
Submitted:
17 April 2024
Posted:
17 April 2024
You are already at the latest version
Abstract
Background: The aim of this audit is to evaluate the characteristics of dental infections requiring hospitalisations, which may help improve preventative and management policies.
Methods: This study retrospectively evaluated the patients’ records admitted to a public hospital due to dental infections between 2018 and 2019.
Results: A total of 102 patients, mostly in thirties with equal gender distribution were admitted with dental infections, presenting with pain (100%), swelling (99%), Trismus (40.2%), dysphagia (27.4%), fever (21%) >37°C, Tachycardia (24.75%) and Tachypnoea (9.3%). Most patients presented (68%) on weekends, outside regular working hours and public holidays. 54 (52.5%) patients had taken prior antibiotics. Dental Caries, smoking, mental health issues and illicit drug use were featured strongly. The majority of patients (56.4%) underwent treatment under local anaesthesia. The total length of hospital stay was 271 days (mean 2.66). Augmentin was the most prescribed antibiotics. Complications were reported in 8.8% patients, primarily related to airway compromise.
Conclusion:
Dental infections leading to hospitalizations continue to be a burden on the healthcare system. A notable finding was the presentations primarily on weekends, outside regular hours and public holidays and the majority requiring dental intervention under local anaesthesia. Provision of on call emergency dental services may reduce length of hospital stay and admissions.
Keywords:
Dental Caries
; Dental Infection
; Odontogenic Infection
; Hospitalisation
; Morbidity
1. Introduction
Dental infection, often referred to as odontogenic infection, is an infection of the alveolus, jaws, or face originating from bacterial invasion of endodontic or periodontal tissues [1]. Etiological factors include dental caries, periodontal infections, pericoronitis, failed endodontic treatments, dental trauma, severe dental attrition, and infected dental cysts [2]. The preventable and treatable nature of these underlying causes emphasizes the importance of timely dental interventions [3]. Without appropriate dental treatment, these conditions may lead to periapical and periodontal abscesses [4]. Advancements in dental science have facilitated the successful treatment of localized dental infections within outpatients setting in dental clinics [5]. However, if left untreated, dental infections can result in severe and potentially life-threatening infections, necessitating hospitalization [6]. In a hospital setting, the management of dental infections often involves surgical intervention under general anaesthesia. This involves removing the infection source and performing surgical incisions with intraoral and/or extraoral drainage and the administration of intravenous antibiotics and supportive care [7,8].
Dental infections resulting in hospitalisation pose a substantial risk to oral health related morbidity and mortality and is a significant burden on public health in the form of potentially preventable hospitalisations [9]. Complications arising from dental infections encompass a wide spectrum, ranging from maxillary sinusitis and osteomyelitis to more severe conditions like Ludwig’s angina leading to airway compromise, and even systemic complications such as septicaemia and septic shock [10]. Dental infection has been reported to be the most common cause of oral health related preventable hospitalisations [11]. Studies have highlighted the considerable financial impact, with reported average hospital costs ranging from $12,228 (Australia) to $47,835 (United States) per patient [12,13].
Recognizing that dental caries and periodontal diseases are preventable and treatable conditions emphasizes the importance of early dental interventions. Proactive oral health related management strategies can mitigate complications and reduce the incidence of preventable hospitalizations [14]. A recent systematic review underscored the need for comprehensive data collection to guide evidence-based policies for the prevention and management of dental infections [11]. In line with this imperative, the current study aims to evaluate the characteristics of patients presenting with dental infections requiring hospitalisations to the emergency department of a major public hospital in Australia to identify patterns which may help improve preventative and management policies.
2. Materials and Methods
2.1. Ethical Application
Human research ethics application (2020/ETH01100) was accepted on 14 June 2020. The site-specific assessment application (2020/STE01811) was accepted on 2 September 2020.
2.2. Patient Selection
This study evaluated records of patients admitted to Nepean Hospital Kingswood NSW 2747 Australia for the management of dental infections in 12 months (July 2018-June 2019), pre covid period. The study population included all the patients presenting to emergency department (ED) of Nepean hospital with dental infections requiring hospitalisations during the study period. Key inclusion criteria included inpatients, without age restriction, presenting with dental infections or post operative dental infections to ED of Nepean Hospital requiring hospitalisation during the study period. Key exclusion criteria included outpatients presenting with dental infections not requiriing hospitalisations, inpatients and outpatients presenting with oral health related emergeny patients other than dental infections and non-oral health related emergency patients presenting to ED of Nepean Hospital.
Patients were identified retrospectively from the excel data provided by the emergency department of the Nepean hospital. Using the excel option ‘sort and filter’, the data was screened for oral health related presentations using various key words. The key words used for screening of patients with dental infections requiring hospitalisation included teeth, tooth, dental, mouth, jaw, facial, neck, maxilla and mandible combined with pain, odontalgia, infection, abscess and swelling, and hospital admission. Patient’s specific data was accessed on medical record software ‘PowerChart’ using patient’s specific medical records number (MRN). According to the International Classification of Disease, revision 11 (ICD-11), code DA09.6, dental infections leading to dental abscesses were identified from patient record which required hospitalisation.
2.3. Date Collection
Deidentified data related to outcome measurement was transferred to Microsoft Excel Software for further analysis. Data was collected for each individual patient for the following variables. Date and time of presentation, age, gender, Aboriginal and Torres Strait Islander status, smoking, comorbidities, BMI, clinical features, vital signs, facial space involvement, aetiology, jaw and teeth involvement, Investigation, treatment, previous treatment, hospital stay, culture and sensitivity/microbiology and outcome.
