
Submitted:
11 April 2024
Posted:
15 April 2024
You are already at the latest version
Abstract
A significant portion of fatalities stemming from acute myocardial infarction (AMI) occur suddenly and without warning. This can be prevented through early detection of coronary stenosis. In recent years, coronary artery calcium (CAC) and computed tomography coronary angiography (CTCA) have been utilized. For instance, a 55-year-old interventional cardiologist had a CAC of 58 with 50% stenosis involving his left anterior descending (LAD) artery. Despite possibly having vulnerable plaque, which carries significant future cardiovascular events, the patient followed a plant-based diet (PBD), took supplements, and continued optimal medical therapy (OMT). After three years, there was a significant regression in both CAC and stenosis. During our discussion, we emphasized the importance of food selection, quantification, and how food is processed (raw) to achieve maximal benefit in regressing atherosclerosis. Additionally, we highlighted the importance of identifying the possibility of vulnerable plaque and the mechanism stabilizing it. The case supported the guidelines set by the American College of Cardiology (ACC) and the American Heart Association (AHA) for managing chronic coronary syndrome (CCS) by emphasizing OMT and lifestyle changes. We hope that in the future, more doctors and patients will take responsibility for implementing lifestyle changes rather than solely relying on medications and sophisticated medical technologies.
Keywords:
plant-based diet
; atherosclerotic
; vulnerable plaque
; supplements
Introduction
Over half of all fatalities resulting from cardiovascular disease (CVD) occur without prior symptoms or diagnosis, what we call silent ischemia [1]. Coronary artery calcium (CAC) and computed tomography coronary angiography (CTCA) are crucial tools for evaluating risk and stratifying individuals as low, moderate, or high risk for future coronary events [2]. Nowadays, it is easy to access such tests. This tool, in addition to risk stratification, is also crucial for determining the appropriate preventive therapy for asymptomatic patients. Clinicians must decide whether to administer further functional tests to identify the presence of silent ischemia, such as using a treadmill test or nuclear imaging, or invasive coronary angiography with sophisticated tools to determine the functional significance of coronary blockages with FFR or to determine the anatomy of the plaque (the size and characteristics) with coronary imaging techniques like intravascular ultrasound (IVUS) or optical coherence tomography (OCT). Ultimately, the decision lies in the hands of the physician who is responsible for the patient's care. Similarly, it is a patient's decision to determine the appropriate intervention for their condition, even in cases of severe symptomatic obstruction. Patients have the right to choose medical therapy over invasive procedures, such as percutaneous coronary intervention (PCI) or coronary artery bypass surgery.
The method of treating patients with stable coronary disease (stable angina) has evolved considerably in recent years, particularly with the introduction of the term chronic coronary syndrome (CCS). A series of large, multicenter studies have reached a consensus: in individuals with CCS, long-term treatment with intensive/ optimal medical therapy (OMT) produces the same cardiovascular outcomes as PCI plus OMT. The Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial involved 2287 patients with severe coronary artery disease (CAD) and CCS who were randomly assigned to either PCI plus OMT or OMT alone [3]. The results showed that stenting in a coronary artery did not reduce the risk of death, myocardial infarction, or other major cardiovascular events compared to medical therapy, and there were no significant differences in the improvement of anginal symptoms between the two groups. In a double-blind, randomized, placebo-controlled trial known as the Objective Randomized Blinded Investigation with Optimal Medical Therapy of Angioplasty in Stable Angina (ORBITA), 230 patients with ischemic symptoms were randomly assigned to either PCI or OMT. The primary endpoint was exercise tolerance at the end of six weeks. The study authors concluded that PCI did not increase exercise tolerance more than patients who received solely OMT [4]. In 2020, the International Study of Comparative Health Effectiveness with Medical and Invasive Approaches (ISCHAEMIA) trial was published, a randomized controlled trial comparing PCI and OMT for 5179 patients with CCS. This study demonstrated no significant difference in ischemic CV events or mortality between treatment groups over a median of 3.2 years [5]. Therefore, patients with CCS who fit the profile of those in ISCHAEMIA and do not have left main of at least 50%, left ventricular systolic function <35%, New York Heart Association Class III or IV heart failure, and estimated glomerular filtration rate (eGFR) <30ml/min, or have unacceptable angina despite OMT, can be treated with OMT alone. According to the study, patients who underwent PCI had better quality of life measures than those in the OMT arm [6]. Recently, Stone et al. conducted a sub-analysis of the ISCHAEMIA trial and concluded that the clinical outcomes of patients in the PCI arm may be improved if complete revascularization, particularly anatomic complete revascularization or ACR, is achieved [7].
68% of myocardial infarctions (MI) are attributable to stenosis of less than 50% [8]. Stenosis of this type may indicate a vulnerable plaque, which is often ignored during coronary angiography and may not receive the appropriate treatment. A variety of advanced, invasive diagnostic tools are currently available for detecting vulnerable plaques, including IVUS in combination with OCT, or hybrid IVUS-OCT/OFDI, NIRS-IVUS (near-infrared spectroscopy), NIRF-IVUS (near-infrared fluorescence), IVPA-IVUS (molecular imaging intravascular photoacoustics), and TRFS-IVUS (time-resolved fluorescence spectroscopy) [9,10]. However, these highly sophisticated tools are not widely accessible in developing countries like Indonesia due to their high cost. One option is to use CTCA, but interpreting vulnerable plaque accurately may require an experienced radiologist.
Recent publications have emphasized the importance of intervening in vulnerable plaques to reduce major adverse cardiovascular events (MACE) and improve patient survival. It is important to note that vulnerable plaque may not cause clinical ischemia or even show negative results in invasive functional tests, such as FFR. However, it may put the patient at risk for future clinical events. If an asymptomatic individual has a stenosis ranging from 40-70% according to the most recent 2023 ACC/AHA guideline for managing CCS, they should receive OMT instead of undergoing further testing to identify vulnerable plaque [11]. Is this the best way to do it?
In April 2024, Park SJ et al. published a noteworthy paper titled "Preventive PCI versus OMT alone for the treatment of vulnerable atherosclerotic coronary plaques (PREVENT)." This study was a multicenter randomized controlled trial that demonstrated that patients with non-flow-limiting vulnerable plaques ( angiographic stenosis of 47-66%) experienced a reduction in MACE when they received preventive PCI using stenting, as opposed to OMT. Given that PREVENT is the first large trial involving 1606 patients to show the potential effect of the local treatment on vulnerable plaques, these findings support consideration to expand indications for PCI to include non-flow-limiting high-risk vulnerable plaques [12,13]. As an interventional cardiologist, I harbor reservations about employing stents to manage vulnerable plaque. This is due to the potential drawbacks associated with their use, such as in-stent restenosis (ISR) and stent thrombosis (ST). In light of these concerns, I am intrigued by the emerging technology of drug-coated balloons (DCB), which promises to leave nothing behind. In late 2023, a study conducted by van Veelen et al. (DEBuT-LRP) indicated the safety and feasibility of utilizing DCBs to promote the stabilization of vulnerable plaque, thereby preventing the development of future adverse events [14]. However, the study was limited to only 20 patients and utilized NIRS-IVUS, which is not widely available.
