
Submitted:
23 April 2024
Posted:
25 April 2024
You are already at the latest version
Abstract
(1)Background: Fascioliasis is considered a neglected tropical disease affecting an estimated 17 million people in more than 70 countries worldwide. The highest prevalence of human fascioliasis is found in regions where livestock farming and consumption of raw or undercooked freshwater plants are common, such as parts of Africa, Asia, Europe, and Latin America. It is responsible for over 90,000 disability-adjusted years of life due to associated abdominal complications. We conducted a study to investigate the prevalence of human fascioliasis through a systematic review and meta-analysis of all available literature in Sun-Saharan Africa.(2). Methods: We screened a total of 126 publications using pubmed online search engine databases; Web of Science and CAB for articles published within a 20-year period between 2000 and 2022. We used a comprehensive search method using a combination of terms, parasite and disease names. The initial search resulted in a screening of articles by title, abstracts and full texts. The relevant information on the prevalence of human fascioliasis in Africa was extracted. Of the 126 publications, 33 articles were selected for meta-analysis. The essential information required was extracted from these documents and determined through statistical analysis in Microsoft Excel for calculating the prevalence of human fascioliasis in sub-Saharan Africa. The variance of each study was assessed using a bimodal distribution and heterogeneity assessment using a I2 index. Analysis was performed using random effects models.(3)Results: A total of 271 articles were searched through the database search and 33 articles were eligible studies that provided qualitative information on the prevalence of human fascioliasis in Africa. These make up 12.17% (n=33). The pooled prevalence estimates for human fascioliasis are 0.032% (IVhet PPE: 0.032% (95%CI 1.4-6.53). The highest prevalence rate was observed in Egypt with a prevalence of 100%. The prevalence of human fascioliasis is very high in some sub-Saharan countries, partly due to neglect of diagnostics, demonstrating the bias of available information for decision-making in human fascioliasis across Africa, given the spatial presence, scarcity and incompleteness are region.(4)Conclusions: The prevalence of Human fascioliasis is very high in some Sub-Saharan Countries partly due to neglect in diagnostics. This presents how highly focal with spatial occurrences, scarcity and patchy the available information for decision making is on Human fascioliasis across the Sub-Saharan African region.
Keywords:
human-fascioliasis
; prevalence
; epidemiology
; Africa
; One-Health
The Scoping Review and Analysis Has Observed the Following Strengths and Limitations
The rigorous and comprehensiveness search methodology of existing studies provided large datasets for standardized statistical pool analysis where a robust conclusion was drawn.
The review highlighted the current burden of fascioliasis in humans in Africa.
There is increased generalizability as datasets were derived from a collection of multiple African countries and longer identification of trends over time (2000-2022). This increased the statistical power and reduced bias.
There shortcomings to this review by the impossibility of disaggregating the datasets relating to sample sizes, diagnostic methods, data scarcity from African Countries, heterogeneity due to environmental, cultural and socioeconomic factors of the disease that affect drawing conclusions.
Introduction
Fascioliasis is a parasitic zoonosis caused by liver flukes of the genus Fasciola that infects both humans and ruminants worldwide [1,2,3]. Human fascioliasis infection causes significant liver obstruction and biliary inflammation in affected patients [1,2,3]. The disease occurs in travelers and immigrants from endemic areas and in sporadic outbreaks due to environmental or social changes. Worldwide, over 17 million people are infected and 180 million are at risk of infection, from over 70 countries including Europe, Asia, Africa, Oceania and the Americas worldwide [1,2,3]. The global burden is underestimated due to the lack of reliable diagnostic tools and monitoring systems as well as low awareness and recognition among health professionals and the general public [4,5,6]. This parasite has a complex life cycle involving an intermediate host of the family Lymnaeidae [1,2,3], an aquatic freshwater plant that acts as a carrier, and a mammalian host like Sheep, goats, cattle and humans [1,2,3]. The infection is responsible for the development of symptoms such as urticaria, eosinophilia and malaise and can also lead to chronic diseases in humans and ruminants [1,2,3]. Human fascioliasis infections are becoming a neglected zoonotic disease across Africa [1,2,3] and are responsible for over 90,000 disability adjusted life years (DALYS) lost associated abdominal complications [1,2,3].