2.4. Data Analysis
The data was rearranged in Microsoft Excel for each measurement, and subsequent analysis was performed utilizing various function. Following the analysis, the data was transferred into a table format in Microsoft Word. Additionally, graphs and figures were generated using Microsoft Excel.
3. Results
A total of 102 patients were admitted with dental infections, presenting with pain (100%), swelling (99%), Trismus (40.2%), dysphagia (27.4%), fever (21%) [>37°C], and Tachycardia (24.75%) and Tachypnoea (9.3%). Most patients (68.6%) requiring hospitalisations presented on weekends, out of regular working hours and public holidays (Figure 1).
Previous treatment related to the presentations was reported in 68 cases (66.7%); notably empirical antibiotic prescription in 54 cases (52.9%) predominantly by the medical practitioners (74%) (Table 1) (Figure 2). Most patients (40) received prescription of antibiotics within 7 days, only 11 had taken antibiotics more than 7 days prior to presentation. There were no gender differences. The mean age of study group was 40.14 years while highest presentations were reported in thirties (Figure 3). Smoking was reported in 51.96% patients. Fifty one percent of the patients reported medical comorbidity before admission; 34.2 % reported mental health issues, 23.3% reported use of illicit drugs use, 5 patients reported diabetes mellitus, 4 patients reported hepatitis C and 10 patients reported allergy to penicillin (Table 2). The main clinical features were pain and facial swelling; however, trismus and dysphagia were reported in 40.2% and 27.4% patients respectively (Table 3).
Abnormal vales for vital signs included high breathing rate (20 plus breaths per minute) in 8 patients, tachycardia in 25 patients, hypertension (140mm HG plus systolic blood pressure) in 28 patients, elevated temperature (>37°C) in 21 patients, higher blood sugar level (12 mmole or more) in 3 patients which were all diabetic (Table 3). Sixty four percent patient presented with 2 or more facial space involvement; buccal (44.9%), Canine (17.6%), Submandibular (13.6%) (Table 4). Dental caries was the main aetiological factor (62.74%) and common teeth involved were molar teeth (40.9%) (Table 5). Elevated value of white blood cells count was reported in 51.64% cases (more than 11x109/L) and C -reactive protein in 78.08% (more than 10mg/L). The most common imaging modality was OPG (89.2%) while contrast CT (73.5%) was used to investigate inflammatory changes (100%) and abscesses (25.3%) (Table 5).
Surgical management was performed in 76.5% cases including extractions (61.8%) mainly under local anaesthesia (56.4%) in the dental clinic, while incision and drainage were mainly intra oral, required in 38 patients. Augmentin was administered as the main antibiotic for both intravenous (69.6%) in hospital and discharge prescriptions (79.4%). Total length of hospital stay was 271 days (mean: 2.66) including 15 days in intensive care unit (Table 6). Specimens were collected for microbiological examinations in 31 patients with positive culture growth in 19 cases predominantly normal oral flora, mostly gram-positive polymorphs and cocci. The associated complications (8.8%) were mainly related to airway compromise (5 patients) with no long-term complication and mortality (Table 7).
4. Discussion
Dental infections requiring hospitalization not only present with significant morbidity and occasional mortality, but also carry significant financial implications for both patients and healthcare systems. Our study sheds light on various aspects of these infections, including their temporal patterns, patient demographics, clinical characteristics, diagnostic approaches, management strategies, and clinical outcomes.
Temporal patterns of presentation reveal a concerning trend, with a majority of dental infections (two-thirds) presenting to public hospital during weekends, out of regular work hours, and on public holidays. Similar patterns have been observed elsewhere, with likely causes attributed to factors such as the limited availability of dentists during these hours, patient education, anxiety and cost concerns [15]. This distribution can lead to increased strain on emergency healthcare services, potentially leading to longer wait times and preventable hospitalizations. Australia’s national health insurance scheme, Medicare, excludes the adult population from dental care, leaving a gap in access to essential services [16]. Consequently, adult patients with dental infections seek dental consultations from general practitioners or presenting to public hospital for treatment. In this study, a large proportion of patients (53%) received empirical antibiotics prescription mainly from general medical practitioners, a finding consistent with previous studies (33-75%) [17,18]. The prevalent prescription of antibiotics without active dental treatment by general practitioners is alarming [19]. The inappropriate use of empirical antibiotic prescription without active dental interventions, can lead to antimicrobial resistance, increase morbidity and mortality, potential adverse reactions, drug interactions and increase healthcare expenditure [20,21].
This study observed an equal distribution of gender presentations, which contrasts with the findings from previous Australian studies reporting predominantly male populations with dental infections requiring hospitalizations. However, the highest presentations of dental infections occurring in the 4th decade of life, a demographic often actively involved in workforce, aligns with both Australian and global data [7,22,23,24,25,26,27]. The prevalence of comorbid conditions such as smoking, illicit drug use and mental health issues is consistent with findings from other studies [11]. Individuals with these conditions are at elevated risk of dental caries and periodontal disease, and are less likely to seek preventative dental care [28].
The clinical presentations of dental infections characterized by severe pain and sudden facial swelling seem to be the main trigger for patients seeking emergency services although trismus and dysphagia were reported in 40% and 27% patients respectively, mainly associated with those originating in mandibular teeth. Abnormal values of vital signs were observed in a small proportion of patient presentations with dental infections (febrile 3%, tachycardia 8% and tachypnoea 24.75%), indicating limited systemic involvement and disease severity. The number of patients presenting with abnormal white blood cell counts and C-Reactive protein reported in this study were comparable with others reports [29].
