Submitted:
22 April 2024
Posted:
23 April 2024
You are already at the latest version
Abstract
The classification of kidney tumors has undergone a remarkable evolution since the early 19th century, reflecting advances in medical science and technology. This historical overview traces the development of renal tumor classification, beginning with early clinical observations and macroscopic descriptions to the integration of molecular diagnostics in contemporary classifications. The establishment of international organizations like the World Health Organization (WHO) facilitated collaboration and standardization in tumor classification, leading to refined classifications and standardized nomenclature. Advancements in histological and molecular studies, particularly genetic analyses, revolutionized the understanding of renal cell carcinomas, enabling precise categorization based on molecular characteristics. The journey from rudimentary classifications to sophisticated systems based on detailed histological, immunohistochemical, and molecular criteria underscores the continuous evolution of kidney tumor classification. This article provides a comprehensive overview of this evolution, highlighting the contributions of scholars and the impact of technological advancements on our understanding and management of kidney tumors.
Keywords:
kidney carcinoma history
1. Introduction
The history of studies and research on kidney tumors and their classification dates back to the early 19th century. The initial studies primarily focused on the clinical and macroscopic aspects of these tumors, and the terminology used by scholars was diverse, with various nomenclatures and classifications. Authors put forward several hypotheses regarding the determinism of these tumors and suggested different names. The technical means available to them for conducting their studies were limited. The pathological anatomy of renal tumors was in its infancy, and scientists who delved into it had their own perspectives and interpretations. It was only in the last decades of the 20th century and the beginning of the 21st, with the advent of new molecular studies, that the pathological anatomy of the kidney underwent a new surge. Studies and classifications of renal tumors have evolved to reach their current state.
In this historical overview, we report on the most significant studies and classifications of renal tumors that have been conducted up to the present day. We do not claim that the list of scholars and works we will mention is exhaustive, but it includes the main studies and will provide the reader with an idea of the evolution of kidney tumors classification.
2. The Precursors and Initiators of Studies and Classifications of Kidney Tumors
The first publication on renal tumor pathology was issued in 1810 when the French surgeon Miriel published his report on a malignant renal tumor [1]. However, the first classification of renal tumors was proposed in 1826 by the German professor Georg König. He based his classification primarily on the macroscopic appearance of these tumors, categorizing them as fungoid, scirrhous, steatomatous, and medullary [2].
Between 1831 and 1836, the French physician Pierre François Olive Rayer collected and studied a series of renal tumors. The results of his study were published in 1841 in the third volume of "Traité de la maladie rénale" (Treatise on Renal Disease). He classified renal tumors based on their macroscopic appearance and the symptoms presented by the patient, including latent tumors, calyceal tumors, and scirrhous tumors [3].
In 1855, the French pathologist Charles-Philippe Robin focused on the origin of renal tumors and proposed a hypothesis that these tumors result from a proliferation of epithelial cells in the renal tubules [4]. The German anatomist Heinrich Wilhelm Waldeyer, possibly unaware of Robin's work, made the same hypothesis in 1867 based on his studies of two cases [5].
In 1876, the German Rudolf Ludwig Karl Virchow published autopsy results, describing small peripheral renal tumors as lipomas, which he supposed to be metaplastic tumors [6]. The Austrian pathologist Carl Von Rokitansky suggested the possibility of a carcinomatous transformation of these tumors [7].
From 1882 to 1885, Charles Sabourin, working on various varieties of renal tumors he called renal adenomas, concluded that these adenomas were undoubtedly of epithelial nature [8].
In 1883, Paul Albert Grawitz of the Berlin Institute, inspired by observations and hypotheses proposed by pathologists in the 19th century, published a work entitled "Les lipomes du rein" ("The Lipomas of the Kidney"). Grawitz considered renal tumors to originate from remnants of the adrenal gland still present in the renal parenchyma and named them "strumæ lipomatodes aberratæ renis" to indicate their adrenal origin, distinguishing them from Virchow, who had named certain hypertrophies of the adrenal capsule "strumæ suprarenales" [9].
