
Submitted:
21 April 2024
Posted:
22 April 2024
You are already at the latest version
Abstract
We report the case of a 61-year-old woman who was referred to the Oral Surgery and Implantology Unit of the University Hospitals of Geneva to take care edentulous sites after dental avulsions of teeth 11 and 21 following traumatic shock due to endotracheal intubation under general anaesthesia. The dental history revealed that the patient had a history of generalized chronic periodontitis that had been treated several years earlier. Treatment consisted, for the first time to our knowledge, of immediate insertion of implants at sites 11 and 21 with simultaneous bone augmentation in a single surgical procedure and immediate restorations.
Keywords:
Dental implant
; Immediate implant
; Immediate restoration
; Periodontitis
; Trauma
; Endotracheal intubation
Periodontitis, the major cause of tooth loss in adults [1], is an infection-driven inflammatory disease in which the composition of the dental plaque, a structurally and functionally organized biofilm, plays a significant role. Dental plaque accumulation at the gingival margin initiates an inflammatory response that, in turn, may lead in susceptible individuals to in irreversible destruction of the periodontal attachment and alveolar bone. This pathological condition represents in addition a risk factor in implant therapy and constitutes a challenge for fixed reconstructions on implants and even more in the context of immediate implant placement [2,3]. Teeth avulsion is one of the most common dental injuries during general anesthesia associated with laryngoscopy for patients with advanced periodontitis [4] that can be detrimental to the patient’s well-being, especially when the patient should not expect complications which significantly disrupt normal function and quality of life [5,6].
A 61-year-old woman was referred to the Oral Surgery and Implantology Unit of the University Hospitals of Geneva for treatment of edentulous sites after dental avulsions of teeth 11 and 21 following traumatic shock due to endotracheal intubation under general anesthesia performed to remove a laryngeal cyst. Past medical history was significant for pharyngeal dysesthesia and a supraglottic cyst. The dental history revealed that the patient had a history of chronic generalized periodontitis treated few years earlier. Clinical and radiological examination showed generalized bone loss especially at the edentulous sockets 11 and 21 and adjacent teeth 12 and 22.
Figure 1.
Clinical view (A) and intra-oral radiographs (B) showing the initial clinical status after dental avulsions due to endotracheal intubation as well as the severe chronic periodontal disease.
Figure 1.
Clinical view (A) and intra-oral radiographs (B) showing the initial clinical status after dental avulsions due to endotracheal intubation as well as the severe chronic periodontal disease.

The treatment plan was based on periodontal maintenance and replacement of edentulous sites 11, 21 using 2 single crowns screwed onto implants. Information regarding implant timing and therapeutic options for temporary prostheses was given to patient, including the benefits and risks. The timing of the implantation chosen and accepted by the patient was immediate implant placement and a provisional prosthetic phase based on 2 immediate restorations using temporary crowns screwed in resin under occlusion.
Our treatment consisted for the first time to our knowledge, upon the patient's awakening from general anesthesia and with her consent, to replace the avulsed teeth by immediately inserting dental implants followed by immediate screw-retained coronal restorations (Figure 2). Immediate placement of dental implants in extraction sockets has proven to be a safe and viable treatment option in case of socket type I [7]. This procedure became a strategy favored by clinicians owing to the associated advantages, such as reducing the number of surgical procedures, stress on the patient and morbidities, shortening treatment duration, and better managing of soft tissue and alveolar morphology. In our case, the socket was not ideal because it had suffered bone loss as part of the history of periodontal disease. Several studies have also reported that the high success rates of this technique were associated with the achievement of primary stability [8]. Bone anchorage for primary stability in immediate implantation primarily depends on the bone at the apical and palatal levels of the alveolus [8]. For this reason, particular attention must be paid to the proximity of neighboring anatomical structures such as the maxillary sinuses, nasal cavities, mandibular canal, and mental foramina. In case of post-extraction sockets in the context of a reduced periodontum, achieving primary stability can be even more complex due to the reduced amount of bone and requires a more meticulous and precise surgical procedure. In our patient, one of the difficulties was to obtain primary stability because, the residual bone height between the apical level of the sockets and the nasal cavity was 6mm, which greatly limited the possibility of apical anchorage. Typically, bone augmentation simultaneous with immediate implantation is required to fill the gaps between the vestibular cortex and the exposed implant surface [8]. In our case, after placing the implants, the filling was carried out. However, the socket being of reduced height, the part of the dehiscent implant surface was limited to only 3mm. Immediate implantation also offers the possibility of an immediate fixed provisional restoration, provided that primary stability is achieved and sufficient insertion torque of around 35 N/cm is applied [9]. In our patient, although the periodontium was reduced in a context of a history of generalized chronic periodontitis, an insertion torque of 38 and 40N/cm was obtained at the level of implants 11 and 21 respectively and immediate restorations were carried out for the first time in this context. The patient followed regular dental and dental prosthesis checkups as well as oral hygiene recall appointments three times a year. During these appointments, the examiner recorded the clinical periodontal parameters and checked the status of the prosthesis. At the end of the appointments, a session of prophylaxis was performed, as necessary. At 3-year follow-up she showed functional results without any recurrence or complications observed and the patient was fully satisfied with the treatment received (Figure 3). Our case highlights that immediate implant placement with immediate restauration can be a good valid alternative to standard treatment in case of non-ideal socket with history of periodontitis.
