
Submitted:
16 April 2024
Posted:
17 April 2024
You are already at the latest version
Abstract
This article explores the emerging concept of atrial myopathy (AM) and its potential role as a risk factor for stroke and dementia, both independently and in association with atrial fibrillation (AF). AM refers to structural and functional abnormalities of the atria, potentially causing blood clots formation and their subsequent embolization even in patients without AF. Echocardiography, particularly Left Atrial (LA) strain analysis, is a promising non-invasive tool for AM evaluation and might offer additional risk stratification beyond the established CHADS2-VASc score, potentially impacting anticoagulation decisions. By understanding AM and utilizing advanced imaging techniques like LA strain, clinicians can achieve a more comprehensive understanding of thromboembolic risk in specific patient groups. Integrating LA strain analysis into routine clinical practice holds promise for improved patient management and targeted therapies, allowing for better risk stratification in AF patients. However, standardized definitions and diagnostic criteria for AM are essential for consistent evaluation and research. Further studies are needed to explore the efficacy and safety of anticoagulation in AM patients without AF.
Keywords:
Atrial fibrillation
; Atrial myopathy
; left atrial strain
1. Introduction
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia among adults, and it is associated with significant morbidity and mortality, including increased risk of stroke and dementia. While the established paradigm attributes these complications to blood stasis within the atria and subsequent thrombus formation with cerebral embolization, recent evidence suggests a key role for atrial myopathy (AM).
AM is characterized by structural and functional abnormalities of the atria, which can occur with or without AF. The study of left atrial (LA) deformation with 2D speckle tracking echocardiography, which measures the ability of the LA to contract and relax, has demonstrated high sensitivity and specificity in identifying myocardial fibrosis and increased atrial stiffness, both markers of AM. Recently, different studies have shown that LA strain can be used to stratify the risk of stroke and dementia, even in patients who do not have AF, suggesting that LA strain alterations, reflecting the presence of underlying AM, may be a more sensitive risk stratifier of thromboembolic events than the presence of AF itself. By exploring these aspects, this article aims to provide a comprehensive understanding of the emerging role of AM in AF-related complications and its potential to refine risk stratification and patient management strategies.
2. Atrial Fibrillation: The Size of the Problem
AF is a supraventricular tachyarrhythmia characterized by an incoordinate atrial electrical activation and consequently ineffective atrial contraction. Electrocardiographic (ECG) characteristics of AF include:
- -
- Irregular R-R intervals (when atrioventricular conduction is not impaired)
- -
- Absence of distinct repeating P waves
- -
- Irregular atrial activations. [1]
AF is the most frequently sustained cardiac arrhythmia among adults [2], with estimated prevalence of 0.4–1% in the general population which increases with age, affecting 9% of people above 80 years. [3] The symptoms associated with AF are heterogeneous, as it may vary from asymptomatic AF incidentally diagnosed during a routine ECG, to highly symptomatic form which manifests through chest pain, shortness of breath, syncope, palpitations, or even stroke or transient ischemic attack (TIA). A diagnosis of AF is associated with a 1.5 to 2-fold increased risk of all-cause mortality and increased morbidity in the general population [4] and diminished quality of life [5] particularly due to higher risk of ischemic stroke and dementia. [6]
3. Pathophysiological Pathway of Atrial Fibrillation
Significant effort has been made over the years to define the underlying cellular, molecular and electrophysiological changes that predispose to the occurrence and maintenance of AF in patients. [7] Progress has been limited by the understanding that AF is a complex arrhythmia that can be the final result of various different pathophysiological processes, with significant heterogeneity between patients. [7] Age is a prominent AF risk factor, but there is an increasing burden of other comorbidities including hypertension, diabetes mellitus, heart failure (HF), coronary artery disease (CAD), chronic kidney disease, [8] obesity, and obstructive sleep apnoea, [9,10,11,12,13] which are all potent contributors to AF development and progression to persistence AF. [14,15]
The development of AF and its lifetime risk depends on age, genetic, and (sub)clinical factors. [16,17,18] The impact of clinical risk factor burden and multiple comorbidities on AF suggests that an early intervention and optimum risk factors control could reduce the incidence of AF.
The mechanism that this risk factors potentially share is the capability to induce atrial electrical and structural remodeling. Electrical remodeling encompasses changes in the properties of ion channels affecting atrial myocardial depolarisation and conduction, while structural remodeling refers to alterations in the tissue architecture, both microscopic (eg, myocardial fibrosis) and macroscopic (eg, atrial dilatation). At this point, the initiation and maintenance of AF can be linked to the interaction between a trigger and the substrate. A ‘trigger’ is a rapidly firing focus that can act as an initiator of the arrhythmia, the maintenance of which generally requires a ‘remodeled substrate’, that is, altered electrophysiological, mechanical and anatomical characteristics of the atria that sustain AF.
It is thought that there is a progression over time from a trigger-driven disease, through to development of an atrial function substrate, followed by predominant atrial structural remodeling. [8] This would correspond to the clinical observation that AF is often initially paroxysmal, before progressing to a persistent and ultimately permanent form of arrhythmia. [19]
4. Association between AF, Stroke/TIA and Dementia - The Emerging Concept of Atrial Myopathy
The presence of AF is associated with a fivefold increased risk of stroke, in fact TIA or ischemic stroke represents the first manifestation of AF in 2-5% of patients. [6] This is usually attributed to LA appendage thrombi formation as a result of blood stasis, with subsequent clot dislodgement and embolization to the systemic circulation, more often to the brain, and frequently after restoration of sinus rhythm.
Furthermore, an independent correlation between AF and various forms of dementia, including Alzheimer disease, has been observed in AF population, irrespective of stroke occurrence. [20,21] The pathophysiology is thus likely to be multifactorial which has not been fully explained. [20] One plausible mechanism may be repetitive microclots/macroclots embolization, chronically leading to brain dysfunction. Studies supporting this hypothesis showed a reduction in the incidence of dementia in AF patients treated with optimum anticoagulation [22,23], or in patients undergoing effective and early AF ablation. [24,25] This would suggest a shared pathophysiology for dementia and stroke/TIA as connected to the atrial disease. The complexity of the mechanism by which these morbidities result from AF has yet to be completely understood, in particular the interaction of various factors involved in thrombus formation which should allow better clinical risk stratification and optimum targeted therapies in these patients.
It is well known that the increased risk of pathological thrombus formation is due to an alteration of the physiological haemostatic mechanisms, known as Virchow’s triad, which consist of the combination of alterated blood constituents (including platelet factor 4, von Willebrand factor, fibrinogen, β-thromboglobulin and D-dimer), blood vessel wall disease and reduced blood flow. The occurrence of AF has been shown to be related to all of the Virchow’s triad components. Specifically, the increased activation of the coagulation cascade and platelet reactivity and with impaired fibrinolysis, processes are also amplified by the usually pre-existing comorbidities. The presence of atrial fibrosis and endothelial dysfunction is related to the development of AF, which promotes further atrial remodeling, thereby providing an increased risk for clot formation and subsequent embolization. In addition, it is also well demonstrated that LA dilatation and the loss of atrial contractile function reduce blood flow, specifically in the LA appendage, as it has been shown with various imaging techniques. [26] For years, the atrial blood stasis hypothesis has been acknowledged as the mechanism of AF-related thromboembolism and morbidity [27], however, recent evidence has emerged to suggest the presence of atrial myopathy (AM) as an alternative hypothesis.
