
Submitted:
12 April 2024
Posted:
15 April 2024
You are already at the latest version
Abstract
Background: Acute kidney disease (AKD) is a known risk factor for increased mortality and evolution towards chronic kidney disease (CKD) in adults. The data regarding children are scarce. The purpose of our study is to explore the risk factor for AKD and impact of AKD following an acute kidney injury (AKI) episode in children on mortality and new-onset CKD.
Methods: We retrospectively evaluated 736 children with ages between 2 and 18 years old with AKI admitted in a tertiary care hospital from the west Romania over a 9 years period.
Results: AKD incidence following AKI was 17%. Patients that developed AKD were older, with higher baseline serum creatinine values, urea, C reactive protein and lower proteins, haemoglobin and sodium. They were more often exposed to sepsis, critical illness and nephrotoxic medications and presented certain susceptibilities like CKD, neoplasia, anemia, heart failure, arterial hypertension, stem cell transplant and female gender. AKI causes that increased the risk of AKD were intrinsic ones. AKD increased the overall mortality by three times. The factors that independently increased the risk of evolution towards CKD were AKD, acute tubular necrosis and higher baseline serum creatinine values.
Conclusions: AKD is an independent risk factor for mortality and new-onset CKD in children.
Keywords:
acute kidney disease
; children
; mortality
; chronic kidney disease
Introduction
Acute kidney injury (AKI) is an already proved risk factor for worse kidney outcomes in adults and children with high mortality and increased hospital stay [1,2,3,4,5]. The evolution of AKI is multidirectional and most often linked to the underlying disease severity. AKI can evolve towards resolution of the episode during the first 7 days or it can progress towards acute kidney disease (AKD) or chronic kidney disease (CKD) [1,3]. The concept of AKD was first introduced by Kidney Disease Improving global outcomes (KDIGO) in the AKI guideline from 2012. [6] The Acute Disease Quality Initiative (ADQI) 16 Workgroup further refined and staged AKD as a subacute or acute loss of kidney function with duration between 7 and 90 days from the initial AKI event based on the KDIGO AKI criteria [7].
Since the concept of AKD was introduced in clinical studies as a prolonged AKI episode with high morbidity and mortality, proving that the relationship between AKI, AKD and CKD represents a continuum of kidney dysfunction or damage time-dependent of the AKI episode. The AKI-AKD-CKD continuum has been studied in adult setting [8,9,10,11]. The latest meta-analysis in adults by Su showed that AKD is an independent risk factor for mortality, CKD development and kidney failure [12]. However, only a few studies evaluated the evolution of AKI towards AKD in children [13,14,15,16,17]. Three of the aforementioned studies evaluated AKD incidence and outcomes in specific groups of children, either in transplantation (allogenic hematopoietic stem cell) [16] or non-kidney solid organ transplantation [14] or following cardiopulmonary by-pass [15]. The later two studies, by Deng [17] and Patel [13] evaluated AKD incidence and outcomes in mixed paediatric patients aged between 1 month and 18 years old.
As kidney function evolution after birth is extremely dynamic, glomerular and tubular function increases immediately postnatal [18]. The dynamic changes in kidney function occur differently in children born preterm or with lower gestational ages. Nevertheless, children reach a glomerular filtration rate equivalent to adults around 2 years of age [19]. Given the high variability of kidney function in the first 2 years of life, we conducted a retrospective cohort study in children with stable and mature kidney function who developed AKD following an AKI episode. In addition, we evaluated the risk factors, outcomes and the risk of CKD development in children with AKD.
Material and Methods
Study Design
We conducted a retrospective observational cohort study in children between 2 and 18 years old, admitted in a tertiary care children’s hospital from west Romania. We analysed and screened for AKI all admissions during 2014 and 2022. We included only the patients with AKI in the analysis of AKD and CKD. Inclusion criteria were: at least two serum creatinine measurements during the first 7 days for the diagnosis of AKI, patients with AKI over 7 days whom had at least one serum creatinine measurement during the first 7 days of AKD and for new-onset CKD a follow-up in serum creatinine 90 days after the initial AKI episode. Data were retrieved from the Electronically Data System of the hospital. Follow-up was performed until death or the last recorded admission. Estimated glomerular filtration rate (eGFR) was calculated using Bedside Schwartz formula for the lowest serum creatinine value [20]. The final cohort comprised a mixed pediatric population, from intensive and non-intensive care units. The Ethics Committee of the “Louis Turcanu” Children’s Hospital approved the study. Informed consent was waived due to the retrospective nature of the study.
Outcomes and Definitions
The primary outcomes of the study were to determine AKD incidence following an AKI episode and to evaluate the risk factors associated with AKD development in children after reaching the adult kidney function. In addition, we evaluated the influence of AKD on mortality, in-hospital and post-discharge, and the impact of AKD on new-onset CKD. The impact of AKD on mortality was evaluated only in patients who survived the first 7 days of AKI and reached the theoretical landmark of AKD development. The baseline serum creatinine was considered the lowest value prior to the AKI episode. If the patient did not have a previous serum creatinine value recorded, we considered baseline serum creatinine the lowest value of serum creatinine recorded after the AKI episode. AKI was defined using the KDIGO AKI criteria for serum creatinine [6]. If a patient presented multiple AKI episodes, we only included the first recorded AKI episode in our analysis. A later AKI episode was considered as subsequent AKI. Acute kidney disease was defined and staged based on the 2021 KDIGO recommendations using the serum creatinine value recorded after day 7 of AKI [21]. The diagnosis of new-onset CKD was based on the 2012 KDIGO guideline based on the following criteria: persistence of kidney damage markers for more than 3 months (albuminuria, proteinuria, etc) or eGFR<60ml/min/1.73sm for more than 3 months [22]. The impact of AKD on new-onset CKD development was performed only in patients with a follow-up longer than 3 months.
