
Submitted:
15 April 2024
Posted:
16 April 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Understanding vaccine hesitancy in organ transplant recipients (OTR) is critical, given clear, alt-hough attenuated, benefits from vaccination. Adult OTR were surveyed regarding vaccine-related values and a novel outcome variable called Vaccine Acceptance Composite Score (VACS) was built as the average Likert score of 7 domains of vaccination confidence. Of 46 OTR included (93.5% kidney transplant recipients), 32.6% were female, 13.3% Black, 6.77% Hispan-ic/Latino/a/x; median age was 58 years. Patients were most concerned about COVID-19 vac-cine-associated risks (46.3%), its potential effect on allograft (47.6%) and motives of government officials involved with vaccine policy (55.6%). Politically conservative patients were likely to have a significantly lower VACS, while those who lived with someone ≥65 had a higher VACS. The VACS was not significantly associated with race, income, religious beliefs, comorbidities, COVID-19 history, or influenza vaccination status. Higher VACS was significantly associated with ≥3 and ≥4 COVID-19 immunizations. This study highlighted political beliefs and elderly household members as correlates of vaccine acceptance among OTR. The VACS may be a useful tool to help standardize multifaceted analyses in vaccination-focused behavioral research, as well as identify individuals and groups at risk for vaccine hesitancy, who may benefit from tai-lored outreach and educational interventions.
Keywords:
COVID-19
; vaccine
; transplant
; vaccine hesitancy
; vaccine attitudes
; public health
1. Introduction
The COVID-19 pandemic has caused an estimated 700 million cases and 7 million deaths worldwide [1]. The rollout of mRNA vaccines in December 2020 was the largest concerted public health campaign in history, saving an estimated 2.4 million lives within the first eight months of implementation [2]. As organ transplant recipients (OTR) may have increased rates of morbidity and mortality from severe COVID-19 disease [3,4], vaccination has been critical in saving OTR lives [5] despite blunted immune response [6].
The pandemic of vaccine hesitancy, recognized by the World Health Organization as one of the top 10 global health threats in 2019 [7], has undermined the reach of public health efforts against COVID-19. Vaccine hesitancy encompasses a spectrum of beliefs that result in indecision, ambivalence, or resistance to a given vaccine. Its wide range of causes includes barriers to access, medical misinformation or lack of information, concerns regarding adverse effects, administration mechanisms, efficacy against infection, and mistrust in the medical system, drug testing process, or the state [8,9,10].
These beliefs are observed across various sociodemographic categories, but overall tend to be more prevalent among populations such as Black/African American individuals, Hispanic/Latino individuals, people who receive less income, and people who have received less education [11,12,13]. Such disparities in the uptake of vaccines, as well as treatments for COVID-19, have been attributed to limited access to healthcare professionals and reduced interaction with the healthcare system, mistrust of biomedical and healthcare institutions founded in historical and present racism and classism, inadequate recruitment in clinical trials, concerns related to the cost of vaccination, and reduced access to educational opportunities, particularly regarding vaccination [12,14,15,16]. At the same time, people of color have faced elevated risks of contracting SARS-CoV-2 and experiencing COVID-associated mortality [16,17], though this disparity seems to have narrowed and even shifted over the course of the pandemic [18]. Still, addressing and overcoming barriers to vaccination to ensure equitable access to protection and health care remains a priority for this and future pandemics, considering patients who have multiply marginalized identities.
Limited data suggest nuances in vaccine-hesitant beliefs extend to individuals who are immunocompromised, including OTR, who may harbor distinct anxieties and fears regarding vaccination such as concerns about interactions with their allograft [19,20,21], comorbid conditions [22], or immunosuppressive medications [20,23,24]. The coalescence of transplant recipients’ experiences of chronic illness and long-term healthcare exposures with race and experiences of racism, religious beliefs, political views, and other identity categories, has yet to be examined in the context of vaccine belief formation.
To this end, we aimed to investigate the perceptions of COVID-19 vaccination among OTR and characterize sociodemographic and interpersonal factors that might influence their beliefs. We surveyed OTR anonymously on their sociodemographic data, medical history, and multiple pillars of vaccine beliefs, and employed a novel metric, the Vaccine Acceptance Composite Score (VACS), to analyze their relative COVID-19 vaccine acceptance. These data can potentially inform clinicians, policymakers, and the broader transplant community about targeted educational and medical outreach [25] that may benefit OTR, as well as other immunocompromised individuals.
2. Materials and Methods
2.1. Study Design and Data Collection
Patients at least 18 years old who received at least 1 organ transplant were surveyed anonymously between May 27 and September 15, 2023. Subjects were sourced from clinical practice at the organ transplant clinics at Rhode Island Hospital (Providence, RI), and recruited through word-of-mouth in routine clinical care, flyers posted at clinic sites, and patient portal messages.
Through a QR code and website link, subjects were invited to complete an anonymous online questionnaire inquiring about their demographic information, self-reported medical history, and beliefs regarding vaccination. The complete content of the survey instrument is available online [26]. Its development was informed by the scoping review protocol on vaccine hesitancy presented by Oduwole et al. [27] and the Centers for Disease Control and Prevention (CDC) Vaccine Confidence Survey Question Bank [28]. No monetary incentive was provided for participation.
The questionnaire and its data were hosted, collected, and stored on Qualtrics XM, versions May-September 2022 (Qualtrics, Provo, Utah). The Lifespan Institutional Review Board determined this study qualified for exemption under the Code of Federal Regulations Title 45 § 46.104(d)(2i)(2ii).
2.2. Data Analyses
Sociodemographic data, medical history, vaccine perceptions and beliefs across the cohort were summarized with the percentage of the cohort represented (with the exception of age, summarized as median with interquartile range).
We further developed a novel comprehensive outcome variable called the Vaccine Acceptance Composite Score (VACS), which was calculated as the average of the Likert scores across seven evaluated domains of vaccination confidence:
- Concern for COVID-19 vaccine-associated risks (Likert scale inverted to correct for confidence orientation of the VACS);
- Safety of the vaccine for the general public;
- Safety of the vaccine for transplant patients;
- Confidence that the vaccine has been adequately studied;
- Confidence that vaccines are useful at preventing infectious diseases;
- Confidence that receiving a vaccine is better than becoming ill from COVID-19;
- Confidence that SARS-CoV-2 is real.
