
Submitted:
19 April 2024
Posted:
22 April 2024
You are already at the latest version
Abstract
Bladder cancer (BC) possesses distinct molecular profiles that influence progression depending on its biological nature and delivered treatment intensity. Muscle-invasive BC (MIBC) and non-MIBC (NMIBC) demonstrate great intrinsic heterogeneity regarding different prognoses, survival, progression, and treatment outcomes. Transurethral resection of bladder tumor (TURBT) is the standard of care in treating NMIBC and serves both diagnostic and therapeutic purposes, despite the prevalent recurrence and progression among many patients. In particular, flat urothelial car-cinoma in situ and urothelial carcinoma with lamina propria invasion are the major precursors of MIBC. A new‐generation photosensitizer, 5‐Aminolevulinic acid (5-ALA), demonstrates high tumor specificity by illuminating the tumor lesion with a specific wavelength of light to produce fluorescence, and has been studied for photodynamic diagnosis to detect precise tumor areas by TURBT. Additionally, it has been applied for treatment by producing its cytotoxic reactive oxygen species, as well as screening for urological carcinomas by excreting porphyrin in the blood and urine. Moreover, 5-ALA may contribute to screening before and after TURBT in NMIBC. Here, we summarize the updated evidence and ongoing research on photodynamic technology for NMIBC, providing insight into the potential for improving patient outcomes.
Keywords:
non-muscle invasive bladder cancer
; transurethral resection of bladder tumor
; 5‐Aminolevulinic acid
; photodynamic diagnosis
; photodynamic therapy
1. Introduction
Bladder cancer (BC) is one of the prevalent tumors that cause health issues globally [1,2]. Cigarette smoking is the most prominent risk factor for developing BC in most countries [3,4]. Overall, BC, with urothelial carcinoma (UC) as the prevalent histology, is comprised of two distinct molecular subtypes based on each molecular heterogeneity and clinical staging: muscle-invasive BC (MIBC), including stages T2 (muscularis propria invasion), T3 (perivesical fat invasion), and T4 (adjacent organ involvement), and non-MIBS (NMIBC), including stages Tis (flat urothelial carcinoma in situ [CIS]), Ta (NMIBC occurs as papillary lesion), and T1 (NMIBC with lamina propria invasion), consisting of 80% BC. NMIBC region of clonally related bladder tumors is frequently treatable [5]. The 5-year survival rate for NMIBC demonstrated no marked changes despite advancements in research and care, and the frequent NMIBC recurrence has burdened public health systems [6,7,8].
Understanding molecular principles of NMIBC tumorigenesis is crucial in developing more effective preventive measures. The sequencing and gene expression studies have guided the discovery of numerous genetic alterations and revealed several distinct molecular signatures and subtypes, thereby providing a more accurate prediction of disease progression in BC.
Transurethral resection of bladder tumor (TURBT) demonstrates both diagnostic and therapeutic functions in effective NMIBC management. TURBT, followed by intravesical Bacillus Calmette–Guérin (BCG) administration, is the standard of care in flat-lesion CIS, despite prevalent recurrence and progression among many patients. The use of photodynamic technology for future management of challenging cases enables the safe and effective performance of TURBT. CIS is usually difficult to detect and differentiate from inflammatory lesions under the cystoscopic examination [9]. Advanced cystoscopy technologies, such as narrow-band imaging, photodynamic diagnosis, and image 1S, are required to improve BC detection. Novel techniques significantly improve the precision of transurethral surgery and lower the risk of complications.
This review aims to summarize the current evidence and recent developments in the molecular and translational aspects of BC biology and discuss their current or potential future clinical applications in managing NMIBC.
2. Common Genetic Alterations in NMIBC
Deletions of chromosome 9, frequently found in NMIBC, include the CDKN2A locus (9p21) that encodes p16 and p14ARF, which are RB and p53 pathway regulators, respectively. Loss of TSC1 (9q34), which is an mTOR signaling regulator, associated with upregulated expression of mTOR targets [10], such as telomerase reverse transcriptase (TERT) activity, has been observed in NMIBC. Overexpressed TERT upregulates oncogenic signaling pathways [11], which are crucial in maintaining tumor immortality and contribute to tumor progression in BC, to maintain telomere integrity [12,13,14,15]. The promoter mutations of TERT are chief genetic alterations occurring with a frequency of 70%–80% in patients with BC [16,17,18,19]. Other copy number alterations in NMIBC (8%–22%), particularly in stage T1 tumors, include gains of 1q, 5p, 18q, 20p, and 20q and losses of 8p, 11p, 17p, and 18q [20], which are more commonly detected in MIBC [21].
FGFR3 point mutations (S249C) were predicted to result from Apolipoprotein B mRNA Editing Catalytic Polypeptide-like(APOBEC) activity [22] as an early event is the most prevalent genetic alteration associated with NMIBC low tumor grade and stage [10,23,24,25,26]. APOBEC targets PIK3CA mutations that are present in <30% of NMIBC [27]. RAS or FGFR3 mutation, found in Ta urothelial carcinoma (UC), are mutually exclusive and associated with low tumor grade and stage [10,27]. These data indicate that both PI3K and RAS–MAPK signaling pathways are usually activated in NMBC. ERBB2 and ERBB3 mutations that provide PI3K activation [28] are detected in <15% of T1 tumors. Micropapillary and plasmacytoid UCs are biologically aggressive subtypes [5]; Micropapillary, UC has a disproportionately higher rate of ERBB2 amplification than conventional UC [29,30,31], and plasmacytoid UC is defined by distinct CDH1 mutations [32]. Inactivating mutations and loss of expression are observed in <30% of low-grade Ta, but in fewer in T1 tumors, and often with FGFR3, PIK3CA, and/or KDM6A (chromatin regulator) mutations [27,33,34]. The exact roles of FGFR3 mutations in NMIBC tumorigenesis remain unknown, but mutant FGFR3 induces overgrowth of the cultured normal human urothelial cells at a confluence, indicating a potential contribution to urothelial hyperplasia in vivo [35].
Moreover, BC demonstrates significant epigenetic dysregulation such as changes in DNA methylation [36]. Identifying frequent mutations and epigenetic modifications may benefit novel therapeutic approaches, as well as urine and blood surveillance for both early detection and disease monitoring after treatments.
3. Tumorigenesis Associated with NMIBC
Relative to treating NMIBC, Ta tumors above all have demonstrated good-prognosis compared to T1 and Tis tumors, and their treatment plan is markedly different [1]. The use of tissue to predict progression from T1to MIBC has been a subject of interest for some time. The American Joint Committee on Cancer (AJCC) indicated that T1 UCs showed that tumor in the lamina propria related to a higher rate of the progress based on a large number of studies [37]. Leivo et al. adopted a cutoff of ≥2.3 mm as the best predictor of muscle-invasive disease progression, acknowledging that additional nonhistopathologic methods may be required to increase broad applicability and further reduce the false-positive threshold [38]. Additional molecular biological approaches (e.g., molecular and/or protein biomarkers) to predicting MIBC progression have been assessed in numerous studies [39,40]. These studies indicated that improved sequencing techniques have contributed to the understanding of BC as a heterogeneous disease and enabled the development of several biomarkers with the potential to help predict treatment response and appropriate patient selection.
T1 tumors frequently share molecular characteristics with MIBC, and these tumors usually differ substantially from low-grade Ta tumors [41,42,43]. High-grade UCs are either NMIBC or MIBC, of which T1 UCs prevalently progress to MIBC, requiring more aggressive clinical treatment and follow-up. No obligate pathway exists from NMIBC to MIBC, and these tumor categories have largely non-overlapping pathogenesis pathways associated with different genetic features [44,45]. Histopathological and molecular data indicate the CIS as the major MIBC precursor, whereas most papillary NMIBC originate from normal-appearing urothelium. However, some patients with NMIBC, particularly those with tumors that invade the lamina propria, demonstrate progression from initially non-invasive to invasive disease. Figure 1 summarizes the correlation between pathological findings of NMIBC and the progress to MIBC.
4. Pathological Diagnosis and Screening of NMIBC
4.1. Urine-Based Diagnosis
A prospective observational study revealed that approximately 75% of patients with BC present with non-symptomatic macrohematuria, with increasing incidence alongside aging [46,47]. Diagnostic evaluation of patients with hematuria should involve a response to urine-based examination. Urine cytology has been credited as an easy, safe, and inexpensive test with high specificity for diagnosing UC [48]. The Paris System for Reporting Urinary Cytology published in 2016 is utilized as a standard classification system in urine cytology specimens [49]. The sensitivity of this analysis is not best, but its specificity is high, especially for high-grade UC; thus, urine cytology remains the well-established technique in BC diagnosis compared with marker-based studies, such as protein- and molecular-based urine tests [49,50,51,52,53,54,55].
4.2. Blood-Based Diagnosis
Circulating cell-free DNA is considered as one of the major breakthroughs in the field of innovative diagnosis, used as a liquid biopsy. Cell-free DNA with tumor-specific alterations is derived from dying (i.e., apoptotic) cells and released into the blood flow (Circulating tumor DNA: ctDNA) [56]. The half-life of ctDNA is ~2 h [57]. It is useful for real-time tracking of tumor burden postoperatively and during oncological treatment. Analysis of ctDNA revealed promising results for early risk stratification of patients, prediction of treatment response, and early detection of metastatic relapse in BC. [58].
4.3. Cystoscopic Diagnosis
Cystoscopy is considered the gold standard for diagnosing BC. White-light (WL) imaging cystoscopy is the conventional method to detect UC but may overlook small and flat lesions, such as CIS. If a lesion is seen on cystoscopy, this is followed by examination under anesthesia at the time of TURBT, although in spite of this thorough diagnostic and staging process, discrepancy between clinical and pathologic stage is a common finding [59]. Pathological examination of patients includes urinary cytology and biopsy analysis or TURBT samples of visible lesions.
4.4. Tissue-Based Diagnosis
Pathological analysis of tissue samples by bladder biopsy or TURBT during cystoscopy is the most prevalent and useful procedure in initially diagnosing the presence of cancer, histological type, and stage. BC is categorized by grade into low-grade and high-grade [5]. UC is the most predominant histological subtype of all BC, with the remainder of minor subtypes including squamous cell carcinoma, adenocarcinoma, and neuroendocrine carcinoma [5,60]. UC occurred as a broad array of variants or subtypes. The World Health Organization Classification of Tumors of the Urinary System and Male Genital Organs defined the several subtypes of UC categories, such as micropapillary, plasmacytoid, nested, and lymphoepithelioma-like carcinomas, which have been associated with unique molecular and/or therapeutic considerations [5,29,30,31,32,61,62]. The UROMOL study categorized NMIBC into classes 1 (luminal-like signature), 2 (luminal-like, epithelial–mesenchymal transition [EMT] and cancer stem cell signatures), and 3 (basal-like signature) [63]. Class 2 tumors are associated with poor prognosis compared with class 1 or 3 tumors [63]. Pathological diagnosis identifies the tumor staging based on the AJCC, currently in its eighth edition [37]. NMIBC occurs as either papillary (pTa) or flat urothelial CIS (pTis). Cancer patients with similar prognosis are grouped by using prognostic stage tables. Lamina propria invasion (pT1), muscularis propria invasion (pT2), perivesical fat (pT3), and adjacent organ involvement (pT4) are associated with a progressive reduction in survival [37].