Twenty years after Grawitz's work, the French physicians Joaquin Albarran and Léon Imbert published "Les tumeurs du rein" ("Tumors of the Kidney") in 1903. They noted that the histological study of renal tumors did not have a distinct history, except in relation to the development of these tumors. They reported various hypotheses and interpretations from scientists during the second half of the 19th century, highlighting the divergence in appellations used. They proposed a classification subdividing renal tumors into adenomas (tubular, papillary, and clear cell), adenocarcinomas, epitheliomas (ordinary and clear cell), lipomas and pseudolipomas (lipomas and hypernephromes), sarcomas, subcapsular fibromas and fibrosarcomas, and mixed tumors [8].
In 1919, the American pathologist James Ewing published "Neoplastic Diseases," discussing tumors of various organs, including the kidney. Advances in neoplastic pathology at the time allowed him to propose a more relevant classification of renal tumors, separating them into adenomas, adenocarcinomas, and hypernephromes [10]. Since then, the classification of renal tumors has continued to evolve with multiple studies and new techniques available to pathologists.
In 1944, the American physician Meyer Melicow proposed a more detailed classification of renal tumor pathology based on architectural and cytological criteria. He classified renal tumors into clear cell carcinomas (alveolar, papillary, and tubular), granular cell carcinomas, true hypernephroma, cystadenoma or cystadenocarcinoma on a single cyst, papillary multiple carcinomas or adenomas, and carcinosarcomas [11].
3. The Creation of the World Health Organisation and Its Impact on International Cooperation and Coordination in the Study of Renal Tumors
When the United Nations included the field of health in its competencies and established the World Health Organization (WHO) in 1948, an organization specialized in the field of health, thing took a better direction towards more coordination and cooperation in various health areas. At the tenth general assembly of this organization in 1957, it was decided to form research groups consisting of ten experts each, with the designation of laboratories or reference research centers for cooperation and collaboration. The goal was to establish a classification of tumors in different organs, with the aim of standardizing the nomenclature of various tumors and their classifications.
In parallel with the research efforts launched under the auspices of the WHO, the Armed Forces Institute of Pathology (AFIP) in the United States also conducted research on cancers. In 1975, it proposed a histological classification of renal tumors, subdividing them into renal adenoma and clear cell or granular cell renal adenocarcinoma [12].
It wasn't until 1981 that the research group designated by the WHO for the development of a classification of kidney tumors, in collaboration with the American Institute of Pathology (AFIP), was able to establish and publish the classification that the WHO would adopt. This marked the first edition of the WHO classification of renal tumors. In this first edition, renal parenchymal tumors were subdivided into adenomas, renal cell carcinomas, and other renal parenchymal tumors [13].
This classification was obviously not considered final, and pathologists continued their studies, benefiting from scientific and technical advances in the medical field to refine it. In 1986, the team led by Wolfgang Carl Theones proposed a classification called the ‘’Mainz classification’’ Some pathologists of the time, particularly in Europe, adopted this Mainz classification and considered it adequate, but others criticized it, finding its classification criteria imprecise [14].
4. The Development of More Relevant Classifications of Renal Tumors Thanks to Scientific and Technological Advances in the Medical Field
The advent of new methods of molecular study, particularly genetic studies of tumors, has initiated more precise classifications of renal cell carcinomas. In 1997, a conference brought together 19 pathologists at the University of Heidelberg in Germany. Following this conference, new histological types were proposed with more precise morphological criteria and relatively specific molecular characteristics. Simultaneously, in the same year in the United States, another conference took place at the Mayo Clinic in Rochester under the auspices of the WHO in collaboration with the International Union Against Cancer (UICC) and the American Joint Committee on Cancer (AJCC). In this conference, pathologists proposed a classification similar to that of the Heidelberg conference and established the basis for TNM staging and prognostic factors for renal cell carcinomas. The similarity and agreement between the two classifications proposed by these conferences led to the development of a more relevant classification called the "Heidelberg-Rochester classification." This laid the foundation for subsequent classifications [15,16].
The following year, the expert group designated by the WHO in 1989 in Hamburg to prepare a second edition completed its work and published it in 1998. This second WHO edition did not consider the Heidelberg-Rochester classification, which only appeared in 1997, while the research group designated by the WHO had been working since 1989 [17].