The majority of dental infections were of pulpal origin followed by periodontitis and pericoronitis, consistent with findings from other studies [11]. Notably, while all teeth were involved, molars teeth (40.9%) including third molar teeth (9.8%), were predominantly presented. The anatomical position of lower molar teeth leading to trismus, dysphagia and airway complications, aligns with the findings of our study [1]. The spread of the dental infection frequently involves multiple spaces, notable buccal, canine space and submandibular, resulting in facial swelling, triggering emergency hospital presentation. In this study, contrast computed tomography was employed in 75 patients revealing a frank collection of abscesses in 19 (25.3%) cases only mostly requiring procedures under general anaesthesia in hospital setup. A significant proportion of inpatients (44 out of 78 patients) were referred to the nearby teaching dental hospital, ‘Nepean Centre for Oral Health’, for procedures under local anaesthesia, which provides dental services during working hours on weekdays to eligible patients. Although, the antibiotic of choice was Augmentin, change of antibiotic was required in 5 patients (definitive antibiotics) due to resistant bacterial strains.
The mean length of hospital stay (2.66 days) and total intensive care unit days (15 days) were both less than those reported in our previous published study [11]. Likewise, the absence of mortality and relatively less complications, primarily related to airway compromise resulting from dental infections represents a favourable outcome compared to previous reports [11]. Despite favourable clinical outcomes observed in our study, the financial impact of odontogenic infections remains a significant concern.
The limitations of the study include small size of the cohort and single centre study. There is some heterogenicity in data reporting as some data is missing or not reported for some patients. Nonetheless, to the best of our knowledge, this is the first study in NSW, the most populated state of Australia, investigating the presentations of dental infections in human population of all age group requiring hospitalisations.
5. Conclusions
In conclusion, this study provides important information about the characteristics, management and trends of dental infections leading to potentially preventable hospitalizations, which continue to be a significant burden on the public healthcare system. A notable finding was the highest presentations of dental infections requiring hospitalisations to the emergency department of Nepean hospital on weekends, outside regular work hours and public holidays, predominantly requiring dental interventions under local anaesthesia. The provision of emergency or on call dental services on weekends, outside regular work hours and public holidays may help reduce the number of potentially preventable hospitalizations and the length of hospital stay. Although, this study provides some insight to dental infections requiring hospitalizations in the limited Australian literature, more nationwide studies with a larger population and statistical co relations between various characteristics and length of hospital stay are required to help guide preventative policies.
Author Contributions
Mafaz Ullah: Conceptualization, methodology, software, validation, formal analysis, investigation, resources, data curation, writing—original draft preparation, writing—review and editing, visualization, project administration. Muhammad Irshad: Resources, writing—review and editing. Albert Yaaccoub: Project administration, writing—review and editing. Eric Carter: writing—review and editing. Stephen Cox: Conceptualization, writing—review and editing, supervision.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Institutional Review Board Statement
The study was approved by the Human Research Ethics Committee (HREC) for Nepean Blue Mountains LHD on studies involving humans. Human research ethics application (2020/ETH01100) was accepted on 14 June 2020. The site-specific assessment application (2020/STE01811) was accepted on 2 September 2020.
Informed Consent Statement
Retrospective clinical audit (Anonymous data)
References
- Ogle, O.E. and L.R. Halpern, Odontogenic Infections: Anatomy, Etiology, and Treatment. Oral and Maxillofacial Surgery, Medicine, and Pathology for the Clinician, 2023: p. 227-241.
- Ogle, O.E., Odontogenic infections. Dental Clinics, 2017. 61(2): p. 235-252.
- Islam, B., S.N. Khan, and A.U. Khan, Dental caries: from infection to prevention. Medical Science Monitor, 2007. 13(11): p. RA196-RA203.
- Prakash, S.K., Dental abscess: A microbiological review. Dental research journal, 2013. 10(5): p. 585.
- López-Píriz, R., L. Aguilar, and M.J. Giménez, Management of odontogenic infection of pulpal and periodontal origin. Medicina Oral, Patología Oral y Cirugía Bucal (Internet), 2007. 12(2): p. 154-159.
- Rastenienė, R.; Pūrienė, A.; Aleksejūnienė, J.; Pečiulienė, V.; Zaleckas, L. Odontogenic Maxillofacial Infections: A Ten-Year Retrospective Analysis. Surg. Infect. 2015, 16, 305–312, . [CrossRef]
- Nadig, K.; Taylor, N.G. Management of odontogenic infection at a district general hospital. Br. Dent. J. 2018, 224, 962–966, . [CrossRef]
- Bowe, C.M.; O’neill, M.A.; O’connell, J.E.; Kearns, G.J. The surgical management of severe dentofacial infections (DFI)—a prospective study. Ir. J. Med Sci. (1971 -) 2018, 188, 327–331, . [CrossRef]
- Allareddy, V., et al., Hospitalizations primarily attributed to dental conditions in the United States in 2008. Oral surgery, oral medicine, oral pathology and oral radiology, 2012. 114(3): p. 333-337.
- Neal, T.W.; Schlieve, T. Complications of Severe Odontogenic Infections: A Review. Biology 2022, 11, 1784, . [CrossRef]
- Ullah, M.; Irshad, M.; Yaacoub, A.; Carter, E.; Thorpe, A.; Zoellner, H.; Cox, S. Dental Infection Requiring Hospitalisation Is a Public Health Problem in Australia: A Systematic Review Demonstrating an Urgent Need for Published Data. Dent. J. 2023, 11, 97, . [CrossRef]
- Han, J.; Liau, I.; Bayetto, K.; May, B.; Goss, A.; Sambrook, P.; Cheng, A. The financial burden of acute odontogenic infections: the South Australian experience. Aust. Dent. J. 2019, 65, 39–45, . [CrossRef]
- Neal, T.W.; Hammad, Y.; Carr, B.R.; Schlieve, T. The Cost of Surgically Treated Severe Odontogenic Infections: A Retrospective Study Using Severity Scores. J. Oral Maxillofac. Surg. 2022, 80, 897–901, . [CrossRef]
- Ozdemir, D. Dental Caries : The Most Common Disease Worldwide and Preventive Strategies. Int. J. Biol. 2013, 5, p55, . [CrossRef]
- Verma, S.; Chambers, I. Dental emergencies presenting to a general hospital emergency department in Hobart, Australia. Aust. Dent. J. 2014, 59, 329–333, . [CrossRef]
- Biggs, A., Overview of Commonwealth involvement in funding dental care. 2008.
