
Submitted:
15 April 2024
Posted:
16 April 2024
You are already at the latest version
Abstract
In Brazil, Brazilian borreliosis (BB), characterized molecularly, exhibits symptoms akin to Lyme disease (LD) but presents unique epidemiological, clinical, and morphological features. This study explores the incidence, diagnostic challenges, and awareness initiatives regarding this disease in Brazil. Employing a narrative review methodology, data were sourced from Pubmed, Ebsco, Google Scholar, and Web of Science without temporal constraints. Results reveal diagnostic complexities in Brazil due to the low sensitivity of conventional tests and the use of North American B. burgdorferi antigens. Despite challenges, epidemiological studies indicate an upswing in cases in humans and animals. Therefore, there is an urgent need to define new biomarkers, molecular strategies, or new antigenic targets to advance the development of vaccines and diagnostics. Early and accurate pathogen identification is crucial for active surveillance to comprehend and manage this zoonosis.
Keywords:
Lyme disease
; neuroborreliosis
; diagnose
; immunological diagnosis
1. Introduction
Lyme disease (LD) stems from spirochetes within the Borrelia burgdorferi species complex, a Gram-negative bacterium [1], prevalent in temperate regions like the USA, Europe, Asia, and the Middle East [2,3]. In Brazil, molecular identification of the same bacterium exists, but isolation or cultivation remains elusive [4]. Thus, the disease is termed Lyme-like or Brazilian borreliosis (BB), Brazilian Lyme-like disease (DLSB), or Baggio-Yoshinari Syndrome (BYS) in Brazil, with cases documented across various regions [5,6,7]. Although BB mirrors LD symptoms, notable epidemiological, clinical, and morphological differences exist [5,8].
Transmission occurs through the bite of an Ixodes tick during a blood meal, causing a multisystemic disease associated with initial phase symptoms typically including skin lesions such as erythema migrans (EM). As the disease progresses, extracutaneous manifestations may affect joints, heart, and nervous system in later stages [9,10,11]. Typically successful antibiotic treatment in the initial phase is typical. However, despite appropriate antibiotic therapy and an absence of clear evidence of ongoing infection, some patients present persistent symptoms. These symptoms, which include joint/muscle pain, depression, fatigue, and cognitive difficulties, are termed posttreatment Lyme disease syndrome (PTDS) or posttreatment Lyme disease syndrome-Lyme (PLSD) [12,13,14]. Diagnosis of this condition relies on clinical symptoms and serological tests. Nevertheless, these tests have low sensitivity and specificity in Brazil when using B. burgdorferi sensu stricto antigens of European or American origin. [8].
In this review, we update information on the challenges of diagnosing LD and Brazilian borreliosis. Identifying specific target proteins as markers for disease identification and monitoring is crucial, given the lack of biomarkers hindering a deeper understanding of the condition.
2. Material and Methods
This literature review aims to provide a comprehensive overview of Lyme disease within the Brazilian context. Various search strategies were employed, encompassing Pubmed, Ebsco, Google Scholar, and Web of Science databases. Key terms such as "LD in Brazil," "Lyme pathogenesis," "Baggio-Yoshinari syndrome (BYS)," "Persistence of Lyme disease," "Borreliosis and diagnosis," "spirochete," and "tickborne disease" were utilized. The search was not constrained by a specific timeframe, ensuring coverage of studies over an extended period. Additionally, animal and in vitro studies were included in the examination. Titles and abstracts were meticulously evaluated during screening to identify pertinent works.
3. Results
3.1. History of Lyme Disease and Brazilian Borreliosis
In the historical context of LD, Alfred Buchwald's 1883 clinical descriptions marked the inception, detailing dermatological manifestations now recognized as chronic atrophic acrodermatitis (ACA) [15]. Benjamin Lipschutz and Arvid Afzelius, early in the 20th century, associated Erythema migrans with tick bites, with Afzelius providing specifics in 1910 [15]. However, it was only in 1976 that LD was officially identified in Lyme, Connecticut, USA, by Dr. Allen C. Steere [16]. The significant milestone of isolating the etiological agent Borrelia burgdorferi occurred in 1982, credited to Willy Burgdorfer [17].
While LD is a prevalent zoonosis in the USA, borreliosis has been documented in South American countries, including Argentina, Bolivia, Colombia, Venezuela, Chile, and Brazil [18]. In the 1980s, the first cutaneous manifestations were diagnosed in Manaus, followed by cases in the 90s with tick bites and seropositivity in Rio de Janeiro and São Paulo states [19,20]. Secondary manifestations like Lyme meningitis were reported in Mato Grosso do Sul staite 1996 [21]. Subsequent studies highlighted recurrent symptoms posttreatment, deviating from patterns observed in American and European Lyme Borreliosis (LBP) [22].
3.2. Morphological Features of Borrelia
Belonging to the order Spirochaetales, Borrelias consists of 42 species categorized into two main groups: the relapsing fever group (GFR) and the Borrelia burgdorferi sensu lato (Bbsl) group [23]. Of the Bbsl group, 20 species are associated with Lyme Borreliosis (BL) [23]. Spirochetes exhibit an elongated, corkscrew-like structure with axial filaments and reproduce through transverse binary fission [24,25]. Notably, Borrelia lacks lipopolysaccharides (LPS) in its outer membrane but possesses a lipid bilayer composed of phospholipids, glycolipids, and lipoproteins [16,26] (Figure 1). The Bbsl complex has a conserved linear chromosome but displays high variability in its 21 plasmids, potentially influencing clinical manifestations and distribution [27].
The spirochete adapted to the Brazilian environment exhibits an "L" shape, suggesting a cell wall deficiency that may enable intracellular localization. PCR tests for flaA, flab, and Osp A genes yielded negative results, but Western Blot analysis consistently identified the 41 kD band. The flgE gene, responsible for the flagellar hook protein, was later confirmed, hinting at an evolutionary process that reduced immunogenicity and antibody production, potentially contributing to survival and dissemination in the Brazilian environment [4,8,22,28].
3.3. Pathogenesis
Although B. burgdorferi does not produce LPS, OspA and OspB proteins play pivotal roles in tick intestine survival [29]. The transition from tick intestine to salivary glands involves a shift in protein expression, with decreased OspA and increased OspC facilitating host infection [30]. Borrelia infection initiates when the organism enters the host, spreads to various tissues, and causes diverse manifestations, including neuroborreliosis [27].
Borrelia relies on its outer membrane lipoproteins and adhesins to establish virulence and adhere to host tissues. These proteins activate immune responses and interact with target tissues. Despite immune system activation, Borrelia often persists, maintaining infection [29]. Macrophages internalize Borrelia through opsonization, a process recognized by receptors such as FcγR and CR3. Notably, the absence of FcγRIIb function may broaden B cell activation and lead to autoimmune responses [31,32]. Neutrophils and macrophages, activated by Toll-like receptors (TLRs) and NOD-like receptors (NLRs), recognize Borrelia peptidoglycan, inducing pro-inflammatory responses [33]. As observed in BB patients, pro-inflammatory cytokines like IL-6, IL-12, TNF-α, and pro-IL1β are activated [34,35]. During infection, elevated levels of IL-8, MIP-1/CCL3, MIP3B/CCL19, and IL-17A were identified, particularly during the acute phase of the disease [36]. These findings indicate a comprehensive immune response, including the Th2 response, which stimulates interleucin-4 (IL-4) production. Interestingly, Borrelia's "L" form potentially evades Th2 response [37].
3.4. Current Situation of Lyme Disease in Brazil
3.4.1. Tick Biological Cycle and Its Relationship with the Spread of the Disease
Tickborne diseases, such as those caused by the bacteria B. burgdorferi, have emerged as a significant epidemiological problem in various regions worldwide, particularly in countries with tropical and subtropical climates where ticks are more prevalent [38]. Ticks from the Argasidae and Ixodidae families (Figure 2) are crucial in transmitting Borrelia spp. Ixodes spp. is a major transmitter in Europe, Asia, and North America [14,39].
