
Submitted:
11 April 2024
Posted:
17 April 2024
You are already at the latest version
Abstract
Background: Metastatic triple-negative breast cancer (TNBC) is aggressive with a poor median overall survival (OS), ranging from 8 to 13 months. There exists considerable heterogeneity in the survival at the individual patient level. To better understand the survival heterogeneity and improve risk stratification, our study aims to identify the factors influencing survival utilizing a large patient sample in the National Cancer Database (NCDB).
Methods: Women diagnosed with metastatic TNBC from 2010 to 2020 in the NCDB were included. Demographic, clinic-pathological, treatment data, and overall survival (OS) outcomes were collected. Kaplan-Meier curves were used to estimate OS. The log-rank test was used to identify OS differences between groups for each variable in the univariate analysis. For the multivariate analysis, the Cox proportional hazard model with backward elimination was used to identify factors affecting OS. Adjusted hazard ratios and 95% confidence intervals are presented.
Results: 2,273 women had a median overall survival of 13.6 months. Factors associated with statistically significantly worse OS included older age, higher comorbidity scores, specific histologies, higher number of metastatic sites, presence of liver or other site metastases in those with only one metastatic site (excluding brain metastases), presence of cranial and extra-cranial metastases, lack of chemotherapy, lack of immunotherapy, lack of surgery to distant sites, lack of radiation to distant sites, and receipt of palliative treatment to alleviate symptoms. In the multivariate analysis, comorbidity score, histology, number of metastatic sites, immunotherapy, and chemotherapy had a statistically significant effect on the OS.
Conclusions: Through NCDB analysis, we have identified prognostic factors for metastatic TNBC. These findings will help improve prognostication at diagnosis, optimize treatment strategies, and facilitate patient stratification in future clinical trials.
Keywords:
metastatic triple negative breast cancer
; overall survival
; prognostic factors
1. Introduction
Breast cancer is the most commonly diagnosed cancer globally, surpassing lung cancer[1]. Triple-negative breast cancer (TNBC) accounts for 15-20% of all breast cancers[2]. TNBCs are estrogen and progesterone receptor-negative: <1% by immunohistochemistry (IHC) and human epidermal growth factor receptor 2 (HER2) negative (0-1+ by IHC or 2+ by IHC with FISH negative). TNBC is more commonly diagnosed in women younger than 40 (odds ratio of 2.13, 95% CI 1.34- 3.39) and African-American women (odds ratio 2.41, 95% CI 1.81- 3.21) compared to those over 50 and Caucasian women respectively[3].
Compared to hormone receptor-positive or HER2-positive breast cancers, TNBC is known for its aggressiveness with larger tumor size, lymph node involvement, higher tumor grade, higher relapse rate of localized TNBC to metastatic TNBC, and a propensity for younger patients [3-5]. Individuals with TNBC experience an increased likelihood of distant recurrence within 5 years of diagnosis with a predilection for visceral as opposed to bony sites of relapse[6-9]. Due to the lack of biomarkers for targeted therapies like hormone receptor or HER-2 expression, there are only a few approved agents for TNBC, and the treatment mainly involves cytotoxic agents[10,11]. All these factors contribute to reduced overall survival in TNBC compared to other types of breast cancer, in both localized and metastatic settings. The 5- year overall survival (OS) for metastatic TNBC is around 11% with a median OS of around 11 to 13 months [5,12]. Despite this bleak prognosis, considerable prognostic heterogeneity exists at the individual patient level, with a wide range of OS of 0.8 months to 99.8 months [5,13].
To better understand this survival heterogeneity and improve risk stratification within de novo metastatic TNBC, our study aims to explore the impact of demographic factors, clinicopathological factors, and treatment factors on OS, utilizing a large patient sample in the National Cancer Data Base (NCDB).
2. Methods
This study utilized the National Cancer Database (NCDB) which includes over 1500 Commission on Cancer (CoC) programs that treat approximately 70% of all newly diagnosed cancers in the United States [14,15]. A retrospective review of de-identified patient data adhering to the established procedures for NCDB analyses was conducted and hence was exempt from our institutional review board. A total of 2,273 women diagnosed with metastatic TNBC between 2010 and 2020, each with all the required data, were included in our study.
Demographics (age, race, and Charlson-Deyo comorbidity score); clinico-pathological variables (histology, HER2 IHC expression, number of metastatic sites, and sites of metastases); and treatment variables (first-line chemotherapy, immunotherapy, days from diagnosis to systemic therapy, distant site surgery, distant site radiation, and palliative treatment to alleviate symptoms) were collected. Charlson-Deyo comorbidity scores were divided into 4 groups: score 0, score 1, score 2, and score 3 or more. Histology included invasive ductal carcinoma, invasive lobular carcinoma, adenocarcinoma with metaplasia, adenocarcinoma not otherwise specified (NOS), and other carcinomas. Other carcinomas included carcinoma NOS, small cell carcinoma, neuroendocrine carcinoma, non-small cell carcinoma, and inflammatory carcinoma predominantly; along with adenoid cystic and cribriform carcinoma and mucoepidermoid carcinoma. The number of metastatic sites refers to the number of organs involved with metastatic cancer. Time to initiation of systemic therapy initiation was categorized as < 2 weeks, 2-4 weeks, >4 weeks, and no systemic therapy. Palliative treatment was referred to as any treatment aimed to relieve symptoms and may involve surgery, radiation, systemic therapy, and/or other pain management. The overall survival (OS) was defined as the time from the diagnosis of metastatic TNBC until death.
Demographic, clinico-pathological data, and treatment data were described using frequencies and percentages. Kaplan-Meier (KM) curves were used to estimate the OS for each variable of interest. The log-rank test was used to identify OS differences between groups for each variable in the univariate analysis. The Cox proportional hazard model with backward elimination was used to identify factors affecting the OS in the multivariate analysis. The median OS in months, adjusted hazard ratios, and 12- month survival estimates with 95% confidence intervals (CI) were reported. PC SAS version 9.4 was used for all analyses. The statistical significance level was set at 0.05 for all analyses.
3. Results
A total of 2,273 women diagnosed with de novo metastatic TNBC had a median OS of 13.6 months (95% CI 12.81- 14.65). Table 1 details demographic, clinico-pathologic, and treatment variables. Most women were aged 41-70 (63.1%), Caucasian (67.4%), and had the Charlson-Deyo comorbidity score 0 (76.2%). The majority had invasive ductal carcinoma (81%), HER-2 IHC expression of 0 (53.5%), extra-cranial metastases only (89%), and a single metastatic site (49.7%). The majority of women received multi-agent chemotherapy as first-line therapy (41.6%), no immunotherapy (80.4%), had > 4 weeks from diagnosis to initiation of systemic therapy (49.8%), no surgery or radiation to the distant lymph node or metastatic site (93.9% and 70.5% respectively), and no palliative treatment to alleviate symptoms (75.7%).