5. Management of NMIBC
5.1. TURBT and En Bloc Resection
Determining pathological diagnosis and staging on TURBT samples is challenging due to the extent of sampling, interpretation artifact caused by cautery or crush degeneration, and lack of objective markers to conclusively determine the presence of muscularis propria. En block resection of Bladder tumor (ERBT) is removal technique of BC in one piece. Dyrskjøt et al. reviewed results from three randomized trial comparing ERBT and TURBT in ≤ 3cm BT as follows [64]. At first, Gellioli et al. reported that the rate of detrusor muscle presence for ERBT was noninferior to that for TURBT (94% vs 95%; n = 248), and T1 substaging was feasible in 80% of TURBT cases versus 100% of ERBT cases (p = 0.02) [65]. In the second trial, D’Andrea et al. reported that ERBT was superior to TURBT in retrieval of detrusor muscle (80.7% vs 71.1%; p = 0.01; n = 452) [66]. Finally, Teoh et al. reported ERBT reduced the 1-year recurrence rates and progression rate compared to TURBT (28.5 % vs 38.1%; p = 0.007 and 0% vs 2.6%; 0.065, respectively; n = 276) [67].
Furthermore, intravesical chemotherapy (CT), along with transurethral resection of the bladder, is quite effective in reducing disease recurrence [68,69].
Either way, increasing the detection rate of tumors may contribute the better prognosis in BC by these procedure.
6. Photodynamic Diagnosis, Photodynamic Therapy, and Photodynamic Screening with 5-Aminolaevulinic Acid
CIS is difficult to detect and differentiate from inflammation. The prognosis of the patients is improved if the expanse of the lesion in the BC, especially in T1 UC, and the flat lesion (CIS), which is the major precursor of MIBC, can be detected and resected exactly. Photodynamic diagnosis (PDD) is a technique that improves the detection of occult bladder tumors during cystoscopy. Photodynamic therapy (PDT) for BC involves either systemic infusion or bladder instillation of a photosensitizer, which undergoes a photochemical reaction when activated by visible light of an appropriate wavelength to produce reactive and singlet oxygen species in situ that are frequently lethal. The amino acid, 5-aminolaevulinic acid (5-ALA), is a new-generation photosensitizer with high tumor specificity.
Generally, 5-ALA is generated in plants and animals from glycine and succinyl CoA. The cytoplasmic 5-ALA precursor is transported to the mitochondria via the ATP-binding cassette (ABC) subfamily B member 6 to produce fluorescent endogenous porphyrins, including protoporphyrin IX (PpIX). Ferrochelatase catalyzes ferrous iron insertion into PpIX to form heme and bilirubin. Ferrochelatase contributes to PpIX catabolism in addition to heme production. However, ferrochelatase is inactive in various cancer types, including BC. Thus, PpIX accumulates more in tumor cells than in healthy cells due to decreased ferrochelatase activity [70,71,72]. The activation of the 5-ALA synthetic enzyme and 5-ALA influx transporter (peptide transporter 1) promotes PpIX production in tumor cells [3]. Additionally, ABC superfamily G member 2, which excretes PpIX, is inactivated in tumor cells, thereby downregulating PpIX excretion from cells [72,73,74].
PpIX possesses photoactivity and emits red fluorescent light of 600–700 nm when excited by light irradiation at a specific wavelength, mainly visible blue light (375–445 nm). Thus, cancer cells were accurately identified via PDD by detecting PpIX fluorescence using ALA. PpIX is excited at low excitation wavelengths in the red (600–740 nm) and green (450–580 nm) visible ranges. PpIX returns from the excited state to the ground state after absorbing the light, while releasing energy, which produces cytotoxic reactive oxygen species (ROS) in tumor cells. ROS damages mitochondria and induces apoptosis of tumor cells, causing cell death. This mechanism emphasizes the effects of PDT with ALA [72].
PpIX accumulates in the mitochondria in the cancer cells, as mentioned above. This excessive PpIX accumulation causes saturation of porphyrin precursors of PpIX (i.e., uroporphyrin and coproporphyrin) and promotes the excretion of these precursors of PpIX in blood and urine. Thus, their amounts in the urine and blood may be increased, particularly in patients with cancer. Photodynamic screening (PDS) aims to measure the amount of porphyrin excreted in urine after oral 5-ALA administration [75]. Figure 2 shows the mechanisms of ALA-PDD, ALA-PDT, and ALA-PDS.
The 5-ALA is administered via oral and transurethral routes. Japan was the first country to approve oral 5-ALA administration as diagnostic agents. The clinical treatment of NMIBC by the Pharmaceuticals and Medical Devices Agency approved ALAGRIO® which was covered by insurance in 2017. ALAGRIO® was approved for visualizing NMIBC during TURBT. The recommended dose of ALA is 20 mg/kg body weight, and ALA-PDD should be initiated approximately 3 h (range: 2–4 h) after oral ALA administration. ALAGRIO® was used in approximately 13,000 cases across approximately 370 institutions in the first 3 years after approval [72].
Transient adverse events for oral ALA include nausea, vomiting, photosensitivity, hypotension, and liver enzyme dysfunction. Our group revealed that among the 76 patients included, 7 (9.2%) experienced hypotension (systolic blood pressure (SBP) of <80 mmHg or mean arterial pressure of <60 mmHg), with a median onset time of 9 (range: 3–28) min after inducing anesthesia [76]. Severe hypotension that requires intensive care management after ALAGRIO® administration has been reported in Japan [77,78,79]. Our group revealed that the multiple factors in the prediction model for ALA (ALAGRIO®)-induced hypotension using the detection tree analysis include the following. First, general anesthesia, age of ≥74 years, and American Society of Anesthesiologists physical status of ≥2; second, SBG of ≤115 mmHg at the beginning of anesthesia under spinal anesthesia; and third, SBP of ≥115 mmHg at the beginning of spinal anesthesia and an estimated glomerular filtration rate of ≤42 ml/min/1.73 cm2 [79]. Liver dysfunction in response to ALAGRIO® was transient and gradually normalized despite no treatment [80].
Adding PDD and narrow-band imaging (NBI) to WL increases the cancer detection rate for flat lesions, which are difficult to detect with conventional WL [81,82,83,84]. A systematic review by Chen et al. indicated that NBI is a more sensitive diagnostic intervention for patients with NMIBC compared with either 5-ALA or hexylaminolevlinate (5-ALA derivative), based on diagnostic test accuracy assessment using WL cystoscopy as the reference standard [85]. However, Hagimoto et al. revealed that ALA-PDD was more sensitive than NBI for CIS lesions (94.6% vs. 54.1%) [86]. NBI improves the cancer detection rate, but its effects on reducing the recurrence rate of BC are unclear, except in patients at low risks (pTa, grade 1, <30 mm, and no CIS) [87]. The Clinical Practice Guidelines for Bladder Cancer in Japan (2019 revision) recommended PDD because it lowers the recurrence rate of BC more than NBI [88].
7. PDD with 5-ALA for TURBT in NMIBCs
ALA-PDD is an effective method for diagnosing NMIBC. Fluorescence light from 5-ALA and WL was previously reported to detect CIS lesions with sensitivities of 92.1% and 47.4%, respectively, and ALA-PDD was significantly more sensitive [76]. However, false-positive lesions increased due to the tangent effect in some distal bladder lesion locations, including the bladder neck, trigone, and prostatic urethra [89]. Thus, ALA-PDD demonstrated lower specificity compared with WL. However, the higher sensitivity of ALA-PDD compared with WL enables more tumor and CIS lesion detection [88]. ALA-PDD may detect more imperceptibly small tumors and CIS lesions compared with WL.
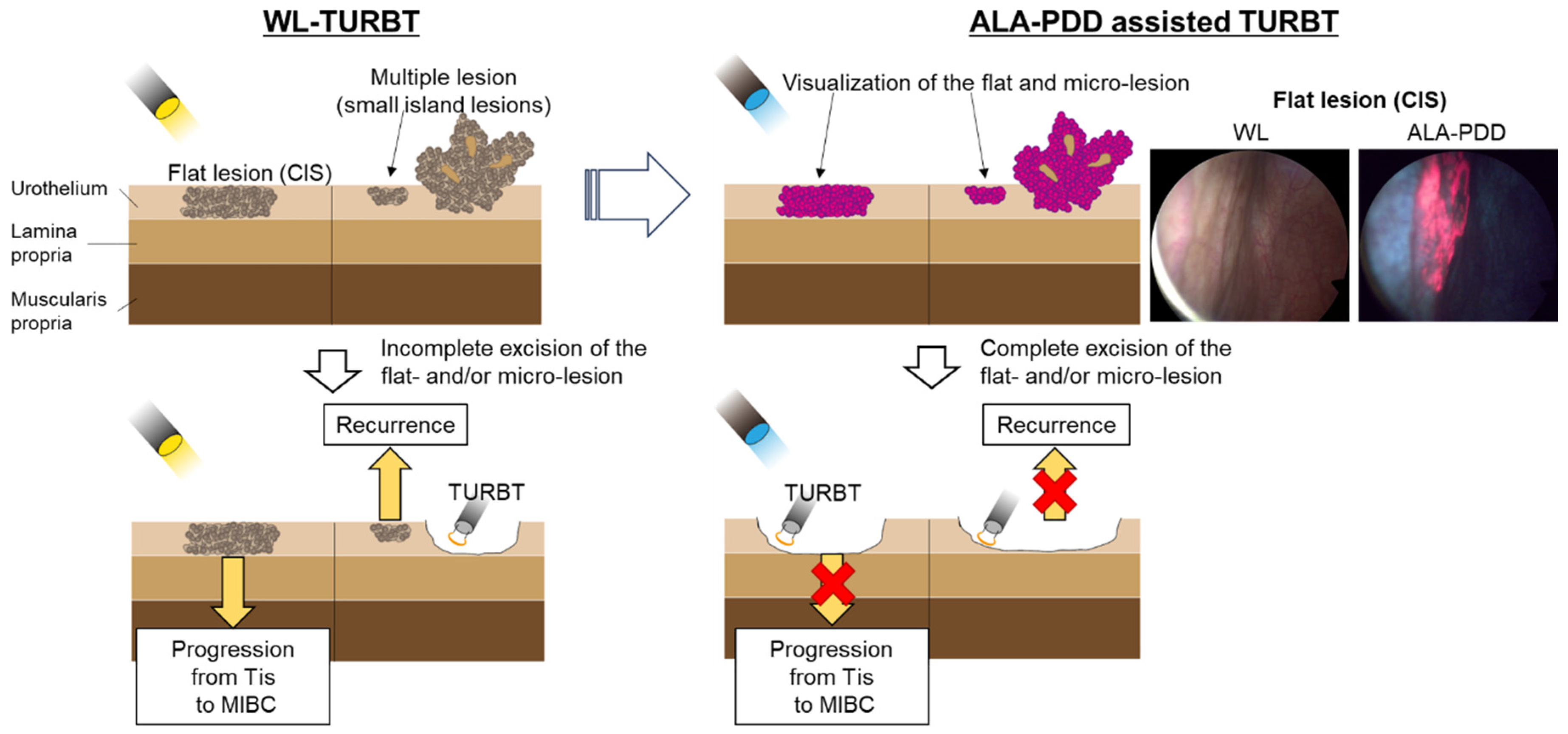
TURBT is the standard surgical treatment for NMIBC. However, conventional TURBT with WL may not detect 4%–41% of small papillary tumors, CIS, multifocal growth, and microscopic lesions [90,91]. Several systematic reviews revealed that PDD-assisted TURBT with 5-ALA or its derivative (hexaminolevulinic acid) increased the detection rate of tumors, particularly for CIS. Additionally, PDD-assisted TURBT with 5-ALA reduced the risk of disease recurrence more than WL-TURBT in patients with NMIBC [92]. Figure 3 shows these concepts.