Brazil's diverse ecosystem and climatic conditions create a conducive environment for ticks. The predominant tick species, acting as disease vectors, belong to the Ixodidae and Argasidae families [38] (Figure 2). Molecular and serological studies in Brazil have identified both Ixodes and Amblyomma ticks participating in the transmission, with ticks becoming infected through feeding on vertebrate reservoirs carrying bacteria [40,41,42]. Transmission routes include transovarial, where inefficiency in maintaining B. burgdorferi has been reported, and the transstadial route, where spirochetes migrate to the tick’s salivary glands during feeding and subsequently inoculating the vertebrate host's skin [43,44]. While deer and rodents are the primary reservoirs, domestic animals like dogs and horses can also play a crucial role [4,45]. Humans become accidental hosts when bitten by infected ticks, especially the challenging-to-detect nymphs [45].
3.4.2. Clinical Picture of DLSB/Lyme
Lyme disease exhibits a range of clinical manifestations, posing challenges for accurate diagnosis. Symptoms like fever, fatigue, headache, muscle and joint pain, and the characteristic skin rash erythema migrans (EM) can resemble other medical conditions. Notably, not all patients exhibit the skin rash, complicating early diagnosis. Studies suggest asymptomatic cases in Europe and a subset in the USA [1,46].
LD progresses through three stages: Acute infection, disseminated disease with neurological or cardiac involvement, and Chronic infection marked by arthritis (Table 1). The absence of specific symptoms in all patients complicates diagnosis. Apart from initial symptoms, Lyme disease can lead to systemic manifestations like eye problems, joint pain, and neurological and cardiac symptoms weeks or months post-infection, potentially resulting in late diagnoses and complications [47]. Neurological diseases associated with Lyme carditis, while rare, can lead to serious complications such as atrioventricular heart block and sudden death if untreated [46,48,49].
Furthermore, studies have identified morphological, epidemiological, and laboratory differences between Brazilian Borreliosis (BB) and North American Lyme disease, influencing clinical manifestations in Brazil [22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45]. Prolonged clinical evolution and recurrent symptoms after treatment are observed, with peculiarities including chronic fatigue syndrome and autoimmune/allergic diseases [50,51,52,53,54,55,56]. Clinical manifestations of BB are categorized into initial and late stages, reflecting the flu-like symptoms and more severe symptoms, respectively [4,8,36,53,56].
3.4.3. Epidemiological Trends of Brazilian Borreliosis Disease
Lyme disease was first reported in the United States in 1991 [57], and from 1996 to 2023, the CDC reported 761.143 cases, with notable peaks in 2009, 2017, and 2022 (Figure 3). However, the case definition for Lyme disease has changed over the years, and these changes may influence surveillance data.
Figure 3 shows the number of cases considering the changes in force in 1996, 2008, and 2022. Despite DLSB being considered rare in Brazil, seropositivity rates in animals, particularly dogs and horses, suggest a potential risk of transmission [58,59,60,61,62,63,64]. Cases of DLSB in Brazil were identified three decades ago [65], with some states instituting notifications. Notably, there was a surge in reported cases in specific regions, emphasizing the need for active surveillance and accurate diagnoses [66,67,68,69].
In Santa Catarina, 20.4% of reported cases and an incidence of 0.7 cases/100 thousand inhabitants were laboratory-confirmed as Lyme Disease, a notable proportion considered autochthonous [70] (Figure 4). These findings underscore the urgency for enhanced surveillance and precise diagnostics to comprehensively understand the disease's spread and incidence.
3.5. Challenges in Brazilian Lyme-like Disease Diagnosis
In Brazil, diagnosing and recognizing Lyme disease remains challenging due to the diversity of tick species and bacterial strains and variations in clinical and epidemiological aspects compared to North America [52]and Europe [15]. Difficulty in serological diagnosis, cross-reactions, and limitations of available tests add to the complexity [53,54].
Availability of Tests and Their Limitations in the Brazilian Context
Effective treatment and prevention of long-term complications in Brazilian Lyme-like disease hinge on accurate diagnosis [9,71,72]. Over the past decade, diagnostic accuracy has become challenging due to diverse clinical presentations and test limitations. Serological tests like ELISA and Western blot are commonly used [52], but false-positive and false-negative results compromise reliability [4,22,73]. While sensitive, PCR and other molecular techniques face challenges in diagnosing persistent arthritis [74]. Various diagnostic methods, including histopathology and imaging, have been explored, each with limitations [75,76,77,78].
In Brazil, the adoption of ELISA and WB tests has been hindered by diagnostic inaccuracies related to antigen variety and test criteria [4,22,56]. Newer methods like the Modified Two-Stage (MTTT) method promise to improve diagnostic accuracy, but challenges persist [79,80,81,82]. The intricacies of Brazilian B. burgdorferi, such as pleomorphic morphology, temperature sensitivity, and slow growth cycle, pose obstacles to effective diagnosis [4,36].
The challenges in diagnosing BB include the similarity of initial symptoms to other diseases, limitations in serology, the impossibility of pathogen culture and isolation, and the necessity of excluding other conditions presenting similar symptoms[83,84,85]. Comprehensive and specific diagnostic approaches are crucial for BB, highlighting the need for ongoing research to enhance understanding and management.
3.6. Characteristics of the Antibody Response to B. burgdorferi
The dermal inflammatory process, triggered by tick bites, leads to Erythema migrans [86]. Antibody production follows, starting with IgM, and is detectable from the third to fourth-week post-infection. IgM levels peak between the sixth and eighth week, indicating a recent infection [87,88,89,90]. However, the persistence of IgM responses for years [88,91] and IgG poses challenges in distinguishing between active and inactive infections [82]. Moreover, IgM antibodies may have the potential to cross-react with antigens that are unrelated to Borrelia [92,93]. During the acute phase, IgA is produced, particularly in the cerebrospinal fluid [94,95,96]. In addition to these antibodies, the generation and persistence of IgE antibodies have been observed in children [97]. This observation suggests using both IgA and IgE as diagnostic markers. Further research is needed to understand the role of IgA and IgE in B. burgdorferi infection and its implications for diagnosis and treatment.
3.7. Recent Advances in DL
Despite the availability of diagnostic tests, challenges persist, and new technologies are emerging. Digital PCR (dPCR) is gaining popularity due to its accuracy and sensitivity, especially in cerebrospinal fluid samples[98,99]. Challenges related to Posttreatment Lyme Disease Syndrome (PTLDS) prompt exploration of biomarkers [100] and antigens using artificial intelligence (AI) and machine learning [101,102]. Among these, elevated levels of CCL-19 [103] and apolipoprotein B [104] have been observed in PTLDS patients, which could serve as biomarkers. Petzke et al. identified 20 genes capable of discriminating with high accuracy (97%) between individuals with acute disseminated Lyme disease and healthy controls and between those in the acute phase and recovery [105]. Additionally, regarding metabolomic biomarkers, sialic acid in N-glycans plays a significant role in many biological activities and in diagnosing Lyme disease [106]. These technologies will contribute to identifying new biomarkers, differentiating between Lyme disease and other infections, and enhancing understanding for better diagnosis and treatment for tickborne disease and other infectious diseases [106].
4. Conclusions
The genetic and morphological variability of this bacterium and the disease's unique clinical manifestations pose challenges to the precision of conventional diagnostic methods. Epidemiological studies highlighting a surge in cases across various country regions underscore the urgency of enhanced surveillance and precise diagnostic procedures. Consequently, the constrained availability of sensitive and specific tests and the absence of standardization present a formidable challenge in identifying and monitoring this disease within the Brazilian context.
In this context, novel approaches, including exploring specific and critical epitope biomarkers and developing more refined diagnostic methods tailored to the nuances of Brazilian Borreliosis, become indispensable for achieving early and accurate diagnoses. Such advancements could enhance the quality of life for individuals impacted by this condition. Recognizing the intricacies of diagnostics and the continual need for methodological refinement is pivotal in advancing the comprehension and management of this disease in Brazil.
