. [Google Scholar] [CrossRef]
- Bolfarine H, Bussab WDO. Elements of sampling. São Paulo: Edgar Blücher; 2005.
- Etikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of Convenience Sampling and Purposive Sampling. Am. J. Theor. Appl. Stat. 2016, 5, 1–4. [Google Scholar] [CrossRef]
- Pedro, A.R.; Gama, A.; Soares, P.; Moniz, M.; Laires, P.A.; Dias, S. COVID-19 Barometer: Social Opinion – What Do the Portuguese Think in This Time of COVID-19? Port. J. Public Heal. 2020, 38, 42–50. [Google Scholar] [CrossRef]
- Marques, J.B.V.; de Freitas, D. Método DELPHI: caracterização e potencialidades na pesquisa em Educação. 2018, 29, 389–415. [Google Scholar] [CrossRef]
- Zarili, T.F.T.; Castanheira, E.R.L.; Nunes, L.O.; Sanine, P.R.; Carrapato, J.F.L.; Machado, D.F.; Ramos, N.P.; Mendonça, C.S.; Nasser, M.A.; Andrade, M.C. Delphi technique in the validation process of the Primary Care Evaluation Questionnaire (QualiAB) for national application. Saude soc 2021, 30, e190505. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Peng, K.; Li, X.; Yang, D.; Chan, S.C.; Zhou, J.; Wan, E.Y.; Chui, C.S.; Lai, F.T.; Wong, C.K.; Chan, E.W.; et al. Risk of autoimmune diseases following COVID-19 and the potential protective effect from vaccination: a population-based cohort study. EClinicalMedicine 2023, 63, 102154. [Google Scholar] [CrossRef]
- Brazil. Brazilian Observatory of Public Policies with the Homeless Population. Faculty of Law. Federal University of Minas Gerais. 2022. https://obpoprua.direito.ufmg.br/ (accessed April 7, 2024).
- Brazilian Institute of Geography and Statistics. Estimates of the resident population for municipalities and federation units. 2023.https://www.ibge.gov.br/estatisticas/sociais/populacao/9103-estimativas-de- populacao.html (accessed April 7, 2024).
- Brasil. Ministério da Saúde Coronavírus Brasil. Brasília. 2021. Available online: https://covid.saude.gov.br (accessed on 12 October 2020).
- Brazil. COVID-19 Vaccinometer. Ministry of Health. 2024. https://infoms.saude.gov.br/extensions/SEIDIGI_DEMAS_Vacina_C19/SEIDIGI_ DEMAS_Vacina_C19.html (accessed April 7, 2024).
- Zuur, A.F.; Ieno, E.N.; Elphick, C.S. A protocol for data exploration to avoid common statistical problems. Methods Ecol. Evol. 2010, 1, 3–14. [Google Scholar] [CrossRef]
- Barry, V.; Dasgupta, S.; Weller, D.L.; Kriss, J.L.; Cadwell, B.L.; Rose, C.; Pingali, C.; Musial, T.; Sharpe, J.D.; Flores, S.A.; et al. Patterns in COVID-19 Vaccination Coverage, by Social Vulnerability and Urbanicity — United States, December 14, 2020–May 1, 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 818–824. [Google Scholar] [CrossRef]
- Claude, K.M.; Serge, M.S.; Alexis, K.K.; Hawkes, M.T. Prevention of COVID-19 in Internally Displaced Persons Camps in War-Torn North Kivu, Democratic Republic of the Congo: A Mixed-Methods Study. Glob. Heal. Sci. Pr. 2020, 8, 638–653. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, R.; Henwood, B.; Lawton, A.; Kleva, M.; Murali, K.; King, C.; Gelberg, L. COVID-19 vaccine access and attitudes among people experiencing homelessness from pilot mobile phone survey in Los Angeles, CA. PLOS ONE 2021, 16, e0255246. [Google Scholar] [CrossRef] [PubMed]
- Dula, J.; Mulhanga, A.; Nhanombe, A.; Cumbi, L.; Júnior, A.; Gwatsvaira, J.; Fodjo, J.N.S.; Villela, E.F.d.M.; Chicumbe, S.; Colebunders, R. COVID-19 Vaccine Acceptability and Its Determinants in Mozambique: An Online Survey. Vaccines 2021, 9, 828. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef]
- Aguiar A, Meireles P, Rebelo R, Barros H. COVID-19 and homelessness: No one can be left behind 2020.