Variables of Interest
All the data were retrieved from the electronically data system of the hospital. We noted gender, environment, age, weight, height, length of stay and biological parameters measured in the first day of identified AKI. In addition, we retrieved data regarding intensive care unit (ICU) admission and the presence of the exposures and susceptibilities in patients with AKI. Also, the exposures and susceptibilities were further analysed in patients with AKD in order to obtain a better image of AKD outcomes in children.
Study Size
Out of 142 762 hospital admissions, 2765 episodes of AKI were identified. We first excluded the subsequent AKI episodes and the cohort comprised 2346 patients. We further excluded the patients between 1 day and 1.99 years old, thus the final cohort comprised 736 patients. The analysis on mortality was performed on 720 patients, after excluding 16 children that died during the first 7 days of AKI. Evaluation of CKD development was performed in patients with more than 3 months follow-up, after excluding the pre-existent CKD, in 313 patients.
Statistical Analysis
The continuous variables were tested for normality using the Shapiro-Wilk test. Because none of our continuous variables followed a normal distribution, we defined median and interquartile range. The categorical variables were defined as numbers and percentages. For continuous variables we used Mann-Whitney test if there were two groups and Kruskal-Wallis for three or more comparison groups. The crude analysis was performed by calculating the odds ratio and 95% confidence interval. The adjusted analysis was performed using multivariable logistic regression models with a backwards selection of the variables (excluded if p>0.1 and included for p<0.05). The crude analysis for CKD development was performed by generating Kaplan-Meier survival curves. For the adjusted analysis on CKD development we used a cox-proportional-hazards regression model. A p values less than 0.05 was considered statistically significant. The statistical analysis was performed using MedCalc® Statistical Software version 22.021 (MedCalc Software Ltd, Ostend, Belgium).
Results
Our cohort included 736 patients with AKI. 125 children developed AKD representing 17%. The demographics and baseline characteristics of the patients are presented in Table 1. Patients who developed AKD were older, with a higher weight, height and body mass index compared with non-AKD ones. The baseline serum creatinine (SCr) was higher in the AKD group, however there were no statistical differences regarding eGFR between the AKD and non-AKD groups. Patients with AKD presented higher maximum SCr, urea levels, uric acid and C reactive protein and lower serum proteins, haemoglobin and sodium levels. The distribution on AKI stages was different between the two groups (p<0.0001). Severe AKI (stages 2 and 3) was present in over half the patients from the non-AKD group, while in patients that developed AKD, AKD stages 2 and 3 comprised more than 78%. Similar, the incidence of AKI stage 1 was higher in the non-AKD group, comprising 41% of the AKI cases as compared to the AKD group were AKD incidence was inversely correlated with AKD severity. These results were translated into higher ICU admissions in patients with AKD when compared to non-AKD (44% versus 30.6%, p=0.003), and longer hospital stay as well (17 days versus 8 days, p<0.0001). Also, the incidence of renal replacement therapy was higher in patients from the AKD group (12 patients versus 4, p<0.0001).
Next, we evaluated the impact of exposures and susceptibilities on AKD development – Table 2. Among the explored exposures, only sepsis, critical illness and nephrotoxic medications increased the risk of AKD by 2, 1.9 and 2.5 times respectively. From susceptibilities, the presence of CKD increased the risk of AKD by 2 times, neoplasia by 2.7 times, anemia by 2.9 times, hearth failure by 4 times, arterial hypertension by 3.6 times, stem cell transplant by 2.7 times and female gender by 1.47 times.
We evaluated the impact of AKI causes on AKD development. It seemed that only intrinsic causes increased the risk of AKD. Thus, renal microvasculature alterations, glomerulonephritis, acute tubular necrosis and acute tubule-interstitial nephritis generated odds ratio of 6.8, 4.7, 5 and 3.3 respectively – Table 3.
We further performed an analysis on AKD stages – Table 4. It seems that AKD severity follows AKI severity as 79% of patients with AKD stage 3 presented prior an AKI stage 3 episode, and 61.5% of children with AKD stage 2 had AKI stage 2. In AKD stage 1, the distribution was more even, with around 40% of stage 1 and 2 AKD presenting stage 1 and 2 of AKI and only 18% of AKD stage 1 patients derived from AKI stage 3. The ICU admission incidence was higher in patients with AKD stage 3 compared with all the other stages. Interestingly, baseline SCr was higher only in AKD stage 1 compared to AKD stage 2 and eGFR was similar between the groups. In addition, there were no statistical differences regarding AKD duration stratified by AKD stages. Subsequent AKI events development was similar between AKD and non-AKD patients and between AKD stages also.
The overall mortality was 9.5% (70 cases). The distribution was different regarding the timeframe. In the first 7 days of AKI, there were 16 cases. For a better evaluation of AKD impact on mortality, we excluded from the analysis patients that died during the first 7 days because they could not reach theoretically an AKD state. The cohort for mortality analysis consisted in 720 patients. In this cohort, the mortality was 7.5 % (54 deaths). We divided the mortality timeframe during hospitalisation and after discharge. There were 36 events during hospitalization and 18 after discharge. The crude analysis and the adjusted analysis for age, sex, environment, subsequent AKI and AKI stages are presented in Table 4. AKD increased the overall mortality risk by 3.7 times in crude analysis and 3 times in adjusted one. In all the subgroups analysis, AKD increased the risk of death – Table 5.
In order to evaluate the risk of new-onset CKD, we included in the analysis only the patients with a follow-up longer than three months and without CKD at admission – 313 patients. The median follow-up was of 22.6 months (IQR=11-41.5 months). The crude analysis of new-onset CKD was performed using the Kaplan-Meier survival curves. The number of censored cases were 10 for non-AKD patients (4.05%) and 10 for AKD group (15.15%). Overall, new-onset CKD was found in 20 patients (6.39%). The presence of AKD increased the risk of new-onset CKD by 7.07 times (95%CI=2.33-21.44, p=0.0005) – Figure 1.