Author Contributions
The authors contributed equally.
Funding
This research was funded by Carlos Chagas Filho Foundation of Research Support of the State of Rio de Janeiro (FAPERJ #010.101.029/2018).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Radolf, J.D.; Strle, K.; Lemieux, J.E.; Strle, F. Lyme disease in humans. Curr Issues Mol Biol 2021, 42, 333–384. [Google Scholar] [CrossRef]
- Lantos, P.M.; Rumbaugh, J.; Bockenstedt, L.K.; Falck-Ytter, Y.T.; Aguero-Rosenfeld, M.E.; Auwaerter, P.G.; Baldwin, K.; Bannuru, R.R.; Belani, K.K.; Bowie, W.R.; et al. Clinical practice guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the prevention, diagnosis, and treatment of Lyme disease. Clin Infect Dis 2021, 72, 1–8. [Google Scholar] [CrossRef]
- Obaidat, M.M.; Alshehabat, M.A.; Hayajneh, W.A.; Roess, A.A. Seroprevalence, spatial distribution and risk factors of Borrelia burgdorferi sensu lato in Jordan. Comp Immunol Microbiol Infect Dis 2020, 73, 101559. [Google Scholar] [CrossRef]
- Yoshinari, N.H.; Bonoldi, V.L.N.; Bonin, S.; Falkingham, E.; Trevisan, G. The Current state of knowledge on Baggio-Yoshinori syndrome (Brazilian Lyme Disease-like Illness): Chronological presentation of historical and scientific events observed over the last 30 years. Pathogens 2022, 11, 889. [Google Scholar] [CrossRef] [PubMed]
- Lopes, F.A.; Rezende, J.; Silva, D.; Alves, F.C.G.; Oliveira, C.E.; Costa, I.P.D. Molecular evidence of Borrelia burgdorferi sensu lato in patients in the Brazilian central-western region. Rev Bras Reumatol Engl Ed 2017, 57, 641–645. [Google Scholar] [CrossRef]
- Vien, V.P.; Bassi, R.; Maxim, T.; Bogoch, I.I. Lyme disease vs. Baggio-Yoshinari syndrome in a returned traveler from Brazil. J Travel Med 2017, 24. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, S.V.d.; Oliveira, K.H.C.d.; Santos, J.P.D.; Gazeta, G.S. Geographical distribution of Lyme-like borreliosis in Brazil: Hot spots for research and surveillance. J Parasitic Dis: DiagTher 2017, 2. [Google Scholar]
- da Silva, V.S.; Santana, M.M.d.; Gomes, D.d.L.X.; Medeiros, É.P.d.; Cordeiro, M.F.; Takenami, I. Baggio-Yoshinari syndrome: A literature review. Rev Med 2020, 99, 503–511. [Google Scholar]
- Wormser, G.P.; McKenna, D.; Karmen, C.L.; Shaffer, K.D.; Silverman, J.H.; Nowakowski, J.; Scavarda, C.; Shapiro, E.D.; Visintainer, P. Prospective evaluation of the frequency and severity of symptoms in Lyme disease patients with Erythema migrans compared with matched controls at baseline, six months, and 12 months. Clin Infect Dis 2020, 71, 3118–3124. [Google Scholar] [CrossRef]
- Geebelen, L.; Lernout, T.; Devleesschauwer, B.; Kabamba-Mukadi, B.; Saegeman, V.; Belkhir, L.; De Munter, P.; Dubois, B.; Westhovens, R.; Van Oyen, H.; et al. Non-specific symptoms and posttreatment Lyme disease syndrome in patients with Lyme borreliosis: A prospective cohort study in Belgium (2016-2020). BMC Infect Dis 2022, 22, 756. [Google Scholar] [CrossRef]
- Donta, S.T. What We Know and Don't Know About Lyme Disease. Front Public Health 2021, 9, 819541. [Google Scholar] [CrossRef] [PubMed]
- Marques, A. Persistent Symptoms After Treatment of Lyme Disease. Infect Dis Clin North Am 2022, 36, 621–638. [Google Scholar] [CrossRef]
- Chung, M.K.; Caboni, M.; Strandwitz, P.; D'Onofrio, A.; Lewis, K.; Patel, C.J. Systematic comparisons between Lyme disease and posttreatment Lyme disease syndrome in the U.S. with administrative claims data. EBioMedicine 2023, 90, 104524. [Google Scholar] [CrossRef]
- Bush, L.M.; Vazquez-Pertejo, M.T. Tickborne illness-Lyme disease. Dis Mon 2018, 64, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Stanek, G.; Strle, F. Lyme disease: European perspective. Infect Dis Clin North Am 2008, 22, 327–339. [Google Scholar] [CrossRef] [PubMed]
- Steere, A.C.; Strle, F.; Wormser, G.P.; Hu, L.T.; Branda, J.A.; Hovius, J.W.; Li, X.; Mead, P.S. Lyme borreliosis. Nat Rev Dis Primers 2016, 2, 16090. [Google Scholar] [CrossRef]
- Snyder, A. Willy Burgdorfer. Lancet 2015, 385, 110. [Google Scholar] [CrossRef]
- Robles, A.; Fong, J.; Cervantes, J. Borrelia Infection in Latin America. Rev Invest Clin 2018, 70, 158–163. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.; Ribeiro-Rodrigues, R.; Talhari, C.; Ferreira, L.C.L.; Zelger, B.; Talhari, S. Presence of Borrelia burgdorferi "Sensu Lato" in patients with morphea from the Amazonic region in Brazil. Int J Dermatol 2011, 50, 1373–1378. [Google Scholar] [CrossRef]
- Fonseca, A.H.d.; Salles, R.d.S.; Salles, S.d.A.N.; Madureira, R.C.; Yoshinari, N.H. Borreliose de Lyme simile: Uma doença emergente e relevante para a dermatologia no Brasil. Anais Brasileiros de Dermatologia 2005, 80, 171–178. [Google Scholar] [CrossRef]
- Costa, I.P.; Yoshinari, N.H.; Barros, P.J.; Bonoldi, V.L.; Leon, E.P.; Zeitune, A.D.; Cossermelli, W. [Lyme disease in Mato Grosso do Sul State, Brazil: Report of three clinical cases, including the first of Lyme meningitis in Brazil]. Rev Hosp Clin Fac Med Sao Paulo 1996, 51, 253–257. [Google Scholar] [PubMed]
- Mantovani, E.; Costa, I.P.; Gauditano, G.; Bonoldi, V.L.; Higuchi, M.L.; Yoshinari, N.H. Description of Lyme disease-like syndrome in Brazil. Is it a new tickborne disease or Lyme disease variation? Braz J Med Biol Res 2007, 40, 443–456. [Google Scholar] [CrossRef] [PubMed]
- Margos, G.; Fingerle, V.; Cutler, S.; Gofton, A.; Stevenson, B.; Estrada-Peña, A. Controversies in bacterial taxonomy: The example of the genus Borrelia. Ticks Tick Borne Dis 2020, 11, 101335. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, S. Spirochete Flagella and Motility. Biomolecules 2020, 10, 550. [Google Scholar] [CrossRef]
- Charon, N.W.; Cockburn, A.; Li, C.; Liu, J.; Miller, K.A.; Miller, M.R.; Motaleb, M.A.; Wolgemuth, C.W. The unique paradigm of spirochete motility and chemotaxis. Annu Rev Microbiol 2012, 66, 349–370. [Google Scholar] [CrossRef] [PubMed]
- Schröder, N.W.; Eckert, J.; Stübs, G.; Schumann, R.R. Immune responses induced by spirochetal outer membrane lipoproteins and glycolipids. Immunobiology 2008, 213, 329–340. [Google Scholar] [CrossRef] [PubMed]