- Fu, B.; McGowan, K.; Sun, H.; Batstone, M. Increasing Use of Intensive Care Unit for Odontogenic Infection Over One Decade: Incidence and Predictors. J. Oral Maxillofac. Surg. 2018, 76, 2340–2347, . [CrossRef]
- Michael, J.A.; Hibbert, S.A. Presentation and management of facial swellings of odontogenic origin in children. Eur. Arch. Paediatr. Dent. 2014, 15, 259–268, . [CrossRef]
- Cope, A.L.; Chestnutt, I.G.; Wood, F.; A Francis, N. Dental consultations in UK general practice and antibiotic prescribing rates: a retrospective cohort study. Br. J. Gen. Pr. 2016, 66, e329–e336, . [CrossRef]
- Liau, I.; Han, J.; Bayetto, K.; May, B.; Goss, A.; Sambrook, P.; Cheng, A. Antibiotic resistance in severe odontogenic infections of the South Australian population: a 9-year retrospective audit. Aust. Dent. J. 2018, 63, 187–192, . [CrossRef]
- Sundararajan, K., et al., Morbidity and mortality in patients admitted with submandibular space infections to the intensive care unit. Anaesthesia & Intensive Care, 2015. 43(3): p. 420-2.
- Fehrenbach, M.J. and S.W. Herring, Spread of dental infection. Practical Hygiene, 1997. 6: p. 13-19.
- Mathew, G.C.; Ranganathan, L.K.; Gandhi, S.; Jacob, M.E.; Singh, I.; Solanki, M.; Bither, S. Odontogenic maxillofacial space infections at a tertiary care center in North India: a five-year retrospective study. Int. J. Infect. Dis. 2012, 16, e296–e302, . [CrossRef]
- Robertson, D.P.; Keys, W.; Rautemaa-Richardson, R.; Burns, R.; Smith, A.J. Management of severe acute dental infections. BMJ 2015, 350, h1300–h1300, . [CrossRef]
- Bridgeman, A.; Wiesenfeld, D.; Hellyar, A.; Sheldon, W. Major maxillofacial infections. An evaluation of 107 cases. Aust. Dent. J. 1995, 40, 281–288, . [CrossRef]
- Fu, B.; McGowan, K.; Sun, J.; Batstone, M. Increasing frequency and severity of odontogenic infection requiring hospital admission and surgical management. Br. J. Oral Maxillofac. Surg. 2020, 58, 409–415, . [CrossRef]
- Uluibau, I.; Jaunay, T.; Goss, A. Severe odontogenic infections. Aust. Dent. J. 2005, 50, S74–S81, . [CrossRef]
- Kisely, S.; Baghaie, H.; Lalloo, R.; Siskind, D.; Johnson, N.W. A Systematic Review and Meta-Analysis of the Association Between Poor Oral Health and Severe Mental Illness. Psychosom. Med. 2015, 77, 83–92, doi:10.1097/psy.0000000000000135.
- Kusumoto, J.; Iwata, E.; Huang, W.; Takata, N.; Tachibana, A.; Akashi, M. Hematologic and inflammatory parameters for determining severity of odontogenic infections at admission: a retrospective study. BMC Infect. Dis. 2022, 22, 1–11, . [CrossRef]
Figure 1.
Percentage of cases based on time of presentations.
