
Submitted:
23 April 2024
Posted:
24 April 2024
You are already at the latest version
Abstract
Three autonomous communities have been the ones that, in the 2022-2023 season, anticipated the document approved by the Public Health Commission, recommending influenza vaccination for all children aged 6 to 59 months. The main objective of this work is to evaluate the attitude of healthcare professionals towards the first universal vaccination campaign in our region, as well as the acceptability of the vaccines used and the attitude towards the piloting of school vaccination. Cross-sectional, survey-based, descriptive study. All healthcare professionals involved in the campaign were invited to participate. The 91.9% of surveyed professionals thought that flu vaccination from 6 to 59 months was important or very important. 89.8% had previous experience regarding the intramuscular vaccine. The professionals valued the intranasal vaccine significantly more positively; however, there were no differences when asking for each of the vaccines without comparison. The inhaled vaccine was preferred by 97.5% for the following campaign. Piloted school vaccination showed 75% acceptance. The inhaled vaccine was preferred by most professionals and the piloted school vaccination was highly accepted, and independently associated to the importance of vaccination as considered by physicians, being a medical doctor, and participation in the pilot program.
Keywords:
Influenza vaccines
; Healthcare professional
; Attitude of Healthcare professional
; intramuscular vaccine
; Inhaled vaccine
1. Introduction
The influenza is a constant threat that causes important morbidity and mortality in the world, being responsible for one million serious cases annually in children under 5 years of age worldwide, which represents a huge public health problem with high socioeconomic implications [1].
In 2012, the World Health Organisation (WHO) [2] included children aged 6 to 59 months as a target population for influenza vaccination because of the high burden of disease in this age group. In the same year, the European Centre for Disease Prevention and Control (ECDC) [3] produced a technical report in which it took a favourable position on vaccination in this age group. The Advisory Committee in Immunization Practices (ACIP) in the USA included universal influenza vaccination for children aged 6 to 23 months in the year 2004 [4], and for those aged 24 to 59 months later in 2006 [5]. More than 70 countries now include influenza vaccination in their childhood and adolescent vaccination schedules [6].
In Spain, the greatest burden of disease occurs in the group of children under 5 years of age, both due to the use of health resources and morbidity associated. Regarding the incidence, the most affected age groups were those under 15 years of age, considering both the last season prior to the COVID-19 pandemic (2019-2020) and in the previous ones. The maximum weekly incidence rate was reported in the 0-4 years group, even overcoming the incidence of the 5-14 years group. It should be noted that in the 2013-2014 to 2019-2020 seasons, the 0 to 4 years age group experienced an average of 4,239 hospital admissions, of which 822 were considered severe hospitalizations and 249 Intensive Care Unit (ICU) admissions and 8 deaths were recorded [7]. Because of this, the Public Health Commission approved in October 2022 the document "Influenza vaccination recommendations for children aged 6 to 59 months" [8] previously approved by the National Immunization Technical Advisory Group in July 2022, thus culminating the work that began years before, in 2019, and which was interrupted by the COVID-19 pandemic. It recommends universal vaccination of all children aged 6 to 59 months, in order to protect them because of their high burden of disease, starting in the 2023–2024 season. This recommendation was reflected in the common lifelong vaccination schedule for 2023 [9].
Three Spanish autonomous communities, Andalusia, Galicia, and the Region of Murcia, have already started with universal vaccination in this age group in the 2022-2023 season. The Region of Murcia was the only Spanish autonomous community to use the live attenuated intranasal vaccine (LAIV) for children aged 24 to 59 months, without any contraindication for this vaccine. In this campaign the inactivated intramuscular vaccine (IIV) was used for children aged 6 to 23 months or for those with contraindication in the use of LAIV [10]. The Vaccination Advisory Committee of the Spanish Association of Paediatrics recommends in its immunisation schedule for the year 2023, preferably, the intranasal influenza vaccine from the age of 24 months onwards [11]
In this first campaign, the coverage objective set in the three autonomous communities was 50%, a relatively ambitious objective for a seasonal vaccination campaign restricted to certain months of the year. In this regard, the communication, information and recruitment strategies carried out by Public Health Authorities, the attitude of healthcare professionals towards influenza vaccination is fundamental due to their informative and active recruitment work, to achieve the objective vaccination coverage set. Therefore, the main objective of this study is to evaluate the attitude of healthcare professionals towards the first universal influenza vaccination campaign in children aged 6 to 59 months in our autonomous community, as well as their degree of acceptability of each of the influenza vaccines used. The secondary objective was to evaluate the attitude of healthcare professionals towards the pilot school influenza vaccination campaign and the possibility of its widespread implementation.
To our understanding, this study provides highly valuable information about healthcare professionals attitude towards universal paediatric vaccination because of the novelty of the program in our country. A detailed analysis of the opinion provided by different type of healthcare professionals involved in vaccinations campaigns may be of high interest for other Spanish or even European authorities, encouraging them to promote similar programs.
2. Materials and Methods
2.1. Study Framework
The FLUTETRA study is a cross-sectional descriptive study to assess the attitude of healthcare professionals providing paediatric care (doctors and nurses) towards childhood influenza vaccination in the Region of Murcia. Once the vaccination campaign had ended, an online questionnaire was sent by e-mail three times, seven days apart, as a reminder to all Primary Care healthcare professionals, both in the public and private settings.
Aiming the higher participation possible in the study, only two inclusion criteria for participation in the study were stablished: i) to be a healthcare professional providing paediatric care, including paediatricians, family doctors and nurses, within the Primary Care setting of the autonomous community under study, the Region of Murcia and ii) ticking the box to give consent of participation in the study. No exclusion criteria were defined.
The analysis was only performed among those healthcare professionals who had directly or indirectly participated in the campaign by vaccination per se, providing counselling or recruiting patients.
2.2. Variables
After agreeing to participate in the study, the healthcare professionals completed the questionnaire designed ad-hoc (provided as a supplementary file), which gathered the following information about the responders: sociodemographic variables, type of healthcare professional, attitude towards influenza vaccination, assessment of available products and factors associated with school influenza vaccination.
A 5-points Likert scale was used to score the survey, from 1 (lowest score) to 5 (higher score). The item evaluated and the response categories vary according to the question (see supplementary file)
2.3. Statistical Analysis
Statistical analysis was performed with SAS v9.4 software through the SAS Enterprise Guide v8.3 interface.
For the descriptive analysis of the qualitative variables, frequency distribution tables and percentages were used. Data analysis was performed both overall and stratified by profession, establishing a Nursing group and a Medical group.
To assess the comparison between qualitative variables, Chi-square test was used when applicable, and Fisher’s exact test was used for those cases of Chi-square non-applicability (i.e. for low frequencies).