AM (or atrial cardiomyopathy or atrial cardiopathy) is defined as “any complex structural, architectural, contractile or electrophysiological changes affecting the atria with the potential for producing clinically relevant manifestations” and appears as LA dysfunction and dilation. [28,29] The European Heart Rhythm Association (EHRA) has proposed in 2016 a working histological/pathophysiological classification scheme for AM (Table 1) which may help to convey the primary underlying pathology that led to its development. Emerging evidence suggests that thromboembolism can occur in the setting of AM even in the absence of AF. [30] However, AM and AF are strictly correlated with a cause-consequence relationship. This relationship is based on the close association between atrial fibrosis, one of the main characteristics of AM, and AF. Even microscopic scar has been documented to affect LA compliance and mechanical function leading to the development of AF. [31] Furthermore, AF and the subsequent volume and fluid overload, may themselves cause atrial remodeling, increasing atrial wall stiffness and fibrosis, and therefore provoking or worsening AM. [32]
5. Evaluation of Atrial Cardiomyopathy
The diagnosis of AM could be suggested based on ECG findings, as AF or other atrial arrhythmias [33,34], serum biomarkers, and imaging evidence for LA dilatation and dysfunction, often associated with myocardial fibrosis. [28,35,36]
LA dilation, in the absence of mitral valve disease, is usually an indicator for chronic increase in wall tension, commonly due to increased LA pressure, [37,38,39,40] paired with impairment of LA function related to AM. [41,42 CS,CT] LA dilatation has been shown to be related to increased incidence of AF and stroke, [43,44,45,46,47,48,49,50,51,52] increased risk of overall mortality after myocardial infarction, [41,42,53,54], increased risk of death and hospitalization in patients with dilated cardiomyopathy, [55,56,57,58,59,60,61,62,63] as well as major cardiac events or death in patients with diabetes mellitus. [64]
LA dilatation is also a well-known marker of severity and chronicity of diastolic dysfunction and its consequent raised LA pressure. [37,38,39,40] Despite that, Kojima T et al. [65] and others have shown that LA function deteriorates before cavity enlargement with 36% of patients with AF having normal LA size. [66] Such controversy suggests the need for thorough and and comprehensive assessment of atrial anatomy, structure, and function for making accurate diagnosis of AM.
Evaluation of atrial morphology is typically made with 2D or 3D echocardiography. For assessment of atrial size, the parasternal long-axis linear dimension using M-mode is the most commonly used method [44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,64,67,68,69]. However, considering the complex 3D nature of the atrium and the usually non-uniform atrial remodeling, this measurement does not guarantee an accurate reflection of LA size. [70,71,72,73,74] Hence, measurement of LA volume has emerged as a more accurate prognostic indicator in a variety of cardiac diseases. [49,51,53,54,55,56,57,58,64,67,68,69,70,71,72,73,74,75,76,77,78,79,80] LA volume from 2D images is best measured using the disk summation algorithm since it includes fewer geometric assumptions. [81,82] 2-D echocardiographic LA volumes are typically smaller than those reported from computed tomography (CT) or cardiac magnetic resonance imaging (CMR), [83,84,85,86,87] however, 3-D echocardiography measured LA volumes have been shown to correlate well with cardiac CT [88,89] and CMR, [90,91], having shown a superior prognostic predictive power than 2D LA volumes. [92,93]
Overall, the recommended normal upper limit for indexed LA volume is 34 mL/m2 for both genders which fits well with a risk-based approach for determining a cut-off between a normal and an enlarged LA. [43,77,78,79]
LA function can be studied by analyzing the electrical remodelling process from surface 12 lead ECG (P wave terminal force in lead V1, P wave axis alterations, P wave voltage reduction, P wave increased area, P wave dispersion or prolonged duration, PR interval (interatrial conduction block)) [94], or, more precisely during an electrophysiological study.
Routine conventional echocardiographic indexes used for studying LA function have limitations, but the evaluation of longitudinal deformation by speckle tracking echocardiography has proven to be a very reliable parameter. LA function has been studied with different echocardiographic tools including pulsed-wave Doppler measurements of late (mitral A) diastolic filling and pulmonary vein atrial reversal velocity, but their absolute values are affected by many factors including age, reduced LV compliance and loading conditions. [39,95,96,97,98,99,100,101,102,103]
The time between the onset of surface ECG “P” wave and the onset of “a” wave on tissue Doppler imaging (TDI), or total atrial conduction time, can be used as a non-invasive marker of atrial electromechanical delay (AEMD)[104,105,106,107,108,109,110,111], which has shown to be accurate, yet an indirect marker of atrial function. This index measures the time required for atrial depolarization to occur which results in active atrial contraction representing a more complete measure of the extent of atrial remodeling than other indices. [112] An increase in TDI-derived AEMD has been shown to predict AF recurrence in patients with paroxysmal AF [104], particularly if measured in the lateral leads, and has been shown to be non-inferior to LA volume index in identifying those patients. [113]
A correlation between TDI-derived AEMD duration and the degree of right atrial appendage fibrosis has been demonstrated in a histological validation study by Müller et al. [114] A good agreement has also been demonstrated between TDI-derived AEMD duration and total atrial conduction time measured in an electrophysiological study in healthy individuals. [115] Its duration was also shown to be affected by several risk factors which are known to play significant role in atrial remodeling including age, hypertension, valvular disease, LV diastolic dysfunction, sleep apnoea and increased body mass index [112]. Additionally, it was found to be related to increased LA volume and inversely related to LA reservoir strain, [116] hence was proposed as an independent predictor of AF after cardiac surgery [117], AF recurrence after electrical cardioversion [118], and catheter ablation [119]. In a recent prospective study of patients free of AF after successful catheter ablation who were not on anticoagulants, a prolonged TDI-derived AEMD was associated with increased stroke incidence and an improved CHA2DS2-VASc score performance [120].
Two-dimensional speckle-tracking echocardiography has emerged as a more sensitive marker for detecting early functional remodelling before anatomical alterations occur. [121,122,123,124,125,126,127,128,129,130,131,132,133,134,135] Strain and strain rate are two measures of myocardial deformation based on estimating spatial gradients in myocardial velocities. [121,124,128,129,136,137,138,139,140] This technique offers important information on early modification of LA structure and function, before volume changes, and is associated with the occurrence and persistence of AF. [35,141] Furthermore, patients with paroxysmal AF have been shown to have increased LA stiffness which is described as low relaxation properties, one of the main features of AM that can be non-invasively measured as the ratio between E/e’ to LA strain. [142] Abnormalities in atrial strain have been observed in many conditions, including AF, valvular pathology, heart failure, hypertension, diabetes, and cardiomyopathies [124,125,131,132,133,134,135]. Population-based studies have shown the prognostic value of LA strain analysis of long-term outcome. [124,130] Interestingly, LA dysfunction with changes in strain and strain rate has been observed in patients with amyloidosis even in the absence of other echocardiographic features of cardiac involvement, thus highlighting its possible application as an early marker of cardiac involvement. [137] The study of LA deformation with 2D speckle tracking echocardiography has also demonstrated high sensitivity in identifying myocardial fibrosis and increased cavity stiffness as compared to CMR measures [35], invasive electrophysiological studies with high density voltage mapping, [143] and with invasive biopsy assessment. [144] Considering the CMR’s high-cost and the risk of side-effects from Gadolinium, echocardiography has been proved as the modality of choice for screening and serially following patients with diseases involving the LA morphology and function. [67,145]
6. Potential Applications of AM Study in Clinical Practice
Based on the strong emerging evidence, many authors used these noninvasive indices to focus attention on the evaluation of AM as lone disease and started to consider AM not just as a “collateral finding” or a consequence of AF, but likely to be the primary cause of the morbidity and poor outcome previously attributed to AF. Sade et al. have demonstrated that a reduction in LA strain was able to stratify the risk of AF onset in patients with cryptogenic stroke irrespective of AF. [146] Moreover, in a low-risk general population Alhakak et al. have shown a reduction in LA reservoir strain as an independent predictor of long-term risk for AF and ischemic stroke [147].
Azemi et al. have also demonstrated that patients with low-risk CHADS2 scores and a history of AF, LA strain values were significantly reduced in those presenting later with stroke or TIA compared with age and gender-matched controls with identical CHADS2 score [148] thus suggesting low LA strain as a a direct contributor to thrombogenic risk (or both). Also, Saha et al. showed a strong association between impairment of LA strain, the presence of AF and higher CHADS2 score, and that in AF patients LA strain was a predictor of stroke events and cardiovascular outcomes. [149]
LA strain provided additional information on acute embolisms over and above the CHA2DS2-VASc score in a population of patients with paroxysmal or permanent AF. [150] Finally, LA strain has proved to be a predictor of new onset AF in patients with heart failure [151] and those with cardiac amyloidosis, being able to identify those at high thrombotic risk, independent of AF. [152]
Evaluation of LA strain, reflecting an underlying AM, also demonstrated a potential as a preoperative predictor of postoperative AF in patients undergoing aortic valve replacement (AVR) for aortic stenosis and coronary artery bypass grafting (CABG). Cameli et al. [153] demonstrated a significant reduction in global peak atrial longitudinal strain (PALS) as the sole independent predictor of postoperative AF. Pastore et al. [154] also proposed a preoperative global PALS below 28% as a specific parameter for stratifying patients at increased risk for postoperative AF (hazard ratio, 3.6 [95% CI, 2.2-5.9]; P<0.001) following CABG. These findings emphasize the use of LA strain assessment in identifying patients with a higher risk of arrhythmias, and applying optimum preventive measures.
