
Submitted:
16 April 2024
Posted:
16 April 2024
You are already at the latest version
Abstract
Abstract: Spinal disorders are some of the most prevalent health concerns, especially among stu-dents. Based on student demographics, this cross-sectional study evaluated the correlation be-tween functional tests (FT) and spinal range of motion (ROM). This study included 206 students from Vasile Alecsandri University of Bacău. Participants' assessments were conducted using the following tests: (i) Ott, (ii) Schober, (iii) Stibor, (iv) finger-to-floor distance, (v) lateral flexion of the cervical and lumbar spine, and (vi) flexion of the cervical spine. Correlation analyses were evaluated using Spearman correlation coefficient analysis. The results indicated a very strong re-lationship between lateral flexion of the lumbar spine on the left (LFLSL) and right (LFSR) for all departments (r = 0.85 to 0.97, p < 0.05). There was a stronger relationship between FT results and spinal ROM of physical education department students compared to students from other de-partments (n = 17, r = -0.38 to 0.93, p < 0.05). There was no statistically significant correlation be-tween FT and spinal ROM based on age (p > 0.05). The study results provide evidence of the pri-mary risk factors that predispose students to postural deviations. Practitioners and physiothera-pists can utilize these values as a reference for potential therapeutic interventions.
Keywords:
spine
; posture
; students
; deviations
1. Introduction
The posture defines the alignment or orientation of body segments while maintaining an upright position. On the other hand, incorrect posture refers to an irregular state in which the body does not support a steady position [1]. The World Health Organization (WHO) reports that spinal disorders and posture deficits are modern society's most common health issues. Nowadays, due to our sedentary lifestyle, spinal disorders are becoming increasingly common in people.
While many populations suffer from incorrect posture due to various factors, students are one of the groups affected [2]. Because the students are spending many hours in the same position while studying using the computer or cell phone, they have high risks for posture deficits, spine diseases, and limited range of motion [3]. A study reported that only 19.4% of boys and 12.3% of girls had good study posture [4]. Therefore, various factors can influence students' posture. Although no evidence suggests that correct posture directly affects students' academic performance, studies have found that physical education and movement-based study programs can positively impact spine mobility and ROM [5,6]. One study revealed that only 31% of students were highly aware of their stance [7]. However, researchers observed that students with a positive attitude towards good posture inconsistently practice it [8]. Additionally, researchers have suggested that motivation levels may be related to good posture [9]. A systematic review reported a positive impact of school furniture dimensions on students' performance and physical responses [10].
On the other hand, researchers observed that postural disorders significantly differed in children living in urban and suburban environments [11,12]. Similar studies have reported conflicting evidence regarding urban-rural differences in the influence of living area on spine ROM [13,14,15]. Finally, age and sex may also impact students' posture. Studies evaluating the relationship between spinal range of motion and sex have reported conflicting results. These contradictory results may be associated with variations in anatomical structures and the frequency of joint use in habitual physical activities between sexs. It may also depend on specific joints or movements [16,17].
Although many factors influence students' posture, there is insufficient empirical evidence for these factors in previous studies. Considering that the young human population also suffers from postural disorders, it is critical to assess students' spinal ROM and uncover associated factors. Functional tests such as the Schober test, Ott test, Stibor sign, and finger floor test are commonly used to assess the range of motion, mobility, and overall functional capabilities of the spine [18]. Although these tests are traditionally used to determine the general population's spine ROM and public health, new evidence suggests that age does not affect test performances [19]. Therefore, these tests can also evaluate students' spine ROM.
This study aimed to evaluate the relationship between students' spinal ROM and functional tests and to determine the effect of demographic factors (students' age, gender, living environment, university program) on this relationship. In this study, we hypothesized that there would be a statistically significant relationship between students' functional tests and spinal ROM at different levels based on four variables (age, gender, living environment, and university program).
2. Materials and Methods
2.1. Study Design
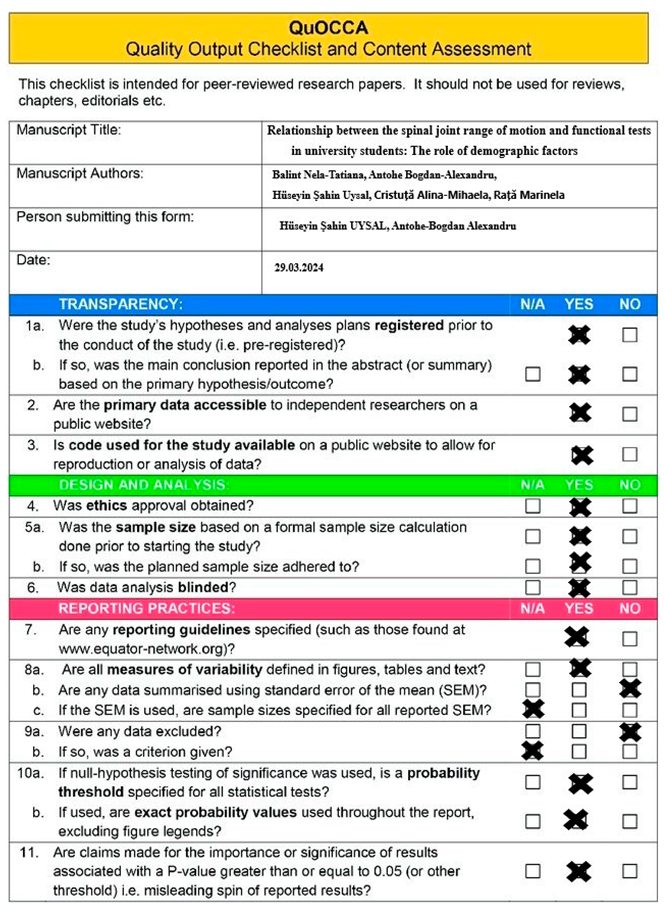
The study was conducted using a single-blind, cross-sectional study design. The Quality Output Checklist and Content Assessment (QuOCCA) checklist was used to enhance the methodological quality of the study, and it is presented in Appendix [20]. Additionally, the study protocol was pre-registered on the Open Science Framework (DOI: https://doi.org/10.17605/OSF.IO/9GC4B), and details of the study files are provided on the website. The study was approved by the Vasile Alecsandri University Ethics Committee (Approval No. 7/1/22.02.2024) and was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all participants involved in the study.
2.2. Participants
This study involved 206 students (106 males and 100 females, age: 19.85 ± 1.80 years, height: 166.86 ± 30.24 cm, and weight: 65.01 ± 14.11 kg) from the Vasile Alecsandri University of Bacău. These students were part of project CNFIS-FDI-2022-0087, which aimed to build a healthy student lifestyle and improve the quality of learning. Permission was obtained from the project manager to include the students in the study. The inclusion criteria for the study were as follows: (i) being a student at the Vasile Alecsandri University of Bacău, (ii) being 18 years or older, (iii) having a minimum class attendance of 80%, and (iv) having no physical limitations that could affect the results of the functional tests. The exclusion criteria included severe scoliosis, disk hernia, Scheuermann kyphosis, lower limb injury or height discrepancy and all the disease which could interfere with the performance of the functional tests.
This study assumed that there would be a small correlation between the students' spinal joint range of motion and functional tests. The minimum sample size of 202 participants was determined based on a priori analysis using G*Power software (version 3.1, from the University of Dusseldorf, Germany). The analysis was conducted with the following parameters (Correlation: bivariate normal model test, two-tailed, α = 0.05, β = 0.95, and r = 0.25).