In order to evaluate if AKD was an independent risk factor for new-onset CKD, we performed a cox-proportional hazards regression analysis. The model was adjusted for age, sex, environment, subsequent AKI, AKI severity, AKI causes and baseline serum creatinine values. The model was good, with a Harrell’s C index of 0.696 (95%CI=0.522-0.871). AKD remained an independent risk factor for new-onset CKD, increasing the risk by 3.01 times (95%CI=1.18-7.71. p=0.021) – Figure 2. In this model only acute tubular necrosis as acute kidney injury cause increased the risk of CKD (OR=22.96, 95%CI=2.38-220.98, p=0.006 with dehydration considered the baseline) and baseline serum creatinine (each unit increase in mg/dl generated an OR=26.64, 95%CI=3.42-207.49, p=0.0017).
Discussions
To best of our knowledge, this is the first study from Europe that evaluated AKD following an AKI episode in children using the KDIGO criteria and third in the world, after Deng’s study from China [17] and Patel’s study from USA [18]. In this study, we showed that AKD is quite common among children aged 2 to 18 years old, following an AKI episode, and is associated with worse clinical and biological markers. In addition, the presence of AKD increases both in-hospital and post discharge mortality. The intrinsic causes of AKI increased the risk of AKD development. AKD was an independent risk for worse outcomes, with high mortality rates (in-hospital and post discharge) and an increased risk of progression towards CKD in children.
The incidence of AKD in our cohort was 17%. This was consistent with previous reported data in children from 1 month to 18 years old where the incidence of AKD ranged between 6 and 56% [13,14,15,16,17]. However, the data are heterogeneous and comprised patients from a wider age spectrum. Yet, Patel [14], LoBasso [15] and Daraskevicius [16] reported AKD incidences of 13%, 11% and 35.3% respectively in specific paediatric patients. Patel evaluated patients with non-kidney solid organ transplantation [14], LoBasso children following cardiopulmonary bypass [15] and Daraskevicius children after allogeneic hematopoietic stem cell transplantation [16]. As we mentioned above, there are only two studies that evaluated a cohort of mixed paediatric patients, including children between 1 month and 18 years old. One study, by Deng et. al, reported an AKD incidence of 42.3% in 990 AKI children from China [17] and the other study, by Patel et. al, reported a 56.3% incidence [13]. Our reported AKD incidence is lower compared to Patel and Deng. These differences can be explained by the geographic area of the studies (Patel from USA and Deng from China). On the other hand, we included only patients older than 2 years. We chose this approach because it is considered that by the age of 2 years old children reach full kidney function with an eGFR similar to adults [19].
Regarding baseline characteristics, the patients from our cohort that developed AKD were older with higher weight and length. Interestingly, they also presented higher body mass index when compared with non-AKD ones. Deng is the only one who reported that higher age was more common in patients with AKD [17], while Patel reported similar ages between children with or without AKD [13]. We report higher ages in patients with AKD compared to Deng [17] (6 years AKD stage 1 and 9 years AKD stage 2-3), and Patel (3.8 years) [13]. The only one who reported BMI was Patel, 15.4 in patients with AKD, without statistical differences among groups [13]. A possible explanation for our higher BMI (18.75) would be the older age of the patients. Older children tend to have higher chances in reaching increased BMIs as the incidence of obesity increases with the age [23]. The relationship between obesity and kidney disease is not as clear as it is in adults. The most recent review on this topic by Carullo showed that childhood obesity is associated with a higher risk of CKD in adults, but the impact before 18 years old is not clear [24].
The AKD group presented with a more severe underlying disease translated into biological parameters alterations. Thus, patients with AKD had higher uric acid and C reactive protein and lower haemoglobin and sodium. For instance, in Deng’s cohort, there were no differences regarding anemia incidence, but he found a higher incidence of hypoalbuminemia in AKD patients, especially in AKD stages 2 and 3 (48.9% vs 23.3% in non AKD children) [17]. The presence of certain exposures and susceptibilities could be a complementary tool in assessing the disease severity in children, besides the known risk factors for AKI development. Patients from the AKD group were found to be at a higher risk for kidney damage when exposed to sepsis, critical illness and nephrotoxic medication. The risk persisted even in the presence of personal certain susceptibilities: neoplasia, anemia, hearth failure, arterial hypertension and stem cell transplant. This resulted in higher ICU admissions in the AKD group (44% vs 30.6%) and longer hospital stay (17 vs 8 days). Deng reported similar results in patients with sepsis and exposure to nephrotoxins in both AKD and non-AKD groups, but with a higher incidence of heart failure in patients from the AKD group [17]. Patel reported mechanical ventilation, prematurity, neoplasia and bone marrow transplant as risk factors for AKD development [13].
The kidney disease history and kidney function per se proved to influence the evolution from AKI to AKD. We report a high incidence of CKD among AKD patients (12% vs 6.5% in non-AKD group) and higher baseline serum creatinine levels. There is a continuum in patients that develop AKI that is dependent of the underlying disease severity. Severe AKI tends to progress to severe AKD, and AKD, regardless of its severity, is an independent risk factor for CKD development. Also, the intrinsic aetiologies of AKI increase the risk of prolonged kidney injury. Yet, our results do not support AKI and AKD severity to be risk factors for progression towards CKD. However, the relationship between patients with pre-existent CKD and an overlapping AKI or AKD episode has been reported only by Deng and Patel [13,17]. Patients with reduced kidney function are at increased risk of developing a more severe and prolonged AKI episode [6]. So far, CKD is a proved risk factor for AKI and AKD development, at least in adult settings [21].
