
Submitted:
20 April 2024
Posted:
22 April 2024
Read the latest preprint version here
Abstract
Hamman’s syndrome is a rare condition that mostly affects young males, often with a predisposition of asthma. It includes the presence of free air in the mediastinum and subcutaneous emfysema with no other underlying cause such as trauma or infection. It occurs spontanously and often in association with prolonged valsalva manouvre. This might explain why there are some cases of Hamman syndrome among young females giving birth. Here we present a case report of a 24-year- old primigravida with Hamman’s syndrome. She presented with symptoms a few hours after an uncomplicated vaginal delivery at 40+1 pregnancy week. The symptoms resolved spontanously after a few days of observation. We also give a systemic review of reported cases since 2000 to provide overview on pathomechanism, symptoms, diagnostics, treatment and management of this condition. Hamman’s syndrome is a rare, usually benign, but potentially serious complication that can occur during the second stage of labour. Diagnostics include inquiring about typical symptoms, clinical examination and chest x-ray or CT scan. Treatment is usually conservative with oxygen, bronchodilators and pain relief. The reccurence rate is low and there is no contraindication to vaginal delivery in future pregnancies. However, it is suggested that physicians and midwives be cautious and consider low threshold for instrumental delivery or caesarean section to avoid excessive valsalva manoeuvre.
Keywords:
Delivery
; Hamman’s syndrome
; Pneumomediastinum
; Pregnancy
Introduction
Spontaneous pneumomediastinum (SPM) during labour is a rare event, occurring in about 1 in 100 000 deliveries. Together with subcutaneous emphysema it is called Hamman syndrome [1]. The condition was named after Louis Hamman (1877-1946), the physician who described it in several case reports from 1939 to 1945 in post partum women [2,3].
SPM is defined as the presence of free air in the mediastinum, with no underlying trauma and mostly affects young males and pregnant females. It may be associated with a pulse-synchronous crunching sound, reffered to as the «Hamman’s sign» best heard when the patient is lying in the left lateral decubitus position [4,5].
Hamman’s syndrome may occur during prolonged labor, usually in the second stage, after prolonged valsalva maneuver. Other predisposing events may be intensive coughing, retching/vomiting or physical activity [6].
The condition is usually benign and self-limiting, but in rare cases there may be complications such as significant dyspnea and chest pain, and even development of malignant pneumomediastinum, which requires surgical intervention [7]. In this paper, we report a case of Hamman’s syndrome in a 24-year-old primigravida with underlying asthma, and we are reporting on the pathomechanisme and management of this condition with regards on overview of 42 other published cases in the last two decads.
Case Presentation
A 24-year old primiparous woman, with a normal pregnancy, presented to the maternity ward in spontaneous labour, with regular uterine contractions at 40+1 weeks. She was a non-smoker and denied drinking alcohol or using illict drugs. Her body mass index was 27.1, and her past medical history was significant for depression, ADHD (Attention Deficit Hyperactivity Disorder) and childhood asthma, without need for medical treatment. There was no history of any heart condition.
In the latent phase of delivery, she recieved morphine for analgesia. The water broke spontaneously, and the amniotic fluid was discolored. The patient had normal temperature and there was no fetal tachycardia or other signs of fetal distres son CTG. The active phase of labor lasted for three hours with normal progress. After one hour of passive descent, she started pushing, and the second stage lasted for 30 minutes. It was a spontaneous vaginal delivery of a healthy baby with normal Apgar score (9-10-10) weighting 4170 g. There was a normal expulsion of the placenta, and there were normal bleeding.
Eight hours after delivery, she complained of pain in the right ear, swelling and pain in the neck, chest tightness, shortness of breath, dysphagia, odynophagia and pain in the upper thorax on the right side. Her vital signs were stable (BP 128/67 mmHg, pulse 91/min., temperature 36.0, respiratory rate 14/min., oxygen saturation 99% on room air). ECG was unremarkable. Blood gas showed normal values with pH 7.45, pCO2 4.2. PCR- test from nasopharynx was negative for viral infections. There were no findings on otoscopy. On palpation, there were subcutaneous crepitations in the neck, parasternal region, right axillary fossa, clavicle and over the chest. Auscultation of the heart and lungs was normal. A chest X-ray (Figure 1) was taken immediately, revealing subcutaneous emphysema extending bilaterally to the neck, but more prominent on the right side, and suspicious for pneumomediastinum. There were no signs of pneumothorax or esophageal or sceletal pathology. The heart configuration was normal. The patient received 1 g of paracetamol and 2.5 mg of morphine intravenously. The situation was clinicaly stable. The next day, a CT scan (Figure 2) without contrast was performed, confirming pneumomediastinum, with air extending from diaphragma up to the thoracic apeces and across larynx. There were descreet amounts of pleural fluid bilaterally, and subcutaneous emphysema from the base of the skull to the neck and upper thorax.
The patient was reviewed by the medical team (radiologist, gynecologist and surgeon), and diagnosed with Hamman`s syndrome. As the patient was hemodynamically stable, she was managed conservatively with observation and analgetics. Her symptoms resolved gradually over the next three days and she was discharged home on her third day post partum. She was advised to avoid strenous physical activity for the next four weeks. On follow up at the 6-weeks postnatal, she was in well being and completely without symptoms. Follow-up correspondance was also done over the phone at five months. The patient had recovered well, and was now practicing normal physical activity.