Managing patients with a significant coronary plaque burden but without symptoms or significant obstruction is a common challenge in cardiology. Although these lesions may not cause significant narrowing of the arteries, research has shown that they are a major predictor of cardiovascular events and death [15]. Therefore, it is important to carefully monitor and manage these patients to reduce their risk of adverse outcomes.
Remember that guidelines, although beneficial, are not mandatory and are subject to change over time as new ideas emerge from innovative and daring individuals who strive to improve the academic world. If no one were to challenge the status quo, guidelines would remain static and unchanged since their initial release.
2. Case Description
Dr. DM, an interventional cardiologist aged 55 years and asymptomatic, underwent a CTCA without any previous cardiac history. His CTCA results were normal two years prior, with a calcium score 0. His most recent treadmill test also showed normal results. Upon presentation at the cardiology clinic, he had a BMI of 23 kg/mm2, a systolic blood pressure of 110 mmHg, a diastolic blood pressure of 76 mmHg, and a heart rate (HR) of 64 pulses per minute. His blood glucose level was 95 mg/dL, and his serum creatinine was 0.9 mg/dL. The laboratory results showed HbA1C at 5.7%, LDL at 70 mg/dL, HDL at 38 mg/dL, Lp (a) at 40 mg/dL (desirable threshold of <14 mg/dL), and elevated hs-CRP of 3.0 mg/L which was three times the upper limit. He has been following an omnivorous diet since childhood. Additionally, there is a strong family history of cardiovascular disease, as both his father and mother experienced heart attack and stroke at an early age. He exercised regularly (> 150 minutes of moderate exercise per week) and maintained a low weight through restricted calorie intake. He had been taking statin and ezetimibe for over 15 years and had consistently maintained his LDL levels in accordance with ACC/AHA guidelines.
The assessment and quantification of his atherosclerotic plaque were accomplished using a 128-slice CTCA. During the procedure, a non-ionic contrast was administered, and his resting heart rate was 60 beats per minute, with a breath hold of 15 seconds. The CTCA revealed a calcium score of 58, concentrated in the proximal LAD, with a lesion of approximately 50%. The plaque was characterized as calcified, fibrotic, and containing a lipid core. The plaque measurements were 24.2 mm3 for the calcified plaque, 96.4 mm3 for the fibrotic plaque, and 15 mm3 for the lipid core. He underwent myocardial perfusion scanning, which was unremarkable.
He decided to enter a lifestyle program to regress/reverse his coronary atherosclerotic plaque. He increased his statin dosage and continued on ezetimibe. He started on low-dose clopidogrel to change his platelet hyperaggregation state to hypoaggregation. He took many supplements as he went along with his lifestyle program (adopting a PBD, avoiding unhealthy foods, and continue doing regular exercise) to maximize the effect of a PBD upon reversing atherosclerotic plaque.
Three years after implementing a lifestyle intervention, his BMI decreased to 21 kg/m2. Additionally, his blood pressure and pulse remained unchanged from three years prior. His HbA1C level significantly decreased to 5.2%, while his LDL cholesterol levels decreased to 50 mg/dL. His Lp(a) level decreased by 40%, and HDL cholesterol increased by 30%. His hs-CRP levels became normalized ( one of the indicators of systemic inflammation), and he regularly measured his nitric oxide (NO) levels using an NO strip under his tongue [16]. Additionally, he ensured that his urine readings remained alkaline most of the time (alkaline urine is one of the markers of following a correct PBD).
It is now time to assess the progress of his lifestyle and supplementation intervention, as well as the outcome of his CAC/ CTCA after three years: The CAC/ CTCA findings showed a calcium score of 42, which had regressed by 28% from 58, and his proximal LAD lesion, which was previously 50%, had decreased to 30%, a regression of 40%. The measurements of the plaque were 17.3 mm3, regressed by approximately 30% for the calcified plaque, 57.8 mm3, regressed by 40% for the fibrotic plaque, and 7.3 mm3, regressed by 50% for the lipid core, as can be seen in Figure 1.
3. Discussion
Is it possible to reverse coronary artery disease? When patients ask their doctors if they can help shrink their coronary artery plaque, many doctors may not know the answer. Some cardiologists may suggest lifestyle changes and statins in combination with ezetimibe or a new anti-lipid injection PCSK9 inhibitor [17]. However, in reality, I have rarely seen any of my patients successfully regress their coronary calcium or stenosis simply by using the doctor’s magic word “changing your lifestyle” and taking high-dose statins or ezetimibe. Prior to my diagnosis of coronary atherosclerotic plaque, as outlined in the case report, I had consistently maintained what I believe was a “healthy lifestyle” due to my strong positive family history of CVD, elevated Lp(a) level, and low HDL, all of which contributed to my CVD risk. Therefore, I have been prescribed statins in conjunction with ezetimibe since their inception in the early 1990s and have adhered to the international lipid guidelines recommended by the European Society of Cardiology (ESC) or the ACC/AHA, which have evolved over time. Currently, the recommended LDL level is below 55 mg/dL. Metabolically, I was not overweight, had normal blood pressure, engaged in moderate exercise, effectively managed stress, obtained adequate sleep, abstained from smoking, and consumed almost no alcohol. Even though I adopted an omnivorous diet in the past, I paid close attention to my food choices, limiting my consumption of saturated fats and refined carbohydrates.
I am confident that my coronary experience is not unique, as I have observed many of my colleagues who were disheartened upon being diagnosed with coronary obstruction. In the past, the guidelines recommended intervening in cases of significant coronary obstruction, such as stenosis above 50% or 70%, and many of my colleagues underwent PCI as a result. Unfortunately, they were not aware that regression or reversal of coronary stenosis was possible. Does this sad reality change now? Apparently not. Not only in my country but also in the United States, until now, the program of reversing/regressing coronary plaques has been confined by professionals who have truly learned how the program may work. In my experience, learning the real healthy lifestyle to regress or reverse coronary plaque is quite challenging, time-consuming, and full of sacrifices.