Additionally, a post-hoc multivariate logistic regression analysis was performed to determine if the healthcare professional characteristics were independently associated with their opinion about the utility/feasibility of extending the school vaccination through the whole Region of Murcia in the next season vaccination campaign. For this purpose, the following covariates were assessed: grade of relevance of paediatric vaccination against influenza, involvement in paediatric vaccination of children from 6 to 59 months, age, profession, sex, prior experience in vaccination against influenza, participation in the pilot experience, LAIV ease/convenience of administration, and LAIV general rating. Variables with p <0.2 in the bivariate logistic regression analysis were considered significant and included in a multivariate model with stepwise selection method, and odds ratio (OR) and 95% CIs were calculated. Test results with p < 0.05 were considered statistically significant.
2.4. Ethics
The study was approved by the Ethics Committee for Investigation with Medicinal Products of Hospital Clínico Universitario Virgen de la Arrixaca-Area 1 of the autonomous community where study was conducted. Participants marked a first mandatory box as acceptance of their participation in the study after due information prior to completing the online questionnaire.
The study was conducted in accordance with Good Clinical Practice guidelines and the regulations contained in the Declaration of Helsinki, which are included in the current legislation on biomedical research.
3. Results
The study survey was provided to a total of 1,140 professionals from which 339 answered the online survey, meaning that the response rate of the survey was 29.73%. Overall responders, 284 professionals (88.47% of those who answered, 95% CI 85.07-91.87%) declared that they participated in the vaccination campaign, both regularly and occasionally. Only the records of involved professionals (n=284) were considered for this analysis, which means 28.16% of the total of 1,140 professionals. The responder’s profile was a female professional, aged 40-49 years with regular experience in influenza vaccination, with a higher proportion of nurses. The detailed sociodemographic description of the participating professionals is summarized in Table 1, with statistically significant differences (p<0.001) between doctors and nurses with respect to age. No statistically significant differences were found regarding other sociodemographic variables, such as sex and previous experience on influenza vaccination.
Among the surveyed population involved in vaccination, most of the nursing group were paediatric nurses (54.4%), followed by family nurses (28.7%), school nurses (16.4%) and family and paediatric nurses (0.5%). Regarding the Medical group, only two types of specialists were involved: paediatricians (80.5%) and family and community doctors (19.5%).
When asked about the importance of influenza vaccination in children aged 6 to 59 months in terms of disease burden, 91.9% of the professionals assigned a score of 4 and 5 on the Likert scale, with statistically significant differences (p<0.001) in relation to profession, with a higher proportion among doctors (n=80; 97.6%) compared to nurses (n=181; 89.6%).
Regarding the ease/comfort of administration assessment of the type of vaccine administered, the mean (±SD) scores in the Likert scale obtained from intranasal and intramuscular vaccines were 4.65±0.6 and 3.8±0.97 respectively. A high percentage of respondents appreciated the ease/comfort of administration of the intranasal influenza vaccine, with significantly higher scores in the overall rating in comparison to intramuscular vaccines (Figure 1).
In addition, both ease/comfort and the overall assessment of each of the vaccines in the study population were evaluated in a comparative analysis by professional group, as well as the percentages of scores according to the Likert scale (Figure 2). Overall, mean scores were 4.64±0.55 for intranasal vaccine and 4.01±0.84 for intramuscular. No statistically significant differences were found between professional groups.
In regard to the preference for using the intranasal vaccine in children aged 24 to 59 months for the next campaign in those cases indicated according to the Summary of the Product, 97.5% of the professionals affirmed that they preferred it (100% of doctors and 96.5% of nurses), with no statistically significant differences by professional category.
Only 13.79% (95% CI 10.12-17.46%) of the surveyed had participated in the school vaccination pilot experience. All the professionals, both participants and not participants in the pilot, were asked about the usefulness/feasibility of extending school influenza vaccination to children under 3 and 4 years of age, and most of them gave scores of 4 or 5 (74.73%). Statistically significant differences by professional category were observed (p<0.001), as shown in Figure 3. Stratified according to participation, a significantly higher percentage (p=0.033) of professionals assigned a score of 4 or 5 (86.36%) in the former compared to the latter (72.27%).
In addition, participants were asked to give their opinion on the importance of the presence of a medical doctor at the school vaccination. The most chosen answer by all participants, independently of professional group, was advisable but not essential (nursing group: 47.2% and medical group: 40.2%). Answers stratified according to professional groups showed that 38.2% of the nursing group judged completely essential the presence of doctors, and only 13.6% considered that the nursing team can autonomously deal with vaccination. In contrast, medical doctors were of the opinion that the nursing team can autonomously deal with vaccination (36.6%) and their presence is only completely essential for 17.1% of the respondents. Answers stratified by professional group were statistically significant (p<0.001). When the stratification was made by those who had participated in the pilot with respect to those who had not, in relation to the recommendation or essential presence of a doctor (72.7% vs 77.6% respectively), despite no statistically significant differences between both groups, the percentage was lower in those of the pilot. However, within each of them, statistically significant differences (p<0.001) were evident by professional category (80.6% in nursing vs 53.8% in doctors in the participants in the pilot, compared to 83.9% in nursing and 62.3% in those who did not participate), also lower in those who took part in the pilot experience.
When asking about the type of vaccine used in school vaccination (intranasal or intramuscular), the vast majority considered the intranasal vaccine as the vaccine of choice for school vaccination (90.6%), evaluating it as recommended or essential for it. Only 5.0% considered the choice of the vaccine to be administered as indifferent and the rest considered the use of the intramuscular vaccine advisable or essential.
According to the logistic regression, three covariates were independently associated with a favourable opinion of extending the school vaccination pilot program. A unitary increase of the grade of relevance of paediatric vaccination (as considered by the healthcare professional) increased in a 0.42 (odds ratio, OR) the favourable opinion, as well as belonging to the Medical group (OR = 0.4). Similarly, the participation in the pilot vaccination school program was considered independently associated with the favourable opinion of extending the school program (OR= 0.26). The univariate and multivariate models extracted from the logistic regression analysis and the odds ratio are displayed in Table 2 and Figure 4 respectively)
4. Discussion
Healthcare professionals are one of the most important sources of information for families in making decisions about vaccination [12,13,14]. This is even more important when discussing a seasonal vaccination campaign and a new vaccination strategy with a vaccine, such as the attenuated vaccine, which has established an unprecedented experience in the Region of Murcia and Spain due to its characteristics and route of administration during the 2022–2023 vaccination campaign.
Our work elicited responses from 82 physicians (paediatricians and family doctors) and 202 nurses (Table 1). The 91.9% of surveyed professionals thought that influenza vaccination in children aged 6 to 59 months was important or very important, a view shared by doctors and nurses, with a statistically significant difference, which is probably not of practical relevance (97.6% vs. 89.6%). Similar results have been described in Quebec, where more than 90% of professionals agreed with influenza vaccination [15], or in the USA, where 84% of paediatricians shared the opinion of the importance of vaccination [16]. These data contrasts with the results obtained in a study carried out in Australia, which found a lack of awareness of the seriousness of influenza in children [17]. The positive attitude detected among our professionals may be because the health authorities [8] and scientific societies agreement on the recommendations [18], and probably also because of the accumulated experience of childhood influenza vaccination in other countries for years.