Table 1 and 3 detail the median OS, Log rank p-value, Hazard ratio (HR), and the 12-month survival estimates of different groups for each demographic, clinico-pathologic, and treatment variable in the univariate analysis; and the results of the multi-variate analysis.
In the demographic variables, the OS was significantly worse for the 71-90 age group with the shortest median OS of 9.6 months compared to the 19-40 age group (HR 1.52, 95% CI 1.24- 1.85); the OS was similar in the 19-40 (median OS 15.5 months) and 41-70 age groups (median OS 15.6 months). The Charlson-Deyo comorbidity score groups of 1 (HR 1.22, 95% CI 1.06-1.41), 2 (HR 1.8, 95% CI 1.47-2.22), and 3 or more (HR 2.46, 95% CI 1.94-3.12) were associated with statistically significantly worse OS compared to the score 0 group, demonstrating a clear trend of decreasing survival as the comorbidity score increased. Women with a score of 3 or more had the shortest median OS of 4.6 months compared to the longest median OS of 15.3 months in the score 0 group. No significant differences were observed in the OS based on race (p= 0.2033).
Within the cancer related/ clinico-pathologic variables, OS was significantly worse for adenocarcinoma NOS with a median OS of 4 months (HR 1.89, 95% CI 1.51-2.37) and the other carcinoma group with a median OS of 6.7 months (HR 1.83, 95% CI 1.55-2.17) compared to the invasive ductal carcinoma group. However, OS was similar among invasive ductal carcinoma (median OS 15.2 months), invasive lobular carcinoma (median OS 12 months), and adenocarcinoma with metaplasia (median OS 14 months) groups. The number of metastatic sites of 2 (HR 1.72, 95% CI 1.53-1.94), 3 (HR 1.99, 95% CI 1.72-2.3), 4 (HR 3.16, 95% CI 2.62-3.8), 5 or 6 (HR 4.61, 95% CI 3.47-6.13) had statistically significantly worse OS compared to only 1 metastatic site, with a clear trend of decreasing survival as the metastatic sites increased. Women with 5 or 6 metastatic sites had the shortest median OS of 2.6 months compared to the longest median OS of 19.8 months in the 1 metastatic site group. In the subgroup analysis of those with only single metastatic site (excluding brain-only metastases due to their known worse prognosis), women with bone only metastases (HR 1.36, 95% CI 1.08-1.72), liver only metastases (HR 1.67, 95% CI 1.29-2.17), other site only metastases (HR 1.85, 95% CI 1.34-2.55) had worse OS compared to those with lymph node only metastases; while the OS was similar in those with lymph node only metastases and lung only metastases. The OS was statistically significantly worse in those with both cranial and extra-cranial metastases with the shortest median OS of 5.3 months compared to cranial only metastases (HR 1.7, 95% CI 1.16-2.49), and OS was similar in the cranial only metastases (median OS 11.8 months) and extra-cranial only metastases (median OS 14.6 months). No significant differences were observed in the OS based on HER2 IHC expression (p= 0.3099).
In the treatment variables, OS was statistically significantly better for women who received either single agent first-line chemotherapy with a median OS of 16.4 months (HR 0.29, 95% CI 0.25-0.33) or mutli-agent first-line chemotherapy with a median OS of 19.9 months (HR 0.23, 95% CI 0.21-0.26) compared to no chemotherapy with a median OS of 2.9 months. This improvement in OS with first-line chemotherapy remained consistent across all the Charlson-Deyo comorbidity score groups in the sub-group analysis, refer to table 2 for details. Women who received immunotherapy had a better OS with a median OS of 25.6 months compared to the median OS of 11.5 months in no immunotherapy group (HR 0.49, 95% CI 0.42-0.56). Regarding the time from diagnosis to initiation of systemic therapy, women with > 4 weeks had a better median OS of 20.6 months (HR 0.21, 95% CI 0.18-0.23), followed by those with 2-4 weeks who had a median OS of 15.6 months (HR 0.26, 95% CI 0.23-0.31) and those with < 2 weeks with a median OS of 10.8 (HR 0.34, 95% CI 0.28-0.43) compared to women with no systemic therapy who had a median OS of 2.7 months.
Surgery of the distant lymph node or distant metastatic site was associated with significantly better OS with a median OS of 29.2 months compared to no surgery with a median OS of 13.1 months (HR 0.5, 95% CI 0.38-0.66). Similarly, women who received radiation to distant site had a significantly better OS with a median OS of 14.7 months compared to no radiation with a median OS of 12.6 months (HR 0.86, 95% CI 0.76-0.98). However, the receipt of palliative treatment to alleviate symptoms was associated with significantly worse OS with a median of 11.3 months compared to no palliative treatment with a median OS of 14.5 months (HR 1.18, 95% CI 1.06-1.32).
Based on the results from the univariate analysis, the following variables were included in the final multivariate analysis: age, Charlson-Deyo comorbidity score group, histology, number of metastatic sites, site of metastases: cranial only/ cranial and extra-cranial/ extra-cranial only, receipt of first line chemotherapy, receipt of immunotherapy, and receipt of palliative treatment to alleviate symptoms. In the multi-variate cox proportional hazard analysis; the Charlson-Deyo comorbidity score, histology, number of metastatic sites, receipt of first-line chemotherapy and receipt of immunotherapy were identified as the five factors independently influencing OS, as detailed in Table 3. Figure 1 displays the univariate Kaplan-Meier survival curves for these five prognostic factors. Surgery and radiation of the distant site variables were excluded from multi-variate analysis, despite significance in the univariate analysis, due to missing information in some patients. Similarly, the time from diagnosis to initiation of systemic therapy variable was also excluded due to its overlapping subgroups with first-line chemotherapy variable.
4. Discussion
Prognostication based on the results observed in therapeutic clinical trials may not realistically estimate prognosis in the real-world. Fewer comorbidities and better functional status due to stringent eligibility criteria, lower cancer burden without visceral crisis or severe symptoms, better treatment compliance, and increased access to health care and other supportive resources typically seen in participants leads to longer OS in clinical trials [16-18]. A meta-analysis of three phase III trials of first line treatment in metastatic TNBC reported a median OS of 17.5 months, surpassing the real-world OS estimates of 11 to 13 months [5,12,18,19]. These reported real-world studies, with limited sample size and selective representation, may not accurately reflect the diverse TNBC patient population in the United States. Our study, the largest to date, included 2,273 metastatic TNBC women from the NCDB, encompassing data from multiple institutions treating over 70 percent of all cancer patients in the United States. It revealed a median OS of 13.6 months, consistent with prior reports.