A recent meta-analysis reported 1- and 2-year recurrence-free survival (RFS) rates after ALA-PDD of 50.4%–89.6% (vs. 39.0%–85.0% for WL) and 40.0%–89.6% (vs. 28.0%–72.0% for WL), respectively. A meta-analysis of nine trials (1782 patients) revealed better 1-year RFS after PDD compared with WL (hazard ratio [HR]: 1.14; 95% confidence interval [CI]: 1.05–1.23, I2 = 70%, p = 0.002), indicating that PDD improved RFS. A meta-analysis of five trials (925 patients) revealed improved 2-year RFS following PDD (HR: 1.25; 95% CI: 1.15–1.35, p ≤ 0.001) [92]. Matsushita et al. reported significantly longer RFS in the PDD group in all subgroups except for tumor size compared with the WL group after 1:1 propensity score matching of 383 patients for age, sex, concomitant history of upper urinary tract UC, preoperative cytology, tumor multiplicity, and tumor size [94]. Moreover, in a study of 1578 consecutive patients with primary NMIBC, Miyake et al. revealed that PDD-TURBT decreased the risk of high- and low-grade tumor recurrences compared with WL-TURBT. PDD significantly reduced the risk of International Bladder Cancer Group-defined progression in patients with NMIBC [95]. However, PDD-TURBT did not reduce recurrence in patients with NMIBC of ≥30 mm [95,96]. The 5-ALA-induced stability of PpIX is dependent on the wavelength and intensity of the right side. PpIX elimination, called photobleaching, is accelerated during WL cystoscopy [90]. Thus, PDD-TURBT did not reduce recurrences in patients with large tumors that require long-term use of WL cystoscopy. Yamashita et al. revealed that a spectrometer with a liquid crystal tunable filter, the 5-ALA-PDD using the average fluorescence altitude of 660–700 nm instead of the peak altitude at 630 nm, is more effective in distinguishing between tumorous and non-tumorous tissues in the gastrointestinal tract, because of the lower photobleaching effect at this specific spectral range [97]. This technique may improve the photobleaching effect in ALA-PDD for NIMBC.
Intravesical BCG instillation induces bladder wall inflammation. This immune response activation induces and supports antitumor mechanisms [98]. BCG therapy prevents intravesical recurrence and progression, thereby prolonging survival in patients with high-grade NMIBC [99]. However, BCG-induced inflammation may cause false-positive fluorescence in PDD. Draga et al. indicated that >3 months of BCG instillation before fluorescence cystoscopy decreases PDD specificity [100]. However, a study of 99 patients by Nakagawa et al. revealed that the combined use of PDD and BCG improved the identification and resection of tumors, especially those that could not be identified by WL alone and may prolong RFS, although the PDD + BCG (PDD-TURBT followed by BCG treatment) group demonstrated higher risk and a high CIS detection rate [101]. Nakagawa et al. proposed several factors that may influence RFS. First, BCG uptake is improved at the tumor resection site. Second, the use of PDD exhibits a photodynamic therapeutic effect [101,102,103]. No significant difference in the 2-year prognosis-free survival (PFS) was detected between the PDD + BCG and WL + BCG groups. However, the PDD + BCG group demonstrated worse PFS [101]. Makino et al. revealed that prior BCG instillation history, particularly BCG unresponsive disease, caused poor cancer recurrence and prognostic factor progression for patients with NMIBC undergoing PDD-TURBT, and special attention should be given to postoperative follow-up [104].
8. PDT with 5-ALA for TURBT in NMIBCs
Rahman et al. reviewed as follows. Bladder tissue is more translucent and readily accessible with a thin fiber optic cable compared with other human tissues, making BC an excellent choice for PDT. Increasing wavelength improves the penetration depth while elevating the chance of muscle damage. Photofrin is given intravenously and red (630 nm) light is used for whole bladder illumination in clinically approved PDT for BC in Canada. However, such treatment conditions caused collateral damage to the whole bladder, particularly the muscle layer, resulting in functional damage to the bladder. In contrast, 5-ALA- or HAL-generating PpIX is excited by a green light that does not penetrate >1 mm into the bladder, thereby sparing the muscular layer [105]. Hence, NMIBC is especially an excellent imminent target for ALA-PDT.
Flat UC demonstrates high recurrence rates. Thus, most patients required additional treatment (e.g., CT and BCG) to prolong recurrence-free intervals and prevent recurrence and disease progression. However, additional intensive care is often necessary after combined modality treatments (such as TURBT + BCG and TURBT + CT) to treat complications associated with chemotherapeutic agent toxicity or BCG-induced severe inflammation [106,107]. ALA-PDT is a painless procedure, and the antitumor effects are induced by low-energy excitation. Thus, patients do not require anesthesia, and the procedure can be repeated. Furthermore, ALA-PDT specifically targets PpIX that has accumulated in tumor cells, like ALA-PDD [108]. In 1996, Kriegmair et al. first reported the use of 5-ALA in PDT for BC treatment, resulting in subsequent clinical studies [103,109,110,111,112,113,114]. These trials were primarily performed in patients with treatment-resistant BC and bladder CIS. Additionally, excitation wavelengths in the green (514 nm), red (630–635 nm), and white (380–700 nm) ranges were used because they can be delivered at a low heat density of 15–100 J/cm2. A study of 45 patients by Filonenko et al. revealed that intraoperative ALA-PDT after TURBT significantly reduced the 1-year recurrence rate for superficial BC (pT stage: Ta-T1) compared with the recurrence rate after TURBT monotherapy (22% vs. 40%–80%). These results were at least equivalent to convenient adjuvant treatments in patients with bladder tumors (1-year recurrence rates were 36%–44% after TURBT + CT and 20%–59% after TURBT + BCG) [115]. ALA-PDT acts on a neoplastic cell attributively and is highly accurate, minimally invasive, and widely applicable. Further improvements, such as a wavelength or the luminescence sensitizer, may be necessary, but ALA-PDT may replace additional treatments for BC, especially CIS. Moreover, large trials with long-term follow-ups should confirm the beneficial effects of ALA-PDT for BC.
9. Screening Using 5-ALA after TURBT in NMIBCs
Urine cytology is frequently performed to screen for BC. Generally, urine cytology is frequently problematic because of its sensitivity in low-grade UC in clinical practice. Interestingly, Yamamichi et al. revealed that 5-ALA-induced fluorescent-selective upper tract urinary cytology, by which the urine sample was centrifuged and the pellets suspended in minimum essential media using 5-ALA hydrochloride was more sensitive than conventional cytology for diagnosing upper urinary tract UC (90.4% vs. 66.3%, p < 0.001) regardless of pT and tumor grade [116]. Therefore, cystoscopy remains necessary as a followup procedure, but the use of ALA-induced cytology together with PDS may be an effective technique for following up after TURBT in NMIBC.
10. Conclusions and Future Perspective
NMIBC and MIBC exhibit great intrinsic heterogeneity regarding different prognoses, survival, progression, and treatment outcomes, but decreasing tumor recurrence in BC (especially in CIS and pT1 UC) that detects the range of the exact lesion and removes them completely is crucial.
A new-generation photosensitizer, 5-ALA, demonstrated high tumor specificity. Moreover, 5-ALA is naturally generated from glycine and succinyl CoA. ALA-PDD and ALA-PDT use 5-ALA. However, ALA-PDD is influenced by the tangent effect and photobleaching, but ALA-PDD has a significantly higher sensitivity for detecting tumors than WL-PDD and NBI, especially in CIS. TURBT, assisted by ALA-PDD, substantially reduces recurrence risk and significantly decreases progression compared with WL-TURBT in patients with NMIBC. Hypotension is well known as a transient adverse event for oral ALA, but our group revealed the multiple factors that are mutually related in the prediction model for ALA-induced hypotension, as mentioned above, and showed the possibility of the conquest of this side effect.
Additionally, ALA-PDT demonstrated limited efficacy for advanced-stage BCs, but it can affect the superficial lesion and prevent muscle damage-induced bladder dysfunction. Therefore, NMIBC is an excellent imminent target for ALA-PDT. In Japan, ALA-PDT has not been recommended yet. ALA-PDT is highly accurate, minimally invasive, and widely applicable and may replace additional BC treatments such as CT and BCG. A clinically successful ALA-PDT for NMIBC may be developed by clinical experiences and a deeper understanding of pathobiology of NMIBC, similar to ALA-PDD.
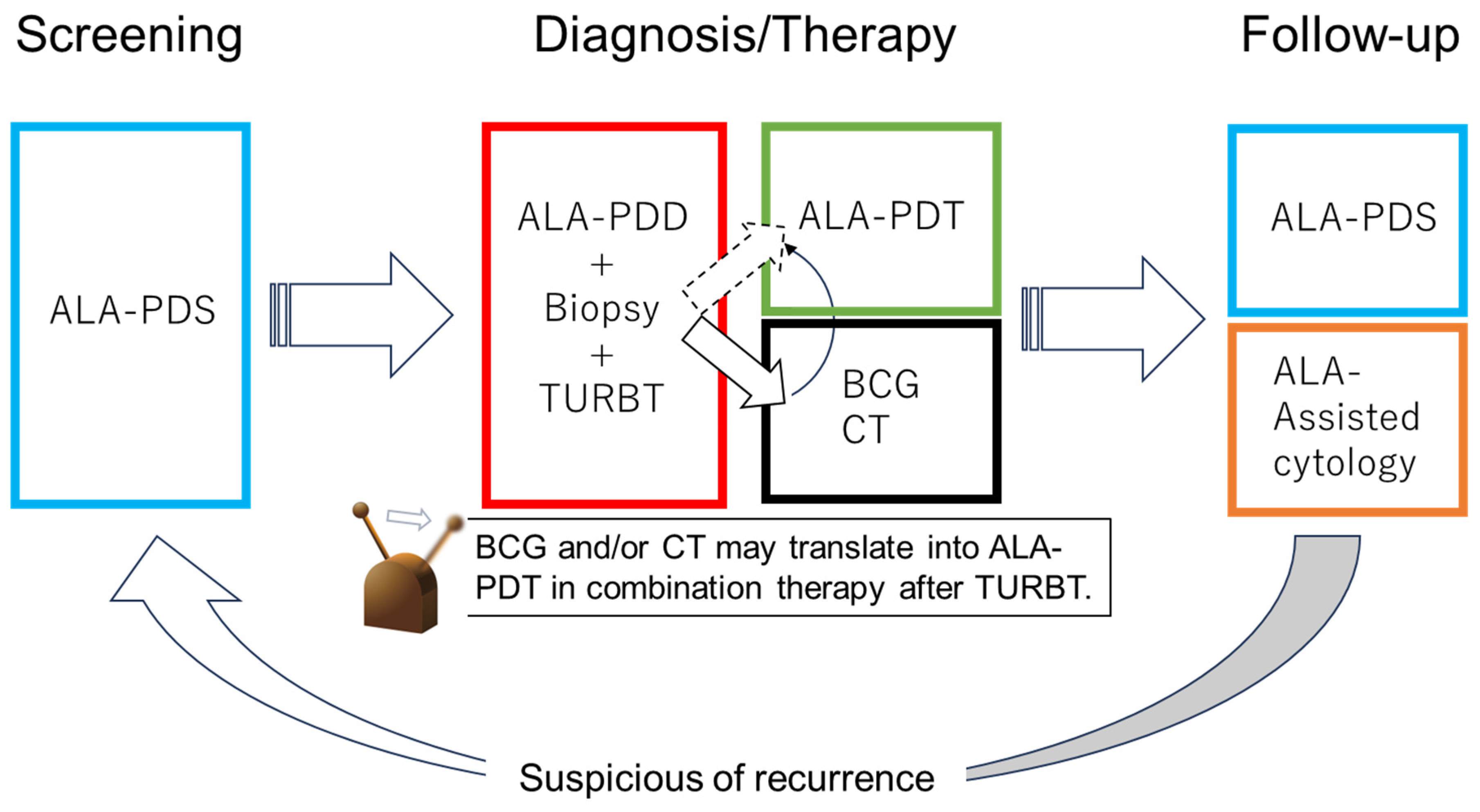
Moreover, in the future, patients with NMIBC will be treated by PDD-TURBT together with ALA-PDT, and then received followup-up using ALA-PDS and ALA-induced fluorescent urinary cytology. Furthermore, BC diagnosis, treatment, and follow-up may be performed using 5-ALA. Techniques using 5-ALA are based on the Warburg effect, which is a basic property across all cancers. The techniques will be used as a therapeutic strategy of various cancer types and can be beneficial for patients.
Figure 4.