A recent interesting attempt to demonstrate the possible influence of underlying AM in increasing the risk of ischemic stroke and dementia in patients with AF has been made in the study by Zhang et al [155] in which the association of AF with stroke and between AF and dementia, adjusted by echocardiographic parameters of AM, has been investigated. The study was particularly powered by a large number of patients. The authors found that, after adjusting for LA volumes and function, particularly of LA reservoir strain, the apparent association between AF and incident stroke and dementia loses its strength and statistical significance. All these studies confirmed that LA strain may be used not only to study LA fibrosis/changes in the interstitial matrix that characterize AM, but also driving the risk of new onset of AF and stroke independent from AF, being a predictor of cardiovascular outcomes.
The main limitations of the methodology are currently the absence of consensus or standardization for the echocardiographic definition of AM. All these authors have used strain parameters that, despite being a sensitive marker of atrial structural rearrangements and fibrosis, still remain “new indices” and are yet not regarded as an objective parameter for defining AM.
LA strain has been already included as an additional parameter in detecting diastolic dysfunction in the latest recommendations of the European Association of CardioVascular Imaging (EACVI) on the use of multimodality imaging for the evaluation of heart failure with preserved ejection fraction (HFpEF). [156] Thus, if the mechanism hypothesized by Zhang et al. for the association between AM and stroke, based on impaired LA structure/function predisposing to thrombus, is confirmed, the use of LA strain in evaluating AM may be considered for better studying the underlying mechanism and better stratifying patient’s thromboembolic risk.
Considering the increasing availability, feasibility, and timelines of obtaining LA strain values, as well as being used within scores as a prognostic stratifier of cardiovascular outcomes, it may also be used to improve risk stratification for stroke and dementia, with important therapeutic consequences on anticoagulation for primary prevention of stroke. This may lead to a general optimization of anticoagulation use, not only including patients at higher risk of stroke without AF but also those in the grey-zones risk of stroke according to current indices (i.e. in the low CHADs-VASC score). These suggestions need randomized controlled trials with safety/efficacy data on AM as lone indication to anticoagulation, which are eagerly awaited in the future.
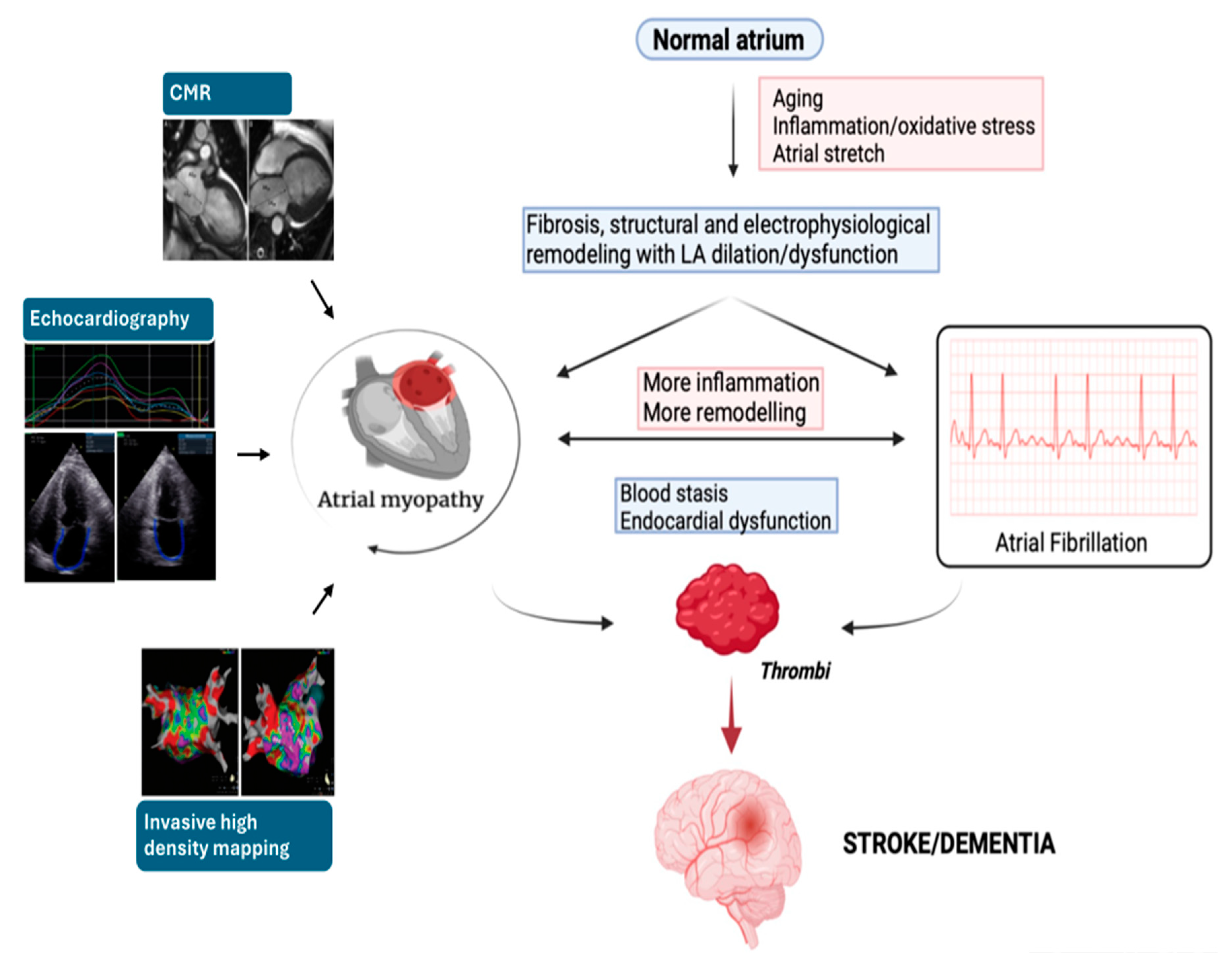
Figure 1.
The interdependency and common pathophysiology of atrial myopathy and atrial fibrillation and their association with Stroke and Dementia. CMR, cardiac magnetic resonance.
Figure 1.
The interdependency and common pathophysiology of atrial myopathy and atrial fibrillation and their association with Stroke and Dementia. CMR, cardiac magnetic resonance.
7. Conclusions
This article examines the emerging concept of AM, its association with thromboembolic events and the consequent increased risk of stroke and dementia, particularly in the context of AF. While the association between AF and these outcomes is well known, AM presents a novel perspective, suggesting its possible role as an independent risk factor.
The Key Takeaway messages are three 1) AM encompasses structural and functional abnormalities of the atria, potentially contributing to thromboembolism even in the absence of AF; 2) Echocardiography emerges as a promising tool for non-invasive evaluation of AM, particularly LA strain analysis; 3) Evidence exists suggesting that LA strain may offer additional risk stratification beyond the established CHADS2-VASc, with potential impactions on anticoagulation.
By acknowledging AM potential role and utilizing advanced imaging techniques like LA strain, we can strive towards a more comprehensive understanding of the mechanism underlying an increased thromboembolic risk in specific sub-groups of patients. The integration of LA strain analysis into routine clinical practice holds promise for improved patient management and targeted therapies thus may allow better clinical risk stratification in AF patients. Nevertheless, standardized definitions and diagnostic criteria for AM are crucial for consistent evaluation and research, and further studies are necessary to explore the efficacy and safety of anticoagulation in AM patients without AF.