We identified 5 independent prognostic variables for survival in metastatic TNBC in the multivariate analysis: Charlson-Deyo comorbidity score, histology, number of metastatic sites, receipt of first-line chemotherapy and receipt of immunotherapy. Affirming the crucial role of overall health in prognosis, there was an inverse correlation between Charlson-Deyo comorbidity score and OS. This finding was consistent with a prior study in non-metastatic TNBC that showed those with a Charlson comorbidity index score of ≥3 had a significantly higher risk of death compared to those without comorbidities in African-American patients, and comorbidities at diagnosis increased risk of death independent of TNBC[20]. In the metastatic setting, our study demonstrated that histology is an independent prognostic factor. Invasive ductal carcinoma, invasive lobular carcinoma, and adenocarcinoma with metaplasia had similar OS, while the adenocarcinoma NOS and other carcinoma (encompassing aggressive histologies like inflammatory carcinoma, neuroendocrine carcinoma, small cell carcinoma) exhibited worse OS. In non-metastatic TNBC, prior studies showed that invasive lobular carcinoma and metaplastic carcinoma were associated with worse OS compared to invasive ductal carcinoma [21,22]. However, another study, adjusting for tumor stage and demographics, found similar OS between invasive lobular carcinoma and invasive ductal carcinoma [23], highlighting the potential OS differences between invasive lobular carcinoma and invasive ductal carcinoma in previous studies due to selection bias and inadequate adjustment for clinically relevant covariates. In our study, there was an inverse correlation between the number of metastatic sites and OS suggesting that the number of metastatic sites may reflect disease burden. This finding was consistent with a prior study that showed higher risk of death for those with more than one metastatic site compared to those with only one metastatic site in TNBC[12]. Receipt of first-line chemotherapy, either single agent or multi-agent, the primary backbone of treatment for metastatic TNBC, was an independent prognostic factor for OS, as those not receiving experienced worse OS likely due to faster cancer progression. Receipt of immunotherapy was also an independent prognostic factor, associated with better OS, consistent with the results from Impassion 130 and Keynote 522 trials. In 2019, Atezolizumab, a PD-L1 inhibitor, was approved as a first line treatment in combination with chemotherapy for PD-L1 ≥1% tumors based on the Impassion130 trial but was later withdrawn in 2021 due to a lack of PFS and OS improvement in the Impassion 131 trial [24,25]. In 2020, Pembrolizumab, a PD-1 inhibitor was approved as first line treatment in combination with chemotherapy in PD-L1 ≥10% tumors based on the Keynote 355 trial [26]. PD-L1 positivity in TNBC is approximately 20-47% [27,28]. In our study, which included patients from 2010-2020, 19.6% of total patients received immunotherapy, some likely in later lines after having received other treatments before the immunotherapy approval.
In our study, poor OS was observed in the 71-90 age group in univariate analyses, but age was not an independent prognostic factor in multi-variate analyses. A prior study on metastatic TNBC surprisingly revealed a poor prognosis in those under 50 years old [5]. Studies in non-metastatic TNBC examining the impact of age at diagnosis on OS yielded conflicting results [29-31]. Age itself may not be an independent prognostic factor, but advanced age is usually linked to a higher burden of comorbidities, poor overall health, and potentially lower chemotherapy uptake, adversely affecting OS[16]. Thus, treatment decisions should consider functional age over chronological age [32]. While OS was worse for those with both cranial and extra-cranial metastases in the univariate analyses, the location of metastases (cranial only Vs. cranial and extra-cranial Vs. extra-cranial only) has lost significance in the multi-variate analyses. TNBC typically has a higher incidence of brain metastases at 30% with a median OS of 5 months after brain metastases [33,34]. Factors impacting mortality in brain metastases include having more than 3 brain lesions, symptomatic brain metastases, lack of brain metastases directed treatment, and uncontrolled extracranial metastases [35]. It is possible that the location of metastases did not emerge as an independent prognostic factor in our study due to smaller number of patients with cranial metastases (only 2% had cranial only metastases and 9% had both cranial and extra-cranial metastases). Alternatively, it is possible that overall cancer burden and ability to receive treatment (both systemic therapy and brain metastases directed local treatments like radiation) are the clinically relevant confounding covariates impacting OS rather than the presence of brain metastases itself. Palliative treatment (to alleviate symptoms), despite showing an association with poor OS in the univariate analysis, was not identified as an independent prognostic factor in the multi-variate analysis, as it likely reflects higher disease burden rather than treatment impact.
In the subgroup analysis of patients with a single metastatic site (excluding brain-only metastases due to their known worse prognosis) [33,35], those with lung only metastases or distant lymph node only mets demonstrated better OS, indicating potential prognostic implications of the site of metastatic disease in this subgroup that warrants further evaluation in future studies. Additionally, the sub-group analysis of first line chemotherapy across all Charlson-Deyo score groups showed that, despite an increased percentage of patients not receiving chemotherapy with higher Charlson-Deyo scores, those who received chemotherapy had better OS in all score groups. This suggests that a higher comorbidity score itself should not automatically deter chemotherapy administration unless there are contra-indications or concerns about serious toxicity.
Receiving chemotherapy more than 4 weeks after diagnosis showed better OS in the univariate analysis, indicating that a delay in chemotherapy initiation by a few weeks may not harm OS in metastatic TNBC. This contrasts with non-metastatic TNBC, where a delay in adjuvant chemotherapy initiation by ≥30 days after surgery was associated with worse OS and recurrence free survival [36,37]. The better OS associated with surgery or radiation to the distant metastatic site in the univariate analysis may be due to selection bias; as these patients are likely to be younger, healthier, and have less metastatic burden to be considered for locoregional treatments. The role of these variables could not be assessed in the multivariate analyses due to missing information in some study patients whether they received surgery or radiation to the distant site. Currently, there is no compelling prospective evidence supporting surgery or radiation to distant metastatic site in TNBC management. The SABR COMET study showed an OS advantage with stereotactic radiation in oligometastatic cancer (only 18 out of the 99 patients had breast cancer), but the NRG BR-00213 study done exclusively in breast cancer patients showed no OS benefit [38]. Similarly, randomized controlled data for surgery of the primary tumor have not demonstrated an OS benefit, and there are no randomized trials examining surgery of the distant metastatic sites[39].