2.3. Procedures
The study was conducted at the Vasile Alecsandri University of Bacău in the Physical Therapy and Occupational Therapy research laboratory. Due to the high number of subjects, assessments were performed by five physical therapy MSc students, supervised by two physical therapists (T.B. and A.M.C.). The study collected data from each participant in a single session. However, the researchers conducted multiple measurement sessions due to the large number of subjects involved. All measurements were taken during the morning, specifically from 9 a.m. to 11 a.m. The room temperature was set to 22 degrees Celsius. Male participants were required to wear shorts for the test, while female participants were asked to wear shorts and a bra. To prevent interference with the results, all participants were instructed to refrain from eating or drinking anything for 60 minutes before the test and to avoid vigorous physical activity. The study protocol was explained to the participants before the measurements to prevent bias. The subjects were instructed to remain relaxed and cooperate with the physical therapist. All measurements were taken using metric tape, and the results were reported in centimeters (cm). The participants followed a standardized warm-up protocol, which included walking on a treadmill for 7 minutes, a 1-minute cobra-cow stretch, and a 1-minute child's pose. The main goal of the warm-up was to eliminate any restrictions in the spine range of motion, which could been caused by insufficient synovial lubrication, before proceeding with the measurements.
2.4. Functional Tests
Cervical spine flexion (CSF). Cervical spine ROM was tested by measuring the distance from the suprasternal notch to the mandibular symphysis. The subject was instructed to bend his head forward while the physical therapist measured the distance between the specified points. If the subject can touch their chin to their chest, it indicates a full flexion ROM of the cervical spine [21,22]. Researchers reported that this measurement has an inter-rater reliability coefficient ranging from 0.92 to 0.88 [23]
Ott Test was used to measure the ROM of the thoracic spine in the sagittal plane. To perform the test, the seventh cervical vertebra was marked as C7, and a second point was placed on the thoracic spine, 30 cm below C7 (C7 – 30.0 cm↓). The distance between the points mentioned above was determined in the body's upright position and during the torso's maximal forward bend. A result of 33 cm or above (normal range of 3.0 cm) is considered significant [24,25,26].
The Schober test was used to determine the ROM of the lumbar spine in the sagittal plane. The first step is to draw two horizontal lines at the L5 spinous process and the other 10 cm above it. The second step measures the distance between these points during maximal forward flexion. A less than 5 cm increase in length indicates a limited range of motion in the lumbar spine [27]. The test reliability is excellent, with an intraclass correlation of 0.96 and an interclass correlation of 0.90 [28].
Stibor sign examines the ROM of the lumbar and thoracic spine during maximal forward flexion. The Stibor sign is a cumulative measure of the other two tests, Schober and Ott. To perform the test, we measure the increase in the distance between two skin marks, one over the first sacral spinous process and the other over the C7 spinous process, after maximal forward bending [27,29].
Finger-Floor Distance. The subject stands with their feet about 15 cm apart. We measure the distance between the fingertips and the floor during maximal flexion of the spine and pelvis with the knees unbent. A higher value indicates greater trunk and lower limb muscle shortening, primarily affecting the hamstring muscles [14,30]. The test reliability is excellent, with an intraclass correlation of 0.999 [31].
Frontal plane tests
Lateral flexion of the lumbar spine. It was measured with the subject standing in a neutral position, with his feet 30 cm apart and his open hands against the thighs. The third finger was kept along the lateral side of the leg and marked with a pen on the thigh bilaterally before and after the measurements. Maximum active lateral flexion of the lumbar spine was measured once in each direction (left and right). A metric tape measured the distance in centimeters between the two marks [32]. [33] reported an intraobserver reproducibility of 0.74 and interobserver reproducibility of 0.96 for this test. Another study found an ICC value ranging from 0.920 to 0.983 [31].
Lateral flexion of the cervical spine. It was measured with tape from the tragus of the ear to the tip of the shoulder (acromion process) on the same side as the direction of neck movement. Compared with radiographs [34], the Spearman coefficient was 0.58 (r = 0.58). It had a Spearman coefficient of 0.58 (r = 0.58) compared to radiographs. The ICC interrater reliability was 0.56 (0.31 to 0.74) and 0.44 (0.16 to 0.66) for interrater reliability [21,22].
2.5. Statistical Analysis
This study investigated the correlation between participants' functional test results and spine ROM. Also, the potential factors that could influence the test outcomes were considered. To avoid assessment bias, researchers performing the statistical analysis were blinded to the data collection process. According to previous studies, it was assumed that four independent variables (university department, region of residence, sex, and age) could affect the results of functional tests [35,36]. Six categorical variables were created based on university majors: (i) IT, (ii) Literature, (iii) Management, (iv) Engineering, (v) Physical Therapy, and (vi) Physical Education. The participants' places of residence were categorized as either rural or urban. Finally, the age variable was analyzed as a numeric variable. The study data were presented with a correlation matrix, which included the correlation value (r) and significance value (p). The normality assumption of the data was checked using Kolmogorov-Smirnov analysis, and it was observed that the data did not meet the normality assumption.
The relationship between functional tests and independent variables was evaluated using Spearman correlation coefficient analysis, and a total of 368 analyses were conducted to report the results. The correlation coefficient was interpreted according to the following reference values: insignificant (< 0.10), small (0.10 to 0.29), moderate (0.30 to 0.49), and strong (0.50 to 0.69), very strong (0.70 to 0.89) or excellent (> 0.90). Statistical analyses were conducted using R software (R Core Team, Vienna, Austria). The {ggplot2}, {patchwork}, and {metan} packages were selected for analysis and data visualization. All analyses were calculated with a 95% confidence interval, and the statistical significance level was set at α < 0.05. Analysis files and R codes used for the study are presented via OSF (https://doi.org/10.17605/OSF.IO/9GC4B).
3. Results
The 206 participants who agreed to participate in this study demonstrated 100% adherence to the study protocol. There were no adverse events or injuries that occurred due to the study protocol, and no participants withdrew from the study.
3.1. Analysis of the Data from the Study Program and Functional Tests
The correlation between LFLSR and LFLSL scores was consistently positive and excellent across all groups (IT: r = 0.95, p = 0.001; Literature: r = 0.92, p = 0.001; Management: r = 0.97, p = 0.001; Engineering: r = 0.92, p = 0.001; Physical therapy: r = 0.92, p = 0.001; Physical education: r = 0.93, p = 0.001). Similarly, a positive correlation was found between the LFCSL and LFCLR scores of the five groups, ranging from very strong to excellent (IT: r = 0.88, p = 0.001; Literature: r = 0.77, p = 0.001; Management: r = 0.91, p = 0.001; Engineering: r = 0.88, p = 0.001; Physical education: r = 0.84, p = 0.001). However, there was a moderate correlation between the LFCSR and LFCSL scores of the physical therapy group (r = 0.43, p = 0.01).
On the other hand, it was revealed that the correlation between the functional test results of the groups varied. While the correlation between the eight functional tests in the IT group was moderate (LFLSL and LFCSR: r = 0.44, p < 0.05; LFLSR and LFCSR: r = 0.40, p < 0.05; LFLSR and LFCSL: r = 0.45, p = 0.01; LFCSL and CSF: r = 0.46, p = 0.01), the correlation between the four functional tests was strong (LFLSL and LFCSL: r = 0.53, p = 0.01; LFCSR and CSF: r = 0.51, p = 0.01). A strong correlation was found among the six functional tests in the literature group (LFCSL and FFD: r = 0.52, p < 0.05; LFCSR and FFD: r = 0.52, p < 0.05; Stibor sign and Schober index: r = 0.65, p = 0.01). Additionally, the Ott sign and four functional tests demonstrated a statistically significant, strong negative correlation (Schober index: r = –0.51, p < 0.05; Stibor sign: r = –0.56, p < 0.05; LFCSL: r = – 0.60, p < 0.05; LFCSR: r = –0.51, p < 0.05). In the management group, there was a very strong to excellent positive correlation between lateral flexion of the lumbar spine and lateral flexion of the cervical spine (r = 0.86 to 0.97, p = 0.001). While the Schober index showed a strong negative correlation with two functional tests (LFCSR: r = –0.56, p < 0.05; LFLSR: r = –0.53, p < 0.05), the Stibor sign exhibited a strong positive correlation with two functional tests (CSF: r = 0.58, p < 0.05; Schober index: r = 0.69, p = 0.01). While the correlation between the Stibor sign and Schober index was strong for the engineering group, no statistically significant results emerged among other functional tests. The physical therapy group indicated a moderate negative correlation between the Schober index, Stibor index, Ott sign, and LFCSL (r = –0.39 to –0.42, p = 0.01). On the other hand, there was a strong relationship between the Stibor index and the Schober index (r = 0.68, p = 0.001). Additionally, small to moderate statistically significant results were found in the 16 functional tests. Finally, in the physical education group, there was a strong relationship between the Stibor and Schober indexes (r = 0.64, p = 0.001). A negative correlation was found between the Schober index and lateral flexion of the cervical spine (r = –0.38, p = 0.01). Additionally, 24 relationship analysis results showed statistically significant findings.