The prevalence of human fascioliasis infections has been reported in over 17 African countries, including Algeria [7], Angola [7], Cape Verde Islands [7], Chad, Egypt, Ethiopia, Djibouti [7], Ghana [7], Libya [8], 1998), Morocco [8], Nigeria, Senegal [9], South Africa [10], Swaziland [10], Tunisia [11], the United Republic Tanzania [12] and Zimbabwe [13] in Africa [1,2,3], which negatively affects the good health of the human and animal population [14].The Epidemiology of fascioliasis depends on the intermediate host snails of the family Lymnaeidae. Diagnosis relies on a number of techniques; using the standard sedimentation method of stool samples for egg concentration, followed by microscopy [15], coproantigen testing using stool samples [16] and antibody detection in blood serum using ELISA [17,18], meat inspections [19] through morphological identification of the adult Fasciola parasites with F.gigantica with a typical, leaf-shaped, dorsoventrally flattened, longer, narrower body of 28–52mm, while F. hepatica is significantly shorter at 12–29mm [20,21]. PCR-based tools provide the best molecular markers for diagnosing and distinguishing the two types of Fasciola infections [22,23,24] in Lymnaeid Snails [25].
The prevention and control of fascioliasis in both animals and humans depends heavily on the use of antiheminthic, with the following approved for regular deworming of animals: triclabendazole, closantel or nitroxynil and the use of triclabendazole in both chronic and acute forms of human infections [26,27]. In addition, health education campaigns aimed at empowering farmers to practice animal hygiene and ensure regular deworming are crucial, alongside established surveillance systems to detect, monitor and report outbreaks. Freshwater snails of the Lymnaeid group play an important role in the maintenance and transmission of fascioliasis [25,28], which has a significant economic impact [29] and biomedical burden [13] worldwide, especially in bovine fascioliasis [30,31]. The transmission potentials are favored by the local tolerance of Lymnaeid snails [32], which therefore requires a precise localization of their epidemiological distribution and identification, which is crucial to combat the infections.
In animals, the infection tends to show a notable reduction in milk production as well as weak reproductive rates [33] with significant associated costs of treatment and meat condemnation, which represent a very large economic loss to the farmer [34,35,36]. While human infections are reported as symptomatic, more non-specific symptoms such as fever, abdominal pain, diarrhea and nausea are reported in individuals during the acute or chronic form of the infections [37,38]. Many studies have documented the prevalence of the infection in domestic and wild populations throughout Africa [39]. However, there is little data on its prevalence in humans across the African region.
Methods and Methods
This study aimed to investigate the prevalence of human fascioliasis through a systematic review and meta-analysis of all available literature in the African region during 2000-2022. The primary outcome of the systematic review and meta-analysis should be available datasets on the prevalence of human fascioliasis in Africa. Secondary outcomes included reviewing available diagnostic methods to estimate the prevalence of infections across the African region.
Information sources and searching approach: A systematic review was performed with the objective of mapping out all the relevant literature needed for the study on Human fascioliasis and intermediate vector snails across Africa. All the publications relevant over 20 year period between 2000-2022were searched using the databases from pubmed, web of science and CAB. The study conducted an online search using the following words “fascioliasis,” “human fascioliasis,” “zoonosis,” “Fasciola liverfluke,” “Fasciola hepatica,” “Fasciola gigantic,” “human fascioliasis epidemiology,” “human fascioliasis distribution,” “research trends in “human fascioliasis,” and “fascioliasis outbreaks in Africa”
Study Materials and Eligibility: All the datasets required for this review were generated from the various databases and later merged into a single one. This helped remove and eliminate duplicate downloads from the records. The reviews were sorted by title and abstract. All articles that focused on non-human fascioliasis and Lymnaeid datasets will be removed from the analysis. The full texts of the remaining study texts follow the admission criteria. The following criteria were used to exclude the reviewed studies:
Reporting parasites other than F.gigantica or F.hepatica across Africa.
Duplicate datasets were removed from the analysis.
All of these followed the PRISMA guideline for reporting systematic and meta-analysis reviews as previously described [40].
Data processing and quality assessments: All retrieved articles were classified based on the following characteristics: study period, population, prevalence, diagnostics used, observed outcomes, and risk factors associated with human fascioliasis. While species identified in the Lymnaeid snails are included in the study, the numbers infected with Fasciola infections are checked. This study also considered article publication years for impact factor and index citations. All records were entered into preformatted tables. The study also conducted quality assessments for all population-based human fascioliasis surveys using the Prevalence Critical Appraisal Tool [41].