Although universal paediatric influenza vaccination started in the 2022–2023 season, 89.8% of the professionals had experience of influenza vaccination with the intramuscular vaccine, while the inhaled vaccine had been scarcely available previously. When asked about ease/comfort of administration, 95% said that the intranasal vaccine is easy or very easy to administer, compared to 65.1% for the intramuscular vaccine (Figure 1). Similarly, when rating their overall experience with the vaccines, 96.5% rated the inhaled vaccine positively or very positively, compared to only 73.2% for the intramuscular vaccine. With respect to the inhaled vaccine, it also remarkable that only 0.7% rated the convenience of its administration negatively, which would support the simplicity of its use, given that this is the first season of widespread administration, and it is expected that the ease of use will increase as experience with it increases throughout the coming seasons. This difference is illustrated when asking comparatively about the two vaccines; however, it is not observed when asking about each of the vaccines without making a comparison between them (Figure 2), as both vaccines score positively or very positively, especially in terms of ease of administration. The intranasal vaccine was preferred by 97.5% of the professionals, who stated that they would prefer it for the next vaccination campaign.
Studies comparing the two vaccines are rare, and ours is one of the few to address this issue. In a study conducted in Quebec [15] more than 90% of the professionals considered that the intranasal attenuated vaccine had been well received, both by parents and by themselves, and 57% rated the ease of administration very positively, a figure that was higher in our data (71%).
Another possible consequence of the preference for one vaccine over another is an eventual increase in vaccination rates in places where the vaccine is available. However, estimating the influence of the type of vaccine administered on the vaccination rate is complex, since this is influenced by multiple factors. In fact, the data available following the withdrawal of the intranasal vaccine in the US in the 2016–2017 season, which made it possible to estimate the evolution of vaccination rates compared to the previous season when the attenuated vaccine was available, are discordant. One study found no change in vaccination rates[19], while another estimated a decrease of 1.6%, with a lower tendency to vaccinate in the second season among the most socially disadvantaged [20].
Our work additionally addresses the acceptability of school vaccination among professionals in the Region of Murcia following a pilot study carried out in 24 schools. In this sense, school influenza vaccination programs have demonstrated an increase in vaccination rates as well as being a valid instrument for mass vaccination in countries such as the USA [21,22], overcoming one of the possible barriers, namely additional visits to the healthcare centre that require both time off work for the legal guardians and time off school for the children [23]. Furthermore, it should also be considered that childhood influenza vaccination in Spain will mean almost one million additional visits to healthcare centres for children aged 6 to 59 months (estimating a vaccination rate of 60%), limited to the a short period of time of approximately 3 months (vaccination campaign estimated duration) based on the National Statistics Institute [INE] data [24]), so incorporating alternative vaccination points can be very useful to avoid saturating the primary healthcare system. School vaccination programs have shown that the cost per dose of vaccine administered can be lower [25] and can lead to cost savings when considering the cost of working hours lost by legal guardians for the vaccination of children [26], and can therefore contribute not only to increasing accessibility and vaccination rates, but also to the efficiency of the system. Furthermore, according to a study published in Eurosurveillance in 2014 with data from the United Kingdom, in relation to vaccination against human papillomavirus in adolescents, the strategy of school vaccination also reduces inequities [27]. Another advantage of school vaccination is that it allows early and rapid vaccination, allowing high vaccine coverage in the children to be vaccinated in just two weeks. This allows you to be prepared for when the flu epidemic season arrives. This is especially important in a epidemic disease that may present early, such as occurred in the United Kingdom in the 2019-20 season [28].
In the Region of Murcia, school influenza vaccination was piloted during the 2022-2023 season in 24 schools. To this end, families were sent a letter with information on intranasal influenza vaccination and its contraindications, requesting consent from parents/legal guardians, and prior review of the medical records by the vaccination teams. In the first 4 centres evaluated, the vaccination rate was increased by 22.5% on a single day of school vaccination [29], so it seems pertinent to obtain the professionals’ opinion before extending the program. When asked about the extension of the pilot program to the entire population of children aged 3 and 4 years with intranasal vaccine, almost 75 % agreed or strongly agreed (with greater support from doctors, 90 %, but also with significant support from nurses, 68.3 %), this support was greater among professionals who had participated in the pilot project, which may express that an initial "fear" is overcome after participation in school vaccination (86.4 vs. 72.7%, p=0.03). These data are supported by the results of the logistic regression performed post-hoc, which confirmed the fact that giving a high importance to paediatric vaccination directly correlates with a favourable opinion of extending the pilot school vaccination throughout the Region of Murcia for the next season (OR =0.42). This analysis also highlighted the support from the medical group to the extension of the pilot program, with a correlation (OR) of 0,40, and the association between the participation in the pilot program and a favourable opinion towards the extension (OR=0.26). Similar studies have been conducted in the USA. The study conducted by Keane and cols showed less support from paediatricians than that seen in Spain, with 73% support for vaccinating children aged 24 to 59 months, which rises to 96 % for children aged 5 years and older[30]. In another study, also carried out in a sample of responders from the American Academy of Pediatrics, paediatricians’ support was 86 %, although with differences depending on the children’s age and possible conditions of risk [31]. In general, support from paediatricians in our setting is somewhat higher, which may be due to the use of the attenuated vaccine since the US surveys did not propose using only the attenuated vaccine in the school setting. In this regard, another study carried out in the USA associated the use of the attenuated vaccine in schools with an increase in vaccination rates, an increase in the speed of administration and children who were calmer during the process [32].
For many years, adolescents have been vaccinated against meningococcal disease and human papillomavirus at school in the Region of Murcia, and, since 2008, in a protocolised manner [33]. As a result of the protocolized school vaccination against the human papillomavirus in girls, some healthcare professionals (predominantly nurses) have traditionally demanded the presence of a paediatrician along with the nursing professionals in charge of school vaccination, and this survey was an excellent opportunity to address this issue. Our data revealed that 2 out of 3 surveyed healthcare professionals do not consider the presence of a doctor necessary, they consider it advisable but not essential, or they have a neutral opinion. As expected according to the line of opinion that had been observed in the nursing teams dedicated to school vaccination, , our data reveal that the presence of physicians is considered completely essential by a higher number of professionals withing the nursing group than the medical group themselves (38.2% vs. 17.1%) and vice versa; doctors are most likely to think that the nursing team can autonomously deal with school vaccination in comparison with nurses themselves (36.6% vs. 13.6%). This can be interpreted as an attempt by physicians to increase the competencies of nursing professionals, considering them sufficiently qualified to lead the vaccination autonomously, as well as a lower number of immediate adverse reactions expected as it is an intranasal vaccine. Probably, the need for the presence of a physician on the part of nursing comes from the previous experience of vaccination against the intramuscular human papillomavirus in adolescents, so these data are presented as a baseline, which will have to be returned to be studied in successive campaigns in which there is more experience in school intranasal influenza vaccination, to see if the presence of a doctor is considered equally or less necessary. In fact, when analysing the data among those who had or had not participated in the pilot, a tendency (not statistically significant) was observed to give less importance to the presence of a doctor in the vaccination. Other plausible hypothesis is that both groups of professionals are indeed saturated for assuming this new responsibility and they attempt to share this emerging task with other healthcare professionals, nursing considering school vaccination a task of the primary care team, of which doctors are also part.
