
Submitted:
16 April 2024
Posted:
16 April 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
During the coronavirus disease 2019 (COVID-19) pandemic, individuals with immune-mediated inflammatory diseases (IMIDs), such as systemic lupus erythematosus and rheumatoid arthritis, face a heightened risk of infection and severe outcomes due to immunological alterations resulting from their underlying conditions and immunosuppressive treatments. Even as the pandemic has transitioned to an endemic state, it remains crucial to recognize that these patients continue to be at risk. In this narrative review, we analyzed existing literature to explore the impact of IMIDs, clinical risk factors, and the influence of immunosuppressive therapies on COVID-19-related risks and outcomes. Notably, certain disease-modifying antirheumatic drugs (DMARDs), like rituximab, are associated with worse COVID-19 outcomes, and rituximab-treated patients show impaired immune responses to COVID-19 vaccination. Additionally, we outline the diverse effects of glucocorticoids on COVID-19 outcomes and management. To highlight real-life challenges faced by clinicians caring for patients with IMIDs, we present an illustrative scenario that underscores the importance of effective vaccination, timely boosting, and additional mitigation strategies against COVID-19. Given the clinical heterogeneity and diverse disease states within IMIDs, it is crucial to understand the ongoing implications and risks associated with COVID-19 in these patients, to guide the implementation of appropriate measures and optimize care and outcomes in the current endemic era.
Keywords:
COVID-19
; SARS-CoV-2
; DMARDs
; immunocompromised
; immune-mediated inflammatory disease
; rheumatic disease
Introduction
The coronavirus disease 2019 (COVID-19), caused by the SARS-CoV-2 virus, has had a profound global impact, with over 757 million confirmed infections and 6.8 million deaths since the pandemic's onset in 2019 [1,2]. Factors such as age, race, underlying medical conditions, and the use of immunosuppressants have been associated with higher risks of severe COVID-19 [1]. Notably, individuals with immune-mediated inflammatory diseases (IMIDs) are particularly vulnerable to COVID-19. Immunological alterations resulting from their underlying disease and/or the medications used for treatment place them at increased risk of severe outcomes, leading to prolonged hospitalization, higher mortality, and increased healthcare resource utilization [2,3].
Understanding the ongoing implications and risks associated with COVID-19 remains crucial, even as the pandemic has transitioned to an endemic state. While the general population has seen reduced disease severity and mortality with the later Omicron variants compared to earlier variants, patients with IMIDs remain at risk for COVID-19 due to their underlying immunocompromised conditions, regardless of vaccination status [1,2,4]. Moreover, recent data indicate a high prevalence of co-infections between COVID-19 and influenza during flu seasons, with evidence suggesting worse hospitalization outcomes associated with COVID-19 compared to influenza [5,6].
In patients with IMIDs, the use of baseline immunosuppressive therapy such as disease-modifying antirheumatic drugs (DMARDs) has been linked to worse COVID-19 outcomes [7,8,9,10]. Studies have shown that patients receiving biological DMARDs (bDMARDs), targeted synthetic DMARDs (tsDMARDs) and conventional synthetic DMARDs (csDMARDs) experience a greater reduction in antibody titers following SARS-CoV-2 vaccination compared to those receiving other therapies [11].
This narrative review seeks to enhance understanding of COVID-19-related risks and outcomes in patients with IMIDs receiving immunosuppressive therapies. By analyzing existing literature, we identify individuals who are particularly susceptible and offer practical guidance on clinical management and preventive measures in the endemic era. Additionally, an illustrative scenario is presented to demonstrate real-life challenges and offer valuable insights into minimizing COVID-19 risks and adverse outcomes.
Literature Review
Understanding the Effects of IMIDs on Risk of COVID-19
IMIDs are associated with higher risks of infection and poorer outcomes: IMIDs and COVID-19 share common features of cytokine dysregulation and increased expression of proinflammatory cytokines [7]. These mechanisms play a critical role in the host’s defense and response against SARS-CoV-2, and in severe cases, can trigger a cytokine storm, resulting in acute respiratory distress syndrome, multiorgan failure and death [12]. Since the onset of the pandemic, numerous studies and meta-analyses have consistently demonstrated an association between IMIDs and an elevated risk of COVID-19.
Specifically, individuals with rheumatoid arthritis (RA), systemic lupus erythematosus (SLE) and psoriasis face a higher risk of poor COVID-19-related outcomes compared to the general population [10]. A meta-analysis of 23 studies found that patients with rheumatic diseases have a relative risk of 1.52 (95% confidence interval [CI], 1.16–2.00) for SARS-CoV-2 infection compared to the general population [10]. Another meta-analysis conducted across different regions, including Asia, Europe, North America, and South America, reported a high incidence of COVID-19 among patients with rheumatic diseases, with an estimated 44% hospitalization rate and elevated rates of mortality, intensive care unit (ICU) admission, and mechanical ventilation [9].
While early studies suggested a higher risk of hospitalization or death among those with RA or connective tissue disease, these risks became non-significant after adjusting for factors like age, sex and comorbidities [10]. However, a subsequent Danish study found a 46% increased risk of COVID-19 hospitalization in patients with rheumatic diseases compared to the general population, with RA patients showing a significantly elevated risk of severe outcomes (hazard ratio [HR] 1.72; 95% CI, 1.29–2.30).[10] Consistent findings were observed across RA phenotypic subgroups, especially in patients with interstitial lung disease (ILD) [8]. Analyses of the UK health records database OpenSAFELY indicated an increased risk of COVID-19-related death, critical care admission or death, and hospital admissions in people with IMIDs compared to non-IMID individuals of similar demographics [13]. Among IMID individuals, those with inflammatory joint diseases like RA, psoriatic arthritis (PsA) and ankylosing spondylitis faced a greater risk of severe outcomes than those with inflammatory skin or bowel disease [13]. Similarly, studies of patients with SLE reported a significantly increased risk of severe COVID-19 outcomes, including mortality, mechanical ventilation, hospitalization, and ICU admissions compared to matched controls, even when considering the presence of other associated comorbidities [14].
The available evidence aligns with the clinical experience of our expert group, indicating that certain IMIDs, such as SLE, inflammatory conditions like RA, PsA and idiopathic inflammatory bowel disease, other autoinflammatory conditions, and comorbidities associated with metabolic syndrome confer a heightened vulnerability to COVID-19 [15].
