
Submitted:
22 April 2024
Posted:
23 April 2024
You are already at the latest version
Abstract
Human papillomavirus (HPV) can potentially compromise both unassisted conception and success rates with assisted reproductive technology (ART). We aimed to evaluate the rates of HPV vaccination among women presenting for fertility care. This was a prospective study analyzing a self-reported intake form completed by all new patients presenting to a fertility clinic. The primary outcome was HPV vaccination status. Among the 523 new patients included in this study 172 (32.9%) were fully vaccinated, 237 (45.3%) were unvaccinated, and 95 (18.2%) patients didn’t respond. There was a significant age difference between fully vaccinated patients (33.1 years) compared to unvaccinated patients (37.4 years) p<0.001 and a significant difference in gravidity between fully vaccinated patients (average 0.65) and unvaccinated patients (average 1.11) p=0.0005. No significant association was found between HPV vaccination status and history of abnormal Pap smears or relationship status (single vs. married). Less than half of patients presenting to our fertility center were vaccinated against HPV, despite being eligible to receive the vaccine. Younger patients with lower gravidity were more likely to be vaccinated against HPV than older patients with higher gravidity. Reproductive Endocrinologists have the opportunity to recommend HPV vaccination for eligible patients presenting for fertility care.
Keywords:
Human papillomavirus (HPV)
; vaccination
; infertility
1. Introduction
Human papillomavirus (HPV) can potentially compromise both unassisted conception and success rates with assisted reproductive technology (ART) [1]. Despite the introduction of the HPV vaccine in the US in 2006, many eligible patients remain unvaccinated. HPV is the most common sexually transmitted infection impacting 43 million people per the Centers for Disease Control and Prevention (CDC) estimates in 2018 with an increased risk of infection with higher number of sexual partners [2]. Certain strains have known adverse outcomes such as genital warts, cervical, vulvar, vaginal, penile, anal and oropharyngeal cancer [3,4]. Additional impacts of this virus remain largely unknown. HPV vaccination can prevent the spread of HPV, development of cervical cancer, genital warts, and oro-pharyngeal cancers [2,5]. The CDC recommends HPV vaccination for all 11–26-year-olds, with an option for vaccination through age 45. The vaccination is ideally recommended for both boys and girls between the ages of 9-11 years old prior to the onset of sexual activity. Very few patients are ineligible for the HPV vaccine. Those who have a severe allergy to any ingredient in the HPV vaccine or previous doses of the HPV vaccine, patients with an allergy to yeast, those currently pregnant, or people with severe illness should not receive the vaccine [2].
In 2006, the quadrivalent HPV vaccine (Gardasil 4) was approved for use in young females and protects against four strains including HPV 6, 11, 16, and 18. Next, in 2014, the 9-valent HPV vaccination (Gardasil 9) was approved and covers high risk strains of HPV that cause cancer as well as low risk strains that lead to warts (Table 1). Those nine strains include HPV 6, 11, 16, 18, 31, 33, 45, 52, and 58. The HPV vaccines have had such high efficacy and success rates at preventing HPV infection that the CDC guidelines continued to expand to include recommendations to vaccinate boys as well as include larger age ranges to capture even more people [6]. The ultimate goal is to eliminate cervical cancer globally and the preventable sequela of HPV infection via vaccinating the majority of the population.
Although the HPV vaccination was introduced in 2006, over half of all adolescents have not completed the vaccination series [6]. This low vaccination rate may be due to inadequate counseling by providers, lack of physician recommendation, discomfort discussing sexual intercourse with patients, uneducated parents, lack of state mandates, misconception that the HPV vaccination is only for sexually active patients, concern for social stigma, etc. More recent gaps in care may be further explained by the Coronavirus (COVID-19) pandemic. Some routine health maintenance visits were skipped as a result of nationwide healthcare shutdowns and growing vaccination hesitancy during this time.
The United States of America has worked towards expanding HPV coverage rates since the introduction of the vaccination in 2006. CDC estimates in 2022 report that 76% of adolescents between ages 13 and 17 in the United States of America have received at least one dose of the HPV vaccination and that approximately 62.6% of those adolescents were fully vaccinated against HPV. Interestingly, coverage was found to be higher amongst those with Medicaid insurance rather than those with private health insurance [7]. Additionally, HPV vaccination rates in the United States of America vary widely among different states due to variations in state laws and local initiatives. Some studies report that states with the lowest rates in HPV vaccination are conservative and considered to be very religious such as Wyoming, Mississippi, South Carolina, Utah and Texas. In contrast, Rhode Island and the District of Columbia had the highest HPV vaccination rates. States with policies involving sex education and an HPV vaccination mandates had higher rates of completion too [8]. Clearly, regional factors can influence the success of HPV vaccination coverage rates within the United States of America and attempts to identify these aspects can help mitigate additional gaps in care moving forward.
Efforts to promote HPV vaccination have increased in the United States of America as well as on a global scale since the introduction of the vaccine and the establishment of CDC guidelines. In 2020, the World Health Organization (WHO) embraced a global initiative to eliminate cervical cancer worldwide by striving towards 90% of all girls being fully vaccinated by age 15 by the year 2030, expanding the goal rates of successful screening for cervical cancer, and increasing the completion of prompt treatment of both pre-invasive lesions and invasive cancer [9]. Recent data suggests that only 15% of girls in the goal age range are fully vaccinated against HPV globally [10]. Therefore, additional interventions are necessary in order to meet this new target and address this public health concern. High income countries like the United States of America and Europe have had the greatest success in HPV vaccination rates to date, while low- and middle-income countries have had lower overall vaccination rates partially due to limited access to HPV vaccination [10]. Strategies targeting improved vaccination rates for individual patients involve educating parents, young adults, and providers, while widespread interventions include policy changes, school mandates, improved access to care, enacting mandatory health insurance coverage, reduced health care disparities, and ensuring the most populous countries are specifically highlighted first [11]. Recent advances also emphasize the need for gender neutral HPV vaccination programs by reducing HPV transmission from men, decreasing misinformation and stigma surrounding vaccination, and aiming towards gender equity [12]. These approaches strive towards the same end result in advancing the health of the global population and ensuring fewer people are impacted by the largely preventable sequelae of HPV infection.