Future perspective of 5-ALA in NMIB. In the future, bladder cancer diagnosis, treatment, and followup-up may be performed with 5-ALA.
Figure 4.
Future perspective of 5-ALA in NMIB. In the future, bladder cancer diagnosis, treatment, and followup-up may be performed with 5-ALA.
Author Contributions
Conceptualization, A.K. and M.F.; writing—original draft preparation, A.K., M.F and K.I.; writing—review and editing, A.K., H.F., K.F., W.I., M.F. and K.I. All authors have read and agreed to the published version of the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sung, H; Ferlay, J; Siegel, RL; Laversanne, M; Soerjomataram, I; Jemal, A; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Antoni, S; Ferlay, J; Soerjomataram, I; Znaor, A; Jemal, A; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur Urol 2017, 71, 96–108. [Google Scholar] [CrossRef]
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between smoking and risk of bladder cancer among men and women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef]
- Wilhelm-Benartzi, C.S.; Christensen., B.C.; Koestler, D.C.; Houseman, E.A.; Schned, A.R.; Karagas, M.R.; Kelsey, K.T.; Marsit, C.J. Association of secondhand smoke exposures with DNA methylation in bladder carcinomas. Cancer Causes Control 2011, 22, 1205–1213. [Google Scholar] [CrossRef]
- Moch, H. Urinary and Male Genital Tumours: WHO Classification of Tumours, 5th ed.; Chee, A.I., Goldman-Levy, G., Lokuhetty, D., Vishal-Rao, B., White, A.V., Eds.; IARC Publications: Lyon, France, 2022; Volume 8, 576p. [Google Scholar]
- Berdik, C. Unlocking bladder cancer. Nature 2017, 551, S34–S35. [Google Scholar] [CrossRef]
- James, A.C.; Gore, J.L. The costs of non-muscle invasive bladder cancer. Urol. Clin. North. Am 2013, 40, 261–269. [Google Scholar] [CrossRef]
- Abdollah, F.; Gandaglia, G.; Thuret, R.; Schmitges, J.; Tian, Z.; Jeldres, C.; Passoni, N.M.; Briganti, A.; Shariat, S.F.; Perrotte, P.; Montorsi, F.; Karakiewicz, P.I.; Sun, M. Incidence, survival and mortality rates of stage-specific bladder cancer in United States: a trend analysis. Cancer Epidemiol 2013, 37, 219–225. [Google Scholar] [CrossRef]
- Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Dominguez; Escrig, J.L.; Gontero, P.; Liedberg, F.; Masson-Lecomte, A.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Seisen, T.; Soukup, V.; Sylvester, R.J. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (Ta, T1, and Carcinoma in Situ). Eur Urol 2022, 81, 75–94. [Google Scholar] [CrossRef]
- Hurst, C.D.; Alder, O.; Platt, F.M.; Droop, A.; Stead, L.F.; Burns, J.E.; Burghel, G.J.; Jain, S.; Klimczak, L.J.; Lindsay, H.; Roulson, J.A.; Taylor, C.F.; Thygesen, H.; Cameron, A.J.; Ridley, A.J.; Mott, H.R.; Gordenin, D.A.; Knowles, M.A. Genomic Subtypes of Non-invasive Bladder Cancer with Distinct Metabolic Profile and Female Gender Bias in KDM6A Mutation Frequency. Cancer Cell 2017, 32, 701–715.e7. [Google Scholar] [CrossRef]
- Ségal-Bendirdjian, E.; Geli, V. Non-canonical roles of telomerase: unraveling the imbroglio. Front. Cell Dev. Biol 2019, 7, 332. [Google Scholar] [CrossRef]
- Agarwal, N.; Rinaldetti, S.; Cheikh, B.B.; Zhou, Q.; Hass, E.P.; Jones, R.T.; Joshi, M.; LaBarbera, D.V.; Knott, S.R.V.; Cech, T.R.; Theodorescu, D. TRIM28 is a transcriptional activator of the mutant TERT promoter in human bladder cancer. Proc Natl Acad Sci USA 2021, 118, e2102423118. [Google Scholar] [CrossRef]
- Borah, S.; Xi, L.; Zaug, A.J.; Powell, N.M.; Dancik, G.M.; Cohen, S.B.; Costello, J.C.; Theodorescu, D.; Cech, T.R. Cancer. TERT promoter mutations and telomerase reactivation in urothelial cancer. Science, 2015; 347, 1006–1010. [Google Scholar]
- Nickerson, M.L.; Witte, N.; Im, K.M.; Turan, S.; Owens, C.; Misner, K.; Tsang, S.X.; Cai, Z.; Wu, S.; Dean, M.; Costello, J.C.; Theodorescu, D. Molecular analysis of urothelial cancer cell lines for modeling tumor biology and drug response. Oncogene 2017, 36, 35–46. [Google Scholar] [CrossRef]
- Nickerson, M.L.; Dancik, G.M.; Im, K.M.; Edwards, M.G.; Turan, S.; Brown, J.; Ruiz-Rodriguez, C.; Owens., C.; Costello, J.C.; Guo, G.; Tsang, S.X.; Li, Y.; Zhou, Q.; Cai, Z.; Moore, L.E.; Lucia, M.S.; Dean, M.; Theodorescu, D. Concurrent alterations in TERT, KDM6A, and the BRCA pathway in bladder cancer. Clin Cancer Res 2014, 20, 4935–4948. [Google Scholar] [CrossRef]
- Rachakonda, P.S.; Hosen, I.; de Verdier, P.J.; Fallah, M.; Heidenreich, B.; Ryk, C.; Wiklund, N.P.; Steineck, G.; Schadendorf, D.; Hemminki, K.; Kumar, R. TERT promoter mutations in bladder cancer affect patient survival and disease recurrence through modification by a common polymorphism. Proc Natl Acad Sci USA 2013, 110, 17426–17431. [Google Scholar] [CrossRef]
- Leão, R.; Lee, D.; Figueiredo, A.; Hermanns, T.; Wild, P.; Komosa, M.; Lau, I.; Mistry, M.; Nunes, N.M.; Price, A.J.; Zhang, C.; Lipman, T.; Poyet, C.; Valtcheva, N.; Oehl, K.; Coelho, H.; Sayyid, R.; Gomes, A.M.; Prado, E.; Castro, L.; Sweet, J.; Vinagre, J.; Apolónio, J.; Stephens, D.; Faleiro, I.; Fadaak, K.; Richard, P.O.; Kulkarni, G.; Zlotta, A.R.; Hamilton, R.J.; Castelo-Branco, P.; Tabori, U. Combined genetic and epigenetic alterations of the TERT promoter affect clinical and biological behavior of bladder cancer. Int J Cancer 2019, 144, 1676–1684. [Google Scholar] [CrossRef]
- Kurtis, B.; Zhuge, J.; Ojaimi, C.; Ye, F.; Cai, D.; Zhang, D.; Fallon, J.T.; Zhong, M. Recurrent TERT promoter mutations in urothelial carcinoma and potential clinical applications. Ann Diagn Pathol 2016, 21, 7–11. [Google Scholar] [CrossRef]
- Allory, Y.; Beukers, W.; Sagrera, A.; Flández, M.; Marqués, M.; Márquez, M.; van der Keur, K.A.; Dyrskjot, L.; Lurkin, I.; Vermeij, M.; Carrato, A.; Lloreta, J.; Lorente, J.A.; Carrillo-de Santa; Pau, E.; Masius, R.G.; Kogevinas, M.; Steyerberg, E.W.; van Tilborg, A.A.; Abas, C.; Orntoft, T.F.; Zuiverloon, T.C.; Malats, N.; Zwarthoff, E.C.; Real, F.X. Telomerase reverse transcriptase promoter mutations in bladder cancer: high frequency across stages, detection in urine, and lack of association with outcome. Eur Urol 2014, 65, 360–366. [Google Scholar] [CrossRef]
- Lindskrog, S.V.; Prip, F.; Lamy, P.; Taber, A.; Groeneveld, C.S.; Birkenkamp-Demtröder, K.; Jensen, J.B.; Strandgaard, T.; Nordentoft, I.; Christensen, E.; Sokac, M.; Birkbak, N.J.; Maretty, L.; Hermann, G.G.; Petersen, A.C.; Weyerer, V.; Grimm, M.O.; Horstmann, M.; Sjödahl, G.; Höglund, M.; Steiniche, T.; Mogensen, K.; de Reyniès, A.; Nawroth, R.; Jordan, B.; Lin, X.; Dragicevic, D.; Ward, D.G.; Goel, A.; Hurst, C.D.; Raman, J.D.; Warrick, J.I.; Segersten, U.; Sikic, D.; van Kessel, K.E.M.; Maurer, T.; Meeks, J.J.; DeGraff, D.J.; Bryan, R.T.; Knowles, M.A.; Simic, T.; Hartmann, A.; Zwarthoff, E.C.; Malmström, P.U.; Malats, N.; Real, F.X.; Dyrskjøt, L. An integrated multi-omics analysis identifies prognostic molecular subtypes of non-muscle-invasive bladder cancer. Nat Commun 2021, 2, 2301. [Google Scholar] [CrossRef]
- Robertson, A.G.; Kim, J.; Al-Ahmadie, H.; Bellmunt, J.; Guo, G.; Cherniack, A.D.; Hinoue, T.; Laird, P.W.; Hoadley, K.A.; Akbani, R.; Castro, M.A.A.; Gibb, E.A.; Kanchi, R.S.; Gordenin, D.A.; Shukla, S.A.; Sanchez-Vega, F.; Hansel, D.E.; Czerniak, B.A.; Reuter, V.E.; Su, X.; de Sa Carvalho, B.; Chagas, V.S.; Mungall, K.L.; Sadeghi, S.; Pedamallu, C.S.; Lu, Y.; Klimczak, L.J.; Zhang, J.; Choo, C.; Ojesina, A.I.; Bullman, S.; Leraas, K.M.; Lichtenberg, T.M.; Wu, C.J.; Schultz, N.; Getz, G.; Meyerson, M.; Mills, G.B.; McConkey, D.J.; TCGA Research Network; Weinstein, J.N.; Kwiatkowski, D.J.; Lerner, S.P. Comprehensive Molecular Characterization of Muscle-Invasive Bladder Cancer. Cell 2017, 171, 540–556.e25. [Google Scholar] [CrossRef]
- Shi, M.J.; Meng, X.Y.; Lamy, P.; Banday, A.R.; Yang, J.; Moreno-Vega, A.; Chen, C.L.; Dyrskjøt, L.; Bernard-Pierrot, I.; Prokunina-Olsson, L.; Radvanyi, F. APOBEC-mediated Mutagenesis as a Likely Cause of FGFR3 S249C Mutation Over-representation in Bladder Cancer. Eur Urol 2019, 76, 9–13. [Google Scholar] [CrossRef]
- van Rhijn, B.W.; Vis, A.N.; van der Kwast, T.H.; Kirkels, W.J.; Radvanyi, F.; Ooms, E.C.; Chopin, D.K.; Boevé, E.R.; Jöbsis, A.C.; Zwarthoff, E.C. Molecular grading of urothelial cell carcinoma with fibroblast growth factor receptor 3 and MIB-1 is superior to pathologic grade for the prediction of clinical outcome. J Clin Oncol 2003, 21, 1912–1921. [Google Scholar] [CrossRef] [PubMed]
- López-Knowles, E.; Hernández, S.; Malats, N.; Kogevinas, M.; Lloreta, J.; Carrato, A.; Tardón, A.; Serra, C.; Real, F.X. PIK3CA mutations are an early genetic alteration associated with FGFR3 mutations in superficial papillary bladder tumors. Cancer Res 2006, 66, 7401–7404. [Google Scholar] [PubMed]
- Hernández, S.; López-Knowles, E.; Lloreta, J.; Kogevinas, M.; Amorós, A.; Tardón, A.; Carrato, A.; Serra, C.; Malats, N.; Real, F.X. Prospective study of FGFR3 mutations as a prognostic factor in nonmuscle invasive urothelial bladder carcinomas. J Clin Oncol 2006, 24, 3664–3671. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, A.; Moser, K.; Kriegmair, M.; Hofstetter, A.; Hofstaedter, F.; Knuechel, R. Frequent genetic alterations in simple urothelial hyperplasias of the bladder in patients with papillary urothelial carcinoma. Am J Pathol 1999, 154, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Hurst, C.D.; Cheng, G.; Platt, F.M.; Castro, M.A.A.; Marzouka, N.S.; Eriksson, P.; Black, E.V.I.; Alder, O.; Lawson, A.R.J.; Lindskrog, S.V.; Burns, J.E.; Jain, S.; Roulson, J.A.; Brown, J.C.; Koster, J.; Robertson, A.G.; Martincorena, I.; Dyrskjøt, L.; Höglund, M.; Knowles, M.A. Stage-stratified molecular profiling of non-muscle-invasive bladder cancer enhances biological, clinical, and therapeutic insight. Cell Rep Med 2021, 2, 100472. [Google Scholar] [CrossRef] [PubMed]