- Strnad, M.; Rudenko, N.; Rego, R.O.M. Pathogenicity and virulence of Borrelia burgdorferi. Virulence 2023, 14, 2265015. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, E.; Marangoni, R.G.; Gauditano, G.; Bonoldi, V.L.; Yoshinari, N.H. Amplification of the flgE gene provides evidence for the existence of a Brazilian borreliosis. Rev Inst Med Trop Sao Paulo 2012, 54, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.F.; Pal, U.; Alani, S.M.; Fikrig, E.; Norgard, M.V. Essential role for OspA/B in the life cycle of the Lyme disease spirochete. J Exp Med 2004, 199, 641–648. [Google Scholar] [CrossRef]
- Pal, U.; Yang, X.; Chen, M.; Bockenstedt, L.K.; Anderson, J.F.; Flavell, R.A.; Norgard, M.V.; Fikrig, E. OspC facilitates Borrelia burgdorferi invasion of Ixodes scapularis salivary glands. J Clin Invest 2004, 113, 220–230. [Google Scholar] [CrossRef]
- Belperron, A.A.; Liu, N.; Booth, C.J.; Bockenstedt, L.K. Dual role for Fcγ receptors in host defense and disease in Borrelia burgdorferi-infected mice. Front Cell Infect Microbiol 2014, 4, 75. [Google Scholar] [CrossRef]
- Danzer, H.; Glaesner, J.; Baerenwaldt, A.; Reitinger, C.; Lux, A.; Heger, L.; Dudziak, D.; Harrer, T.; Gessner, A.; Nimmerjahn, F. Human Fcγ-receptor IIb modulates pathogen-specific versus self-reactive antibody responses in Lyme arthritis. Elife 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Jutras, B.L.; Lochhead, R.B.; Kloos, Z.A.; Biboy, J.; Strle, K.; Booth, C.J.; Govers, S.K.; Gray, J.; Schumann, P.; Vollmer, W.; et al. Borrelia burgdorferi peptidoglycan is a persistent antigen in patients with Lyme arthritis. Proc Natl Acad Sci USA 2019, 116, 13498–13507. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C.; Brissette, C.A. The brilliance of Borrelia: Mechanisms of host immune evasion by Lyme disease-causing spirochetes. Pathogens 2021, 10, 281. [Google Scholar] [CrossRef] [PubMed]
- Petnicki-Ocwieja, T.; Kern, A. Mechanisms of Borrelia burgdorferi internalization and intracellular innate immune signaling. Front Cell Infect Microbiol 2014, 4, 175. [Google Scholar] [CrossRef] [PubMed]
- Bonoldi, V.L.N.; Yoshinari, N.H.; Aniz, P.A.E.A.; Pereira, R.M.R. Innate and Th1/Th17 adaptive immunity in acute and convalescent Brazilian borreliosis disease. Braz J Infect Dis 2021, 25, 101575. [Google Scholar] [CrossRef]
- McManus, M.; Cincotta, A. Effects of Borrelia on host immune system: Possible consequences for diagnostics. Adv Integ Med 2015, 2, 81–89. [Google Scholar] [CrossRef]
- Nogueira, B.C.F.; Campos, A.K.; Muñoz-Leal, S.; Pinter, A.; Martins, T.F. Soft and hard ticks (Parasitiformes: Ixodida) on humans: A review of Brazilian biomes and the impact of environmental change. Acta Trop 2022, 234, 106598. [Google Scholar] [CrossRef] [PubMed]
- Beard, C.B.; Eisen, L.; Eisen, R.J. The Rise of Ticks and Tickborne Diseases in the United States-introduction. J Med Entomol 2021, 58, 1487–1489. [Google Scholar] [CrossRef]
- Abel, I.S.; Marzagão, G.; Yoshinari, N.H.; Schumaker, T.T. Borrelia-like spirochetes recovered from ticks and small mammals collected in the Atlantic Forest Reserve, Cotia county, State of São Paulo, Brazil. Mem Inst Oswaldo Cruz 2000, 95, 621–624. [Google Scholar] [CrossRef]
- Dall'Agnol, B.; Michel, T.; Weck, B.; Souza, U.A.; Webster, A.; Leal, B.F.; Klafke, G.M.; Martins, J.R.; Ott, R.; Venzal, J.M.; et al. Borrelia burgdorferi sensu lato in Ixodes longiscutatus ticks from Brazilian Pampa. Ticks Tick Borne Dis 2017, 8, 928–932. [Google Scholar] [CrossRef]
- Montandon, C.E.; Yoshinari, N.H.; Milagres, B.S.; Mazioli, R.; Gomes, G.G.; Moreira, H.N.; Padilha Ade, F.; Wanderley, G.G.; Mantovani, E.; Galvão, M.A.; et al. Evidence of Borrelia in wild and domestic mammals from Minas Gerais, Brazil. Rev Bras Parasitol Vet 2014, 23, 287–290. [Google Scholar] [CrossRef]
- Rocha, S.C.; Velásquez, C.V.; Aquib, A.; Al-Nazal, A.; Parveen, N. Transmission Cycle of Tickborne infections and co-infections, animal models and diseases. Pathogens 2022, 11, 1309. [Google Scholar] [CrossRef]
- Steinbrink, A.; Brugger, K.; Margos, G.; Kraiczy, P.; Klimpel, S. The evolving story of Borrelia burgdorferi sensu lato transmission in Europe. Parasitol Res 2022, 121, 781–803. [Google Scholar] [CrossRef]
- Basile, R.C.; Yoshinari, N.H.; Mantovani, E.; Bonoldi, V.N.; Macoris, D.D.; Queiroz-Neto, A. Brazilian borreliosis with special emphasis on humans and horses. Braz J Microbiol 2017, 48, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.R.; Strle, F.; Wormser, G.P. Comparison of Lyme Disease in the United States and Europe. Emerg Infect Dis 2021, 27, 2017–2024. [Google Scholar] [CrossRef]
- Daher, N.; Bachiega, T.M.; Vetorasso, G.H.; Duarte, T.F.; Capalbo, R.V. Manifestações neuroftalmológicas associadas a doença de Lyme. Revista Brasileira de Oftalmologia 2019, 78, 133–136. [Google Scholar]
- Sanchez, J.L. Clinical Manifestations and Treatment of Lyme Disease. Clin Lab Med 2015, 35, 765–778. [Google Scholar] [CrossRef]
- Quintero, J.A.; Attah, R.; Khianey, R.; Capitle, E.; Schutzer, S.E. Arthritis and Diagnostics in Lyme Disease. Trop Med Infect Dis 2021, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Monco, J.C.; Benach, J.L. Lyme Neuroborreliosis: Clinical Outcomes, Controversy, Pathogenesis, and Polymicrobial Infections. Ann Neurol 2019, 85, 21–31. [Google Scholar] [CrossRef]
- Rosa Neto, N.S.; Gauditano, G.; Yoshinari, N.H. Chronic lymphomonocytic meningoencephalitis, oligoarthritis, and erythema nodosum: Report of Baggio-Yoshinari syndrome of long and relapsing evolution. Rev Bras Reumatol 2014, 54, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Ross Russell, A.L.; Dryden, M.S.; Pinto, A.A.; Lovett, J.K. Lyme disease: Diagnosis and management. Pract Neurol 2018, 18, 455–464. [Google Scholar] [CrossRef]
- Gouveia, E.A.; Alves, M.F.; Mantovani, E.; Oyafuso, L.K.; Bonoldi, V.L.; Yoshinari, N.H. Profile of patients with Baggio-Yoshinari Syndrome admitted at "Instituto de Infectologia Emilio Ribas. " Rev Inst Med Trop Sao Paulo 2010, 52, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Yoshinari, N.H. A long journey to understand Borrelia burgdorferi in Brazil. Rev Bras Reumatol 2009, 49, 483–484. [Google Scholar] [CrossRef]
- Naka, E.N.; Costa, I.P.d.; Soares, C.O.; Yoshinari, N.H. Síndrome de Lyme-símile ou complexo infecto-reacional do carrapato: Uma causa de artrite reacional. In Anais do Congresso. Belo Horizonte: Fac Med. 2006. [Google Scholar]
- Yoshinari, N.H.; Mantovani, E.; Bonoldi, V.L.; Marangoni, R.G.; Gauditano, G. Brazilian lyme-like disease or Baggio-Yoshinari syndrome: Exotic and emerging Brazilian tickborne zoonosis. Rev Assoc Med Bras (1992) 2010, 56, 363–369. [Google Scholar] [CrossRef]