Sexually transmitted infections (STIs) including Chlamydia trachomatis, Neisseria gonorrhoeae, Syphilis, Human immunodeficiency virus (HIV) and Herpes simplex virus (HSV) have been proven to cause impairments in fertility and in some cases, infertility. Numerous studies have been conducted to analyze the impact of HPV on fertility for both female and male patients. These studies highlight the adverse effects of HPV including abnormal semen characteristics, poor embryo development, increased rates of spontaneous abortion, and lower pregnancy success rates [13,14,15]. Moreover, HPV infection may play a role in tubal damage [16]. As a result, the American Society for Reproductive Medicine (ASRM) currently recommends that the HPV vaccine be offered to women seeking fertility care. While the HPV vaccine is not recommended during pregnancy, there is no evidence that the vaccine is harmful if given. In addition, no intervention is needed for women who inadvertently receive the vaccine while pregnant [17]. With regards to men, studies suggest that HPV vaccination decreases the presence of HPV infected semen and improves some sperm parameters. Therefore, HPV vaccination among male partners may improve fertility [18]. As with many other sexually transmitted infections, current data emphasizes the harmful impacts of HPV infection on fertility.
Recent evidence suggests that an HPV infection can have detrimental effects on pregnancy as well. HPV can increase apoptosis and thus reduce endometrial implantation and lead to an increased risk of miscarriage. Vertical transmission of HPV during pregnancy may be involved in the pathophysiology of preterm rupture of membranes and spontaneous preterm birth [1,13,19,20,21]. Studies site a reduction in adverse pregnancy outcomes in cohorts of women offered the HPV vaccine [22]. The HPV vaccination is safe and effective, and research has shown that there is no evidence of induced infertility among women who have received the vaccine [23]. Moreover, data suggests that HPV vaccination can also increase pregnancy rates. One study found that HPV vaccination was positively associated with fecundability among women with a history of sexually transmitted infections [24]. As a result, HPV vaccination in adolescents and young women is increasingly important for reproductive health due to its multiple proposed benefits including a potential increase in pregnancy rates for those struggling with infertility and a reduced rate of poor outcomes for those who successfully become pregnant [25].
Previous studies have highlighted the lack of knowledge about HPV vaccination among patients presenting to Reproductive Endocrinology and Infertility physicians [26]. This presents an opportunity for physicians to discuss HPV vaccination with patients prior to conception, improve their health, and possibly increase their chances of becoming pregnant. As a result, at our fertility center, the new patient intake form was amended in October 2020 to include questions regarding HPV vaccination status in order to evaluate the rates of HPV vaccination among women presenting for fertility care and improve patient education for those who have not received the vaccine.
2. Materials and Methods
2.1. Study Design
This was a Northwell Health Institutional Review Board approved, prospective study analyzing a self-reported intake form completed by all new patients presenting to a Reproductive Endocrinology and Infertility clinic from January – December 2021 at a single academic institution in New York. Patients were required to complete this new patient intake form prior to their initial appointment to establish care with a Reproductive Endocrinology and Infertility physician at this center. Afterwards, it was reviewed with the physician upon evaluation, utilized for treatment plan recommendations, and then uploaded to their chart in the electronic medical record for future reference. The data for the study were extracted from the electronic medical record.
All new patients during the study period were identified from the electronic medical record and included in the study. Exclusion criteria were patients that did not have a self-reported intake form associated with their electronic charts either due to failure to complete the form or an error with uploading the form to the patient’s chart.
2.2. Outcomes
The primary outcome of this study was the patient’s self-reported HPV vaccination status including fully vaccinated, partially vaccinated, unsure if vaccinated, unvaccinated, and those who left the response blank failing to answer the question. Additional patient specific variables were also collected at the time of the new patient visit including patient age, gravidity, history of abnormal Pap smears and relationship status (single or married) at the time the self-reported intake form was completed.
2.3. Statistical Analysis
T-test and chi squared analyses were utilized to compare age, gravidity, relationship status (single or married), and history of abnormal Pap smear between fully vaccinated and unvaccinated patients with p<0.05 defining statistical significance. All collected information was anonymized and deidentified prior to analysis.
3. Results
During the year long study period, 528 new fertility patients were seen in the office, of which 5 were excluded from the study for missing intake forms in their electronic medical record (Figure 1). Among the 523 eligible patients, 172 (32.9%) were fully vaccinated against HPV, 10 (1.9%) were partially vaccinated, 237 (45.3%) were unvaccinated, 9 (1.7%) were unsure if they received the vaccine, and 95 (18.2%) patients abstained from answering this question (Figure 2).
There was a statistically significant age difference between fully vaccinated patients (33.1 years) compared to unvaccinated patients (37.4 years) p<0.001 and a statistically significant difference in gravidity between fully vaccinated patients (average 0.65) compared to unvaccinated patients (average 1.11) p=0.0005 (Figure 3). However, no significant association was found between HPV vaccination status and history of abnormal Pap smears or relationship status (single vs. married) (Table 2).
4. Discussion
Ensuring that patients are up to date with all recommended vaccinations is part of the comprehensive pre-conception evaluation. For example, immunity against measles, mumps, rubella and varicella are all screened for by Obstetricians and Gynecologists prior to pregnancy and patients are offered vaccinations if they are non-immune. Furthermore, during pregnancy, vaccinations such as Tetanus, Diptheria, Pertuussis (TDAP), Influenza, COVID-19, and Respiratory Syncytial Virus (RSV) are recommended by Obstetricians, Gynecologists, midwives, family medicine physicians, and all other healthcare providers. Similarly, Reproductive Endocrinology and Infertility physicians ensure that their patients are up to date with other basic age-appropriate screening measures such as Pap smears, mammograms, and colonoscopies throughout their routine evaluations. These practices ensure that the patient has optimal health with all recommended immunizations prior to conception for both the patient’s own health and the well-being of the patient’s future children. Consultation with a Reproductive Endocrinology and Infertility physician provides a unique opportunity to address HPV vaccination status as well and to educate patients regarding the benefits to both themselves and their future offspring if applicable.
