
Submitted:
18 April 2024
Posted:
18 April 2024
You are already at the latest version
Abstract
Keywords: Tendon injuries; Mallet finger; Suture techniques
Keywords:
tendon injuries
; mallet finger
; suture techniques
1. Introduction
Tendinous mallet finger deformities occurs when forced flexion to an extended distal interphalangeal (DIP) joint damages the extensor apparatus inserting onto the base of the distal phalanx. Although closed trauma is the most common cause of damage, open trauma is also recognized as etiological cause [1,2]. Regardless of the type and etiology of the deformity, it is imperative to attempt to repair it, either conservatively or surgically, to reduce the possibility of complications, such as persistent extension lag of the DIP joint and its instability. In addition, mallet finger deformity may cause a swan-neck deformity as a deformity in one interphalangeal (IP) joint brings about a compensatory deformity in the adjacent IP joint. This complex deformity produces pain, functional problems in finger flexion, and disruption of the functional grasp as well as dissatisfied cosmetic appearance [3,4]. Most medical experts advise non-operative treatment where a finger splint is applied in DIP extended position with an immobilization period of 6–12 weeks. The most common mean extension lag in the literature is approximately five to ten degrees, but the deficit can be much higher in some patients, leading to permanent functional disability and unpleasing aesthetic results [5,6]. There have been many studies which propose effective treatments for open and chronic mallet injuries as well as mallet fractures. However, surgical treatment of acute closed tendinous mallet injuries has not been well established, even though many surgical techniques have been tested to determine the optimal method for treating tendinous mallet finger deformities. In this study, we have proposed a refined technique that uses an open approach and a direct suture method to treat closed tendinous mallet finger injuries.
2. Materials and Methods
Between 2019 and 2021, 19 patients with closed mallet fingers without fracture were enrolled in our study; patients with open injuries or bony injuries were excluded from the study. A retrospective chart study was performed on the participants. There were 12 males (63%) and 7 females (37%) aged between 19 and 54 years (mean: 31 years). The small finger was injured in seven cases (37%), index finger in six cases (31%), middle finger in three cases (16%), ring finger in three cases (16%). Injury duration was <1 week in eight, <2 weeks in six, 2–4 weeks in three, and 4–8 weeks in two cases. The patients were examined at an outpatient clinic after 6 months from the beginning of treatment, where data on pain, extension lag, and loss of flexion were recorded. The extensor lag before surgery was between -25 and -45 degrees (mean: -29 degrees). Outcomes were classified according to the criteria described by Crawford (Table 1). The Institutional Review Board of Seoul National Bundang University Hospital approved this study (IRB No. B-2301-804-106). This study conformed to the World Medical Association Declaration of Helsinki and subsequent amendments and was conducted in accordance with the highest ethical standards.
3. Surgical Technique
The procedure was performed under regional anesthesia. After administration of the local anesthetic, we waited for approximately 10 min for anesthesia to take effect. A gold post-shaped line was drawn on the dorsal aspect of the DIP joint of the affected finger. The incision was made to be wide enough to expose the extensor tendon insertion area and the site of laceration on the base of the distal phalanx. The skin incision was superficial to the extensor paratenon, which was raised obliquely to avoid overlapping with the skin incision. Retraction of the very thin paratenon edges showed separation of the tendon ends. Both the proximal and distal edges of the extensor were undermined by approximately 3 mm to facilitate the suture. Meticulous gentle approximation of the flat tendon ends using 6-0 PDS was the most reliable approach. Slowly absorbable suture materials, such as Dexon or nonabsorbable nylon, can also be used. The sutures should be placed 1 or 2 mm away from the free ends of the separate tendon with simple interrupted sutures, eliminating the need for multiple passages through these fragile lacerated structures. After tendon repair, the reflected paratenon was reapproximated with 6-0 PDS to avoid tendon adhesion to the skin, which could act as a protective barrier between the skin and tendon. The skin was sutured with one-layer closure using 5-0 nylon thread. Proper immobilization is essential for preservation of tenuous repairs and a delicate care with the application of a fine Kirschner wire to keep the DIP joint in extension ensures the best possible outcome. The DIP joint is fixed in a neutral position or slightly extended using a 0.9 mm Kirschner wire in a retrograde manner through the fingertip across the joint. The pin was cut beneath the skin and a protective garment or finger orthosis was applied. Postoperatively, only the DIP joint was immobilized in a finger orthosis splint. Patients were encouraged to actively move the proximal interphalangeal and metacarpophalangeal joints which may enable immediate return-to-work after treatment in some patients. During the orthosis period, the affected finger was maintained on a flat surface in a finger splint to allow the patient and clinician to inspect the skin and cleanse the pin insertion site. The Kirschner wire was removed after 4 weeks, the DIP joint was gradually weaned from immobilization, and night splinting was recommended for two additional weeks (Figure 1).