The VACS was captured as a continuous variable and transformed into a 3-category ordinal variable: <2.5; 2.5-4.0; >4.0. We applied ordinal logistic regression and relative operating characteristic (ROC) analyses to examine the association of VACS with several sociodemographic and medical factors, as well as individual adherence to COVID-19 vaccine recommendations, respectively. We calculated univariable odds ratios (OR), with VACS as an ordinal variable, and ROC areas under the curve (AUC), with VACS as a continuous variable relative to ≥3 and ≥4 prior vaccinations, with 95% confidence intervals (CI). Statistical analyses were conducted using R, version 4.0.5 (R Foundation for Statistical Computing). A two-tailed p-value of 0.05 determined statistical significance.
3. Results
Of 51 OTR who started the survey, 4 did not complete it; only one patient was unvaccinated and therefore excluded as an outlier from analysis. 46 OTR who completed the survey had received at least one dose of a COVID vaccine and were therefore included for analysis.
3.1. Study Cohort
Sociodemographic data and medical history are summarized in Table 1. The median age was 58 (interquartile range (IQR) 48-64) years. 32.6% identified as female. 68.9% identified as White, 13.3% identified as Black or African American, and 6.7% identified as Hispanic or Latino/a/x. 21.7% were born outside of the United States, and three spoke English as a second language. 78.3% had at least some college education. Nearly all (92.9%) caregivers reported that their children received all pediatrician-recommended vaccines. 47.8% were currently working, while 34.8% were retired. 47.7% identified as liberal, left or Democrat; 13.6% as conservative, right or Republican; and 38.6% as independent or without a party affiliation. 33.3% of the cohort had changed their political affiliation over time. 90.7% of patients were raised Catholic or another Christian denomination, though only 54.5% identified as currently spiritual or religious. Socioeconomically, this cohort skewed wealthier, with 32.6% of patients in the highest quintile of annual household income ($141,001+).
Regarding medical history (Table 1): 82.6% of patients received one organ transplant, 93.5% a kidney (other organs were heart, pancreas, lung and liver). 52.3% of our cohort received a transplant since mid-2020, overlapping with the timepoint when the COVID-19 vaccine mandate for procedures at our transplant center in effect. 78.3% of patients had two or more medical comorbidities, mainly chronic kidney disease, hypertension, diabetes, or congestive heart failure. 63.0% had previously had COVID-19 disease, 89.3% of whom contracted it since vaccine rollout in December 2020. 5 of 27 respondents (18.5%) with a history of COVID-19 illness required hospitalization. 82.6% of patients had received ≥3 COVID-19 immunizations, the majority of whom ≥4 (aligned with the CDC recommendations at the time of the survey).
3.2. Vaccine Hesitancy
Perceptions and values related to the COVID-19 vaccine and vaccination more broadly are summarized in Table 2. Only one respondent answered all values-related questions with extreme (1 or 5) Likert scores. The most common concerns were: COVID-19 vaccine-associated risks (46.3%), close to COVID-19-associated risks (59.1%), with 21.7% unconfident that receiving the vaccine is superior to contracting COVID-19 while unvaccinated; the vaccine’s potential effect on allograft (47.6%); and motives of government officials involved with vaccine policy (55.6%). 26.7% of patients were doubtful that SARS-CoV-2 is real. 32.6% of patients were doubtful that vaccines are useful against infectious diseases. Of 5 patients who contracted COVID before being vaccinated, only 1 felt confident that the vaccine would have helped avoid symptoms. Three patients reported they had received medical advice to avoid COVID-19 vaccination. Patients expressed high levels of doubt in understanding of the vaccine among their colleagues and friends (66.7%), family (43.5%), and even self (32.6%), with nearly half reporting difficulty assessing the accuracy of COVID-19 information in the media. OTR with no history of COVID-19 disease did not have significantly different vaccine beliefs compared to OTR with a positive history.
OR correlating sociodemographic and self-reported medical data with VACS are presented in Figure 1, and the ROC curves correlating ≥3 or 4 immunizations with the VACS in Figure 2. Patients who identified as politically conservative were likely to have a lower VACS (OR 0.35, 95%CI 0.18-0.69), while those who lived with someone ≥65 years old were likely to have a higher VACS (OR 2.02, 95%CI 1.18-3.46). The VACS was not significantly associated with race, income, religious beliefs, number of comorbidities, COVID-19 history, or influenza vaccination status. Higher VACS was strongly associated with history of at least 3 (ROC AUC 0.87, 95%CI 0.76-0.98) and 4 (OR 2.04, 95%CI 1.27-3.29; ROC AUC 0.84, 95%CI 0.72-0.96) COVID-19 immunizations.
4. Discussion
Characterizing the pervasiveness and “emotional epidemiology” of the vaccine hesitancy landscape [8] is critical to limiting its adverse impact on human health, especially for vulnerable populations. However, it is difficult to compare vaccine hesitancy through time and space given non-standardized, disjointed, and asynchronous data collection, as well as evolving vaccine access. In May 2021 in China, 77.2% of 813 OTR surveyed were classified as vaccine-hesitant, and only 5.7% were vaccinated at the time [22]. On the contrary, in early 2022, of 1019 OTR surveyed at a single center in Italy who had already received 2 immunizations and were eligible for a third, only 5% were considered hesitant [9].
Many factors lead to incomparability of such surveys, including different country-wide experiences of the COVID-19 pandemic, cultural attitudes toward the vaccine, varying definitions for vaccine hesitancy, non-standardized survey methods, and different inclusion groups. Overall, however, vaccine hesitancy likely decreased over the course of the pandemic: a metanalysis in India aggregating more than 60,000 respondents found that hesitancy dropped from 37% in December 2020 to 12.1% in November 2021, as most people who chose to “wait and see”, especially those who were medically compromised, opted into vaccination [29]. An international study aggregating 23,000 responses from 23 countries likewise reported about a 4% decrease in vaccine hesitancy from 2020 to 2021 [30]. In the above metanalysis from India, the three most common factors contributing to vaccine hesitancy were fear of adverse effects, inefficacy, and poor safety––largely congruent with studies focused on OTR [9,19,20,21,22,23,24,31,32], including our own.