Numerous studies have underscored the critical significance of PBDs in managing chronic inflammatory diseases, including atherosclerosis, hyperlipidemia, obesity, non-insulin-dependent diabetes mellitus (NIDDM), and hypertension. It has been widely acknowledged that PBD may not only contribute to the prevention of atherosclerosis but may also cause regression of coronary plaques that have occurred [18,19,20,21,22,23,24]. The role of PBDs as an anti-inflammatory, immunomodulatory, and assisting vascular healing (important following intervention) has been recognized and published as beneficial in chronic inflammatory diseases, especially atherosclerosis. Consuming PBD in conjunction with anti-platelet drugs may aid in mitigating thrombosis processes, potentially reducing the risk of developing acute coronary syndrome (ACS) [25,26,27,28,29,30,31]. This is particularly relevant for managing vulnerable plaque, as it may lessen the future potential for the plaque to cause an ACS.
Atherosclerosis is a systemic disease resulting from metabolic dysfunction and persistent inflammation rather than a localized process. Consequently, it is classified as a metabolic chronic inflammatory condition. Patients who have experienced coronary obstruction due to the atherosclerosis process have typically exhibited a state of metabolic disorder and systemic inflammation for a prolonged period. Cardiologists who exclusively employ interventions such as using stent implantation or DCB technology to manage systemic diseases are likely to be disappointed if they do not address these systemic issues. Following coronary interventions, the balloon causes localized arterial distortion, and the implantation of a foreign body, such as a stent, or using a drug-coated balloon (DCB) results in a healing process for the local injury. However, the systemic environment plays a significant role in the local healing process. At a minimum, the systemic process of atherosclerosis continues to develop. Even if a patient does not experience ISR or ST, there may still be an ongoing atherosclerosis process that could form new coronary stenosis in the vessels distinct from those treated with coronary interventions. As such, it is not advisable to manage patients with coronary atherosclerotic plaque solely by addressing the local vessel issue. This explains why clinical trials that compared PCI with OMT have produced disappointing results for PCI. Interventional cardiologists often neglect the metabolic and systemic issues of their patients, leading to increased MACE after coronary intervention. They may be unable to perform complete revascularization due to complex, challenging coronary anatomies or high-risk interventions. These interventions can only be performed at top centers with minimal complications. These factors may create significant negative outcomes during the comparison study, PCI vs OMT. Studies have shown complete revascularization (CR) is only achieved in approximately 50% of PCI cases [6,32,33,34,35,36,37,38]. Additionally, as previously discussed, they tend to overlook the presence of vulnerable plaques.
In 1998, a small randomized controlled trial known as the Lifestyle Heart Trial was conducted by Ornish et al. The study demonstrated that intensive lifestyle changes with PBD could reverse coronary atherosclerosis. The most important mechanism of this process is the repair of endothelial dysfunction [39]. In 2014, Esselstyn et al. presented a famous image, as depicted in Figure 2, which illustrated strict PBD (without oil) can regress coronary stenosis [40].
It has been a decade since the remarkable research studies on atherosclerosis have garnered significant praise and acceptance within the PBD community and among practitioners who recommend PBD. Despite this, the widespread adoption of recommending PBD to patients has not been extensively embraced within the interventional cardiology community. As an interventional cardiologist myself, I initially had reservations about these findings. However, after being diagnosed with coronary stenosis on my CAC/ CTCA, I decided to follow the advice of these PBD experts. Experience in my case also has been applied to many of my patients and almost all showed regression and reversal of their coronary obstructions. Moreover, I found that this method effectively reduced the incidence of my patient’s ISR and ST [41].
Eating poor-quality food that is high in sugar (refined carbohydrate), devoid of fiber-phytonutrients, highly processed, and contains saturated and trans fats, cholesterol, and chemicals that promote chronic inflammation is a major contributor to the development of atherosclerosis. The consumption of these unhealthy foods has been demonstrated to increase levels of LDL cholesterol, triglycerides, apolipoprotein (a), apolipoprotein (b), C-reactive protein (CRP), pro-inflammatory mediators, pro-inflammatory chemokines/ cytokines, Trimethylamine N-oxide (TMAO), persistent organic pollutants (POPs), oxidative stress, tumor promotion, and cell proliferation, among other factors. All of these factors play a significant role in the development of atherosclerosis and make plaque more vulnerable [42,43]. On the contrary, eating healthy PBD with adequate supplementation will enhance our body's ability to fight against inflammation. Healthy foods such as vegetables, fruits, and legumes contain carotenoids, isoflavones, phytoestrogens, and phytosterols, which have been shown to prevent atherosclerosis. These polyphenols and phytochemicals' role in molecular signaling are anti-inflammatory, antiplatelet aggregation, inhibitor to VSMCs proliferation and migration, and safeguard for lipid oxidation [44,45]. Oxidized LDL (ox-LDL), in addition to its infamous role in causing atherosclerosis, also plays a significant part in developing vulnerable plaque [46]. Healthy PBD will also help to restore endothelial function.