4. Results
The senior author (SC Eun) treated nineteen non-bony mallet finger patients, between 2019 and 2021, using the direct tendon suture and paratenon repair technique. Functional outcomes were evaluated using Crawford’s criteria. The follow-up period was between 3 and 12 months (mean: 5.4 months). All patients resumed their daily activities after 4 weeks. The mean initial DIP joint extension lag was 29 degrees (range: 25–45 degrees). The mean DIP joint extension lag at the final follow-up was 6.5 degrees (range: 0–15 degrees. 89% of the patients demonstrated excellent or good outcomes according to Crawford’s evaluation criteria (Figure 3). The Crawford grade was excellent in three fingers, good in 14 fingers, and fair in two fingers. One patient showed a relapse due to poor compliance with medical advice, but skin necrosis, pin-track/steel-tread infections, or postoperative pain was not observed (Table 2).
Figure 2.
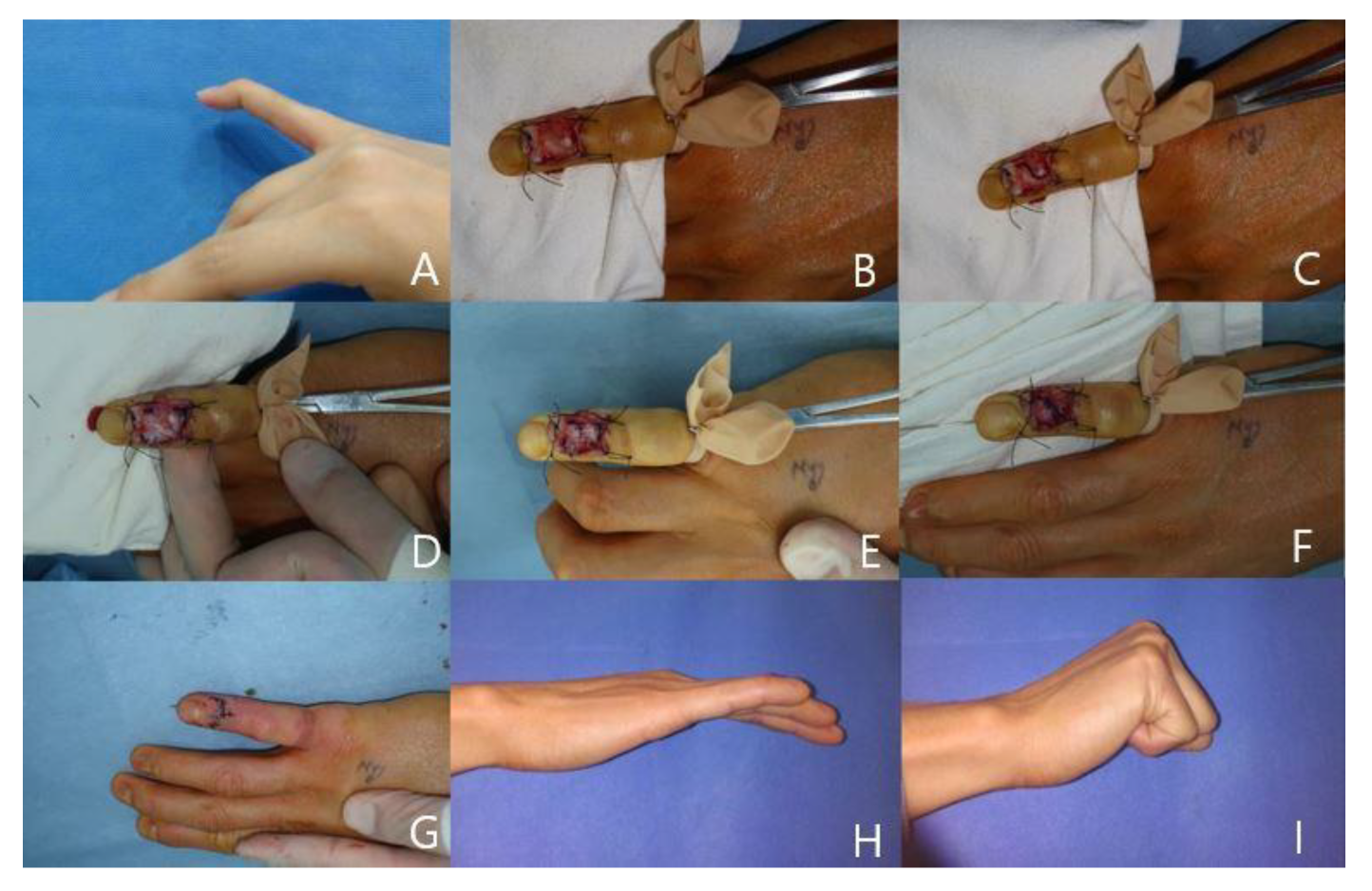
(A) A 31-year-old female patient with right little finger mallet injury and extension lag was noted. (B) After skin incision and reflection. (C) Paratenon incision design. (D) Tendon severance noted. (E) Tendon sutured. (F) Paratenon sutured. The DIP joint is fixed in neutral position by using a 0.9 mm Kirschner wire. (G) After skin closure. (H,I) Finger extension and flexion position after 6 months follow up period. It shows excellent results.