Author Contributions
Conceptualization, A.C. and M.L.; resources, M.C.P. and G.E.M.; writing—original draft preparation, A.C.; writing—review and editing, M.H. and A.R.; visualization, Y.F.F.C. and A.P.; supervision, M.L and M.C.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC [published correction appears in Eur Heart J. 2021 Feb 1;42(5):507] [published correction appears in Eur Heart J. 2021 Feb 1;42(5):546-547] [published correction appears in Eur Heart J. 2021 Oct 21;42(40):4194]. Eur Heart J. 2021;42(5):373-498. [CrossRef]
- Colilla S, Crow A, Petkun W, Singer DE, Simon T, Liu X. Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am J Cardiol. 2013;112(8):1142-1147. [CrossRef]
- Freedman JE, Gersh BJ. Atrial fibrillation and stroke prevention in aging patients: what's good can be even better. Circulation. 2014;130(2):129-131. [CrossRef]
- Sankaranarayanan R, Kirkwood G, Visweswariah R, Fox DJ. How does Chronic Atrial Fibrillation Influence Mortality in the Modern Treatment Era?. Curr Cardiol Rev. 2015;11(3):190-198. [CrossRef]
- Thrall G, Lane D, Carroll D, Lip GY. Quality of life in patients with atrial fibrillation: a systematic review. Am J Med. 2006;119(5):. [CrossRef]
- January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society [published correction appears in J Am Coll Cardiol. 2019 Jul 30;74(4):599]. J Am Coll Cardiol. 2019;74(1):104-132. [CrossRef]
- Schotten U, Verheule S, Kirchhof P, Goette A. Pathophysiological mechanisms of atrial fibrillation: a translational appraisal [published correction appears in Physiol Rev. 2011 Oct;91(4):1533]. Physiol Rev. 2011;91(1):265-325. [CrossRef]
- Boriani G, Savelieva I, Dan GA, et al. Chronic kidney disease in patients with cardiac rhythm disturbances or implantable electrical devices: clinical significance and implications for decision making-a position paper of the European Heart Rhythm Association endorsed by the Heart Rhythm Society and the Asia Pacific Heart Rhythm Society. Europace. 2015;17(8):1169-1196. [CrossRef]
- Aune D, Feng T, Schlesinger S, Janszky I, Norat T, Riboli E. Diabetes mellitus, blood glucose and the risk of atrial fibrillation: A systematic review and meta-analysis of cohort studies. J Diabetes Complications. 2018;32(5):501-511. [CrossRef]
- Cadby G, McArdle N, Briffa T, et al. Severity of OSA is an independent predictor of incident atrial fibrillation hospitalization in a large sleep-clinic cohort. Chest. 2015;148(4):945-952. [CrossRef]
- Hobbelt AH, Siland JE, Geelhoed B, et al. Clinical, biomarker, and genetic predictors of specific types of atrial fibrillation in a community-based cohort: data of the PREVEND study. Europace. 2017;19(2):226-232. [CrossRef]
- Nalliah CJ, Sanders P, Kalman JM. The Impact of Diet and Lifestyle on Atrial Fibrillation. Curr Cardiol Rep. 2018;20(12):137. Published 2018 Oct 12. [CrossRef]
- Lip GYH, Coca A, Kahan T, et al. Hypertension and cardiac arrhythmias: a consensus document from the European Heart Rhythm Association (EHRA) and ESC Council on Hypertension, endorsed by the Heart Rhythm Society (HRS), Asia-Pacific Heart Rhythm Society (APHRS) and Sociedad Latinoamericana de Estimulación Cardíaca y Electrofisiología (SOLEACE). Europace. 2017;19(6):891-911. [CrossRef]
- Gallagher C, Hendriks JML, Elliott AD, et al. Alcohol and incident atrial fibrillation - A systematic review and meta-analysis. Int J Cardiol. 2017;246:46-52. [CrossRef]
- Ricci C, Gervasi F, Gaeta M, Smuts CM, Schutte AE, Leitzmann MF. Physical activity volume in relation to risk of atrial fibrillation. A non-linear meta-regression analysis. Eur J Prev Cardiol. 2018;25(8):857-866. [CrossRef]
- Benjamin EJ, Muntner P, Alonso A, et al. Heart Disease and Stroke Statistics-2019 Update: A Report From the American Heart Association [published correction appears in Circulation. 2020 Jan 14;141(2):e33]. Circulation. 2019;139(10):e56-e528. [CrossRef]
- Allan V, Honarbakhsh S, Casas JP, et al. Are cardiovascular risk factors also associated with the incidence of atrial fibrillation? A systematic review and field synopsis of 23 factors in 32 population-based cohorts of 20 million participants. Thromb Haemost. 2017;117(5):837-850. [CrossRef]
- Feghaly J, Zakka P, London B, MacRae CA, Refaat MM. Genetics of Atrial Fibrillation. J Am Heart Assoc. 2018;7(20):e009884. [CrossRef]
- Wijesurendra RS, Casadei B. Mechanisms of atrial fibrillation. Heart. 2019;105(24):1860-1867. [CrossRef]
- Lubitz SA, Yin X, McManus DD, et al. Stroke as the Initial Manifestation of Atrial Fibrillation: The Framingham Heart Study. Stroke. 2017;48(2):490-492. [CrossRef]
- Bunch TJ. Atrial Fibrillation and Dementia. Circulation. 2020;142(7):618-620. [CrossRef]
- Friberg L, Rosenqvist M. Less dementia with oral anticoagulation in atrial fibrillation. Eur Heart J. 2018;39(6):453-460. [CrossRef]
- Jacobs V, Woller SC, Stevens S, et al. Time outside of therapeutic range in atrial fibrillation patients is associated with long-term risk of dementia. Heart Rhythm. 2014;11(12):2206-2213. [CrossRef]
- Bunch TJ, Crandall BG, Weiss JP, et al. Patients treated with catheter ablation for atrial fibrillation have long-term rates of death, stroke, and dementia similar to patients without atrial fibrillation. J Cardiovasc Electrophysiol. 2011;22(8):839-845. [CrossRef]
- Jin MN, Kim TH, Kang KW, et al. Atrial Fibrillation Catheter Ablation Improves 1-Year Follow-Up Cognitive Function, Especially in Patients With Impaired Cognitive Function. Circ Arrhythm Electrophysiol. 2019;12(7):e007197. [CrossRef]
- Ding WY, Gupta D, Lip GYH. Atrial fibrillation and the prothrombotic state: revisiting Virchow's triad in 2020. Heart. 2020;106(19):1463-1468. [CrossRef]
- Watson T, Shantsila E, Lip GY. Mechanisms of thrombogenesis in atrial fibrillation: Virchow's triad revisited. Lancet. 2009;373(9658):155-166. [CrossRef]
- Goette A, Kalman JM, Aguinaga L, et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: Definition, characterization, and clinical implication. Heart Rhythm. 2017;14(1):e3-e40. [CrossRef]
- Kamel H, Bartz TM, Elkind MSV, et al. Atrial Cardiopathy and the Risk of Ischemic Stroke in the CHS (Cardiovascular Health Study). Stroke. 2018;49(4):980-986. [CrossRef]
- Brambatti M, Connolly SJ, Gold MR, et al. Temporal relationship between subclinical atrial fibrillation and embolic events. Circulation. 2014;129(21):2094-2099. [CrossRef]
- Triposkiadis F, Pieske B, Butler J, et al. Global left atrial failure in heart failure. Eur J Heart Fail. 2016;18(11):1307-1320. [CrossRef]
- Miller JD, Aronis KN, Chrispin J, et al. Obesity, Exercise, Obstructive Sleep Apnea, and Modifiable Atherosclerotic Cardiovascular Disease Risk Factors in Atrial Fibrillation. J Am Coll Cardiol. 2015;66(25):2899-2906. [CrossRef]
- Binici Z, Intzilakis T, Nielsen OW, Køber L, Sajadieh A. Excessive supraventricular ectopic activity and increased risk of atrial fibrillation and stroke. Circulation. 2010;121(17):1904-1911. [CrossRef]