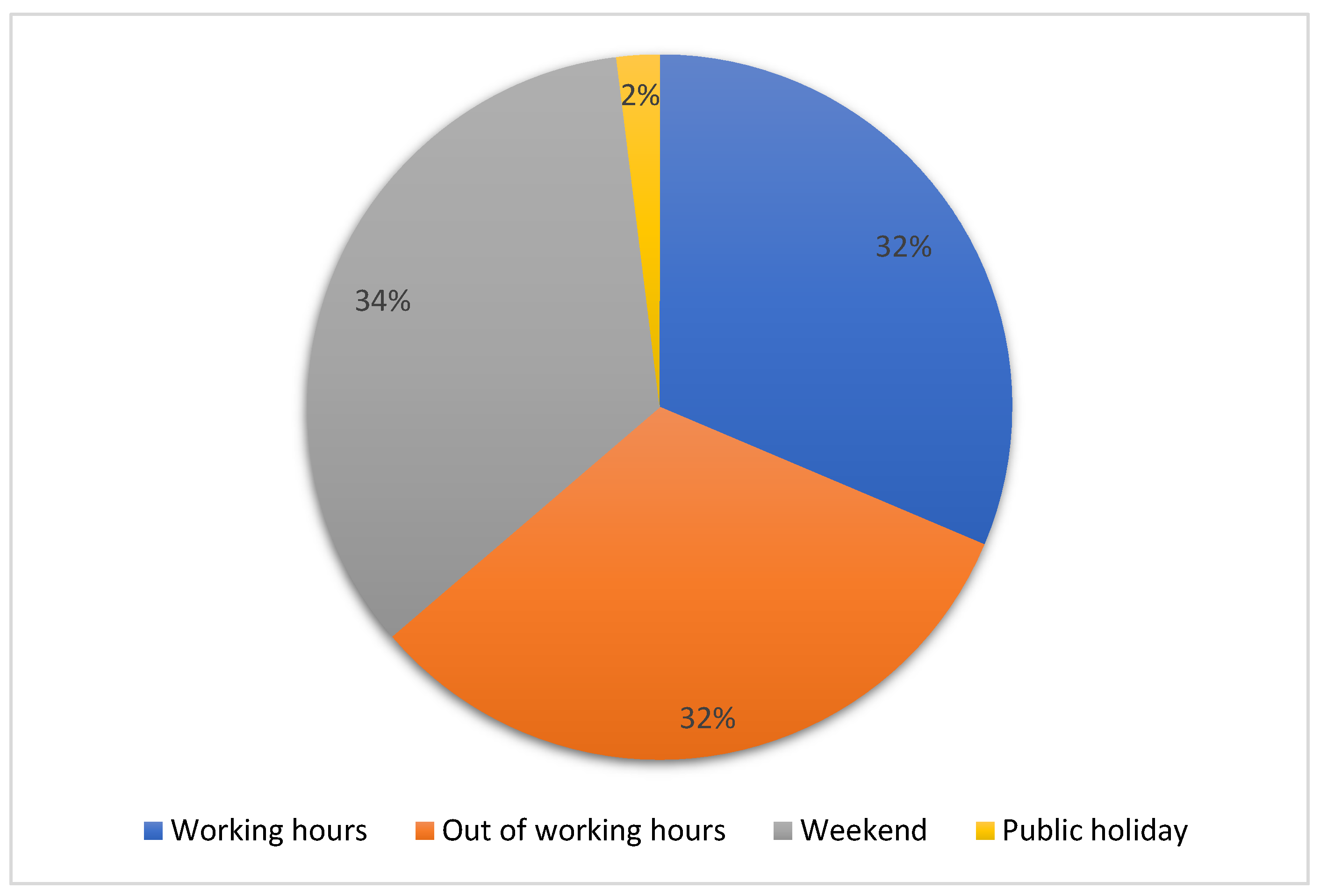
Figure 2.
Percentage of cases with empirical antibiotics prescription prior to presentations.
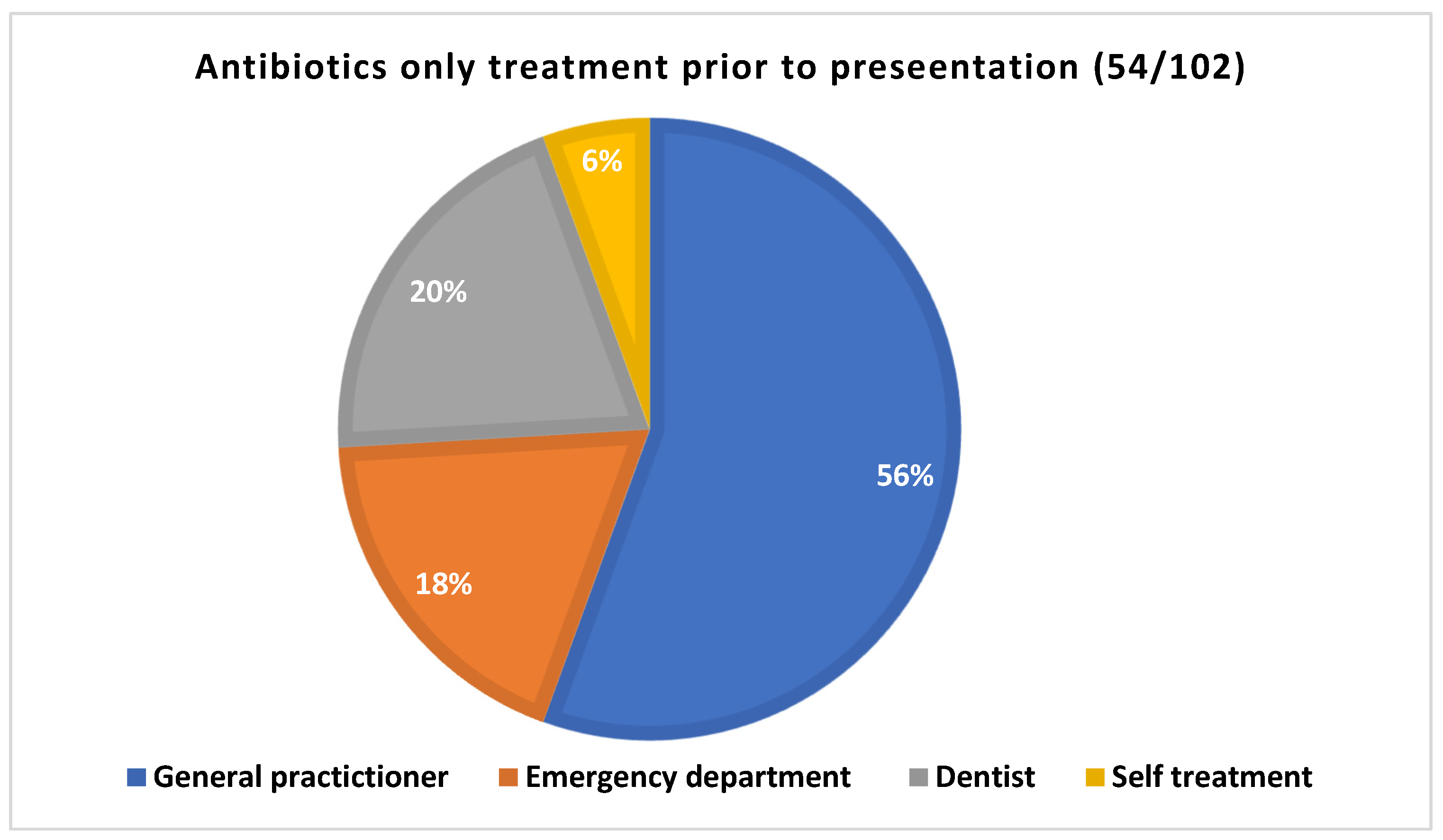
Figure 3.