- Kugeler, K.J.; Schwartz, A.M.; Delorey, M.J.; Mead, P.S.; Hinckley, A.F. Estimating the frequency of Lyme disease diagnoses, United States, 2010-2018. Emerg Infect Dis 2021, 27, 616–619. [Google Scholar] [CrossRef]
- Nascimento, D.A.; Vieira, R.F.; Vieira, T.S.; Toledo, R.D.; Tamekuni, K.; Santos, N.J.; Gonçalves, D.D.; Vieira, M.L.; Biondo, A.W.; Vidotto, O. Serosurvey of Borrelia in dogs, horses, and humans exposed to ticks in a rural settlement of southern Brazil. Rev Bras Parasitol Vet 2016, 25, 418–422. [Google Scholar] [CrossRef]
- O'Dwyer, L.H.; Soares, C.O.; Massard, C.L.; Souza, J.C.P.d.; Flausino, W.; Fonseca, A.H.d. Soroprevalência de Borrelia burgdorferi latu sensu associada à presença de carrapatos em cães de áreas rurais do Estado do Rio de Janeiro, Brasil. Ciência Rural 2004, 34, 201–205. [Google Scholar] [CrossRef]
- Gonçalves, E.S.; Cordeiro, M.D.; Dos Santos, L.M.R.; Araújo, I.M.; da Fonseca, A.H.; Labruna, M.B.; Guedes, E. Research of Rickettsia spp. and Borrelia spp. in dogs in Southeast Brazil. Vet Parasitol Reg Stud Rep 2022, 30, 100706. [Google Scholar] [CrossRef]
- Joppert, A.M.; Hagiwara, M.K.; Yoshinari, N.H. Borrelia burgdorferi antibodies in dogs from Cotia county, São Paulo State, Brazil. Rev Inst Med Trop Sao Paulo 2001, 43, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Galo, K.R.; Fonseca, A.H.; Madureira, R.C.; Barbosa Neto, J.D. Freqüência de anticorpos homólogos anti-Borrelia burgdorferi em eqüinos na mesorregião metropolitana de Belém, Estado do Pará. Pesq Vet Brasileira 2009, 29, 229–232. [Google Scholar] [CrossRef]
- Prado, R.F.S.; Campos, C.H.C.; Cordeiro, M.D.; Pires, M.S.; Mafra, C.; Cepeda, M.B.; Massard, C.L.; Fonseca, A.H. Seroprevalence of homologous anti Borrelia burgdorferi antibodies in horses of military use in Brazil. Rev Bras Ciência Veterinária 2017, 24. [Google Scholar]
- Santos, A.; Souza, A.M.; Bueno, M.G.; Catao-Dias, J.L.; Toma, H.K.; Pissinati, A.; Molina, C.V.; Kierulff, M.C.M.; Silva, D.G.F.; Almosny, N.R.P. Molecular detection of Borrelia burgdorferi in free-living golden headed lion tamarins (Leontopithecus chrysomelas) in Rio de Janeiro, Brazil. Rev Inst Med Trop Sao Paulo 2018, 60, e53. [Google Scholar] [CrossRef] [PubMed]
- Costa, I.P.; Yoshinari, N.H.; Barros, P.J.L.; Bonoldi, V.L.N.; Leon, E.P.; Zeitune, A.D.; Cossermelli, W. Doenca de lyme em mato grosso do sul: Relato de tres casos clinicos, incluindo o primeiro caso de meningite de lyme no brasil. Rev Hosp Clin Fac Med Univ Sao Paulo 1996, 51, 253–257. [Google Scholar]
- Brazil. Boletim epidemiológico. Tocantins, TO: Setor de vigilância em saúde e segurança do paciente. HDT-UFT/EBSERH. 2018. Available online: https://www.gov.br/ebserh/pt-br/hospitais-universitarios/regiao-norte/hdt-uft/saude/boletim-epidemiologico-do-hdt-uft/BoletimEpidemiolgico2018.pdf (accessed on 10 January 2024).
- Brazil. Boletim epidemiológico do HDT-UFT. Tocantins, TO. 2019. Available online: https://www.gov.br/ebserh/pt-br/hospitais-universitarios/regiao-norte/hdt-uft/saude/boletim-epidemiologico-do-hdt-uft/copy_of_BoletimEpidemiolgicodoHDTUFT2019.pdf (accessed on 10 January 2024).
- Brazil. Secretaria Municipal de Saúde de Vila Velha. Boletim Epidemiológico. 1º Semestre 2021. Available online: https://www.vilavelha.es.gov.br/midia/paginas/BE%2001-2021%20REVISADO.pdf (accessed on 14 December 2023).
- Brazil. Secretaria Municipal de Saúde de Vila Velha. Boletim Epidemiológico. 1º Semestre 2020. Available online: https://www.vilavelha.es.gov.br/midia/paginas/BE%2001-2021%20REVISADO.pdf (accessed on 14 December 2023).
- Brazil. Relatório da diretoria de vigilância epidemiológica (2019–2022). Santa Catarina: Secreta ria de Estado da Saúde. Available online: https://dive.sc.gov.br/index.php/a-dive (accessed on 10 January 2024).
- Kobayashi, T.; Auwaerter, P.G. Diagnostic testing for Lyme disease. Infect Dis Clin North Am 2022, 36, 605–620. [Google Scholar] [CrossRef] [PubMed]
- Waddell, L.A.; Greig, J.; Mascarenhas, M.; Harding, S.; Lindsay, R.; Ogden, N. The Accuracy of Diagnostic Tests for Lyme Disease in Humans, A systematic review and meta-analysis of North American research. PLoS ONE 2016, 11, e0168613. [Google Scholar] [CrossRef] [PubMed]
- Theel, E.S. The Past, Present, and (possible) future of serologic testing for Lyme disease. J Clin Microbiol 2016, 54, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Alby, K.; Capraro, G.A. Alternatives to serologic testing for the diagnosis of Lyme disease. Clin Lab Med 2015, 35, 815–825. [Google Scholar] [CrossRef]
- Li, X.; McHugh, G.A.; Damle, N.; Sikand, V.K.; Glickstein, L.; Steere, A.C. Burden and viability of Borrelia burgdorferi in skin and joints of patients with erythema migrans or lyme arthritis. Arthritis Rheum 2011, 63, 2238–2247. [Google Scholar] [CrossRef]
- Müllegger, R.R.; Glatz, M. Skin manifestations of lyme borreliosis: Diagnosis and management. Am J Clin Dermatol 2008, 9, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Sell, M.G.; Alcorta, D.A.; Padilla, A.E.; Nollner, D.W.; Hasenkampf, N.R.; Lambert, H.S.; Embers, M.E.; Spector, N.L. Visualizing Borrelia burgdorferi infection using a small-molecule imaging probe. J Clin Microbiol 2021, 59, e0231320. [Google Scholar] [CrossRef] [PubMed]
- Eisendle, K.; Grabner, T.; Zelger, B. Focus floating microscopy: "gold standard" for cutaneous borreliosis? Am J Clin Pathol 2007, 127, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Mead, P.; Petersen, J.; Hinckley, A. Updated CDC recommendation for serologic diagnosis of Lyme disease. MMWR Morb Mortal Wkly Rep 2019, 68, 703. [Google Scholar] [CrossRef] [PubMed]
- Sabin, A.P.; Scholze, B.P.; Lovrich, S.D.; Callister, S.M. Clinical evaluation of a Borrelia modified two-tiered testing (MTTT) shows increased early sensitivity for Borrelia burgdorferi but not other endemic Borrelia species in a high incidence region for Lyme disease in Wisconsin. Diagn Microbiol Infect Dis 2023, 105, 115837. [Google Scholar] [CrossRef] [PubMed]
- Pegalajar-Jurado, A.; Schriefer, M.E.; Welch, R.J.; Couturier, M.R.; MacKenzie, T.; Clark, R.J.; Ashton, L.V.; Delorey, M.J.; Molins, C.R. Evaluation of modified two-tiered testing algorithms for Lyme disease laboratory diagnosis using well-characterized serum samples. J Clin Microbiol 2018, 56. [Google Scholar] [CrossRef]