Discussion
Hamman’s syndrome is a rare clinical entity. Its incidence is 1:100 000 women giving birth. The incidence is higher in the case og accidents og emergencies and has a male predisposition, accounting for 76% of cases [8]. It is believed to be a result of a sudden increase in intra-alveolar pressure. Mostly it is associated with valsalva manouver, extensive vomiting, or coughing, all of which can occur in pregnancy and labour.
There have been several cases on Hamman’s syndrome occuring in labour, but it has also been reported in association with other medical conditions, such as diabetic ketoacidosis with repeated vomiting or Kussmaul breathing [9,10] and bronchial asthma, with vomiting and coughing as common precipitating factors [11,12]. There has also been reports of SPM occuring after intense coughing during strenous physical activity [13] or hyperemesis gravidarum [14].
In our case, extensive breathing during the first stage and intensive Valsalva manouver in the second stage of labour in a patient with an underlying bronchial asthma, led to the development of symptoms of Hamman’s syndrome after delivery. The CT scan of the chest was taken to exclude other severe diseases like pulmonary embolism, amniotic fluid embolism, myocardial infarction and Boerhaave syndrome.
The pathophysiology of Hamman’s syndrome is explained as follows: The intra-alveolar pressure is acutely increased during the Valsalva manoeuvre causing rupture of marginal alveoli adjacent to blood vessels. The free air moves from ruptured alveoli along peribronchial vascular sheaths towards the hilum of the lung. From there, it extends proximally and can spread within the mediastinum, pericardium, neck, subcutaneous tissue and retroperitoneum. The absence of transverse fascial planes in the mediastinum allows the unobstructed passage of air along tissue planes into the neck and around the larynx. The air may also be trapped between the parietal and visceral pleura, causing pneumothorax. The pressure of the interstitial air rarely causes respiratory compromise [1]. Coughing, vomiting, screaming and the force of pushing in labor, all together, can increase the intrathoracic pressure.
The most common symptoms are chest (retrosternal) pain radiating to the back or neck, dyspnea, and swelling of face and neck. The crepitus palpable in the face and neck is pathognomonic of the condition [4,15]. Other symptoms include change of voice (dysphonia), cough, sore throat, tachycardia, dysphagia and haemoptysis. A characteristic sign is the bubbling or crunching sounds over the heart, synchronous with the cardiac cycle known as Hamman’s sign or murmur. The occurence of the symptoms, time onset after/during delivery, severity of the condition and management can be very variable, as it is described in our summarized overview on the reported cases over the last two decades (Table 1).
In our case, the woman presented immediately after delivery with pain around the ear and the feeling of plugged ear. A few hours later she reported swelling of the neck, chest tightness and shortness of breath. On examination, the crepitus on the neck and thorax was obvious, but there was no typical Hamman’s murmur.
Hamman’s syndrome is usually a benign and non-recurrent condition, however, in rare cases it may be life threatening and lead to cardiac tamponade with significant hemodynamic compromise. Such situation require surgical intervention [16]. Prior to any intervention, it is important to exclude other serious, potentially life-threathening conditions such as esophageal rupture (cancer related), Boerhaave syndrome (rupture of the esophagus due to forceful vomiting), pharyngeal rupture, pulmonary embolism, amniotic fluid embolism, aortic dissection, myocardial infarction, pneumopericardium, or pneumothorax of any cause [17,18].
Apart from the clinical picture, a CT scan is the gold standard in diagnosing pneumomediastinum. In a systematic review, it was found that about 30% of cases of pneumomediastinum were poorly detected by chest x-ray, but were easily detected on a CT-scan [19]. The CT also provides more accurate information on the extension of subcutaneous emphysema and other thoracic pathologies. An additional tool that can be considered is diagnostic endoscopy (bronchoscopy or esophagoscopy) or esophagography [20].
Initial management is supportive treatment with oxygen, sedatives and analgetics, as needed. In severe cases, the treatment with antibiotics and bronchodilators, along with oxygen support may added. The patient should be reassured about good prognosis and expected spontaneous resolution within (3-14 days) [21]. Patients can be discharged if they are in good general condition and do not have a significant pneumothorax. There is no recommended rutine follow up.
Conclusion
Post partum pneumomediastinum (Hammans syndrome) is a rare complication however its timely diagnosis is necessary for patient safety and management. The most cases in pregnant women occur in the second stage of labour, as a result of excessive straining and valsalva maneuver. The recurrence rate in subsequent pregnancies is low, and there are no established guidelines on the management. It is suggested that measures which can be implemented are to minimise barotrauma with the low threshold for instrumental or operative delivery, and approaches limiting the duration of the second stage of labour. However his is not evidence based and may require meta-analytical approach.
Author Contributions
KOB: original draft preparation, clinical management; MMK: retrieving clinical data, database search, clinical management; KK: methodology, conceptualization; LJR: clinical management, original draft preparation; JV: writing, review and editing; PZ: writing and original draft preparation, clinical management, conceptualization, review and editing, supervision. All authors heave read and agreed to the published version of the manuscript.
Funding
The manuscript received no funding.
Conflict of interest statement
The authors declare that there is no conflict o finterests regarding the publication of this paper.
Acknowledgements
Authors thank to Mrs. Petra Zuborova, PhD for technical help with managing this paper and to the pasient who approved the content of the paper and signed the consent for the publishing of this case.