In relation to the type of vaccine preferred for administration in the school environment, the results obtained are expected since, for the vast majority of professionals, the vaccine of choice should be the intranasal vaccine due to its ease of administration and being painless, which makes it possible to administer it to young children in schools without incidents.
Our work has several limitations. Firstly, the response rate was 29.7%, despite having sent the information three times, each separated by 7 days, which could mean that the respondents were particularly motivated. However, there are other studies carried out in the USA that had similar response rates [14,30], in addition to the fact that most of the literature consulted had similar or smaller sample sizes. Secondly, the study was conducted during the first season of influenza vaccination in the paediatric population in the autonomous community under study, so we do not have our own comparative data with respect to previous campaigns. To solve this second limitation, the study is being reproduced in this second influenza vaccination season. A third limitation of our work is that we do not have a history of vaccination against the influenza nor the willingness to be vaccinated against it. In different recently published papers it has been found that the willingness of health professionals to be vaccinated against influenza varies between 52 and 54.9% [34,35], which contrasts with the support for vaccination of the paediatric population of our study (91.9%). Nevertheless, we might consider this comparation cautiously, because the acceptance of self-vaccination and the recommendation of paediatric vaccination, may not be correlative. It might be reasonable to expect that the non-responders were less willing to support the vaccination, and therefore to refuse to participate in the study, nevertheless we consider that other reasons for not participating are more plausible such as high workload, lack of motivation to complete the survey or even forgetfulness. We believe that the simultaneous study of support for vaccination of patients and healthcare workers themselves is an interesting endpoint for future research since it may provide a different point of view to evaluate the healthcare professionals positioning regarding influenza vaccination.
5. Conclusions
In conclusion, the results of our study show the significant support of healthcare professionals involved in childhood influenza vaccination for the use of a vaccine such as the attenuated intranasal vaccine, which had not been used before, and has achieved a 97% of preference for the next vaccination campaign. Our data reveals a good acceptance for extending the school vaccination program, with almost 75% of professionals supporting it and intranasal vaccine as the suitable for school vaccination. Additionally, we have found an association between the grade of relevance given to paediatric vaccination, being a medical doctor and the participation in the pilot program with a favourable opinion for extending the pilot throughout the Region of Murcia.
6. Future Directions
There is still a need for information and training of professionals to strengthen vaccination programs, so further research into their opinions and attitudes in order that programs can be tailored to their needs, even more so in seasonal vaccination campaigns such as the influenza campaign in the paediatric population, which requires a high recommendation to achieve coverage objectives.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1.
Author Contributions
Conceptualization: J.J.P.M, M.Z.M. and A.I.A. Formal analysis: J.J.P.M. and M.Z.M. Investigation: J.J.P.M, M.Z.M. and A.I.A. Methodology: J.J.P.M, M.Z.M. and A.I.A. Writing – original draft: J.J.P.M., M.Z.M. and A.I.A. Writing – review and editing: J.J.P.M., M.Z.M. and A.I.A.
Funding
Statistical assistance and Editorial assistance of this work was funded by AstraZeneca Spain. Article publication charges (APC) were funded by AstraZeneca Spain.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Hospital Clínico Universitario Virgen de la Arrixaca-Area 1 Ethics Committee.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
The authors acknowledge all involved healthcare professionals for participating in the study. Editorial assistance was provided by Reyes Prieto, and statistical analysis was performed by David Calbet from Evidenze Health España S.L.U.
Conflicts of Interest
The authors declare having received funding from AstraZeneca for training and dissemination activities. J.J.P.M. declares having received funding from CSL Seqirus for training and dissemination activities and M.Z.M. for training activities.
References
- Ruf, B.R.; Knuf, M. The burden of seasonal and pandemic influenza in infants and children. Eur J Pediatr 2014, 173, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Vaccines against influenza WHO position paper November 2012, No. 47.
- ECDC scientific advice on seasonal influenza vaccination of children and pregnant women. 2012.
- Harper, S.A.; Fukuda, K.; Uyeki, T.M.; Cox, N.J.; Bridges, C.B.; Centers for Disease, C.; Prevention Advisory Committee on Immunization, P. Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2004, 53, 1–40. [Google Scholar] [PubMed]
- Advisory Committee on Immunization, P.; Smith, N.M.; Bresee, J.S.; Shay, D.K.; Uyeki, T.M.; Cox, N.J.; Strikas, R.A. Prevention and Control of Influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep 2006, 55, 1–42. [Google Scholar]
- European Centre for Disease Prevention and Control. Recommended immunization for influenza. Available online: https://vaccine-schedule.ecdc.europa.eu/ (accessed on November 16).
- Informe de Vigilancia de la Gripe en España. Temporada 2019-2020.
- Recommendations for children aged 6 to 59 months of the Programme and Registry of Vaccinations. October 2022.
- Common lifelong vaccination schedule. Recommended schedule for 2023. December 2022.
- Influenza vaccination in the healthy paediatric population aged 6 to 59 months. Season 2022–2023. 2022.
- Alvarez Garcia, F.J.; Cilleruelo Ortega, M.J.; Alvarez Aldean, J.; Garces-Sanchez, M.; Garrote Llanos, E.; Iofrio de Arce, A.; Montesdeoca Melian, A.; Navarro Gomez, M.L.; Pineda Solas, V.; Rivero Calle, I.; et al. Immunisation schedule of the Spanish Association of Paediatrics: 2023 Recommendations. An Pediatr (Engl Ed) 2023, 98, 58 e51-58 e10. [Google Scholar] [CrossRef] [PubMed]
- Torun, S.D.; Torun, F.; Catak, B. Healthcare workers as parents: attitudes toward vaccinating their children against pandemic influenza A/H1N1. BMC Public Health 2010, 10, 596. [Google Scholar] [CrossRef]
- Kang, G.J.; Culp, R.K.; Abbas, K.M. Facilitators and barriers of parental attitudes and beliefs toward school-located influenza vaccination in the United States: Systematic review. Vaccine 2017, 35, 1987–1995. [Google Scholar] [CrossRef]
- Balgovind, P.; Mohammadnezhad, M. Factors affecting childhood immunization: Thematic analysis of parents and healthcare workers’ perceptions. Hum Vaccin Immunother 2022, 18, 2137338. [Google Scholar] [CrossRef]
- Dube, E.; Gagnon, D.; Kiely, M.; Boulianne, N.; Landry, M. Acceptability of live attenuated influenza vaccine by vaccine providers in Quebec, Canada. Hum Vaccin Immunother 2015, 11, 956–960. [Google Scholar] [CrossRef]
- Edwards, N.M.; Baumann-Blackmore, N.L.; Saari, T.N. Attitudes of Wisconsin pediatricians toward influenza immunization. WMJ 2011, 110, 63–67. [Google Scholar] [PubMed]
- Biezen, R.; Grando, D.; Mazza, D.; Brijnath, B. Why do we not want to recommend influenza vaccination to young children? A qualitative study of Australian parents and primary care providers. Vaccine 2018, 36, 859–865. [Google Scholar] [CrossRef] [PubMed]
- Recommendations 2022–2023. AEP September 2022.