All the other correlation analyses conducted did not reveal any statistically significant results. The analysis results relating to the study program and functional tests are presented in Figure 1.
Legend. A: Information technology student; B: Literature student; C: Management student; D: Engineering student; E: Physical therapy student; F: Physical education student; FFD: Finger floor distance; LFLSL: Lateral flexion lumbar spine left; LFLSR: Lateral flexion lumbar spine right; LFCSL: Lateral flexion cervical spine left; LFCSR: Lateral flexion cervical spine right; CSF: Cervical spine flexion; ns = p >= 0.05; * = p < 0.05; ** = p < 0.01; *** = p < 0.001. The correlation matrix uses color gradients to represent the correlation between dependent variables. The negative correlation of red or near-red color tones, the positive correlation of blue or near-blue hues, and color tones close to white and white indicate a neutral correlation, respectively. While the correlation value is displayed in the boxes, the statistical significance of this value is indicated below the value.
3.2. Analysis of the Data from the Region of Residence and Functional Tests
While there was an excellent positive correlation between LFLSR and LFLSL scores of rural region participants (r = 0.91, p = 0.001), there was also a very strong positive correlation between LFCSL and LFCSR (r = 0.86, p = 0.001). Similarly, there were positive moderate correlations between the flexion cervical spine and the flexion lumbar spine tests (r = 0.43 to 0.53, p = 0.001). On the other hand, a strong positive correlation was found between the Schober index and the Stibor sign (r = 0.62, p = 0.001). Finally, small levels and statistically significant correlations were observed in the ten relationship analyses for the group residing in rural areas.
Similar results were observed in participants residing in urban areas. While an excellent positive correlation was found between LFLSR and LFLSL (r = 0.94, p = 0.001), a very strong positive correlation was also found between LFCSR and LFCSL (r = 0.79, p = 0.001). Additionally, the results revealed a strong positive correlation between the Stibor sign and the Schober index (r = 0.66, p = 0.001). A moderate positive correlation was observed between the CSF, LFCSL, LFCSR, LFLSL, and LFLSR tests in eight analyses (r = 0.29 to 0.41, p = 0.01). Although significant differences were found in six functional test analyses, the level of correlation was determined to be small. The analysis details for the region of residence are presented in Figure 2.
Legend. A: Rural region; B: Urban region; FFD: Finger floor distance; LFLSL: Lateral flexion lumbar spine left; LFLSR: Lateral flexion lumbar spine right; LFCSL: Lateral flexion cervical spine left; LFCSR: Lateral flexion cervical spine right; CSF: Cervical spine flexion; ns = p >= 0.05; * = p < 0.05; ** = p < 0.01; *** = p < 0.001. The correlation matrix uses color gradients to represent the correlation between dependent variables. The negative correlation of red or near-red color tones, the positive correlation of blue or near-blue hues, and color tones close to white and white indicate a neutral correlation, respectively. While the correlation value is displayed in the boxes, the statistical significance of this value is indicated below the value.
3.3. Analysis of the Data between Sex and Functional Tests
The correlation between LFLSR and LFLSL was positive and excellent for both sex (male: r = 0.92, p = 0.001; female: r = 0.91, p = 0.001). The analysis results showed a very strong positive correlation between LFCSL and LFCSR (male: r = 0.79, p = 0.001; female: r = 0.74, p = 0.001). A strong positive correlation was also found between the Stibor sign and the Schober index (male: r = 0.56, p = 0.001; female: r = 0.70, p = 0.001). The results of 13 functional test analyses of male participants showed small but statistically significant correlation results, while 12 analyses of female participants also revealed small yet statistically significant results. Details of the relationship between functional tests according to sex are presented in Figure 3.
Legend. A: Male; B: Female; FFD: Finger floor distance; LFLSL: Lateral flexion lumbar spine left; LFLSR: Lateral flexion lumbar spine right; LFCSL: Lateral flexion cervical spine left; LFCSR: Lateral flexion cervical spine right; CSF: Cervical spine flexion; ns = p >= 0.05; * = p < 0.05; ** = p < 0.01; *** = p < 0.001. The correlation matrix uses color gradients to represent the correlation between dependent variables. The negative correlation of red or near-red color tones, the positive correlation of blue or near-blue hues, and color tones close to white and white indicate a neutral correlation, respectively. While the correlation value is displayed in the boxes, the statistical significance of this value is indicated below the value.
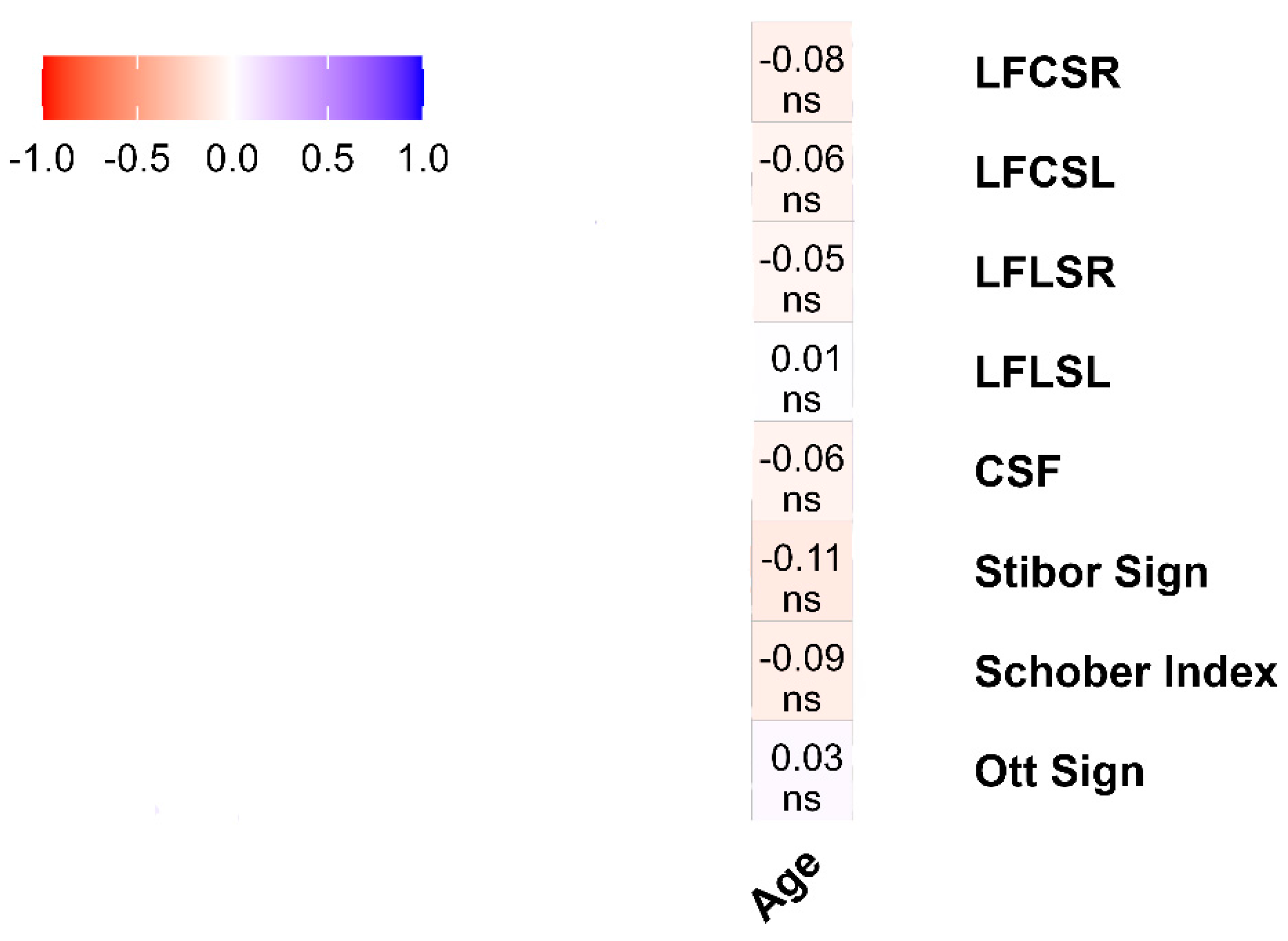
3.4. Analysis of the Data between Age and Functional Tests
Although the age variable was analyzed with eight functional tests as a numerical variable, no statistically significant relationship was observed between age and any functional test. Details about the relationship between age and functional tests are presented in Figure 4.