Informed consent statement
Written informed consent was obtain from the patient. Under the all management steps and in case presentation the principles of the Helsinki Declaration were followed.
Institutional review board statement
The presented study was carried out following the rules of the Declaration of Helsinky of 1975, revised in 2013. According to local IRB principles, ethical approval from IRB for a single case is not required, as long as data are kept anonymous and subject signed informed consend with the publishing.
Data availability statement
Data sharing nor applicable to this article as no datasets were generated or analyzed during the current study. The data presented in this study are available on request.
References
- Kuruba, N.; Hla, T.T. Postpartum spontaneous pneumomediastinum and subcutaneous emphysema: Hamman's syndrome. Obstet Med. 2011, 4, 127–128. [Google Scholar] [CrossRef] [PubMed]
- Hamman, L. Spontaneous mediastinal emphysema. Bull of Johns Hopkins Hospital 1939, 64, 1–21. [Google Scholar]
- Hamman, L. Mediastinal emphysema. J. Am. Med. Assoc. 1945, 128, 1–6. [Google Scholar] [CrossRef]
- Khurram, D.; Patel, B.; Farra, M.W. Hamman's Syndrome: A Rare Cause of Chest Pain in a Postpartum Patient. Case Rep Pulmonol. 2015, 2015, 201051. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.G. Hamman's Crunch: An historical note. Bull N Y Acad Med. 1971, 47, 1111–1112. [Google Scholar] [PubMed]
- Gomes, S.; Mogne, T.; Carvalho, A.; Pereira, B.; Ramos, A. Post-partum Hamman's Syndrome. Cureus. 2022, 14, e33144. [Google Scholar] [CrossRef] [PubMed]
- Cho, C.; Parratt, J.R.; Smith, S.; Patel, R. Spontaneous pneumomediastinum (Hamman's syndrome): a rare cause of postpartum chest pain. BMJ Case Rep. 2015, 2015, bcr1220103603. [Google Scholar] [CrossRef] [PubMed]
- Kouritas, V.K.; Papagiannopoulos, K.; Lazaridis, G.; Baka, S.; Mpoukovinas, I.; Karavasilis, V.; Lampaki, S.; Kioumis, I.; Pitsiou, G.; Papaiwannou, A.; Karavergou, A.; Kipourou, M.; Lada, M.; Organtzis, J.; Katsikogiannis, N.; Tsakiridis, K.; Zarogoulidis, K.; Zarogoulidis, P. Pneumomediastinum. J Thorac Dis. 2015, 7 (Suppl 1), S44–S49. [Google Scholar] [PubMed]
- Yamashita, K.; Hongo, T.; Nojima, T.; Yumoto, T.; Nakao, A.; Naito, H. Hamman`s Syndrome Accompanied by Diabetic Ketoacidosis; a Case Report. Arch Acad Emerg Med. 2022, 10, e68. [Google Scholar]
- Kamei, S.; Kaneto, H.; Tanabe, A.; Shigemoto, R.; Irie, S.; Hirata, Y.; Takai, M.; Kohara, K.; Shimoda, M.; Mune, T.; Kaku, K. Hamman`s syndrome triggered by the onset of type 1 diabetes mellitus accompanied by diabetic ketoacidosis. Acta Diabetol. 2016, 53, 1067–1068. [Google Scholar] [CrossRef]
- Kelly, S.; Hughes, S.; Nixon, S.; Paterson-Brown, S. Spontaneous pneumomediastinum (Hamman`s syndrome). Surgeon. 2010, 8, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Früh, J.; Abbas, J.; Cheufou, D.; Baron, S.; Held, M. Spontaneous pneumomediastinum (Hamman's syndrome) with pneumorrhachis as a rare cause of acute chest pain in a young patient with acute asthma exacerbation. Pneumologie. 2023, 77, 430–434. [Google Scholar] [PubMed]
- Rosinhas, J.F.A.M.; Soares, S.M.C.B.; Pereira, A.B.M. Hamman`s syndrome. J Bras Pneumol. 2018, 44, 433. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, G.M.; Franklin, V. Hamman and Boerhaave syndromes - diagnostic dilemmas in a patient presenting with hyperemesis gravidarum: a case report. Scott Med J. 2014, 59, e12–e16. [Google Scholar] [CrossRef] [PubMed]
- Jayran-Nejad, Y. Subcutaneous emphysema in labour. Anaesthesia. 1993, 48, 139–140. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, P.N.V.P.; Stefanini, F.S.; Bitencourt, A.G.V.; Gross, J.L.; Chojniak, R. Computed tomography-guided percutaneous drainage of tension pneumomediastinum. Radiol Bras. 2022, 55, 62–63. [Google Scholar] [CrossRef] [PubMed]
- La Verde, M.; Palmisano, A.; Iavarone, I.; Ronsini, C.; Labriola, D.; Cianci, S.; Schettino, F.; Reginelli, A.; Riemma, G.; De Franciscis, P. A Rare Complication during Vaginal Delivery, Hamman's Syndrome: A Case Report and Systematic Review of Case Reports. Int J Environ Res Public Health. 2022, 19, 4618. [Google Scholar] [CrossRef]