In this study assessing attitudes toward COVID-19 vaccination among 46 OTR at our transplant center, we found that patients expressed vaccine-hesitant beliefs across domains ranging from the vaccine itself, to potential interference with their health, to societal and political factors at play during its development and rollout. Patients were most concerned about the degree to which the COVID-19 vaccine had been studied, the potential for adverse effects of the vaccine on their allograft, and the motives of vaccine-supportive policymakers (Table 2). Nearly half were concerned about the effect of the vaccine on their transplant organ (Table 2), a concern noted in prior studies as well [19,20,21]. Patients who lived in households with adults ages 65 and older, and patients who did not identify as conservative or politically right-leaning, had higher VACS (Figure 1), which correlated with receiving the full vaccine series (Figure 1 and Figure 2).
The employment of the Emergency Use Authorization by the Food and Drug Administration (FDA) to fast-track vaccine research and rollout, and intense government financial and other resources toward vaccine development and deployment [25], against the United States’ tumultuous partisan political backdrop in the early 2020s, likely contributed to engendering mistrust in policymaker motives among the American populace. Our study showed the OTR population was no exception. In a longitudinal study in mid-2020 before vaccine rollout, Fridman et al. observed a decline in pro-vaccine sentiment among Republicans, though not Democrats [33], at a time when the former US president vocally favored accelerated vaccine research and development [34]. This hesitancy of the constituent party despite concordant leadership may be rooted in modern conservative values of government mistrust above leadership concordance [35].
Notably, age, gender, race, education, income, comorbidities, and history of SARS-CoV-2 infection were not correlated with a change in VACS. The level of education and influenza vaccine history did not correlate with higher VACS, either, in contrast to one previous study of OTR [22]. Although such observations could be attributed to our small sample, they could also reflect higher level of trust in more established, longer studied, fully FDA-approved preventative interventions. The finding that Black identity did not correlate with vaccine hesitancy aligns with several prior studies: a case-control study of 930 total patients [36] who noted the diminishing discrepancy of vaccination rates between Black patients and other racial and ethnic groups over the course of the pandemic; a national survey conducted over the course of six waves of COVID [37] noting increased rate of vaccine uptake in this population compared to White respondents; and a Rhode Island-specific study that demonstrated no significant discrepancy in vaccine hesitancy associated with race or ethnicity, though with small samples of non-White respondents [38]. However, these findings contrast with a nationwide review from 2021 pooling over 100,000 participants that demonstrated significantly higher vaccine hesitancy among Black and Hispanic Americans compared to their White counterparts [12]. It is possible that well-orchestrated, local outreach efforts with trauma-informed and transparent language [39] may have contributed toward diminishing hesitancy towards vaccination among racial and ethnic minorities.
Importantly, a third of the study cohort was not confident that vaccines are useful for preventing infectious disease (Table 2); over a fourth doubted the existence of SARS-CoV-2; and a fifth felt unconfident that receiving a COVID vaccine was superior to falling ill with COVID (Table 2). Patients expressed doubt in their own understanding, as well as their family’s, friends’, and colleagues’ understanding of the vaccine, and admitted difficulty evaluating the veracity of media, indicating a need to strengthen basic vaccine education, even among this group with otherwise highly specialized medical care, including vaccine mandates. With such high-touch care and longstanding relationships with this patient cohort, providers have a uniquely powerful opportunity [31,32] to relay clear, firm, and positive vaccine messaging, to combat ambiguous or negative medical messaging patients may have received or perceived, evidenced in this (Table 2) and prior studies [22,25,40].
Our study has several strengths. It was hosted at a single hospital and thus captures a distinct spatiotemporal moment of vaccine hesitancy in a specific, homogeneous cohort during a rather narrow timeframe spanning the most recent phases of the pandemic. The variety and specificity of questions provide depth and breadth to understanding patients’ beliefs. It was self-directed, unobserved and without monetary incentive, potentially decreasing response bias. It also introduced and internally validated the VACS, a novel metric that could offer future standardization and depth for similar studies. The survey itself, although extensive (Suppl. Material), had a high completion rate once started, with only 4 participants excluded for incomplete responses.
This study also has its limitations: The survey tool and VACS were piloted with a relatively small single-center sample size. Our results have not been externally validated yet. The small sample size further precluded multivariable analyses. Data on the number of online viewings of the survey were not collected, so a response rate cannot be derived. The survey itself is thus susceptible to self-selection bias, for individuals with strong pro- or anti-vaccination opinions being more likely to complete the survey, leading to extreme responding. However, only one respondent answered all values-related questions with extreme (1 or 5) Likert scores, supporting the limited effect of self-selecting for strong attitudes in the present study. Three patients spoke English as their second language, and the survey was not offered in their primary language. Although the questionnaire offered depth into the respondents’ positionalities and beliefs, it was not totally comprehensive, e.g., questions on food or drug allergies–which may affect vaccine uptake and beliefs. Zip codes were not asked, while local geography often correlates with socioeconomic status and even access to vaccination, based on studies from larger states [36], although less so in the smallest state; notably, income and education were not found to significantly correlate with the VACS.
Last, this study excluded one respondent who had never received a COVID-19 vaccine. However, it is unclear how many patients had received at least one immunization primarily driven by their own volition versus solely to remain eligible to receive a transplant, as one patient noted in the free response portion at the end of the survey. Unfortunately, it was not possible to parse these two populations based on the survey data. 52.3% of our cohort received a transplant since mid-2020, providing an upper bound for the maximum number of individuals who could have been affected by the hospital mandate. Mandating vaccination among vaccine-hesitant individuals would not have skewed the VACS directly, as the composite score is attitude rather than behavior-based (Figure 1). Moreover, the vaccine mandate only required 2 doses, so it is less likely that the ROC measuring adherence to the CDC recommendation of 4 immunizations at time of survey would be substantially affected (Figure 2).
In conclusion, this study identified demographic factors associated with vaccine-hesitant beliefs using a novel composite metric of vaccine confidence, which correlated with number of immunizations received, in a cohort of OTR at a single transplant center. It further identified areas of misinformation and self-doubt within participants’ understanding of COVID-19 and the vaccines against it, highlighting the need for continued provider efforts in patient education. Future research should investigate which factors of the VACS drive its correlation with these demographic features and number of immunizations the most, and how to tailor, generalize, or relatively weight its components to other vulnerable populations or to the general public. After external validation, the VACS may offer a fast, comprehensive, and standardized option of assessing vaccine hesitancy in cohorts including and beyond OTR.