Legend. FFD: Finger floor distance; LFLSL: Lateral flexion lumbar spine left; LFLSR: Lateral flexion lumbar spine right; LFCSL: Lateral flexion cervical spine left; LFCSR: Lateral flexion cervical spine right; CSF: Cervical spine flexion; ns = p >= 0.05. The correlation matrix uses color gradients to represent the correlation between dependent variables. The negative correlation of red or near-red color tones, the positive correlation of blue or near-blue hues, and color tones close to white and white indicate a neutral correlation, respectively. While the correlation value is displayed in the boxes, the statistical significance of this value is indicated below the value.
4. Discussion
This study aimed to investigate the relationship between functional tests assessing spine ROM) and various demographic factors among students, including their university department, region of residence, sex, and age. The findings uncovered several notable correlations, providing insights into potential implications for preventing and treating spinal health issues in this population.
Upon examining the correlation between the university department variable and functional tests, it was discovered that students majoring in Literature and Management exhibited a stronger correlation with the lateral flexion of the lumbar and cervical spine tests. Consistent with previous studies, a high prevalence of postural deviations in the frontal plane of the spine was observed among students [37,38]. Furthermore, previous studies have indicated a higher incidence of scoliosis among female students [39,40].
Literature, Management, and Engineering students are more likely to correlate with functional tests on the sagittal plane. There was a slight difference in the direction of students from urban areas in the sagittal plane. Moreover, women showed many positive correlations with the functional tests, especially for the Schober and cervical spine flexion tests. We also found in the literature that kyphosis is a joint spine deformity in students, especially in women. Also, forward head posture was found in 63.96% of students [41,42,43]. These findings supported our study results since most students were between 18 and 21 years old, and 67% were women. It has been observed that students majoring in Literature, Management, and Engineering are more likely to show a higher correlation with sagittal plane functional tests. However, there was a slight difference in the results for students from urban areas in the sagittal plane. In addition, women showed a positive correlation with functional tests, especially for the Schober and cervical spine flexion tests. Literature also suggests that spine deformities such as kyphosis commonly affect students, particularly women [44]. Furthermore, it was found that 63.96% of students had a forward head posture [45], and 67% of them were women.
The risk factors associated with this type of deviation, which are characteristics of students, include poor sitting posture, muscle imbalances, sitting away from the table, and poorly positioned lower limbs [46,47]. Prolonged smartphone usage is another critical factor in the correlations found in the cervical spine flexion test [48,49]. Excessive smartphone use can shift the head's center of gravity forward. Poor sitting posture, muscle imbalances, sitting away from the table, and poorly positioned lower limbs are risk factors associated with the deviations above among students [46]. According to researchers, prolonged use of smartphones is also a critical factor in the correlation with cervical spine flexion tests [47].
Frontal and sagittal plane dysfunctions of the spine, such as forward head posture, kyphosis, and scoliosis, can increase the risk of degenerative disk disease, disk hernia, vertebral body compression, and zygapophysial joint arthritis [50,51,52]. We found no correlations between variables when analyzing the results based on age. This may be because our subjects were all similar age, ranging from 19 to 23 years old. Although the literature suggests that age is a risk factor for spine deformities, it usually refers to those aged between 13 and 15 years old or older adults [40,53]. Additionally, the absence of correlations does not necessarily indicate the lack of future spine deformities. Our subjects are young people who spend more than two hours on their smartphones and computers and are vulnerable to health problems associated with prolonged device use [54]. Age can be an essential factor for posture deformities. Still, it should be considered along with other risk factors such as sex, environment, level of physical activity, etc.
The lack of significant correlations between age and functional test outcomes suggests that age may not be this population's primary determinant of spinal range of motion [19]. Our findings indicate that factors other than age may have a greater influence on spinal health among young individuals. The studies on spinal mobility in different sexs have produced mixed results. While some studies have found no significant differences in spine mobility between sexs [13,14,15], other studies suggest that sex differences in spinal mobility may be influenced by factors such as job type, disease, and spinal level. Our findings indicate significant differences in postural deviations between men and women, with a stronger correlation observed in women. The strength of muscles and fascia, as well as the stiffness of joints, are vital factors that affect men's spinal health [55]. Moreover, anatomic variations in spine pedicles, which are more prominent in males, may explain these differences [55]. While physically demanding occupations can help maintain men's spinal health, they also pose a risk for reduced intervertebral disc height and range of motion [56]. On the other hand, the primary risk factor for spine deformities in women is their increased range of motion compared to men [57,58], as well as static jobs and hormonal laxity [59].
It is a commonly accepted fact that rural residents tend to engage in more physical activity than those who live in urban areas [60]. This indicates that the environment in which one lives can be a risk factor for spine-related health problems. According to our study results, urban dwellers are more likely to suffer from spine-related issues due to stress, pollution, and sedentary jobs. These conditions can significantly increase the chances of developing spine diseases [61]. On the other hand, rural residents who tend to be more physically active need to be cautious not to indulge in excessive physical activity as it can also lead to spine-related problems. Overloading the spine with excessive physical activity can result in health problems, too. Furthermore, the positive correlations observed between specific functional tests, such as lateral flexion of the lumbar spine and cervical spine, among different student groups suggest the presence of consistent patterns in spinal mobility among individuals with diverse living environments and lifestyles [62,63].
Although we collected data on several variables, it is essential to acknowledge the limitations of our research. This study did not measure the rotation and extension of the spine, which would have doubled the number of variables and made it challenging to include all the data in our study. We should have validated our tape measure against the gold radiography standard. However, we validated our measurements through inter- and intraclass correlations, which support the accuracy of our data. Furthermore, subjecting healthy volunteers to radiation raised ethical concerns. It is worth noting that the results of our study may not be directly applicable to young students.
5. Conclusions
It has been observed that postural asymmetries in the frontal plane of study participants can be influenced by various factors such as age, sex, environment, and living conditions. These findings emphasize the necessity of interventions to enhance postural habits and decrease the prevalence of postural changes in students.
Moving forward, longitudinal studies are needed to elucidate further the underlying mechanisms driving these correlations and to inform the development of effective preventive strategies tailored to individual needs and circumstances. Variations were observed in the strength and direction of correlations between different functional tests within each student group. This variability may be attributed to many factors, including individual biomechanical differences, habitual movement patterns, and environmental influences.