- Tixier, H.; Rattin, C.; Dunand, A.; Peaupardin, Y.; Douvier, S.; Sagot, P.; Mourtialon, P. Hamman's syndrome associated with pharyngeal rupture occurring during childbirth. Acta Obstet Gynecol Scand. 2010, 89, 407–408. [Google Scholar] [CrossRef] [PubMed]
- Kaneki, T.; Kubo, K.; Kawashima, A.; Koizumi, T.; Sekiguchi, M.; Sone, S. Spontaneous pneumomediastinum in 33 patients: yield of chest computed tomography for the diagnosis of the mild type. Respiration. 2000, 67, 408–411. [Google Scholar] [CrossRef]
- Jougon, J.B.; Ballester, M.; Delcambre, F.; Mac Bride, T.; Dromer, C.E.; Velly, J.F. Assessment of spontaneous pneumomediastinum: experience with 12 patients. Ann Thorac Surg. 2003, 75, 1711–1714. [Google Scholar] [CrossRef]
- Brandfass, R.T.; Martinez, D.M. Mediastinal and subcutaneous emphysema in labor. South Med J. 1976, 69, 1554–1555. [Google Scholar] [CrossRef] [PubMed]
- Balkan, M.E.; Alver, G. Spontaneous pneumomediastinum in 3rd trimester of pregnancy. Ann Thorac Cardiovasc Surg. 2006, 12, 362–364. [Google Scholar]
- Sutherland, F.W.; Ho, S.Y.; Campanella, C. Pneumomediastinum during spontaneous vaginal delivery. Ann Thorac Surg. 2002, 73, 314–315. [Google Scholar] [CrossRef]
- Miguil, M.; Chekairi, A. Pneumomediastinum and pneumothorax associated with labour. Int J Obstet Anesth. 2004, 13, 117–119. [Google Scholar] [CrossRef] [PubMed]
- Duffy, B.L. Post partum pneumomediastinum. Anaesth Intensive Care. 2004, 32, 117–119. [Google Scholar] [CrossRef]
- Bonin, M.M. Hamman's syndrome (spontaneous pneumomediastinum) in a parturient: a case report. J Obstet Gynaecol Can. 2006, 28, 128–131. [Google Scholar] [CrossRef]
- Norzilawati, M.N.; Shuhaila, A.; Zainul Rashid, M.R. Postpartum pneumomediastinum. Singapore Med J. 2007, 48, e174–e176. [Google Scholar] [PubMed]
- Yadav, Y.; Ramesh, L.; Davies, J.A.; Nawaz, H.; Wheeler, R. Gross spontaneous pneumomediastinum (Hamman's syndrome) in a labouring patient. J Obstet Gynaecol. 2008, 28, 651–652. [Google Scholar] [CrossRef]
- Mahboob, A.; Eckford, S.D. Hamman's syndrome: an atypical cause of postpartum chest pain. J Obstet Gynaecol. 2008, 28, 652–653. [Google Scholar] [CrossRef] [PubMed]
- Zapardiel, I.; Delafuente-Valero, J.; Diaz-Miguel, V.; Godoy-Tundidor, V.; Bajo-Arenas, J.M. Pneumomediastinum during the fourth stage of labor. Gynecol Obstet Invest. 2009, 67, 70–72. [Google Scholar] [CrossRef]
- Revicky, V.; Simpson, P.; Fraser, D. Postpartum pneumomediastinum: an uncommon cause for chest pain. Obstet Gynecol Int. 2010, 2010, 956142. [Google Scholar] [CrossRef] [PubMed]
- Beynon, F.; Mearns, S. Spontaneous pneumomediastinum following normal labour. BMJ Case Rep. 2011, 2011, bcr0720114556. [Google Scholar] [CrossRef] [PubMed]
- Wozniak, D.R.; Blackburn, A. Postpartum pneumomediastinum manifested by surgical emphysema. Should we always worry about underlying oesophageal rupture? BMJ Case Rep. 2011, 2011, bcr0420114137. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, A.; Acharya, S. Subcutaneous emphysema in pregnancy. JNMA J Nepal Med Assoc. 2011, 51, 141–143. [Google Scholar] [CrossRef] [PubMed]
- McGregor, A.; Ogwu, C.; Uppal, T.; Wong, M.G. Spontaneous subcutaneous emphysema and pneumomediastinum during second stage of labour. BMJ Case Rep. 2011, 2011, bcr0420114067. [Google Scholar] [CrossRef] [PubMed]
- Houari, N.; Labib, S.; Berdai, M.A.; Harandou, M. Postpartum pneumomediastinum associated with subcutaneous emphysema: a case report. Ann Fr Anesth Reanim. 2012, 31, 728–730. [Google Scholar] [CrossRef] [PubMed]
- Kandiah, S.; Iswariah, H.; Elgey, S. Postpartum pneumomediastinum and subcutaneous emphysema: two case reports. Case Rep Obstet Gynecol. 2013, 2013, 735154. [Google Scholar] [CrossRef] [PubMed]
- Kouki, S.; Fares, A.A. Postpartum spontaneous pneumomediastinum 'Hamman's syndrome'. BMJ Case Rep. 2013, 2013, bcr2013010354. [Google Scholar] [CrossRef] [PubMed]
- Khoo, J.; Mahanta, V.R. Spontaneous pneumomediastinum with severe subcutaneous emphysema secondary to prolonged labor during normal vaginal delivery. Radiol Case Rep. 2015, 7, 713. [Google Scholar] [CrossRef]
- Wijesuriya, J.; Van Hoogstraten, R. Postpartum Hamman's syndrome presenting with facial asymmetry. BMJ Case Rep. 2015, 2015, bcr2015213397. [Google Scholar] [CrossRef]