- Wood, S.P. Vaccination Programs among Urban Homeless Populations: A Literature Review. J. Vaccines Vaccin. 2012, 3. [Google Scholar] [CrossRef]
- Hino, P.; Santos, J.d.O.; Rosa, A.d.S. People living on the street from the health point of view. Rev. Bras. de Enferm. 2018, 71, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Corrêa SMC, Vasconcelos PF de, Passos JS dos, Marques VG, Tanajura NPM, Nascimento DR do, et al. The possible causes of non-adherence to immunization in Brazil: a literature review | Revista Eletrônica Acervo Saúde 2021.
- Knight, K.R.; Duke, M.R.; Carey, C.A.; Pruss, G.; Garcia, C.M.; Lightfoot, M.; Imbert, E.; Kushel, M. COVID-19 Testing and Vaccine Acceptability Among Homeless-Experienced Adults: Qualitative Data from Two Samples. J. Gen. Intern. Med. 2021, 37, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Brazil. Manual on health care for the homeless population. Ministry of Health. Health Care Secretariat. Department of Primary Care. DF: Brasília: Ministry of Health; 2012.
- Brazil. Manual on health care for the homeless population. Ministry of Health. Health Care Secretariat. Department of Primary Care. DF: Brasília: Ministry of Health; 2015.
- Mecenero AC. Homeless Population and Social Rights, 2022.
- Platt, L.; Rathod, S.D.; Cinardo, P.; Guise, A.; Hosseini, P.; Annand, P.; Surey, J.; Burrows, M. Prevention of COVID-19 among populations experiencing multiple social exclusions. J. Epidemiology Community Heal. 2021, 76, 107–108. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Density of the estimated homeless population and indicators related to COVID- 19, Brazil (2020-2024). Legend: (A) Density of the percentage of the homeless population; (B) Density of the percentage of the population that has completed the COVID-19 vaccination schedule; (C) Density of the COVID-19 incidence rate; (D) Density of the COVID-19 mortality rate.
Figure 1.
Density of the estimated homeless population and indicators related to COVID- 19, Brazil (2020-2024). Legend: (A) Density of the percentage of the homeless population; (B) Density of the percentage of the population that has completed the COVID-19 vaccination schedule; (C) Density of the COVID-19 incidence rate; (D) Density of the COVID-19 mortality rate.
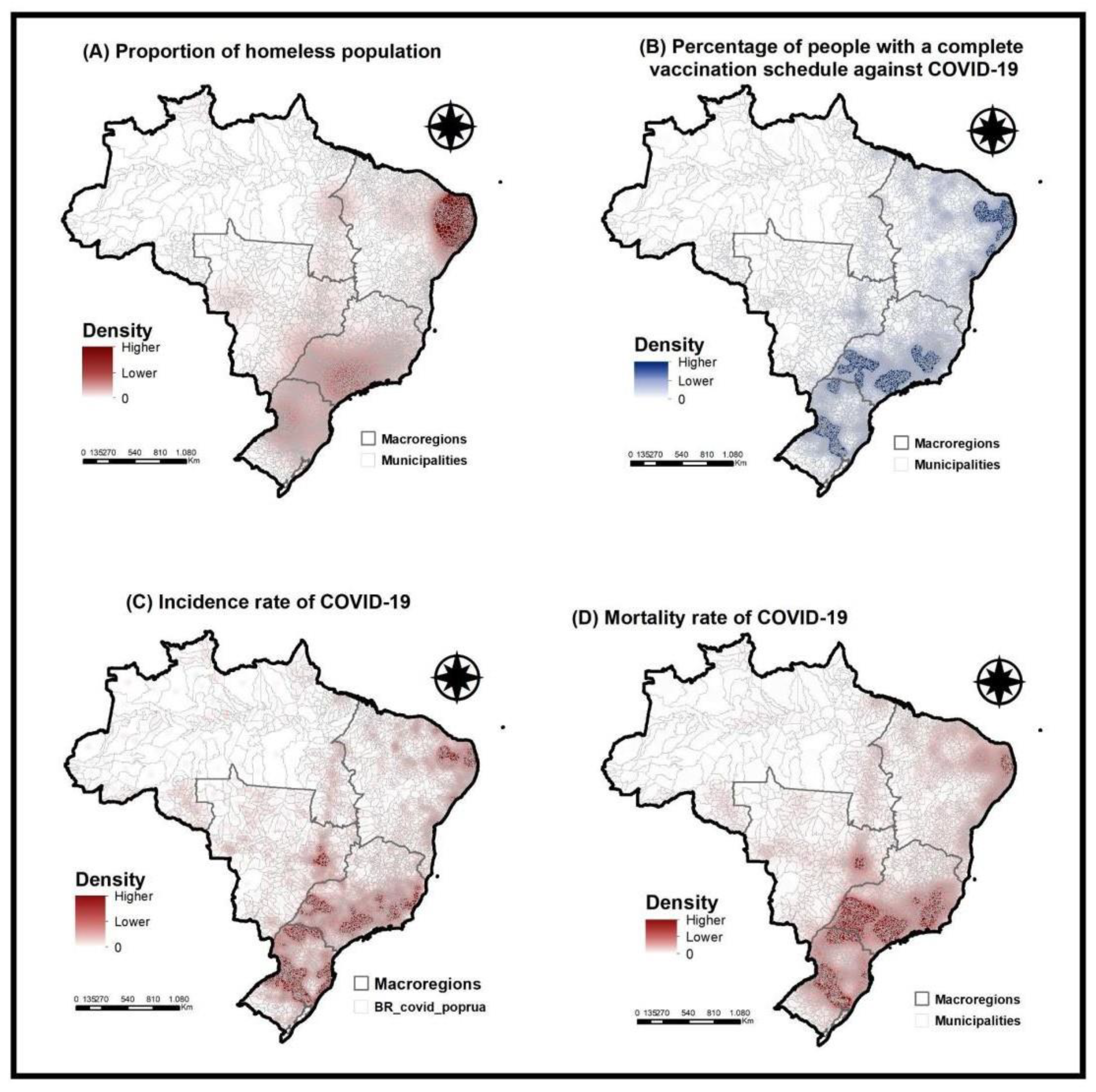

Table 1.
Sociodemographic profile of people living on the streets, Brazil, 2022-2023.
| Variables | Frequency (n) |
% |
|---|---|---|
| Gender | ||
| Male | 961 | 69,0 |
| Female | 429 | 30,8 |
| Others | 2 | 0,2 |
| Race/Color | ||
| Black/Brown | 1097 | 78,8 |
| White | 295 | 21,2 |
| Marital status | ||
| Single, Divorced, Widowed | 1247 | 89,6 |
| Married/stable union | 145 | 10,4 |
| Occupation | ||
| Unemployed | 669 | 48,0 |
| Informal | 328 | 23,6 |
| Formal | 229 | 16,5 |
| Retired | 96 | 6.9 |
| Student | 70 | 5,0 |
| Education | ||
| Fundamental | 1060 | 76,1 |
| High School | 273 | 19,6 |
| Higher or more | 53 | 3,9 |
| No schooling | 6 | 0.4 |
| Income in minimum wage | ||
| Above 10 | 2 | 0,1 |
| From 1 to 5 | 648 | 46,6 |
Table 2.
COVID-19 diagnosis, vaccination schedule and PSR perceptions of measures to deal with the pandemic. Brazil, 2022-2023.
Table 2.