- Kenyon, S.M.; Chan, S.L. A focused review on Lyme disease diagnostic testing: An update on serology algorithms, current ordering practices, and practical considerations for laboratory implementation of a new testing algorithm. Clin Biochem 2023, 117, 4–9. [Google Scholar] [CrossRef]
- Melo, I.S.d.; Gadelha, A.d.R.; Ferreira, L.C.d.L. Estudo histopatológico de casos de eritema crônico migratório diagnosticados em Manaus. Anais Brasil Dermatol 2003, 78, 169–177. [Google Scholar] [CrossRef]
- Rodrigues, B.D.; Meireles, V.M.d.B.; Braz, M.N. Borreliose de lyme símile: Relato de caso. Revista Paraense de Medicina 2007, 21, 63–67. [Google Scholar] [CrossRef]
- Talhari, S.; de Souza Santos, M.N.; Talhari, C.; de Lima Ferreira, L.C.; Silva, R.M.; Zelger, B.; Massone, C.; Ribeiro-Rodrigues, R. Borrelia burgdorferi "sensu lato" in Brazil: Occurrence confirmed by immunohistochemistry and focus floating microscopy. Acta Trop 2010, 115, 200–204. [Google Scholar] [CrossRef]
- Lahdenne, P.; Panelius, J.; Saxen, H.; Heikkilä, T.; Sillanpää, H.; Peltomaa, M.; Arnez, M.; Huppertz, H.I.; Seppälä, I.J.T. Improved serodiagnosis of erythema migrans using novel recombinant borrelial BBK32 antigens. J Med Microbiol. 2003, 52 Pt 7, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Dattwyler, R.J.; Volkman, D.J.; Luft, B.J. Immunologic aspects of Lyme borreliosis. Rev Infect Dis 1989, 11 (Suppl. S6), S1494–S1498. [Google Scholar] [CrossRef]
- Kalish, R.A.; McHugh, G.; Granquist, J.; Shea, B.; Ruthazer, R.; Steere, A.C. Persistence of immunoglobulin M or immunoglobulin G antibody responses to Borrelia burgdorferi 10-20 years after active Lyme disease. Clin Infect Dis 2001, 33, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Kannian, P.; McHugh, G.; Johnson, B.J.; Bacon, R.M.; Glickstein, L.J.; Steere, A.C. Antibody responses to Borrelia burgdorferi in patients with antibiotic-refractory, antibiotic-responsive, or non-antibiotic-treated Lyme arthritis. Arthritis Rheum 2007, 56, 4216–4225. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, G.S.; Alugupalli, K.R. Deciphering the role of Toll-like receptors in humoral responses to Borreliae. Front Biosci (Schol Ed) 2012, 4, 699–712. [Google Scholar] [CrossRef] [PubMed]
- Aguero-Rosenfeld, M.E.; Wang, G.; Schwartz, I.; Wormser, G.P. Diagnosis of lyme borreliosis. Clin Microbiol Rev 2005, 18, 484–509. [Google Scholar] [CrossRef] [PubMed]
- Markowicz, M.; Reiter, M.; Gamper, J.; Stanek, G.; Stockinger, H. Persistent anti-Borrelia IgM antibodies without Lyme borreliosis in the clinical and immunological Context. Microbiol Spectr 2021, 9, e0102021. [Google Scholar] [CrossRef] [PubMed]
- Grąźlewska, W.; Holec-Gąsior, L. Antibody cross-reactivity in serodiagnosis of Lyme disease. Antibodies 2023, 12, 63. [Google Scholar] [CrossRef]
- Stiernstedt, G.; Eriksson, G.; Enfors, W.; Jörbeck, H.; Svenungsson, B.; Sköldenberg, B.; Granström, M. Erythema chronicum migrans in Sweden: Clinical manifestations and antibodies to Ixodes ricinus spirochete measured by indirect immunofluorescence and enzyme-linked immunosorbent assay. Scand J Infect Dis 1986, 18, 217–224. [Google Scholar] [CrossRef]
- D'Arco, C.; Dattwyler, R.J.; Arnaboldi, P.M. Borrelia burgdorferi-specific IgA in Lyme Disease. EBioMedicine 2017, 19, 91–97. [Google Scholar] [CrossRef]
- Djukic, M.; Schmidt-Samoa, C.; Lange, P.; Spreer, A.; Neubieser, K.; Eiffert, H.; Nau, R.; Schmidt, H. Cerebrospinal fluid findings in adults with acute Lyme neuroborreliosis. J Neurol 2012, 259, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Bluth, M.H.; Robin, J.; Ruditsky, M.; Norowitz, K.B.; Chice, S.; Pytlak, E.; Nowakowski, M.; Durkin, H.G.; Smith-Norowitz, T.A. IgE anti-Borrelia burgdorferi components (p18, p31, p34, p41, p45, p60) and increased blood CD8+CD60+ T cells in children with Lyme disease. Scand J Immunol 2007, 65, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Quan, P.L.; Sauzade, M.; Brouzes, E. dPCR: A Technology Review. Sensors 2018, 18, 1271. [Google Scholar] [CrossRef] [PubMed]
- Leth, T.A.; Joensen, S.M.; Bek-Thomsen, M.; Møller, J.K. Establishment of a digital PCR method for detection of Borrelia burgdorferi sensu lato complex DNA in cerebrospinal fluid. Sci Rep 2022, 12, 19991. [Google Scholar] [CrossRef] [PubMed]
- Aucott, J.N. Posttreatment Lyme disease syndrome. Infect Dis Clin North Am 2015, 29, 309–323. [Google Scholar] [CrossRef] [PubMed]
- DeGroat, W.; Abdelhalim, H.; Patel, K.; Mendhe, D.; Zeeshan, S.; Ahmed, Z. Discovering biomarkers associated and predicting cardiovascular disease with high accuracy using a novel nexus of machine learning techniques for precision medicine. Sci Rep 2024, 14, 1. [Google Scholar] [CrossRef] [PubMed]
- Boligarla, S.; Laison, E.K.E.; Li, J.; Mahadevan, R.; Ng, A.; Lin, Y.; Thioub, M.Y.; Huang, B.; Ibrahim, M.H.; Nasri, B. Leveraging machine learning approaches for predicting potential Lyme disease cases and incidence rates in the United States using Twitter. BMC Med Inform Decis Mak 2023, 23, 217. [Google Scholar] [CrossRef]
- Aucott, J.N.; Soloski, M.J.; Rebman, A.W.; Crowder, L.A.; Lahey, L.J.; Wagner, C.A.; Robinson, W.H.; Bechtold, K.T. CCL19 as a Chemokine risk factor for posttreatment Lyme disease syndrome: A prospective clinical cohort study. Clin Vaccine Immunol 2016, 23, 757–766. [Google Scholar] [CrossRef]
- Crowley, J.T.; Drouin, E.E.; Pianta, A.; Strle, K.; Wang, Q.; Costello, C.E.; Steere, A.C. A Highly Expressed human protein, apolipoprotein b-100, serves as an autoantigen in a subgroup of patients with Lyme disease. J Infect Dis 2015, 212, 1841–1850. [Google Scholar] [CrossRef]
- Petzke, M.M.; Volyanskyy, K.; Mao, Y.; Arevalo, B.; Zohn, R.; Quituisaca, J.; Wormser, G.P.; Dimitrova, N.; Schwartz, I. Global transcriptome analysis identifies a diagnostic signature for early disseminated Lyme disease and its resolution. mBio 2020, 11. [Google Scholar] [CrossRef]
- Haslund-Gourley, B.S.; Hou, J.; Woloszczuk, K.; Horn, E.J.; Dempsey, G.; Haddad, E.K.; Wigdahl, B.; Comunale, M.A. Host glycosylation of immunoglobulins impairs the immune response to acute Lyme disease. eBioMedicine 2024, 100, 104979. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions, and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions, or products referred to in the content. |
Figure 1.