Figure 2.
(A) A 31-year-old female patient with right little finger mallet injury and extension lag was noted. (B) After skin incision and reflection. (C) Paratenon incision design. (D) Tendon severance noted. (E) Tendon sutured. (F) Paratenon sutured. The DIP joint is fixed in neutral position by using a 0.9 mm Kirschner wire. (G) After skin closure. (H,I) Finger extension and flexion position after 6 months follow up period. It shows excellent results.
Patient Reports
Case 1
A 31-year-old woman injured her right 5th finger and was diagnosed with acute tendinous mallet with -55o of extension lag of DIP joint. At 2 weeks after the initial injury, we performed an direct suture with paratenon repair technique. At 6 months after surgery, range of motion at the DIP joint improved to 0 o of extension with no flexion loss. According to Crawford’s criteria, the patient had excellent result with no complications (Figure 2).
Case 2
A 43-year-old man injured his left 3rd finger and was diagnosed with acute tendinous mallet finger with -25o of extension lag of DIP joint. At 1 weeks after the initial injury, we performed an direct suture with paratenon repair technique. At 4 months after surgery, range of motion at the DIP joint improved to 0 o of extension with no flexion loss. According to Crawford’s criteria, the patient had excellent result (Figure 3).
Case 3
A 23-year-old man injured his right 4th finger and was diagnosed with acute tendinous mallet finger with -35o of extension lag of DIP joint. At 1 weeks after the initial injury, we performed an direct suture with paratenon repair technique. At 12 months after surgery, range of motion at the DIP joint improved to -5o of extension with no flexion loss. According to Crawford’s criteria, the patient had good result (Figure 4).
5. Discussion
Closed mallet finger is one of the most common chief complaints in the cases of hand trauma, leading to loss of active extension of the DIP joint. Sudden flexion of the DIP joint causes the extensor tendon to be stretched, partially torn, ruptured, or avulsed with a bony fragment at the base of the distal phalanx. The numerous conservative and operative methods described for the treatment of mallet finger deformities indicate that none of these approaches result in good or very good functional outcomes. Especially, acute closed tendinous mallet finger has not been well documented for its gold standard management. Several studies have demonstrated that a very good outcome is possible through continuous splinting of the DIP joint in neutral extension or slight hyperextension for 6–8 weeks in an acute tendinous mallet finger case. However, a high level of patient compliance is an essential prerequisite for the successful treatment because the balance of the extensor mechanism tends to be easily disturbed by even a small carelessness. Suboptimal immobilization and distraction of the healing tendon following compliance problem results in a persistent extension lag and a swan-neck deformity [7,8,9].
Skin sloughing or nail deformity is more likely to occur in surgical treatment than in conservative treatment. Several surgical techniques have been introduced to avoid surgical complications; however, some disadvantages still exist. The pull-out wire technique, one of the most widely used conventional treatments, can cause pressure sores or sensory neuroma under the button, prolonging the rehabilitation period [9,10]. Transarticular K-wire fixation of the DIP joint results in PIP joint flexion contracture and stiffness in some patients [11]. In addition, the Fowler central slip release technique, hemilateral band technique, percutaneous tenodermodesis, and micro screw fixation have a risk of PIP hyperextension, complete detachment of the hemilateral band from the extensor hood or boutonniere deformity, suture failure following skin breakage, and bone fragmentation [12,13,14,15].