Supplementary Materials
The complete content of the survey instrument is available online at: https://brown.co1.qualtrics.com/jfe/preview/previewId/3de88941-5624-4c93-86ce-cb271f6c03d8/SV_3HMs57IdLpULMdE?Q_CHL=preview&Q_SurveyVersionID=current.
Author Contributions
Conceptualization, R.L. and D.F.; methodology, R.L., D.G., and D.F.; software, R.L., P.A., D.G., and D.F.; validation, R.L., P.A., D.G., and D.F.; formal analysis, R.L., P.A., D.G., and D.F.; investigation, R.L., D.G., and D.F.; resources, R.L., D.G., and D.F.; data curation, R.L., D.G., and D.F.; writing—original draft preparation, R.L., D.G., and D.F.; writing—review and editing, R.L., P.A., D.G., and D.F.; visualization, R.L., P.A., and D.F.; supervision, R.L. and D.F.; project administration, R.L. and D.F.; funding acquisition, R.L., D.G., P.A., and D.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Infectious Diseases Society of America Grants for Emerging Researchers/Clinicians Mentorship Program; the Emerging Infectious Diseases Scholars Program, grant number R25AI140490; and the Brown University Summer Research Assistantship Program.
Institutional Review Board Statement
This study was determined to qualify for exemption under the Code of Federal Regulations Title 45 § 46.104(d)(2i)(2ii) by the Institutional Review Board of Lifespan Health System.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Acknowledgments
The authors are grateful to the patients and medical providers of the Transplant Center at Rhode Island Hospital for making this research possible and valuable for future patients. The present study will be partially presented at the American Transplant Conference, 2024.
Conflicts of Interest
DF has received research support from Viracor, Astellas, Merck, and AstraZeneca, and consultant fees from Viracor. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Worldometer. Coronavirus Death Tool. Available online: https://www.worldometers.info/coronavirus/coronavirus-death-toll/.
- Agrawal, V.; Sood, N.; Whaley, C.M. The impact of the global COVID-19 vaccination campaign on all-cause mortality; National Bureau of Economic Research: 2023.
- Hippisley-Cox, J.; Coupland, C.A.; Mehta, N.; Keogh, R.H.; Diaz-Ordaz, K.; Khunti, K.; A Lyons, R.; Kee, F.; Sheikh, A.; Rahman, S.; et al. Risk prediction of covid-19 related death and hospital admission in adults after covid-19 vaccination: National prospective cohort study. BMJ 2021, 374, n2244. [Google Scholar] [CrossRef]
- Søfteland, J.M.; Li, H.; Magnusson, J.M.; Leach, S.; Friman, V.; Gisslén, M.; Felldin, M.; Schult, A.; Karason, K.; Baid-Agrawal, S.; et al. COVID-19 Outcomes and Vaccinations in Swedish Solid Organ Transplant Recipients 2020–2021: A Nationwide Multi-Register Comparative Cohort Study. Viruses 2024, 16, 271. [Google Scholar] [CrossRef]
- Lerner, A.H.; Arvanitis, P.; Vieira, K.; Klein, E.J.; Farmakiotis, D. mRNA Vaccination Decreases COVID-19-Associated Morbidity and Mortality Among Organ Transplant Recipients: A Contemporary Cohort Study. Open Forum Infect. Dis. 2022, 9, ofac503. [Google Scholar] [CrossRef]
- Chen, X.; Luo, D.; Mei, B.; Du, J.; Liu, X.; Xie, H.; Liu, L.; Su, S.; Mai, G. Immunogenicity of COVID-19 vaccines in solid organ transplant recipients: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 29, 441–456. [Google Scholar] [CrossRef]
- Ten threats to global health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019.
- Larson, H.J.; Gakidou, E.; Murray, C.J. The Vaccine-Hesitant Moment. New Engl. J. Med. 2022, 387, 58–65. [Google Scholar] [CrossRef]
- Costantino, A.; Morlacchi, L.; Donato, M.F.; Gramegna, A.; Farina, E.; Dibenedetto, C.; Campise, M.; Redaelli, M.; Perego, M.; Alfieri, C.; et al. Hesitancy toward the Full COVID-19 Vaccination among Kidney, Liver and Lung Transplant Recipients in Italy. Vaccines 2022, 10, 1899. [Google Scholar] [CrossRef]
- Thunström, L.; Ashworth, M.; Finnoff, D.; Newbold, S.C. Hesitancy Toward a COVID-19 Vaccine. Ecohealth 2021, 18, 44–60. [Google Scholar] [CrossRef]
- Reece, S.; CarlLee, S.; Scott, A.J.; Willis, D.E.; Rowland, B.; Larsen, K.; Holman-Allgood, I.; McElfish, P.A. Hesitant adopters: COVID-19 vaccine hesitancy among diverse vaccinated adults in the United States. Infect. Med. 2023, 2, 89–95. [Google Scholar] [CrossRef]
- Khubchandani, J.; Macias, Y. COVID-19 vaccination hesitancy in Hispanics and African-Americans: A review and recommendations for practice. Brain, Behav. Immun. - Heal. 2021, 15, 100277. [Google Scholar] [CrossRef]
- Yasmin, F.; Najeeb, H.; Moeed, A.; Naeem, U.; Asghar, M.S.; Chughtai, N.U.; Yousaf, Z.; Seboka, B.T.; Ullah, I.; Lin, C.-Y.; et al. COVID-19 Vaccine Hesitancy in the United States: A Systematic Review. Front. Public Heal. 2021, 9, 770985. [Google Scholar] [CrossRef]
- Klein, E.J.; Hardesty, A.; Vieira, K.; Farmakiotis, D. Use of anti-spike monoclonal antibodies in kidney transplant recipients with COVID-19: Efficacy, ethnic and racial disparities. Am. J. Transplant. 2022, 22, 640–645. [Google Scholar] [CrossRef]
- Fu, J.; Reid, S.A.; French, B.; Hennessy, C.; Hwang, C.; Gatson, N.T.; Duma, N.; Mishra, S.; Nguyen, R.; Hawley, J.E.; et al. Racial Disparities in COVID-19 Outcomes Among Black and White Patients With Cancer. JAMA Netw. Open 2022, 5, e224304. [Google Scholar] [CrossRef]
- Pandita, A.; Gil, R.M.; Farmakiotis, D. Call for Action: Racial Disparities in Clinical Research. Clin. Infect. Dis. 2020, 73, 356–357. [Google Scholar] [CrossRef]