Previous studies on racial disparities in TNBC OS outcomes yielded inconsistent results [11,12,40-42]. Disparities in comorbidities and care may have contributed to worse OS outcomes for African-Americans in some studies as no racial differences in TNBC survival were observed when they received similar treatment under comparable conditions [20,40,41]. In our study, OS did not significantly different among races, indicating metastatic TNBC behaves biologically similarly across all racial groups and equitable access to health care are likely to result in similar OS. HER-2 expression level in TNBC does not influence biology or gene expression [43], hence HER-2 expression level itself did not influence OS in our study, aligning with findings in other studies [44]. However, with the newer treatment option, Trastuzumab deruxtecan, approved for metastatic HER-2 low ( IHC 1+ or IHC 2+ with negative FISH) TNBC in 2022 based on the DESTINY BREAST-04 trial, patients with HER-2 low TNBC are likely to have better OS than those with HER-2 zero TNBC in the future[45].
One limitation of our study is that the newer FDA-approved treatments like Olaparib/ Talazoparib (PARP inhibitors), Atezolizumab (PD-L1 inhibitor, later withdrawn from the market in 2021), Pembrolizumab (PD-1 inhibitor), Sacituzumab govitecan (Trop-2 directed antibody drug conjugate), and Trastuzumab deruxtecan (HER-2 directed antibody drug conjugate), introduced mainly after 2018, have resulted in slightly improved OS for metastatic TNBC, which is not completely reflected in our 2010-2020 data [26,45-49]. While these new treatments demonstrated improved OS in clinical trials, it is important to note that the absolute difference in OS ranged only from 0 to 6 months compared to control arms. In the real world, this OS difference may be even smaller, as patients tend to experience better outcomes in clinical trials than in real-world settings. Our study results will serve as a benchmark for assessing progress in treatment of metastatic TNBC in future decades.
Our study’s limitations stem from the NCDB, a hospital-based data collection system that pools data from multiple centers, which may introduce variations in data collection due to possible distinct data collection standards at each center, alongside potential errors during data abstraction and entry from the medical records. The NCDB also lacks information about relapsed metastatic TNBC, response to first-line therapy, longitudinal treatment data (provides only first line treatment without subsequent treatment information), patient reported outcomes like quality of life, and cause of death.
5. Conclusions
In conclusion, our study on OS in metastatic TNBC is the largest of its kind to comprehensively explore the impact of various factors on OS to better understand the survival heterogeneity. These findings empower clinicians to offer personalized prognostic information at diagnosis and tailor treatment strategies. This may involve considering options of aggressive systemic therapy versus focusing on comfort/quality of life based on expected prognosis, and the consideration for more frequent scans to assess response to treatment given short window for therapeutic interventions, especially in those with poor prognostic factors. Our study highlights the clear unmet need for newer therapeutic options to improve outcomes particularly for those with poor prognostic factors and can aid in the development of prognostic groups for use in future clinical trials.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: a cancer journal for clinicians 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Foulkes, W.D.; Smith, I.E.; Reis-Filho, J.S. Triple-negative breast cancer. N Engl J Med 2010, 363, 1938–1948. [Google Scholar] [CrossRef] [PubMed]
- Trivers, K.F.; Lund, M.J.; Porter, P.L.; Liff, J.M.; Flagg, E.W.; Coates, R.J.; Eley, J.W. The epidemiology of triple-negative breast cancer, including race. Cancer Causes Control 2009, 20, 1071–1082. [Google Scholar] [CrossRef] [PubMed]
- Nam, Y.H. A Study on the Factors and Prediction Model of Triple-Negative Breast Cancer for Public Health Promotion. Diagnostics (Basel) 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Kassam, F.; Enright, K.; Dent, R.; Dranitsaris, G.; Myers, J.; Flynn, C.; Fralick, M.; Kumar, R.; Clemons, M. Survival outcomes for patients with metastatic triple-negative breast cancer: implications for clinical practice and trial design. Clin Breast Cancer 2009, 9, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Pinilla, S.M.; Sarrio, D.; Honrado, E.; Hardisson, D.; Calero, F.; Benitez, J.; Palacios, J. Prognostic significance of basal-like phenotype and fascin expression in node-negative invasive breast carcinomas. Clin Cancer Res 2006, 12, 1533–1539. [Google Scholar] [CrossRef] [PubMed]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; Van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C. , et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl Cancer Inst 2000, 92, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Dent, R.; Hanna, W.M.; Trudeau, M.; Rawlinson, E.; Sun, P.; Narod, S.A. Pattern of metastatic spread in triple-negative breast cancer. Breast Cancer Res Treat 2009, 115, 423–428. [Google Scholar] [CrossRef]