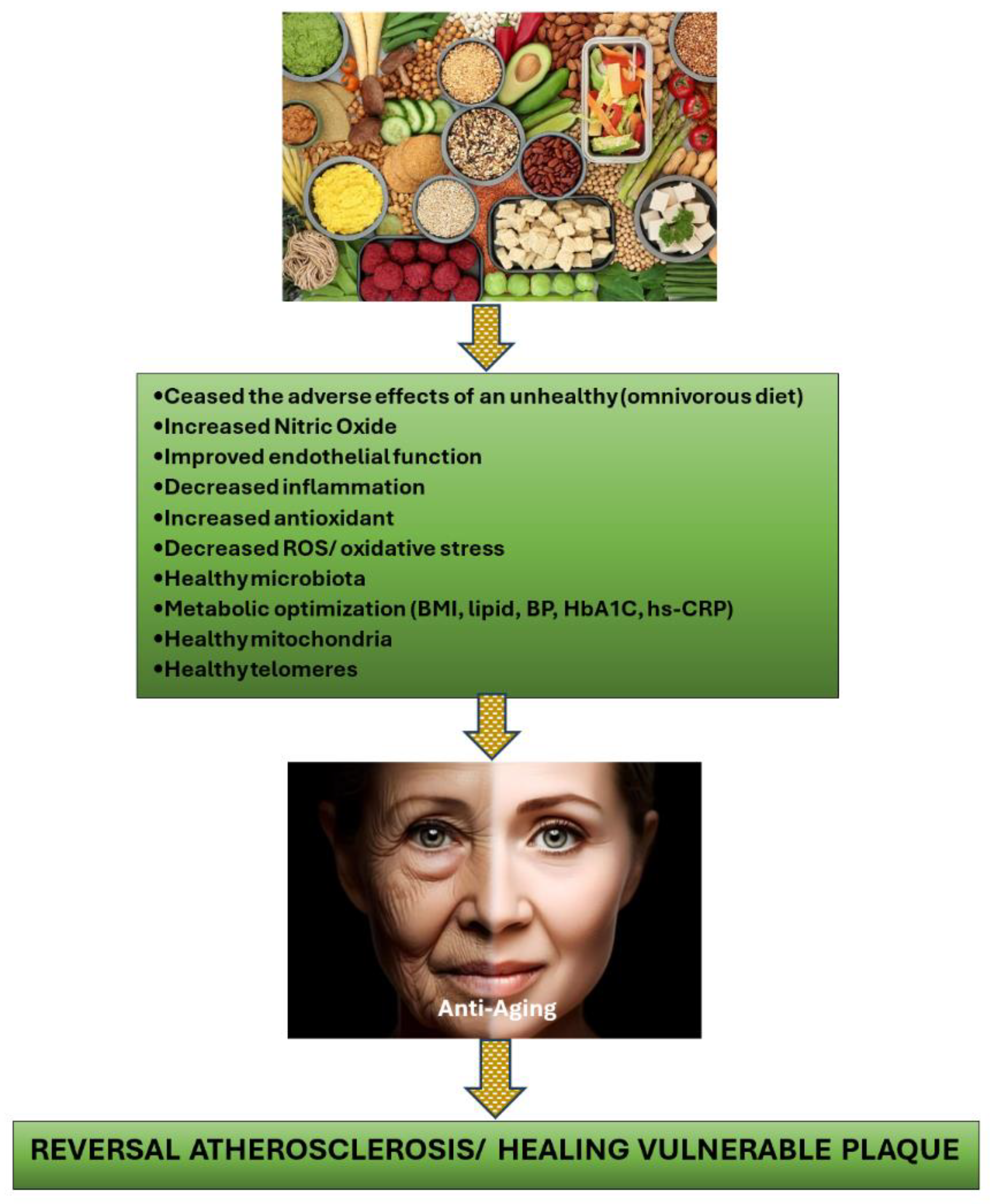
The key mechanism by which a healthy PBD can reverse atherosclerotic plaque and stabilize vulnerable plaque is by changing one’s diet to PBD, thereby eliminating the consumption of foods that contribute to the development of atherosclerotic plaque in the first place. These unhealthy eating behaviors have also been linked to dyslipidemia, insulin resistance, hypertension, glucose intolerance, endothelial dysfunction, chronic systemic inflammation, increased oxidative stress, elevated trimethylamine N-oxide (TMAO), low nitric oxide (NO), gut dysbiosis, mitochondrial damage, and shortened telomeres (accelerating the aging process) [41,47,48,49,50,51]. All of these are widely accepted as risk factors for the development of atherosclerosis.
The processes through which PBD aids in the regression of atherosclerotic plaque include enhancing NO availability, modifying the microbiota, repairing endothelial dysfunction, reducing inflammation, protecting against oxidative stress, fortifying mitochondria, and extending telomeres [41]. It is crucial for individuals who utilize PBD for regressing coronary plaque purpose, to pay close attention to their food choices and consume items that possess properties that suppress inflammation, combat oxidative stress, increase NO availability, support healthy microbiota, strengthen mitochondria, heal telomeres, and exhibit anti-thrombotic properties [41] as can be seen in Figure 3. The precise quantity of these foods must also be determined to prevent nutrient deficiencies (protein, Omega 3, B12, D, K2, Fe, Zn, Cu, and Se), and the food processing method should be carefully considered to ensure maximum benefit. For instance, to obtain the highest NO source from vegetables, consuming them raw rather than cooked is recommended.
Many nutrition experts have specifically emphasized the deficiency of essential nutrients in PBDs, such as vitamins B12 and D, and minerals, like iodine, iron, zinc, selenium, and calcium, which can have detrimental effects, particularly for pregnant individuals. In this context, I have included dietary supplements in my dietary program, including vitamin C, vitamin D, vitamin K2, vitamin B3/NAD+, zinc, copper, selenium, and natural anti-inflammatory products such as astaxanthin, curcumin, quercetin, as well as CoQ10, taurine, and multivitamins (containing various small doses of minerals and vitamins as recommended for daily RDA). These supplements ensure no nutrient deficiency occurs when following PBDs and enhance the anti-inflammatory, antioxidant, immunomodulator, repair mitochondria, and strengthen telomere, which will be useful in the anti-aging process, including regressing coronary plaques.
4. Conclusion
Being diagnosed with coronary stenosis of 50% does not necessarily indicate it is benign since it does not need immediate intervention, as studies have shown that 68% of acute myocardial infarctions (AMIs) are caused by coronary obstruction less than 50%, likely due to a vulnerable plaque [8]. Recent developments have suggested that identifying the presence of a vulnerable plaque and intervening before it causes an acute coronary syndrome may be beneficial [13,14]. However, sophisticated tools are required to diagnose a vulnerable plaque but are currently unavailable in Indonesian hospitals. Therefore, individuals diagnosed with 40-70% stenosis in their coronary arteries have three options: 1. Finding hospitals that have sophisticated tools to determine and intervene the vulnerable plaque 2. Waiting until the lesion becomes symptomatic or causes an acute coronary syndrome, at which point coronary intervention is recommended. 3. Implementing the correct lifestyle changes and pursuing OMT. Simply advising patients to modify their lifestyle may not be effective, but medical practitioners must be knowledgeable about the lifestyle program, including selecting appropriate foods with the correct quantities and knowing the processing methods. They must also understand how to avoid nutrient deficiencies while following the program. Additionally, understanding the role of vitamins, minerals, and nutraceuticals, particularly those that may aid in plaque regression, is necessary.
In the past, doctors even recommended smoking to their patients, but through research and advancing knowledge, smoking is now banned in almost all countries worldwide. We believe that unhealthy foods will eventually be viewed in a similar manner, and individuals who consume them will be warned, similar to smoking.
Author Contributions
Conceptualization, D.M.; investigation, D.M.; writing-original draft preparation, D.M.; writing-review and editing, D.M., A.M.H. and I.N.E.L.; visualization, D.M.; supervision, D.M., A.M.H. and I.N.E.L. All authors have read and agreed in the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
not applicable.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
Given the problems associated with protecting patients' personal data, data confirming the results presented can be obtained from the corresponding author upon any reasonable request.
Acknowledgments
We would like to thank Dr. Daniel Ruslim for providing CAC and CTCA data analysis.