- Laurencin, C.T.; Wu, Z.H.; McClinton, A.; Grady, J.J.; Walker, J.M. Excess Deaths Among Blacks and Latinx Compared to Whites During Covid-19. J. Racial Ethn. Heal. Disparities 2021, 8, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Laurencin, C.T.; Wu, Z.H.; Grady, J.J.; Wu, R.; Murray, M.M.; Slivinsky, M. The Shift: COVID-19-Associated Deaths are Now Trending Lower Among Blacks and Hispanics Compared to Whites. J. Racial Ethn. Heal. Disparities 2023, 10, 3188–3193. [Google Scholar] [CrossRef] [PubMed]
- Basic-Jukic, N.; Furic-Cunko, V.; Jelakovic, B. COVID-19 vaccine hesitancy in renal transplant recipients. Ther. Apher. Dial. 2021, 26, 482–483. [Google Scholar] [CrossRef] [PubMed]
- Liew, I.; Kadir, H.; Thangaraju, S.; Ho, Q.; Ng, E.; Foo, F.; Kee, T. COVID-19 vaccine acceptance among kidney transplant recipients in Singapore. Singap. Med J. 2023. [Google Scholar] [CrossRef]
- Ou, M.T.B.; Boyarsky, B.J.; Zeiser, L.B.S.; Chiang, T.P.-Y.; Ruddy, J.B.; Rasmussen, S.E.B.V.P.; Martin, J.; Russell, J.P.S.C.; Durand, C.M.; Avery, R.K.; et al. Kidney Transplant Recipient Attitudes Toward a SARS-CoV-2 Vaccine. Transplant. Direct 2021, 7, e713. [Google Scholar] [CrossRef]
- Chen, T.; Li, X.; Li, Q.; Huang, L.; Cai, Q.; Wang, Y.; Jiang, Y.; Xu, Q.; Lv, Q.; Wang, J. COVID-19 vaccination hesitancy and associated factors among solid organ transplant recipients in China. Hum. Vaccines Immunother. 2021, 17, 4999–5006. [Google Scholar] [CrossRef]
- Tsapepas, D.; Husain, S.A.; King, K.L.; Burgos, Y.; Cohen, D.J.; Mohan, S. Perspectives on COVID-19 vaccination among kidney and pancreas transplant recipients living in New York City. Am. J. Heal. Pharm. 2021, 78, 2040–2045. [Google Scholar] [CrossRef]
- MacEwan, S.R.; Gaughan, A.A.; Dixon, G.N.; Olvera, R.G.; Tarver, W.L.; Rahurkar, S.; Rush, L.J.; Schenk, A.D.; Stevens, J.; McAlearney, A.S. Understanding Concerns about COVID-19 and Vaccination: Perspectives from Kidney Transplant Recipients. Vaccines 2023, 11, 1134. [Google Scholar] [CrossRef]
- Rutten, L.J.F.; Zhu, X.; Leppin, A.L.; Ridgeway, J.L.; Swift, M.D.; Griffin, J.M.; Sauver, J.L.S.; Virk, A.; Jacobson, R.M. Evidence-Based Strategies for Clinical Organizations to Address COVID-19 Vaccine Hesitancy. Mayo Clin. Proc. 2021, 96, 699–707. [Google Scholar] [CrossRef]
- Lerner, R.; Guermazi, D.; Farmakiotis, D. Vaccine Hesitancy Among Organ Transplant Recipients Survey - Preview. Available online: https://brown.co1.qualtrics.com/jfe/preview/previewId/3de88941-5624-4c93-86ce-cb271f6c03d8/SV_3HMs57IdLpULMdE?Q_CHL=preview&Q_SurveyVersionID=current.
- Oduwole, E.; Pienaar, E.D.; Mahomed, H.; Wiysonge, C.S. Current tools available for investigating vaccine hesitancy: A scoping review protocol. BMJ Open 2019, 9, e033245. [Google Scholar] [CrossRef]
- Vaccine Confidence Survey Question Bank. Available online: https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence/rca-guide/downloads/CDC_RCA_Guide_2021_Tools_AppendixD_Surveys-508.pdf.
- Dey, S.; Kusuma, Y.S.; Kant, S.; Kumar, D.; Gopalan, R.B.; Sridevi, P.; Aggarwal, S. COVID-19 vaccine acceptance and hesitancy in Indian context: A systematic review and meta-analysis. Ann. Trop. Med. Parasitol. 2023, 1–14. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Wyka, K.; White, T.M.; Picchio, C.A.; Rabin, K.; Ratzan, S.C.; Leigh, J.P.; Hu, J.; El-Mohandes, A. Revisiting COVID-19 vaccine hesitancy around the world using data from 23 countries in 2021. Nat. Commun. 2022, 13, 1–14. [Google Scholar] [CrossRef]
- Pan, Y.; Gong, S.; Zhu, X.; Xue, C.; Jing, Y.; Sun, Y.; Qian, Y.; Zhang, J.; Xia, Q. Investigation on the hesitancy of COVID-19 vaccination among liver transplant recipients: A cross-sectional study in China. Front. Public Heal. 2022, 10, 1014942. [Google Scholar] [CrossRef]
- Tharmaraj, D.; Dendle, C.; Polkinghorne, K.R.; Mulley, W.R. Kidney transplant recipients’ attitudes toward COVID-19 vaccination and barriers and enablers to vaccine acceptance. Transpl. Infect. Dis. 2021, 24, e13749. [Google Scholar] [CrossRef]
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and vaccine hesitancy: A longitudinal study. PLoS ONE 2021, 16, e0250123. [Google Scholar] [CrossRef]
- Hoffman, J. President Trump on vaccines: From skeptic to cheerleader. The New York Times 2020, 9. [Google Scholar]
- Hornsey, M.J.; Finlayson, M.; Chatwood, G.; Begeny, C.T. Donald Trump and vaccination: The effect of political identity, conspiracist ideation and presidential tweets on vaccine hesitancy. J. Exp. Soc. Psychol. 2020, 88, 103947. [Google Scholar] [CrossRef]
- Edwards, A.L.; Tavakol, M.M.; Mello, A.; Kerney, J.; Roberts, J.P. Pretransplantation coronavirus disease 2019 vaccination requirements: A matched case-control study of factors associated with waitlist inactivation. Am. J. Transplant. 2024, 24, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Kranzler, E.C.; Luchman, J.N.; Margolis, K.A.; Ihongbe, T.O.; Kim, J.-E.C.; Denison, B.; Vuong, V.; Hoffman, B.; Dahlen, H.; Yu, K.; et al. Association between vaccination beliefs and COVID-19 vaccine uptake in a longitudinal panel survey of adults in the United States, 2021–2022. Vaccine: X 2024, 17, 100458. [Google Scholar] [CrossRef] [PubMed]
- Rogers, B.G.; Tao, J.; Almonte, A.; Toma, E.; Nagel, K.; Fain, R.; Napoleon, S.C.; Maynard, M.A.; Murphy, M.; Sarkar, I.N.; et al. Statewide evaluation of COVID-19 vaccine hesitancy in Rhode Island. PLoS ONE 2022, 17, e0268587. [Google Scholar] [CrossRef] [PubMed]
- Rabin, Y.; Kohler, R.E. COVID-19 Vaccination Messengers, Communication Channels, and Messages Trusted Among Black Communities in the USA: A Review. J. Racial Ethn. Heal. Disparities 2023, 1–14. [Google Scholar] [CrossRef]
- Tagini, S.; Brugnera, A.; Ferrucci, R.; Priori, A.; Compare, A.; Parolin, L.; Pravettoni, G.; Silani, V.; Poletti, B. Behind the Scenes of COVID-19 Vaccine Hesitancy: Psychological Predictors in an Italian Community Sample. Vaccines 2022, 10, 1158. [Google Scholar] [CrossRef]
Figure 1.