We report AKD to be an independent mortality risk factor during hospital stay and also post-discharge, similar to previous studies [15,17,25]. However, mortality rates in children with AKD are heterogeneous and inconsistent. Deng reported a 12% and 15.9% mortality rates in children with AKD at 30 and 90 days respectively [17], while LoBasso reported a 31.8% mortality rate after cardio-pulmonary by-pass [15]. Our 17.6% seems to reflect the mortality rates in children with AKD considering that we included patients who reached adult eGFR, however similar to 17.5% mortality rates in children with severe malaria [25].
The final analysis in our study referred to the risk of new-onset CKD. The crude analysis showed that AKD increases the risk of new-onset CKD by seven times and in the adjusted one, by three times. In addition, we showed that acute tubular necrosis increased the risk of new-onset CKD as well as higher baseline creatinine. Similar, Patel reported the risk of new-onset CKD to be 2.7 times greater in patients with AKD [13]. However, patients with AKD following non-kidney solid organ transplantation had a 29 times higher risk to develop CKD [14]. Interestingly, AKI severity did not increase the risk of CKD similar to previous reported data [13]. Subsequent AKI episodes did not increased the risk of new-onset CKD, even though Patel found previous AKI episodes to be associated with a higher risk of CKD development [13].
The major limitations are regarding the nature of the study – single-centre, retrospective and observational. On the other hand, the lack of urine output in diagnosing and staging AKI is a drawback. The number of patients, the long follow-up and the individual evaluation of AKD impact on mortality and CKD represent the strong points. In addition, exploring the AKI causes and their relationship to AKD development increases the quality of the paper. Nevertheless, our study is the first one that evaluates AKD incidence and outcomes in a mixed paediatric patients from Europe, following an AKI episode, in children older than 2 years.
Children who develop AKD have a higher mortality risk that persists even after discharge. AKD is an independent risk factor for new-onset CKD. Attention should focus on children with pre-existent CKD as these patients are more susceptible to prolonged and severe kidney injury. Follow-up at least 3 months after an AKI episode should assess kidney function markers and urinalysis.
Author Contributions
Conceptualization, F.C. and V.I; Methodology, F.C.; Software, L.C.; Validation, A.S, A.M., L.M., R.S. R.M.S.; Formal Analysis, A.M.; Investigation, F.C.; Resources, F.C., R.S.; Data Curation, L.C.; Writing – Original Draft Preparation, F.C., V.I.; Writing – Review & Editing, all authors.; Visualization, A.M., L.M., R.S., R.M.S.; Supervision, A.S.,M.G.; Project Administration, F.C.; Funding Acquisition, R.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The Ethics Committee of the “Louis Turcanu” hospital approved the study (protocol code 9485, date of approval: 20.06.2023). The study was conducted according to the guidelines of the Declaration of Helsinki
Informed Consent Statement
Informed consent was obtained from all legal guardians of the children involved in the study.
Data Availability Statement
The data collected for this study will be available for others, at request directly to the corresponding author. The data that will be available is represented by deidentified participant data. The inform consent form and statistical analysis plan will be available at request. The data will be available with publication. The data will be available at request at the e–mail address ivan.viviana@umft.ro. The data will be shared after direct request and after approval of the proposal by all the authors.
Acknowledgements
We would like to acknowledge Victor Babes University of Medicine and Pharmacy from Timisoara for supporting the article processing charges for this manuscript
Conflicts of Interest
The authors declare no conflict of interest
References
- Kellum JA, Romagnani P, Ashuntantang G, Ronco C, Zarbock A, Anders HJ. Acute kidney injury. Nat Rev Dis Primers. 2021 Jul 15;7(1):52. [CrossRef]
- Susantitaphong P, Cruz DN, Cerda J, Abulfaraj M, Alqahtani F, Koulouridis I, Jaber BL; Acute Kidney Injury Advisory Group of the American Society of Nephrology. World incidence of AKI: a meta-analysis. Clin J Am Soc Nephrol. 2013 Sep;8(9):1482-93. Epub 2013 Jun 6. Erratum in: Clin J Am Soc Nephrol. 2014 Jun 6;9(6):1148. [CrossRef]
- Hsu CN, Chen HL, Tain YL. Epidemiology and outcomes of community-acquired and hospital-acquired acute kidney injury in children and adolescents. Pediatr. Res 2018;83:622–629. [CrossRef]
- Kaddourah A, Basu RK, Bagshaw SM, Goldstein SL. AWARE investigators. Epidemiology of acute kidney injury in critically Ill children and young adults. N. Engl. J. Med. 2017;376(1):11–20. [CrossRef]