Representation of the membrane structure. (A) Gram-negative bacterial membrane. (B) Spirochete membrane. The outer membrane of spirochetes has several lipoproteins and glycolipids that do not include LPS.
Figure 1.
Representation of the membrane structure. (A) Gram-negative bacterial membrane. (B) Spirochete membrane. The outer membrane of spirochetes has several lipoproteins and glycolipids that do not include LPS.
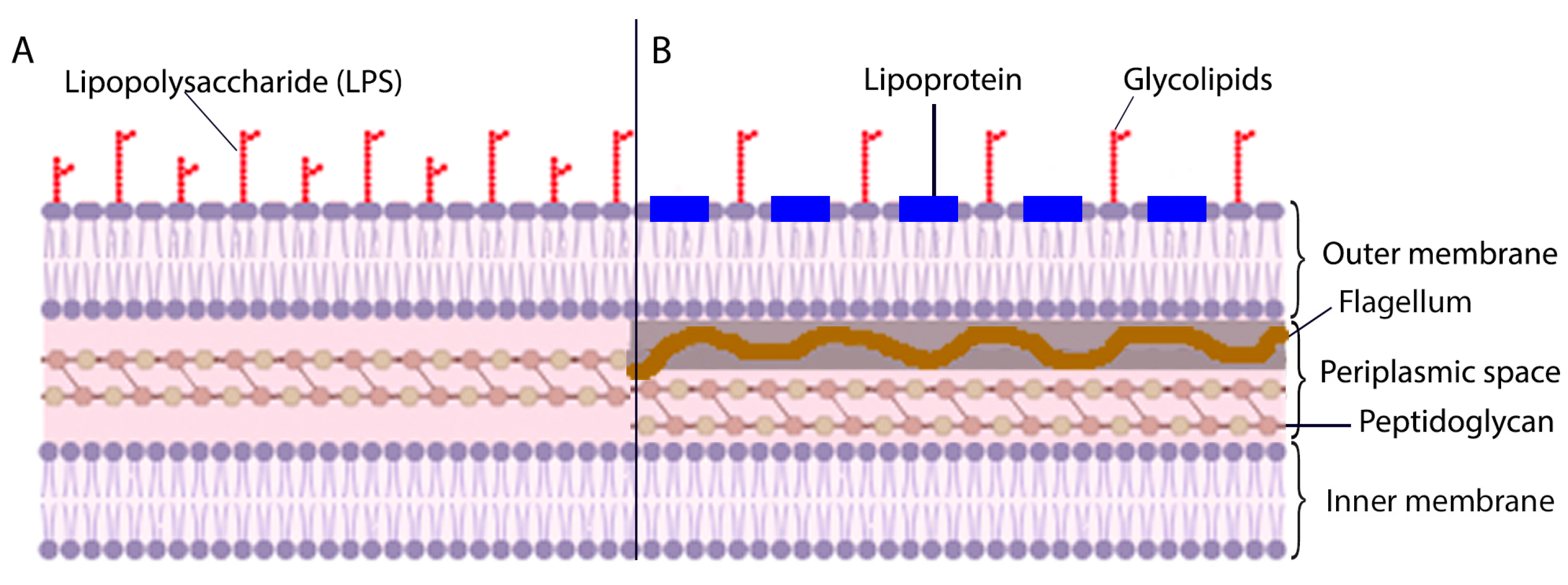
Figure 2.
Taxonomic classification of the Ixodida tick species.
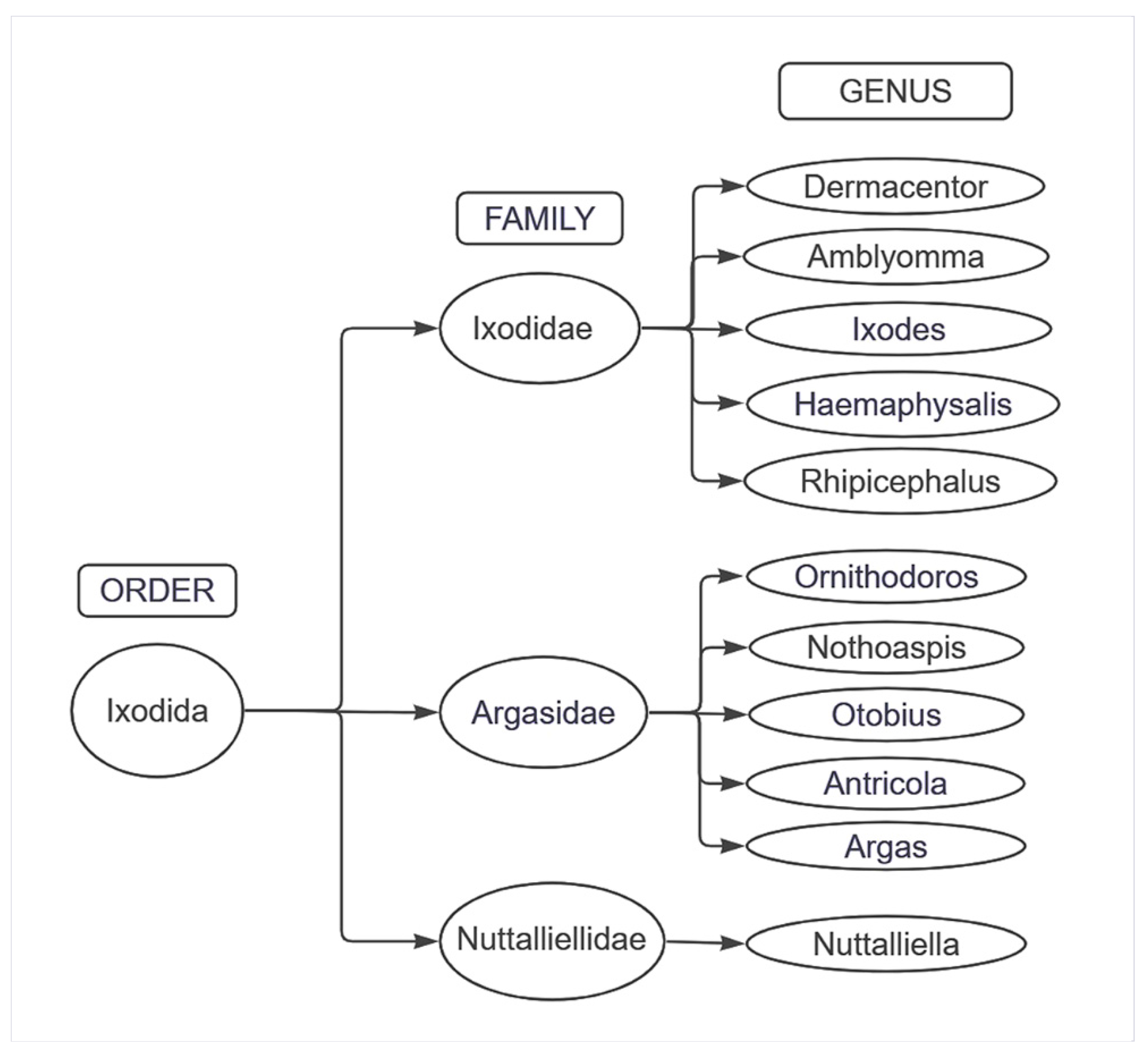
Figure 3.
Number of reported cases of Lyme disease in the United States of America, 1996-2022.