Author Contributions
Conceptualization, A.P. and T.L.; validation, A.P. and T.L.; investigation, A.P. and A.B.F.; writing—original draft preparation, AP. and A.B.F.; writing—review and editing, A.P. and T.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The presented study adhered to the Helsinki Declaration of ethical principles by the World Medical Association. The study did not require approval of the Ethics Commission on Human Research of Geneva (CCER-Geneva) according to the Federal Human Research Act (Art.3al.a) since the study involved less than five patients.
Informed Consent Statement
Written informed consent was obtained from the patient to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Könönen, E.; Gursoy, M.; Gursoy, U.K. Periodontitis: A Multifaceted Disease of Tooth-Supporting Tissues. J. Clin. Med. 2019, 8, 1135. [Google Scholar] [CrossRef] [PubMed]
- Perez, A.; Layac, M.; Lombardi, T. Immediate Implant Placement at an Inflammatory Periapical Cyst Site in the Aesthetic Area. Preprints. 2024, 2024011883. [Google Scholar] [CrossRef]
- Perez, A.; Hamzah, S.; Lombardi, T. Immediate versus Delayed Implant Placement in Patients with Tooth Agenesis: An In-Line Retrospective Pilot Study Comparing Clinical and Patient-Related Outcomes. Appl. Sci. 2023, 13, 9368. [Google Scholar] [CrossRef]
- Neto, J.M.; Teles, A.R.; Barbosa, J.; Santos, O. Teeth Damage during General Anesthesia. J. Clin. Med. 2023, 12, 5343. [Google Scholar] [CrossRef] [PubMed]
- Ansari, S.; Rajpurohit, V.; Dev, V. Dental Trauma due To Intubating during General Anaesthesia: Incidence, Risks Factors, and Prevention. Oral Health Dent. Manag 2016, 31, 33. [Google Scholar]
- Lee, J.Y.; Divaris, K. Hidden consequences of dental trauma: The social and psychological effects. Pediatr. Dent. 2009, 31, 96–101. [Google Scholar] [PubMed]
- Elian, E.; Cho, S.; Froum, S.; Smith, R.B.; Tarnow, D.P. A simplified socket classification and repair technique. Pract Proced Aesthet Dent. 2007, 2, 99–104. [Google Scholar]
- Hämmerle, C.H.F.; Chen, S.T.; Wilson, T.G. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants. 2004, 1 9 Suppl, 26–28. [Google Scholar] [PubMed]
- Greenstein, G.; Cavallaro, J. Implant Insertion Torque: Its Role in Achieving Primary Stability of Restorable Dental Implants. Compend Contin Educ Dent. 2017, 38, 88–95. [Google Scholar] [PubMed]
Figure 2.
(A-N). Intraoperative view of showing sockets after curettage (A, B) and control of the drilling axes of site 11 and 21 (C, D), occlusal view showing implant bed preparation (E). Occlusal (F, G) and buccal (H) view after placement of implants (Bone Level, Ø3.4x10 mm, Straumann, Switzerland) at sites 11 and 21, showing small buccal bone defect ‘’dehiscence- like’’ at sites 11 and 21. Buccal view with transfer device screwed onto the implants for impression taking (I). Clinical view showing the augmented sites using autogenous bone chips and alloplastic bone (BoneCeramicTM, Straumann, Switzerland), after the impression (J) and 3 hours later (K) during fixation of the screw-retained temporary crowns (L, M) and periapical 2D radiographs taken immediately after implants placement (N).
Figure 2.