- Larsen BS, Kumarathurai P, Falkenberg J, Nielsen OW, Sajadieh A. Excessive Atrial Ectopy and Short Atrial Runs Increase the Risk of Stroke Beyond Incident Atrial Fibrillation. J Am Coll Cardiol. 2015;66(3):232-241. [CrossRef]
- Kuppahally SS, Akoum N, Burgon NS, et al. Left atrial strain and strain rate in patients with paroxysmal and persistent atrial fibrillation: relationship to left atrial structural remodeling detected by delayed-enhancement MRI. Circ Cardiovasc Imaging. 2010;3(3):231-239. [CrossRef]
- Peigh G, Shah SJ, Patel RB. Left Atrial Myopathy in Atrial Fibrillation and Heart Failure: Clinical Implications, Mechanisms, and Therapeutic Targets. Curr Heart Fail Rep. 2021;18(3):85-98. [CrossRef]
- Appleton CP, Galloway JM, Gonzalez MS, Gaballa M, Basnight MA. Estimation of left ventricular filling pressures using two-dimensional and Doppler echocardiography in adult patients with cardiac disease. Additional value of analyzing left atrial size, left atrial ejection fraction and the difference in duration of pulmonary venous and mitral flow velocity at atrial contraction. J Am Coll Cardiol. 1993;22(7):1972-1982. [CrossRef]
- Geske JB, Sorajja P, Nishimura RA, Ommen SR. The relationship of left atrial volume and left atrial pressure in patients with hypertrophic cardiomyopathy: an echocardiographic and cardiac catheterization study. J Am Soc Echocardiogr. 2009;22(8):961-966. [CrossRef]
- Guron CW, Hartford M, Rosengren A, Thelle D, Wallentin I, Caidahl K. Usefulness of atrial size inequality as an indicator of abnormal left ventricular filling. Am J Cardiol. 2005;95(12):1448-1452. [CrossRef]
- Simek CL, Feldman MD, Haber HL, Wu CC, Jayaweera AR, Kaul S. Relationship between left ventricular wall thickness and left atrial size: comparison with other measures of diastolic function. J Am Soc Echocardiogr. 1995;8(1):37-47. [CrossRef]
- Ersbøll M, Andersen MJ, Valeur N, et al. The prognostic value of left atrial peak reservoir strain in acute myocardial infarction is dependent on left ventricular longitudinal function and left atrial size. Circ Cardiovasc Imaging. 2013;6(1):26-33. [CrossRef]
- Lønborg JT, Engstrøm T, Møller JE, et al. Left atrial volume and function in patients following ST elevation myocardial infarction and the association with clinical outcome: a cardiovascular magnetic resonance study. Eur Heart J Cardiovasc Imaging. 2013;14(2):118-127. [CrossRef]
- Barnes ME, Miyasaka Y, Seward JB, et al. Left atrial volume in the prediction of first ischemic stroke in an elderly cohort without atrial fibrillation. Mayo Clin Proc. 2004;79(8):1008-1014. [CrossRef]
- Benjamin EJ, D'Agostino RB, Belanger AJ, Wolf PA, Levy D. Left atrial size and the risk of stroke and death. The Framingham Heart Study. Circulation. 1995;92(4):835-841. [CrossRef]
- Bolca O, Akdemir O, Eren M, Dagdeviren B, Yildirim A, Tezel T. Left atrial maximum volume is a recurrence predictor in lone atrial fibrillation: an acoustic quantification study. Jpn Heart J. 2002;43(3):241-248. [CrossRef]
- Di Tullio MR, Sacco RL, Sciacca RR, Homma S. Left atrial size and the risk of ischemic stroke in an ethnically mixed population. Stroke. 1999;30(10):2019-2024. [CrossRef]
- Flaker GC, Fletcher KA, Rothbart RM, Halperin JL, Hart RG. Clinical and echocardiographic features of intermittent atrial fibrillation that predict recurrent atrial fibrillation. Stroke Prevention in Atrial Fibrillation (SPAF) Investigators. Am J Cardiol. 1995;76(5):355-358. [CrossRef]
- Kottkamp H. Fibrotic atrial cardiomyopathy: a specific disease/syndrome supplying substrates for atrial fibrillation, atrial tachycardia, sinus node disease, AV node disease, and thromboembolic complications. J Cardiovasc Electrophysiol. 2012;23(7):797-799. [CrossRef]
- Tsang TS, Barnes ME, Bailey KR, et al. Left atrial volume: important risk marker of incident atrial fibrillation in 1655 older men and women. Mayo Clin Proc. 2001;76(5):467-475. [CrossRef]
- Vaziri SM, Larson MG, Benjamin EJ, Levy D. Echocardiographic predictors of nonrheumatic atrial fibrillation. The Framingham Heart Study. Circulation. 1994;89(2):724-730. [CrossRef]
- Tsang TS, Barnes ME, Gersh BJ, Bailey KR, Seward JB. Risks for atrial fibrillation and congestive heart failure in patients >/=65 years of age with abnormal left ventricular diastolic relaxation. Am J Cardiol. 2004;93(1):54-58. [CrossRef]
- Tsang TS, Gersh BJ, Appleton CP, et al. Left ventricular diastolic dysfunction as a predictor of the first diagnosed nonvalvular atrial fibrillation in 840 elderly men and women. J Am Coll Cardiol. 2002;40(9):1636-1644. [CrossRef]
- Beinart R, Boyko V, Schwammenthal E, et al. Long-term prognostic significance of left atrial volume in acute myocardial infarction. J Am Coll Cardiol. 2004;44(2):327-334. [CrossRef]
- Moller JE, Hillis GS, Oh JK, et al. Left atrial volume: a powerful predictor of survival after acute myocardial infarction. Circulation. 2003;107(17):2207-2212. [CrossRef]
- Dini FL, Cortigiani L, Baldini U, et al. Prognostic value of left atrial enlargement in patients with idiopathic dilated cardiomyopathy and ischemic cardiomyopathy. Am J Cardiol. 2002;89(5):518-523. [CrossRef]
- Kim H, Cho YK, Jun DH, et al. Prognostic implications of the NT-ProBNP level and left atrial size in non-ischemic dilated cardiomyopathy. Circ J. 2008;72(10):1658-1665. [CrossRef]
- Modena MG, Muia N, Sgura FA, Molinari R, Castella A, Rossi R. Left atrial size is the major predictor of cardiac death and overall clinical outcome in patients with dilated cardiomyopathy: a long-term follow-up study. Clin Cardiol. 1997;20(6):553-560. [CrossRef]
- Sabharwal N, Cemin R, Rajan K, Hickman M, Lahiri A, Senior R. Usefulness of left atrial volume as a predictor of mortality in patients with ischemic cardiomyopathy. Am J Cardiol. 2004;94(6):760-763. [CrossRef]
- Maddukuri PV, Vieira ML, DeCastro S, et al. What is the best approach for the assessment of left atrial size? Comparison of various unidimensional and two-dimensional parameters with three-dimensional echocardiographically determined left atrial volume. J Am Soc Echocardiogr. 2006;19(8):1026-1032. [CrossRef]
- Wang Y, Gutman JM, Heilbron D, Wahr D, Schiller NB. Atrial volume in a normal adult population by two-dimensional echocardiography. Chest. 1984;86(4):595-601. [CrossRef]
- Whitlock M, Garg A, Gelow J, Jacobson T, Broberg C. Comparison of left and right atrial volume by echocardiography versus cardiac magnetic resonance imaging using the area-length method. Am J Cardiol. 2010;106(9):1345-1350. [CrossRef]
- Aune E, Baekkevar M, Roislien J, Rodevand O, Otterstad JE. Normal reference ranges for left and right atrial volume indexes and ejection fractions obtained with real-time three-dimensional echocardiography. Eur J Echocardiogr. 2009;10(6):738-744. [CrossRef]
- Peluso D, Badano LP, Muraru D, et al. Right atrial size and function assessed with three-dimensional and speckle-tracking echocardiography in 200 healthy volunteers. Eur Heart J Cardiovasc Imaging. 2013;14(11):1106-1114. [CrossRef]