- Scala, R.; Madioni, C.; Manta, C.; Maggiorelli, C.; Maccari, U.; Ciarleglio, G. Spontaneous pneumomediastinum in pregnancy: A case report. Rev Port Pneumol (2006). 2016, 22, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Elshirif, A.; Tyagi-Bhatia, J. Postpartum pneumomediastinum and subcutaneous emphysema (Hamman's syndrome). J Obstet Gynaecol. 2016, 36, 281–282. [Google Scholar] [CrossRef] [PubMed]
- Berdai, M.A.; Benlamkadem, S.; Labib, S.; Harandou, M. Spontaneous Pneumomediastinum in Labor. Case Rep Obstet Gynecol. 2017, 2017, 6235076. [Google Scholar] [CrossRef] [PubMed]
- Lou, Y.Y. Hamman's syndrome: spontaneous pneumomediastinum and subcutaneous emphysema during second stage of labour. Int J Reprod Contracept Obstet Gynecol. 2017, 6, 2622–2624. [Google Scholar] [CrossRef]
- Sagar, D.; Rogers, T.K.; Adeni, A. Postpartum pneumomediastinum and subcutaneous emphysema. BMJ Case Rep. 2018, 2018, bcr2018224800. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.I.; Shah, R.A.; Yasir, S.; Ahmed, M.S. Post partumpneumomediastinum (Hamman syndrome): A case report. J Pak Med Assoc. 2018, 68, 1108–1109. [Google Scholar]
- Jakes, A.D.; Kunde, K.; Banerjee, A. Case report: Postpartum pneumomediastinum and subcutaneous emphysema. Obstet Med. 2019, 12, 143–145. [Google Scholar] [CrossRef] [PubMed]
- Madhok, D.; Smith, V.; Gunderson, E. An Unexpected Case of Intrapartum Pneumomediastinum. Case Rep Obstet Gynecol. 2019, 2019, 4093768. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Young, A. Hamman syndrome: spontaneous postpartum pneumomediastinum. Intern Med J. 2019, 49, 130–131. [Google Scholar] [CrossRef]
- Chavan, R. Hamman’s syndrome in a parturient: a case report. BJMP 2019, 12, a007. [Google Scholar]
- Opstelten, J.L.; Zwinkels, J.R.; van Velzen, E. Sudden dyspnoea and facial swelling during labour. Ned Tijdschr Geneeskd. 2019, 163, D3044. [Google Scholar]
- Oshovskyy, V.; Poliakova, Y. A rare case of spontaneous pneumothorax, pneumomediastinum and subcutaneous emphysema in the II stage of labour. Int J Surg Case Rep. 2020, 70, 130–132. [Google Scholar] [CrossRef] [PubMed]
- Badran, D.; Ismail, S.; Ashcroft, J. Pneumomediastinum following spontaneous vaginal delivery: report of a rare phenomenon. J Surg Case Rep. 2020, 2020, rjaa076. [Google Scholar] [CrossRef] [PubMed]
- Zethner-Møller, R.; Wulff, C.B. Spontaneous pneumomediastinum during labour. Ugeskr Laeger. 2021, 183, V05210403. [Google Scholar] [PubMed]
- Mullins, K.V.J.; Mlawa, G. Postpartum chest pain and the Hamman syndrome. J Clin Images Med Case Rep. 2021, 2, 1522. [Google Scholar] [CrossRef]
- Peña-Vega, C.J.; Buitrón-García, R.; Zavala-Barrios, B.; Aguirre-García, R. Postpartum Hamman (pneumomediastinal) syndrome. Synthesis of the literature and case report. Ginecol Obstet Mex. 2023, 91, 197–209. [Google Scholar]
- Chooi, K.Y.L. Hamman’s syndrome: a case of pneumomediastinum, pneumothorax and extensive subcutaneous emphysema in the second stage of labour. The Royal Australian and New Zealand College of Obstetricians and Gynaecologists Congress. Perth, 28.10.-1.11.2023. Aiming higher: More than healthcare. Poster. https://ranzcogasm.com.au/wp-content/uploads/2019/10/80.pdf.
- Hülsemann, P.; Vollmann, D.; Kulenkampff, D. Spontaneous Pneumomediastinum-Hamman Syndrome. Dtsch Arztebl Int. 2023, 120, 525. [Google Scholar] [CrossRef]
- Inesse, A.A.; Ilaria, R.; Camille, O. Protracted Labor Complicated by Pneumomediastinum and Subcutaneous Emphysema: A Rare Case Report and Management Considerations. Am J Case Rep. 2023, 24, e940989. [Google Scholar] [CrossRef]
- Chen, N.; Daly, T.K.; Nadaraja, R. Pneumomediastinum and Pericardium During Labour: A Report on a Rare.
Figure 1.
Plain radiograph scan showing typical gas accumulations seen subcutaneous and with pneumomediastinum (arrows, part A): There is significant subcutaneous emphysema, more pronounced on the right side (arrow, part A). We can see an outlining of the pericardium both in lateral projection (arrow, part B) and with «continuous diaphragm sign» on frontal projection (arrow, part A). You can also see continuous lucencies along upper mediastinum to the neck, through upper thoracic aperture.