- Meena J, Mathew G, Kumar J, Chanchlani R. Incidence of Acute Kidney Injury in Hospitalized Children: A Meta–analysis. Pediatrics. 2023; 151(2):e2022058823. [CrossRef]
- Kidney Disease Improving global outcomes (KDIGO) acute kidney injury work group KDIGO clinical practice guideline for acute kidney injury. Kidney Int. 2012;2:1–138. [CrossRef]
- Chawla LS, Bellomo R, Bihorac A, Goldstein SL, Siew ED, Bagshaw SM, et al. Acute Disease Quality Initiative Workgroup 16.. Acute kidney disease and renal recovery: consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat Rev Nephrol. 2017 Apr;13(4):241-257. Epub 2017 Feb 27. [CrossRef]
- Kofman N, Margolis G, Gal-Oz A, Letourneau-Shesaf S, Keren G, Rozenbaum Z, et al. Long-term renal outcomes and mortality following renal injury among myocardial infarction patients treated by primary percutaneous intervention. Coron Artery Dis. (2019) 30:87–92. [CrossRef]
- Fujii T, Uchino S, Takinami M, Bellomo R. Subacute kidney injury in hospitalized patients. Clin J Am Soc Nephrol. (2014) 9:457–61. [CrossRef]
- Yan P, Duan XJ, Liu Y, Wu X, Zhang NY, Yuan F, et al. Acute kidney disease in hospitalized acute kidney injury patients. PeerJ. (2021) 9:e11400. [CrossRef]
- James MT, Levey AS, Tonelli M, Tan Z, Barry R, Pannu N, et al. Incidence and prognosis of acute kidney diseases and disorders using an integrated approach to laboratory measurements in a universal health care system. JAMA Network Open. (2019) 2:e191795. [CrossRef]
- Su CC, Chen JY, Chen SY, Shiao CC, Neyra JA, Matsuura R, et al. Outcomes associated with acute kidney disease: A systematic review and meta-analysis. EClinicalMedicine. 2022 Dec 13;55:101760. [CrossRef]
- Patel M, Hornik C, Diamantidis C, Selewski DT, Gbadegesin R. Patient level factors increase risk of acute kidney disease in hospitalized children with acute kidney injury. Pediatr Nephrol. 2023 Oct;38(10):3465-3474. [CrossRef]
- Patel M, Heipertz A, Joyce E, Kellum JA, Horvat C, Squires JE, et al. Acute kidney disease predicts chronic kidney disease in pediatric non–kidney solid organ transplant patients. Pediatr Transplant. 2022; 26(6):e14172. [CrossRef]
- LoBasso M, Schneider J, Sanchez-Pinto LN, Del Castillo S, Kim G, Flynn A, et al. Acute kidney injury and kidney recovery after cardiopulmonary bypass in children. Pediatr Nephrol. 2022; 37(3):659–665. [CrossRef]
- Daraskevicius J, Azukaitis K, Dziugeviciute-Tupko J, Peciulyte M, Planciunaite R, Vaitkeviciene G, et al. Phenotypes and Baseline Risk Factors of Acute Kidney Injury in Children After Allogeneic Hematopoietic Stem Cell Transplantation. Front Pediatr. 2020; 8:499. [CrossRef]
- Deng YH, Yan P, Zhang NY, Luo XQ, Wang XF, Duan SB. Acute Kidney Disease in Hospitalized Pediatric Patients With Acute Kidney Injury in China. Front Pediatr. 2022; 10:885055. [CrossRef]
- Ayesa N. Mian, George J. Schwartz, Measurement and Estimation of Glomerular Filtration Rate in Children, Advances in Chronic Kidney Disease, Volume 24, Issue 6, 2017, Pages 348-356, ISSN 1548-5595. 2017; 24. [CrossRef]
- Heilbron DC, Holliday MA, Al-Dahwi A. et al. Expressing glomerular filtration rate in children. Pediatr Nephrol 5, 5–11 (1991). [CrossRef]
- Schwartz GJ, Muñoz A, Schneider MF, et al. (2009) New equations to estimate GFR in children with CKD. J Am Soc Nephrol 20:629–637. [CrossRef]
- Lameire NH, Levin A, Kellum JA, et al. (2021) Harmonizing acute and chronic kidney disease definition and classification: report of a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Int 100:516–526. [CrossRef]
- KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney inter., Suppl. 2013; 3, 5–14. [CrossRef]
- Stierman B, Afful J, Carroll MD, Chen T, Davy O, Fink S et al. National Health and Nutrition Examination Survey 2017–March 2020 Prepandemic Data Files Development of Files and Prevalence Estimates for Selected Health Outcomes: Corporate Authors(s) : National Center for Health Statistics (U.S.) Published Date : 06/14/2021 Series : NHSR No. 158 Source : National Health Statistics Reports URL : https://stacks.cdc.gov/view/cdc/106273.
- Carullo N, Zicarelli M, Michael A, Faga T, Battaglia Y, Pisani A, et al. Childhood Obesity: Insight into Kidney Involvement. Int J Mol Sci. 2023 Dec 12;24(24):17400. [CrossRef]
- Namazzi R, Batte A, Opoka RO, Bangirana P, Schwaderer AL, Berrens Z, et al. Acute kidney injury, persistent kidney disease, and post-discharge morbidity and mortality in severe malaria in children: A prospective cohort study. EClinicalMedicine. 2022 Feb 12;44:101292. [CrossRef]
Figure 1.
Kaplan-Meier survival analysis on the risk of new-onset chronic kidney disease. Legend figure 1: AKD = acute kidney disease.
Figure 1.
Kaplan-Meier survival analysis on the risk of new-onset chronic kidney disease. Legend figure 1: AKD = acute kidney disease.