Conflict of Interest
The authors declare no conflict of interest.
References
- Ahmed, A.H.; Shankar, K.; Eftekhari, H.; Munir; Robertson, J.; Brewer, A.; Stupin, I.V.; Casscells, S.W. Silent myocardial ischemia: Current perspectives and future directions. 2007, 12, 189–96. [Google Scholar]
- Bergström, G.; Persson, M.; Adiels, M.; Björnson, E.; Bonander, C.; Ahlström, H.; Alfredsson, J.; Angerås, O.; Berglund, G.; Blomberg, A.; et al. Prevalence of Subclinical Coronary Artery Atherosclerosis in the General Population. Circ. 2021, 144, 916–929. [Google Scholar] [CrossRef]
- Boden, W.E.; O'Rourke, R.A.; Teo, K.K.; Hartigan, P.M.; Maron, D.J.; Kostuk, W.J.; Knudtson, M.; Dada, M.; Casperson, P.; Harris, C.L.; et al. Optimal Medical Therapy with or without PCI for Stable Coronary Disease. New Engl. J. Med. 2007, 356, 1503–1516. [Google Scholar] [CrossRef]
- Al-Lamee, R.; Thompson, D.; Dehbi, H.-M.; Sen, S.; Tang, K.; Davies, J.; Keeble, T.; Mielewczik, M.; Kaprielian, R.; Malik, I.S.; et al. Percutaneous coronary intervention in stable angina (ORBITA): a double-blind, randomised controlled trial. Lancet 2017, 391, 31–40. [Google Scholar] [CrossRef]
- Maron, D.J.; Hochman, J.S.; Reynolds, H.R.; Bangalore, S.; O’Brien, S.M.; Boden, W.E.; Chaitman, B.R.; Senior, R.; López-Sendón, J.; Alexander, K.P.; et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N. Engl. J. Med. 2020, 382, 1395–1407. [Google Scholar] [CrossRef]
- Kurup, R.; Wijeysundera, H.C.; Bagur, R.; Ybarra, L.F. Complete Versus Incomplete Percutaneous Coronary Intervention-Mediated Revascularization in Patients With Chronic Coronary Syndromes. Cardiovasc. Revascularization Med. 2023, 47, 86–92. [Google Scholar] [CrossRef]
- Stone, G.W.; Ali, Z.A.; O’brien, S.M.; Rhodes, G.; Genereux, P.; Bangalore, S.; Mavromatis, K.; Horst, J.; Dressler, O.; Poh, K.K.; et al. Impact of Complete Revascularization in the ISCHEMIA Trial. J. Am. Coll. Cardiol. 2023, 82, 1175–1188. [Google Scholar] [CrossRef]
- Doenst, T.; Haverich, A.; Serruys, P.; Bonow, R.O.; Kappetein, P.; Falk, V.; Velazquez, E.; Diegeler, A.; Sigusch, H. PCI and CABG for Treating Stable Coronary Artery Disease. J. Am. Coll. Cardiol. 2019, 73, 964–976. [Google Scholar] [CrossRef]
- van Veelen, A.; van der Sangen, N.M.R.; Delewi, R.; Beijk, M.A.M.; Henriques, J.P.S.; Claessen, B.E.P.M. Detection of Vulnerable Coronary Plaques Using Invasive and Non-Invasive Imaging Modalities. J. Clin. Med. 2022, 11, 1361. [Google Scholar] [CrossRef]
- Tomaniak, M.; Katagiri, Y.; Modolo, R.; de Silva, R.; Khamis, R.Y.; Bourantas, C.V.; Torii, R.; Wentzel, J.J.; Gijsen, F.J.H.; van Soest, G.; et al. Vulnerable plaques and patients: state-of-the-art. Eur. Hear. J. 2020, 41, 2997–3004. [Google Scholar] [CrossRef]
- Virani, S.S.; Newby, L.K.; Arnold, S.V.; Bittner, V.; Brewer, L.C.; Demeter, S.H.; Dixon, D.L.; Fearon, W.F.; Hess, B.; Johnson, H.M.; et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2023, 148, E9–E119, Epub 2023 Jul 20. Erratum in: Circulation. 2023 Sep 26;148(13):e148. Erratum in: Circulation. 2023 Dec 5;148(23):e186. PMID: 37471501. [Google Scholar] [CrossRef]
- Stone, G.W.; Maehara, A.; Ali, Z.A.; Held, C.; Matsumura, M.; Kjøller-Hansen, L.; Bøtker, H.E.; Maeng, M.; Engstrøm, T.; Wiseth, R.; et al. Percutaneous Coronary Intervention for Vulnerable Coronary Atherosclerotic Plaque. J. Am. Coll. Cardiol. 2020, 76, 2289–2301. [Google Scholar] [CrossRef]
- Park, S.-J.; Ahn, J.-M.; Kang, D.-Y.; Yun, S.-C.; Ahn, Y.-K.; Kim, W.-J.; Nam, C.-W.; Jeong, J.-O.; Chae, I.-H.; Shiomi, H.; et al. Preventive percutaneous coronary intervention versus optimal medical therapy alone for the treatment of vulnerable atherosclerotic coronary plaques (PREVENT): a multicentre, open-label, randomised controlled trial. . 2024. [Google Scholar] [CrossRef]
- van Veelen, A.; Küçük, I.T.; Fuentes, F.H.; Kahsay, Y.; Garcia-Garcia, H.M.; Delewi, R.; Beijk, M.A.M.; Hartog, A.W.D.; Grundeken, M.J.; Vis, M.M.; et al. First-in-Human Drug-Eluting Balloon Treatment of Vulnerable Lipid-Rich Plaques: Rationale and Design of the DEBuT-LRP Study. J. Clin. Med. 2023, 12, 5807. [Google Scholar] [CrossRef]
- Mortensen, M.B.; Dzaye, O.; Steffensen, F.H.; Bøtker, H.E.; Jensen, J.M.; Sand, N.P.R.; Kragholm, K.H.; Sørensen, H.T.; Leipsic, J.; Mæng, M.; et al. Impact of Plaque Burden Versus Stenosis on Ischemic Events in Patients With Coronary Atherosclerosis. J. Am. Coll. Cardiol. 2020, 76, 2803–2813. [Google Scholar] [CrossRef]
- Babateen, A.M.; Shannon, O.M.; Mathers, J.C.; Siervo, M. Validity and reliability of test strips for the measurement of salivary nitrite concentration with and without the use of mouthwash in healthy adults. Nitric Oxide 2019, 91, 15–22. [Google Scholar] [CrossRef]
- Puri, R.; Nissen, S.E.; Somaratne, R.; Cho, L.; Kastelein, J.J.; Ballantyne, C.M.; Koenig, W.; Anderson, T.J.; Yang, J.; Kassahun, H.; et al. Impact of PCSK9 inhibition on coronary atheroma progression: Rationale and design of Global Assessment of Plaque Regression with a PCSK9 Antibody as Measured by Intravascular Ultrasound (GLAGOV). Am. Hear. J. 2016, 176, 83–92. [Google Scholar] [CrossRef]
- Peña-Jorquera, H.; Cid-Jofré, V.; Landaeta-Díaz, L.; Petermann-Rocha, F.; Martorell, M.; Zbinden-Foncea, H.; Ferrari, G.; Jorquera-Aguilera, C.; Cristi-Montero, C. Plant-Based Nutrition: Exploring Health Benefits for Atherosclerosis, Chronic Diseases, and Metabolic Syndrome—A Comprehensive Review. Nutrients 2023, 15, 3244. [Google Scholar] [CrossRef]