However, the technique described in this study, a direct open suture technique, provided excellent and good results in 89% of patients without complication. Our direct suture technique has the following advantages: (1) it allows early postoperative mobilization and leads to early free hand movement, (2) a successful functional recovery is expected, (3) it helps healing of the damaged extensor and the normal alignment of fingers is maintained, and (4) the surgical technique is simple and easy to follow. A mallet finger treatment outcome assessment classification was proposed by Crawford. It is the most commonly used classification for outcome assessment after mallet finger. An excellent outcome is no pain with full range of motion at the DIP joint, less than 10-degree extension deficit is a good outcome, 10–25 degrees of extension deficit with no pain is a fair outcome, and more than 25 degrees of extension deficit or persistent pain is considered a poor outcome [16].
The intrasynovial tendon surface is covered with a lining cells of the visceral sheet of the synovial sheath, the epitenon, that permits smooth, low friction tendon gliding under the pulley. The extrasynovial tendon surface is covered with loose connective tissue called paratenon [17]. Unlike the epitenon, the paratenon is a loose areolar tissue on the surface of tendons that has an abundance of vascular networks and has been used to cover the exposed tendon or bone.The paratenon functions as an elastic sleeve that permits some movement of the tendon against the surrounding tissue [18]. The paratenon around the tendon may help prevent adhesion of surrounding tissues. Thus, after tendon repair, the paratenon may prevent adhesion by forming a gliding surface for the tendon [19].
In all of our cases, Kirschner wire fixation and external splinting were applied to prevent flexion of the distal phalanx while changing the dressing, and no complications related to either Kirschner wire or splint use were identified. However, maintaining the fingers in an extended position for a considerable period may lead to a stiff joint. Therefore, although we immobilized patients with a splint