- Robison, S.G.; Dunn, A.G.; Richards, D.L.; Leman, R.F. Changes in Influenza Vaccination Rates After Withdrawal of Live Vaccine. Pediatrics 2017, 140. [Google Scholar] [CrossRef]
- Fogel, B.; Hicks, S. Influenza vaccination rates in children decline when the live attenuated influenza vaccine is not recommended. Vaccine 2017, 35, 5278–5282. [Google Scholar] [CrossRef]
- Pannaraj, P.S.; Wang, H.L.; Rivas, H.; Wiryawan, H.; Smit, M.; Green, N.; Aldrovandi, G.M.; El Amin, A.N.; Mascola, L. School-located influenza vaccination decreases laboratory-confirmed influenza and improves school attendance. Clin Infect Dis 2014, 59, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.; Wang, H.L.; Mascola, L.; El Amin, A.N.; Pannaraj, P.S. Parental perceptions and predictors of consent for school-located influenza vaccination in urban elementary school children in the United States. Influenza Other Respir Viruses 2015, 9, 255–262. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Schaffer, S.; Rand, C.M.; Goldstein, N.P.N.; Hightower, A.D.; Younge, M.; Eagan, A.; Blumkin, A.; Albertin, C.S.; DiBitetto, K.; et al. Impact of elementary school-located influenza vaccinations: A stepped wedge trial across a community. Vaccine 2018, 36, 2861–2869. [Google Scholar] [CrossRef]
- Resident population by date, sex and age. Available online: https://www.ine.es/jaxiT3/Tabla.htm?t=4028&L=0 (accessed on November 2023).
- Wilson, T. Economic evaluation of a metropolitan-wide, school-based hepatitis B vaccination program. Public Health Nurs 2000, 17, 222–227. [Google Scholar] [CrossRef]
- Cawley, J.; Hull, H.F.; Rousculp, M.D. Strategies for implementing school-located influenza vaccination of children: a systematic literature review. J Sch Health 2010, 80, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.; Mesher, D.; White, J.; Soldan, K. Coverage of the English national human papillomavirus (HPV) immunisation programme among 12 to 17 year-old females by area-level deprivation score, England, 2008 to 2011. Euro Surveill 2014, 19. [Google Scholar] [CrossRef]
- RSC: Public health data. Weekly reports. April 2020. . 2020.
- Hernández Fuentes, F.; Navarro Esteban, M.T.; Rueda Nieto, S.; Zornoza Moreno, M.; Pérez Martin, J.J. Cobertura antigripal en menores de 5 años tras la campaña de vacunación escolar en una región del sur de España [Presentation at a congress]. In Proceedings of the 69th Congress of the Spanish Association of Paediatrics, 1-3 June 2023., Granada (Spain).
- Keane, V.A.; Hudson, A.R.; King, J.C., Jr. Pediatrician attitudes concerning school-located vaccination clinics for seasonal influenza. Pediatrics 2012, 129 Suppl 2, S96–S100. [Google Scholar] [CrossRef]
- Kempe, A.; Wortley, P.; O’Leary, S.; Crane, L.A.; Daley, M.F.; Stokley, S.; Babbel, C.; Dong, F.; Beaty, B.; Seewald, L.; et al. Pediatricians’ attitudes about collaborations with other community vaccinators in the delivery of seasonal influenza vaccine. Acad Pediatr 2012, 12, 26–35. [Google Scholar] [CrossRef]
- Kwong, J.C.; Pereira, J.A.; Quach, S.; Pellizzari, R.; Dusome, E.; Russell, M.L.; Hamid, J.S.; Feinberg, Y.; Winter, A.L.; Gubbay, J.B.; et al. Randomized evaluation of live attenuated vs. inactivated influenza vaccines in schools (RELATIVES) pilot study: a cluster randomized trial. Vaccine 2015, 33, 535–541. [Google Scholar] [CrossRef]
- Protocol for the administration of vaccines in schools. October 2022.
- Lecce, M.; Biganzoli, G.; Agnello, L.; Belisario, I.; Cicconi, G.; D’Amico, M.; De Giorgi, F.; Ferilli, A.; Ferraguzzi, G.; Guzzardi, F.; et al. COVID-19 and Influenza Vaccination Campaign in a Research and University Hospital in Milan, Italy. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef]
- Alobwede, S.M.; Kidzeru, E.B.; Katoto, P.; Lumngwena, E.N.; Cooper, S.; Goliath, R.; Jackson, A.; Wiysonge, C.S.; Shey, M.S. Influenza Vaccination Uptake and Hesitancy among Healthcare Workers in Early 2021 at the Start of the COVID-19 Vaccine Rollout in Cape Town, South Africa. Vaccines (Basel) 2022, 10. [Google Scholar] [CrossRef]
Figure 1.
Percentage of healthcare professionals who rated the intranasal vs intramuscular vaccines used in the vaccination campaign in a comparative analysis according to a Likert scale; being 1 the lowest possible score and 5 being the highest. Figure 1A. represents the scores given to “Ease/comfort of administration” (survey question 10, supplementary file). For this analysis, scores of 1 and 2 on the Likert scale were translated as the very poor/poor, scores of 3 as neither poor nor good, and scores of 4 and 5 as good/very good rating (p<0.001). and Figure 1B. represents the scores given to “General rating of professional’s experience with the vaccine” (survey question 11, supplementary file). For this analysis, scores of 1 and 2 on the Likert scale were translated as the worst possible experience/poor experience, scores of 3 as neither poor nor good experience, and scores of 4 and 5 as good experience/best possible experience (p<0.001)..
Figure 1.
Percentage of healthcare professionals who rated the intranasal vs intramuscular vaccines used in the vaccination campaign in a comparative analysis according to a Likert scale; being 1 the lowest possible score and 5 being the highest. Figure 1A. represents the scores given to “Ease/comfort of administration” (survey question 10, supplementary file). For this analysis, scores of 1 and 2 on the Likert scale were translated as the very poor/poor, scores of 3 as neither poor nor good, and scores of 4 and 5 as good/very good rating (p<0.001). and Figure 1B. represents the scores given to “General rating of professional’s experience with the vaccine” (survey question 11, supplementary file). For this analysis, scores of 1 and 2 on the Likert scale were translated as the worst possible experience/poor experience, scores of 3 as neither poor nor good experience, and scores of 4 and 5 as good experience/best possible experience (p<0.001)..