Supplementary Materials
Author Contributions
Conceptualization, Bogdan Antohe and Marinela Rață; Data curation, Nela-Tatiana Balint and Mihaela-Alina Cristuta; Formal analysis, Nela-Tatiana Balint, Mihaela-Alina Cristuta and Marinela Rață; Funding acquisition, Nela-Tatiana Balint, Bogdan Antohe, Mihaela-Alina Cristuta and Marinela Rață; Investigation, Bogdan Antohe and Mihaela-Alina Cristuta; Methodology, Bogdan Antohe and Huseyin Uysal; Project administration, Bogdan Antohe; Resources, Nela-Tatiana Balint and Marinela Rață; Software, Bogdan Antohe and Huseyin Uysal; Supervision, Huseyin Uysal; Validation, Nela-Tatiana Balint, Mihaela-Alina Cristuta and Marinela Rață; Visualization, Nela-Tatiana Balint and Marinela Rață; Writing – original draft, Bogdan Antohe and Huseyin Uysal; Writing – review & editing, Marinela Rață.
Funding
This research was founded by „Vasile Alecsandri” University of Bacău.
Institutional Review Board Statement
The study was approved by „Vasile Alecsandri” University of Bacău Ethics Committee (Approval No. 7/1/22.02.2024).
Informed Consent Statement
“Informed consent was obtained from all subjects involved in the study.”
Data Availability Statement
Acknowledgments
no acknowledgements
Conflicts of Interest
“The authors declare no conflicts of interest.”
Appendix 1. QuOCCA Checklist of the Study
References
- R. Kousar, S. S. Mir, S. Sarfaraz, K. Fatima, F. Islam, and A. Raza, “Knowledge, Attitude and Practice Survey on Body Posture Among Undergraduate Physiotherapy Students,” Pak-Euro Journal of Medical and Life Sciences, vol. 5, no. 2, pp. 399–404, Jun. 2022. [CrossRef]
- P. J. Penha, N. L. J. Penha, B. K. G. De Carvalho, R. M. Andrade, A. C. B. Schmitt, and S. M. A. João, “Posture Alignment of Adolescent Idiopathic Scoliosis: Photogrammetry in Scoliosis School Screening,” J Manipulative Physiol Ther, vol. 40, no. 6, pp. 441–451, Jul. 2017. [CrossRef]
- J. P. Scannell and S. M. McGill, “Lumbar Posture—Should It, and Can It, Be Modified? A Study of Passive Tissue Stiffness and Lumbar Position During Activities of Daily Living,” Phys Ther, vol. 83, no. 10, pp. 907–917, Oct. 2003. [CrossRef]
- O. Horodetska and B. Kuts, “Functional condition of students with different types of posture,” Health, sport, rehabilitation, vol. 8, no. 2, pp. 21–30, Jun. 2022. [CrossRef]
- A. Sudre, I. T. Figuereido, C. Lukas, B. Combe, and J. Morel, “On the impact of a dedicated educational program for ankylosing spondylitis: Effect on patient satisfaction, disease knowledge and spinal mobility, a pilot study,” Joint Bone Spine, vol. 79, no. 1, pp. 99–100, Jan. 2012. [CrossRef]
- J. C. Espinola et al., “Body awareness on postural sitting habits among college students in online classes”.
- F. J. González Espinosa de los Monteros, G. Gonzalez-Medina, E. M. G. Ardila, J. R. Mansilla, J. P. Expósito, and P. O. Ruiz, “Use of Neurodynamic or Orthopedic Tension Tests for the Diagnosis of Lumbar and Lumbosacral Radiculopathies: Study of the Diagnostic Validity,” Int J Environ Res Public Health, vol. 17, no. 19, p. 7046, Sep. 2020. [CrossRef]
- R. Kousar, S. S. Mir, S. Sarfaraz, K. Fatima, F. Islam, and A. Raza, “Knowledge, Attitude and Practice Survey on Body Posture Among Undergraduate Physiotherapy Students,” Pak-Euro Journal of Medical and Life Sciences, vol. 5, no. 2, pp. 399–404, Jun. 2022. [CrossRef]
- X. Yang, X. Zhao, X. Tian, and B. Xing, “Effects of environment and posture on the concentration and achievement of students in mobile learning,” Interactive Learning Environments, vol. 29, no. 3, pp. 400–413, Apr. 2021. [CrossRef]
- H. I. Castellucci, P. M. Arezes, J. F. M. Molenbroek, R. de Bruin, and C. Viviani, “The influence of school furniture on students’ performance and physical responses: results of a systematic review,” Ergonomics, vol. 60, no. 1, pp. 93–110, Jan. 2017. [CrossRef]
- B. P.-G. T. Š. M. R. M. B. and M. K. Ksenija Radaković, “POSTURAL AND NUTRITIONAL STATUS OF STUDENTS FROM URBAN AND SUBURBAN ENVIRONMENT,” EXERCISE AND QUALITY OF LIFE, vol. 7, no. 1, 2015.
- P. Montuori et al., “Assessment on Practicing Correct Body Posture and Determinant Analyses in a Large Population of a Metropolitan Area,” Behavioral Sciences, vol. 13, no. 2, p. 144, Feb. 2023. [CrossRef]
- P. Patel and L. Parmar, “Normative values of trunk mobility in normal adults,” Int J Health Sci (Qassim), pp. 6171–6179, Jun. 2022. [CrossRef]
- J. L. Garrido-Castro et al., “Validation of a new objective index to measure spinal mobility: the University of Cordoba Ankylosing Spondylitis Metrology Index (UCOASMI),” Rheumatol Int, vol. 34, no. 3, pp. 401–406, Mar. 2014. [CrossRef]
- R. Lenková and V. Vasilišinová, “Spinal Mobility in Women with Sedentary Job,” Acta Facultatis Educationis Physicae Universitatis Comenianae, vol. 59, no. 2, pp. 138–147, Nov. 2019. [CrossRef]
- J. Hwang and M.-C. Jung, “Age and sex differences in ranges of motion and motion patterns,” International Journal of Occupational Safety and Ergonomics, vol. 21, no. 2, pp. 173–186, Apr. 2015. [CrossRef]
- I. Saidu, S. Maduagwu, A. Abbas, O. Adetunji, and A. Jajere, “Lumbar spinal mobility changes among adults with advancing age,” J Midlife Health, vol. 2, no. 2, p. 65, 2011. [CrossRef]
- M. J., H. L. D., G. J. R., S. R. L., & W. S. Northgraves, “Spinal mobility and its relationship to balance and functional mobility among community-dwelling adults.,” J Manipulative Physiol Ther, vol. 39, no. 4, pp. 267–276, 2016.