- Poulsen MK, Dahl JS, Henriksen JE, et al. Left atrial volume index: relation to long-term clinical outcome in type 2 diabetes. J Am Coll Cardiol. 2013;62(25):2416-2421. [CrossRef]
- Kojima T, Kawasaki M, Tanaka R, et al. Left atrial global and regional function in patients with paroxysmal atrial fibrillation has already been impaired before enlargement of left atrium: velocity vector imaging echocardiography study. Eur Heart J Cardiovasc Imaging. 2012;13(3):227-234. [CrossRef]
- Gupta DK, Shah AM, Giugliano RP, et al. Left atrial structure and function in atrial fibrillation: ENGAGE AF-TIMI 48. Eur Heart J. 2014;35(22):1457-1465. [CrossRef]
- Lang RM, Badano LP, Mor-Avi V, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2015;28(1):1-39.e14. [CrossRef]
- Olshansky B, Heller EN, Mitchell LB, et al. Are transthoracic echocardiographic parameters associated with atrial fibrillation recurrence or stroke? Results from the Atrial Fibrillation Follow-Up Investigation of Rhythm Management (AFFIRM) study. J Am Coll Cardiol. 2005;45(12):2026-2033. [CrossRef]
- Rusinaru D, Tribouilloy C, Grigioni F, et al. Left atrial size is a potent predictor of mortality in mitral regurgitation due to flail leaflets: results from a large international multicenter study. Circ Cardiovasc Imaging. 2011;4(5):473-481. [CrossRef]
- Wade MR, Chandraratna PA, Reid CL, Lin SL, Rahimtoola SH. Accuracy of nondirected and directed M-mode echocardiography as an estimate of left atrial size. Am J Cardiol. 1987;60(14):1208-1211. [CrossRef]
- Lester SJ, Ryan EW, Schiller NB, Foster E. Best method in clinical practice and in research studies to determine left atrial size. Am J Cardiol. 1999;84(7):829-832. [CrossRef]
- Loperfido F, Pennestri F, Digaetano A, et al. Assessment of left atrial dimensions by cross sectional echocardiography in patients with mitral valve disease. Br Heart J. 1983;50(6):570-578. [CrossRef]
- Vyas H, Jackson K, Chenzbraun A. Switching to volumetric left atrial measurements: impact on routine echocardiographic practice. Eur J Echocardiogr. 2011;12(2):107-111. [CrossRef]
- Gottdiener JS, Kitzman DW, Aurigemma GP, Arnold AM, Manolio TA. Left atrial volume, geometry, and function in systolic and diastolic heart failure of persons > or =65 years of age (the cardiovascular health study). Am J Cardiol. 2006;97(1):83-89. [CrossRef]
- Rossi A, Cicoira M, Zanolla L, et al. Determinants and prognostic value of left atrial volume in patients with dilated cardiomyopathy. J Am Coll Cardiol. 2002;40(8):1425. [CrossRef]
- Takemoto Y, Barnes ME, Seward JB, et al. Usefulness of left atrial volume in predicting first congestive heart failure in patients > or = 65 years of age with well-preserved left ventricular systolic function. Am J Cardiol. 2005;96(6):832-836. [CrossRef]
- Tani T, Tanabe K, Ono M, et al. Left atrial volume and the risk of paroxysmal atrial fibrillation in patients with hypertrophic cardiomyopathy. J Am Soc Echocardiogr. 2004;17(6):644-648. [CrossRef]
- Tsang TS, Abhayaratna WP, Barnes ME, et al. Prediction of cardiovascular outcomes with left atrial size: is volume superior to area or diameter?. J Am Coll Cardiol. 2006;47(5):1018-1023. [CrossRef]
- Pritchett AM, Jacobsen SJ, Mahoney DW, Rodeheffer RJ, Bailey KR, Redfield MM. Left atrial volume as an index of left atrial size: a population-based study. J Am Coll Cardiol. 2003;41(6):1036-1043. [CrossRef]
- Jenkins C, Bricknell K, Marwick TH. Use of real-time three-dimensional echocardiography to measure left atrial volume: comparison with other echocardiographic techniques. J Am Soc Echocardiogr. 2005;18(9):991-997. [CrossRef]
- Thomas L, Levett K, Boyd A, Leung DY, Schiller NB, Ross DL. Compensatory changes in atrial volumes with normal aging: is atrial enlargement inevitable?. J Am Coll Cardiol. 2002;40(9):1630-1635. [CrossRef]
- Yamaguchi K, Tanabe K, Tani T, et al. Left atrial volume in normal Japanese adults. Circ J. 2006;70(3):285-288. [CrossRef]
- Maceira AM, Cosín-Sales J, Roughton M, Prasad SK, Pennell DJ. Reference left atrial dimensions and volumes by steady state free precession cardiovascular magnetic resonance. J Cardiovasc Magn Reson. 2010;12(1):65. Published 2010 Nov 11. [CrossRef]
- Rodevan O, Bjornerheim R, Ljosland M, Maehle J, Smith HJ, Ihlen H. Left atrial volumes assessed by three- and two-dimensional echocardiography compared to MRI estimates. Int J Card Imaging. 1999;15(5):397-410. [CrossRef]
- Stojanovska J, Cronin P, Patel S, et al. Reference normal absolute and indexed values from ECG-gated MDCT: left atrial volume, function, and diameter. AJR Am J Roentgenol. 2011;197(3):631-637. [CrossRef]
- Ujino K, Barnes ME, Cha SS, et al. Two-dimensional echocardiographic methods for assessment of left atrial volume. Am J Cardiol. 2006;98(9):1185-1188. [CrossRef]
- Aurigemma GP, Gottdiener JS, Arnold AM, Chinali M, Hill JC, Kitzman D. Left atrial volume and geometry in healthy aging: the Cardiovascular Health Study. Circ Cardiovasc Imaging. 2009;2(4):282-289. [CrossRef]
- Miyasaka Y, Tsujimoto S, Maeba H, et al. Left atrial volume by real-time three-dimensional echocardiography: validation by 64-slice multidetector computed tomography. J Am Soc Echocardiogr. 2011;24(6):680-686. [CrossRef]
- Rohner A, Brinkert M, Kawel N, et al. Functional assessment of the left atrium by real-time three-dimensional echocardiography using a novel dedicated analysis tool: initial validation studies in comparison with computed tomography. Eur J Echocardiogr. 2011;12(7):497-505. [CrossRef]
- Artang R, Migrino RQ, Harmann L, Bowers M, Woods TD. Left atrial volume measurement with automated border detection by 3-dimensional echocardiography: comparison with Magnetic Resonance Imaging. Cardiovasc Ultrasound. 2009;7:16. Published 2009 Mar 31. [CrossRef]
- Mor-Avi V, Yodwut C, Jenkins C, et al. Real-time 3D echocardiographic quantification of left atrial volume: multicenter study for validation with CMR. JACC Cardiovasc Imaging. 2012;5(8):769-777. [CrossRef]
- Caselli S, Canali E, Foschi ML, et al. Long-term prognostic significance of three-dimensional echocardiographic parameters of the left ventricle and left atrium. Eur J Echocardiogr. 2010;11(3):250-256. [CrossRef]
- Suh IW, Song JM, Lee EY, et al. Left atrial volume measured by real-time 3-dimensional echocardiography predicts clinical outcomes in patients with severe left ventricular dysfunction and in sinus rhythm. J Am Soc Echocardiogr. 2008;21(5):439-445. [CrossRef]
- Chen L.Y., Ribeiro A.L.P., Platonov P.G., Cygankiewicz I., Soliman E.Z., Gorenek B., Ikeda T., Vassilikos V.P., Steinberg J.S., Varma N., et al. P Wave Parameters and Indices: A Critical Appraisal of Clinical Utility, Challenges, and Future Research-A Consensus Document Endorsed by the International Society of Electrocardiology and the International Society for Holter and Noninvasive Electrocardiology. Circ. Arrhythmia Electrophysiol. 2022;15:e010435.