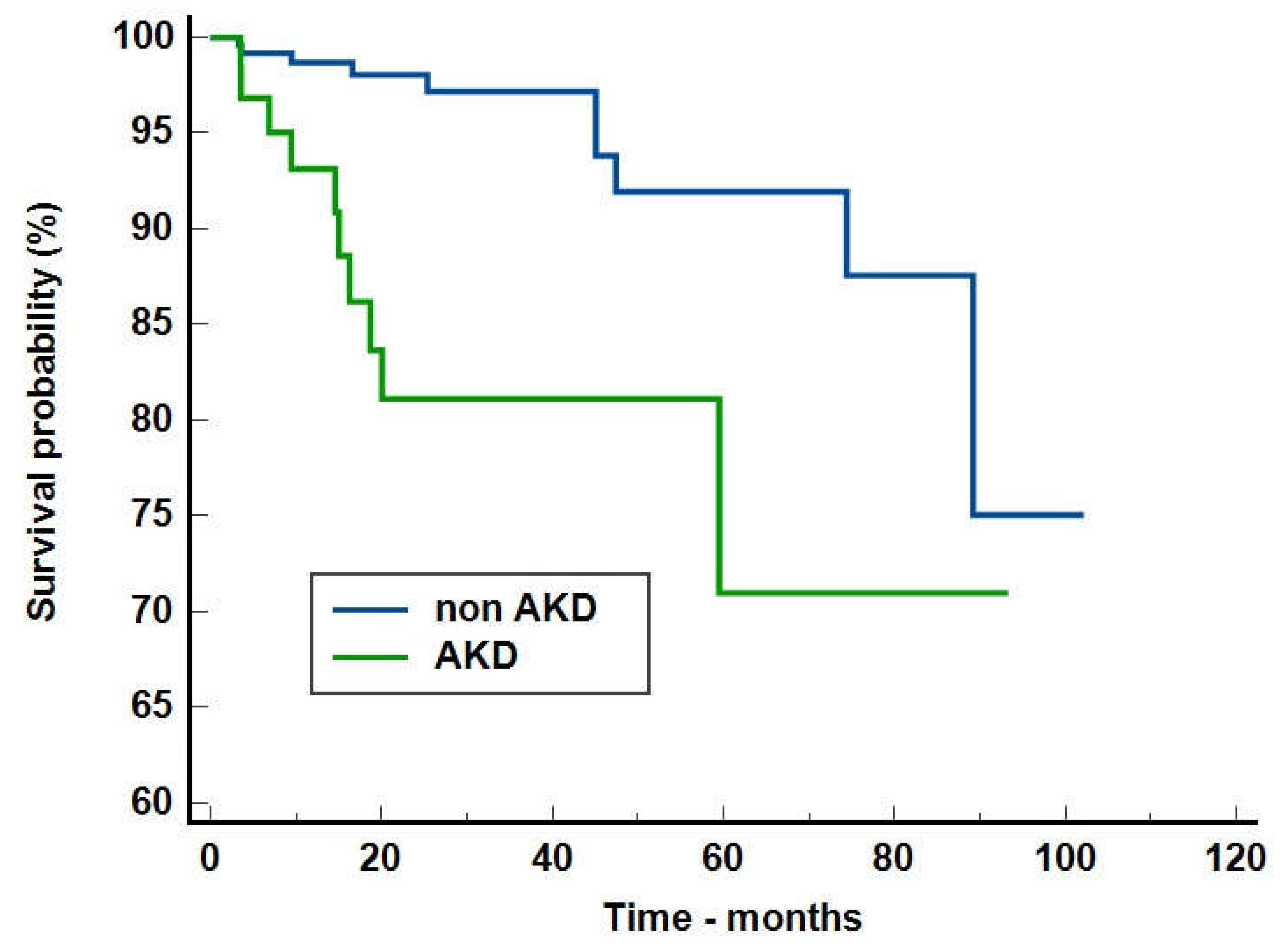
Figure 2.
Cox proportional-hazards regression model on the risk of new-onset chronic kidney disease stratified by acute kidney disease presence Legend figure 2: AKD = acute kidney disease.
Figure 2.
Cox proportional-hazards regression model on the risk of new-onset chronic kidney disease stratified by acute kidney disease presence Legend figure 2: AKD = acute kidney disease.
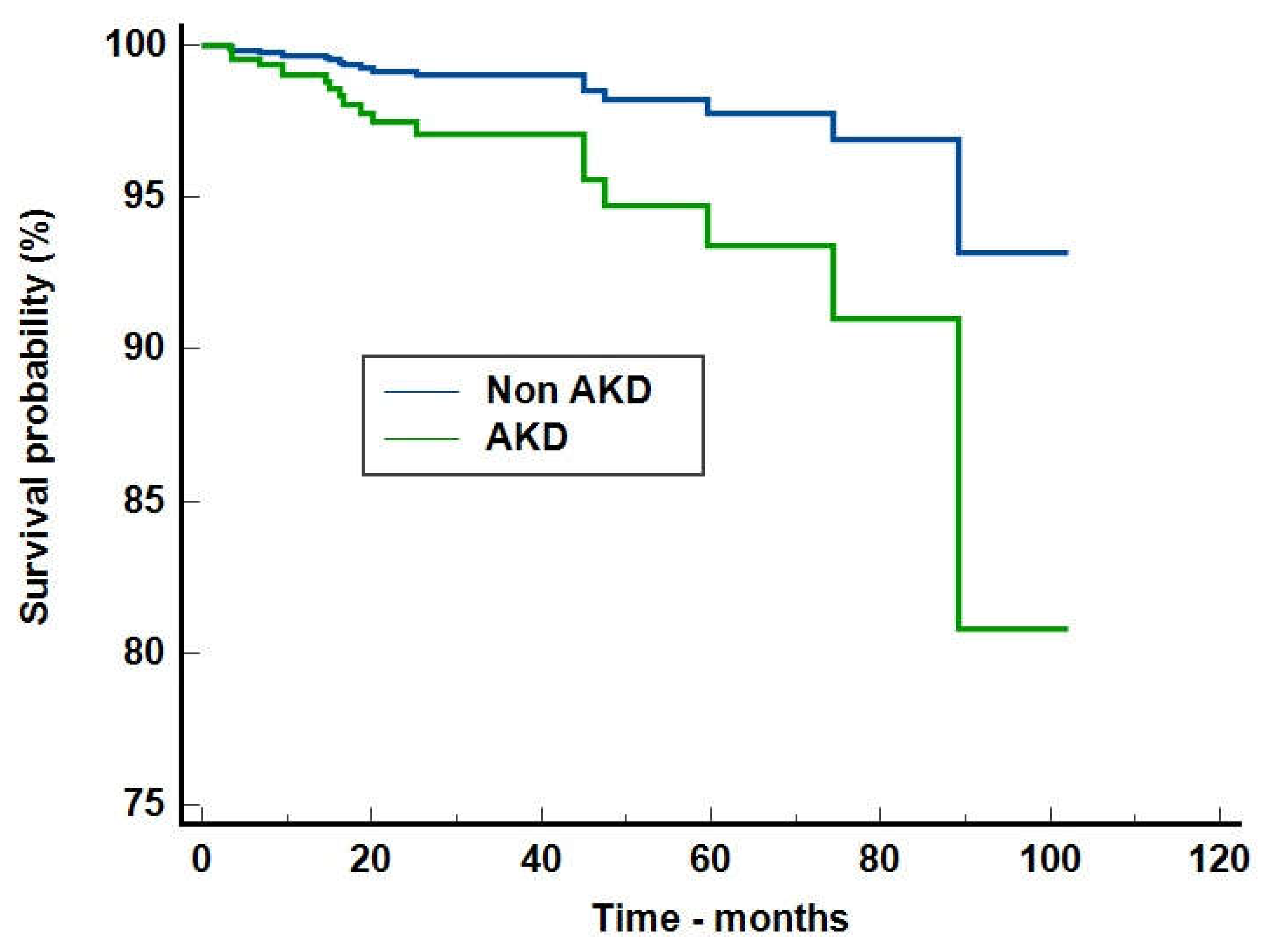

Table 1.