- Salehin, S.; Rasmussen, P.; Mai, S.; Mushtaq, M.; Agarwal, M.; Hasan, S.M.; Salehin, S.; Raja, M.; Gilani, S.; Khalife, W.I. Plant Based Diet and Its Effect on Cardiovascular Disease. Int. J. Environ. Res. Public Heal. 2023, 20, 3337. [Google Scholar] [CrossRef]
- Koutentakis, M.; Surma, S.; Rogula, S.; Filipiak, K.J.; Gąsecka, A. The Effect of a Vegan Diet on the Cardiovascular System. J. Cardiovasc. Dev. Dis. 2023, 10, 94. [Google Scholar] [CrossRef]
- Tucci, M.; Marino, M.; Martini, D.; Porrini, M.; Riso, P.; Del Bo’, C. Plant-Based Foods and Vascular Function: A Systematic Review of Dietary Intervention Trials in Older Subjects and Hypothesized Mechanisms of Action. Nutrients 2022, 14, 2615. [Google Scholar] [CrossRef]
- Islam, S.U.; Ahmed, M.B.; Ahsan, H.; Lee, Y.-S. Recent Molecular Mechanisms and Beneficial Effects of Phytochemicals and Plant-Based Whole Foods in Reducing LDL-C and Preventing Cardiovascular Disease. Antioxidants 2021, 10, 784. [Google Scholar] [CrossRef]
- Mehta, P.; Tawfeeq, S.; Padte, S.; Sunasra, R.; Desai, H.; Surani, S.; Kashyap, R. Plant-based diet and its effect on coronary artery disease: A narrative review. World J. Clin. Cases 2023, 11, 4752–4762. [Google Scholar] [CrossRef]
- Bruns, A.; Greupner, T.; Nebl, J.; Hahn, A. Plant-based diets and cardiovascular risk factors: a comparison of flexitarians, vegans and omnivores in a cross-sectional study. BMC Nutr. 2024, 10, 1–13. [Google Scholar] [CrossRef]
- Di Sotto, A.; Vitalone, A.; Di Giacomo, S. Plant-Derived Nutraceuticals and Immune System Modulation: An Evidence-Based Overview. Vaccines 2020, 8, 468. [Google Scholar] [CrossRef]
- Xu, K.; Al-Ani, M.K.; Pan, X.; Chi, Q.; Dong, N.; Qiu, X. Plant-Derived Products for Treatment of Vascular Intima Hyperplasia Selectively Inhibit Vascular Smooth Muscle Cell Functions. Evidence-Based Complement. Altern. Med. 2018, 2018, 1–17. [Google Scholar] [CrossRef]
- Monsalve, B.; Concha-Meyer, A.; Palomo, I.; Fuentes, E. Mechanisms of Endothelial Protection by Natural Bioactive Compounds from Fruit and Vegetables. 2017, 89, 615–633. [CrossRef]
- Aquila, G.; Marracino, L.; Martino, V.; Calabria, D.; Campo, G.; Caliceti, C.; Rizzo, P. The Use of Nutraceuticals to Counteract Atherosclerosis: The Role of the Notch Pathway. Oxidative Med. Cell. Longev. 2019, 2019, 1–30. [Google Scholar] [CrossRef]
- Moss, J.W.E.; Ramji, D.P. Nutraceutical therapies for atherosclerosis. Nat. Rev. Cardiol. 2016, 13, 513–532. [Google Scholar] [CrossRef]
- Wei, T.; Liu, J.; Zhang, D.; Wang, X.; Li, G.; Ma, R.; Chen, G.; Lin, X.; Guo, X. The Relationship Between Nutrition and Atherosclerosis. Front. Bioeng. Biotechnol. 2021, 9. [Google Scholar] [CrossRef]
- Mitu, O.; Cirneala, I.A.; Lupsan, A.I.; Iurciuc, M.; Mitu, I.; Dimitriu, D.C.; Costache, A.D.; Petris, A.O.; Costache, I.I. The Effect of Vitamin Supplementation on Subclinical Atherosclerosis in Patients without Manifest Cardiovascular Diseases: Never-ending Hope or Underestimated Effect? Molecules 2020, 25, 1717. [Google Scholar] [CrossRef]
- Garcia, S.; Sandoval, Y.; Roukoz, H.; Adabag, S.; Canoniero, M.; Yannopoulos, D.; Brilakis, E.S. Outcomes After Complete Versus Incomplete Revascularization of Patients With Multivessel Coronary Artery Disease. J. Am. Coll. Cardiol. 2013, 62, 1421–1431. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, Y.; Brilakis, E.S.; Garcia, S. Completeness of revascularization in multivessel coronary artery disease. J. Thorac. Dis. 2016, 8, E1493–E1496. [Google Scholar] [CrossRef] [PubMed]
- Hwang, D.; Kang, J.; Yang, H.-M.; Yang, S.; Park, J.; Han, J.-K.; Kang, H.-J.; Koo, B.-K.; Kim, H.-S. Better Prognosis After Complete Revascularization Using Contemporary Coronary Stents in Patients With Chronic Kidney Disease. Circ. Cardiovasc. Interv. 2019, 12, e007907. [Google Scholar] [CrossRef]
- Iqbal, M.B.; Moore, P.T.; Nadra, I.J.; Robinson, S.D.; Fretz, E.; Ding, L.; Fung, A.; Aymong, E.; Chan, A.W.; Hodge, S.; et al. Complete revascularization in stable multivessel coronary artery disease: A real world analysis from the British Columbia Cardiac Registry. Catheter. Cardiovasc. Interv. 2021, 99, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Williams, T.; Mittal, A.; Karageorgiev, D.; Romo, A.I.; Aminian, A.; Portalese, J.F.; Kharrat, E.; Gómez-Hospital, J.A.; Firman, D.; Nouche, R.T.; et al. Complete revascularization optimizes patient outcomes in multivessel coronary artery disease: Data from the e-Ultimaster registry. Catheter. Cardiovasc. Interv. 2021, 99, 961–967. [Google Scholar] [CrossRef]
- Pham, V.; Moroni, A.; Gall, E.; Benedetti, A.; Zivelonghi, C.; Picard, F. Revascularization and Medical Therapy for Chronic Coronary Syndromes: Lessons Learnt from Recent Trials, a Literature Review. J. Clin. Med. 2023, 12, 2833. [Google Scholar] [CrossRef] [PubMed]
- Giubilato, S.; Lucà, F.; Abrignani, M.G.; Gatto, L.; Rao, C.M.; Ingianni, N.; Amico, F.; Rossini, R.; Caretta, G.; Cornara, S.; et al. Management of Residual Risk in Chronic Coronary Syndromes. Clinical Pathways for a Quality-Based Secondary Prevention. J. Clin. Med. 2023, 12, 5989. [Google Scholar] [CrossRef] [PubMed]
- Ornish, D.; Scherwitz, L.W.; Billings, J.H.; Gould, K.L.; Merritt, T.A.; Sparler, S.; Armstrong, W.T.; Ports, T.A.; Kirkeeide, R.L.; Hogeboom, C.; et al. Intensive Lifestyle Changes for Reversal of Coronary Heart Disease. JAMA 1998, 280, 2001–2007. [Google Scholar] [CrossRef]
- Esselstyn CB Jr, Gendy G, Doyle J, et al. A way to reverse CAD? J Fam Pract. 2014 Jul;63(7):356-364b. PMID: 25198208.