As demonstrated in this study, there is an overall low HPV vaccination rate in this population with the majority of patients being unvaccinated against HPV. We found an association between age and vaccination status, with younger patients more likely to be vaccinated against HPV. Similarly, this study revealed an association between gravidity and vaccination status, with patients with lower gravidity more likely to be vaccinated against HPV. Although patients with lower gravidity had higher vaccination rates, this relationship may be explained by the younger age in this group. Recent advances targeting vaccinating women, especially adolescents and young adults could justify the difference in vaccination rates by age seen in this study. Whether patients remain unvaccinated due to the recent introduction of the vaccine, the fact that they haven’t been offered the vaccine in the past, or if there is an alternative reason remains uncertain.
Results of our study found no significant association between patient’s HPV vaccination status and their history of abnormal Pap smears. Due to the relatively recent introduction of the HPV vaccination and age range of patients included in this study, perhaps some patients received the HPV vaccination after receiving results of an abnormal Pap smear. Future studies including the dates that patients had abnormal Pap smears and the dates they received the HPV vaccination, if applicable, would help determine this timeline. More research evaluating patients at many points in time with larger patient populations encompassing multiple geographic locations are warranted to investigate these findings further.
Interestingly, current studies reveal that HPV vaccination can continue to offer benefits for patients regardless of positive HPV infection status. Gynecologic oncologists report that adjuvant HPV vaccination in the setting of surgical excision of cervical intraepithelial neoplasm (CIN) 2 or greater is associated with a reduced risk of recurrent cervical dysplasia overall, recurrent CIN, CIN 2, vulvar intraepithelial neoplasia (VIN) and genital warts, especially for the most oncogenic strains HPV 16 and 18. Proposed mechanisms for the efficacy of adjuvant vaccination include one hypothesis that surgical removal of the primary lesion disrupts the local inflammatory environment and creates a new immune background of the mucosa that is receptive to HPV vaccination. Another hypothesis is that HPV vaccination will protect the patient against acquiring additional strains of HPV following the procedure and can offer cross protection against other HPV strains [27,28]. Therefore, HPV vaccination should be considered in all patients with HPV infection and for those patients undergoing surgical treatment for CIN. Further research is necessary to determine whether adjuvant HPV vaccination can benefit patients prior to conception by improving fertility and birth outcomes in a similar fashion.
Researchers have sought estimates to determine the frequency of HPV infection in the male population as well. Recent data from meta-analyses and systematic reviews cite the prevalence of HPV infection in men are as high as one in three people, while approximately one in five men are infected with at least one high risk HPV subtype [29]. Although the majority of HPV infections involving men are asymptomatic, clinical manifestations may include anogenital warts, and penile, anal and oropharyngeal cancers [30]. Not only does HPV infection negatively affect men, it has significant repercussions for women. HPV infections in the male population lead to continued transmission of the infection via sexual activity. Reducing the rates of genital HPV infection in men will undoubtedly benefit both genders.
HPV vaccination status of male partners is also of concern for couples seeking fertility treatment due to a possible association between HPV and male infertility cited in numerous studies [31,32,33,34]. Other chronic viral infections such as HIV, Hepatitis B virus (HBV), Hepatitis C virus (HVC) and HSV have the ability to infect sperm and increase the risk of male infertility [16,35]. Studies suggest HPV negatively impacts sperm parameters too including sperm count, vitality, motility, and morphology. The virus can alter the composition of semen fluid including pH, semen viscosity, leukocyte number, DNA fragmentation, and anti-sperm antibodies contributing to male infertility [36,37,38,39,40,41,42]. These findings may be consistent with resultant prostate disturbances indicative of glandular dysfunction in those infected with HPV [43]. Similarly, testicular biopsies in men with azoospermia have located HPV DNA sequences in Leydig and Sertoli cells [44]. These data suggest that HPV infection negatively impacts male fertility via a multitude of pathways and as a result, HPV vaccination may have the potential to improve male fertility.
Conventional semen washing procedures for assisted reproductive technology rarely eliminates HPV, which can negatively impact fertility, fetal development, and lead to early miscarriage [45,46,47]. Furthermore, patients with HPV semen infection may benefit from counseling for prophylactic vaccination prior to proceeding with artificial insemination and in vitro fertilization (IVF) as it has been shown to reduce the prevalence of HPV semen infection and increase viral clearance [48]. Adjuvant HPV vaccination is associated with higher rates of HPV clearance in semen, increased rates of natural pregnancies and more live births [18]. Additional studies are necessary to determine whether these findings are clinically significant and whether HPV infection is a risk factor for male infertility. All health care providers should continue to offer HPV vaccination to male partners per CDC guidelines.
Initiatives across the United States of America and among many countries around the world have focused on developing strategies to increase vaccination rates. One common approach has concentrated on advocacy for the establishment of gender neutral HPV vaccination programs. Highlighting the importance of male vaccination is crucial because of the countless benefits of vaccinating men against HPV in addition to women. Benefits of gender neutral HPV vaccination programs encompass public health implications such as achieving herd immunity from HPV infection and thus, exponentially improving the overall impact of vaccination efforts. Many studies in various geographic locations have evaluated this process and determined that gender neutral HPV vaccination programs are cost effective. In addition, they avoid gender discrimination and promote equity in access to preventative health services. Men who have sex with men are at a higher risk of obtaining sexually transmitted infections and would benefit from higher HPV vaccination rates as well. Research analyzing the significance of gender neutral HPV vaccination exists for countries such as Africa, Spain, the United Kingdom, Netherlands, Japan, Belgium, Germany, Hong Kong, among many others [49,50,51,52,53,54,55,56]. Vaccination of both men and women against HPV has gained popularity on a global scale over the past couple of years and has the potential to significantly decrease HPV infection rates.
This study design has some inherent weaknesses. Limitations of the study include a small sample size of patients, short study time period, the inclusion of a single institution, lack of information about patient education level and dates of abnormal Pap smears and/or HPV vaccination. Although 99% of patients in this study completed the new patient intake form, only 81.8% of patients answered the specific questions regarding HPV vaccination status. Almost one out of five patients did not answer these questions, which may have impacted study results. Also, the 5 missing new patient intake forms could have been attributable to the failure of patients to complete the new patient intake form or healthcare providers ineffectively uploading it to the patient’s electronic medical record. The low response rate specifically to questions regarding HPV vaccination rate may be due to lack of understanding the question, inadequate knowledge surrounding HPV vaccination, and/or unfamiliarity with the relevance of HPV vaccination as it pertains to the patient’s fertility journey. The contrast in response rate between overall survey completion and questions specific to HPV vaccination highlights the need to discuss HPV vaccination further with patients and the role for continued patient education regarding its importance.