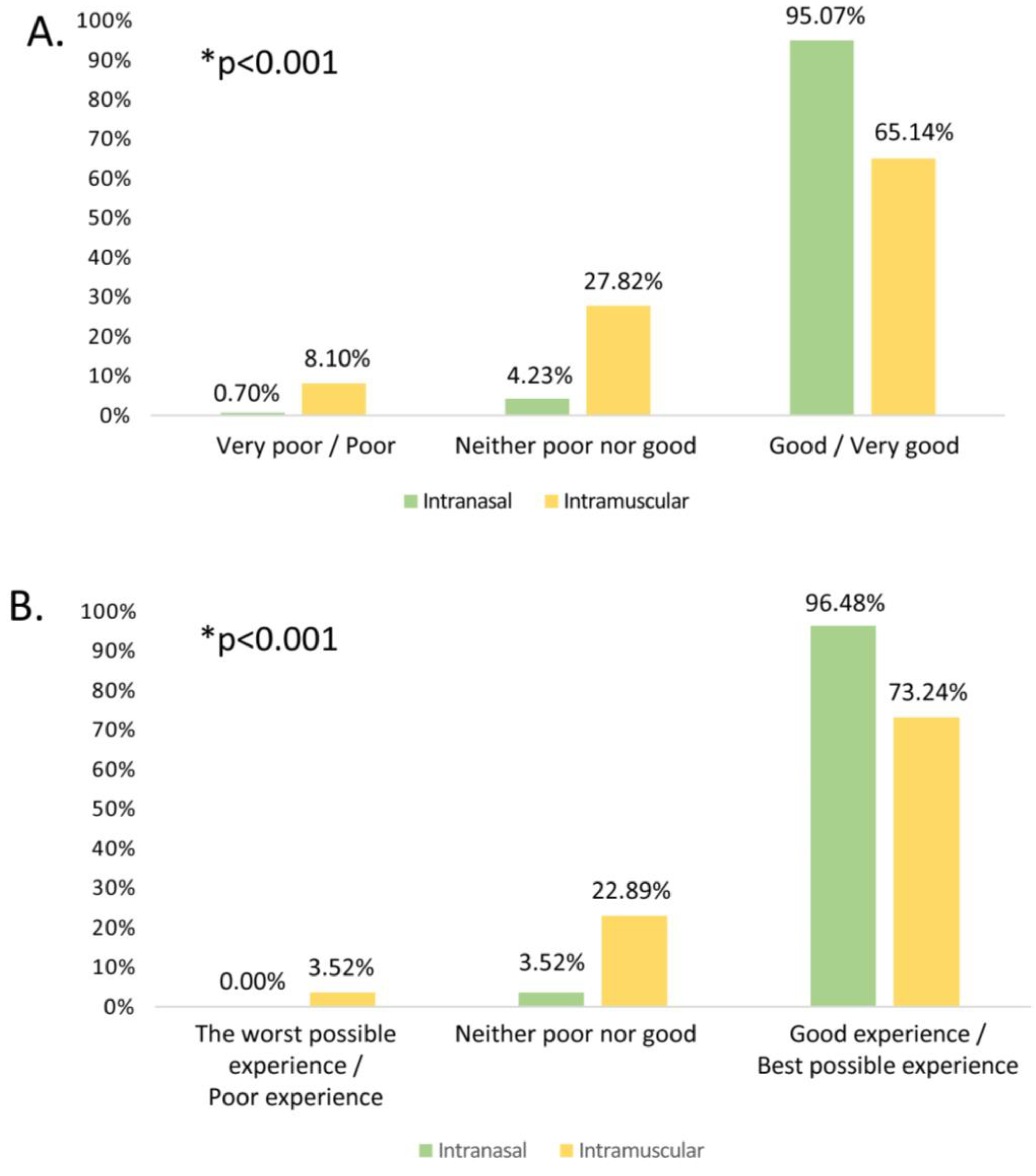
Figure 2.
Overall Likert 5-points scale score (blue), and comparing by professional category (doctors in dark orange vs. nurses in light orange). A. Ease/comfort of intranasal vaccine administration (p=0.013 in the comparison according to professional group). B. General rating of professional’s experience with the vaccine (p>0.05 in the comparison according to professional group). C. Ease/comfort of administration of intramuscular vaccines (p<0.001 in the comparison according to professional group). D. General rating of professional’s experience with the vaccine (p=0.001 in the comparison according to professional group).
Figure 2.
Overall Likert 5-points scale score (blue), and comparing by professional category (doctors in dark orange vs. nurses in light orange). A. Ease/comfort of intranasal vaccine administration (p=0.013 in the comparison according to professional group). B. General rating of professional’s experience with the vaccine (p>0.05 in the comparison according to professional group). C. Ease/comfort of administration of intramuscular vaccines (p<0.001 in the comparison according to professional group). D. General rating of professional’s experience with the vaccine (p=0.001 in the comparison according to professional group).
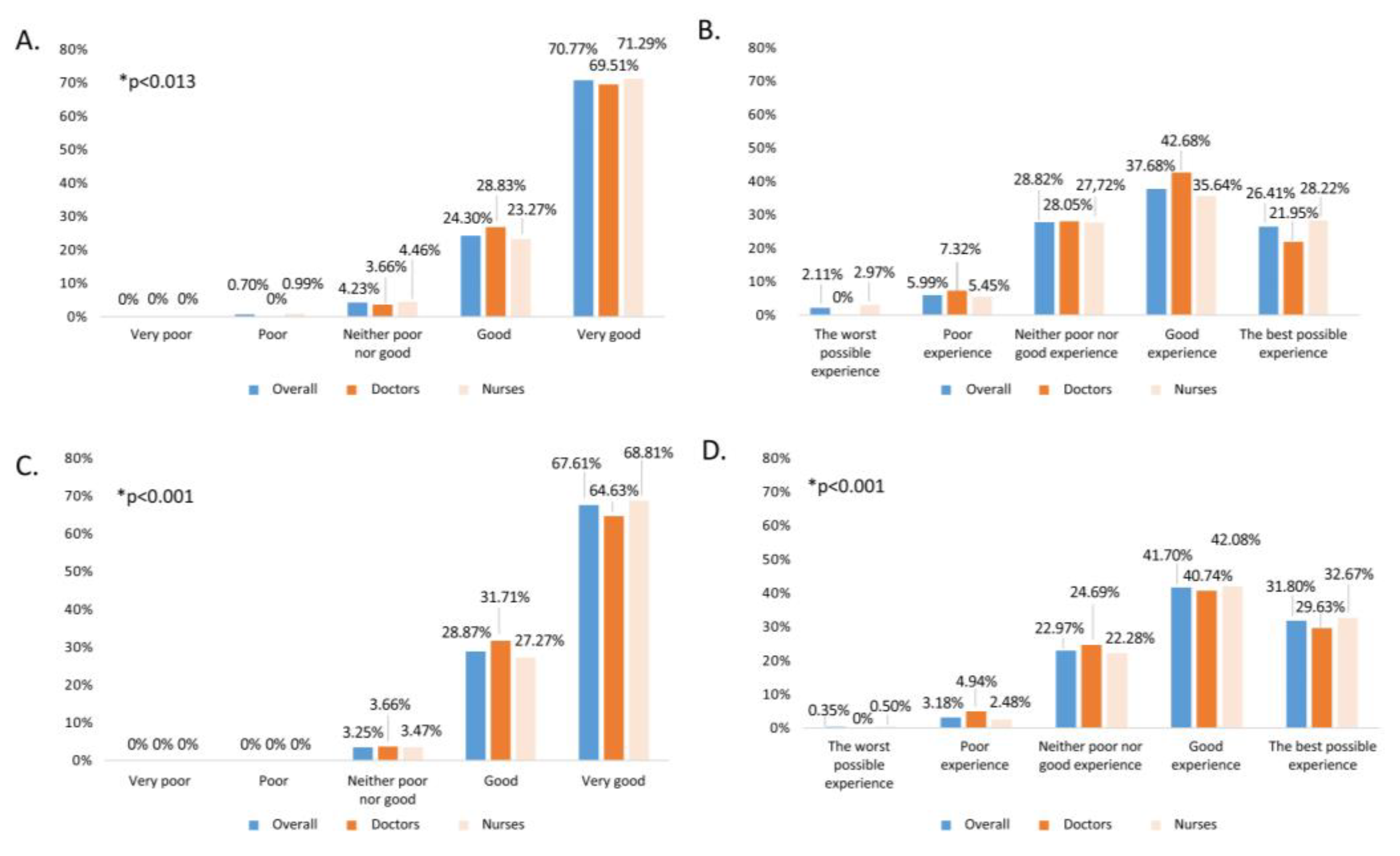
Figure 3.