- Alexandrov, L.B.; Nik-Zainal, S.; Wedge, D.C.; Aparicio, S.A.; Behjati, S.; Biankin, A.V.; Bignell, G.R.; Bolli, N.; Borg, A.; Børresen-Dale, A.L.; Boyault, S.; Burkhardt, B.; Butler, A.P.; Caldas, C.; Davies, H.R.; Desmedt, C.; Eils, R.; Eyfjörd, J.E.; Foekens, J.A.; Greaves, M.; Hosoda, F.; Hutter, B.; Ilicic, T.; Imbeaud, S.; Imielinski, M.; Jäger, N.; Jones, D.T.; Jones, D.; Knappskog, S.; Kool, M.; Lakhani, S.R.; López-Otín, C.; Martin, S.; Munshi, N.C.; Nakamura, H.; Northcott, P.A.; Pajic, M.; Papaemmanuil, E.; Paradiso, A.; Pearson, J.V.; Puente, X.S.; Raine, K.; Ramakrishna, M.; Richardson, A.L.; Richter, J.; Rosenstiel, P.; Schlesner, M.; Schumacher, T.N.; Span, P.N.; Teague, J.W.; Totoki, Y.; Tutt, A.N.; Valdés-Mas, R.; van Buuren, M.M.; van ‘t Veer, L.; Vincent-Salomon, A.; Waddell, N.; Yates, L.R.; Australian Pancreatic Cancer Genome Initiative; ICGC Breast Cancer Consortium; ICGC MMML-Seq Consortium; ICGC PedBrain; Zucman-Rossi, J.; Futreal, P.A.; McDermott, U.; Lichter, P.; Meyerson, M.; Grimmond, S.M.; Siebert, R.; Campo, E.; Shibata, T.; Pfister, S.M.; Campbell, P.J.; Stratton, M.R. Signatures of mutational processes in human cancer. Nature 2013, 500, 415–421. [Google Scholar]
- Ching, C.B.; Amin, M.B.; Tubbs, R.R.; Elson, P.; Platt, E.; Dreicer, R.; Fergany, A.; Hansel, D.E. HER2 gene amplification occurs frequently in the micropapillary variant of urothelial carcinoma: analysis by dual-color in situ hybridization. Mod Pathol. 2011, 24, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Willis, D.L.; Flaig, T.W.; Hansel, D.E.; Milowsky, M.I.; Grubb, R.L.; Al-Ahmadie, H.A.; Plimack, E.R.; Koppie, T.M.; McConkey, D.J.; Dinney, C.P.; Hoffman, V.A.; Droller, M.J.; Messing, E.; Kamat, A.M. Micropapillary bladder cancer: current treatment patterns and review of the literature. Urol Oncol 2014, 32, 826–832. [Google Scholar] [CrossRef]
- Isharwal, S.; Huang, H.; Nanjangud, G.; Audenet, F.; Chen, Y.B.; Gopalan, A.; Fine, S.W.; Tickoo, S.K.; Lee, B.H.; Iyer, G.; Chadalavada, K.; Rosenberg, J.E.; Bajorin, D.F.; Herr, H.W.; Donat, S.M.; Dalbagni, G.; Bochner, B.H.; Solit, D.B.; Reuter, V.E.; Al-Ahmadie, H.A. Intratumoral heterogeneity of ERBB2 amplification and HER2 expression in micropapillary urothelial carcinoma. Hum Pathol 2018, 77, 63–69. [Google Scholar] [CrossRef]
- Teo, M.Y.; Al-Ahmadie, H.; Seier, K.; Tully, C.; Regazzi, A.M.; Pietzak, E.; Solit, D.B.; : Tickoo, S.; Reuter, V.; Cha, E.K.; Herr, H.; Donahue, T.; Donat, S.M.; Dalbagni, G.; Bochner, B.H.; Funt, S.; Iyer, G.V.; Bajorin, D.F.; Ostrovnaya, I.; Rosenberg, J.E. Natural history, response to systemic therapy, and genomic landscape of plasmacytoid urothelial carcinoma. Br J Cancer 2021, 124, 1214–1221. [Google Scholar] [CrossRef]
- Taylor, C.F.; Platt, F.M.; Hurst, C.D.; Thygesen, H.H.; Knowles, M.A. Frequent inactivating mutations of STAG2 in bladder cancer are associated with low tumour grade and stage and inversely related to chromosomal copy number changes. Hum Mol Genet 2014, 23, 1964–1974. [Google Scholar] [CrossRef] [PubMed]
- Gordon, N.S.; Humayun-Zakaria, N.; Goel, A.; Abbotts, B.; Zeegers, M.P.; Cheng, K.K.; James, N.D.; Arnold, R.; Bryan, R.T.; Ward, D.G. STAG2 Protein Expression in Non-muscle-invasive Bladder Cancer: Associations with Sex, Genomic and Transcriptomic Changes, and Clinical Outcomes. Eur Urol Open Sci 2022, 38, 88–95. [Google Scholar] [CrossRef] [PubMed]
- di Martino, E.; L’Hôte, C.G.; Kennedy, W.; Tomlinson, D.C.; Knowles, M.A. Mutant fibroblast growth factor receptor 3 induces intracellular signaling and cellular transformation in a cell type- and mutation-specific manner. Oncogene 2009, 28, 4306–4316. [Google Scholar] [CrossRef] [PubMed]
- Kandimalla, R.; van Tilborg, A.A.; Zwarthoff, E.C. DNA methylation-based biomarkers in bladder cancer. Nat Rev Urol 2013, 10, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.B.; Greene, F.L. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: Berlin, Germany, 2017; 1049p. [Google Scholar]
- Leivo, M.Z.; Sahoo, D.; Hamilton, Z.; Mirsadraei, L.; Shabaik, A.; Parsons, J.K.; Kader, A.K.; Derweesh, I.; Kane, C.; Hansel, D.E. Analysis of T1 Bladder Cancer on Biopsy and Transurethral Resection Specimens: Comparison and Ranking of T1 Quantification Approaches to Predict Progression to Muscularis Propria Invasion. Am J Surg Pathol 2018, 42, e1–e10. [Google Scholar] [CrossRef] [PubMed]
- Soria, F.; Dutto, D.; Gontero, P. Clinical and biological markers for risk-stratification of T1 high-grade non-muscle invasive bladder cancer. Curr Opin Urol 2022, 32, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Castaneda, P.R.; Theodorescu, D.; Rosser, C.J.; Ahdoot, M. Identifying novel biomarkers associated with bladder cancer treatment outcomes. Front Oncol 2023, 13, 1114203. [Google Scholar] [CrossRef] [PubMed]
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur Urol 2017, 71, 96–108. [Google Scholar] [CrossRef]
- IARC. Global Cancer Observatory: Cancer Tomorrow. WHO (2023).
- Tran, L.; Xiao, J.F.; Agarwal, N.; Duex, J.E.; Theodorescu, D. Advances in bladder cancer biology and therapy. Nat Rev Cancer 2021, 21, 104–121. [Google Scholar] [CrossRef]
- Matuszczak, M.; Salagierski, M. Diagnostic and Prognostic Potential of Biomarkers CYFRA 21.1, ERCC1, p53, FGFR3 and TATI in Bladder Cancers. Int J Mol Sci 2020, 21, 3360. [Google Scholar] [CrossRef]
- Mertens, L.S.; Claps, F.; Mayr, R.; Bostrom, P.J.; Shariat, S.F.; Zwarthoff, E.C.; Boormans, J.L.; Abas, C.; van Leenders, G.J.L.H.; Götz, S.; Hippe, K.; Bertz, S.; Neuzillet, Y.; Sanders, J.; Broeks, A.; Peters, D.; van der Heijden, M.S.; Jewett, M.A.S.; Stöhr, R.; Zlotta, A.R.; Eckstein, M.; Soorojebally, Y.; van der Schoot, D.K.E.; Wullich, B.; Burger, M.; Otto, W.; Radvanyi, F.; Sirab, N.; Pouessel, D.; van der Kwast, T.H.; Hartmann, A.; Lotan, Y.; Allory, Y.; Zuiverloon, T.C.M.; van Rhijn, B.W.G. Prognostic markers in invasive bladder cancer: FGFR3 mutation status versus P53 and KI-67 expression: a multi-center, multi-laboratory analysis in 1058 radical cystectomy patients. Urol Oncol 2022, 40, 110.e1–110.e9. [Google Scholar] [CrossRef] [PubMed]
- Cummings, K.B.; Barone, J.G.; Ward, W.S. Diagnosis and staging of bladder cancer. Urol Clin North Am 1992, 19, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Khadhouri, S.; Gallagher, K.M.; MacKenzie, K.R.; Shah, T.T.; Gao, C.; Moore, S.; Zimmermann, E.F.; Edison, E.; Jefferies, M.; Nambiar, A.; Mannas, M.P.; Lee, T.; Marra, G.; Lillaz, B.; Gómez; Rivas, J.; Olivier, J.; Assmus, M.A.; Uçar, T.; Claps, F.; Boltri, M.; Burnhope, T.; Nkwam, N.; Tanasescu, G.; Boxall, N.E.; Downey, A.P.; Lal, A.A.; Antón-Juanilla, M.; Clarke, H.; Lau, D.H.W.; Gillams., K.; Crockett, M.; Nielsen, M.; Takwoingi, Y.; Chuchu, N.; O’Rourke, J.; MacLennan, G.; McGrath, J.S.; Kasivisvanathan, V.; IDENTIFY Study group. The IDENTIFY study: the investigation and detection of urological neoplasia in patients referred with suspected urinary tract cancer - a multicentre observational study. BJU Int 2021, 128, 440–450. [Google Scholar] [CrossRef]
- Xing, J.; Reynolds, J.P. Diagnostic Advances in Urine Cytology. Surg Pathol Clin 2018, 11, 601–610. [Google Scholar] [CrossRef]
- Barkan, G.A.; Wojcik, E.M.; Nayar, R.; Savic-Prince, S.; Quek, M.L.; Kurtycz, D.F.; Rosenthal, D.L. The Paris System for Reporting Urinary Cytology: The Quest to Develop a Standardized Terminology. Adv Anat Pathol 2016, 23, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Nikas, I.P.; Seide, S.; Proctor, T.; Kleinaki, Z.; Kleinaki, M.; Reynolds, J.P. The Paris System for Reporting Urinary Cytology: A Meta-Analysis. J Pers Med 2022, 12, 170. [Google Scholar] [CrossRef] [PubMed]
- Guo, A.; Wang, X.; Gao, L.; Shi, J.; Sun, C.; Wan, Z. Bladder tumour antigen (BTA stat) test compared to the urine cytology in the diagnosis of bladder cancer: A meta-analysis. Can Urol Assoc J 2014, 8, E347–E352. [Google Scholar] [CrossRef] [PubMed]
- Dimashkieh, H.; Wolff, D.J.; Smith, T.M.; Houser, P.M.; Nietert, P.J.; Yang, J. Evaluation of urovysion and cytology for bladder cancer detection: a study of 1835 paired urine samples with clinical and histologic correlation. Cancer Cytopathol 2013, 121, 591–597. [Google Scholar] [CrossRef]
- Zippe, C.; Pandrangi, L.; Agarwal, A. NMP22 is a sensitive, cost-effective test in patients at risk for bladder cancer. J Urol 1999, 161, 62–65. [Google Scholar] [CrossRef]
- He, H.; Han, C.; Hao, L.; Zang, G. ImmunoCyt test compared to cytology in the diagnosis of bladder cancer: A meta-analysis. Oncol Lett 2016, 12, 83–88. [Google Scholar] [CrossRef]
- Wang, Z.; Que, H.; Suo, C.; Han, Z.; Tao, J.; Huang, Z.; Ju, X.; Tan, R.; Gu, M. Evaluation of the NMP22 BladderChek test for detecting bladder cancer: a systematic review and meta-analysis. Oncotarget 2017, 8, 100648–100656. [Google Scholar] [CrossRef] [PubMed]
- Heitzer, E.; Auinger, L.; Speicher, M.R. Cell-Free DNA and Apoptosis: How Dead Cells Inform About the Living. Trends Mol Med 2020, 26, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Khier, S.; Lohan, L. Kinetics of circulating cell-free DNA for biomedical applications: critical appraisal of the literature. Future Sci OA 2018, 4, FSO295. [Google Scholar] [CrossRef] [PubMed]
- Christensen, E.; Birkenkamp-Demtröder, K.; Sethi, H.; Shchegrova, S.; Salari, R.; Nordentoft, I.; Wu, H.T.; Knudsen, M.; Lamy, P.; Lindskrog, S.V.; Taber, A.; Balcioglu, M.; Vang, S.; Assaf, Z.; Sharma, S.; Tin, A.S.; Srinivasan, R.; Hafez, D.; Reinert, T.; Navarro, S.; Olson, A.; Ram, R.; Dashner, S.; Rabinowitz, M.; Billings, P.; Sigurjonsson, S.; Andersen, C.L.; Swenerton, R.; Aleshin, A.; Zimmermann, B.; Agerbæk, M.; Lin, C.J.; Jensen, J.B.; Dyrskjøt, L. Early Detection of Metastatic Relapse and Monitoring of Therapeutic Efficacy by Ultra-Deep Sequencing of Plasma Cell-Free DNA in Patients With Urothelial Bladder Carcinoma. J Clin Oncol 2019, 37, 1547–1557. [Google Scholar] [CrossRef] [PubMed]