Another disadvantage of this study is the fact that it assesses patients at a single point in time rather than a longitudinal fashion. Similarly, the study takes place at a sole clinic in one specific geographic region. Therefore, additional studies are required to determine whether this study is applicable to different patient populations in alternate geographic regions. Another possible drawback to this study is the lack of information regarding patient education level since higher HPV vaccination rates have been linked to increased education efforts [57]. Finally, the lack of information about the dates that patients had an abnormal Pap smear and/or dates that the patient’s received the HPV vaccination make the results difficult to interpret in regard to the efficacy of the vaccine at preventing abnormal Pap smears in this population. Further research is warranted to address these study limitations to better evaluate HPV vaccination status among fertility patients.
The impacts of HPV infection extend across multiple organs, impact both men and women of all races, ethnicities, socioeconomic status, geographic locations, and have diverse negative outcomes associated. The HPV vaccination has been shown to significantly decrease the morbidity of HPV infection and prevent many sequelae from occurring in the first place. Thus, efforts to increase global vaccination rates are necessary and remain a major public health mission. While current practices rely largely on pediatricians and primary care physicians to offer vaccinations and therefore raise HPV vaccination rates, this study highlights the role of specialty physicians, such as Reproductive Endocrinology and Infertility physicians, in advocating for patients to be up to date with vaccines, educating patients about HPV, and offering vaccines to those eligible. Broadening the responsibility of vaccinating patients to diverse doctors in different specialties ensures that a wide range of patients have access to information and thus, improved preventative care. With additional healthcare providers motivated to reduce HPV infection, HPV vaccination rates have the potential to meet the desired goal set by the World Health Organization.
5. Conclusions
During the study period less than half of the patients presenting to our fertility center were vaccinated against HPV, despite being eligible to receive the vaccine. Younger patients with lower gravidity were more likely to be vaccinated against HPV than older patients with higher gravidity. Since the most common strains of HPV are largely preventable with vaccination, patients and their partners may be more inclined to become vaccinated as well as vaccinate their children with effective counseling by physicians. Reproductive Endocrinology and Infertility physicians have the opportunity to recommend HPV vaccination for eligible patients presenting for fertility care. More research in this topic would be beneficial to women and men seeking fertility care.
Author Contributions
Conceptualization, M.T., S.R.B., R.H.G., G.L.G., and C.M.; methodology, M.T., S.R.B., R.H.G., and C.M.; formal analysis, M.T..; investigation, M.T. and E.B.; resources, M.T. and E.B.; data curation, M.T. and E.B.; writing—original draft preparation, M.T.; writing—review and editing, A.K., S.R.B., R.H.G., G.L.G., and C.M.; methodology, M.T., S.R.B., R.H.G., and C.M.; supervision, R.H.G., G.L.G., and C.M.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review of Northwell Health (IRB# 23-0224 on April 4th, 2023).
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Acknowledgments
The authors thank the doctors, nurses, and patients for their contributions.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Pereira, N., Kucharczyk, K. M., Estes, J. L., Gerber, R. S., Lekovich, J. P., Elias, R. T., & Spandorfer, S. D. (2015). Human papillomavirus infection, infertility, and assisted reproductive outcomes. Journal of pathogens, 2015. [CrossRef]
- Centers for Disease Control and Prevention. (2022). Genital HPV Infection–Basic Fact Sheet.
- Moody, C. A., & Laimins, L. A. (2010). Human papillomavirus oncoproteins: Pathways to transformation. Nature Reviews Cancer, 10(8), 550-560. [CrossRef]
- Crosbie, E. J., Einstein, M. H., Franceschi, S., & Kitchener, H. C. (2013). Human papillomavirus and cervical cancer. The Lancet, 382(9895), 889-899. [CrossRef]
- Centers for Disease Control and Prevention (CDC. (2012). Human papillomavirus-associated cancers-United States, 2004-2008. MMWR: Morbidity & Mortality Weekly Report, 61(15).
- Harper, D.M. and DeMars, L.R., 2017. HPV vaccines–a review of the first decade. Gynecologic oncology, 146(1), pp.196-204. [CrossRef]
- Pingali, C. (2023). Vaccination coverage among adolescents aged 13–17 years—National immunization survey–teen, United States, 2022. MMWR. Morbidity and Mortality Weekly Report, 72. [CrossRef]
- Dilley, S., Miller, K. M., & Huh, W. K. (2020). Human papillomavirus vaccination: Ongoing challenges and future directions. Gynecologic oncology, 156(2), 498-502. [CrossRef]
- World Health Organization. (2020). Global strategy to accelerate the elimination of cervical cancer as a public health problem. World Health Organization.