Percentage of healthcare professionals assigning Likert scale scores to the question of usefulness/feasibility of extending school influenza vaccination to all schools globally among healthcare professionals and comparatively by professional category.
Figure 3.
Percentage of healthcare professionals assigning Likert scale scores to the question of usefulness/feasibility of extending school influenza vaccination to all schools globally among healthcare professionals and comparatively by professional category.
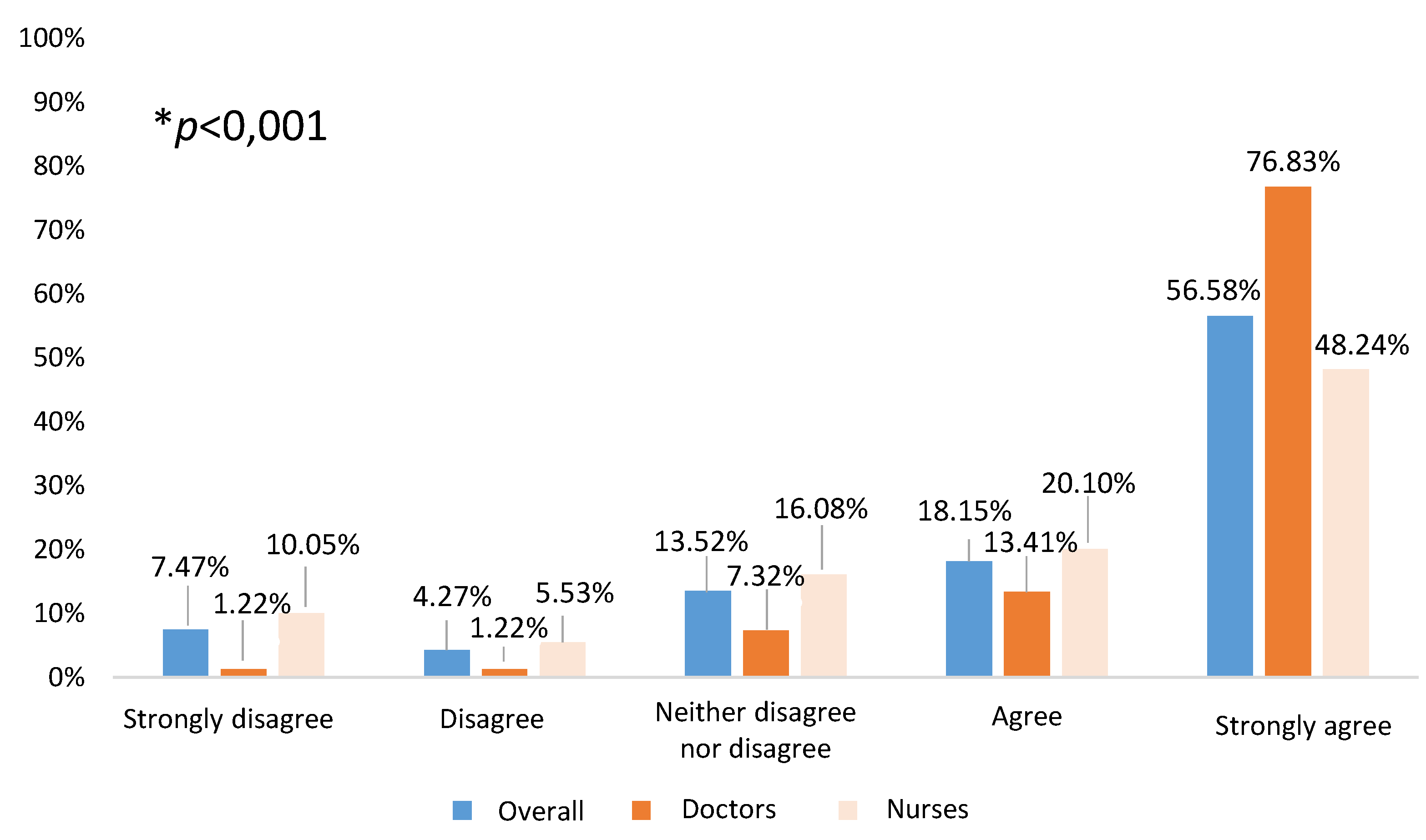
Figure 4.
Factors independently associated with a favourable opinion of extending the school vaccination program for the next season. The x-axis represents the Odds ratio of each covariate analysed in the multivariate analysis (y-axis) along with the 95% CI.
Figure 4.
Factors independently associated with a favourable opinion of extending the school vaccination program for the next season. The x-axis represents the Odds ratio of each covariate analysed in the multivariate analysis (y-axis) along with the 95% CI.