- Vasan RS, Larson MG, Levy D, et al. Doppler transmitral flow indexes and risk of atrial fibrillation (the Framingham Heart Study). Am J Cardiol. 2003;91(9):1079-1083. [CrossRef]
- Mattioli AV, Tarabini Castellani E, Vivoli D, Molinari R, Mattioli G. Restoration of atrial function after atrial fibrillation of different etiological origins. Cardiology. 1996;87(3):205-211. [CrossRef]
- Yuda S, Nakatani S, Isobe F, Kosakai Y, Miyatake K. Comparative efficacy of the maze procedure for restoration of atrial contraction in patients with and without giant left atrium associated with mitral valve disease. J Am Coll Cardiol. 1998;31(5):1097-1102. [CrossRef]
- Shizukuda Y, Bolan CD, Tripodi DJ, et al. Significance of left atrial contractile function in asymptomatic subjects with hereditary hemochromatosis. Am J Cardiol. 2006;98(7):954-959. [CrossRef]
- Manning WJ, Leeman DE, Gotch PJ, Come PC. Pulsed Doppler evaluation of atrial mechanical function after electrical cardioversion of atrial fibrillation. J Am Coll Cardiol. 1989;13(3):617-623. [CrossRef]
- Oki T, Fukuda N, Iuchi A, et al. Left Atrial Systolic Performance in the Presence of Elevated Left Ventricular End-Diastolic Pressure: Evaluation by Transesophageal Pulsed Doppler Echocardiography of Left Ventricular Inflow and Pulmonary Venous Flow Velocities. Echocardiography. 1997;14(1):23-32. [CrossRef]
- Oki T, Iuchi A, Tabata T, et al. Transesophageal pulsed Doppler echocardiographic evaluation of left atrial systolic performance in hypertrophic cardiomyopathy: combined analysis of transmitral and pulmonary venous flow velocities. Clin Cardiol. 1997;20(1):47-54. [CrossRef]
- Sakai H, Kunichika H, Murata K, et al. Improvement of afterload mismatch of left atrial booster pump function with positive inotropic agent. J Am Coll Cardiol. 2001;37(1):270-277. [CrossRef]
- Iuchi A, Oki T, Tabata T, et al. J Cardiol. 1995;25(6):317-324.
- Ari H, Ari S, Akkaya M, et al. Predictive value of atrial electromechanical delay for atrial fibrillation recurrence. Cardiol J. 2013;20(6):639-647. [CrossRef]
- Hoshi Y, Nozawa Y, Ogasawara M, et al. Atrial electromechanical interval may predict cardioembolic stroke in apparently low risk elderly patients with paroxysmal atrial fibrillation. Echocardiography. 2014;31(2):140-148. [CrossRef]
- Acar G, Akcay A, Sokmen A, et al. Assessment of atrial electromechanical delay, diastolic functions, and left atrial mechanical functions in patients with type 1 diabetes mellitus. J Am Soc Echocardiogr. 2009;22(6):732-738. [CrossRef]
- Nar G, Ergul B, Aksan G, Inci S. Assessment of Atrial Electromechanical Delay and Left Atrial Mechanical Functions in Patients with Ulcerative Colitis. Echocardiography. 2016;33(7):970-976. [CrossRef]
- Aksan G, Nar G, Soylu K, et al. Assessment of atrial electromechanical delay and left atrial mechanical functions in patients with psoriasis vulgaris. Echocardiography. 2015;32(4):615-622. [CrossRef]
- Ilter A, Kırış A, Kaplan Ş, et al. Atrial conduction times and left atrium mechanical functions in patients with active acromegaly. Endocrine. 2015;48(2):653-660. [CrossRef]
- Akıl MA, Akıl E, Bilik MZ, et al. The relationship between atrial electromechanical delay and left atrial mechanical function in stroke patients. Anatol J Cardiol. 2015;15(7):565-570. [CrossRef]
- Pozios I, Vouliotis AI, Dilaveris P, Tsioufis C. Electro-Mechanical Alterations in Atrial Fibrillation: Structural, Electrical, and Functional Correlates. J Cardiovasc Dev Dis. 2023;10(4):149. Published 2023 Mar 31. [CrossRef]
- Müller P, Weijs B, Bemelmans NMAA, et al. Echocardiography-derived total atrial conduction time (PA-TDI duration): risk stratification and guidance in atrial fibrillation management. Clin Res Cardiol. 2021;110(11):1734-1742. [CrossRef]
- Akamatsu K, Ito T, Miyamura M, Kanzaki Y, Sohmiya K, Hoshiga M. Usefulness of tissue Doppler-derived atrial electromechanical delay for identifying patients with paroxysmal atrial fibrillation. Cardiovasc Ultrasound. 2020;18(1):22. Published 2020 Jun 22. [CrossRef]
- Müller P, Hars C, Schiedat F, et al. Correlation between total atrial conduction time estimated via tissue Doppler imaging (PA-TDI Interval), structural atrial remodeling and new-onset of atrial fibrillation after cardiac surgery. J Cardiovasc Electrophysiol. 2013;24(6):626-631. [CrossRef]
- Erdem FH, Erdem A, Özlü F, et al. Electrophysiological validation of total atrial conduction time measurement by tissue doppler echocardiography according to age and sex in healthy adults. J Arrhythm. 2016;32(2):127-132. [CrossRef]
- Abou R, Leung M, Tonsbeek AM, et al. Effect of Aging on Left Atrial Compliance and Electromechanical Properties in Subjects Without Structural Heart Disease. Am J Cardiol. 2017;120(1):140-147. [CrossRef]
- Özlü MF, Erdem K, Kırış G, et al. Predictive value of total atrial conduction time measured with tissue Doppler imaging for postoperative atrial fibrillation after coronary artery bypass surgery. J Interv Card Electrophysiol. 2013;37(1):27-33. [CrossRef]
- Müller P, Schiedat F, Dietrich JW, et al. Reverse atrial remodeling in patients who maintain sinus rhythm after electrical cardioversion: evidence derived from the measurement of total atrial conduction time assessed by PA-TDI interval. J Echocardiogr. 2014;12(4):142-150. [CrossRef]
- Den Uijl DW, Delgado V, Bertini M, et al. Impact of left atrial fibrosis and left atrial size on the outcome of catheter ablation for atrial fibrillation. Heart. 2011;97(22):1847-1851. [CrossRef]
- Chao TF, Lin YJ, Tsao HM, et al. Prolonged atrium electromechanical interval is associated with stroke in patients with atrial fibrillation after catheter ablation. J Cardiovasc Electrophysiol. 2013;24(4):375-380. [CrossRef]
- Inaba Y, Yuda S, Kobayashi N, et al. Strain rate imaging for noninvasive functional quantification of the left atrium: comparative studies in controls and patients with atrial fibrillation. J Am Soc Echocardiogr. 2005;18(7):729-736. [CrossRef]
- Vianna-Pinton R, Moreno CA, Baxter CM, Lee KS, Tsang TS, Appleton CP. Two-dimensional speckle-tracking echocardiography of the left atrium: feasibility and regional contraction and relaxation differences in normal subjects. J Am Soc Echocardiogr. 2009;22(3):299-305. [CrossRef]
- Kim DG, Lee KJ, Lee S, et al. Feasibility of two-dimensional global longitudinal strain and strain rate imaging for the assessment of left atrial function: a study in subjects with a low probability of cardiovascular disease and normal exercise capacity. Echocardiography. 2009;26(10):1179-1187. [CrossRef]
- Cameli M, Caputo M, Mondillo S, et al. Feasibility and reference values of left atrial longitudinal strain imaging by two-dimensional speckle tracking. Cardiovasc Ultrasound. 2009;7:6. Published 2009 Feb 8. [CrossRef]
- Cianciulli TF, Saccheri MC, Lax JA, Bermann AM, Ferreiro DE. Two-dimensional speckle tracking echocardiography for the assessment of atrial function. World J Cardiol. 2010;2(7):163-170. [CrossRef]
- Cameli M, Lisi M, Focardi M, et al. Left atrial deformation analysis by speckle tracking echocardiography for prediction of cardiovascular outcomes. Am J Cardiol. 2012;110(2):264-269. [CrossRef]
- Thomas L, McKay T, Byth K, Marwick TH. Abnormalities of left atrial function after cardioversion: an atrial strain rate study. Heart. 2007;93(1):89-95. [CrossRef]