Correlation of VACS with sociodemographic features and medical history. Values are displayed on a logarithmic scale. Significant (p<0.05) associations are bolded. VACS = Vaccine Acceptance Composite Score; CI = confidence interval.
Figure 1.
Correlation of VACS with sociodemographic features and medical history. Values are displayed on a logarithmic scale. Significant (p<0.05) associations are bolded. VACS = Vaccine Acceptance Composite Score; CI = confidence interval.
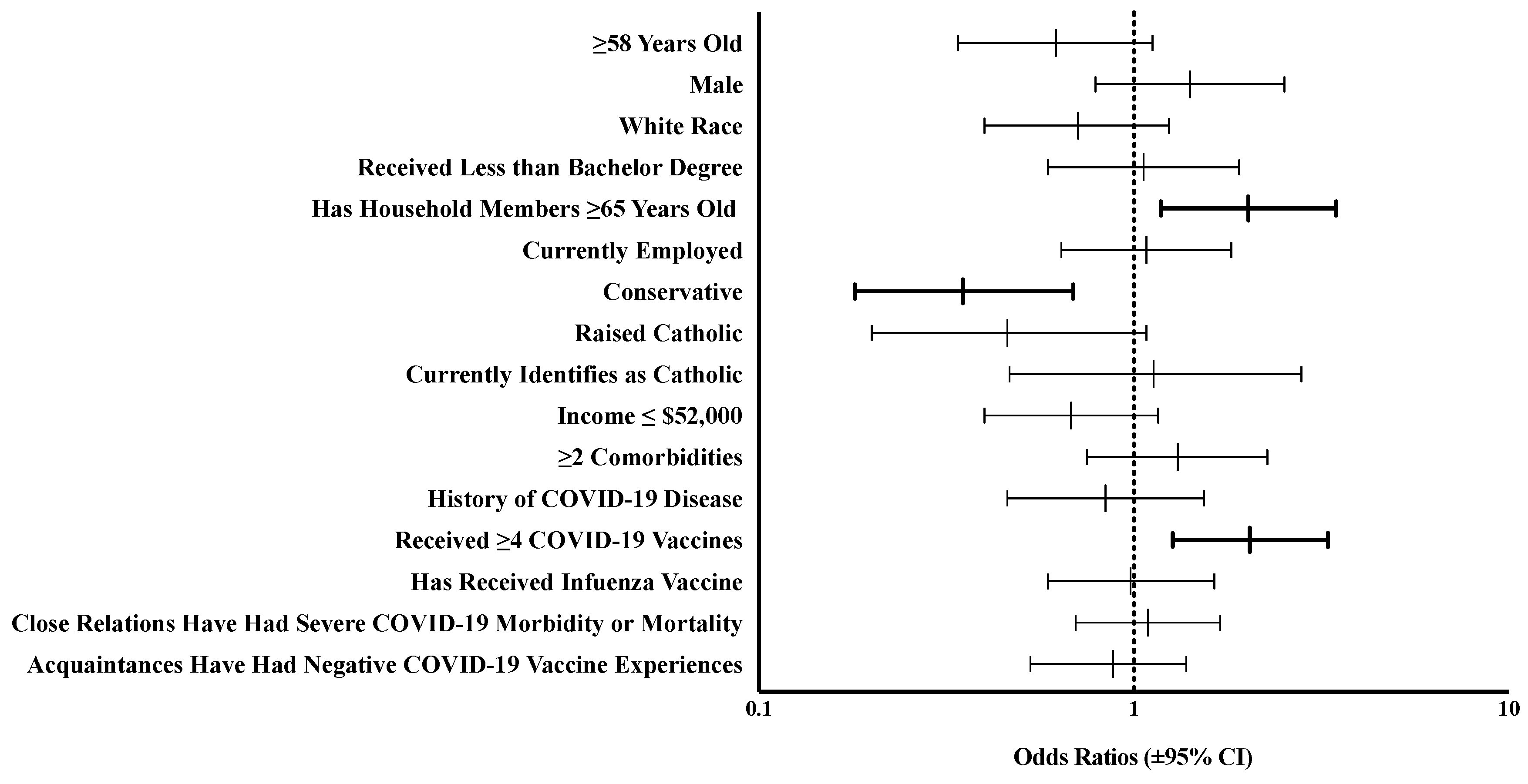
Figure 2.
ROC curves for VACS by number of vaccine doses received. AUC = area under the curve; CI = confidence intervals; ROC = relative operating characteristic; VACS = Vaccine Acceptance Composite Score.
Figure 2.
ROC curves for VACS by number of vaccine doses received. AUC = area under the curve; CI = confidence intervals; ROC = relative operating characteristic; VACS = Vaccine Acceptance Composite Score.