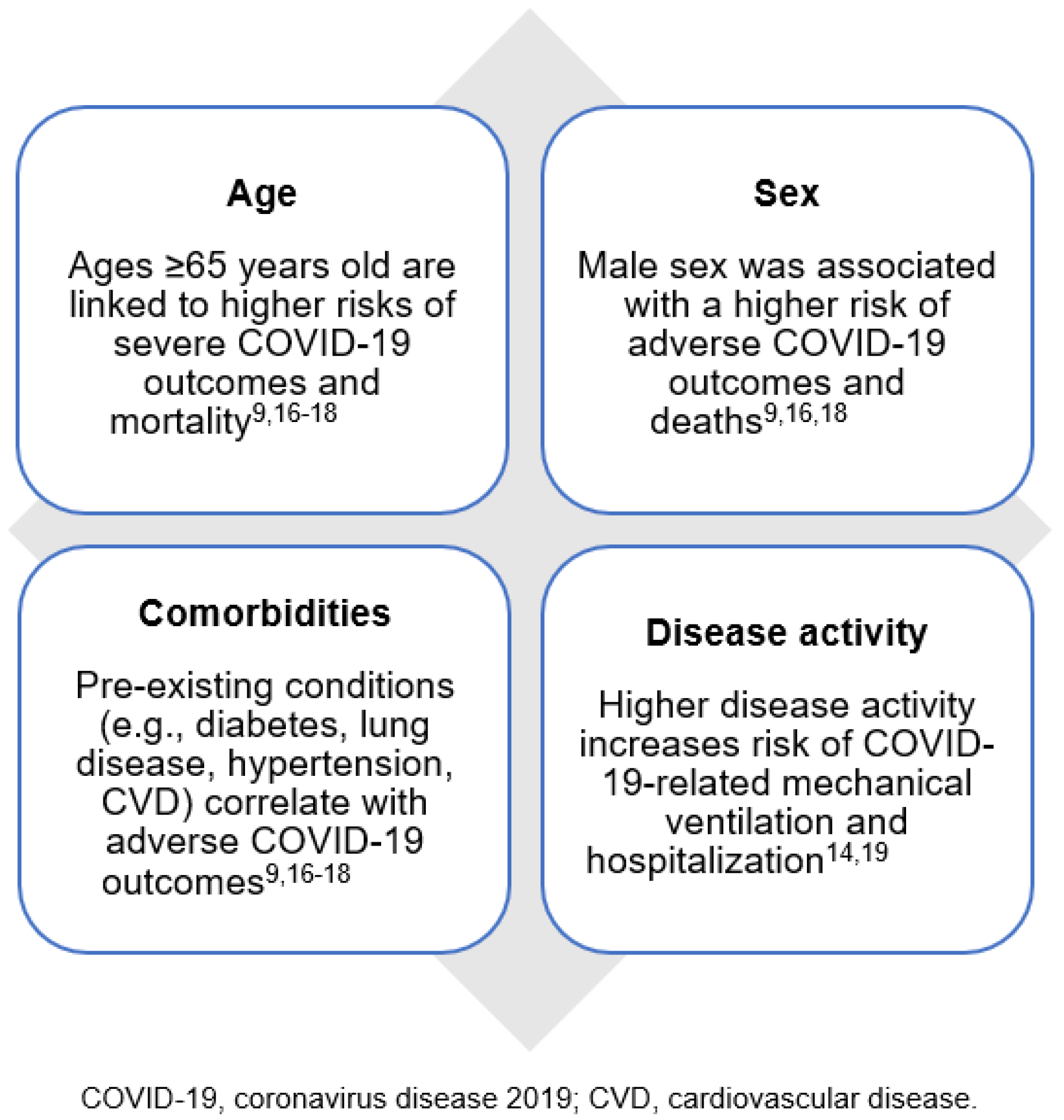
Comorbidities and clinical risk factors linked to COVID-19 outcomes in IMIDs: Certain clinical characteristics, such as age and sex, and comorbid conditions are predictors of poor outcomes in patients with IMIDs (Figure 1), highlighting the varying levels of risk and their correlation with adverse COVID-19 outcomes [9,16,17]. In the UK, 90% of COVID-19-related deaths occurred in people over 60, and 60% in men [16].
In the COVID-19 Global Rheumatology Alliance (C19-GRA) physician-reported registry of adults with rheumatic diseases and COVID-19 in Japan, older age (≥65 years) was associated with a higher risk of severe COVID-19 progression (defined as death or requiring oxygen inhalation) (odds ratio [OR] 3.52; 95% CI, 1.69–7.33) [17]. The likelihood of progression to severe disease, along with rates of mortality and critical disease, increased across age groups [17].
Additionally, comorbidities strongly correlate with adverse COVID-19 outcomes in patients with rheumatic diseases [9,16,17]. In the C19-GRA registry studies, pre-existing conditions like diabetes, lung disease (including chronic obstructive pulmonary disease, asthma and ILD), hypertension, cardiovascular disease, and chronic renal insufficiency were identified as potential risk factors for severe COVID-19 outcomes [17]. These findings align with an analysis of RA patients in a US COVID-19 health record database (Optum®) [18]. Unsurprisingly, higher disease activity in rheumatic patients correlated with higher odds of poor outcomes, including death [19]. In the case of SLE patients, severe disease activity increased the risk of mechanical ventilation (OR 5.83; 95% CI, 2.60–13.07) and hospitalization (OR 3.97; 95% CI, 2.37–6.65) [14].
Figure 1.
Clinical risk factors and patient characteristics associated with poor COVID-19 outcomes in IMIDs.
Figure 1.
Clinical risk factors and patient characteristics associated with poor COVID-19 outcomes in IMIDs.
COVID-19 burden remains high among patients with rheumatic disease during the Omicron era: The Omicron variant, although more transmissible, is associated with milder disease compared to the Delta variant. Factors like reduced social distancing measures, relaxed masking policies, and waning vaccination efficacy have influenced its spread and effect [3]. Emerging data from the Omicron phase provide important insights on the evolving impact of COVID-19 on patients with rheumatic diseases [3].
Real-world data from China during the Omicron wave showed a high COVID-19 infection rate (84.3%) among patients with rheumatic diseases, with a shorter time since last vaccination (<3 months) reducing the risk of hospitalization [20]. Age over 60 years and comorbidities were independent risk factors for hospitalization, while booster vaccinations protected against hospitalization [20]. Interestingly, among rheumatic conditions, RA patients had a lower likelihood of infection, whereas SLE patients tended to have more severe COVID-19 [20].
Reassuringly, recent findings from Israel demonstrated improved outcomes among patients with rheumatic diseases during the Omicron period compared to Delta.[3] Hospitalization and mortality rates decreased markedly from 3.9% to 1.3% and 3.2% to 1.1%, respectively [3]. The study did not find significant differences in hospitalization risks between the Omicron and Delta periods based on rheumatic disease type, comorbidities, or treatments [3]. Similarly, an analysis of a Japanese COVID-19 registry showed a progressive improvement in COVID-19 prognosis among patients with rheumatic disease over time, spanning different periods of onset and dominant SARS-CoV-2 strains [21]. Hypoxemia rates decreased from 34.9% in the earliest period until June 2021 to 6.1% in the Omicron BA.5 period from July to December 2022. Mortality rates also decreased from 5.6% to 0% during the same period.
Overall, these findings suggest progressive improvement in COVID-19 prognosis among patients with rheumatic diseases, potentially due to higher vaccination rates and the milder Omicron variant [3]. However, COVID-19 risks remained elevated for patients with IMIDs compared to the general population due to reduced immune responses to the SARS-CoV-2 vaccine. Their risks of poor COVID-19 outcomes are further influenced by comorbidities and background therapies [3,10,17].
Understanding the Effects of DMARDs on COVID-19 Outcomes in Patients with IMIDs
In patients with IMIDs, the use of immunomodulatory and immunosuppressive therapies is known to increase their vulnerability to viral and bacterial infections [22]. Therapies like glucocorticoids have broad immunosuppressive effects that can impair innate and adaptive immunity against various pathogens [23,24]. Studies consistently show that patients on these therapies, particularly those on methotrexate, anti-CD20 antibody rituximab and mycophenolate mofetil (MMF), exhibit impaired vaccine response to COVID-19 vaccination [24,25,26]. However, certain therapies used in the treatment of IMIDs target proinflammatory cytokines that are induced in COVID-19 [24]. Cytokine inhibitors, as well as b/tsDMARDs targeting interleukin-6 (IL-6) and IL-1, tumor necrosis factor-inhibitors (TNFis) and Janus kinase inhibitors (JAKis) (Figure 2) [16,27,28,29] have shown efficacy in controlling disease activity of IMIDs such as RA [1,12,24]. The impact of b/tsDMARDs on COVID-19 outcomes has received particular interest given the potential of these medications in fighting the cytokine storm syndrome associated with severe COVID-19 [12,30]. While evidence suggests that certain b/tsDMARDs can lower the risk of severe COVID-19 by modulating the immune response, the baseline use of specific b/tsDMARDs like rituximab or abatacept may be associated with worse COVID-19 outcomes due to impaired viral immune defenses [30].