- Wang T, Wang M, Fung JW, et al. Atrial strain rate echocardiography can predict success or failure of cardioversion for atrial fibrillation: a combined transthoracic tissue Doppler and transoesophageal imaging study. Int J Cardiol. 2007;114(2):202-209. [CrossRef]
- Schneider C, Malisius R, Krause K, et al. Strain rate imaging for functional quantification of the left atrium: atrial deformation predicts the maintenance of sinus rhythm after catheter ablation of atrial fibrillation. Eur Heart J. 2008;29(11):1397-1409. [CrossRef]
- Mirza M, Caracciolo G, Khan U, et al. Left atrial reservoir function predicts atrial fibrillation recurrence after catheter ablation: a two-dimensional speckle strain study. J Interv Card Electrophysiol. 2011;31(3):197-206. [CrossRef]
- O'Connor K, Magne J, Rosca M, Piérard LA, Lancellotti P. Left atrial function and remodelling in aortic stenosis. Eur J Echocardiogr. 2011;12(4):299-305. [CrossRef]
- O'Connor K, Magne J, Rosca M, Piérard LA, Lancellotti P. Impact of aortic valve stenosis on left atrial phasic function. Am J Cardiol. 2010;106(8):1157-1162. [CrossRef]
- Todaro MC, Choudhuri I, Belohlavek M, et al. New echocardiographic techniques for evaluation of left atrial mechanics. Eur Heart J Cardiovasc Imaging. 2012;13(12):973-984. [CrossRef]
- Nikitin NP, Witte KK, Thackray SD, Goodge LJ, Clark AL, Cleland JG. Effect of age and sex on left atrial morphology and function. Eur J Echocardiogr. 2003;4(1):36-42. [CrossRef]
- Tsai WC, Lee CH, Lin CC, et al. Association of left atrial strain and strain rate assessed by speckle tracking echocardiography with paroxysmal atrial fibrillation. Echocardiography. 2009;26(10):1188-1194. [CrossRef]
- Wang Z, Tan H, Zhong M, Jiang G, Zhang Y, Zhang W. Strain rate imaging for noninvasive functional quantification of the left atrium in hypertensive patients with paroxysmal atrial fibrillation. Cardiology. 2008;109(1):15-24. [CrossRef]
- Modesto KM, Dispenzieri A, Cauduro SA, et al. Left atrial myopathy in cardiac amyloidosis: implications of novel echocardiographic techniques. Eur Heart J. 2005;26(2):173-179. [CrossRef]
- Di Salvo G, Caso P, Lo Piccolo R, et al. Atrial myocardial deformation properties predict maintenance of sinus rhythm after external cardioversion of recent-onset lone atrial fibrillation: a color Doppler myocardial imaging and transthoracic and transesophageal echocardiographic study. Circulation. 2005;112(3):387-395. [CrossRef]
- D'Andrea A, Caso P, Romano S, et al. Association between left atrial myocardial function and exercise capacity in patients with either idiopathic or ischemic dilated cardiomyopathy: a two-dimensional speckle strain study. Int J Cardiol. 2009;132(3):354-363. [CrossRef]
- D'Andrea A, Caso P, Romano S, et al. Different effects of cardiac resynchronization therapy on left atrial function in patients with either idiopathic or ischaemic dilated cardiomyopathy: a two-dimensional speckle strain study. Eur Heart J. 2007;28(22):2738-2748. [CrossRef]
- Cameli M, Mandoli GE, Loiacono F, Sparla S, Iardino E, Mondillo S. Left atrial strain: A useful index in atrial fibrillation. Int J Cardiol. 2016;220:208-213. [CrossRef]
- Yoon YE, Kim HJ, Kim SA, et al. Left atrial mechanical function and stiffness in patients with paroxysmal atrial fibrillation. J Cardiovasc Ultrasound. 2012;20(3):140-145. [CrossRef]
- Laish-Farkash A, Perelshtein Brezinov O, Valdman A, et al. Evaluation of left atrial remodeling by 2D-speckle-tracking echocardiography versus by high-density voltage mapping in patients with atrial fibrillation. J Cardiovasc Electrophysiol. 2021;32(2):305-315. [CrossRef]
- Lisi M, Mandoli GE, Cameli M, et al. Left atrial strain by speckle tracking predicts atrial fibrosis in patients undergoing heart transplantation. Eur Heart J Cardiovasc Imaging. 2022;23(6):829-835. [CrossRef]
- Lisi M, Cameli M, Mandoli GE, et al. Detection of myocardial fibrosis by speckle-tracking echocardiography: from prediction to clinical applications. Heart Fail Rev. 2022;27(5):1857-1867. [CrossRef]
- Sade LE, Keskin S, Can U, et al. Left atrial mechanics for secondary prevention from embolic stroke of undetermined source. Eur Heart J Cardiovasc Imaging. 2022;23(3):381-391. [CrossRef]
- Alhakak AS, Biering-Sørensen SR, Møgelvang R, et al. Usefulness of left atrial strain for predicting incident atrial fibrillation and ischaemic stroke in the general population. Eur Heart J Cardiovasc Imaging. 2022;23(3):363-371. [CrossRef]
- Azemi T, Rabdiya VM, Ayirala SR, McCullough LD, Silverman DI. Left atrial strain is reduced in patients with atrial fibrillation, stroke or TIA, and low risk CHADS(2) scores. J Am Soc Echocardiogr. 2012;25(12):1327-1332. [CrossRef]
- Saha SK, Anderson PL, Caracciolo G, et al. Global left atrial strain correlates with CHADS2 risk score in patients with atrial fibrillation. J Am Soc Echocardiogr. 2011;24(5):506-512. [CrossRef]
- Obokata M, Negishi K, Kurosawa K, et al. Left atrial strain provides incremental value for embolism risk stratification over CHA₂DS₂-VASc score and indicates prognostic impact in patients with atrial fibrillation. J Am Soc Echocardiogr. 2014;27(7):709-716.e4. [CrossRef]
- Park JJ, Park JH, Hwang IC, Park JB, Cho GY, Marwick TH. Left Atrial Strain as a Predictor of New-Onset Atrial Fibrillation in Patients With Heart Failure. JACC Cardiovasc Imaging. 2020;13(10):2071-2081. [CrossRef]
- Akintoye E, Majid M, Klein AL, Hanna M. Prognostic Utility of Left Atrial Strain to Predict Thrombotic Events and Mortality in Amyloid Cardiomyopathy. JACC Cardiovasc Imaging. 2023;16(11):1371-1383. [CrossRef]
- Cameli M, Lisi M, Reccia R, et al. Pre-operative left atrial strain predicts post-operative atrial fibrillation in patients undergoing aortic valve replacement for aortic stenosis. Int J Cardiovasc Imaging. 2014;30(2):279-286. [CrossRef]
- Pastore MC, Degiovanni A, Grisafi L, et al. Left Atrial Strain to Predict Postoperative Atrial Fibrillation in Patients Undergoing Coronary Artery Bypass Grafting. Circ Cardiovasc Imaging. 2024;17(1):e015969. [CrossRef]
- Zhang MJ, Ji Y, Wang W, et al. Association of Atrial Fibrillation With Stroke and Dementia Accounting for Left Atrial Function and Size. JACC Adv. 2023;2(5):100408. [CrossRef]
- Smiseth OA, Morris DA, Cardim N, et al. Multimodality imaging in patients with heart failure and preserved ejection fraction: an expert consensus document of the European Association of Cardiovascular Imaging. Eur Heart J Cardiovasc Imaging. 2022;23(2):e34-e61. [CrossRef]

Table 1.
The European Heart Rhythm Association (EHRAS) classification of atrial myopathy. [28].
Table 1.
The European Heart Rhythm Association (EHRAS) classification of atrial myopathy. [28].
| Atrial Myopathy: EHRAS classification | |
|---|---|
| EHRAS CLASS | HISTOLOGICAL FEATURES |
| I | Morphological/molecular changes affecting the cardiomyocytes (hypertrophy and myocytolysis). Absence of significant tissue fibrosis or interstitial changes |
| II | Predominance of fibrotic changes. Normal appearance of cardiomyocytes |
| III | Combination of changes in the cardiomyocyte and tissue fibrosis |
| IV a f i o |
Non-fibrotic alteration of interstitial matrix Amyloid accumulation Fatty infiltration Inflammatory cells Other interstitial alterations |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