- Mulijono, D. Mechanism of How Plant-Based Diet (PBD) Reduces the Risk of In-Stent Restenosis (ISR) and Stent Thrombosis (ST). Preprints 2024, 2024040628. [Google Scholar] [CrossRef]
- Rose, S.; Strombom, A. A Comprehensive Review of the Prevention and Treatment of Heart Disease with a Plant-Based Diet. J. Cardiol. Cardiovasc. Ther. 2018, 12, 1–12. [Google Scholar] [CrossRef]
- Bilal, M.; Ashraf, S.; Zhao, X. Dietary Component-Induced Inflammation and Its Amelioration by Prebiotics, Probiotics, and Synbiotics. Front. Nutr. 2022, 9, 931458. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, S.; Dixit, M. Role of Polyphenols and Other Phytochemicals on Molecular Signaling. Oxid. Med. Cell. Longev. 2015, 2015, 504253. [Google Scholar] [CrossRef]
- Wu, Y.-T.; Chen, L.; Tan, Z.-B.; Fan, H.-J.; Xie, L.-P.; Zhang, W.-T.; Chen, H.-M.; Li, J.; Liu, B.; Zhou, Y.-C. Luteolin Inhibits Vascular Smooth Muscle Cell Proliferation and Migration by Inhibiting TGFBR1 Signaling. Front. Pharmacol. 2018, 9, 1059. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.G.; Florida, E.; Li, H.; Parel, P.M.; Mehta, N.N.; Sorokin, A.V. Oxidized low-density lipoprotein associates with cardiovascular disease by a vicious cycle of atherosclerosis and inflammation: A systematic review and meta-analysis. Front. Cardiovasc. Med. 2023, 9, 1023651. [Google Scholar] [CrossRef] [PubMed]
- Marchio, P.; Guerra-Ojeda, S.; Vila, J.M.; Aldasoro, M.; Victor, V.M.; Mauricio, M.D. Targeting Early Atherosclerosis: A Focus on Oxidative Stress and Inflammation. Oxid. Med. Cell Longev. 2019, 2019, 8563845. [Google Scholar] [CrossRef] [PubMed]
- Ray, A.; Maharana, K.C.; Meenakshi, S.; Singh, S. Endothelial dysfunction and its relation in different disorders: Recent update. Heal. Sci. Rev. 2023, 7. [Google Scholar] [CrossRef]
- Almeida, C.; Barata, P.; Fernandes, R. The influence of gut microbiota in cardiovascular diseases—a brief review. Porto Biomed. J. 2021, 6, e106. [Google Scholar] [CrossRef] [PubMed]
- Pollicino, F.; Veronese, N.; Dominguez, L.J.; Barbagallo, M. Mediterranean diet and mitochondria: New findings. Exp. Gerontol. 2023, 176, 112165. [Google Scholar] [CrossRef]
- Cinegaglia, N.; Antoniazzi, L.; Rosa, D.; Miranda, D.; Acosta-Navarro, J.; Bortolotto, L.; Hong, V.; Sandrim, V. Shortening telomere is associated with subclinical atherosclerosis biomarker in omnivorous but not in vegetarian healthy men. Aging 2019, 11, 5070–5080. [Google Scholar] [CrossRef]
Figure 1.
CCTA results before and after lifestyle intervention to regress or reverse coronary artery stenosis or calcified plaque.
Figure 1.
CCTA results before and after lifestyle intervention to regress or reverse coronary artery stenosis or calcified plaque.