- Bruni, L., Saura-Lázaro, A., Montoliu, A., Brotons, M., Alemany, L., Diallo, M. S., ... & Bloem, P. (2021). HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010–2019. Preventive medicine, 144, 106399. [CrossRef]
- Escoffery, C., Petagna, C., Agnone, C., Perez, S., Saber, L. B., Ryan, G., ... & Fernandez, M. E. (2023). A systematic review of interventions to promote HPV vaccination globally. BMC Public Health, 23(1), 1262. [CrossRef]
- Dykens, J. A., Peterson, C. E., Holt, H. K., & Harper, D. M. (2023). Gender neutral HPV vaccination programs: Reconsidering policies to expand cancer prevention globally. Frontiers in Public Health, 11, 1067299. [CrossRef]
- Isaguliants, M., Krasnyak, S., Smirnova, O., Colonna, V., Apolikhin, O., & Buonaguro, F. M. (2021). Genetic instability and anti-HPV immune response as drivers of infertility associated with HPV infection. Infectious Agents and Cancer, 16(1), 1-18. [CrossRef]
- Souho, T., Benlemlih, M., & Bennani, B. (2015). Human papillomavirus infection and fertility alteration: A systematic review. PLoS ONE, 10(5), e0126936. [CrossRef]
- Zacharis, K., Messini, C. I., Anifandis, G., Koukoulis, G., Satra, M., & Daponte, A. (2018). Human papilloma virus (HPV) and fertilization: A mini review. Medicina, 54(4), 50. [CrossRef]
- Farsimadan, M., & Motamedifar, M. (2021). The effects of human immunodeficiency virus, human papillomavirus, herpes simplex virus-1 and-2, human herpesvirus-6 and-8, cytomegalovirus, and hepatitis B and C virus on female fertility and pregnancy. British Journal of Biomedical Science, 78(1), 1-11. [CrossRef]
- Practice Committee of the American Society for Reproductive Medicine. (2018). Current recommendations for vaccines for female infertility patients: A committee opinion. Fertility and Sterility, 110(5), 838-841. [CrossRef]
- Garolla, A., De Toni, L., Bottacin, A., Valente, U., De Rocco Ponce, M., Di Nisio, A., & Foresta, C. (2018). Human Papillomavirus Prophylactic Vaccination improves reproductive outcome in infertile patients with HPV semen infection: A retrospective study. Scientific reports, 8(1), 1-9. [CrossRef]
- Gomez, L. M., Ma, Y., Ho, C., McGrath, C. M., Nelson, D. B., & Parry, S. (2008). Placental infection with human papillomavirus is associated with spontaneous preterm delivery. Human reproduction, 23(3), 709-715. [CrossRef]
- Huang, Q. T., Zhong, M., Gao, Y. F., Huang, L. P., Huang, Q., Wang, W., ... & Yu, Y. H. (2014). Can HPV vaccine have other health benefits more than cancer prevention? A systematic review of association between cervical HPV infection and preterm birth. Journal of Clinical Virology, 61(3), 321-328. [CrossRef]
- Bonde, U., Joergensen, J. S., Mogensen, O., & Lamont, R. F. (2014). The potential role of HPV vaccination in the prevention of infectious complications of pregnancy. Expert Review of Vaccines, 13(11), 1307-1316. [CrossRef]
- Yuill, S., Egger, S., Smith, M., Velentzis, L., Wrede, C. D., Bateson, D., & Canfell, K. (2020). Has human papillomavirus (HPV) vaccination prevented adverse pregnancy outcomes? Population-level analysis after 8 years of a national HPV vaccination program in Australia. The Journal of infectious diseases, 222(3), 499-508. [CrossRef]
- Schmuhl, Nicholas B.; et al. "No association between HPV vaccination and infertility in US females 18–33 years old." Vaccine 38.24 (2020): 4038-4043. [CrossRef]
- McInerney, K. A., Hatch, E. E., Wesselink, A. K., Mikkelsen, E. M., Rothman, K. J., Perkins, R. B., & Wise, L. A. (2017). The effect of vaccination against human papillomavirus on fecundability. Paediatric and perinatal epidemiology, 31(6), 531-536. [CrossRef]
- Ciavattini, A., Marconi, C., Giannella, L., Delli Carpini, G., Sopracordevole, F., & Di Giuseppe, J. (2021). The Impact of 9-Valent HPV Vaccination on Couple Infertility Prevention: A Comprehensive Review. Frontiers in Medicine, 1332. [CrossRef]
- Estevez, S. L., Tarrash, M., Brownridge, S. R., Goldman, R. H., & Mullin, C. (2021). HPV Vaccination rate amongst women presenting for fertility care. Fertility and Sterility, 116(3), e404. [CrossRef]
- Lichter, K., Krause, D., Xu, J., Tsai, S. H. L., Hage, C., Weston, E., ... & Levinson, K. (2020). Adjuvant human papillomavirus vaccine to reduce recurrent cervical dysplasia in unvaccinated women: A systematic review and meta-analysis. Obstetrics & Gynecology, 135(5), 1070-1083. [CrossRef]
- Di Donato, V., Caruso, G., Petrillo, M., Kontopantelis, E., Palaia, I., Perniola, G., ... & Bogani, G. (2021). Adjuvant HPV vaccination to prevent recurrent cervical dysplasia after surgical treatment: A meta-analysis. Vaccines, 9(5), 410. [CrossRef]
- Bruni, L., Albero, G., Rowley, J., Alemany, L., Arbyn, M., Giuliano, A. R., ... & Taylor, M. (2023). Global and regional estimates of genital human papillomavirus prevalence among men: A systematic review and meta-analysis. The Lancet Global Health, 11(9), e1345-e1362. [CrossRef]
- Giuliano, A. R., Anic, G., & Nyitray, A. G. (2010). Epidemiology and pathology of HPV disease in males. Gynecologic oncology, 117(2), S15-S19. [CrossRef]
- Lyu, Z., Feng, X., Li, N., Zhao, W., Wei, L., Chen, Y., ... & Dai, M. (2017). Human papillomavirus in semen and the risk for male infertility: A systematic review and meta-analysis. BMC infectious diseases, 17(1), 1-9. [CrossRef]
- Xiong, Y. Q., Chen, Y. X., Cheng, M. J., He, W. Q., & Chen, Q. (2018). The risk of human papillomavirus infection for male fertility abnormality: A meta-analysis. Asian journal of andrology, 20(5), 493. [CrossRef]
- Moghimi, M., Zabihi-Mahmoodabadi, S., Kheirkhah-Vakilabad, A., & Kargar, Z. (2019). Significant correlation between high-risk HPV DNA in semen and impairment of sperm quality in infertile men. International Journal of Fertility & Sterility, 12(4), 306. [CrossRef]