Demographics and baseline characteristics of patients with and without AKD.
| Variable | AKD N=125 | Non-AKD N=611 | Total N=736 | P value | |
| Gender - male | 56 (44.8%) | 333 (54.5%) | 389 (52.9%) | 0.047 | |
| Environment - urban | 67 (53.6%) | 331 (54.2%) | 398 (54.1%) | 0.906 | |
| Age – years M+IQR | 12 (8-15) | 8 (4-14) | 9 (4-14) | <0.0001 | |
| Weight – kg (M+IQR) | 44 (25-59.25) | 26 (16-50) | 29 (16-52) | <0.0001 | |
| Height – cm (M+IQR) | 154 (134.75-164.25) | 126 (103-154) | 131 (104-158) | <0.0001 | |
| BMI – kg/sm (M+IQR) | 18.75 (15.48-23.91) | 17.04 (14.12-20.78) | 17.35 (14.31-21.59) | 0.0125 | |
| Maximum SCr mg/dl (M+IQR) | 1.41 (0.9-3.05) | 0.87 (0.61-1.18) | 0.92 (0.63-1.34) | <0.0001 | |
| Baseline SCr mg/dl (M+IQR) | 0.43 (0.31-0.7) | 0.36 (0.27-0.54) | 0.37 (0.28-0.56) | 0.0005 | |
| GFR ml/min/1.73sm (M+IQR) | 133.5 (83.2-174.3) | 138.4 (109.5-174-2) | 137.7 (106.6-174) | 0.087 | |
| Urea mmol/l (M+IQR) | 10.5 (6.4-23.21) | 5.75 (4.34-8.2) | 6.11 (4.45-9.76) | <0.0001 | |
| Uric acid umol/l (M+IQR) | 391 (259.5-618.5) | 284 (203.75-400) | 297 (217-441) | <0.0001 | |
| Serum proteins g/l (M+IQR) | 56 (44.55-65.4) | 60.2 (51.02-65.87) | 59.5 (49.6-65.77) | 0.031 | |
| Procalcitonin ng/ml | 2.13 (0.48-19.12) | 3.08 (0.37-17.86) | 3.03 (0.4-18.21) | 0.866 | |
| C Reactive protein mg/l (M+IQR) | 59.92 (11.41-184.05) | 28.73 (3.74-132.4) | 35.73 (4.58-14.06) | 0.004 | |
| Sodium mmol/l (M+IQR) | 134 (131-138) | 137 (134-139) | 137 (133-139) | 0.001 | |
| Potassium mmol/l (M+IQR) | 4.3 (3.6-5) | 4.3 (3.8-4.8) | 4.3 (3.8-4.8) | 0.71 | |
| Haemoglobin g/dl (M+IQR) | 9.1 (7.6-11.2) | 11.05 (9.2-12.5) | 10.8 (8.8-12.3) | <0.0001 | |
| AKI stage | 1 | 27 (21.6%) | 275 (45%) | 302 (41%) | <0.0001 |
| 2 | 44 (35.2%) | 195 (31.9%) | 239 (32.5%) | ||
| 3 | 54 (43.2%) | 414 (23.1%) | 195 (26.5%) | ||
| Hospital stay days (M+IQR) | 17 (9.75-31.5) | 8 (4-15) | 9 (5-18) | <0.0001 | |
| IH AKI | 67 (53.6%) | 353 (57.8%) | 420 (57.1%) | 0.39 | |
| ICU admission | 55 (44%) | 187 (30.6%) | 242 (32.9%) | 0.003 | |
| RRT necessity | 12 (9.6%) | 4 (0.7%) | 16 (2.2%) | <0.0001 | |
Legend: AKD=acute kidney disease, N=number, M+IQR=median and interquartile range, kg=kilograms, cm=centimetre, sm=square meter, SCr=serum creatinine, mg=miligrams, dl=decilitre, umol=micromoles, l=litre, g=grams, mmol=milimols, AKI=acute kidney injury, IH=in hospital, ICU=intensive care unit. Statistical tests: Chi-square test or Mann-Whitney test as appropriate.
Table 2.