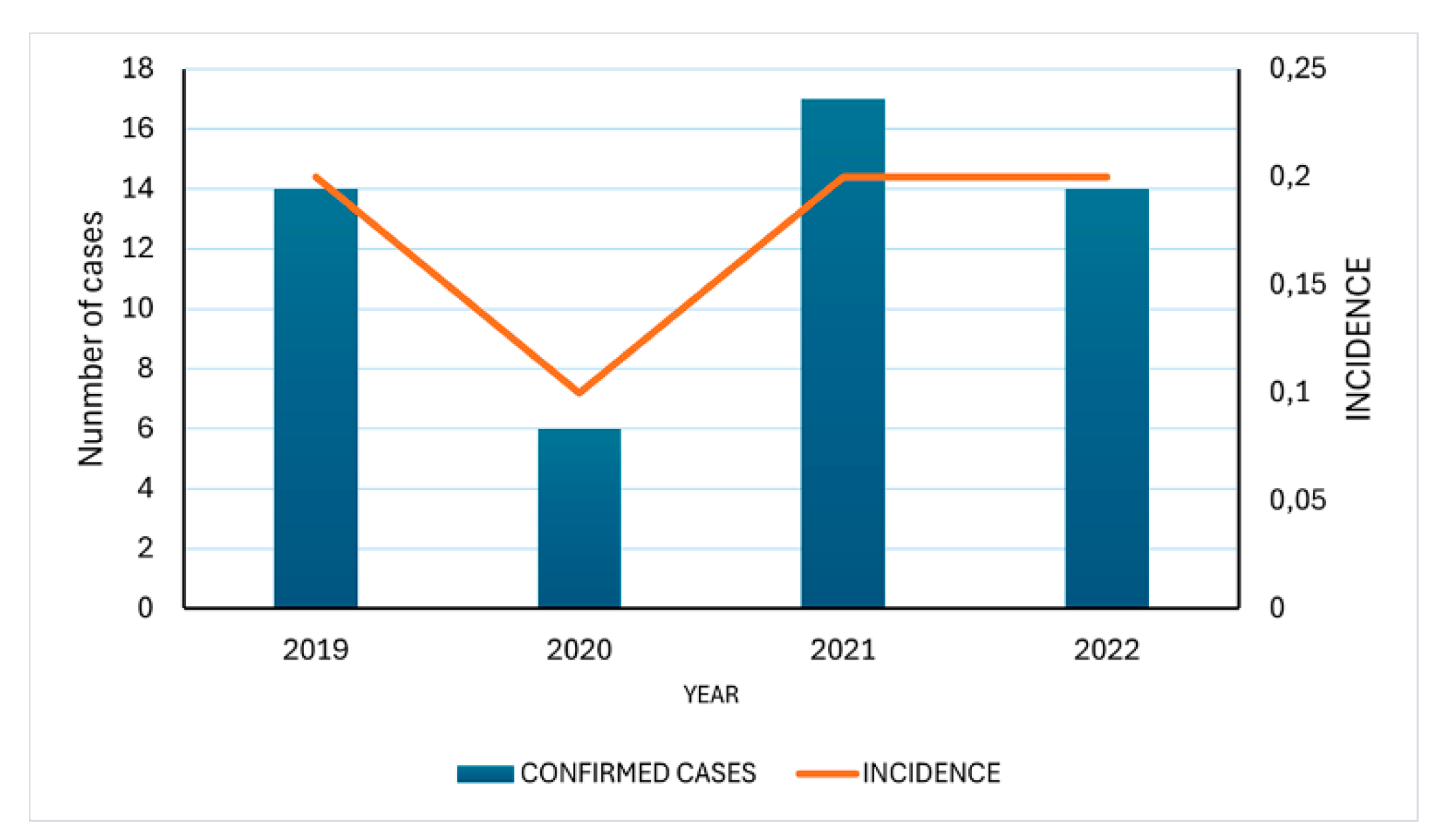
Figure 4.
The number of confirmed cases of Lyme Disease in Santa Catarina state, Brazil (2019 to 2022) was reported by the Santa Catarina Epidemiological Surveillance Directorate.
Figure 4.
The number of confirmed cases of Lyme Disease in Santa Catarina state, Brazil (2019 to 2022) was reported by the Santa Catarina Epidemiological Surveillance Directorate.
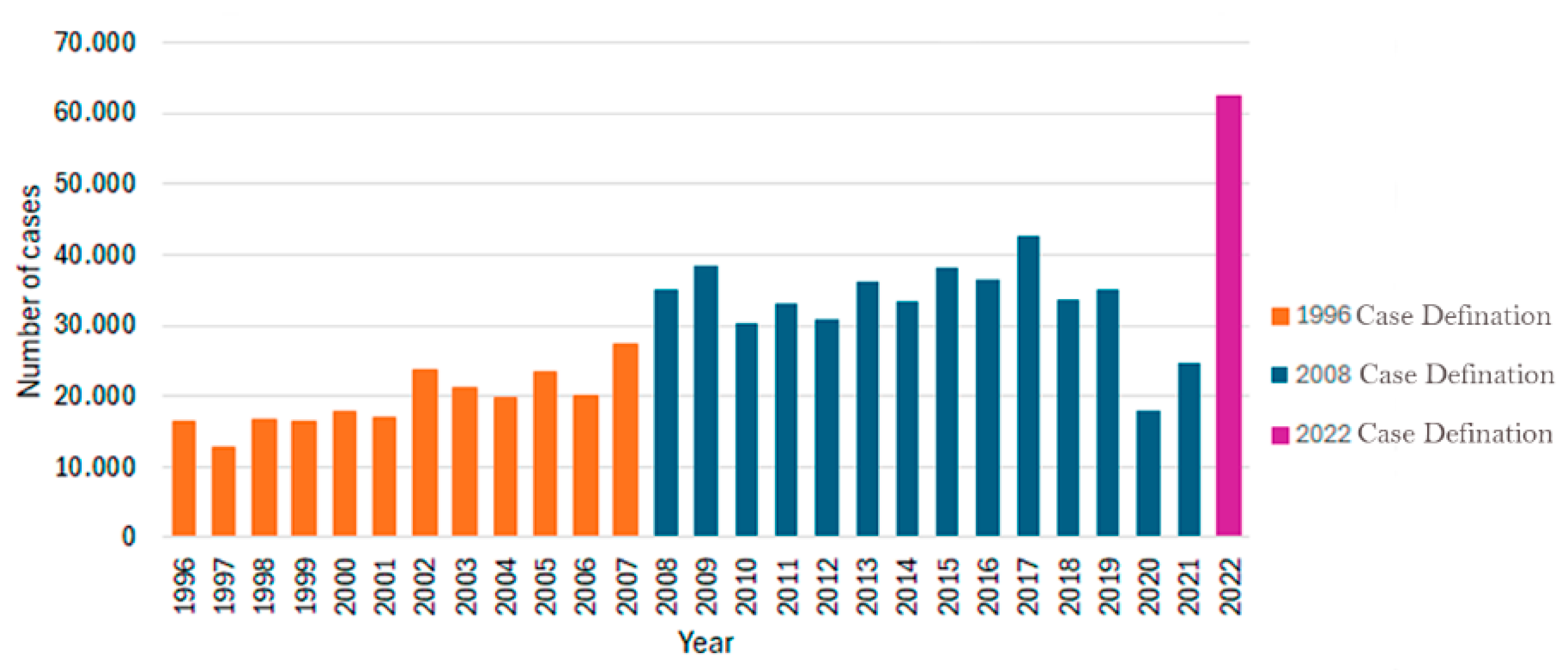

Table 1.
Clinical manifestation of Brazilian borreliosis (Lyme disease).
| Stage of the disease | USA | Brazil | Ref. |
|---|---|---|---|
| Acute infection | ME, fever, headache, arthralgia, myalgia. | Cutaneous manifestation, fever, general malaise, myalgias | [4,8,46,47] |
| Disseminated Disease | Migratory arthralgias, Lyme carditis, meningitis, facial paralysis | ||
| Chronic infection | Encephalopathy, monoarthritis, peripheral neuropathy | Neurological changes, ocular symptoms, psychiatric and psychosocial disorders, oligoarthritis, autoimmune symptoms, and chronic fatigue syndrome |
1 EM, erythema migrans.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