COVID-19 diagnosis, vaccination schedule and PSR perceptions of measures to deal with the pandemic. Brazil, 2022-2023.
| Variables | Frequency (n) |
% |
|---|---|---|
| Diagnosed with COVID-19 | ||
| Yes | 397 | 28,5 |
| No | 981 | 70,5 |
| I don't know | 14 | 1,0 |
|
Incomplete basic scheme against COVID-19 | ||
| Yes | 1165 | 83,7 |
| No | 227 | 16,3 |
|
Complete basic scheme against COVID- 19 | ||
| Yes | 869 | 62,4 |
| No | 523 | 37,6 |
|
Do you feel social pressure to take the COVID-19 vaccine? | ||
| Yes | 416 | 29,9 |
| No | 881 | 63,3 |
| I don't know | 95 | 6,8 |
|
Do you agree with mandatory vaccination against COVID-19? | ||
| Yes | 810 | 58,2 |
| No | 488 | 35,1 |
| I don't know | 94 | 6,8 |
| Trust in the effectiveness of vaccines | ||
| Yes | 975 | 70,0 |
| No | 325 | 23,3 |
| I don't know | 92 | 6,6 |
|
Trust in the federal government's actions on vaccines | ||
| Trust | 959 | 68,9 |
| Doesn't trust | 325 | 23,3 |
| I don't know | 108 | 7,8 |
|
Trusts the state government's actions on vaccines | ||
| Trust | 1018 | 73,1 |
| Doesn't trust | 267 | 19,2 |
| I don't know | 107 | 7,7 |
|
Trusts the actions of the municipal government on vaccines | ||
| Trust | 1014 | 72,8 |
| Doesn't trust | 271 | 19,5 |
| I don't know | 107 | 7,7 |
Table 3.
Sources of information about the COVID-19 vaccine by homeless people, Brazil, 2022-2023.
| Variables | Frequency (n) | % |
|---|---|---|
| Sources of official information | ||
| No | 1320 | 94,8 |
| Yes | 72 | 5,2 |
| Unofficial sources of information | ||
| No | 1305 | 93,8 |
| Yes | 87 | 6,3 |
| Health professionals | ||
| No | 1107 | 79,5 |
| Yes | 285 | 20,5 |
| Social media | ||
| No | 1234 | 88,6 |
| Yes | 158 | 11,4 |
|
NGOs, street clinics, community leaders |
||
| No | 1207 | 86,7 |
| Yes | 185 | 13,3 |
| Official press | ||
| No | 187 | 13,4 |
| Yes | 1205 | 86,6 |
| Searched for information | ||
| No | 1215 | 87,3 |
| Yes | 177 | 12,7 |
Table 4.
- Factors associated with completeness of the vaccination schedule among homeless people, Brazil, 2022-2023.
Table 4.
- Factors associated with completeness of the vaccination schedule among homeless people, Brazil, 2022-2023.
| Variable | Coefficient | Odds Ratio (95%CI) | p-value |
|---|---|---|---|
| Gender Male | -0,34 | 0,70 [0,46 - 1,06] | 0,09 |
| Received any kind of government aid | 0,45 | 1,58 [1,09 - 2,30] | 0,01* |
| Uses SUS | 0,45 | 1,58 [0,99 - 2,50] | 0,06 |
| Visited by ACS | 11,61 | 3,19 [1,95 - 5,36] | <0,01* |
| UBS in the neighborhood | -0,49 | 0,60 [0,40 - 0,91] | 0,01* |
| There was COVID-19 | 17,53 | 5,77 [3,17 - 11,15] | <0,01* |
| Do you agree with mandatory vaccinations? |
13,27 | 3,76 [2,48 - 5,76] | <0,01* |
| Believes in the effectiveness of vaccines |
13,68 | 3,92 [2,63 - 5,89] | <0,01* |
| Searched for unofficial information to stay informed about COVID-19 |
-32,17 | 0,04 [0,01 - 0,25] | <0,01* |
| He sought information from NGOs, street clinics, community leaders to keep himself informed about COVID-19 | 0,64 | 1,91 [1,01 - 3,88] | 0,04* |
| You have sought information from the official press to stay informed about COVID-19 |
-30,89 | 0,04 [0,01 - 0,23] | <0,01* |
| Did not seek information to stay informed about COVID-19 |
-0,97 | 0,37 [0,24 - 0,59] | <0,01* |
| Potential level of trust in the federal government over vaccines |
0,45 | 1,57 [1,06 - 2,31] | 0,02* |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