- Garolla, A., Engl, B., Pizzol, D., Ghezzi, M., Bertoldo, A., Bottacin, A., ... & Foresta, C. (2016). Spontaneous fertility and in vitro fertilization outcome: New evidence of human papillomavirus sperm infection. Fertility and Sterility, 105(1), 65-72. [CrossRef]
- Garolla, A., Pizzol, D., Bertoldo, A., Menegazzo, M., Barzon, L., & Foresta, C. (2013). Sperm viral infection and male infertility: Focus on HBV, HCV, HIV, HPV, HSV, HCMV, and AAV. Journal of reproductive immunology, 100(1), 20-29. [CrossRef]
- Yang, Y., Jia, C. W., Ma, Y. M., Zhou, L. Y., & Wang, S. Y. (2013). Correlation between HPV sperm infection and male infertility. Asian journal of andrology, 15(4), 529. [CrossRef]
- Foresta, C., Noventa, M., De Toni, L., Gizzo, S., & Garolla, A. (2015). HPV-DNA sperm infection and infertility: From a systematic literature review to a possible clinical management proposal. Andrology, 3(2), 163-173. [CrossRef]
- Foresta, C., Pizzol, D., Moretti, A., Barzon, L., Palù, G., & Garolla, A. (2010). Clinical and prognostic significance of human papillomavirus DNA in the sperm or exfoliated cells of infertile patients and subjects with risk factors. Fertility and Sterility, 94(5), 1723-1727. [CrossRef]
- Weinberg, M., Nahshon, C. S. S., Feferkorn, I., & Bornstein, J. (2020). Evaluation of human papilloma virus in semen as a risk factor for low sperm quality and poor in vitro fertilization outcomes: A systematic review and meta-analysis. Fertility and sterility, 113(5), 955-969. [CrossRef]
- Bezold, G., Politch, J. A., Kiviat, N. B., Kuypers, J. M., Wolff, H., & Anderson, D. J. (2007). Prevalence of sexually transmissible pathogens in semen from asymptomatic male infertility patients with and without leukocytospermia. Fertility and sterility, 87(5), 1087-1097. [CrossRef]
- Kaspersen, M. D., Larsen, P. B., Ingerslev, H. J., Fedder, J., Petersen, G. B., Bonde, J., & Höllsberg, P. (2011). Identification of multiple HPV types on spermatozoa from human sperm donors. PLoS ONE, 6(3), e18095. [CrossRef]
- Jeršovienė, V., Gudlevičienė, Ž., Rimienė, J., & Butkauskas, D. (2019). Human papillomavirus and infertility. Medicina, 55(7), 377. [CrossRef]
- Damke, E., Kurscheidt, F. A., Balani, V. A., Takeda, K. I., Irie, M. M., Gimenes, F., & Consolaro, M. E. (2017). Male partners of infertile couples with seminal infections of human papillomavirus have impaired fertility parameters. BioMed Research International, 2017. [CrossRef]
- Martorell, M., Gil-Salom, M., Pérez-Vallés, A., Garcia, J. A., Rausell, N., & Senpere, A. (2005). Presence of human papillomavirus DNA in testicular biopsies from nonobstructive azoospermic men. Archives of Pathology & Laboratory Medicine, 129(9), 1132-1136. [CrossRef]
- Foresta, C., Pizzol, D., Bertoldo, A., Menegazzo, M., Barzon, L., & Garolla, A. (2011). Semen washing procedures do not eliminate human papilloma virus sperm infection in infertile patients. Fertility and Sterility, 96(5), 1077-1082. [CrossRef]
- Garolla, A., Pizzol, D., & Foresta, C. (2011). The role of human papillomavirus on sperm function. Current Opinion in Obstetrics and Gynecology, 23(4), 232-237. [CrossRef]
- Garolla, A., Engl, B., Pizzol, D., Ghezzi, M., Bertoldo, A., Bottacin, A., ... & Foresta, C. (2016). Spontaneous fertility and in vitro fertilization outcome: New evidence of human papillomavirus sperm infection. Fertility and sterility, 105(1), 65-72. [CrossRef]
- Foresta, C., Garolla, A., Parisi, S., Ghezzi, M., Bertoldo, A., Di Nisio, A., & De Toni, L. (2015). HPV prophylactic vaccination in males improves the clearance of semen infection. EBioMedicine, 2(10), 1487-1493. [CrossRef]
- Chido-Amajuoyi, O. G., Domgue, J. F., Obi-Jeff, C., Schmeler, K., & Shete, S. (2019). A call for the introduction of gender-neutral HPV vaccination to national immunisation programmes in Africa. The Lancet Global Health, 7(1), e20-e21. [CrossRef]
- Linertová, R., Guirado-Fuentes, C., Mar-Medina, J., & Teljeur, C. (2022). Cost-effectiveness and epidemiological impact of gender-neutral HPV vaccination in Spain. Human Vaccines & Immunotherapeutics, 18(6), 2127983. [CrossRef]
- Lechner, M., Jones, O. S., Breeze, C. E., & Gilson, R. (2019). Gender-neutral HPV vaccination in the UK, rising male oropharyngeal cancer rates, and lack of HPV awareness. The Lancet Infectious Diseases, 19(2), 131-132. [CrossRef]
- Simons, J. J., Vida, N., Westra, T. A., & Postma, M. J. (2020). Cost-effectiveness analysis of a gender-neutral human papillomavirus vaccination program in the Netherlands. Vaccine, 38(30), 4687-4694. [CrossRef]
- Palmer, C., Tobe, K., Negishi, Y., You, X., Chen, Y. T., & Abe, M. (2023). Health impact and cost effectiveness of implementing gender-neutral HPV vaccination in Japan. Journal of Medical Economics, 26(1), 1546-1554. [CrossRef]
- Simoens, S., Bento-Abreu, A., Merckx, B., Joubert, S., Vermeersch, S., Pavelyev, A., ... & Morais, E. (2021). Health impact and cost-effectiveness of implementing gender-neutral vaccination with the 9-valent human papillomavirus vaccine in Belgium. Frontiers in Pharmacology, 12, 628434. [CrossRef]
- Wähner, C., Hübner, J., Meisel, D., Schelling, J., Zingel, R., Mihm, S., ... & Reuschenbach, M. (2023). Uptake of HPV vaccination among boys after the introduction of gender-neutral HPV vaccination in Germany before and during the COVID-19 pandemic. Infection, 1-12. [CrossRef]
- Cheung, T. H., Cheng, S. S. Y., Hsu, D., Wing-Lei Wong, Q., Pavelyev, A., Sukarom, I., & Saxena, K. (2023). Health impact and cost-effectiveness of implementing gender-neutral vaccination with the 9-valent HPV vaccine in Hong Kong. Human Vaccines & Immunotherapeutics, 2184605. [CrossRef]
- Thanasas, I., Lavranos, G., Gkogkou, P., & Paraskevis, D. (2020). Understanding of young adolescents about HPV infection: How health education can improve vaccination rate. Journal of Cancer Education, 35, 850-859. [CrossRef]
Figure 1.
Patients included in study.