Figure 1.
Plain radiograph scan showing typical gas accumulations seen subcutaneous and with pneumomediastinum (arrows, part A): There is significant subcutaneous emphysema, more pronounced on the right side (arrow, part A). We can see an outlining of the pericardium both in lateral projection (arrow, part B) and with «continuous diaphragm sign» on frontal projection (arrow, part A). You can also see continuous lucencies along upper mediastinum to the neck, through upper thoracic aperture.
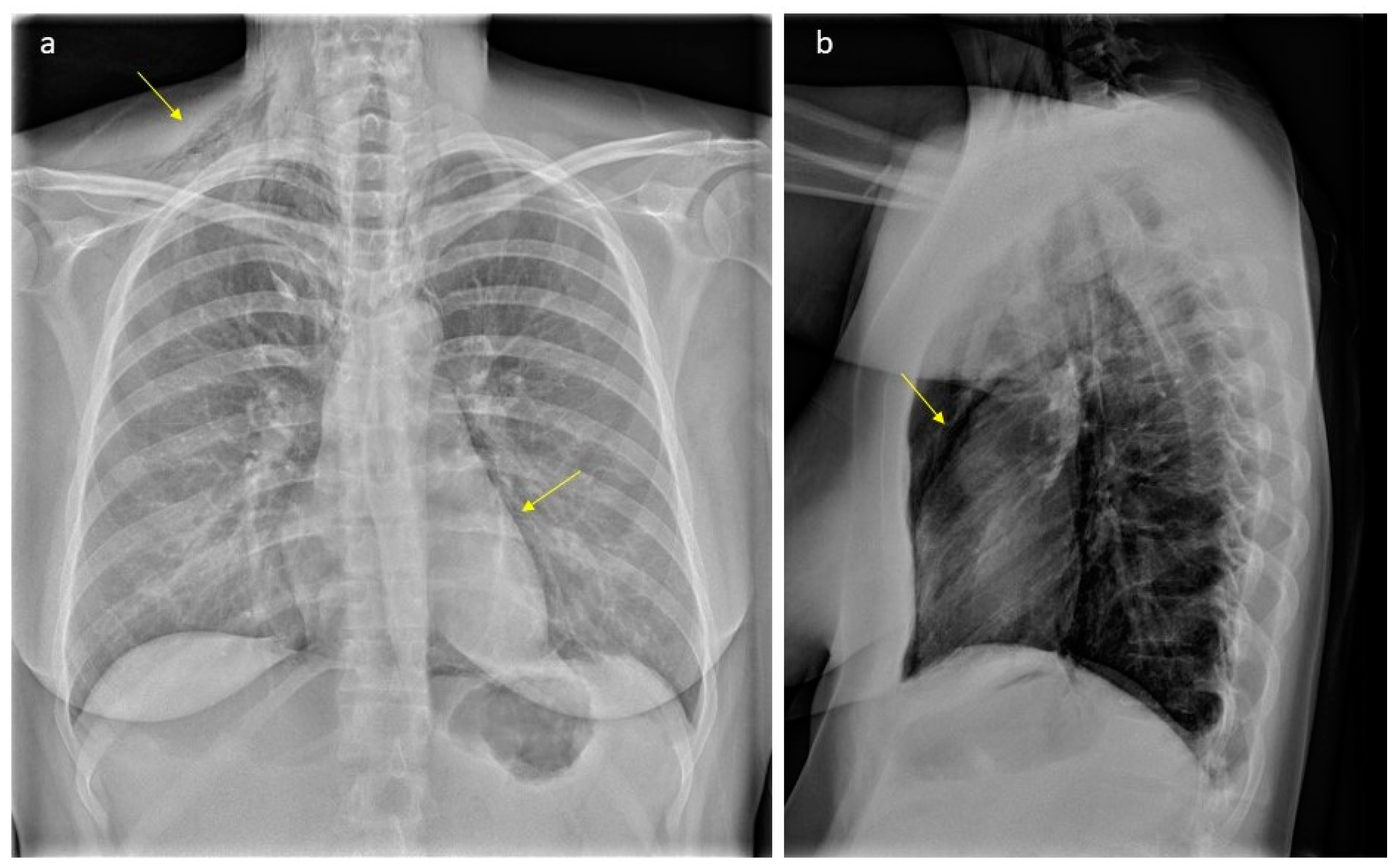
Figure 2.
Low dose CT scan showing air within the mediastinum starting caudally in the level of hiatus aorticus, surrounding the pericardium, throughout the mediastinum. In the neck level, air was seen subcutaneously (part A), along the great vessels (carotid space) and in the retropharyngeal space (part B). The patient has an «azygos lobe», a normal variant with the vena azygos running laterally with a pleural fissure surrounding it (arrow, part A). Air bubbles can be seen along the vein and small amounts of air within the pleural cavity apically on the right side. Apart from this, no signs of pneumothorax. Small amounts of pleural effusion is seen bilaterally. The upper abdomen was included in the low-dose scan, without any signs of air below the diaphragm.
Figure 2.