(A-N). Intraoperative view of showing sockets after curettage (A, B) and control of the drilling axes of site 11 and 21 (C, D), occlusal view showing implant bed preparation (E). Occlusal (F, G) and buccal (H) view after placement of implants (Bone Level, Ø3.4x10 mm, Straumann, Switzerland) at sites 11 and 21, showing small buccal bone defect ‘’dehiscence- like’’ at sites 11 and 21. Buccal view with transfer device screwed onto the implants for impression taking (I). Clinical view showing the augmented sites using autogenous bone chips and alloplastic bone (BoneCeramicTM, Straumann, Switzerland), after the impression (J) and 3 hours later (K) during fixation of the screw-retained temporary crowns (L, M) and periapical 2D radiographs taken immediately after implants placement (N).
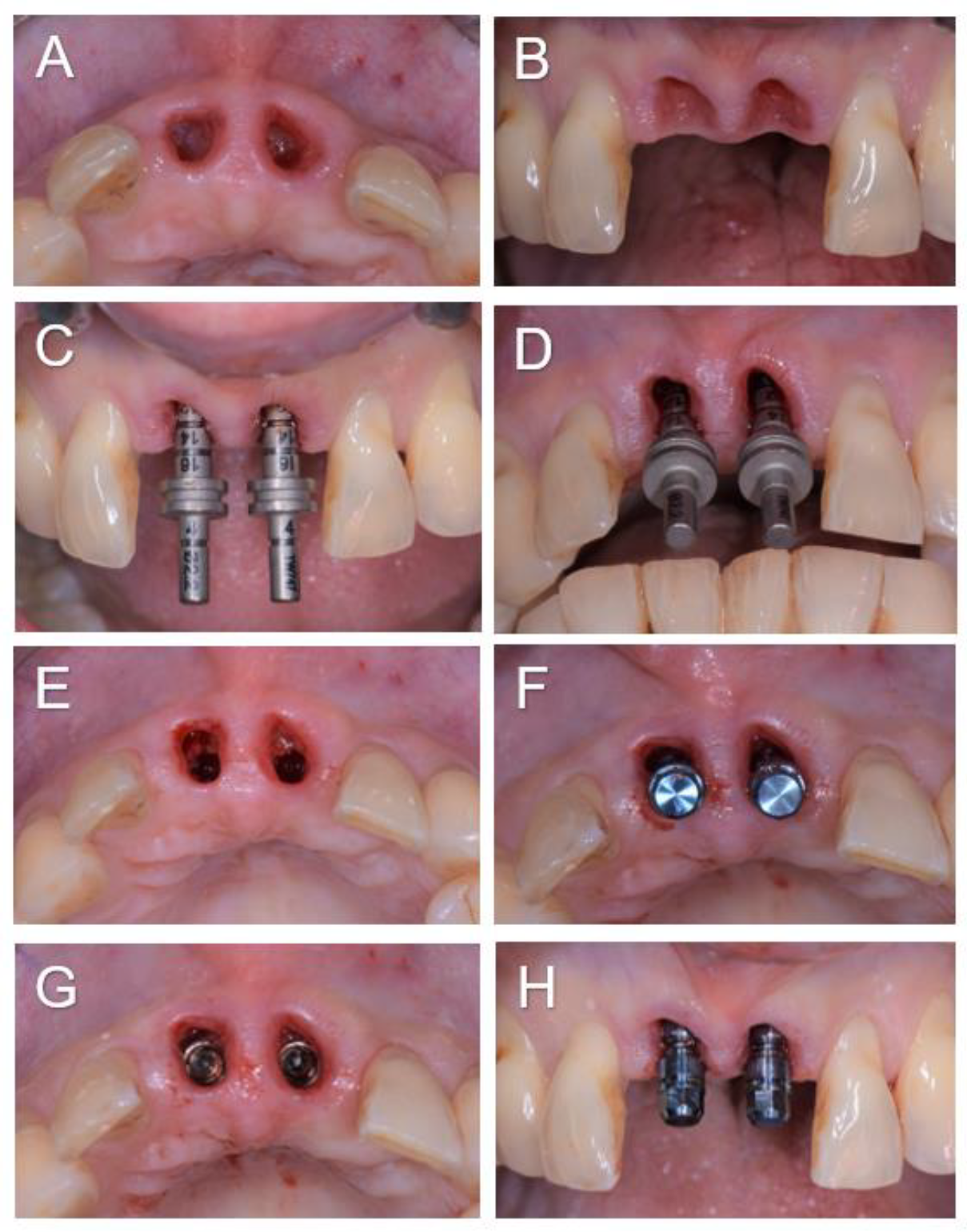
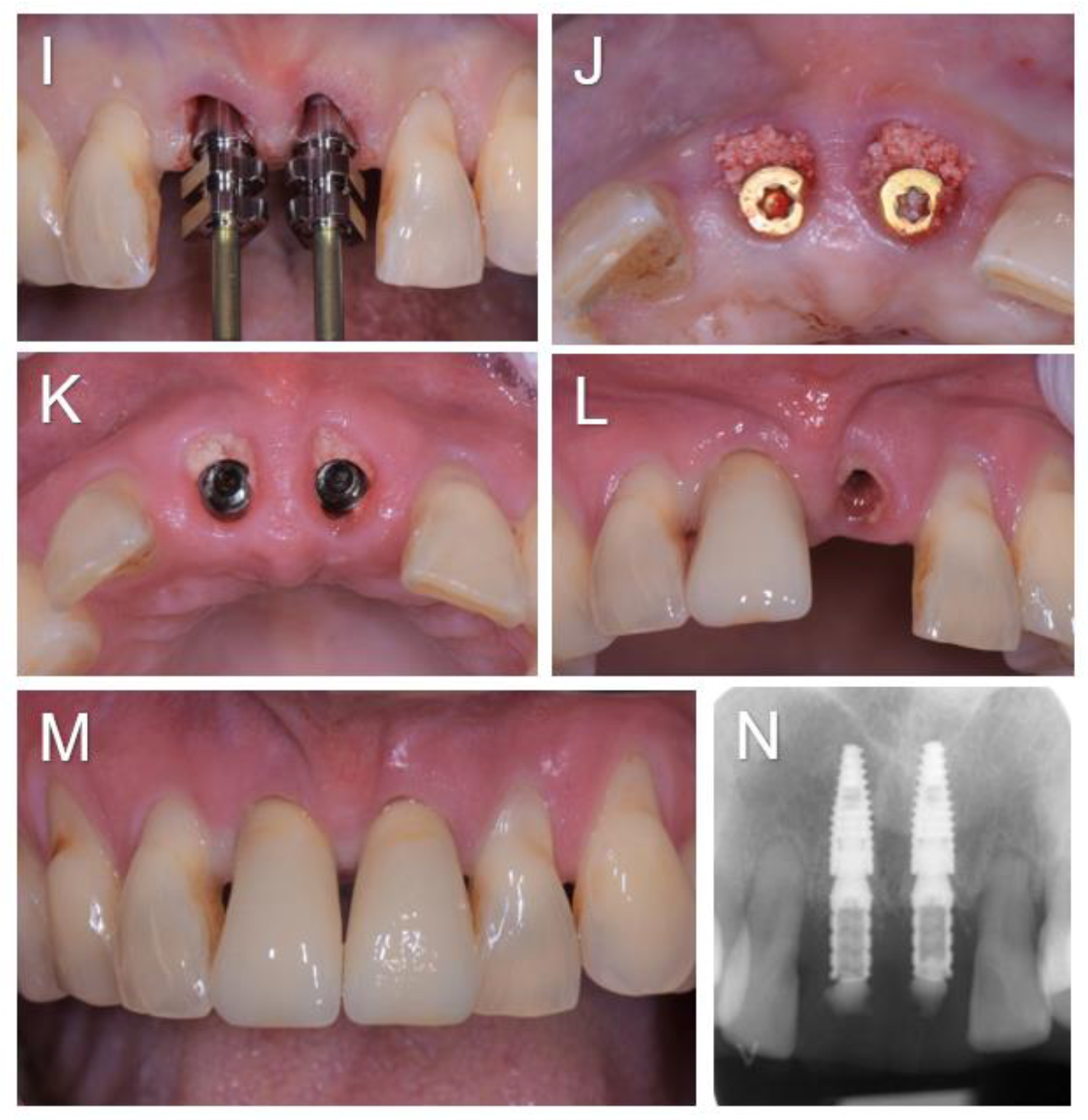
Figure 3.
(A-D). Soft tissues condition when the two screw-retained single-unit crowns (E-max. press) were delivered 3 months post-operatively (A, B), and clinical and radiographic examination at 3-year follow-up (C-G).
Figure 3.
(A-D). Soft tissues condition when the two screw-retained single-unit crowns (E-max. press) were delivered 3 months post-operatively (A, B), and clinical and radiographic examination at 3-year follow-up (C-G).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