Figure 2.
Overview of immunosuppressive and immunomodulatory therapies indicated for IMIDs.

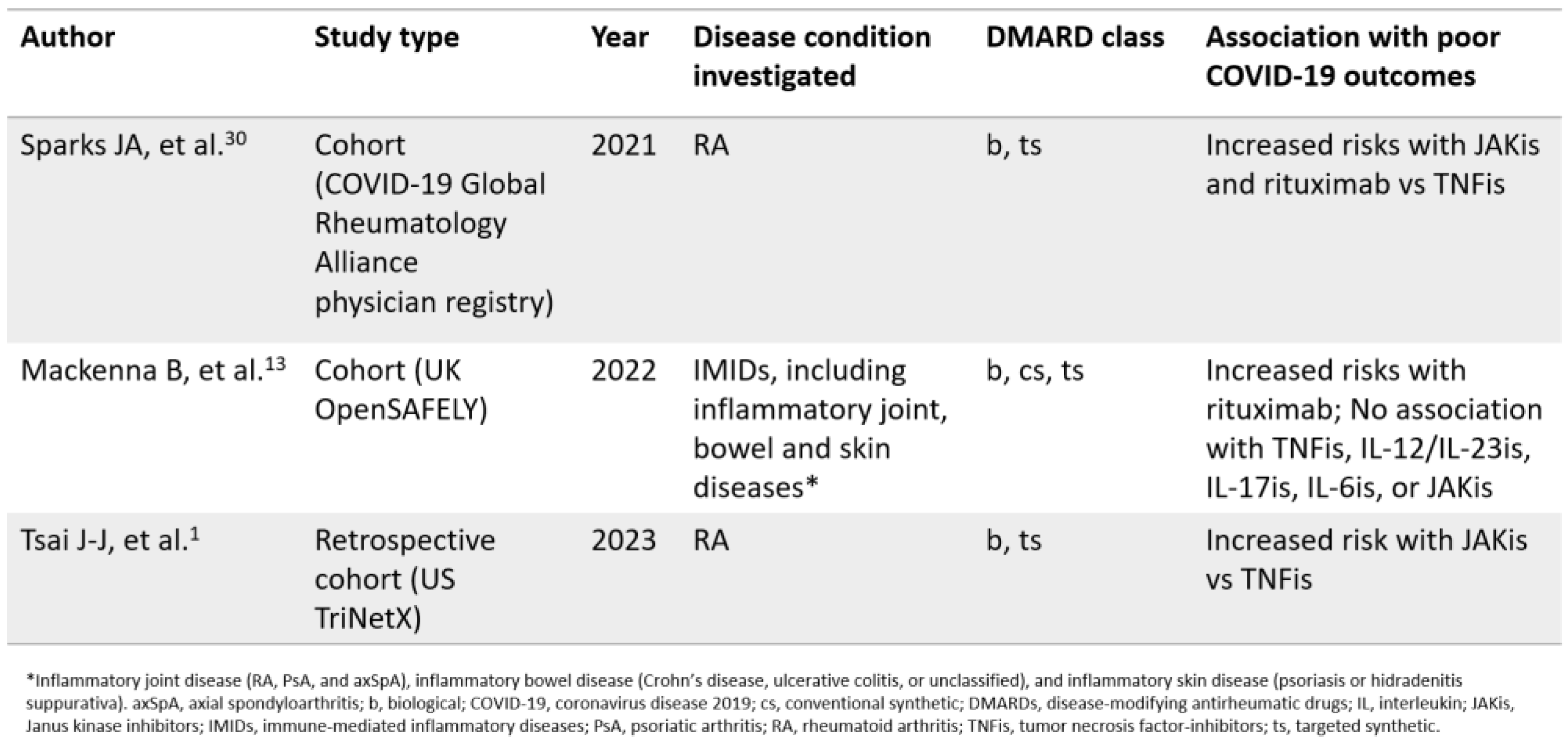
DMARD classes have diverse effects on COVID-19 outcomes: The available evidence highlights the variability in the effects of different DMARD classes on COVID-19 outcomes (Table 1). Studies have shown that, in general, the use of tsDMARDs does not increase the risk of severe COVID-19, with the exceptions of rituximab or JAKis [13], while therapies such as TNFis were found to decrease the risk of severe COVID-19 [1,10,13]. The C19-GRA registry reported that patients receiving JAKis or rituximab prior to COVID-19 had higher odds of poor outcomes compared to those on TNFi therapy [30]. Analysis of the UK OpenSAFELY database, which included over 1 million people with IMIDs, demonstrated that the use of various b/tsDMARDs including TNFis, IL-12/IL-23is, IL-17is, IL-6is, or JAKis did not increase the risk of COVID-19 related death compared to standard systemic therapy [13]. However, rituximab was associated with an increased risk of critical care admission or death.
A real-world study from Taiwan compared outcomes among patients with RA on various b/tsDMARDs, including JAKi, TNFi, and IL-6i, using data from the US Collaborative Network in TriNetX between January 2018 and December 2022 [1]. Compared to TNFi, RA patients on JAKi had a significantly higher risk of hospitalization (HR: 1.194, 95% CI: 1.003 to 1.423), mortality (HR: 1.440, 95% CI: 1.049 to 1.976) and composite adverse outcomes (HR: 1.242, 95% CI: 1.051 to 1.468) [1]. These findings were largely consistent with the C19-GRA registry studies, despite differences in the study period and different dominant variants of concern. Importantly, the study highlighted that the mortality risk tended to be significantly higher in the JAKi group among patients who were not vaccinated against COVID-19 (HR: 1.511, 95% CI: 1.077 to 2.121) [1]. The findings also suggest that the effects of JAKis on COVID-19 outcomes appear to be inconsistent, and there is a possibility that, like glucocorticoids, they may have divergent effects based on the underlying disease, although further confirmation is needed [10].

Table 1.
Summary of findings from large cohort studies comparing effects of DMARD classes on COVID-19 outcomes
Table 1.
Summary of findings from large cohort studies comparing effects of DMARD classes on COVID-19 outcomes
Baseline glucocorticoids negatively impact COVID-19 outcomes: While glucocorticoids have shown benefits when initiated for the treatment of moderate-to-severe COVID-19, they have been associated with worse outcomes among those who are already on baseline glucocorticoids at the time of infection [13,24,30,31]. Notably, patients with SLE on glucocorticoids experienced severe outcomes when infected with COVID-19 [14]. Studies from the C19-GRA registry found that higher dosages of glucocorticoids (≥10 mg/day of prednisolone equivalent) were linked to an increased risk of hospitalization in patients with rheumatic diseases [30,31]. Even doses below 10 mg/day have been associated with an elevated risk of worse outcomes [9,14]. Consensus guidelines by the British Society for Rheumatology identified a corticosteroid dose of ≥20 mg (0.5 mg/kg) prednisolone (or equivalent) per day for more than 4 weeks as posing a very high risk for COVID-19, providing a valuable principle for risk stratification [32]. The existing literature strongly supports our expert group’s real-world observations and experiences regarding the impact of glucocorticoids on COVID-19 outcomes, underscoring the importance of controlling disease activity to reduce baseline glucocorticoid dosage and mitigate the risk of severe COVID-19 [33]. This is particularly crucial for patients with SLE who frequently use glucocorticoids [14].