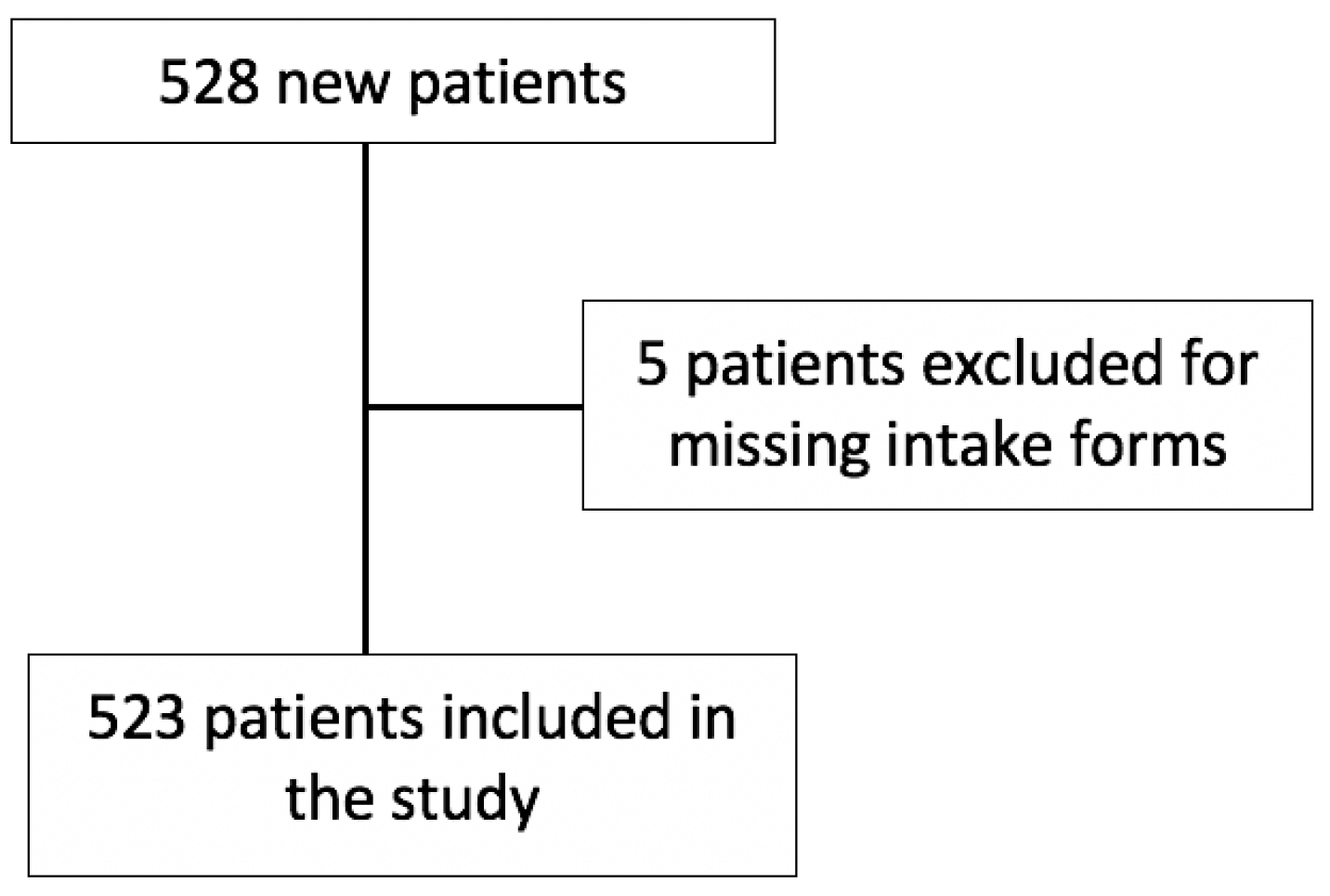
Figure 2.
Percentage of Fertility Patients Who Received the HPV Vaccine.
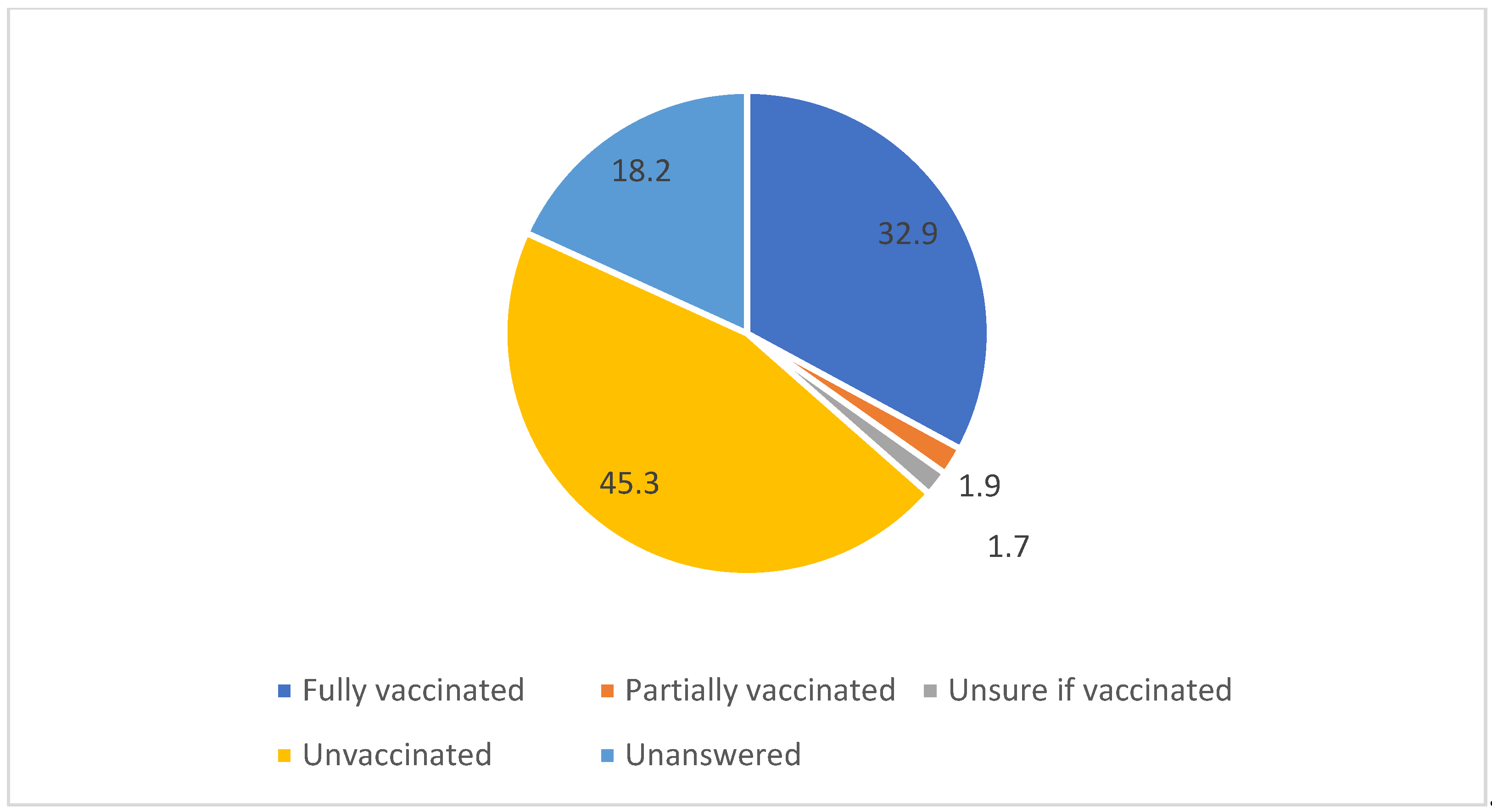
Figure 3.