Patient distribution based on gender and age.
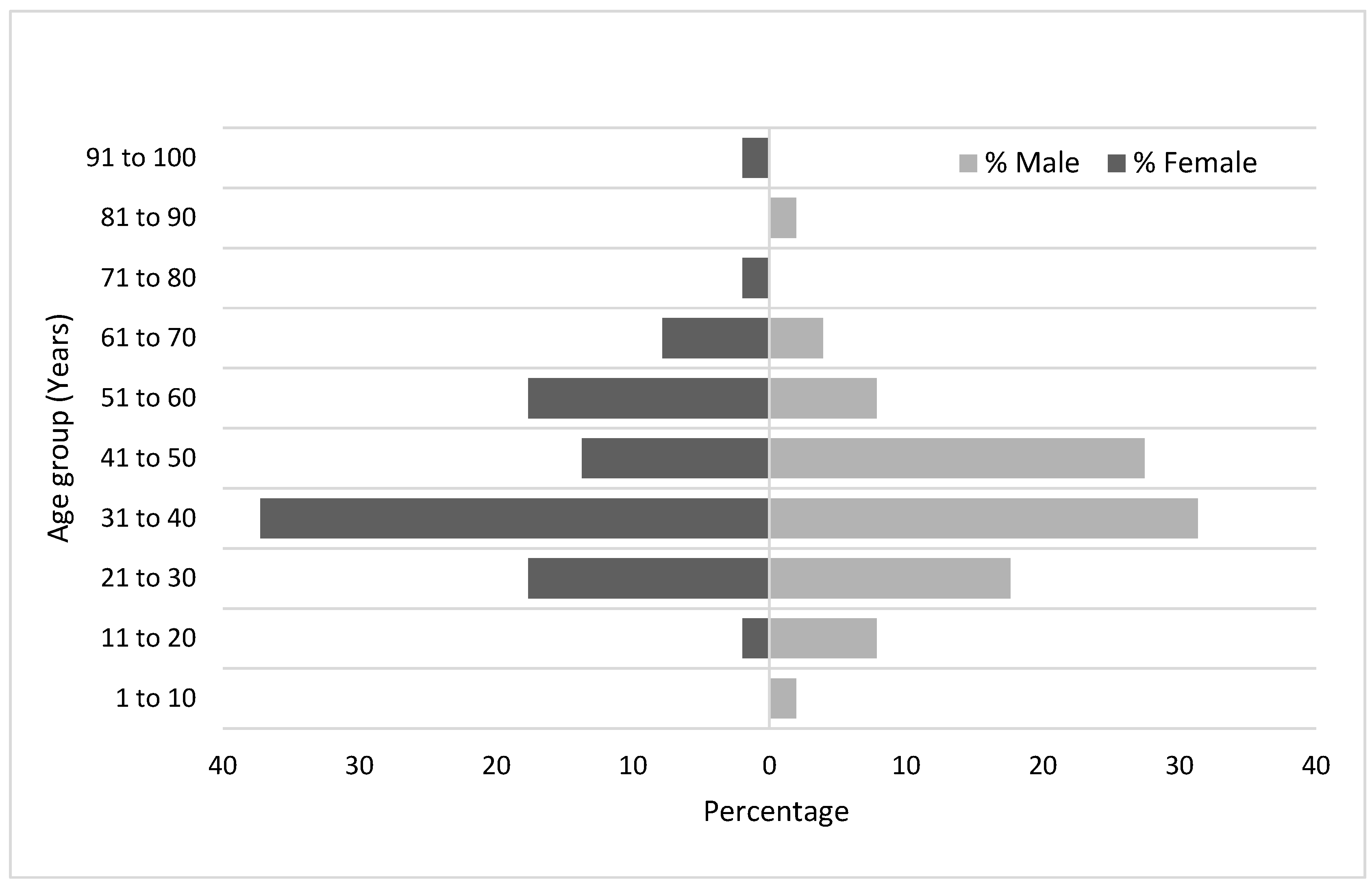

Table 1.
Treatment prior to ED presentations.
| Previous treatment | 68 (66.7%) | |
| Antibiotics only | 54 (52.9%) | |
|
Time of prescription (n=51) |
More than a week | 11 |
| Less than a week | 40 | |
| Two or more than two prescriptions | 11 | |
| Dental treatment | Extractions +/- Antibiotics | 12 |
| Pulp extirpations +/- Antibiotics | 8 | |
|
Type of antibiotics prescribed prior to presentations (Multiple prescriptions were reported in 11 cases) |
Augmentin | 19 |
| Augmentin plus metronidazole | 1 | |
| Amoxicillin | 15 | |
| Amoxicillin plus Metronidazole | 5 | |
| Keflex | 2 | |
| Cephalexin | 1 | |
| Cephalexin plus metronidazole | 1 | |
| Clindamycin | 1 | |
| Clindamycin plus metronidazole | 1 | |
| Flucloxacillin plus metronidazole | 1 | |
| metronidazole | 1 | |
Table 2.