Impact of rituximab therapy in the context of evolving COVID-19 variants: Rituximab, an anti-CD20 therapy, has been associated with increased susceptibility to other viral infections and poor COVID-19 outcomes in conditions other than rheumatic diseases [10,24]. Given its impact on humoral immunity as a B cell-depleting agent, concerns were raised about the safe use of rituximab during the pandemic [10]. Multiple studies have indicated an increased risk of poor COVID-19-related outcomes, including deaths, in patients with rheumatic diseases treated with rituximab compared to the general population or those on other DMARDs [7,13,34].
Studies conducted during later stages of the pandemic continue to demonstrate the susceptibility of rituximab-treated patients to COVID-19 [34]. Despite high vaccination rates, approximately a third of patients experienced breakthrough SARS-CoV-2 infections while receiving rituximab therapy, but the majority had mild outcomes.[34] The incidence rates of moderate-to-severe COVID-19 were comparable across different SARS-CoV-2 variants (wild-type or Alpha, Delta and Omicron) [34]. Predictors of moderate-to-severe outcomes included an increasing number of comorbidities and hypogammaglobulinemia, while the risk of severe outcomes substantially decreased with each vaccine dose received [34].
These findings suggest that breakthrough SARS-CoV-2 infections were common but mostly mild among rituximab-treated patients during the Omicron phase [34]. Considering the emergence of less severe SARS-CoV-2 variants, increased vaccination rates, reduced social restrictions, and the availability of new therapies, careful consideration is needed when balancing the risks of rituximab treatment against under-treating patients with severe disease, especially when alternative treatment options are limited [34]. Increased vigilance is necessary for patients with comorbidities and low immunoglobulin concentrations [34].
Response to COVID-19 Vaccination in Patients with IMID on DMARDs
The available data indicate that patients with IMIDs, despite generally tolerating SARS-CoV-2 vaccination, are at risk of losing humoral immune protection due to their lower and less enduring response to SARS-CoV-2 vaccination [24,35,36,37]. Research has shown that patients with IMID experienced delayed and reduced responses to SARS-CoV-2 vaccination that appears to be a disease-related effect [11]. Compared to immunocompetent individuals, significantly more patients with IMID failed to develop neutralizing antibodies after vaccination [11]. Furthermore, there is ample evidence indicating that immunosuppressive treatments including cytokine inhibitors can dampen the adaptive immune response to SARS-CoV-2 vaccines [35].
While prioritization for vaccination is crucial for mitigating COVID-19 risks in patients with IMID, the complexity of treatment in this patient group and suboptimal immune responses following vaccination remain a challenge for healthcare professionals. The following sections provide an overview of the current literature related to immunogenicity of patients with IMIDs following COVID-19 vaccination, focusing on different classes of DMARDs and specific indications such as RA, PsA, axial spondyloarthritis (axSpA) and SLE. Understanding the various factors influencing vaccine responses in IMID patients is crucial for guiding clinical practice.
Impaired COVID-19 vaccine response observed in IMID patients: It is well established that individuals with IMIDs respond less favorably to routine vaccinations than healthy adults [38]. Although initial COVID-19 vaccine trials excluded patients with IMIDs, it quickly became evident that following the recommended 2-dose primary series of COVID-19 vaccination, serologic response rates were lower among patients with IMID compared to immunocompetent individuals [38]. A systematic review and meta-analysis reported a pooled seroresponse rate of 83% among all patients with IMIDs and 80% among the subgroup of patients with rheumatic diseases [38]. Patients with rheumatic diseases had lower odds of seroconversion compared to healthy controls (OR, 0.068; 95% CI, 0.016–0.29) [38]. Additional prospective studies also showed reduced seroconversion rates among IMID populations (range, 63%–91%) compared with healthy controls (range, 98%–100%) [38]. Another study assessing humoral, CD4 and CD8 responses after a 2-dose SARS-CoV-2 vaccination demonstrated significantly lower seroconversion rates and cellular immune responses in IMID patients compared to healthy individuals [29]. The diminished vaccine immunogenicity observed in IMID patients may be attributed to intrinsic dysregulation of the immune response associated with the underlying IMRD and/or immunosuppressive therapies.
DMARD class impacts COVID-19 antibody response in IMID patients: Studies have indicated that DMARDs reduced the immune response following COVID-19 vaccination after six weeks [39]. A study investigating the effectiveness of SARS-CoV-2 vaccination in patients with RA on DMARDs reported the lowest seroconversion rates in patients treated with abatacept, rituximab (<6 months from infusion) and those on concomitant methotrexate [40]. These findings align with previous data for rituximab, which showed impaired antibody responses to influenza and pneumococcal vaccines [40]. The impact of abatacept on vaccine response remains uncertain. In the study, no patients treated with abatacept achieved seroconversion after the first dose, but 50% achieved seroconversion after the second dose, likely due to abatacept’s effects on both T and B cells and its known ability to inhibit antibodies [40]. Substantially better seroconversion rates were observed with TNFis versus rituximab and with age ≤50. In terms of T cell responses, individual drugs had limited impact except for a potential effect associated with corticosteroids [40].
Another study involving patients with RA, SpA and inflammatory bowel disease showed that patients receiving b/tsDMARDs had significantly reduced antibody levels and neutralizing antibody titres six months after SARS-CoV-2 vaccination [41]. This reduction was attributed to a faster decline in antibody levels, indicating a significantly reduced duration of vaccination-induced immunity compared with healthy controls or patients receiving csDMARDs [41].Furthermore, there was a reduced response to booster vaccination, highlighting the need for earlier booster vaccination strategies based on specific antibody levels in patients under b/tsDMARD therapy [41]. These findings were supported by data from a Chinese cohort study involving RA patients, which showed that patients treated with bDMARDs, JAKis and prednisone had significantly lower neutralizing antibody titers when compared with healthy controls [42]. However, no significant decrease was observed in RA patients treated with csDMARDs [42].
Altogether, these findings indicate that patients treated with a combination of csDMARD and bDMARD face a higher disease risk than those exclusively on conventional drugs. Moreover, compared to patients not on DMARD treatment, patients treated with any type of DMARD or glucocorticoid at any dose exhibit substantially lower responses to SARS-CoV-2 vaccines [39]. Specifically, glucocorticoids, methotrexate, MMF, TNFis, and B cell-depleting therapy have been identified as posing a risk in attenuating serological responses [43]. However, it is important to note that some data suggest that even in patients on different medications who experienced insufficient seroconversion for neutralizing antibodies and SARS-CoV-2 immunoglobulin G, a second vaccination covered almost all patients, regardless of DMARD therapy [40].