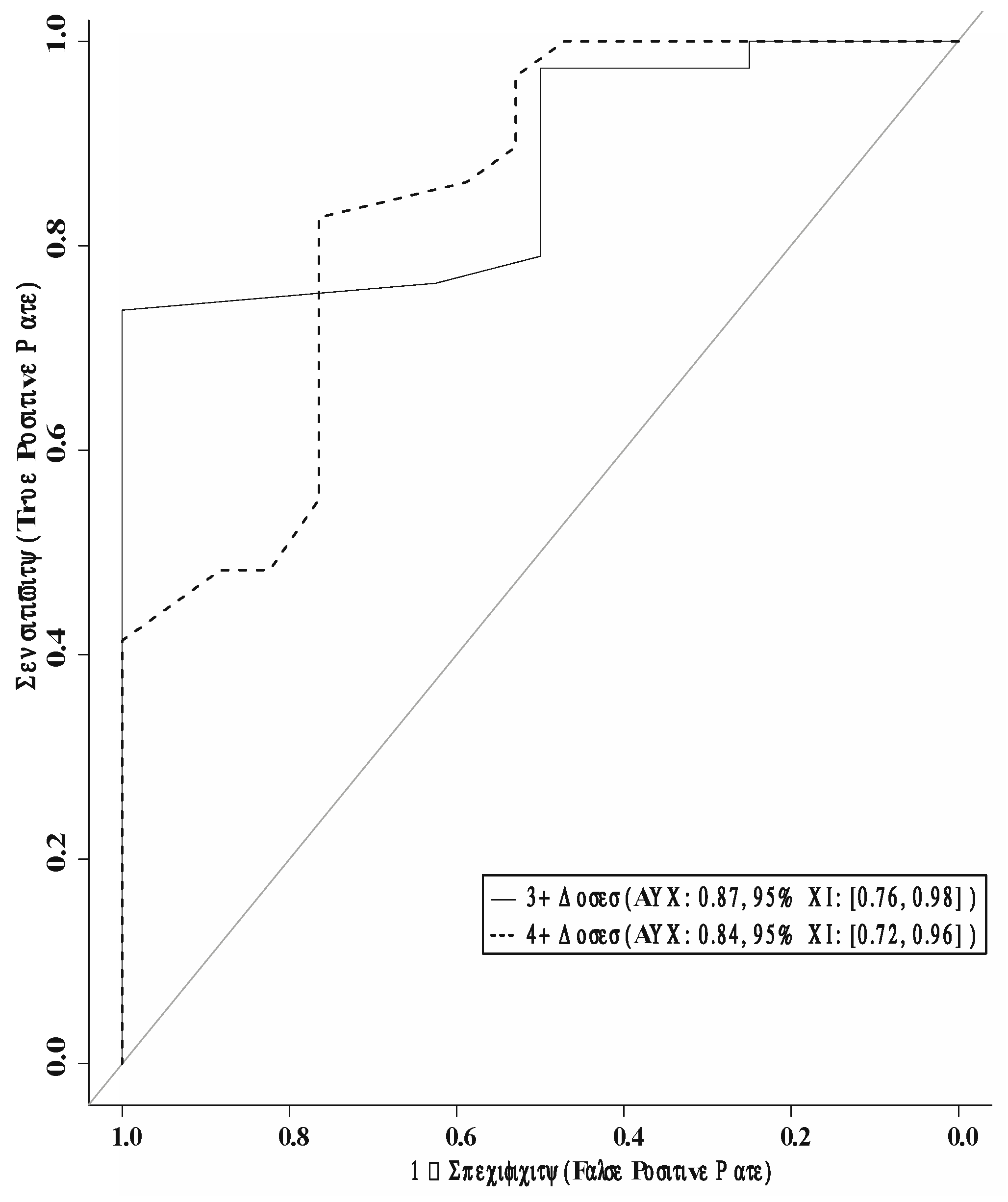

Table 1.
Sociodemographic factors and medical history.
| Category | Total responses (n) | Categorical responses † |
|---|---|---|
| Total number of respondents | 46 | - |
| Age (years) | 30 | 58 (48-64) |
| Male gender identity | 46 | 31 (67.4) |
| Transgender identity | 46 | 2 (4.3) |
| Heterosexual identity | 45 | 44 (97.8) |
| Ethnicity and race ‡ | 45 | - |
| White/European American | - | 31 (68.9) |
| Middle Eastern/North African | - | 2 (4.4) |
| Black or African American | - | 6 (13.3) |
| Asian | - | 3 (6.7) |
| Hispanic and/or Latino/a/x | - | 3 (6.7) |
| Access to racially congruent medical care for patients who identify as other than exclusively White | 14 | 4 (28.6) |
| English as a second language | 46 | 3 (6.5) |
| Has access to primary language-concordant medical care | 3 | 2 (66.7) |
| Born in the United States | 46 | 36 (78.3) |
| Highest level of education | 46 | - |
| Less than high school | - | 2 (4.3) |
| High school or equivalent | - | 8 (17.4) |
| Some college | - | 15 (32.6) |
| Bachelor’s degree or higher | - | 21 (45.7) |
| Primary caregiver to at least one child | 46 | 16 (34.8) |
| Household children received all recommended pediatrician-scheduled vaccines | 14 | 13 (92.9) |
| Has household members >65 years old | 45 | 11 (24.4) |
| Current employment status | 46 | - |
| Working § | - | 22 (47.8) |
| Not employed due to disability | - | 3 (6.5) |
| Not employed for other reasons | - | 4 (8.7) |
| Retired | - | 16 (34.8) |
| Other | - | 1 (2.2) |
| Political party | 44 | - |
| Democrat, liberal or left | - | 21 (47.7) |
| Republican, conservative or right | - | 6 (13.6) |
| Independent or no party affiliation | - | 17 (38.6) |
| Has maintained same political party affiliation | 42 | 28 (66.7) |
| Raised with religion | 44 | 32 (72.7) |
| Childhood religion ‡ | 32 | - |
| Catholicism | - | 23 (71.9) |
| Other Christian denominations | - | 6 (18.8) |
| Hinduism, Buddhism | - | 3 (9.4) |
| Other | - | 4 (12.5) |
| Currently spiritual or religious | 44 | 24 (54.5) |
| Current religion ‡ | 34 | - |
| Catholicism | - | 14 (41.2) |
| Other Christian denominations | - | 5 (14.7) |
| Hinduism, Buddhism | - | 4 (11.8) |
| Other | - | 3 (8.8) |
| Annual household income | 43 | - |
| $27,000 or less | - | 5 (11.6) |
| $27,001-$52,000 | - | 9 (20.9) |
| $52,001-$85,000 | - | 8 (18.6) |
| $85,001-$141,000 | - | 7 (16.3) |
| $141,001 or more | - | 14 (32.6) |
| Eligible for social programs | 22 | 8 (36.4) |
| Number of organ transplants received | 46 | - |
| One | - | 38 (82.6) |
| Two or three | - | 8 (17.4) |
| Transplanted organ types ‡ | 46 | - |
| Kidney | - | 43 (93.5) |
| Heart | - | 1 (2.2) |
| Pancreas | - | 1 (2.2) |
| Lung | - | 1 (2.2) |
| Liver | - | 1 (2.2) |
| Three or fewer years since last transplant | 44 | 23 (52.3) |
| Comorbidities ‡ | 46 | - |
| Hypertension | - | 34 (73.9) |
| Diabetes mellitus | - | 22 (47.8) |
| Chronic kidney disease | - | 38 (82.6) |
| Congestive heart failure | - | 6 (13.0) |
| Chronic pulmonary conditions | - | 3 (6.5) |
| Chronic hepatic conditions | - | 1 (2.2) |
| Malignancy | - | 9 (19.6) |
| Two or more comorbidities | - | 36 (78.3) |
| Limitations in activities of daily living due to a physical or psychological condition | 46 | 7 (15.2) |
| Deaf or hard of hearing | 46 | 3 (6.5) |
| Blind or visually impaired | 46 | 5 (10.9) |
| Positive history of COVID-19 disease ‡ | 46 | 29 (63.0) |
| Infection requiring hospitalization | 27 | 5 (18.5) |
| Multiple COVID-19 infections | 28 | 5 (17.9) |
| Last diagnosed with COVID-19 after vaccine release (December 14, 2020) | 28 | 25 (89.3) |
| Close relations with severe COVID-19 morbidity or mortality | 45 | 19 (42.2) |
| Number of vaccine doses received | 46 | - |