- Ploeg, M.; Kiemeney, L.A.; Smits, G.A.; Vergunst, H.; Viddeleer, A.C.; Geboers, A.D.; van Berkel, H.; van Boven, E.; Aben, K.K.; Witjes, J.A. Discrepancy between clinical staging through bimanual palpation and pathological staging after cystectomy. Urol Oncol 2012, 30, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Pasin, E.; Josephson, D.Y.; Mitra, A.P.; Cote, R.J.; Stein, J.P. Superficial bladder cancer: an update on etiology, molecular development, classification, and natural history. Rev Urol 2008, 10, 31–43. [Google Scholar] [PubMed]
- Edgerton, N.; Sirintrapun, S.J.; Munoz, M.; Chen, Z.; Osunkoya, A.O. Micropapillary urothelial carcinoma of the urinary bladder: a clinicopathological analysis of 24 cases. Int J Urol 2011, 18, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Fernández, M.I.; Williams, S.B.; Willis, D.L.; Slack, R.S.; Dickstein, R.J.; Parikh, S.; Chiong, E.; Siefker-Radtke, A.O.; Guo, C.C.; Czerniak, B.A.; McConkey, D.J.; Shah, J.B.; Pisters, L.L.; Grossman, H.B.; Dinney, C.P.; Kamat, A.M. Clinical risk stratification in patients with surgically resectable micropapillary bladder cancer. BJU Int 2017, 119, 684–691. [Google Scholar] [CrossRef]
- Hedegaard, J.; Lamy, P.; Nordentoft, I.; Algaba, F.; Høyer, S.; Ulhøi, B.P.; Vang, S.; Reinert, T.; Hermann, G.G.; Mogensen, K.; Thomsen, M.B.H.; Nielsen, M.M.; Marquez, M.; Segersten, U.; Aine, M.; Höglund, M.; Birkenkamp-Demtröder, K.; Fristrup, N.; Borre, M.; Hartmann, A.; Stöhr, R.; Wach, S.; Keck, B.; Seitz, A.K.; Nawroth, R.; Maurer, T.; Tulic, C.; Simic, T.; Junker, K.; Horstmann, M.; Harving, N.; Petersen, A.C.; Calle, M.L.; Steyerberg, E.W.; Beukers, W.; van Kessel, K.E.M.; Jensen, J.B.; Pedersen, J.S.; Malmström, P.U.; Malats, N.; Real, F.X.; Zwarthoff, E.C.; Ørntoft, T.F.; Dyrskjøt, L. Comprehensive Transcriptional Analysis of Early-Stage Urothelial Carcinoma. Cancer Cell 2016, 30, 27–42. [Google Scholar] [CrossRef]
- Dyrskjøt, L.; Hansel, D.E.; Efstathiou, J.A.; Knowles, M.A.; Galsky, M.D.; Teoh, J.; Theodorescu, D. Bladder cancer. Nat Rev Dis Primers 2023, 9, 58. [Google Scholar] [CrossRef]
- Gallioli, A.; Diana, P.; Fontana, M.; Territo, A.; Rodriguez-Faba, Ó.; Gaya, J.M.; Sanguedolce, F.; Huguet, J.; Mercade, A.; Piana, A.; Aumatell, J.; Bravo-Balado, A.; Algaba, F.; Palou, J.; Breda, A. En Bloc Versus Conventional Transurethral Resection of Bladder Tumors: A Single-center Prospective Randomized Noninferiority Trial. Eur Urol Oncol 2022, 5, 440–448. [Google Scholar] [CrossRef]
- D’Andrea, D.; Soria, F.; Hurle, R.; Enikeev, D.; Kotov, S.; Régnier, S.; Xylinas, E.; Lusuardi, L.; Heidenreich, A.; Cai, C.; Frego, N.; Taraktin, M.; Ryabov, M.; Gontero, P.; Compérat, E.; Shariat, S.F.; eBLOC Study Team. En Bloc Versus Conventional Resection of Primary Bladder Tumor (eBLOC): A Prospective, Multicenter, Open-label, Phase 3 Randomized Controlled Trial. Eur Urol Oncol, 2023; 6, 508–515. [Google Scholar]
- Teoh, Y.C.J.; Chan, T.; Tsang, C.; Li, K.; Cheng, K.-C.; Cho, C.; Chan, H.-C.; Chiu, Y.; Ho., B.; Li, T.; Law, M.; Lee, Y.; Cheng, C.; Lo, K.; Lam, K.; Chan, K; So, H.-S.; Leung, C.; Chan, C.; Yiu, M.; Ng, C.; Poon, V.; Leung, C.; Chi-Fai, N.; The EB-StaR Study Group. A0707 - Transurethral en bloc resection versus standard resection of bladder tumour: a multi-center randomized trial (EB-StaR Study). Eur Urol 2023 83, S997–S998.Babjuk, M.; Burger, M.; Compérat, E.M,, Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.G.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; Zigeuner, R.; Capoun, O.; Cohen, D.; Escrig, J.L.D.; Hernández, V.; Peyronnet, B.; Seisen, T.; Soukup, V. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ) - 2019 Update. Eur Urol 2019, 76, 639–657. [Google Scholar]
- Messing, E.M.; Tangen, C.M.; Lerner, S.P.; Sahasrabudhe, D.M.; Koppie, T.M.; Wood, D.P., Jr.; Mack, P.C.; Svatek, R.S.; Evans, C.P.; Hafez, K.S.; Culkin, D.J.; Brand, T.C.; Karsh, L.I.; Holzbeierlein, J.M.; Wilson, S.S.; Wu, G.; Plets, M.; Vogelzang, N.J.; Thompson, I.M., Jr. Effect of Intravesical Instillation of Gemcitabine vs Saline Immediately Following Resection of Suspected Low-Grade Non-Muscle-Invasive Bladder Cancer on Tumor Recurrence: SWOG S0337 Randomized Clinical Trial. JAMA 2018, 319, 1880–1888. [Google Scholar] [CrossRef]
- Höltl, L.; Eder, I.E.; Klocker, H.; Hobisch, A.; Bartsch, G.; Stenzl, A. Photodynamic diagnosis with 5-aminolevulinic acid in the treatment of secondary urethral tumors: first in vitro and in vivo results. Eur. Urol 2001, 39, 178–182. [Google Scholar]
- Nakai, Y.; Tatsumi, Y.; Miyake, M.; Anai, S.; Kuwada, M.; Onishi, S.; Chihara, Y.; Tanaka, N.; Hirao, Y.; Fujimoto, K. Expression of ferrochelatase has a strong correlation in protoporphyrin IX accumulation with photodynamic detection of bladder cancer. Photodiagn Photodyn Ther, 2016; 13, 225–232. [Google Scholar]
- Inoue, K.; Fukuhara, H.; Yamamoto, S.; Karashima, T.; Kurabayashi, A.; Furihata, M.; Hanazaki, K.; Lai, H.W.; Ogura, S.I. Current status of photodynamic technology for urothelial cancer. Cancer Sci 2022, 113, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Hagiya, Y.; Endo, Y.; Yonemura, Y.; Takahashi, K.; Ishizuka, M.; Abe, F.; Tanaka, T.; Okura, I.; Nakajima, M.; Ishikawa, T.; Ogura, S. Pivotal roles of peptide transporter PEPT1 and ATP-binding cassette (ABC) transporter ABCG2 in 5-aminolevulinic acid (ALA)-based photocytotoxicity of gastric cancer cells in vitro. Photodiagnosis Photodyn Ther 2012, 9, 204–214. [Google Scholar] [CrossRef] [PubMed]
- Hagiya, Y.; Fukuhara, H.; Matsumoto, K.; Endo, Y.; Nakajima, M.; Tanaka, T.; Okura, I.; Kurabayashi, A.; Furihata, M.; Inoue, K.; Shuin, T.; Ogura, S. Expression levels of PEPT1 and ABCG2 play key roles in 5-aminolevulinic acid (ALA)-induced tumor-specific protoporphyrin IX (PpIX) accumulation in bladder cancer. Photodiagnosis Photodyn Ther 2013, 10, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Ishizuka, M.; Hagiya, Y.; Mizokami, Y.; Honda, K.; Tabata, K.; Kamachi, T.; Takahashi, K.; Abe, F.; Tanaka, T.; Nakajima, M.; Ogura, S.; Okura, I. Porphyrins in urine after administration of 5-aminolevulinic acid as a potential tumor marker. Photodiagnosis Photodyn Ther 2011, 8, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Fukuhara, H.; Karashima, T.; Inoue, K. Real-world experience with 5-aminolevulinic acid for the photodynamic diagnosis of bladder cancer: Diagnostic accuracy and safety. Photodiagnosis Photodyn Ther 2020, 32, 101999. [Google Scholar] [CrossRef]
- Yatabe, T.; Marie, S.L.; Fukuhara, H.; Karashima, T.; Inoue, K.; Yokoyama, M. 5-Aminolevulinic acid-induced severe hypotension during transurethral resection of a bladder tumor: a case report. J Anesth Clin Rep 2019, 5, 58. [Google Scholar] [CrossRef]
- Nohara, T.; Kato, Y.; Nakano, T.; Nakagawa, T.; Iwamoto, H.; Yaegashi, H.; Nakashima, K.; Iijima, M.; Kawaguchi, S.; Shigehara, K.; Izumi, K.; Kadono, Y.; Mizokami, A. Intraoperative hypotension caused by oral administration of 5-aminolevulinic acid for photodynamic diagnosis in patients with bladder cancer. Int J Urol 2019, 26, 1064–1068. [Google Scholar] [CrossRef] [PubMed]
- Yatabe, T.; Karashima, T.; Kume, M.; Kawanishi, Y.; Fukuhara, H.; Ueba, T.; Inoue, K.; Okuhara, Y.; Yokoyama, M. Identification of risk factors for post-induction hypotension in patients receiving 5-aminolevulinic acid: a single-center retrospective study. J Anesth Clin Rep 2020, 6, 35. [Google Scholar] [CrossRef] [PubMed]
- Fukuhara, H.; Nohara, T.; Nishimoto, K.; Hatakeyama, Y.; Hyodo, Y.; Okuhara, Y.; Oyama, M.; Mizokami, A.; Inoue, K.; Matsuyama, H. Japan Urological Photodynamic Society. Identification of risk factors associated with oral 5-aminolevulinic acid-induced hypotension in photodynamic diagnosis for non-muscle invasive bladder cancer: a multicenter retrospective study. BMC Cancer 2021, 21, 1223. [Google Scholar] [CrossRef] [PubMed]
- Kriegmair, M.; Baumgartner, R.; Knüchel, R.; Stepp, H.; Hofstädter, F.; Hofstetter, A. Detection of early bladder cancer by 5-aminolevulinic acid induced porphyrin fluorescence. J Urol 1996, 155, 105–109. [Google Scholar] [CrossRef] [PubMed]
- Filbeck, T.; Roessler, W.; Knuechel, R.; Straub, M.; Kiel, H.J.; Wieland, W.F. Clinical results of the transurethreal resection and evaluation of superficial bladder carcinomas by means of fluorescence diagnosis after intravesical instillation of 5-aminolevulinic acid. J Endourol 1999, 13, 117–121. [Google Scholar] [CrossRef]
- De Dominicis, C.; Liberti, M.; Perugia, G.; De Nunzio, C.; Sciobica, F.; Zuccalà, A.; Sarkozy, A.; Iori, F. Role of 5-aminolevulinic acid in the diagnosis and treatment of superficial bladder cancer: improvement in diagnostic sensitivity. Urology 2001, 57, 1059–1062. [Google Scholar] [CrossRef]
- Zaak, D.; Kriegmair, M.; Stepp, H.; Stepp, H.; Baumgartner, R.; Oberneder, R.; Schneede, P.; Corvin, S.; Frimberger, D.; Knüchel, R.; Hofstetter, A. Endoscopic detection of transitional cell carcinoma with 5-aminolevulinic acid: results of 1012 fluorescence endoscopies. Urology 2001, 57, 690–694. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Huang, H.; Zhao, Y.; Liu, H.; Luo, Y.; Sylvester, R.J.; Li, J.P.; Lam, T.B.; Lin, T.; Huang, J. Diagnostic accuracy of photodynamic diagnosis with 5-aminolevulinic acid, hexaminolevulinate and narrow band imaging for non-muscle invasive bladder cancer. J Cancer 2020, 11, 1082–1093. [Google Scholar] [CrossRef]