Low dose CT scan showing air within the mediastinum starting caudally in the level of hiatus aorticus, surrounding the pericardium, throughout the mediastinum. In the neck level, air was seen subcutaneously (part A), along the great vessels (carotid space) and in the retropharyngeal space (part B). The patient has an «azygos lobe», a normal variant with the vena azygos running laterally with a pleural fissure surrounding it (arrow, part A). Air bubbles can be seen along the vein and small amounts of air within the pleural cavity apically on the right side. Apart from this, no signs of pneumothorax. Small amounts of pleural effusion is seen bilaterally. The upper abdomen was included in the low-dose scan, without any signs of air below the diaphragm.
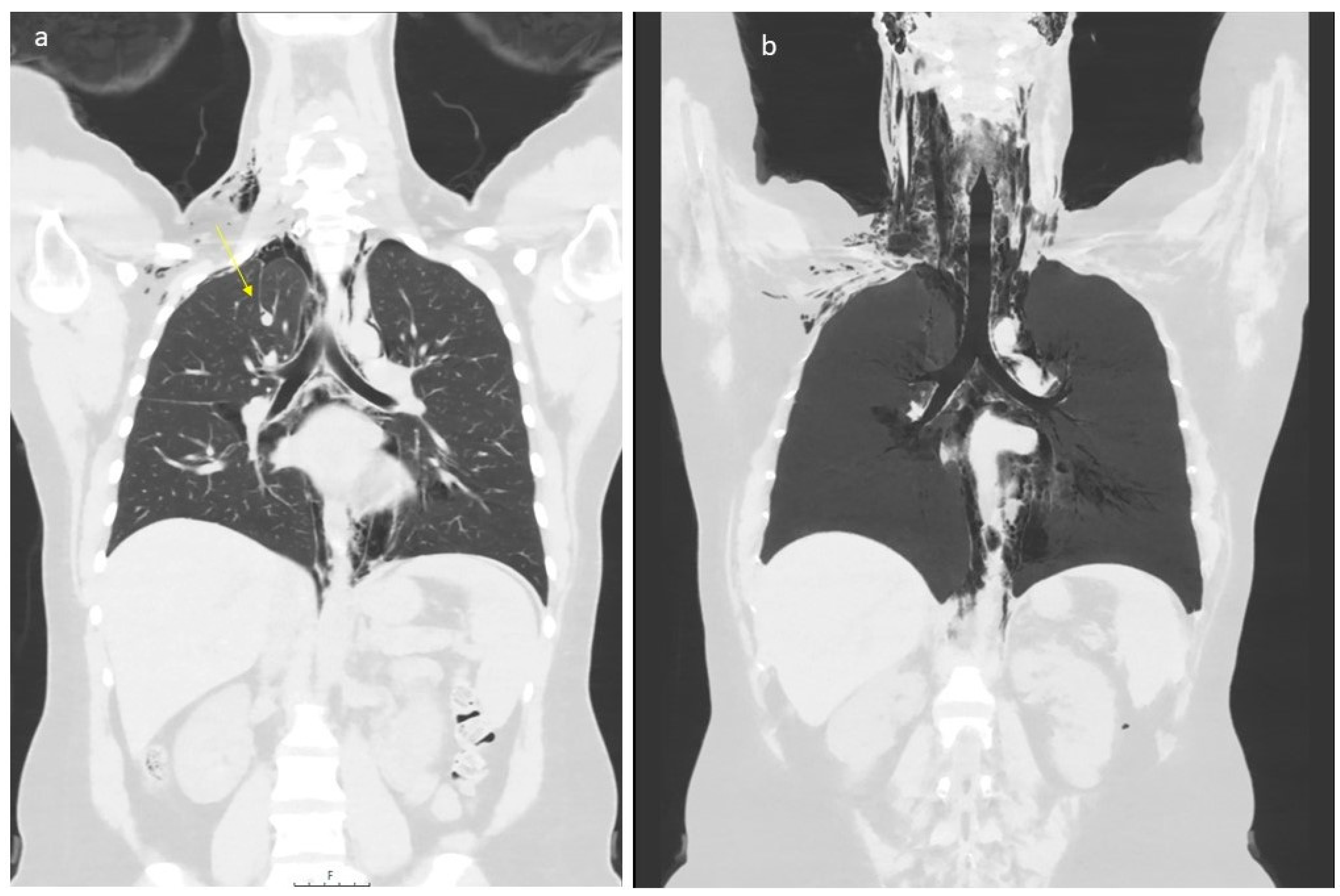

Table 1.
An overview on 42 previously published cases of pregnancy associated Hamman`s syndrome (database Pubmed.gov from from 2000 to 3/2024). Abbreviations: N/A - not available; IV – intravenous; h - hours.
Table 1.
An overview on 42 previously published cases of pregnancy associated Hamman`s syndrome (database Pubmed.gov from from 2000 to 3/2024). Abbreviations: N/A - not available; IV – intravenous; h - hours.