| 1-2 | - | 8 (17.4) |
| 3 | - | 9 (19.6) |
| 4+ | - | 29 (63.0) |
| Received at least 1 mRNA vaccine | 46 | 43 (93.5) |
| Received ≥1 bivalent COVID-19 booster | 43 | 35 (81.4) |
| Previously received the influenza vaccine | 46 | 24 (52.2) |
| Up to date on other (non-COVID-19, non-flu) vaccinations | 46 | 40 (87.0) |
| Knows a family member, friend or colleague who had a poor experience with the COVID-19 vaccine | 44 | 15 (34.1) |
| Has had personal past negative experiences with health care workers | 45 | 10 (22.2) |
Only one respondent (out of 45 who answered) cited cost as a barrier to obtaining transplant-related medication. † All values are listed as (n, %) with the exception of age (median, interquartile range). ‡ As categories are nonexclusive, sums may exceed total number of patients. One patient received both a kidney and pancreas transplant. § Includes homemaking.
Table 2.
Values related to, and perceptions of, the COVID-19 vaccine.
| Category | Total responses (n) | Categorical responses (n, %) |
|---|---|---|
| Concerned about COVID-19-associated risks | 44 | 26 (59.1) |
| Concerned about COVID-19 vaccine-associated risks | 41 | 19 (46.3) |
| Concerned about safety of COVID-19 vaccine for the general public | 44 | 14 (31.8) |
| Concerned about safety of COVID-19 vaccine for transplant patients | 46 | 16 (34.8) |
| Predicts significant magnitude of effect of COVID-19 vaccine on allograft | 42 | 20 (47.6) |
| Expects lower likelihood of peer/colleague vaccination | 45 | 23 (51.1) |
| Expects lower likelihood of friends/family vaccination | 46 | 17 (37.0) |
| Has difficulty determining veracity of COVID-19 information in the news/on social media | 46 | 22 (47.8) |
| Amount of information received on COVID-19 vaccines is... | 46 | - |
| Too much | - | 6 (13.0) |
| The right amount | - | 29 (63.0) |
| Not enough | - | 11 (23.9) |
| Uses ___ as a primary source for COVID-19 information † | 45 | - |
| Doctors and/or official government materials | - | 17 (37.8) |
| Right-wing media | - | 6 (13.3) |
| Left-wing media | - | 26 (57.8) |
| Social media | - | 8 (17.8) |
| Unconfident in health care worker competence | 46 | 10 (21.7) |
| Unconfident that motives of vaccine-supportive policymakers are well-intentioned | 45 | 25 (55.6) |
| Unconfident that COVID-19 vaccines have been adequately studied | 44 | 26 (59.1) |
| Unconfident that vaccines are useful at preventing infectious disease | 46 | 15 (32.6) |
| Unconfident that receiving a COVID -19 vaccine is better than becoming ill from COVID-19 | 46 | 10 (21.7) |
| Of patients who were first vaccinated after contracting COVID-19 – unconfident that vaccination would have helped avoid COVID-19 symptoms | 5 | 4 (80.0) |
| Unconfident that SARS-CoV-2 is real | 45 | 12 (26.7) |
| Unconfident in own understanding and judgment of the COVID-19 vaccine | 46 | 15 (32.6) |
| Unconfident in colleagues' or friends' understanding and judgment of the COVID-19 vaccine | 45 | 30 (66.7) |
| Unconfident in family's understanding and judgment of the COVID-19 vaccine | 46 | 20 (43.5) |
| Lower sense of responsibility for health and safety of non-relatives | 44 | 21 (47.7) |
| Lower sense of responsibility for health and safety of relatives | 44 | 12 (27.3) |
| Received advice from a medical provider to not be vaccinated against COVID-19 | 44 | 3 (6.8) |
The spectrum of vaccine hesitancy was incorporated as Likert scores between either 1-3 or 3-5, depending on the orientation of the question posed. † Four individuals utilized both right and left-wing news sources. Political leanings of media sources were informed by the Media Bias Ratings on AllSides (https://www.allsides.com/media-bias).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