Durability of vaccine response and hybrid immunity during Omicron: In the context of the Omicron wave, it becomes increasingly crucial to understand vaccine response, waning immunity, and the concept of hybrid immunity. Recent data reported that patients with IMID including RA, axSpA and psoriatic disease treated with biologics experienced greater waning of antibody and T cell responses to SARS-CoV-2 three months after the second dose of SARS-CoV-2 vaccine compared to healthy controls [43]. Notably, those receiving TNFi had substantially lower antibody levels and neutralization efficacy against variants of concern, with undetectable levels against Omicron three months after the second dose [43]. Based on these findings, it was concluded that administering a third vaccine dose of SARS-CoV-2 vaccine and continuously monitoring immune responses are critical for patients with IMIDs [43].
In a study involving patients with autoimmune rheumatic diseases who had completed primary series of vaccination, 17.4% experienced an Omicron infection [44]. Those with hybrid immunity (vaccinated individuals with a history of COVID-19 infection) had better protection against breakthrough infections during the Omicron wave compared to those who were only vaccinated [44]. Age and time since the last event (second dose of vaccination or past COVID-19 infection, whichever was later) did not significantly correlate with breakthrough infections. In the hybrid group, the order of infection and vaccination did not affect the risk of breakthrough infections [44]. These real-world findings suggest that hybrid immunity may potentially protect patients with IMIDs against breakthrough infections [44].
Illustrative Scenario: A Patient with Severe Active RA on Multiple cs/bDMARDs
The case presented is for illustrative purposes only and do not represent a specific individual. It is a hypothetical scenario derived from the authors’ collective clinical experience.
Background: A 56-year-old woman was diagnosed with seropositive RA in 2015. Her past medical history includes shingles. Her initial treatment for RA included prednisolone prescribed by her GP. Subsequently, she was started on methotrexate (MTX) at a maximum dosage of 22.5 mg administered subcutaneously. Hydroxychloroquine (HCQ) was added to her regimen, followed by low-dose sulfasalazine, which had to be discontinued due to a rash. Leflunomide was prescribed, but her RA remained refractory to csDMARD treatment. In 2016, she agreed to start golimumab, with HCQ and leflunomide discontinued and a reduction in methotrexate dosage to 10–15 mg weekly. However, her RA activity persisted. After six months on golimumab, in 2017, she switched to rituximab. Taking an active role in her treatment choices, the patient expressed preference to have subsequent rituximab courses administered based on disease activity. Rituximab was given in May 2019, August 2020 and March 2022. During this time, she received a series of COVID-19 vaccinations in April 2021, May 2021, and November 2021.
COVID-19 clinical management: In January 2022, her SARS-CoV-2 neutralizing antibody test returned negative. As a precautionary measure, she received tixagevimab 150 mg plus cilgavimab 150 mg in April 2022. Due to persistent active arthritis, the patient agreed to switch her primary treatment from rituximab to baricitinib in July 2022 while continuing MTX, HCQ and prednisolone. In September 2022, the patient contracted a COVID-19 infection. Although she did not seek treatment for the infection, she opted to discontinue methotrexate while continuing on baricitinib. Her symptoms eventually resolved, with no severe disease manifestations. Antibody testing 2 weeks post infection showed a SARS-CoV-2 neutralizing antibody level of 98% and an anti-S antibody level of 679.7 U/ml. Three months later in December 2022, she was given an additional SARS-CoV-2 vaccine.
Current status: The patient underwent a successful right total knee replacement surgery the following year and is currently managing her RA well with baricitinib, MTX, HCQ, and prednisolone.
Key takeaways: This case highlights the challenges in managing patients with severe RA and the need for a sequential treatment approach involving different cs/bDMARDs due to refractory disease. Despite receiving a series of COVID-19 vaccinations, the patient exhibited a negative SARS-CoV-2 neutralizing antibody titer, consistent with evidence on reduced immunogenicity in this patient population. Pre-exposure prophylaxis (PrEP) with monoclonal antibodies helped mitigate COVID-19-related risk, and the patient experienced only mild symptoms while on DMARD therapy. Post-infection antibody testing revealed a strong immune response likely attributed to natural infection and the effects of PrEP, suggesting potential protection against future SARS-CoV-2 infections. This aligns with existing literature on stronger antibody responses in individuals with prior SARS-CoV-2 infection, regardless of DMARD therapy, suggesting potential protective effects of hybrid immunity.[40,44] This case presents an interesting scenario of severe RA, where despite the challenges in managing the disease, the patient’s risk was effectively managed, and a significant level of protection was achieved through a comprehensive management approach using PrEP, vaccination, and personalized treatment strategies based on COVID-19 clinical severity.
Discussion
The approach to managing COVID-19 in people with rheumatic disease depends on the phase of the disease, whether it is the early viral replication phase or the late hyperinflammatory phase [10]. To guide treatment strategies, the National Institute of Allergy and Infection Diseases (NIAID) has developed an ordinal scale for grading COVID-19 disease severity, providing a framework for appropriate interventions [45]. Expert recommendations from the US National Institutes of Health (NIH), the European Alliance of Associations for Rheumatology (EULAR) and the American College of Rheumatology (ACR) offer evidence-based guidance for managing people with rheumatic disease in the context of COVID-19 [46,47,48,49]. When it comes to patients with IMIDs who are substantially immunosuppressed, it is important to recognize that they may experience prolonged infection, necessitating individualized assessment and treatment approaches [10].Therefore, the management of COVID-19 in patients with IMIDs should consider risk factors for poor outcomes, such as age, comorbidities, immunosuppression, and clinical severity, and proactive monitoring should be implemented for high-risk patients [10].
Therapeutic Strategies for Treatment of COVID-19 in Patients with IMIDs
The development of critical illness in individuals infected with SARS-CoV-2 is associated with a systemic and uncontrolled inflammatory response of the innate and adaptive immune response with the release of a plethora of proinflammatory cytokines, referred to as cytokine storm syndrome [45]. Management of patients who are hospitalized with COVID-19 should be based on the severity of illness, particularly with regard to oxygen requirements and ventilatory status [10]. Patients who do not require oxygen therapy typically do not require specific immunomodulatory or antiviral therapy [10,45]. However, in severe cases including hospitalized patients who require supplemental oxygen, non-invasive, or mechanical ventilation, remdesivir in combination with dexamethasone have shown positive outcomes, and additional immunomodulation with IL-6is such as tocilimzumab and sarilumab and JAKis such as bariticitinib may be beneficial [10,45]. This approach is supported by studies indicating the potential benefit of combination immunosuppressive therapy in reducing disease progression and mortality in certain subsets of patients [10]. In a double-blinded randomized controlled trial, the combination of baricitinib and remdesivir was superior to remdesivir alone in reducing mortality, shortening recovery time, and accelerating clinical improvement [45]. Baricitinib is thought to modulate inflammation and hinder SARS-CoV-2 entry into target cells, thereby reducing viral load and controlling the cytokine storm [50,51,52]. The addition of IL-6is, such as tocilizumab or sarilumab, to glucocorticoid therapy has been shown to decrease mortality in patients experiencing rapid respiratory decompensation in the REMAP-CAP study, and those with high levels of C-reactive protein and oxygen requirements in the RECOVERY study [10]. The NIH and EULAR have subsequently provided updated guidelines on the use of immunomodulatory therapies in COVID-19 management [53,54].
Protecting Patients with IMIDs: Vaccination Recommendations and Additional Considerations
The case scenario described illustrates an example of challenging patients with IMIDs in the real-world setting and highlights the importance of vaccination, timely boosting, and PrEP with monoclonal antibodies as critical strategies to mitigate COVID-19 risks in these vulnerable individuals. Extensive evidence supports the clinical effectiveness of primary and booster vaccinations in protecting high-risk individuals, even in the presence of B-cell depletion [34].