- Mandapati, A.; Lukong, K.E. Triple negative breast cancer: approved treatment options and their mechanisms of action. J Cancer Res Clin Oncol 2023, 149, 3701–3719. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Reis-Filho, J.S.; Ashley, S.; Steele, D.; Ashworth, A.; Lakhani, S.R.; Smith, I.E. Basal-like breast carcinomas: clinical outcome and response to chemotherapy. J Clin Pathol 2006, 59, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Bauer, K.R.; Brown, M.; Cress, R.D.; Parise, C.A.; Caggiano, V. Descriptive analysis of estrogen receptor (ER)-negative, progesterone receptor (PR)-negative, and HER2-negative invasive breast cancer, the so-called triple-negative phenotype: a population-based study from the California cancer Registry. Cancer 2007, 109, 1721–1728. [Google Scholar] [CrossRef] [PubMed]
- Skinner, K.E.; Haiderali, A.; Huang, M.; Schwartzberg, L.S. Real-world effectiveness outcomes in patients diagnosed with metastatic triple-negative breast cancer. Future Oncol 2021, 17, 931–941. [Google Scholar] [CrossRef] [PubMed]
- Dent, R.; Trudeau, M.; Pritchard, K.I.; Hanna, W.M.; Kahn, H.K.; Sawka, C.A.; Lickley, L.A.; Rawlinson, E.; Sun, P.; Narod, S.A. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res 2007, 13, 4429–4434. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Stewart, A.K.; Winchester, D.P.; Ko, C.Y. The National Cancer Data Base: a powerful initiative to improve cancer care in the United States. Ann Surg Oncol 2008, 15, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Boffa, D.J.; Rosen, J.E.; Mallin, K.; Loomis, A.; Gay, G.; Palis, B.; Thoburn, K.; Gress, D.; McKellar, D.P.; Shulman, L.N. , et al. Using the National Cancer Database for Outcomes Research: A Review. JAMA Oncol 2017, 3, 1722–1728. [Google Scholar] [CrossRef] [PubMed]
- Batra, A.; Kong, S.; Cheung, W.Y. Eligibility of real-world patients with metastatic breast cancer for clinical trials. Breast 2020, 54, 171–178. [Google Scholar] [CrossRef]
- Gong, I.Y.; Yan, A.T.; Earle, C.C.; Trudeau, M.E.; Eisen, A.; Chan, K.K.W. Comparison of outcomes in a population-based cohort of metastatic breast cancer patients receiving anti-HER2 therapy with clinical trial outcomes. Breast Cancer Res Treat 2020, 181, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Li, C.H.; Karantza, V.; Aktan, G.; Lala, M. Current treatment landscape for patients with locally recurrent inoperable or metastatic triple-negative breast cancer: a systematic literature review. Breast Cancer Res 2019, 21, 143. [Google Scholar] [CrossRef] [PubMed]
- Celik, A.; Berg, T.; Jensen, M.B.; Jakobsen, E.; Nielsen, H.M.; Kümler, I.; Glavicic, V.; Jensen, J.D.; Knoop, A. Real-World Survival and Treatment Regimens Across First- to Third-Line Treatment for Advanced Triple-Negative Breast Cancer. Breast Cancer (Auckl) 2023, 17, 11782234231203292. [Google Scholar] [CrossRef] [PubMed]
- Swede, H.; Sarwar, A.; Magge, A.; Braithwaite, D.; Cook, L.S.; Gregorio, D.I.; Jones, B.A.; R Hoag, J.; Gonsalves, L.; L Salner, A. , et al. Mortality risk from comorbidities independent of triple-negative breast cancer status: NCI-SEER-based cohort analysis. Cancer Causes Control 2016, 27, 627–636. [Google Scholar] [CrossRef] [PubMed]
- Montagna, E.; Maisonneuve, P.; Rotmensz, N.; Cancello, G.; Iorfida, M.; Balduzzi, A.; Galimberti, V.; Veronesi, P.; Luini, A.; Pruneri, G. , et al. Heterogeneity of triple-negative breast cancer: histologic subtyping to inform the outcome. Clin Breast Cancer 2013, 13, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Balkenhol, M.C.A.; Vreuls, W.; Wauters, C.A.P.; Mol, S.J.J.; van der Laak, J.A.W.M.; Bult, P. Histological subtypes in triple negative breast cancer are associated with specific information on survival. Ann Diagn Pathol 2020, 46, 151490. [Google Scholar] [CrossRef] [PubMed]
- Joshi, U.; Budhathoki, P.; Gaire, S.; Yadav, S.K.; Shah, A.; Adhikari, A.; Choong, G.; Couzi, R.; Giridhar, K.V.; Leon-Ferre, R.A. , et al. Clinical outcomes and prognostic factors in triple-negative invasive lobular carcinoma of the breast. Breast Cancer Res Treat 2023, 200, 217–224. [Google Scholar] [CrossRef]
- Miles, D.; Gligorov, J.; André, F.; Cameron, D.; Schneeweiss, A.; Barrios, C.; Xu, B.; Wardley, A.; Kaen, D.; Andrade, L. , et al. Primary results from IMpassion131, a double-blind, placebo-controlled, randomised phase III trial of first-line paclitaxel with or without atezolizumab for unresectable locally advanced/metastatic triple-negative breast cancer. Ann Oncol 2021, 32, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.A.; Shaw Wright, G. , et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N Engl J Med 2018, 379, 2108–2121. [Google Scholar] [CrossRef] [PubMed]
- Cortes, J.; Rugo, H.S.; Cescon, D.W.; Im, S.A.; Yusof, M.M.; Gallardo, C.; Lipatov, O.; Barrios, C.H.; Perez-Garcia, J.; Iwata, H. , et al. Pembrolizumab plus Chemotherapy in Advanced Triple-Negative Breast Cancer. N Engl J Med 2022, 387, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Mittendorf, E.A.; Philips, A.V.; Meric-Bernstam, F.; Qiao, N.; Wu, Y.; Harrington, S.; Su, X.; Wang, Y.; Gonzalez-Angulo, A.M.; Akcakanat, A. , et al. PD-L1 expression in triple-negative breast cancer. Cancer Immunol Res 2014, 2, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Xu, D.; Tang, B.; Ren, Y.; Han, Y.; Liang, G.; Wang, J.; Wang, L. Expression of programmed death ligand-1 and programmed death-1 in samples of invasive ductal carcinoma of the breast and its correlation with prognosis. Anticancer Drugs 2018, 29, 904–910. [Google Scholar] [CrossRef]
- Kaplan, H.G.; Malmgren, J.A.; Atwood, M.K. Triple-negative breast cancer in the elderly: Prognosis and treatment. Breast J 2017, 23, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Rayson, D.; Payne, J.I.; Michael, J.C.R.; Tsuruda, K.M.; Abdolell, M.; Barnes, P.J. Impact of Detection Method and Age on Survival Outcomes in Triple-Negative Breast Cancer: A Population-Based Cohort Analysis. Clin Breast Cancer 2018, 18, e955–e960. [Google Scholar] [CrossRef]