Summary measures and synthesis of results: The study examined a total of 126 publications. All populations based on the studies were screened for a descriptive analysis of the populations infected with human fascioliasis to determine the proportion of infected individuals. The magnitude of significance associations was determined using Wilson’s score at 95%CI for subjects infected with fascioliasis. We performed chi-square tests to determine associations between risk factors for fascioliasis infections in humans and their presence. Odds ratios and associated Wilsons score at 95%CI were also determined.
Results
A total of 271 articles were searched through the database search. An additional 10 records were identified from other sources and 33 articles were eligible studies that provided qualitative information on the prevalence of human fascioliasis in Africa (Figure 1). After duplicate records were deleted from the system database, a total of 85 records were retained and subjected to a further verification process. At this point, we determined that 26 datasets were ineligible based on the exclusion criteria and were excluded from the final qualitative review and analysis. The final database contained a total of 33 articles that were considered for further synthesis. In total, a total of 33 (n=33) articles were included for full review in the systematic and meta-analytic review of human fascioliasis. Of 26 (n=26) studies, 78.8% were from Egypt, seven were from Nigeria (n=07), which 21.2%, while a single study was conducted in the remaining countries where studies on human fascioliasis were conducted including Angola (n=01), Ethiopia (n=01), Ghana (n=01), South Africa (n=01), Tanzania (n=01) and Tunisia (n=01).
Figure 1.
Showing PRISMA Flow of Study Selection. Studies were assessed using a 10-point Quality Index scorecard (Qi). Results were rated on a scale of 1-4 as low, 5-6 as moderate and 7-10 as high. The final analysis revealed that 9 studies from Egypt (n=06), Nigeria (n=02) and Tunisia (n=01) were rated as high. The majority (n=20) of studies from Egypt (n=14), Nigeria (n=02), South Africa (n=03) were rated as low and thirteen from Angola (n=01) were rated as moderate. Egypt (n=06), Ethiopia (n=01), Ghana (n=01), Nigeria (n=01) and Tanzania (n=01).
Figure 1.
Showing PRISMA Flow of Study Selection. Studies were assessed using a 10-point Quality Index scorecard (Qi). Results were rated on a scale of 1-4 as low, 5-6 as moderate and 7-10 as high. The final analysis revealed that 9 studies from Egypt (n=06), Nigeria (n=02) and Tunisia (n=01) were rated as high. The majority (n=20) of studies from Egypt (n=14), Nigeria (n=02), South Africa (n=03) were rated as low and thirteen from Angola (n=01) were rated as moderate. Egypt (n=06), Ethiopia (n=01), Ghana (n=01), Nigeria (n=01) and Tanzania (n=01).