Continuing its programs, the WHO assigned a group of researchers during its 2002 session in Lyon the task of preparing a third edition of the WHO classification of renal cell carcinomas. This group based its work on the Mainz and Heidelberg-Rochester classifications and, in 2004, developed the third edition, which was characterized by the integration for the first time of a category of molecular diagnosis represented by Xp translocation carcinomas [18].
Twelve years later, a fourth edition of this classification was published by the WHO in 2016. This classification subdivided renal cell carcinomas into 16 histological types based on more precise morphological, immunohistochemical, and molecular criteria.
The fifth edition was promptly published by the WHO in 2022. It includes 21 histological subtypes, with 7 belonging to the category of molecularly defined carcinomas. The diagnostic criteria have become much more detailed. This is due to the advancement of molecular studies of the various histological types, resulting in the categorization of one-third of histological types as molecular variants, with diagnosis relying on the detection of a genetic anomaly identified through various cytogenetic tests.
5. Conclusions
The first attempts at classifying kidney tumors date back to the 19th century. Since then, these classifications have evolved due to the development of available study methods in each period. Initially, the categorization of these tumors was based on clinical signs and macroscopic appearance. However, the advent of optical microscopy allowed for the development of more relevant classifications based on histological appearance and immunohistochemical profiling. The early 21st century witnessed the integration of molecular tests as a diagnostic tool in the medical field. These studies enabled the detection of certain genetic anomalies with increased specificity and considerable diagnostic value, leading to relevant classifications based on histological, immunohistochemical, and molecular criteria.
Author Contributions
Rafik BEN TAYEB : Conceptualization, Writing—original draf, Hinde EL FATEMI :Validation.
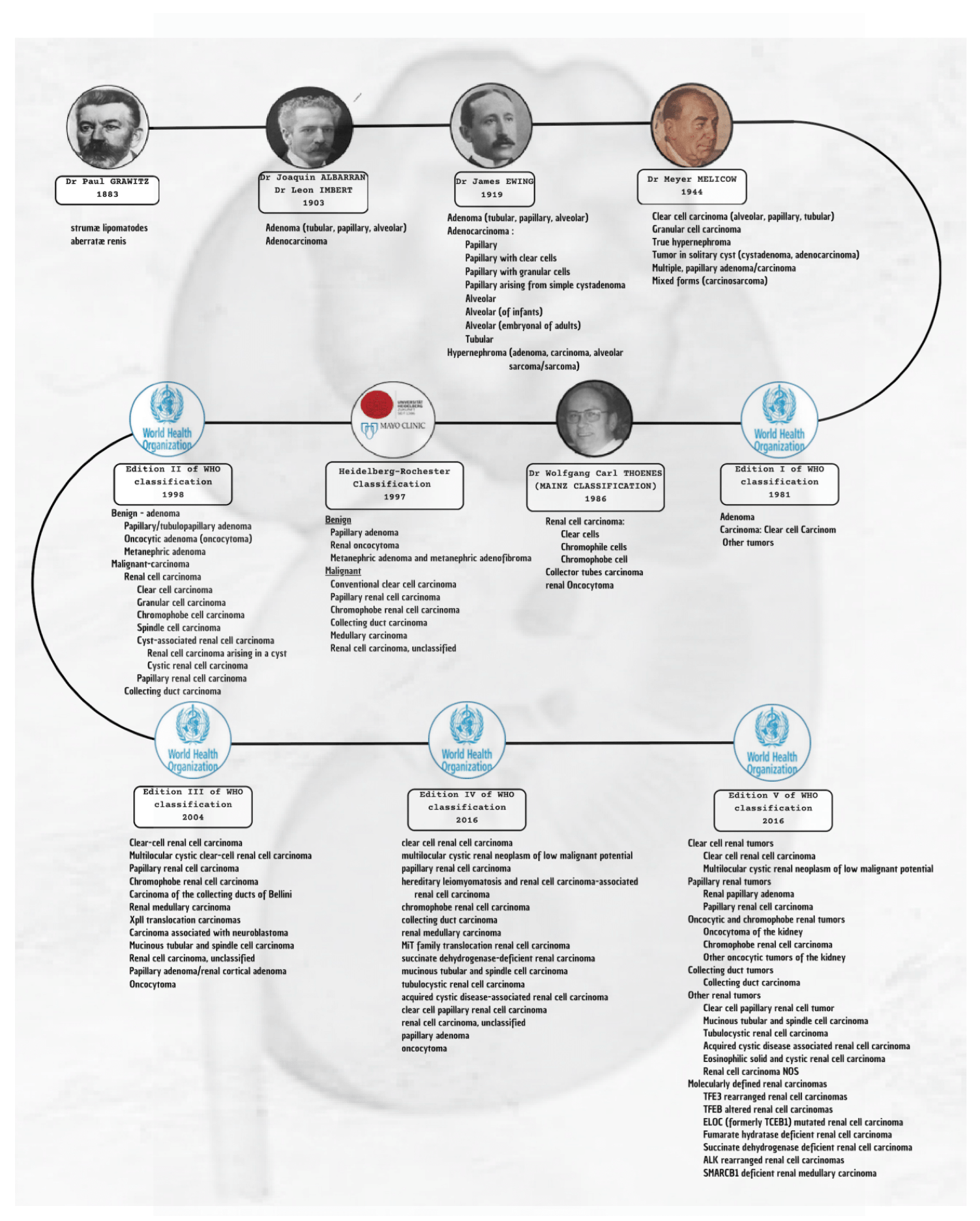
The main classifications of kidney tumors
References
- Miriel, G. Summarized thoughts on the importance of a diagnosis. Paris: 1810.
- Koënig, G. Practical treatment of diseases of the kidney as explained by case histories. Leipzig: C. Cnobloch; 1826.