- Hagimoto, H.; Makita, N.; Mine, Y.; Kokubun, H.; Murata, S.; Abe, Y.; Kubota, M.; Tsutsumi, N.; Yamasaki, T.; Kawakita, M. Comparison between 5-aminolevulinic acid photodynamic diagnosis and narrow-band imaging for bladder cancer detection. BMC Urol 2021, 21, 180. [Google Scholar] [CrossRef]
- Naito, S.; Algaba, F.; Babjuk, M.; Bryan, R.T.; Sun, Y.H.; Valiquette, L.; de la Rosette, J. The Clinical Research Office of the Endourological Society (CROES) multicentre randomised trial of narrow band imaging-assisted Transurethral Resection of Bladder Tumour (TURBT) versus conventional white light imaging-assisted TURBT in primary non-muscle-invasive bladder cancer patients: trial protocol and 1-year results. Eur Urol 2016, 70, 506–515. [Google Scholar]
- Matsumoto, H.; Shiraishi, K.; Azuma, H.; Inoue, K.; Uemura, H.; Eto, M.; Ohyama, C.; Ogawa, O.; Kikuchi, E.; Kitamura, H.; Shinohara, N.; Takahashi, S.; Tsuzuki, T.; Nakagawa, M.; Narumi, Y.; Nishiyama, H.; Habuchi, T.; Hinotsu, S.; Fujii, Y.; Fujimoto, K.; Fujimoto, H.; Mizowaki, T.; Matsuyama, H. Clinical Practice Guidelines for Bladder Cancer 2019 update by the Japanese Urological Association: Summary of the revision. Int J Urol 2020, 27, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Miyake, M.; Maesaka, F.; Marugami, N.; Miyamoto, T.; Nakai, Y.; Ohnishi, S.; Gotoh, D.; Owari, T.; Hori, S.; Morizawa, Y.; Itami, Y.; Inoue, T.; Anai, S.; Torimoto, K.; Fujii, T.; Shimada, K.; Tanaka, N.; Fujimoto, K. A Potential Application of Dynamic Contrast-Enhanced Magnetic Resonance Imaging Combined with Photodynamic Diagnosis for the Detection of Bladder Carcinoma in Situ: Toward the Future ‘MRI-PDD Fusion TURBT’. Diagnostics (Basel) 2019, 9, 112. [Google Scholar] [CrossRef] [PubMed]
- Witjes, J.A.; Babjuk, M.; Gontero, P.; Jacqmin, D.; Karl, A.; Kruck, S.; Mariappan, P.; Redorta, J.P.; Stenzl, A.; Velthoven van, R.; Zaak, D. Clinical and cost effectiveness of hexaminolevulinate-guided blue-light cystoscopy: evidence review and updated expert recommendations. Eur Urol 2014, 66, 863–871. [Google Scholar] [CrossRef] [PubMed]
- Hungerhuber, E.; Stepp, H.; Kriegmair, M.; Stief, C.; Hofstetter, A.; Hartman, A.; Knuechel, R.; Karl, A.; Trischler, S.; Zaak, D. Seven years’ experience with 5-aminolevulinic acid in detection of transitional cell carcinoma of the bladder. Urology 2007, 69, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Rink, M.; Babjuk, M.; Catto, J.W.; Jichlinski, P.; Shariat, S.F.; Stenzl, A.; Stepp, H.; Zaak, D.; Witjes, J.A. Hexyl aminolevulinate-guided fluorescence cystoscopy in the diagnosis and follow-up of patients with non-muscle-invasive bladder cancer: a critical review of the current literature. Eur Urol 2013, 64, 624–638. [Google Scholar] [CrossRef] [PubMed]
- Veeratterapillay, R.; Gravestock, P.; Nambiar, A.; Gupta, A.; Aboumarzouk, O.; Rai, B.; Vale, L.; Heer, R. Time to turn on the blue lights: a systematic review and meta-analysis of photodynamic diagnosis for bladder cancer. Eur Urol Open Sci 2021, 31, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, Y.; Miyake, M.; Nishimura, N.; Nishimoto, K.; Fukuhara, H.; Kobayashi, K.; Oyama, M.; Inoue, K.; Matsuyama, H.; Fujimoto, K.; Miyake, H. Comparative assessment of disease recurrence after transurethral resection of non-muscle-invasive bladder cancer with and without a photodynamic diagnosis using 5-aminolevulinic acid: a propensity score-matching analysis. Int J Clin Oncol 2024, 29, 205–212. [Google Scholar] [CrossRef]
- Miyake, M.; Nishimura, N.; Nakahama, T.; Nishimoto, K.; Oyama, M.; Matsushita, Y.; Miyake, H.; Fukuhara, H.; Inoue, K.; Kobayashi, K.; Matsumoto, H.; Matsuyama, H.; Fujii, T.; Hirao, Y.; Fujimoto, K. Additional oncological benefit of photodynamic diagnosis with blue light cystoscopy in transurethral resection for primary non-muscle-invasive bladder cancer: A comparative study from experienced institutes. BJUI Compass 2023, 4, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, K.; Matsuyama, H.; Oka, S.; Nakamura, K.; Misumi, T.; Hiroyoshi, T.; Ito, H.; Isoyama, N.; Hirata, H.; Matsumoto, H.; Shiraishi, K. Risks and benefits of transurethral resection of the bladder tumor using photodynamic diagnosis with oral 5-aminolevulinic acid hydrochloride according to age and history of recurrence in patients with non-muscle invasive bladder cancer. Photodiagnosis Photodyn Ther 2023, 41, 103294. [Google Scholar] [CrossRef]
- Yamashita, T.; Kinoshita, H.; Sakaguchi, T.; Isomoto, H. Objective tumor distinction in 5-aminolevulinic acid-based endoscopic photodynamic diagnosis, using a spectrometer with a liquid crystal tunable filter. Ann Transl Med 2020, 8, 178. [Google Scholar] [CrossRef]
- Brandau, S.; Suttmann, H. Thirty years of BCG immunotherapy for non-muscle invasive bladder cancer: a success story with room for improvement. Biomed Pharmacother 2007, 61, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Sylvester, R.J.; van der MEIJDEN, A.P.; Lamm, D.L. Intravesical bacillus Calmette-Guerin reduces the risk of progression in patients with superficial bladder cancer: a meta-analysis of the published results of randomized clinical trials. J Urol 2002, 168, 1964–1970. [Google Scholar] [CrossRef]
- Draga, R.O.; Grimbergen, M.C.; Kok, E.T.; Jonges, T.N.; van Swol, C.F.; Bosch, J.L. Photodynamic diagnosis (5-aminolevulinic acid) of transitional cell carcinoma after bacillus Calmette-Guerin immunotherapy and mitomycin C intravesical therapy. Eur Urol 2010, 57, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, R.; Nohara, T.; Naito, R.; Kadomoto, S.; Iwamoto, H.; Yaegashi, H.; Kawaguchi, S.; Shigehara, K.; Izumi, K.; Kadono, Y.; Mizokami, A. Intravesical BCG therapy with photodynamic diagnosis-guided transurethral resection of bladder tumors improves recurrence-free survival. Photodiagnosis Photodyn Ther 2023, 42, 103574. [Google Scholar] [CrossRef] [PubMed]
- Pichler, R.; Fritz, J.; Zavadil, C.; Schäfer, G.; Culig, Z.; Brunner, A. Tumor-infiltrating immune cell subpopulations influence the oncologic outcome after intravesical Bacillus Calmette-Guérin therapy in bladder cancer. Oncotarget 2016, 7, 39916–39930. [Google Scholar] [CrossRef] [PubMed]
- Inoue, K. 5-Aminolevulinic acid-mediated photodynamic therapy for bladder cancer. Int J Urol 2017, 24, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Makino, T.; Ofude, M.; Kawahara, T.; Hori, T.; Urata, S.; Miyagi, T. Poor Prognosis With Intravesical Bacillus Calmette-Guerin History After Photodynamic Diagnosis-assisted Transurethral Resection Using 5-Aminolevulinic Acid. In Vivo 2022, 36, 2952–2959. [Google Scholar] [CrossRef] [PubMed]
- Rahman, K.M.M.; Giram, P.; Foster, B.A.; You, Y. Photodynamic Therapy for Bladder Cancers, A Focused Review. Photochem Photobiol 2023, 99, 420–436. [Google Scholar] [CrossRef]
- Zein, T.A.; Friedberg, N.; Kim, H. Bone marrow suppression after intravesical mitomycin C treatment. J Urol 1986, 136, 459–460. [Google Scholar] [CrossRef]
- Wittes, R.; Klotz, L.; Kosecka, U. Severe bacillus Calmette-Guerin cystitis responds to systemic steroids when antituberculous drugs and local steroids fail. J Urol 1999, 161, 1568–1569. [Google Scholar] [CrossRef]
- Ishizuka, M.; Abe, F.; Sano, Y.; Takahashi, K.; Inoue, K.; Nakajima, M.; Kohda, T.; Komatsu, N.; Ogura, S.; Tanaka, T. Novel development of 5-aminolevurinic acid (ALA) in cancer diagnoses and therapy. Int Immunopharmacol 2011, 11, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Kriegmair, M.; Baumgartner, R.; Lumper, W.; Waidelich, R.; Hofstetter, A. Early clinical experience with 5-aminolevulinic acid for the photodynamic therapy of superficial bladder cancer. Br J Urol 1996, 77, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Waidelich, R.; Stepp, H.; Baumgartner, R.; Weninger, E.; Hofstetter, A.; Kriegmair, M. Clinical experience with 5-aminolevulinic acid and photodynamic therapy for refractory superficial bladder cancer. J Urol 2001, 165, 1904–1907. [Google Scholar] [CrossRef] [PubMed]
- Shackley, D.C.; Briggs, C.; Gilhooley, A.; Whitehurst, C.; O’Flynn, K.J.; Betts, C.D.; Moore, J.V.; Clarke, N.W. Photodynamic therapy for superficial bladder cancer under local anaesthetic. BJU Int 2002, 89, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.P.; Steiner, H.; Stenzl, A.; Akkad, T.; Bartsch, G.; Holtl, L. Photodynamic therapy with intravesical instillation of 5-aminolevulinic acid for patients with recurrent superficial bladder cancer, a single-center study. Urology 2003, 61, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Waidelich, R.; Beyer, W.; Knüchel, R.; Stepp, H.; Baumgartner, R.; Schröder, J.; Hofstetter, A.; Kriegmair, M. Whole bladder photodynamic therapy with 5-aminolevulinic acid using a white light source. Urology 2003, 61, 332–337. [Google Scholar] [CrossRef] [PubMed]
- Skyrme, R.J.; French, A.J.; Datta, S.N.; Allman, R.; Mason, M.D.; Matthews, P.N. A phase-1 study of sequential mitomycin C and 5-aminolaevulinic acid-mediated photodynamic therapy in recurrent superficial bladder carcinoma. BJU Int 2005, 95, 1206–1210. [Google Scholar] [CrossRef] [PubMed]
- Filonenko, E.V.; Kaprin, A.D.; Alekseev, B.Y.; Apolikhin, O.I.; Slovokhodov, E.K.; Ivanova-Radkevich, V.I.; Urlova, A.N. 5-Aminolevulinic acid in intraoperative photodynamic therapy of bladder cancer (results of multicenter trial). Photodiagnosis Photodyn Ther 2016, 16, 106–109. [Google Scholar] [CrossRef]
- Yamamichi, G.; Nakata, W.; Yoshimura, A.; Tsujimura, G.; Tsujimoto, Y.; Nin, M.; Mimura, A.; Miwa, H.; Tsujihata, M. High performance of 5-aminolevulinic acid-induced fluorescent selective upper tract urinary cytology. Int J Urol 2020, 27, 213–218. [Google Scholar] [CrossRef]
Figure 1.