to protect the suture during daily activities, we allow patients to intermittently remove the splint when hygienic management is needed. After the protective device is removed, suture breakage is possible because patients can theoretically tear the suture with active flexion or direct trauma. Thus, it is important to educate the patients with the emphasis on protection and prevention of active DIP joint flexion in the early period for satisfactory outcomes.
In conclusion, direct tendon suture and paratenon repair technique is an effective method for the treatment of acute tendinous mallet fingers. Since it can promote the healing of tendons and reduce the friction, we recommend its wide clinical application.
Author Contributions
Conceptualization, S.E.; Formal analysis, S.L., and S.E.; Investigation, S.L. and S.E.; Data curation, S.E.; Writing-original drat, S.E.; Writiing-review & editing, S.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of Seoul National University (B-2301-804-106).
Informed Consent Statement
Patient consent was waived due to retrospective design of the study.
Data Availability Statement
The Data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Renfree, KJ. Acute, closed tendinous mallet injuries. J Hand Surg Am. 2014, 39, 2502–2505. [Google Scholar] [CrossRef] [PubMed]
- Thompson JS, Asheville NC, Littler JW, et al. The spiral oblique retinacular ligament (SORL). J Hand Surg. 1978, 3, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Griffin M, Hindocha S, Jordan D, et al. Management of extensor tendon injuries. Open Orthop J. 2012, 6, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Kontor, JA. Extensor tendon injuries and repairs in the hand. Can Fam Physician. 1982, 28, 1159–1163. [Google Scholar] [PubMed]
- Warren RA, Kay NRM, Ferguson DG. Mallet finger: comparison between operative and conservative management in those cases failing to be cured by splintage. J Hand Surg. 1988, 13, 159–160. [Google Scholar]
- Vernet P, Igeta Y, Facca S, et al. Treatment of tendinous mallet fingers using a stack splint versus a dorsal glued splint. Eur J Orthop Surg Traumatol. 2011, 15, 177–181. [Google Scholar]