Recently updated ACR guidelines on COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases emphasize optimizing vaccination timing to avoid disease exacerbation or reduced vaccine effectiveness, taking into account concurrent medication and disease activity [55,56]. These guidelines serve as a reminder to prioritize timely vaccination and minimize missed opportunities [55,56]. Adequate disease control and ongoing monitoring of post-acute COVID-19 sequelae are crucial for managing IMIDs, especially in rheumatic diseases associated with altered immunity, either from underlying conditions, comorbidities or the use of immunosuppressive therapies [55,56]. Furthermore, available evidence suggests that the benefits of COVID-19 vaccines outweigh the risks in patients with rheumatic diseases, including the potential for new-onset autoimmune reactions (e.g., anti-RNA antibodies in SLE patients) [55].
COVID-19 vaccination recommendations continue to evolve as experience and knowledge accumulate. Based on the current understanding of COVID-19 vaccines, the administration recommendations are similar to those for routine vaccinations, including ensuring the timely administration of indicated vaccinations [56]. For patients on methotrexate, it is advisable to hold the treatment for two weeks following immunization. Adjustments to treatments such as rituximab, cytokine inhibitors and prednisolone dose ≥20 mg should be made as necessary at the time of vaccination [56].
It is important to note that in certain individuals with IMIDs on immunosuppressive therapies, vaccination alone may not provide sufficient protection against ongoing COVID-19 risk and additional protective measures may be necessary. Our case report highlights the potential use of monoclonal antibodies, such as tixagevimab/cilgavimab (T/C), for individuals with inadequate neutralizing antibody production against SARS-CoV-2 [57]. T/C has been approved for PrEP in adults, reducing the risk of COVID-19 infection by 77% within the first six months after treatment, and is indicated for the treatment of COVID-19 in individuals at increased risk of progressing to severe disease but do not require supplemental oxygen [57]. Monoclonal antibodies, including bamlanivimab plus etesevimab, casirivimab plus imdevimab and sotrovimab, have been indicated for reducing the risk of severe COVID-19 progression [45,57]. Ongoing studies will further inform the clinical utility of monoclonal antibodies in managing the challenges posed by new and emerging SARS-CoV-2 variants of concern [58].
Conclusions and Clinical Implications
Our expert group acknowledges the ongoing risks and impact of COVID-19 on individuals with IMIDs despite the current endemicity. Particularly, patients undergoing immunosuppressive therapies, including glucocorticoids and DMARDs, may experience diminished immune responses following SARS-CoV-2 vaccination, increasing their susceptibility to the virus. Furthermore, there is data indicating that COVID-19 can impact the disease course of IMIDs, leading to treatment interruption, risk of disease flares, and new onset autoimmune diseases, underscoring the lasting consequences of COVID-19 on the quality of life and underlying conditions of IMID patients.
Considering the clinical heterogeneity and diverse disease states within IMIDs, our expert opinion emphasizes the importance of a pragmatic approach to patient evaluation. This approach involves considering key factors to identify individuals at higher risk and implementing personalized measures accordingly. These factors encompass assessing whether the underlying IMID is associated with an increased risk of COVID-19, evaluating the patient's current treatment regimen, including any immunosuppressive therapies. Additionally, it is crucial to take into account specific patient factors such as age, comorbidities, vaccination status, and adherence to protective measures such as PrEP and social distancing. Adjustments to the patient's ongoing disease management should be made to optimize both COVID-19 protection and IMID control during the endemic phase. Continuous research and vigilance are essential to enhance our understanding and continually optimize care for this vulnerable population.
Funding
Funding for this manuscript was provided by AstraZeneca for medical writing support to summarize the existing literature and develop draft visuals for review and interpretation by the authors.
Acknowledgment
The authors wish to thank Hennis Tung of GCI Health for writing of the manuscript, and Glen Halliwell, Manuel von Osten, and Samantha Chua of GCI Health for literature review, data analysis, data visualizations, and editorial input.
Conflicts of interest/Competing interests
Following the International Committee of Medical Journal Editors’ (ICMJE) guidelines, Nguyen Chau Tuan and Cao Thanh Ngoc have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants, or patents received or pending, or royalties. Pinyo Rattanaumpawan reports receiving research grants, honoraria and travel grants from AstraZeneca and Pfizer. Yee-Chun Chen is the President of the Infection Control Society of Taiwan, a board member of both Infectious Diseases Society of Taiwan and Taiwan Society of Virology and Vaccinology, and a committee member of ACIP, Taiwan. Ahlam Al Marzooqi reports receiving consulting fees from AstraZeneca. Kong Kok Ooi reports receiving payment or honoraria for lectures and presentations, from Boehringer Ingelheim Singapore, GSK, AstraZeneca and Novartis. He has also received payment for his expert testimony from Singapore Medical Council and Ministry of Health Singapore.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
Not applicable.
Code availability
Not applicable.
Authors’ contribution
The authors confirm their contribution to the paper as follows: Kong Kok Ooi, Pinyo Rattanaumpawan, Nguyen Chau Tuan, Cao Thanh Ngoc, Yee-Chun Chen, Ahlam Al Marzooqi contributed to conception and design, acquisition, analysis and interpretation of data; provided critical feedback and inputs for important intellectual content; and provided final approval of the version to be published. Kong Kok Ooi contributed to the hypothetical case scenario development.
References
- Tsai J-J, Liu L-T, Chen C-H, Chen L-J, Wang S-I, Wei JC-C. COVID-19 outcomes in patients with rheumatoid arthritis with biologic or targeted synthetic DMARDs. RMD Open. 2023;9:e003038.
- Ketkar A, Willey V, Pollack M, Glasser L, Dobie C, Wenziger C, et al. Assessing the risk and costs of COVID-19 in immunocompromised populations in a large United States commercial insurance health plan: the EPOCH-US Study. Current Medical Research and Opinion. 2023;0:1–16.
- Bieber A, Brikman S, Novack L, Ayalon S, Abu-Shakra M, Zeller L, et al. SARS-CoV-2 infection among patients with autoimmune rheumatic diseases; comparison between the Delta and Omicron waves in Israel. Semin Arthritis Rheum. 2023;58:152129.
- Barnes E, Goodyear CS, Willicombe M, Gaskell C, Siebert S, I de Silva T, et al. SARS-CoV-2-specific immune responses and clinical outcomes after COVID-19 vaccination in patients with immune-suppressive disease. Nat Med. 2023;29:1760–74.
- Tang CY, Boftsi M, Staudt L, McElroy JA, Li T, Duong S, et al. SARS-CoV-2 and influenza co-infection: A cross-sectional study in central Missouri during the 2021–2022 influenza season. Virology. 2022;576:105–10.
- Chu RBH, Zhao S, Zhang JZ, Chan KCK, Ng PY, Chan C, et al. Comparison of COVID-19 with influenza A in the ICU: a territory-wide, retrospective, propensity matched cohort on mortality and length of stay. BMJ Open. 2023;13:e067101.
- Alhowaish TS, Alhamadh MS, Alhabeeb AY, Aldosari SF, Masuadi E, Alrashid A. Outcomes of COVID-19 in Inflammatory Rheumatic Diseases: A Retrospective Cohort Study. Cureus. 2022;14:e26343.