- Rayer, P. Cancer of the kidney. In: Treatise on disease of the kidney and the alteration of urinary secretion. Paris; Book 3:1841. p. 675–718.
- Robin, C.P. Treatise on epitheliomas of the kidney and the thin granulated filaments from urinary tubules that are expelled with urine. Gaz d’Hop Civ et Med 1855;28:186–203.
- Waldeyer, W. The development of carcinoma. Arch Pathol Anat Physiol Klin Med 1867;41:470–523.
- Virchow, R. Ueber die Bildung von Knochencysten. Monatsschrift der Berl Akad d Wissensch. Phys-math. Cl. 1876.
- Rokitansky, C. Textbook of pathological anatomy. Braumu¨ ller: Wein, Book 3, 1861.
- Albarran J, Imbert L. Les Tumours du Rein. Paris: Masson et Cie; 1903.
- Grawitz, P. The so-called lipoma of the kidney. Arch Path Anat Physiol Klin Med 1883;93:39–63.
- Ewing, J. Neoplastic diseases. Philadelphia: WB Saunders; 1919.
- Melicow, M.M. Classification of renal neoplasms. A clinical and pathological study based on 199 cases. J Urol 1944;51:333–85. [CrossRef]
- Bennington JBB. Tumors of the kidney, renal pelvis, and ureter.
- Atlas of Tumor Pathology. Vol. 12. Washington: Armed Forces Institute of Pathology 1975.
- Mostofi FK, editor. Histological typing of kidney tumours. World Health Organization,Geneva; (International Histological Classification of Tumours No. 25), 1981.
- Thoenes W, Störkel S, Rumpelt HJ. Histopathology and classification of renal cell tumors (adenomas; oncocytomas and carcinomas). The basic cytological and histopathologicalelements and their use for diagnosis. Path Res Pract 1986;181:125–43.
- Kovacs G, Akhtar M, Beckwith BJ, et al. The Heidelberg classification of renal cell tumours.J Pathol 1997;183:131–3.
- Störkel S, Eble JN, Adlakha K, et al. Classification of renal cell carcinoma. Cancer 1997;80:987–9.
- Mostofi FK, Davis CJ, editors. Histological typing of kidney tumours. 2nd edition. Geneva (Switzerland): World Health Organization; 1998.
- Eble JN, Sauter G, Epstein JI, et al, editors. Pathology and genetics of tumours of the urinary system and male genital organs. World Health Organization Classification of Tumours.Lyon (France): IARC Press; 2004.
- Moch H, Humphrey PA, Ulbright TM, Reuter VE. WHO Classification of Tumours of the Urinary System and Male Genital Organs. Lyon (France): IARC Press 2016.
- WHO Classification of Tumours, Urinary and Male Genital Tumours. Lyon (France): IARC Press 2022.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