- Georgescu AV, Capota IMV, Matei IRG. A new surgical treatment for mallet finger deformity: deepithelialised pedicled skin flap technique. Injury. 2013, 44, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Zhang L, Zuo YM, Huo YX, et al. Scar overlapping suture for treating chronic tendinous mallet finger in children. J Orthop Surg Res. 2019, 14, 1–5. [Google Scholar]
- Yao JM, Zhao FJ. Mallet finger deformities treated by buried purse-string suture. Chin J Traumatol. 2011, 14, 237–240. [Google Scholar]
- Jiang B, Wang P, Zhang Y, et al. Modification of the internal suture technique for mallet finger. Medicine. 2015, 94, e536. [Google Scholar] [CrossRef] [PubMed]
- Park JK, Cha JK, Min KT. Kirschner wire fixation with distal interphalangeal joint hyperextension for treatment of chronic tendinous mallet finger. J Hand Surg. 2020, 0, 1–2. [Google Scholar]
- Houpt P, Dijkstra R, Storm Van Leeuwen JB. Fowler’s tenotomy for mallet deformity. J Hand Surg. 1993, 18B, 499–500. [Google Scholar]
- Rozmaryn, LM. Central slip tenotomy with distal repair in the treatment of severe chronic mallet fingers. J Hand Surg Am. 2014, 39, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Kardestuncer T, Bae DS, Waters PM. The results of tenodermodesis for severe chronic mallet finger deformity in children. J Pediatr Orthop. 2008, 28, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Royen KV, Muneer M, Tsai TM. Percutaneous tenodermodesis for mallet fingers: an office-based procedure. Tech Hand Up Extrem Surg. 2021, 25, 56–58. [Google Scholar] [CrossRef] [PubMed]
- Rubin G, Ammuri A, Mano UD, Shay R, Svorai SB, Sagiv R, Rozen N. Outcome Differences between Conservatively Treated Acute Bony and Tendinous Mallet Fingers. J Clin Med. 2023, 12, 6557. [Google Scholar] [CrossRef] [PubMed]
- Momose T, Amadio PC, Zobitz ME, Zhao C, An KN. Effect of paratenon and repetitive motion on the gliding resistance of tendon of extrasynovial origin. Clin Anat. 2002, 15, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Carmont MR, Highland AM, Rochester JR, Paling EM, Davies MB. An anatomical and radiological study of the fascia cruris and paratenon of the Achilles tendon. Foot Ankle Surg. 2011, 17, 186–92. [Google Scholar] [CrossRef] [PubMed]