- Figueroa-Parra G, Gilbert EL, Valenzuela-Almada MO, Vallejo S, Neville MR, Patel NJ, et al. Risk of severe COVID-19 outcomes associated with rheumatoid arthritis and phenotypic subgroups: a retrospective, comparative, multicentre cohort study. Lancet Rheumatol. 2022;4:e765–74.
- Wang F, Ma Y, Xu S, Liu H, Chen Y, Yang H, et al. Prevalence and risk of COVID-19 in patients with rheumatic diseases: a systematic review and meta-analysis. Clin Rheumatol. 2022;41:2213–23.
- Grainger R, Kim AHJ, Conway R, Yazdany J, Robinson PC. COVID-19 in people with rheumatic diseases: risks, outcomes, treatment considerations. Nat Rev Rheumatol. 2022;18:191–204.
- Simon D, Tascilar K, Fagni F, Krönke G, Kleyer A, Meder C, et al. SARS-CoV-2 vaccination responses in untreated, conventionally treated and anticytokine-treated patients with immune-mediated inflammatory diseases. Ann Rheum Dis. 2021;80:1312–6.
- Ruscitti P, Conforti A, Cipriani P, Giacomelli R, Tasso M, Costa L, et al. Pathogenic implications, incidence, and outcomes of COVID-19 in autoimmune inflammatory joint diseases and autoinflammatory disorders. Adv Rheumatol. 2021;61:45.
- MacKenna B, Kennedy NA, Mehrkar A, Rowan A, Galloway J, Matthewman J, et al. Risk of severe COVID-19 outcomes associated with immune-mediated inflammatory diseases and immune-modifying therapies: a nationwide cohort study in the OpenSAFELY platform. The Lancet Rheumatology. 2022;4:e490–506.
- Bruera S, Lei X, Zhao H, Yazdany J, Chavez-MacGregor M, Giordano SH, et al. Risks of mortality and severe coronavirus disease 19 (COVID-19) outcomes in patients with or without systemic lupus erythematosus. Lupus Sci Med. 2023;10:e000750.
- Chang R, Yen-Ting Chen T, Wang S-I, Hung Y-M, Chen H-Y, Wei C-CJ. Risk of autoimmune diseases in patients with COVID-19: A retrospective cohort study. eClinicalMedicine. 2023;56:101783.
- Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584:430–6.
- Kihara M, Sugihara T, Asano J, Sato M, Kaneko H, Muraoka S, et al. Clinical characteristics of COVID-19 patients with underlying rheumatic diseases in Japan: data from a multicenter observational study using the COVID-19 Global Rheumatology Alliance physician-reported registry. Clin Rheumatol. 2022;41:3661–73.
- Ye Y, Yue X, Krueger WS, Wegrzyn LR, Maniccia AW, Winthrop KL, et al. Factors Associated with Severe COVID-19 Among Patients with Rheumatoid Arthritis: A Large, Nationwide Electronic Health Record Cohort Study in the United States. Adv Ther. 2023;40:3723–38.
- Strangfeld A, Schäfer M, Gianfrancesco MA, Lawson-Tovey S, Liew JW, Ljung L, et al. Factors associated with COVID-19-related death in people with rheumatic diseases: results from the COVID-19 Global Rheumatology Alliance physician-reported registry. Annals of the Rheumatic Diseases. 2021;80:930–42.
- Geng Y, Fan Y, Deng X, Wang Y, Zhao J, Ji L, et al. The Recent Outbreak of COVID-19 in China During the Omicron Variant Predominance: Clinical Features and Outcomes in Patients with Autoimmune Inflammatory Rheumatic Diseases. Rheumatol Ther. 2023;10:1039–53.
- Kashiwado Y, Kimoto Y, Oku K, Yamamoto M, Ohshima S, Ito S, et al. Prognostic improvement and treatment of COVID-19 in patients with rheumatic diseases until December 2022: Analysis of the JCR COVID-19 registry in Japan. Modern Rheumatology. 2023;road057.
- Montero F, Martínez-Barrio J, Serrano-Benavente B, González T, Rivera J, Molina Collada J, et al. Coronavirus disease 2019 (COVID-19) in autoimmune and inflammatory conditions: clinical characteristics of poor outcomes. Rheumatol Int. 2020;40:1593–8.
- Hsu C-Y, Ko C-H, Wang J-L, Hsu T-C, Lin C-Y. Comparing the burdens of opportunistic infections among patients with systemic rheumatic diseases: a nationally representative cohort study. Arthritis Res Ther. 2019;21:211.
- Fagni F, Simon D, Tascilar K, Schoenau V, Sticherling M, Neurath MF, et al. COVID-19 and immune-mediated inflammatory diseases: effect of disease and treatment on COVID-19 outcomes and vaccine responses. Lancet Rheumatol. 2021;3:e724–36.
- Petri M, Joyce D, Haag K, Fava A, Goldman DW, Zhong D, et al. Effect of Systemic Lupus Erythematosus and Immunosuppressive Agents on COVID-19 Vaccination Antibody Response. Arthritis Care & Research. 2023;75:1878–85.
- Meunier L, Sanavio M, Dumortier J, Meszaros M, Faure S, Ursic Bedoya J, et al. Mycophenolate mofetil decreases humoral responses to three doses of SARS-CoV-2 vaccine in liver transplant recipients. Liver Int. 2022;42:1872–8.
- Fraenkel L, Bathon JM, England BR, St Clair EW, Arayssi T, Carandang K, et al. 2021 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis. Arthritis Rheumatol. 2021;73:1108–23.
- Di Iorio M, Cook CE, Vanni KMM, Patel NJ, D’Silva KM, Fu X, et al. DMARD disruption, rheumatic disease flare, and prolonged COVID-19 symptom duration after acute COVID-19 among patients with rheumatic disease: A prospective study. Semin Arthritis Rheum. 2022;55:152025.
- Sieiro Santos C, Calleja Antolin S, Moriano Morales C, Garcia Herrero J, Diez Alvarez E, Ramos Ortega F, et al. Immune responses to mRNA vaccines against SARS-CoV-2 in patients with immune-mediated inflammatory rheumatic diseases. RMD Open. 2022;8:e001898.
- Sparks JA, Wallace ZS, Seet AM, Gianfrancesco MA, Izadi Z, Hyrich KL, et al. Associations of baseline use of biologic or targeted synthetic DMARDs with COVID-19 severity in rheumatoid arthritis: Results from the COVID-19 Global Rheumatology Alliance physician registry. Ann Rheum Dis. 2021;annrheumdis-2021-220418.
- Gianfrancesco M, Hyrich KL, Al-Adely S, Carmona L, Danila MI, Gossec L, et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: data from the COVID-19 Global Rheumatology Alliance physician-reported registry. Annals of the Rheumatic Diseases. 2020;79:859–66.
- Price E, MacPhie E, Kay L, Lanyon P, Griffiths B, Holroyd C, et al. Identifying rheumatic disease patients at high risk and requiring shielding during the COVID-19 pandemic. Clin Med (Lond). 2020;20:256–61.
- Hasseli R, Mueller-Ladner U, Hoyer BF, Krause A, Lorenz H-M, Pfeil A, et al. Older age, comorbidity, glucocorticoid use and disease activity are risk factors for COVID-19 hospitalisation in patients with inflammatory rheumatic and musculoskeletal diseases. RMD Open. 2021;7:e001464.