Demographic Information and Associated Comorbidities.
| Gender | M | 51 (50%) |
| F | 51 (50%) | |
| Age (Years) | Mean | 40.14 |
| Median | 37.5 | |
| Range | 6 to 93 | |
| Country of Birth | Australia | 84 (82.35 %) |
| Overseas | 18 (17.65 %) | |
| Aboriginality status | Aboriginal or Torres straits islanders | 7 (6.86 %) |
| Smoking status | Smokers | 53 (51.96 %) |
| Non-smokers | 49 (48.04 %) | |
| Smoking Frequency (cigarette per day) | Mean | 3-30 |
| Range | 13.62 | |
| Co-morbidity (n=52) | Mental Health Issues | 25 (34.2%) |
| Drug Use | 17 (23.3%) | |
| Allergy to penicillin | 10 (13.7%) | |
| Diabetes mellitus | 5 (6.8%) | |
| Hepatitis C | 4 (5.5%) | |
| Cancer | 2 (2.7%) | |
| Fatty liver | 2 (2.7%) | |
| Myocardial infarction | 1 (1.7%) | |
| Cardiomyopathy | 1 (1.7%) | |
| COPD | 1 (1.7%) | |
| Epilepsy | 1 (1.7%) | |
| Osteoporosis | 1 (1.7%) | |
| Crohn’s disease | 1 (1.7%) | |
| Heavy alcohol | 1 (1.7%) | |
| Hypothyroid | 1 (1.7%) | |
| BMI (n=89) | Mean | 29.9 |
| Median | 29.14 | |
| Range | 16.59 to 75.99 |
Table 3.
Clinical Features.
| Pain (n=102) | 101 (99 %) | |
| Facial Swelling (n=102) | 102 (100 %) | |
| Trismus (n=102) | 41 (40.2 %) | |
| Dysphagia (n=102) | 28 (27.4 %) | |
| Respiratory rate (n=86) (Number of breathings pre minute) |
Mean | 18.49 |
| Median | 18 | |
| Range | 14-31 | |
| >20 | 8 | |
| Oxygen Saturation (%) (n=100) | Mean | 97.6 |
| Median | 98 | |
| Range | 95-100 | |
| Pulse Rate (n=101) | Mean | 91.16 |
| Median | 89 | |
| Range | 61-165 | |
| >100 | 25 | |
| Systolic blood pressure (mm Hg) (n=96) |
Mean | 132.51 |
| Median | 130 | |
| Range | 102-189 | |
| >140 | 28 | |
| Diastolic blood pressure (n=95) (mm Hg) | Mean | 81.97 |
| Median | 82 | |
| Range | 52-114 | |
| >90 | 13 | |
| Mean Arterial pressure (n=94) ) (mm Hg) | Mean | 97.65 |
| Median | 98 | |
| Range | 39.4-125 | |
| >100 | 39 | |
| Temperature (°C) (n=100) | Mean | 36.64 |
| Median | 36.6 | |
| Range | 35.5-39.2 | |
| 37.1-38 | 18 | |
| >38 | 3 | |
| Random blood sugar level (mmol/L) Nondiabetic patients (n=62) |
Mean | 5.27 |
| Median | 5.25 | |
| Range | 3.7-7.2 | |
| Random blood sugar level (mmol/L) Diabetic patients (n=4) |
Mean | 15.7 |
| Median | 17.15 | |
| Range | 5-23.5 | |
Table 4.
Facial Space Involvement.
|
1 space (n=37) (36%) |
Buccal | 27 | |||||
| Canine | 8 | ||||||
| Sub-masseteric | 1 | ||||||
| Lower lip | 1 | ||||||
| 2 spaces (n=40) (39%) | Buccal | Submandibular | 11 | ||||
| Buccal | Canine | 8 | |||||
| Buccal | Maxillary sinus | 7 | |||||
| Canine | Upper lip | 3 | |||||
| Canine | Orbital | 3 | |||||
| Buccal | Masticator | 2 | |||||
| Buccal | Palatal | 1 | |||||
| Buccal | Sublingual | 1 | |||||
| Buccal | sub masseteric | 1 | |||||
| Submandibular | Submental | 1 | |||||
| Submandibular | Masticator | 1 | |||||
| Submental | Lower lip | 1 | |||||
|
3 spaces (n=21) (21%) |
Canine | Buccal | Maxillary sinus | 4 | |||
| Canine | Buccal | Upper lip | 4 | ||||
| Buccal | Submandibular | Masticator | 2 | ||||
| Submandibular | Masticator | Pharyngeal | 2 | ||||
| Buccal | Sub-masseteric | Pharyngeal | 1 | ||||
| Buccal | Sub-masseteric | Submandibular | 1 | ||||
| Buccal | Sub-masseteric | Masticator | 1 | ||||
| Buccal | Sub-masseteric | Maxillary sinus | 1 | ||||
| Buccal | Sublingual | Submandibular | 1 | ||||
| Buccal | Sublingual | Submental | 1 | ||||
| Buccal | Maxillary sinus | Orbital | 1 | ||||
| Buccal | Canine | Orbital | 1 | ||||
| Sublingual | Submandibular | Masticator | 1 | ||||
| ≥ 4 spaces (n=4) (4%) | Buccal | Sublingual | Submandibular | Pharyngeal | 1 | ||
| Sublingual* | Submandibular* | Submental | Sub-masseteric | 1 | |||
| Canine | Buccal space | Maxillary sinus | Orbital | 1 | |||
| Buccal | Submandibular | Masticator | Pharyngeal | 1 | |||
| Total | 102 | ||||||
*Bilateral involvement in Ludwig’s angina.
Table 5.