- Shibata R, Takeda S, Yamauchi KI, Hirata H. Use of Triceps Tendon and Paratenon Composite Graft for Extensor Tendon Reconstruction in the Hand: A Case Report. J Hand Surg Asian Pac Vol. 2022, 27, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A) After skin incision, extensor paratenon is designed to be raised obliquely, having no overlap with the skin incision. (B) After retraction of the paratenon edges, ruptured extensor digitorum tendon is identified and undermined. (C) Meticulous gentle approximation of the tendon ends is done with simple interrupted sutures, 1–2 mm away from the free ends of the tendon, to avoid multiple passages through these fragile structures. (D) After tendon repair, reflected paratenon is reapproximated to avoid tension adhesion to the skin.
Figure 1.
(A) After skin incision, extensor paratenon is designed to be raised obliquely, having no overlap with the skin incision. (B) After retraction of the paratenon edges, ruptured extensor digitorum tendon is identified and undermined. (C) Meticulous gentle approximation of the tendon ends is done with simple interrupted sutures, 1–2 mm away from the free ends of the tendon, to avoid multiple passages through these fragile structures. (D) After tendon repair, reflected paratenon is reapproximated to avoid tension adhesion to the skin.
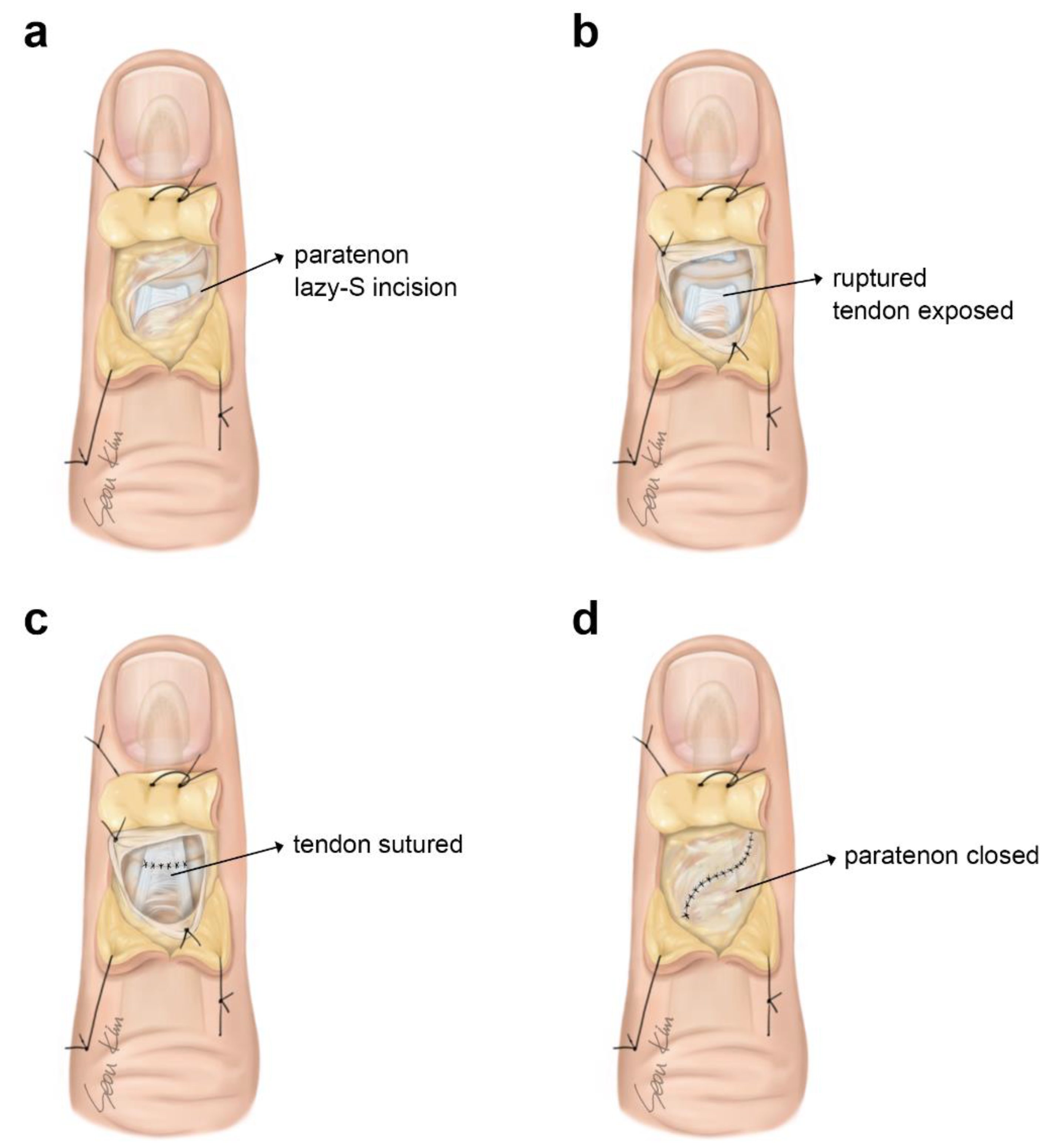
Figure 3.
(A) A 43-year old male patient witht tendinous mallet finger injury on his left third finger. (B) The gold-post skin incision. (C) Extensor paratenon designed to be raised. (D) Ruptured extensor digitorum tendon identified (E) Tendon sutured. (F) Skin closed. (G,H) Finger extension and flexion position after 4 months follow up period.
Figure 3.
(A) A 43-year old male patient witht tendinous mallet finger injury on his left third finger. (B) The gold-post skin incision. (C) Extensor paratenon designed to be raised. (D) Ruptured extensor digitorum tendon identified (E) Tendon sutured. (F) Skin closed. (G,H) Finger extension and flexion position after 4 months follow up period.
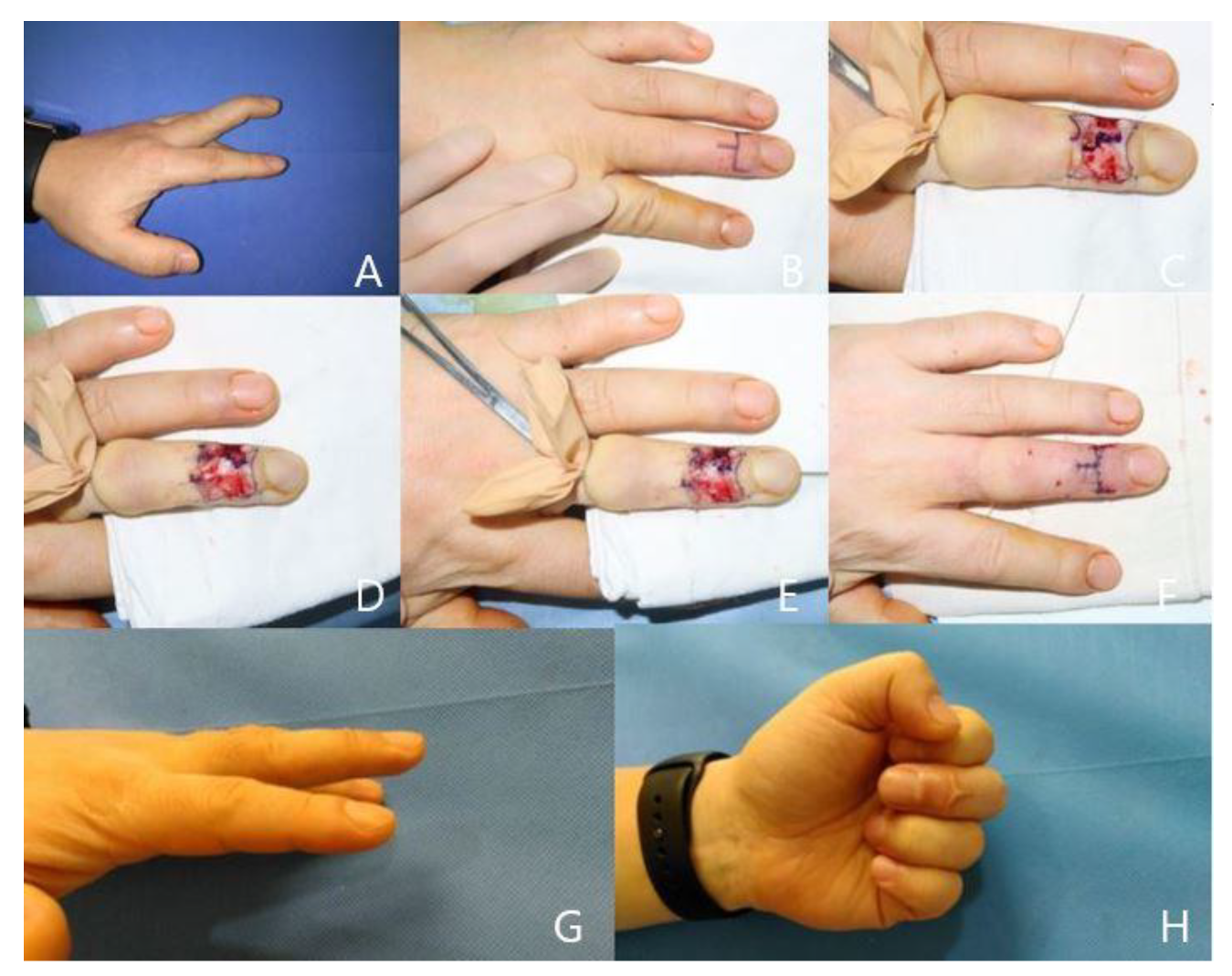