The correlation between pathological findings and MIBC progression in NMIBC. The CIS and pT1 UCs are the major MIBC precursors. pTis: flat urothelial CIS; pT1a: non-invasive papillary lesion; pT1: UCs with invasion of the lamina propria.
Figure 1.
The correlation between pathological findings and MIBC progression in NMIBC. The CIS and pT1 UCs are the major MIBC precursors. pTis: flat urothelial CIS; pT1a: non-invasive papillary lesion; pT1: UCs with invasion of the lamina propria.
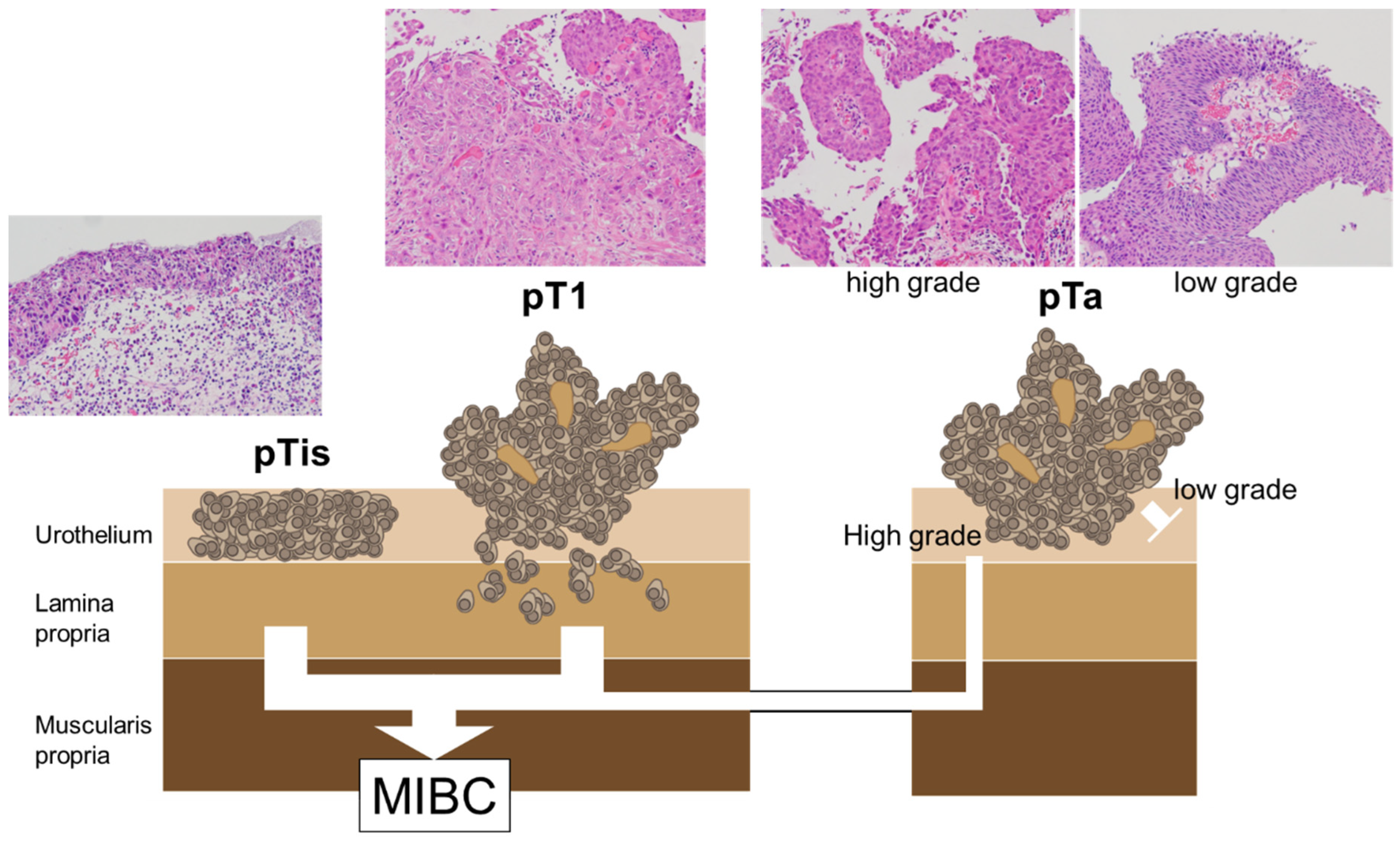
Figure 2.
The mechanisms of ALA-PDD, ALA-PDT, and ALA-PDS.
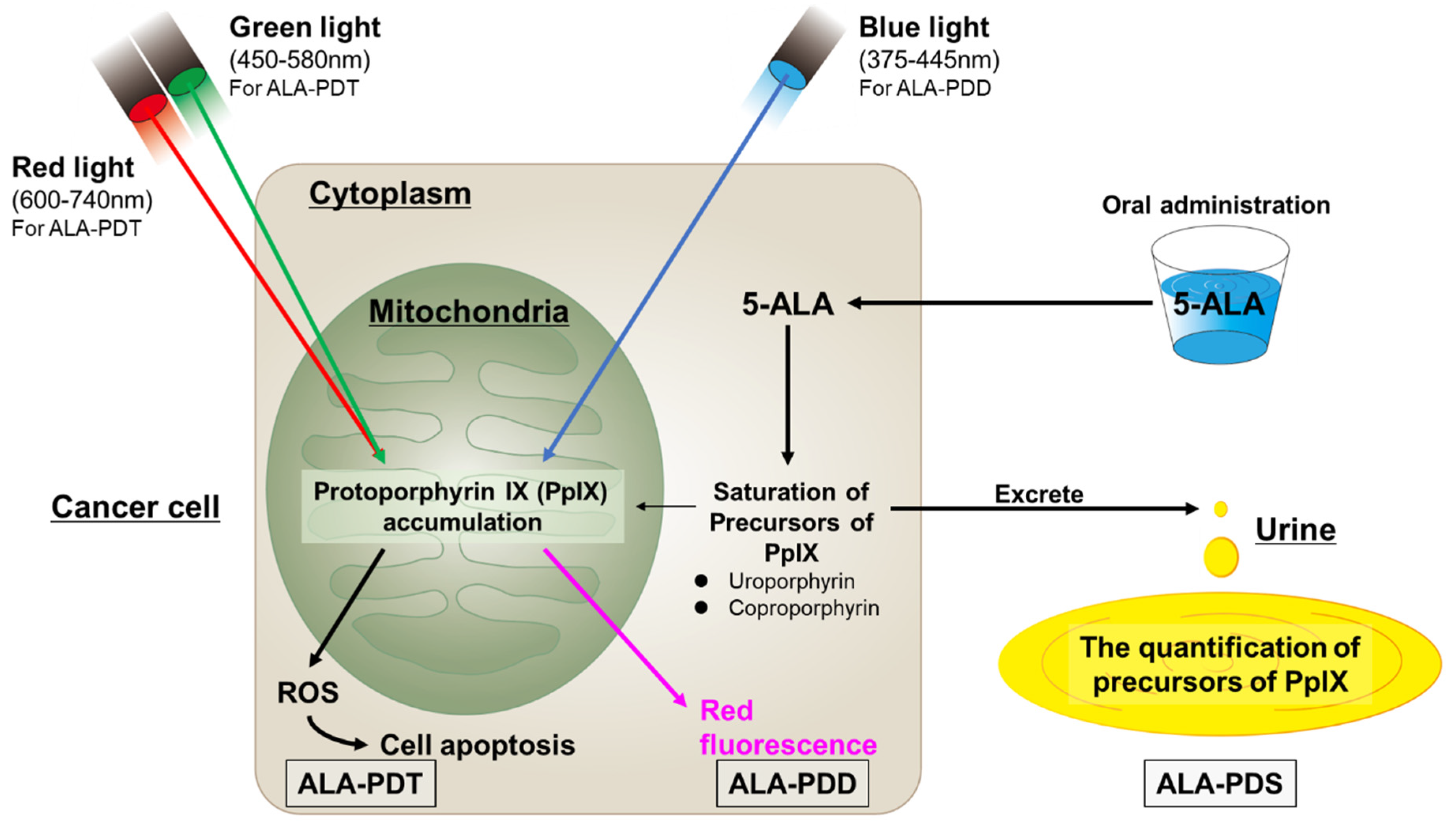
Figure 3.
Comparison between WL and 5-ALA for TURBT. PDD-assisted TURBT with 5-ALA increased the detection rate of tumors, particularly for CIS. Additionally, PDD-assisted TURBT with 5-ALA reduced the risk of disease recurrence more than WL-TURBT in patients with NMIBC.
Figure 3.
Comparison between WL and 5-ALA for TURBT. PDD-assisted TURBT with 5-ALA increased the detection rate of tumors, particularly for CIS. Additionally, PDD-assisted TURBT with 5-ALA reduced the risk of disease recurrence more than WL-TURBT in patients with NMIBC.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