- A. A. Butler, J. C. Menant, A. C. Tiedemann, and S. R. Lord, “Age and gender differences in seven tests of functional mobility,” J Neuroeng Rehabil, vol. 6, no. 1, p. 31, Dec. 2009. [CrossRef]
- M. E. Héroux et al., “Quality Output Checklist and Content Assessment (QuOCCA): a new tool for assessing research quality and reproducibility,” BMJ Open, vol. 12, no. 9, p. e060976, Sep. 2022. [CrossRef]
- S. E. Asha and R. Pryor, “Validation of a Method to Assess Range of Motion of the Cervical Spine Using a Tape Measure,” J Manipulative Physiol Ther, vol. 36, no. 8, pp. 538–545, Oct. 2013. [CrossRef]
- C.-Y. Hsieh and B. W. Yeung, “Active Neck Motion Measurements with a Tape Measure,” Journal of Orthopaedic & Sports Physical Therapy, vol. 8, no. 2, pp. 88–92, Aug. 1986. [CrossRef]
- A. Balogun, O. K. Abereoje, M. O. Olaogun, and V. A. Obajuluwa, “Inter- and Intratester Reliability of Measuring Neck Motions with Tape Measure and Myrin ® Gravity—Reference Goniometer,” Journal of Orthopaedic & Sports Physical Therapy, vol. 10, no. 7, pp. 248–253, Jan. 1989. [CrossRef]
- T. Consmüller, A. Rohlmann, D. Weinland, C. Druschel, G. N. Duda, and W. R. Taylor, “Comparative evaluation of a novel measurement tool to assess lumbar spine posture and range of motion,” European Spine Journal, vol. 21, no. 11, pp. 2170–2180, Nov. 2012. [CrossRef]
- M. Orzechowska and E. Prętkiewicz-Abacjew, “The Range of Thoracic-Lumbar Segment of Spine Mobility in Saggital and Transverse Plane among Young Men Divided into Three Groups Differing in the Current Commitment to Physical Activity,” Balt J Health Phys Act, vol. 3, no. 3, Jan. 2011. [CrossRef]
- C. Theisen et al., “Co-occurrence of outlet impingement syndrome of the shoulder and restricted range of motion in the thoracic spine - a prospective study with ultrasound-based motion analysis,” BMC Musculoskelet Disord, vol. 11, no. 1, p. 135, Dec. 2010. [CrossRef]
- R. Bednár et al., “Low back pain in patients hospitalised with liver cirrhosis- a retrospective study,” BMC Musculoskelet Disord, vol. 24, no. 1, p. 310, Apr. 2023. [CrossRef]
- P. S. F. J. et al. Rahali-Khachlouf H, “ Validité et reproductibilité des mesures cliniques rachidiennes dans la spondylarthrite ankylosante. Ann Réadapt Méd Phys 2001; 44 : 205 – 12,” LiSSa, LA PLATEFORME D’INDEXATION DE RÉFÉRENCE POUR LES REVUES DES PROFESSIONS DE SANTÉ EN LANGUE FRANÇAISE, vol. 44, no. 4, pp. 205–12, 2001.
- C. V. de Souza, E. C. M. Miranda, C. Garcia Jr, F. J. P. Aranha, C. A. de Souza, and A. C. Vigorito, “Functional evaluation indicates physical losses after hematopoietic stem cell transplantation,” Rev Bras Hematol Hemoter, vol. 34, no. 5, pp. 345–351, 2012. [CrossRef]
- A. Moriyasu et al., “Pole Exercise Causes Body Changes in Physical Flexibility and Exercise Function,” J Nov Physiother, vol. 08, no. 01, 2018. [CrossRef]
- M. Johnson and M. J. Mulcahey, “Interrater Reliability of Spine Range of Motion Measurement Using a Tape Measure and Goniometer,” J Chiropr Med, vol. 20, no. 3, pp. 138–147, Sep. 2021. [CrossRef]
- M. Alricsson, K. Harms-Ringdahl, K. Eriksson, and S. Werner, “The effect of dance training on joint mobility, muscle flexibility, speed and agility in young cross-country skiers – a prospective controlled intervention study,” Scand J Med Sci Sports, vol. 13, no. 4, pp. 237–243, Aug. 2003. [CrossRef]
- G. P. Mellin, “Accuracy of measuring lateral flexion of the spine with a tape,” Clinical Biomechanics, vol. 1, no. 2, pp. 85–89, 86. 19 May. [CrossRef]
- Viitanen, “Neck mobility assessment in ankylosing spondylitis: a clinical study of nine measurements including new tape methods for cervical rotation and lateral flexion,” Rheumatology, vol. 37, no. 4, pp. 377–381, Apr. 1998. [CrossRef]
- J. Drzał-Grabiec and S. Snela, “The influence of rural environment on body posture.,” Ann Agric Environ Med, vol. 19, no. 4, pp. 846–50, 2012.
- D. Trzcińska, D. Świderska, P. Tabor, and E. Olszewska, “ENVIRONMENTAL DIVERSITY IN BODY POSTURE OF SIX-YEAR-OLD CHILDREN,” pjst, vol. 20, no. 3, pp. 205–210, Sep. 2013. [CrossRef]
- J. A. Sedrez, M. I. Z. Da Rosa, M. Noll, F. da S. Medeiros, and C. T. Candotti, “Fatores de risco associados a alterações posturais estruturais da coluna vertebral em crianças e adolescentes,” Revista Paulista de Pediatria, vol. 33, no. 1, pp. 72–81, Mar. 2015. [CrossRef]
- P. J. Penha, N. L. J. Penha, B. K. G. De Carvalho, R. M. Andrade, A. C. B. Schmitt, and S. M. A. João, “Posture Alignment of Adolescent Idiopathic Scoliosis: Photogrammetry in Scoliosis School Screening,” J Manipulative Physiol Ther, vol. 40, no. 6, pp. 441–451, Jul. 2017. [CrossRef]
- S. Nery, R. Halpern, P. C. Nery, K. P. Nehme, and A. Tetelbom Stein, “Prevalence of scoliosis among school students in a town in southern Brazil,” Sao Paulo Medical Journal, vol. 128, no. 2, pp. 69–73, 2010. [CrossRef]
- P. Baroni et al., “Factors Associated With Scoliosis in Schoolchildren: a Cross-Sectional Population-Based Study,” J Epidemiol, vol. 25, no. 3, pp. 212–220, 2015. [CrossRef]
- S. B. R. N. Arfa Naz, “Prevalance of forward head posture amonguniversity students,” Rawal Medical Journal, vol. 44, no. 2, 2018.
- J. R. Sofaer Derevenski, “Sex differences in activity-related osseous change in the spine and the gendered division of labor at Ensay and Wharram Percy, UK,” Am J Phys Anthropol, vol. 111, no. 3, pp. 333–354, Mar. 2000. [CrossRef]
- B. G. Diebo, J. Henry, V. Lafage, and P. Berjano, “Sagittal deformities of the spine: factors influencing the outcomes and complications,” European Spine Journal, vol. 24, no. S1, pp. 3–15, Jan. 2015. [CrossRef]
- Z. S. F. Ms. F. A. Ms. H. N. P. Mohammad Karimizadeh Ardakani1 *, “Effect of Thoracic Hyper-Kyphosis Posture on Upper Extremity Function of Female Students,” Journal of Rehabilitation Sciences and Research, vol. 9, no. 1, pp. 30–35, 2022.
- V. Ramalingam and A. Subramaniam, “Prevalence and Associated Risk Factors of Forward Head Posture among University Students,” Indian J Public Health Res Dev, vol. 10, no. 7, p. 775, 2019. [CrossRef]
- L. G. L. Araújo, V. P. Rodrigues, I. A. Figueiredo, and M. N. L. Medeiros, “Association between sitting posture on school furniture and spinal changes in adolescents,” Int J Adolesc Med Health, vol. 34, no. 6, pp. 469–475, Nov. 2022. [CrossRef]
- M.-L. Nault et al., “Relations Between Standing Stability and Body Posture Parameters in Adolescent Idiopathic Scoliosis,” Spine (Phila Pa 1976), vol. 27, no. 17, pp. 1911–1917, Sep. 2002. [CrossRef]
- S. I. Jung, N. K. Lee, K. W. Kang, K. Kim, and D. Y. Lee, “The effect of smartphone usage time on posture and respiratory function,” J Phys Ther Sci, vol. 28, no. 1, pp. 186–189, 2016. [CrossRef]
- N. W. A. W. I. A. W. and S. A. P. T. N. P. Wiguna, “The Relationship Between Smartphone Addiction and Forward Head Posture in Junior High School Students in North Denpasar,” Jurnal Epidemiologi Kesehatan Komunitas, vol. 4, no. 2, pp. 84–89, 2019.