- Zhu, W.; Perez, E.A.; Hong, R.; Li, Q.; Xu, B. Age-Related Disparity in Immediate Prognosis of Patients with Triple-Negative Breast Cancer: A Population-Based Study from SEER Cancer Registries. PLoS One 2015, 10, e0128345. [Google Scholar] [CrossRef] [PubMed]
- Maltoni, R.; Ravaioli, S.; Bronte, G.; Mazza, M.; Cerchione, C.; Massa, I.; Balzi, W.; Cortesi, M.; Zanoni, M.; Bravaccini, S. Chronological age or biological age: What drives the choice of adjuvant treatment in elderly breast cancer patients? Transl Oncol 2022, 15, 101300. [Google Scholar] [CrossRef]
- Morris, P.G.; Murphy, C.G.; Mallam, D.; Accordino, M.; Patil, S.; Howard, J.; Omuro, A.; Beal, K.; Seidman, A.D.; Hudis, C.A. , et al. Limited overall survival in patients with brain metastases from triple negative breast cancer. Breast J 2012, 18, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Venkitaraman, R.; Joseph, T.; Dhadda, A.; Chaturvedi, A.; Upadhyay, S. Prognosis of patients with triple-negative breast cancer and brain metastasis. Clin Oncol (R Coll Radiol) 2009, 21, 729–730. [Google Scholar] [CrossRef] [PubMed]
- Jin, J.; Gao, Y.; Zhang, J.; Wang, L.; Wang, B.; Cao, J.; Shao, Z.; Wang, Z. Incidence, pattern and prognosis of brain metastases in patients with metastatic triple negative breast cancer. BMC Cancer 2018, 18, 446. [Google Scholar] [CrossRef]
- Cai, L.; Tong, Y.; Zhu, X.; Shen, K.; Zhu, J.; Chen, X. Prolonged Time to Adjuvant Chemotherapy Initiation Was Associated with Worse Disease Outcome in Triple Negative Breast Cancer Patients. Sci Rep 2020, 10, 7029. [Google Scholar] [CrossRef] [PubMed]
- Morante, Z.; Ruiz, R.; Araujo, J.M.; Pinto, J.A.; Cruz-Ku, G.; Urrunaga-Pastor, D.; Namuche, F.; Flores, C.; Mantilla, R.; Luján, M.G. , et al. Impact of the Delayed Initiation of Adjuvant Chemotherapy in the Outcome of Triple Negative Breast Cancer. Clin Breast Cancer 2021, 21, 239–246.e234. [Google Scholar] [CrossRef]
- Burgaleta, A.M.; Burguete, A.B.; Gutiérrez, L.R.; Nuín, E.B.; Felipe, G.A.; de la Vega, F.A. Local treatment in oligometastasis from breast cancer: an overview. Clin Transl Oncol 2023, 25, 2861–2867. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, M.J.; Mokbel, K. Locoregional therapy in de novo metastatic breast cancer. The unanswered question. Breast 2021, 58, 170–172. [Google Scholar] [CrossRef]
- Pacheco, J.M.; Gao, F.; Bumb, C.; Ellis, M.J.; Ma, C.X. Racial differences in outcomes of triple-negative breast cancer. Breast Cancer Res Treat 2013, 138, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Dawood, S.; Broglio, K.; Kau, S.W.; Green, M.C.; Giordano, S.H.; Meric-Bernstam, F.; Buchholz, T.A.; Albarracin, C.; Yang, W.T.; Hennessy, B.T. , et al. Triple receptor-negative breast cancer: the effect of race on response to primary systemic treatment and survival outcomes. J Clin Oncol 2009, 27, 220–226. [Google Scholar] [CrossRef] [PubMed]
- O'Brien, K.M.; Cole, S.R.; Tse, C.K.; Perou, C.M.; Carey, L.A.; Foulkes, W.D.; Dressler, L.G.; Geradts, J.; Millikan, R.C. Intrinsic breast tumor subtypes, race, and long-term survival in the Carolina Breast Cancer Study. Clin Cancer Res 2010, 16, 6100–6110. [Google Scholar] [CrossRef] [PubMed]
- Schettini, F.; Chic, N.; Brasó-Maristany, F.; Paré, L.; Pascual, T.; Conte, B.; Martínez-Sáez, O.; Adamo, B.; Vidal, M.; Barnadas, E. , et al. Clinical, pathological, and PAM50 gene expression features of HER2-low breast cancer. NPJ Breast Cancer 2021, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Gampenrieder, S.P.; Dezentjé, V.; Lambertini, M.; de Nonneville, A.; Marhold, M.; Le Du, F.; Cortés Salgado, A.; Alpuim Costa, D.; Vaz Batista, M.; Chic Ruché, N. , et al. Influence of HER2 expression on prognosis in metastatic triple-negative breast cancer-results from an international, multicenter analysis coordinated by the AGMT Study Group. ESMO Open 2023, 8, 100747. [Google Scholar] [CrossRef] [PubMed]
- Modi, S.; Jacot, W.; Yamashita, T.; Sohn, J.; Vidal, M.; Tokunaga, E.; Tsurutani, J.; Ueno, N.T.; Prat, A.; Chae, Y.S. , et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. N Engl J Med 2022, 387, 9–20. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food & Drug administration. Oncology (Cancer)/ Hematologic Malignancies Approval Notifications. https://www.fda.gov/drugs/resources-information-approved-drugs/oncology-cancer-hematologic-malignancies-approval-notifications, 2023.
- Robson, M.E.; Im, S.A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Tung, N.; Armstrong, A.; Dymond, M. , et al. OlympiAD extended follow-up for overall survival and safety: Olaparib versus chemotherapy treatment of physician's choice in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer. Eur J Cancer 2023, 184, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Hurvitz, S.A.; Mina, L.A.; Rugo, H.S.; Lee, K.H.; Gonçalves, A.; Diab, S.; Woodward, N.; Goodwin, A.; Yerushalmi, R. , et al. Talazoparib versus chemotherapy in patients with germline BRCA1/2-mutated HER2-negative advanced breast cancer: final overall survival results from the EMBRACA trial. Ann Oncol 2020, 31, 1526–1535. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Hurvitz, S.A.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Sardesai, S.D.; Kalinsky, K.; Zelnak, A.B. , et al. Sacituzumab Govitecan in Metastatic Triple-Negative Breast Cancer. N Engl J Med 2021, 384, 1529–1541. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Kaplan-Meier survival curves of the five significant variables in the multi-variate analysis.
Figure 1.
Kaplan-Meier survival curves of the five significant variables in the multi-variate analysis.