| Author | Age y/o |
Parity | When symptoms developed | Duration of labour | Week of gestation | Treatment |
|---|---|---|---|---|---|---|
| Sutherland et al. 2002 [23] | 32 | Para 1 | Post partum | 8h | N/A | None |
| Sutherland et al. 2002 [23] | 22 | Para 1 | 13h post partum | N/A | N/A | None |
| Miguil et al. 2004 [24] | 19 | Para 0 | N/A | N/A | 40 | Oxygen & analgetics, C-section |
| Duffy 2004 [25] | 19 | Para 0 | 2h | 90 min 2nd stage | 40 | Oxygen v analgetics |
| Bonin et al. 2006 [26] | 27 | Para 0 | 2nd stage | 6h | 38 | Lorazepam for anxiety & anxiolytics for dyspnea |
| Norzilawati et al. 2007 [27] | 21 | Para 0 | 12h post partum | 4h, 100 min 2nd stage | 40 | None |
| Yadav et al. 2008 [28] | 21 | Para 0 | 2nd stage | 2nd stage 1,5h | N/A | Oxygen & analgesics |
| Mahboob et al. 2008 [29] | 24 | Para 0 | 18h post partum | N/A Normal |
39 | Oral antibiotics, iv fluids & analgetics |
| Zapardiel et al. 2009 [30] | 29 | Para 0 | Post partum | N/A | 39 | Oxygen |
| Revicky et al. 201031 | 32 | Para 0 | 3h | 14h | 40 | None |
| Beynon et al. 2011 [32] | 18 | Para 0 | 8h post partum | 4h | 39 | Antibiotics & analgetics |
| Wozniak et al. 2011 [33] | 20 | Para 0 | 5h post partum | 9h | 41 | Observation |
| Shrestha et al. 2011 [34] | 19 | Para 0 | N/A | N/A | 36 | None |
| Kuruba et al. 2011 [1] | 32 | Para 1 | 2nd stage | 1.5h | 40 | None |
| McGregor et al. 2011 [35] | 27 | Para 0 | 2nd stage | 7,5h | 40 | Oxygen & analgetics |
| Houari et al. 2012 [36] | 21 | Para 0 | Post partum | N/A | 40 | Conservative management |
| Kandiah et al. 2013 [37] | 25 | Para 0 | 2nd day post partum | 2nd stage 3h, 16 min. Ending in a C-section | 40 | Observation |
| Kandiah et al. 2013 [37] | 30 | Para 0 | 2nd stage | 6h | 38 | Observation |
| Kouki et al. 2013 [38] | 23 | Para 0 | 2nd stage | 9h | 40 | Oxygen & analgesics and sedatives |
| Khoo et al. 2015 [39] | 33 | Para 0 | 2nd stage | 12h | 40 | Analgetics & bed rest |
| Cho et al. 2015 [7] | 28 | Para 0 | 2nd stage | 5h | 36 | Oxygen & analgesics |
| Wijesuriya et al. 2015 [40] | 24 | Para 0 | N/A | N/A | N/A | N/A |
| Khurram et al. 2015 [4] | 24 | Para 1 | 2h post partum | 2nd stage prolonged | 40 | None |
| Scala et al. 2016 [41] | 30 | N/A | 2nd stage | N/A | 40 | None |
| Elshirif et al. 2016 [42] | 27 | Para 0 | 4h post partum | 19h 2nd stage 3h |
41 | Analgetics, oxygen & antibiotics |
| Berdai et al. 2017 [43] | 22 | Para 0 | 2nd stage | 2h | 40 | Oxygen |
| Lou et al. 2017 [44] | 29 | Para 0 | 2nd stage | Prolonged | At term | Supportive |
| Sagar et. al 2018 [45] | 22 | Para 0 | 3h post partum | 4,5h | 37 | None |
| Khan et al. 2018 [46] | 30 | Para 0 | N/A | N/A | N/A | Antibiotics, oxygen & bronchodilators |
| Jakes et al. 201947 | 23 | Para 0 | 40 min post partum | 2nd stage 2h | 38 | Oxygen |
| Madhok et al. 2019 [48] | 21 | Para 0 | 2h post partum | 3h | 39 | None |
| Lee et al. 2019 [49] | 31 | Para 0 | 2nd stage | 8,4h | 41 | IV antibiotics, hydrokortison & Loratadine |
| Chavan et al. 2019 [50] | 33 | Para 0 | 10h post partum | 90 min 2nd stage | 38 | Oxygen & analgetics |
| Opstelten et al. 2019 [51] | 25 | Para 0 | 2nd stage | N/A | N/A | N/A |
| Oshovskyy et al. 2020 [52] | 34 | Para 4 | 2nd stage | 4,5h | 39 | Pigtail catheter |
| Badran et al. 2020 [53] | N/A | Para 0 | 4h post partum | N/A | Full term | Nil by mouth |
| Zethner-Møller et al. 2021 [54] | 35 | Para 1 | 2nd stage | N/A | 36 | Oxygen |
| Mullins et al. 2021 [55] | 17 | Para 0 | post partum, prolonged second stage | N/A | 39 | Oxygen & opioids |
| La Verde et al. 2022 [17] | 23 | Para 0 | 2nd stage | 5h | 41 | None |
| Gomes et al. 202 [26] | 21 | Para 0 | 2nd stage | N/A | 40 | C-section & observation |
| Peña-Vega 2023 [56] | 18 | Para 0 | 30h post partum | 12h | 39 | Oxygen |
| Chooi et al. 2023 [57] | 22 | Para 0 | 2nd stage | 3h 2nd stage | 39 | None |
| Hülsemann et al. 2023 [58] | 21 | Para 0 | 2nd stage | Prolonged | N/A | N/A |
| Inesse et al. 2023 [59] | 29 | Para 0 | 1h post partum | 2nd stage lasted 2h, 40 min active pushing | 40 | None |
| Chen et al. 2023 [60] | 20 | Para 0 | immediately after delivery | Prolonged | 43 | Analgetics & antibiotics iv |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