Figure 4.
(A) A 23-year-old male patient with right fourth finger mallet injury. (B) The extensor paratenon incision design. (C) Ruptured extensor digitorum tendon exposed (D) Tendon sutured. (E) Skin closed. (F) Twelve-month postoperative view with no extension lag.
Figure 4.
(A) A 23-year-old male patient with right fourth finger mallet injury. (B) The extensor paratenon incision design. (C) Ruptured extensor digitorum tendon exposed (D) Tendon sutured. (E) Skin closed. (F) Twelve-month postoperative view with no extension lag.
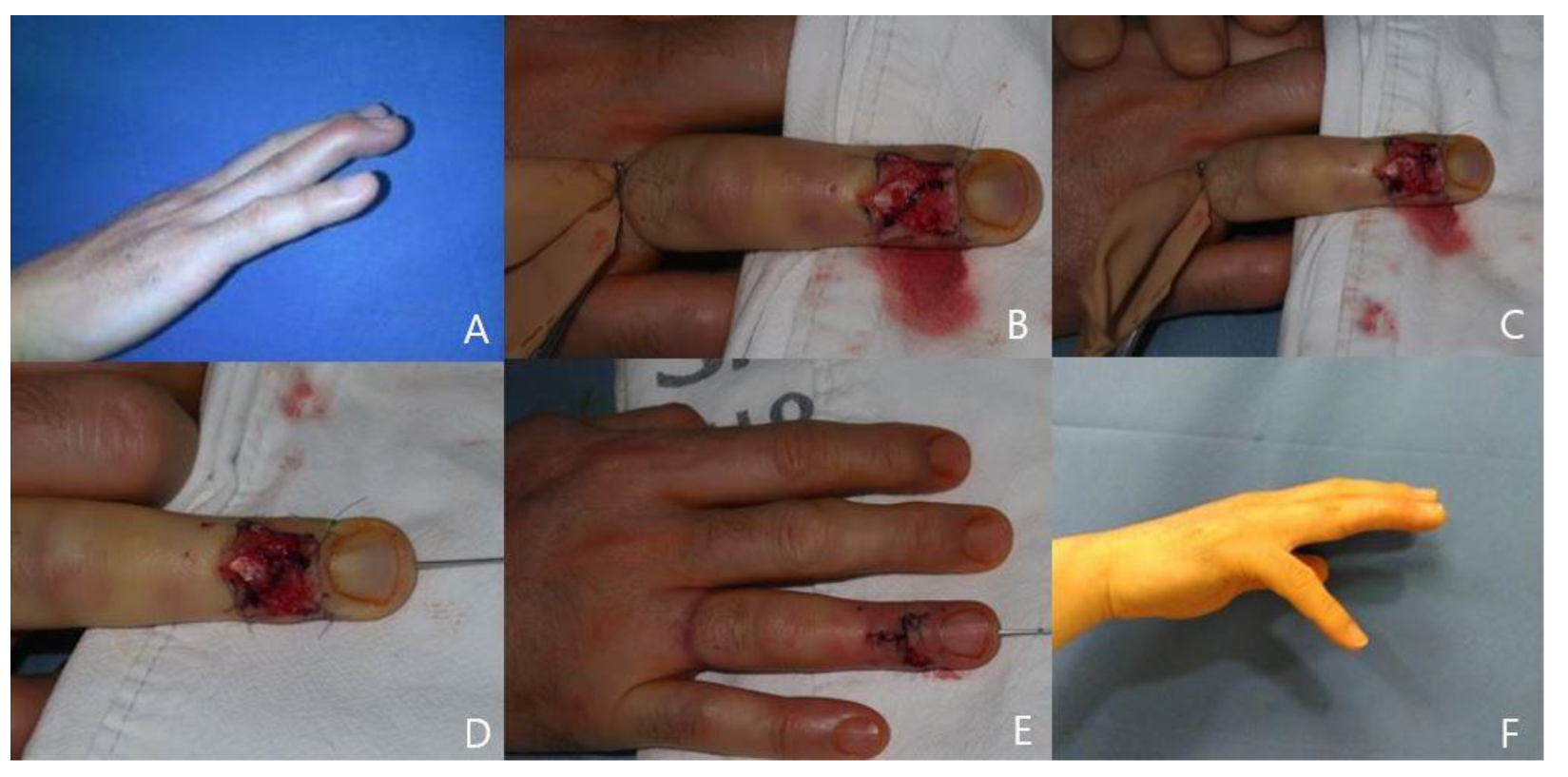

Table 1.
Crawford Criteria Assessment of Mallet Finger.
| Grade | Characteristics of DIP Joint |
| Excellent | Full extension, Full flexion, No pain |
| Good | Extension deficit 0 to 10, Full flexion, No pain |
| Fair | Extension deficit 10 to 25, Any flexion loss, No pain |
| Poor | Extension deficit >25, Persistent pain |
DIP, distal interphalangeal.
Table 2.
Patient demographics and perioperative evaluations.
| No. | Sex | Age (y) | Location | Follow-up (mo) | Extension lag (before) |
Extension lag (after) |
Crawford evaluation criteria |
| 1 | M | 43 | Rt 5th F | 6 | -25 | -5 | Good |
| 2 | F | 25 | Rt 2nd F | 3 | -30 | -10 | Good |
| 3 | F | 19 | Lt 5th F | 4 | -25 | -5 | Good |
| 4 | M | 43 | Lt 3rd F | 4 | -25 | 0 | Excellent |
| 5 | M | 32 | Lt 4th F | 3 | -35 | -5 | Good |
| 6 | M | 23 | Lt 2nd F | 6 | -25 | -10 | Good |
| 7 | M | 46 | Lt 5th F | 9 | -30 | -5 | Good |
| 8 | M | 45 | Lt 5th F | 8 | -40 | -10 | Good |
| 9 | M | 54 | Lt 2nd F | 4 | -35 | -25 | Fair |
| 10 | F | 31 | Rt 5th F | 6 | -35 | 0 | Excellent |
| 11 | M | 25 | Lt 2nd F | 3 | -30 | -5 | Good |
| 12 | M | 18 | Rt 3rd F | 4 | -45 | -15 | Fair |
| 13 | M | 23 | Rt 4th F | 12 | -35 | -5 | Good |
| 14 | M | 35 | Lt 2nd F | 6 | -25 | -5 | Good |
| 15 | M | 32 | Rt 5th F | 4 | -30 | -5 | Good |
| 16 | F | 61 | Rt 4th F | 4 | -30 | -10 | Good |
| 17 | F | 23 | Lt 4th F | 6 | -35 | -5 | Good |
| 18 | F | 52 | Lt 3rd F | 6 | -35 | -5 | Good |
| 19 | M | 21 | Lt 5th F | 5 | -25 | 0 | Excellent |
| Mean | 31.2 | Rt 2nd F | 5.4 | -29 | -6.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