- Md Yusof MY, Arnold J, Saleem B, Vandevelde C, Dass S, Savic S, et al. Breakthrough SARS-CoV-2 infections and prediction of moderate-to-severe outcomes during rituximab therapy in patients with rheumatic and musculoskeletal diseases in the UK: a single-centre cohort study. Lancet Rheumatol. 2023;5:e88–98.
- Simon D, Tascilar K, Kleyer A, Fagni F, Krönke G, Meder C, et al. Impact of Cytokine Inhibitor Therapy on the Prevalence, Seroconversion Rate, and Longevity of the Humoral Immune Response Against SARS-CoV-2 in an Unvaccinated Cohort. Arthritis Rheumatol. 2022;74:783–90.
- Widdifield J, Kwong JC, Chen S, Eder L, Benchimol EI, Kaplan GG, et al. Vaccine effectiveness against SARS-CoV-2 infection and severe outcomes among individuals with immune-mediated inflammatory diseases tested between March 1 and Nov 22, 2021, in Ontario, Canada: a population-based analysis. Lancet Rheumatol. 2022;4:e430–40.
- Frey S, Chiang TP-Y, Connolly CM, Teles M, Alejo JL, Boyarsky BJ, et al. Antibody durability 6 months after two doses of SARS-CoV-2 mRNA vaccines in patients with rheumatic and musculoskeletal disease. Lancet Rheumatol. 2022;4:e241–3.
- Finckh A, Ciurea A, Raptis CE, Rubbert-Roth A. Susceptibility to COVID-19 and Immunologic Response to Vaccination in Patients With Immune-Mediated Inflammatory Diseases. J Infect Dis. 2023;228:S13–23.
- Schreiber K, Graversgaard C, Petersen R, Jakobsen H, Bojesen AB, Krogh NS, et al. Reduced Humoral Response of SARS-CoV-2 Antibodies following Vaccination in Patients with Inflammatory Rheumatic Diseases-An Interim Report from a Danish Prospective Cohort Study. Vaccines (Basel). 2021;10:35.
- Saleem B, Ross RL, Bissell L-A, Aslam A, Mankia K, Duquenne L, et al. Effectiveness of SARS-CoV-2 vaccination in patients with rheumatoid arthritis (RA) on DMARDs: as determined by antibody and T cell responses. RMD Open. 2022;8:e002050.
- Tobudic S, Simader E, Deimel T, Straub J, Kartnig F, Heinz LX, et al. The accelerated waning of immunity and reduced effect of booster in patients treated with bDMARD and tsDMARD after SARS-CoV-2 mRNA vaccination. Frontiers in Medicine [Internet]. 2023 [cited 2023 Jun 7];10. Available from: https://www.frontiersin.org/articles/10.3389/fmed.2023.1049157.
- Zhao T, Wang B, Shen J, Wei Y, Zhu Y, Tian X, et al. Third dose of anti-SARS-CoV-2 inactivated vaccine for patients with RA: Focusing on immunogenicity and effects of RA drugs. Front Med (Lausanne). 2022;9:978272.
- Dayam RM, Law JC, Goetgebuer RL, Chao GYC, Abe KT, Sutton M, et al. Accelerated waning of immunity to SARS-CoV-2 mRNA vaccines in patients with immune-mediated inflammatory diseases. JCI Insight [Internet]. 2022 [cited 2023 Aug 9];7. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9220925/.
- Benny L, Mehta P, Ahmed S, Paul A, Sukumaran A, Mohanan M, et al. Correlates of breakthrough Omicron (B.1.1.529) infections in a prospective cohort of vaccinated patients with rheumatic diseases. Rheumatol Int. 2023;43:1033–9.
- Drosos AA, Pelechas E, Voulgari PV. Treatment strategies of COVID-19: A rheumatology perspective. Eur J Intern Med. 2022;102:17–23.
- Clinical Spectrum [Internet]. COVID-19 Treatment Guidelines. [cited 2023 Aug 24]. Available from: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/.
- Nonhospitalized Adults: Therapeutic Management [Internet]. COVID-19 Treatment Guidelines. [cited 2023 Aug 24]. Available from: https://www.covid19treatmentguidelines.nih.gov/management/clinical-management-of-adults/nonhospitalized-adults--therapeutic-management/.
- Mikuls TR, Johnson SR, Fraenkel L, Arasaratnam RJ, Baden LR, Bermas BL, et al. American College of Rheumatology Guidance for the Management of Rheumatic Disease in Adult Patients During the COVID-19 Pandemic: Version 3. Arthritis Rheumatol. 2021;73:e1–12.
- Landewé RB, Machado PM, Kroon F, Bijlsma HW, Burmester GR, Carmona L, et al. EULAR provisional recommendations for the management of rheumatic and musculoskeletal diseases in the context of SARS-CoV-2. Ann Rheum Dis. 2020;79:851–8.
- Zhang X, Zhang Y, Qiao W, Zhang J, Qi Z. Baricitinib, a drug with potential effect to prevent SARS-COV-2 from entering target cells and control cytokine storm induced by COVID-19. Int Immunopharmacol. 2020;86:106749.
- Gómez RI, Méndez R, Palanques-Pastor T, Ballesta-López O, Almenar CB, Vericat JEM, et al. Baricitinib against severe COVID-19: effectiveness and safety in hospitalised pretreated patients. Eur J Hosp Pharm. 2022;29:e41–5.
- Costanzo G, Cordeddu W, Chessa L, Del Giacco S, Firinu D. COVID-19: Considerations about immune suppression and biologicals at the time of SARS-CoV-2 pandemic. World J Clin Cases. 2021;9:5352–7.
- Alunno A, Najm A, Machado PM, Bertheussen H, Burmester G-RR, Carubbi F, et al. 2021 update of the EULAR points to consider on the use of immunomodulatory therapies in COVID-19. Ann Rheum Dis. 2022;81:34–40.
- Information on COVID-19 Treatment, Prevention and Research [Internet]. COVID-19 Treatment Guidelines. [cited 2023 Aug 25]. Available from: https://www.covid19treatmentguidelines.nih.gov/.
- Curtis JR, Johnson SR, Anthony DD, Arasaratnam RJ, Baden LR, Bass AR, et al. American College of Rheumatology Guidance for COVID-19 Vaccination in Patients With Rheumatic and Musculoskeletal Diseases: Version 5. Arthritis Rheumatol. 2023;75:E1–16.
- Guideline Update: ACR Advises on Vaccinations for Patients with Rheumatic Diseases [Internet]. 2023 [cited 2023 Aug 25]. Available from: https://www.practicalpainmanagement.com/resources/clinical-practice-guidelines/acr-advises-vaccinations-patients-with-rheumatic-disease.
- Bellino S. COVID-19 treatments approved in the European Union and clinical recommendations for the management of non-hospitalized and hospitalized patients. Ann Med. 54:2856–60.
- AstraZeneca. A Phase I/III Randomized, Double Blind Study to Evaluate the Safety, Efficacy and Neutralizing Activity of AZD5156/AZD3152 for Pre Exposure Prophylaxis of COVID 19 in Participants With Conditions Causing Immune Impairment. Sub-study: Phase II Open Label Sub-study to Evaluate the Safety, PK, and Neutralizing Activity of AZD3152 for Pre-exposure Prophylaxis of COVID-19 [Internet]. clinicaltrials.gov; 2023 Jun. Report No.: NCT05648110. Available from: https://clinicaltrials.gov/study/NCT05648110.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