- M. Cho, Y. Lee, C. S. Kim, and W. Gong, “Correlations among Sacral Angle, Lumbar Lordosis, Lumbar ROM, Static and Dynamic Lumbar Stability in College Students,” J Phys Ther Sci, vol. 23, no. 5, pp. 793–795, 2011. [CrossRef]
- P. Roussouly and C. Nnadi, “Sagittal plane deformity: an overview of interpretation and management,” European Spine Journal, vol. 19, no. 11, pp. 1824–1836, Nov. 2010. [CrossRef]
- B. G. Diebo, J. Henry, V. Lafage, and P. Berjano, “Sagittal deformities of the spine: factors influencing the outcomes and complications,” European Spine Journal, vol. 24, no. S1, pp. 3–15, Jan. 2015. [CrossRef]
- S. Sung, “Different coordination and flexibility of the spine and pelvis during lateral bending between young and older adults,” Hum Mov Sci, vol. 46, pp. 229–238, Apr. 2016. [CrossRef]
- Castro, M. Kwon, A. Filler, T. Kowatsch, and M. P. Schaub, “Smartphone use and smartphone addiction among young people in Switzerland,” J Behav Addict, vol. 4, no. 4, pp. 299–307, Dec. 2015. [CrossRef]
- M. McGill, K. Jones, G. Bennett, and P. J. Bishop, “Passive stiffness of the human neck in flexion, extension, and lateral bending,” Clinical Biomechanics, vol. 9, no. 3, pp. 193–198, 94. 19 May. [CrossRef]
- M. O. Oyakhire and C. Agi, “Assessment of the Spine in a Healthy Working Population : A Radiographic Study of the Lumbrosacral Angle in Relation to Occupation in Southern Nigeria,” Asian J Med Sci, vol. 5, no. 2, pp. 99–105, Dec. 2013. [CrossRef]
- T. Seacrist et al., “Passive cervical spine flexion: The effect of age and gender,” Clinical Biomechanics, vol. 27, no. 4, pp. 326–333, 12. 20 May. [CrossRef]
- B. D. Stemper et al., “Lumbar Spinal Mechanics in Pure Bending: Influence of Gender, Spinal Level, and Degeneration Grade,” in ASME 2009 Summer Bioengineering Conference, Parts A and B, American Society of Mechanical Engineers, Jun. 2009, pp. 1257–1258. [CrossRef]
- J. C. Prior, Y. M. Vigna, M. T. Schechter, and A. E. Burgess, “Spinal Bone Loss and Ovulatory Disturbances,” New England Journal of Medicine, vol. 323, no. 18, pp. 1221–1227, Nov. 1990. [CrossRef]
- Hughes, L. Thornton, A. Venn, K. Squibb, and K. Ball, “A Qualitative Study of Environmental Factors Important for Physical Activity in Rural Adults,” PLoS One, vol. 10, no. 11, p. e0140659, Nov. 2015. [CrossRef]
- J. A. Sedrez, M. I. Z. Da Rosa, M. Noll, F. da S. Medeiros, and C. T. Candotti, “Fatores de risco associados a alterações posturais estruturais da coluna vertebral em crianças e adolescentes,” Revista Paulista de Pediatria, vol. 33, no. 1, pp. 72–81, Mar. 2015. [CrossRef]
- M. J. Northgraves, S. C. Hayes, P. Marshall, L. A. Madden, and R. V. Vince, “The test-retest reliability of four functional mobility tests in apparently healthy adults,” Isokinet Exerc Sci, vol. 24, no. 3, pp. 171–179, Aug. 2016. [CrossRef]
- K. Vishal, A. Walkay, H. Teo, V. S. Bhat, and Y. V. R. Neelapala, “The relationship between cervical spine range of motion and postural sway in mechanical neck pain: A cross-sectional study,” Hong Kong Physiotherapy Journal, vol. 43, no. 02, pp. 129–135, Dec. 2023. [CrossRef]
Figure 1.
The results of the correlation between functional and spinal range of motion tests based on departments.
Figure 1.
The results of the correlation between functional and spinal range of motion tests based on departments.
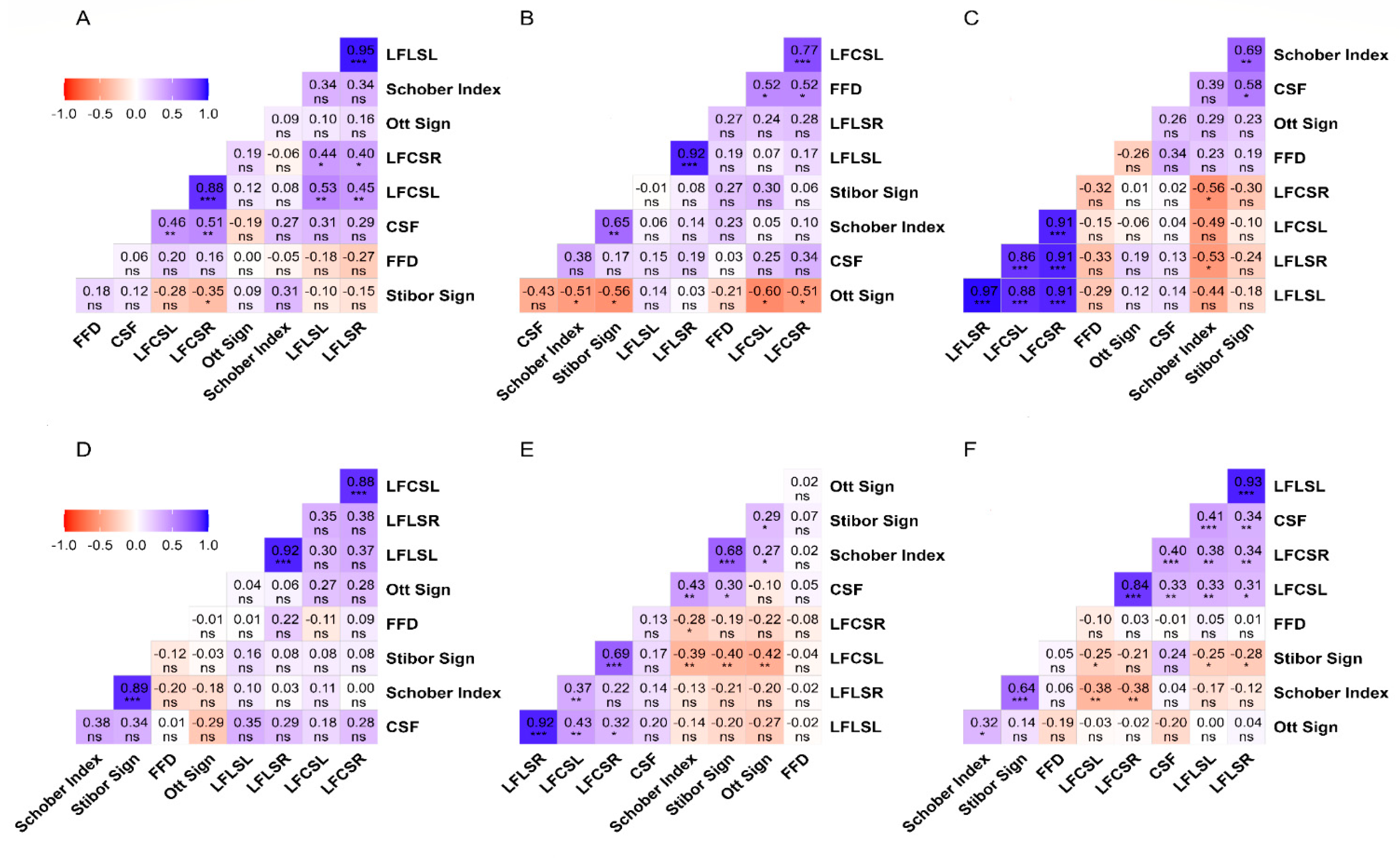
Figure 2.
The results of the correlation between functional and spinal range of motion tests based on lived region.
Figure 2.
The results of the correlation between functional and spinal range of motion tests based on lived region.