Exposures and susceptibilities distribution in patients with and without AKD.
| Parameter | AKD N=125 | Non-AKD N=611 | Total N=736 | OR and 95%CI | P value | |
| Exposures | Mechanical ventilation | 36 (28.8%) | 136 (22.3%) | 172 (23.4%) | 1.41 (0.91-2.17) | 0.115 |
| Sepsis | 57 (45.6%) | 178 (29.1%) | 235 (31.9%) | 2.03 (1.37-3.02) | 0.0003 | |
| Critical illness | 17 (13.6%) | 45 (7.4%) | 62 (8.4%) | 1.97 (1.09-2.65) | 0.022 | |
| Hypovolemic shock | 3 (2.4%) | 18 (2.9%) | 21 (2.9%) | 0.81 (0.23-2.79) | 0.738 | |
| Trauma | 2 (1.6%) | 35 (5.7%) | 37 (5%) | 0.26 (0.06-1.12) | 0.054 | |
| Major non-cardiac surgery | 10 (8%) | 62 (10.1%) | 72 (9.8%) | 0.77 (0.38-1.54) | 0.461 | |
| Nephrotoxins | 49 (39.2%) | 122 (20%) | 171 (23.2%) | 2.58 (1.71-3.89) | <0.0001 | |
| Poisonous plants | 3 (2.4%) | 12 (2%) | 15 (2%) | 1.22 (0.34-4.41) | 0.735 | |
| Susceptibilities | Dehydration/Volume depletion | 115 (92%) | 584 (95.6%) | 699 (95%) | 0.53 (0.25-1.12) | 0.095 |
| Chronic kidney disease | 15 (12%) | 39 (6.4%) | 54 (7.3%) | 2 (1.06-2.73) | 0.028 | |
| Chronic disease (heart, liver and lung) | 19 (15.2%) | 68 (11.1%) | 87 (11.8%) | 1.43 (0.83-2.47) | 0.199 | |
| Diabetes mellitus | 3 (2.4%) | 25 (4.1%) | 28 (3.8%) | 0.57 (0.17-1.93) | 0.368 | |
| Neoplasia | 41 (32.8%) | 93 (15.2%) | 134 (18.2%) | 2.71 (1.76-4.19) | <0.0001 | |
| Anaemia | 92 (73.6%) | 295 (48.3%) | 387 (52.6%) | 2.98 (1.94-4.58) | <0.0001 | |
| Heart failure | 27 (21.6%) | 39 (6.4%) | 66 (9%) | 4.04 (2.36-6.9) | <0.0001 | |
| Arterial hypertension | 26 (20.8%) | 41 (6.7%) | 67 (9.1%) | 3.65 (2.13-6.23) | <0.0001 | |
| Stem cell transplant | 8 (6.4%) | 15 (2.5%) | 23 (3.1%) | 2.71 (1.12-6.55) | 0.021 | |
| Female gender | 69 (55.2%) | 278 (45.5%) | 347 (47.1%) | 1.47 (1-2.17) | 0.047 |
Legend: AKD=acute kidney disease, N=number. The statistical test is Chi-square test.
Table 3.
AKI causes and AKD development.
| AKI cause | OR (95%CI) | P value | |
| Prerenal | Hypovolemia/ Dehydration | 0.11 (0.06-0.19) | <0.0001 |
| Systemic vasodilatation | 1.25 (0.76-2.06) | 0.361 | |
| Hypoxia/ Ischemia | 0.74 (0.25-2.17) | 0.588 | |
| Renal | Renal microvasculature alterations | 6.89 (2.34-20.23) | 0.0004 |
| Glomerulonephritis | 4.74 (1.96-11.42) | 0.0005 | |
| Acute tubular necrosis | 5.01 (1.23-20.33) | 0.023 | |
| Acute tubule-interstitial nephritis | 3.39 (2.26-5.08) | <0.0001 | |
| Postrenal | Urinary tract malformation/ obstruction | 0.97 (0.32-2.9) | 0.966 |
Legend: OR=odds ratio, 95%CI=95% confidence interval.
Table 4.
Acute kidney disease stages analysis.
| Non AKD N=611 (83%) | AKD stage 1 N=55 (7.5%) | AKD stage 2 N=26 (3.5%) | AKD stage 3 N=44 (6%) | P value | ||
| AKI | AKI stage 1 N=302 (41%) | 275 (45%) | 22 (40%) | 1 (3.8%) | 4 (9.1%) | <0.0001 |
| AKI stage 2 N=239 (32.5%) | 195 (31.9%) | 23 (41.8%) | 16 (61.5%) | 5 (11.4%) | ||
| AKI stage 3 N=195 (26.5%) | 141 (23.1%) | 10 (18.2%) | 9 (34.6%) | 35 (79.5%) | ||
| ICU admission | 187 (30.6%) | 17 (30.9%) | 9 (34.6%) | 29 (65.9%) | <0.0001 | |
| Hospital stay | 8 (4-15) | 12 (8-24.2) | 18 (10-33) | 24 (14.5-39.5) | <0.0001 | |
| Baseline creatinine | 0.36 (0.27-0.54) | 0.5 (0.36-0.71) | 0.34 (0.27-0.5) | 0.39 (0.32-0.77) | 0.0005 | |
| Baseline GFR | 138.4 (109.5-174.2) | 125.5 (88.3-173.2) | 140.2 (95.3-214.3) | 132.7 (69.3-170.9) | 0.207 | |
| AKD duration | - | 6 (3-19.75) | 8.5 (3-20) | 11 (5-23) | 0.354 | |
| Subsequent AKI events | 54 (8.8%) | 3 (5.5%) | 3 (11.5%) | 3 (6.8%) | 0.752 | |
Legend: AKD=acute kidney disease, AKI=acute kidney injury, N=number, statistical analysis: Chi-square test or Kruskal-Wallis test as appropriate.
Table 5.
Acute kidney disease influence on mortality.
| Crude analysis OR and 95%CI | Adjusted analysis OR and 95%CI | |
| Mortality risk during hospitalization | 4.22 (2.11-8.4), p<0.0001 | 3.13 (1.5-6.51), p=0.0022 |
| Mortality risk after discharge | 2.73 (1.003-7.44), p=0.049 | 2.73 (1.003-7.44), p=0.049 |
| Overall mortality | 3.75 (2.09-6.72), p<0.0001 | 2.98 (1.63-5.45), p=0.0004 |
Legend: OR=odds ratio, 95%CI=95% confidence interval, adjusted for age, sex, environment, acute kidney injury stages and subsequent acute kidney injury. The adjusted performed analysis was performed using logistic regression.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