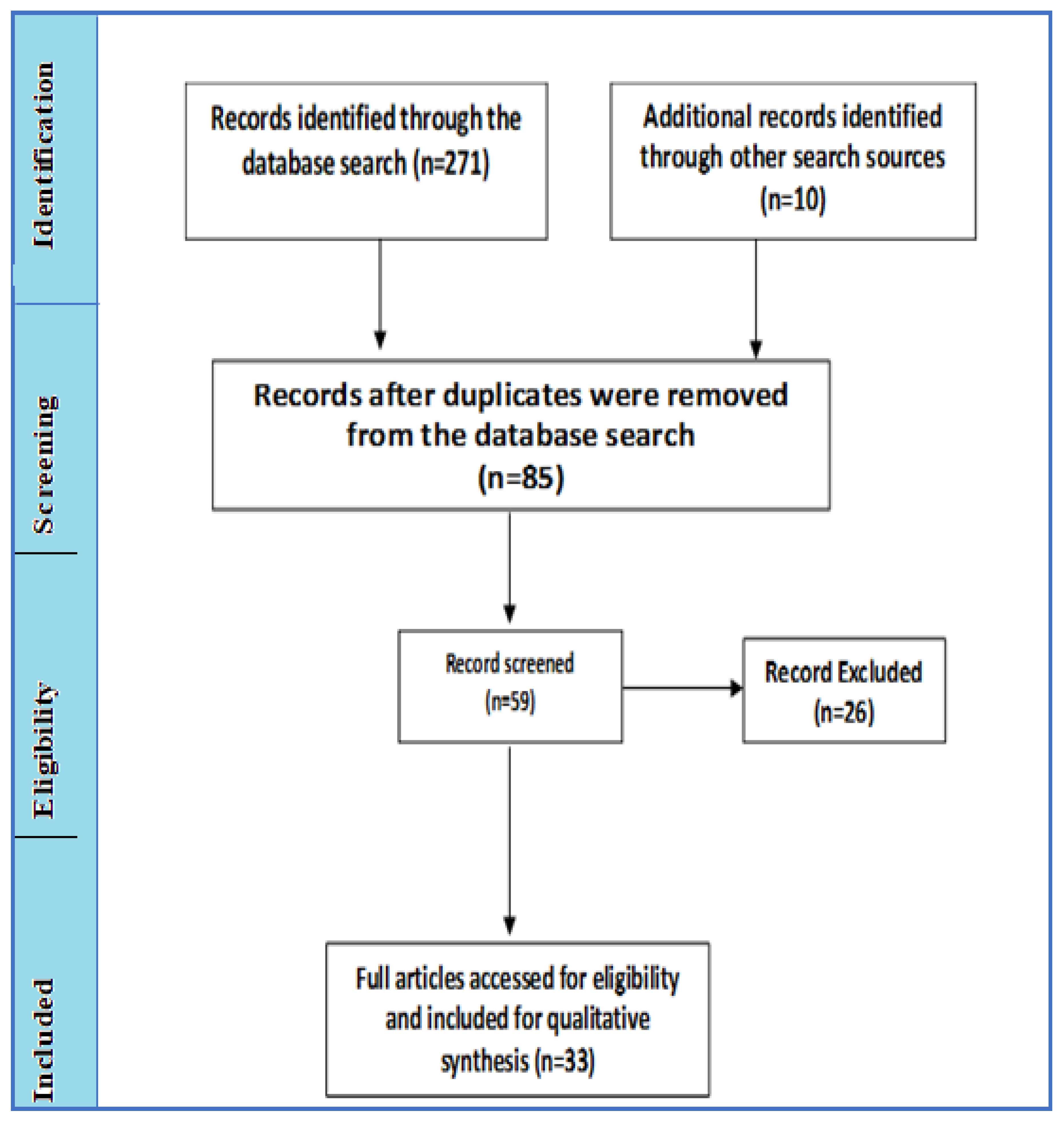

Table 1.
Showing characteristics of the Studies included in the Qi Analysis on human Fascioliasis across Africa 2000-2022.
Table 1.
Showing characteristics of the Studies included in the Qi Analysis on human Fascioliasis across Africa 2000-2022.
| Author Name | Sample Size & (%) | Country | Year | Article type | %Qi | Evaluation | Citation |
|---|---|---|---|---|---|---|---|
| Abaver et al.,2012 | 480(1.04) | Nigeria | 2012 | Clinical Reviews | 50.0 | low | [42] |
| Abo-Madyan et al.,2004 | 1,019(1.67) | Egypt | 2004 | clinical trial | 50.0 | low | [43] |
| Abou-Basha et al.,2000 | 2,492(4.45) | Egypt | 2000 | Clinical Reviews | 40.0 | low | [44] |
| Adarosy et al.,2013a | 1,868(0,59) | Egypt | 2013 | clinical trial | 30.0 | low | [45] |
| Adarosy et al.,2013b | 1,868(1.07) | Egypt | 2013 | clinical trial | 30.0 | low | [45] |
| Adarosy et al.,2013c | 1,868(0.75) | Egypt | 2013 | clinical trial | 30.0 | low | [45] |
| Arinola et al.,2015 | 349(0.29) | Nigeria | 2015 | Impact Evaluation | 37.5 | high | [46] |
| Black et al. 2013a | 3(33.33) | South Africa | 2013 | Case report article | 30.0 | low | [47] |
| Black et al.,2013b | 3(66.67) | South Africa | 2013 | Case report article | 30.0 | low | [47] |
| Curtale et al.,2000 | 8,854(2.88) | Egypt | 2000 | Parasitological Reviews | 62.5 | moderate | [48] |
| Curtale et al.,2003 | 1,331(5.41) | Egypt | 2003 | Crossectional Survey | 80.0 | low | [49] |
| de Alegría et al.,2017 | 372(0.27) | Angola | 2017 | Crossectional Survey | 100.0 | moderate | [50] |
| El Shazly et al.,2006 | 3,180(4.78) | Egypt | 2006 | Parasitological Survey | 12.5 | high | [51] |
| El-Karaksy et al.,2018 | 4,475(0.85) | Egypt | 2018 | Clinical Reviews | 37.5 | high | [52] |
| el-Shazly et al.,2001 | 605(52.56) | Egypt | 2001 | clinical trial | 37.5 | moderate | [53] |
| El-Shazly et al.,2002a | 1,000(8.20) | Egypt | 2002 | Serological Evaluation | 50.0 | moderate | [54] |
| El-Shazly et al.,2002b | 6(33.33) | Egypt | 2002 | Rectal Biospy | 50.0 | moderate | [55] |
| el-Shazly et al.,2006 | 1,000(0.40) | Egypt | 2006 | Clinical Reviews | 37.5 | low | [54] |
| El-Shazly et al.,2009 | 3,000(3.27) | Egypt | 2009 | Clinical Reviews | 33.3 | low | [53] |
| Esteban et al.,2003 | 678(19.03) | Egypt | 2003 | Clinical Reviews | 70.0 | low | [56] |
| Fawzi et al.,2004 | 575(2.43) | Egypt | 2004 | Public Health Reviews | 55.6 | moderate | [57] |