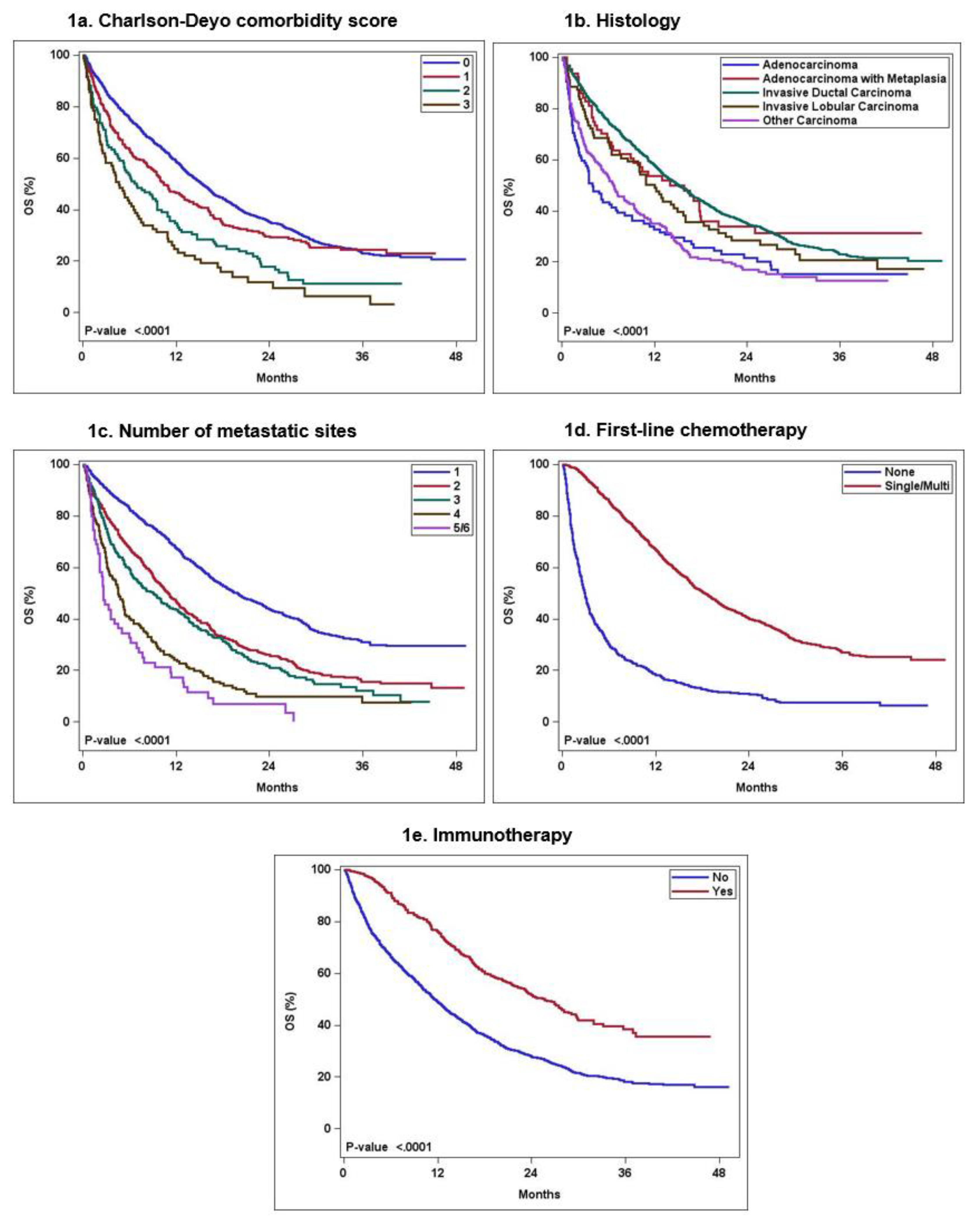

Table 1.
Univariate analysis of demographic, disease, and treatment characteristics on OS.
| No. of patients (% of total patients) |
Median OS in months (95% CI) |
Logrank p-value | Hazard Ratio (95% CI) |
12-month survival estimates | |
|---|---|---|---|---|---|
| Demographic Characteristics | |||||
|
Age 19-40 41-70 71-90 |
179 (7.9) 1435 (63.1) 659 (29) |
15.5 (13.2-18.2) 15.6 (14.2-16.7) 9.6 (8.0-11.4) |
<0.0001 |
Reference 1.05 (0.87-1.27) 1.52 (1.24-1.85) |
0.64 (0.57-0.72) 0.58 (0.55-0.60) 0.44 (0.41-0.48) |
|
Race Caucasian African-American Other |
1532 (67.4) 638 (28.1) 103 (4.5) |
13.6 (12.7-14.8) 13.4 (11.9-15.2) 16.9 (12.3-28.3) |
0.2033 |
Reference 1.02 (0.91-1.14) 0.8 (0.62-1.03) |
0.54 (0.52-0.57) 0.54 (0.5-0.58) 0.6 (0.51-0.71) |
|
Charlson -Deyo score 0 1 2 3 or more |
1732 (76.2) 339 (14.9) 118 (5.2) 84 (3.7) |
15.3 (14.3-16.3) 10.4 (9.1-13.1) 6.9 (5.2-9.6) 4.6 (2.9- 6.9) |
< 0.0001 |
Reference 1.22 (1.06-1.41) 1.8 (1.47-2.22) 2.46 (1.94-3.12) |
0.59 (0.56-0.61) 0.46 (0.41-0.52) 0.35 (0.27-0.45) 0.25 (0.17-0.36) |
| Clinicopathologic/ Cancer Characteristics | |||||
|
Histology Invasive ductal carcinoma Invasive lobular carcinoma Adenocarcinoma with metaplasia Adenocarcinoma NOS Other carcinoma |
1840 (81) 79 (3.5) 64 (2.8) 105 (4.6) 185 (8.1) |
15.2 (14.1-16.3) 12 (8.5-16.0) 14.0 (8.9-20.3) 4.0 (2.9-8.1) 6.7 (5.2-9.3) |
< 0.0001 |
Reference 1.23 (0.95 -1.60) 1.0 (0.73-1.4) 1.89 (1.51-2.37) 1.83 (1.55-2.17) |
0.58 (0.56-0.60) 0.49 (0.39-0.61) 0.54 (0.43-0.68) 0.33 (0.25-0.44) 0.35 (0.29-0.43) |
|
HER-2 IHC expression 0 1+ 2+ |
1217 (53.5) 634 (27.9) 422 (18.6) |
13.1 (12.2-14.5) 14.2 (12.5-16.1) 14.7 (12.8-17.2) |
0.3099 |
Reference 0.95 (0.84-1.07) 0.91 (0.79-1.04) |
0.53 (0.50-0.56) 0.55 (0.51-0.59) 0.57 (0.53-0.62) |
|
No. of metastatic sites 1 2 3 4 5 and 6 |
1129 (49.7) 603 (26.5) 328 (14.4) 157 (6.9) 56 (2.4) |
19.8 (18.1-22.2) 11 (9.8-12.3) 9.1 (6.9-11.2) 4.6 (3.5-5.6) 2.6 (2.2- 5) |
< 0.0001 |
Reference 1.72 (1.53-1.94) 1.99 (1.72-2.30) 3.16 (2.62-3.80) 4.61 (3.47-6.13) |
0.67 (0.65-0.70) 0.47 (0.43-0.51) 0.43 (0.38-0.49) 0.24 (0.18-0.32) 0.17 (0.10-0.31) |
|
Site of metastatic involvement (subgroup analysis in those with single metastatic site only after excluding brain metastases ) LN only Bone only Liver only Lung only Other only |
233 317 165 286 83 |
24.4 (21.8-33.5) 18.9 (16.6-24.7) 15.6 (13.3-19.4) 22.8 (17.6-26.5) 12.3 (10.2-23.0) |
0.0001 |
Reference 1.36 (1.08-1.72) 1.67 (1.29-2.17) 1.23 (0.97-1.56) 1.85 (1.34-2.55) |
0.8 (0.75-0.85) 0.67 (0.61-0.72) 0.61 (0.54-0.69) 0.7 (0.65-0.76) 0.5 (0.41-0.63) |
|
Location of metastases Cranial only Cranial +extra-cranial Extra-cranial only |
45 (2) 204 (9) 2024 (89) |
11.8 (7.2-19.8) 5.3 (4.5-7.2) 14.6 (13.6-15.8) |
< 0.0001 |
Reference 1.7 (1.16-2.49) 0.86 (0.60-1.22) |
0.47 (0.34-0.64) 0.32 (0.26-0.4) 0.57 (0.55-0.59) |
| Treatment characteristics | |||||
|
First-line chemotherapy None Single-agent Multi-agent |
613 (27) 714 (31.4) 946 (41.6) |
2.9 (2.6-3.3) 16.4 (14.6-18.4) 19.9 (18.1-22) |
< 0.0001 |
Reference 0.29 (0.25-0.33) 0.23 (0.21-0.26) |
0.18 (0.15-0.22) 0.61 (0.58-0.65) 0.71 (0.68-0.74) |
|
Immunotherapy No Yes |
1827 (80.4) 446 (19.6) |
11.5 (10.9-12.6) 25.6 (22.3-29.1) |
< 0.0001 |
Reference 0.49 (0.42-0.56) |