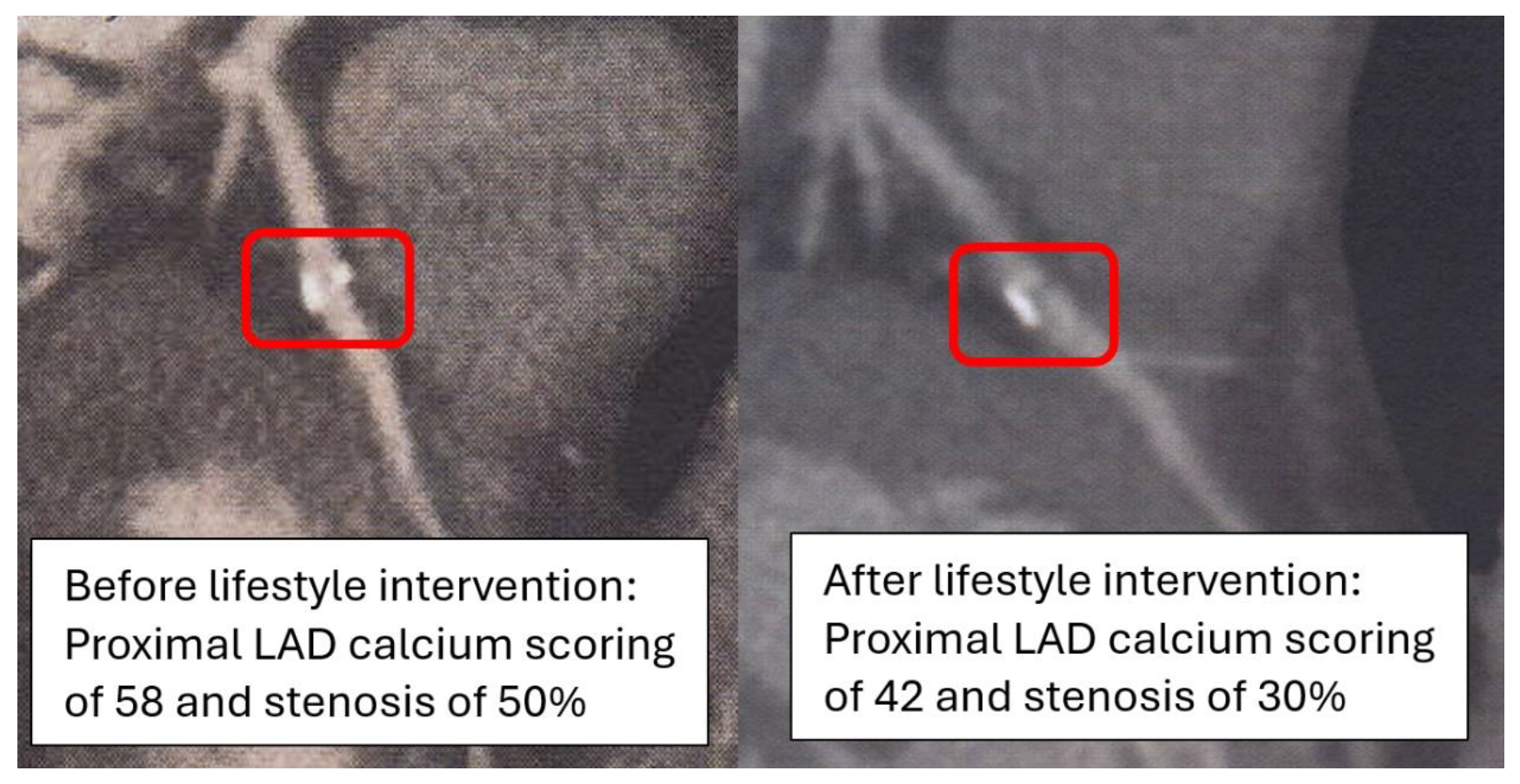
Figure 2.
Reversal of coronary artery disease.
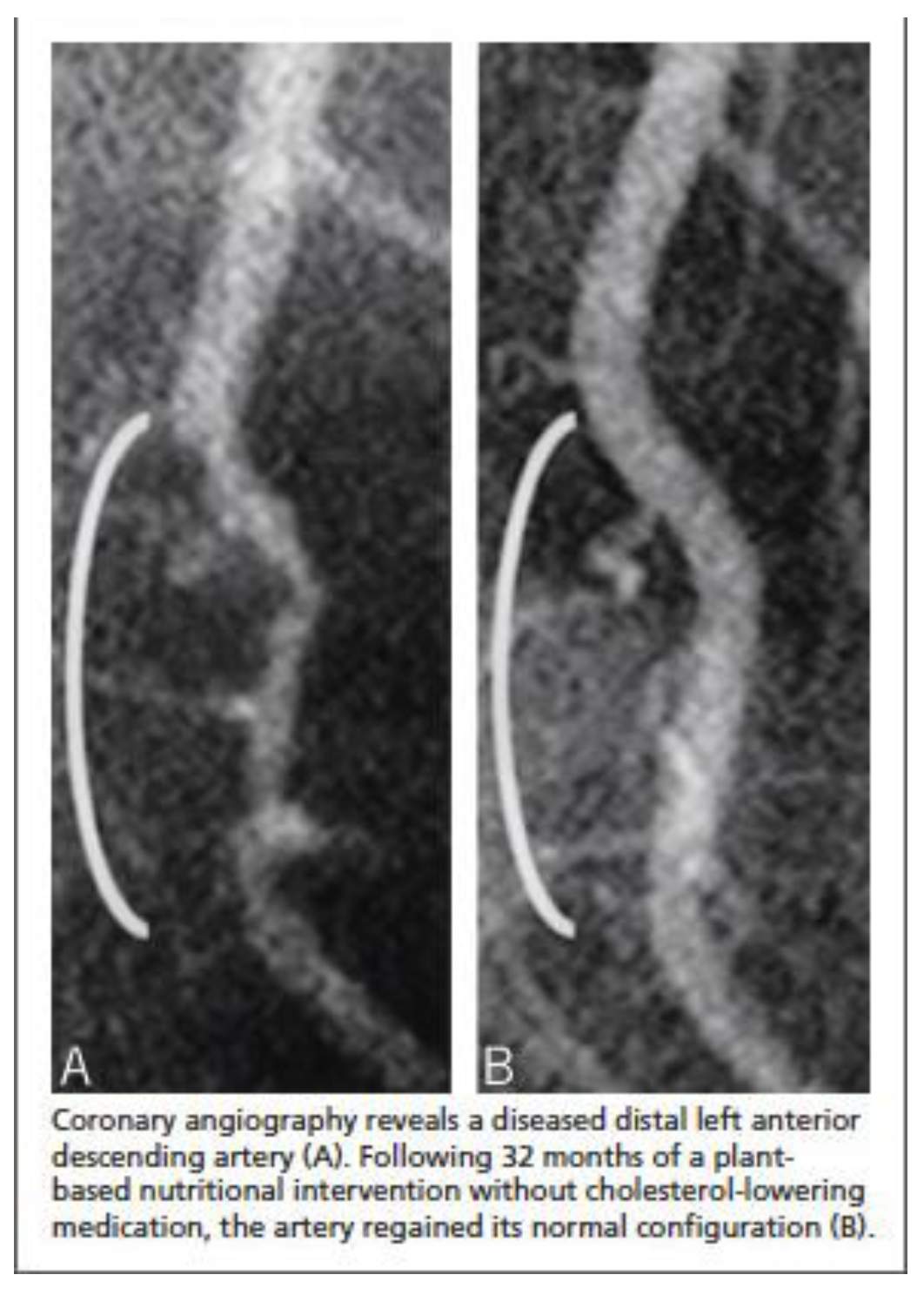
Figure 3.
Mechanisms of how PBD regress the atherosclerotic plaque.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