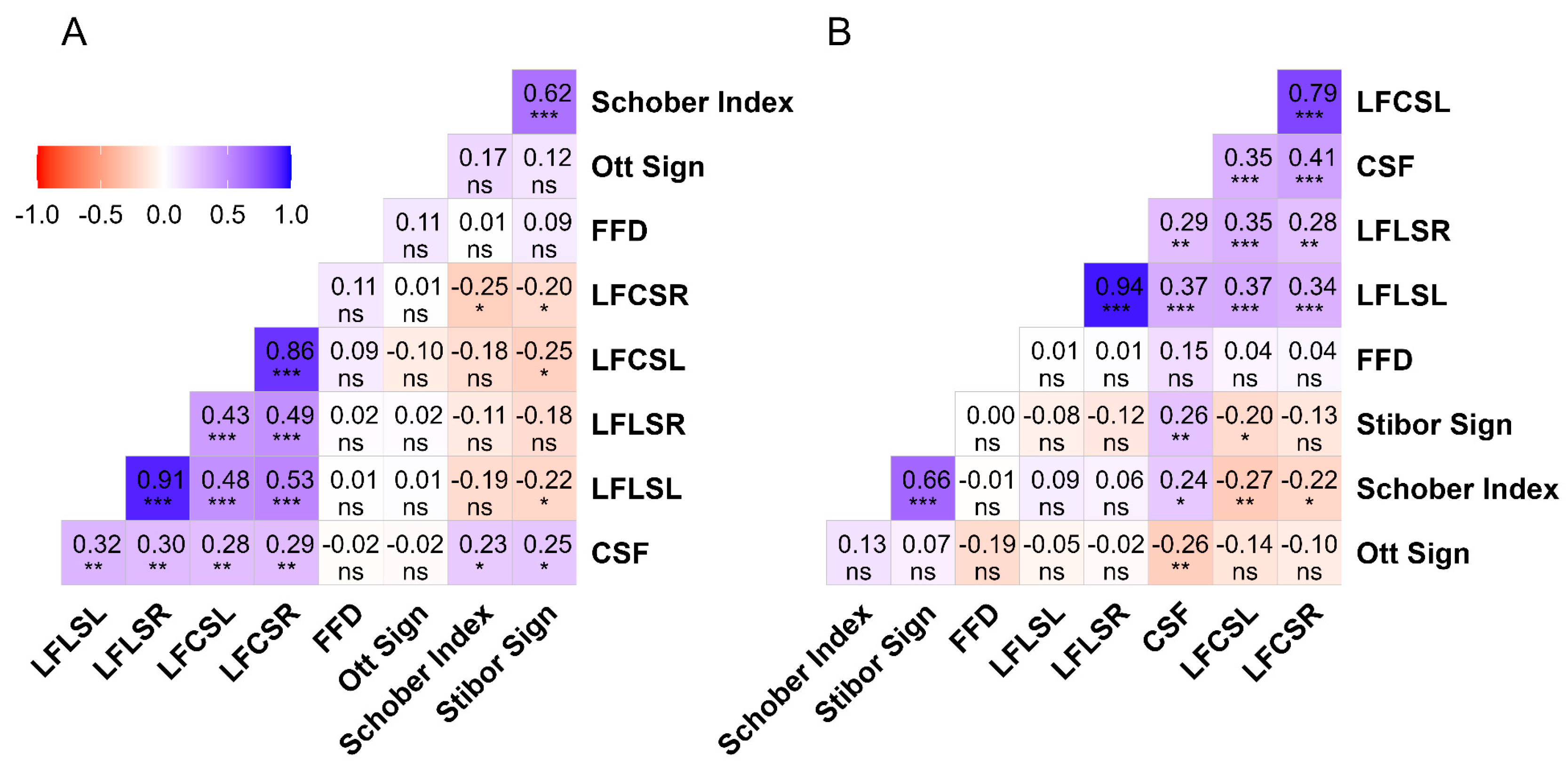
Figure 3.
The results of the correlation between functional and spinal range of motion tests based on sex.
Figure 3.
The results of the correlation between functional and spinal range of motion tests based on sex.
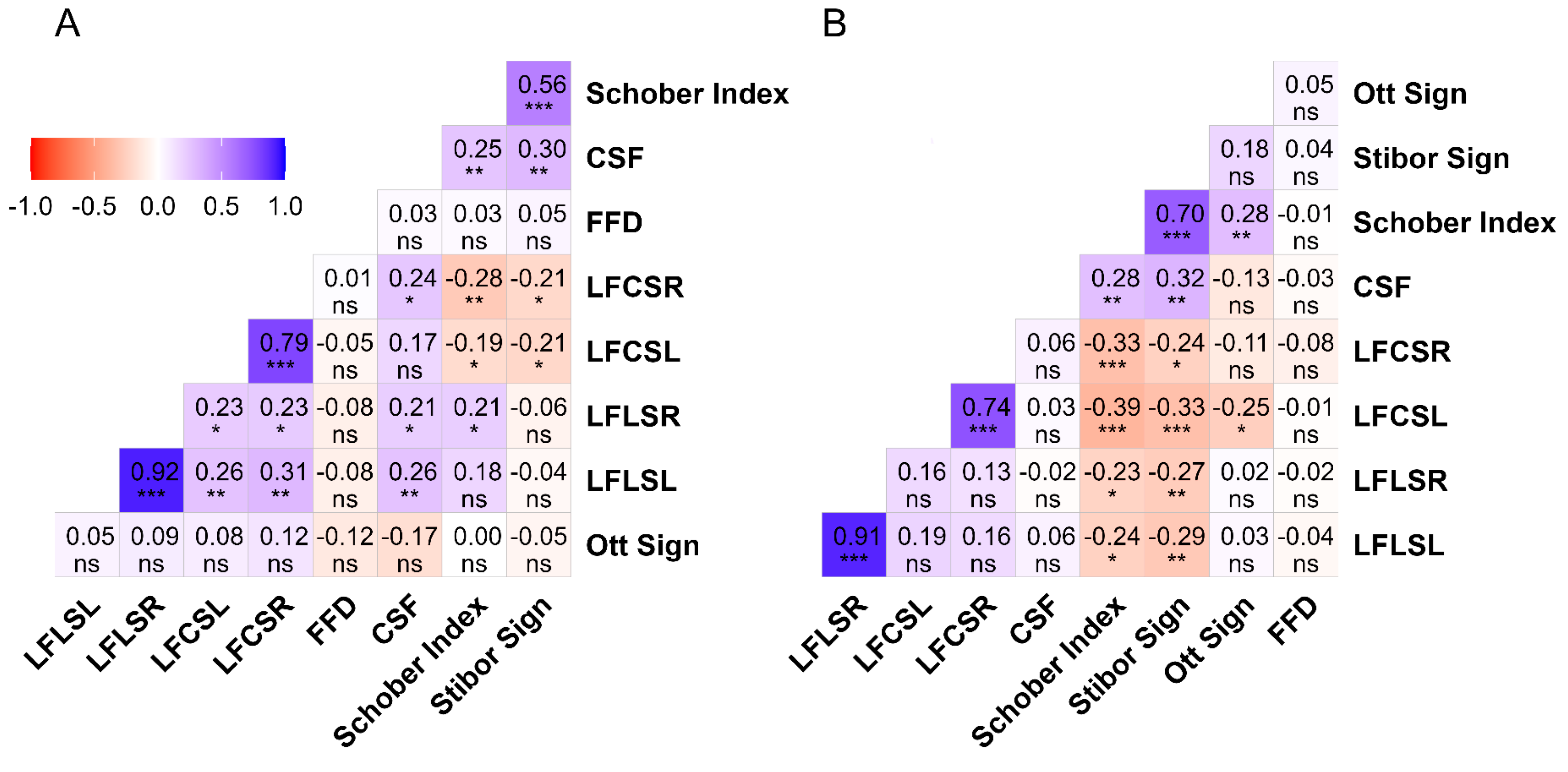
Figure 4.
The results of the correlation between functional and spinal range of motion tests based on the age.
Figure 4.
The results of the correlation between functional and spinal range of motion tests based on the age.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