Average age of vaccinated versus unvaccinated patients.
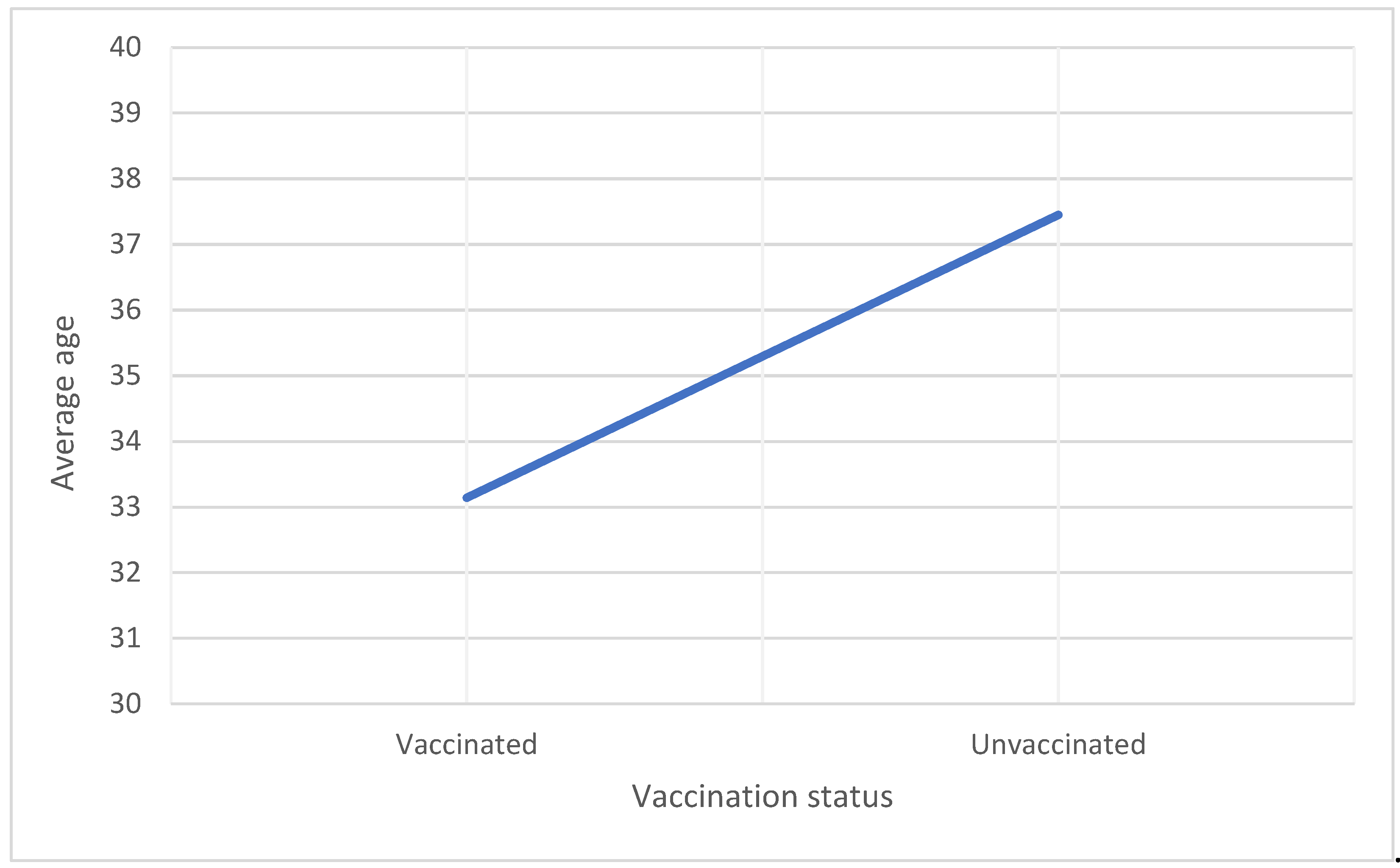

Table 1.
HPV strains covered by type of HPV vaccine.
| Type of HPV vaccine | HPV strains covered |
|---|---|
| Quadrivalent HPV vaccine | 6, 11, 16, 18 |
| 9-valent HPV vaccine | 6, 11, 16, 18, 31, 33, 45, 52, 58 |
Table 2.
Demographic characteristics stratified by HPV Vaccination Status.
|
Vaccinated n=172 (32.9%) |
Unvaccinated n=237 (45.3%) |
p-value | |
|---|---|---|---|
|
Average age (years) |
33.14 ± 4.65 |
37.45 ± 5.54 |
p=<0.001 |
|
History of abnormal Pap smear (n) |
49 (28.5%) |
53 (22.4%) | p=0.098 |
|
Relationship Status Married (n) |
115 (66.9%) |
159 (67.1%) |
p=0.961 |
| Gravidity |
0.65 |
1.11 |
p=0.0005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