0.49 (0.47-0.51) 0.76 (0.72-0.80) |
|
Time from Dx to systemic therapy None < 2 weeks 2-4 weeks >4 weeks |
579 (25.5) 138 (6.1) 425 (18.7) 1131 (49.8) |
2.7 (2.4-3.1) 10.8 (9.2-15) 15.6 (14.2-16.8) 20.6 (19.3-22.6) |
< 0.0001 |
Reference 0.34 (0.28-0.43) 0.26 (0.23-0.31) 0.21 (0.18-0.23) |
0.47 (0.39-0.56) 0.61 (0.57-0.66) 0.71 (0.68-0.73) 0.17 (0.14-0.2) |
|
Surgery of distant site (LN or other site) No Yes |
2134 (93.9) 106 (4.7) |
13.1 (12.5-14.1) 29.2 (23.0-NE) |
< 0.0001 |
Reference 0.50 (0.38-0.66) |
0.53 (0.51-0.55) 0.76 (0.69-0.85) |
|
Radiation to the distant site No Yes |
1603 (70.5) 482 (21.2) |
12.6 (11.5-13.6) 14.7 (12.7-17.5) |
0.0204 |
Reference 0.86 (0.76-0.98) |
0.51 (0.49-0.54) 0.57 (0.53-0.61) |
|
Palliative treatment (to alleviate symptoms) No Yes |
1721 (75.7) 552 (24.3) |
14.5 (13.5-15.6) 11.3 (10.0-12.9) |
0.0037 |
Reference 1.18 (1.06-1.32) |
0.56 (0.54-0.59) 0.48 (0.44-0.53) |
Table 2.
Sub-group analysis of first-line chemotherapy receipt in each Charlson-Deyo comorbidity score groups.
Table 2.
Sub-group analysis of first-line chemotherapy receipt in each Charlson-Deyo comorbidity score groups.
| No. of patients |
Median OS in months (95% CI) |
Logrank p-value | Hazard Ratio (95% CI) |
12-month survival estimates | |
|---|---|---|---|---|---|
| Charlson-Deyo comorbidity score 0; no. of patients= 1732 (76.2%) | |||||
|
First-line chemotherapy None Single-agent Multi-agent |
401 550 781 |
3.3 (2.9-4.0) 17.3 (15.5-19.7) 20.1 (18.4-22.4) |
<0.0001 |
Reference 0.31 (0.27-0.36) 0.26 (0.23-0.3) |
0.22 (0.18-0.27) 0.65 (0.61-0.69) 0.72 (0.69-0.75) |
| Charlson-Deyo comorbidity score 1; no. of patients= 339 (14.9%) | |||||
|
First-line chemotherapy None Single-agent Multi-agent |
111 112 116 |
2.4 (1.7-3.3) 13.1 (9.6-17.7) 19.9 (16.4-29.1) |
<0.0001 |
Reference 0.28 (0.21-0.38) 0.19 (0.14-0.26) |
0.15 (0.09-0.24) 0.51 (0.43-0.62) 0.7 (0.62-0.79) |
| Charlson-Deyo comorbidity score 2; no. of patients= 118 (5.2%) | |||||
|
First-line chemotherapy None Single-agent Multi-agent |
52 31 35 |
2.2 (1.4-3.4) 13.2 (10.9- NE) 16.8 (8.6-25.2) |
< 0.0001 |
Reference 0.19 (0.11-0.33) 0.21 (0.13-0.35) |
0.08 (0.03-0.21) 0.57 (0.41-0.77) 0.54 (0.4-0.74) |
| Charlson-Deyo comorbidity score=3 or more; no. of patients= 84 (3.7%) | |||||
|
First-line chemotherapy None Single-agent Multi-agent |
49 21 14 |
2.2 (1.5-3.7) 10.9 (5.3-21.2) 12.1 (7.5- NE) |
< 0.0001 |
Reference 0.3 (0.16-0.54) 0.28 (0.14-0.56) |
0.1 (0.04-0.24) 0.41 (0.24-0.7) 0.5 (0.3-0.84) |
Table 3.
Multi-variate Cox proportional Hazard analysis.
| Hazard ratio (95% CI) | Overall p-value | |
|---|---|---|
|
Charlson-Deyo score 0 1 2 3 |
Reference 1.23 (1.07-1.42) 1.57 (1.27-1.93) 1.97 (1.55- 2.51) |
< 0.0001 |
|
Histology Invasive ductal carcinoma Invasive lobular carcinoma Adenocarcinoma with metaplasia Adenocarcinoma NOS Other carcinoma |
Reference 1.04 (0.80-1.35) 0.83 (0.60-1.14) 1.29 (1.03-1.62) 1.54 (1.29-1.82) |
< 0.0001 |
|
No. of metastatic sites 1 2 3 4 5 and 6 |
Reference 1.90 (1.69-2.15) 2.16 (1.86-2.5) 3.58 (2.96-4.33) 4.81 (3.61-6.42) |
< 0.0001 |
|
First-line chemotherapy None Single-agent and Multi-agent |
Reference 0.28 (0.25-0.32) |
< 0.0001 |
|
Immunotherapy No Yes |
Reference 0.56 (0.49-0.65) |
< 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