Aetiology and Investigations.
| Aetiology (n=102) | Dental caries (n=64) | Un-restored caries | 46 (45.5%) |
| Retained roots caries | 14 (13.9%) | ||
| Restored caries | 3 (3%) | ||
| Periapical cyst | 1 (1%) | ||
| Periodontal origin (n=10) | Pericoronitis | 6 (5.9%) | |
| Periodontal abscess | 4 (4%) | ||
| Post extraction | 13 (12.9%) | ||
| Post pulp extirpation | 8 (7.9%) | ||
| Failed root canal treatment | 4 (4%) | ||
| Occlusal wear | 2 (2%) | ||
| Tooth fracture | 1 (1%) | ||
| Jaw Involvement | Upper jaw (Maxilla) | 49 (48%) | |
| Lower jaw (Mandible) | 53 (52%) | ||
| Jaw side involvement | Right | 50 (49%) | |
| Left | 52 (51%) | ||
|
Teeth involvement (Some cases had multiple teeth involved) |
Anterior teeth | Incisor teeth | 19 (15.6%) |
| Canine teeth | 13 (10.6%) | ||
| Premolar teeth | 39 (32%) | ||
| 1st and 2nd molar teeth | 38 (31.1%) | ||
| 3rd molar teeth | 12 (9.8%) | ||
| Deciduous teeth | 1 (0.8 %) | ||
| Investigations | White blood cell count (n=91) (Valuex109/L) |
Mean | 11.16 |
| Median | 11.2 | ||
| Range | 1.5-20.8 | ||
| Less than 4 | 1 | ||
| 4 to 11 | 43 | ||
| More than 11 | 47 | ||
| C-reactive protein (n=73) (mg/L) | Mean | 47.71 | |
| Median | 35 | ||
| Range | 3-186 | ||
| 3 to 10 | 16 | ||
| More than 100 | 8 | ||
| Imaging | Orthopantomogram | 91 (89.2%) | |
| Contrast CT | 75 (73.5%) | ||
| Contrast CT results (n=75) | Inflammatory changes | 75 (100%) | |
| Frank collection | 19 (25.3%) | ||
Table 6.
In-patient Management and Length of Hospital Stay.
| Management | Non-surgical management (antibiotics only) | 24 (23.5%) | |
| Surgical management | 78 (76.5%) | ||
| Anaesthesia | LA (Dental facility-NCOH) | 44 (56.4%) | |
| GA (Hospital Facility) | 34 (43.6%) | ||
| Surgical options | Extractions | 63 (61.8%) | |
| Incision and drainage (n=38) (37.2%) |
Intra oral | 33 (32.3%) | |
| Extra oral | 1 (1%) | ||
| Combined | 4 (3.9%) | ||
| Pulp extirpation | 4 (3.9) | ||
| Referral to dentist for extraction or pulp extirpation | 11 (10.8%) | ||
| Intravenous antibiotics (n=102) | Augmentin alone | 71 (69.6%) | |
| Augmentin plus metronidazole | 14 (13.7%) | ||
| Benzylpenicillin plus metronidazole | 4 (3.9%) | ||
| Clindamycin | 3 (2.9%) | ||
| Clindamycin plus metronidazole | 4 (3.9%) | ||
| Metronidazole alone | 1 (1%) | ||
| Ceftriaxone | 1 (1%) | ||
| Bactrim plus metronidazole | 1 (1%) | ||
| Cephazolin | 1 (1%) | ||
| Cephazolin plus metronidazole | 1 (1%) | ||
| Augmentin plus metronidazole, BenPen PICC line | 1 (1%) | ||
| Change of Intravenous antibiotics | 5 | ||
| Consultation with infectious disease specialist | 2 | ||
| Antibiotic on discharge (n=97) |
Augmentin | 77 (79.4%) | |
| Augmentin plus metronidazole | 4 (4.1%) | ||
| Amoxicillin plus metronidazole | 2 (2%) | ||
| Benzylpenicillin plus metronidazole | 2 (2%) | ||
| Clindamycin | 5 (5.1%) | ||
| Clindamycin plus metronidazole | 3 (3.1%) | ||
| Bactrim plus metronidazole | 1 (1%) | ||
| Metronidazole | 1 (1%) | ||
| Keflex | 1 (1%) | ||
| Keflex plus metronidazole | 1 (1%) | ||
| Length of hospital stay (days) | Total days | 271 | |
| Ward days | 256 | ||
| Intensive care unit days | 15 | ||
| Mean | 2.66 | ||
| Median | 2 | ||
| Range | 1-8 | ||
Table 7.
Microbiology and Morbidity.
| Microbiological Studies | Swab culture | 31 |
| Blood culture | 1 | |
| PCR | 2 | |
| Culture Growth | No Growth | 12 |
| Growth | 19 | |
|
Microorganisms Isolated |
Normal flora | 12 |
| Streptococcus Milleri group | 4 | |
| Candida | 4 | |
| Staph aureus | 2 | |
| Staph epidermis | 1 | |
| Lactobacilli | 1 | |
| Streptococcus oralis | 1 | |
| Viridin group of streptococci | 1 | |
| Yeast cells | 1 | |
|
Susceptibility test (n=3) |
Staph aureus | 2 |
| Strep Milleri group | 1 | |
| Resistance to penicillin | 2 | |
|
Gram staining (n=14) |
G+ve polymorphs | 14 |
| G+ve Cocci | 10 | |
| G+ve Rods | 5 | |
| G-ve Rods | 1 | |
| Complications | Airway related complications | 5 |
| Eye related complication (blurred vision, Diplopia) | 1 | |
| Osteomyelitis | 1 | |
| Severe hypotension | 1 | |
| Hardware infection | 1 | |
| Mortality | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