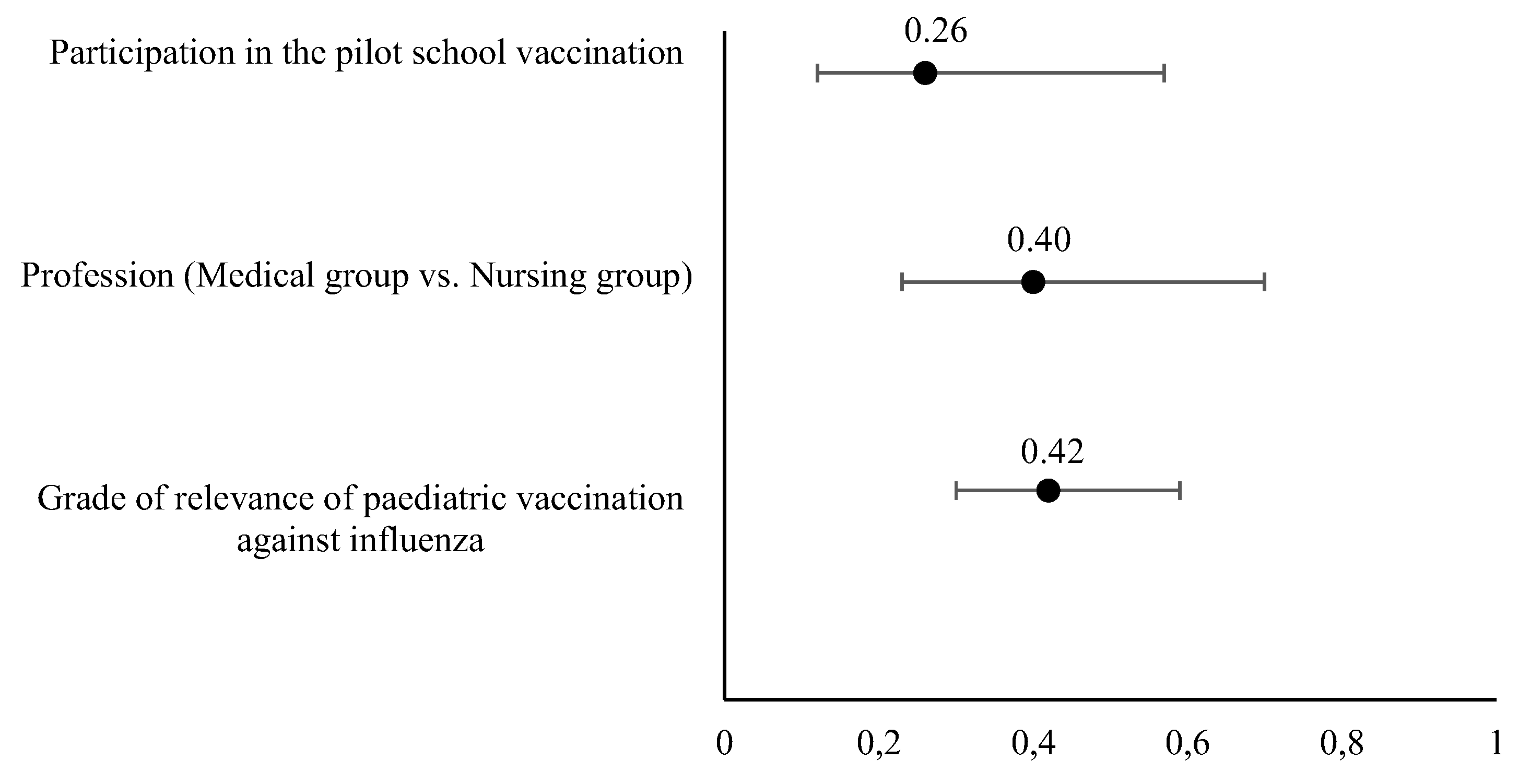

Table 1.
Sociodemographic variables of healthcare professionals involved in the 2022–2023 influenza vaccination campaign in the paediatric population aged 6 to 59 months.
Table 1.
Sociodemographic variables of healthcare professionals involved in the 2022–2023 influenza vaccination campaign in the paediatric population aged 6 to 59 months.
| Doctor – N (%) | Nurse – N (%) | Total – N (%) | p-value | ||
|---|---|---|---|---|---|
| Age | < 20 years | 0 (0.0%) | 1 (0.4%) | 1 (0.4%) | <0.001 |
| 20–29 years | 0 (0.0%) | 8 (3.9%) | 8 (2.8%) | ||
| 30–39 years | 22 (26.8%) | 35 (17.3%) | 57 (20.1%) | ||
| 40–49 years | 19 (23.2%) | 75 (37.1%) | 94 (33.1%) | ||
| 50–59 years | 27 (32.9%) | 56 (27.7%) | 83 (29.2%) | ||
| ≥ 60 years | 14 (17.1%) | 27 (13.4%) | 41 (14.4%) | ||
| Sex | Male | 22 (26.8%) | 48 (23.8%) | 70 (24.6%) | 0.587 |
| Female | 60 (73.2%) | 154 (76.2%) | 214 (75.4%) | ||
| Previous experience in influenza vaccination | No | 1 (1.2%) | 2 (1.0%) | 3 (1.1%) | 0.076 |
| Occasional | 8 (9.8%) | 18 (8.9%) | 26 (9.2%) | ||
| Regular | 73 (89.0%) | 182 (90.1%) | 255 (89.8%) | ||
| Total number of participants | 82 (28.9%) | 202 (71.1%) | 284 (100%) | ||
Table 2.
Univariate and multivariate analyses extracted from the logistic regression model used to estimate the healthcare professional characteristics independently related with the opinion of extending the school vaccinating program.
Table 2.
Univariate and multivariate analyses extracted from the logistic regression model used to estimate the healthcare professional characteristics independently related with the opinion of extending the school vaccinating program.
| Covariates | Univariate analysis | Multivariate analysis | ||
|---|---|---|---|---|
| * | p-value | OR (95% CI) | p-value | |
| Grade of relevance of paediatric vaccination against influenza (1), | 0.35 | <0.001 | 0.42 (0.30-0.59) | <0.001 |
| Involved in paediatric vaccination of children from 6 to 59 months (2) | 88.4% | 0.457 | - | - |
| Age (3) | 0.363 | |||
| <20 | 4.0±0.0 | - | - | |
| 20-29 | 3.9±1.5 | - | - | |
| 30-39 | 4.4±1.0 | - | - | |
| 40-49 | 4.2±1.2 | - | - | |
| 50-59 | 3.9±1.4 | - | - | |
| >60 | 4.1±1.3 | - | - | |
| Profession (4) | ||||
| Medical group | 27.4% | <0.001 | 0.40 (0.23-0.70) | 0.001 |
| Nursing group | 72.6% | |||
| Sex (5) | ||||
| Female | 89.0 % | 0.143 | - | - |
| Male | 11.0 % | |||
| General rating of intranasal vaccine (2) | 0.19 | 0.005** | - | - |
| Participation in pilot experience (2) | 13.8% | 0.003 | 0.26 (0.12-0.57) | <0.001 |
| Ease/convenience of intranasal vaccine (1) | ||||
| 1-3 | 3.2±1.6 | 0.004 | 0.48 (0.17-1.35) | 0.164 |
| 4-5 | 4.2±1.2 | |||
| Ease/convenience of intramuscular vaccine (1) | ||||
| 1-3 | 4.0±1.3 | 0.259 | - | - |
| 4-5 | 4.2±1.2 | |||
*Values in the univariate analysis are presented by statistical dispersion measures (mean±standard deviation), frequency (%), and correlation coefficient, depending on the type of covariate analysed. **The variable “general rating of intranasal vaccine” resulted significant in the univariate analysis but was not included in the multivariate analysis due to it is already related to another covariate included in the model. (1) For these variables no reference categories are indicated. The values in the univariate analysis represent the change in the dependent variable considering 1 point increase in the numerical covariate (independent); (2) Reference category: No, (3) Reference category: >60 years, (4) Reference category: Nursing group, (5) Reference category: male.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