| Fawzi et al.,2004 | 575 | Egypt | 2004 | Crossectional Survey | 50.0 | high | [57] |
| Fentie et al.,2013 | 520(3.27) | Ethiopia | 2013 | Crossectional Survey | 90.0 | moderate | [58] |
| Hammami et al.,2007 | 30(6.67) | Tunisia | 2007 | Crossectional Survey | 25.0 | high | [59] |
| Ihesiulor et al.,2013 | 570(0.88) | Nigeria | 2013 | Parasitological Reviews | 37.5 | moderate | [60] |
| Ijagbone et al.,2006 | 533(0.56) | Nigeria | 2006 | Parasitological Survey | 44.4 | moderate | [61] |
| Keiser et al.,2011 | 1,215(3.37) | Egypt | 2011 | clinical trial | 62.5 | moderate | [62] |
| Lukambagire et al.,2015 | 1,460(20.89) | Tanzania | 2015 | Crossectional Survey | 55.6 | moderate | [12] |
| Mas-Coma.2004 | 7,071(6.84) | Africa | 2004 | research article | 30.0 | low | [39] |
| Mekky et al.,2015a | 23(8.70) | Egypt | 2015 | research article | 25.0 | low | [63] |
| Mekky et al.,2015b | 23(100) | Egypt | 2015 | research article | 80.0 | high | [63] |
| Mekky et al.,2015c | 23(100) | Egypt | 2015 | research article | 80.0 | high | [63] |
| Mekky et al.,2015d | 23(65.22) | Egypt | 2015 | research article | 80.0 | high | [63] |
| Mekky et al.,2015e | 23(13.04) | Egypt | 2015 | research article | 37.5 | low | [63] |
| Mekky et al.,2015f | 23(13.04) | Egypt | 2015 | research article | 37.5 | low | [63] |
| Na’acha et al.,2017 | 438(0.46) | Nigeria | 2017 | Crossectional Survey | 50.0 | high | [64] |
| Nxasana et al.,2013 | 162(0.62) | South Africa | 2013 | Crossectional Survey | 87.5 | low | [65] |
| Okaka et al.,2000 | 6,430(2.32) | Nigeria | 2000 | Public Health Reviews | 25.0 | moderate | [66] |
| Osman et al.,2011 | 6,214(2.29) | Egypt | 2011 | Impact Evaluation | 62.5 | low | [67] |
| Periago et al.,2021 | 6,657(1.44) | Egypt | 2021 | Crossectional Survey | 12.5 | high | [68] |
| Shitta et al.,2017 | 254(33.07) | Nigeria | 2017 | Crossectional Survey | 50.0 | low | [69] |
| Soliman,2008 | 3,000(3.0) | Egypt | 2008 | research article | 30.0 | low | [70] |
| Squire et al.,2018 | 95(1.05) | Ghana | 2018 | Parasitological Survey | 50.0 | moderate | [71] |
The pooled prevalence estimates (PPE) for human fascioliasis were 0.032% and the inverse variance quasi likelihood based alternative pooled prevalence estimates (IVhet PPE) at 0.032% (95% CI 1.4-5.3) and the statistic meta-analysis of prevalence worthwhile or worthless (I2) estimated at 98.7% (95% CI; 98.548-98.859) with Chi2, p=0.000.
Figure 2.
Showing Forest Plot for PPE Analysis for Human Fascioliasis in Africa for period 2000-2022.
Figure 2.
Showing Forest Plot for PPE Analysis for Human Fascioliasis in Africa for period 2000-2022.
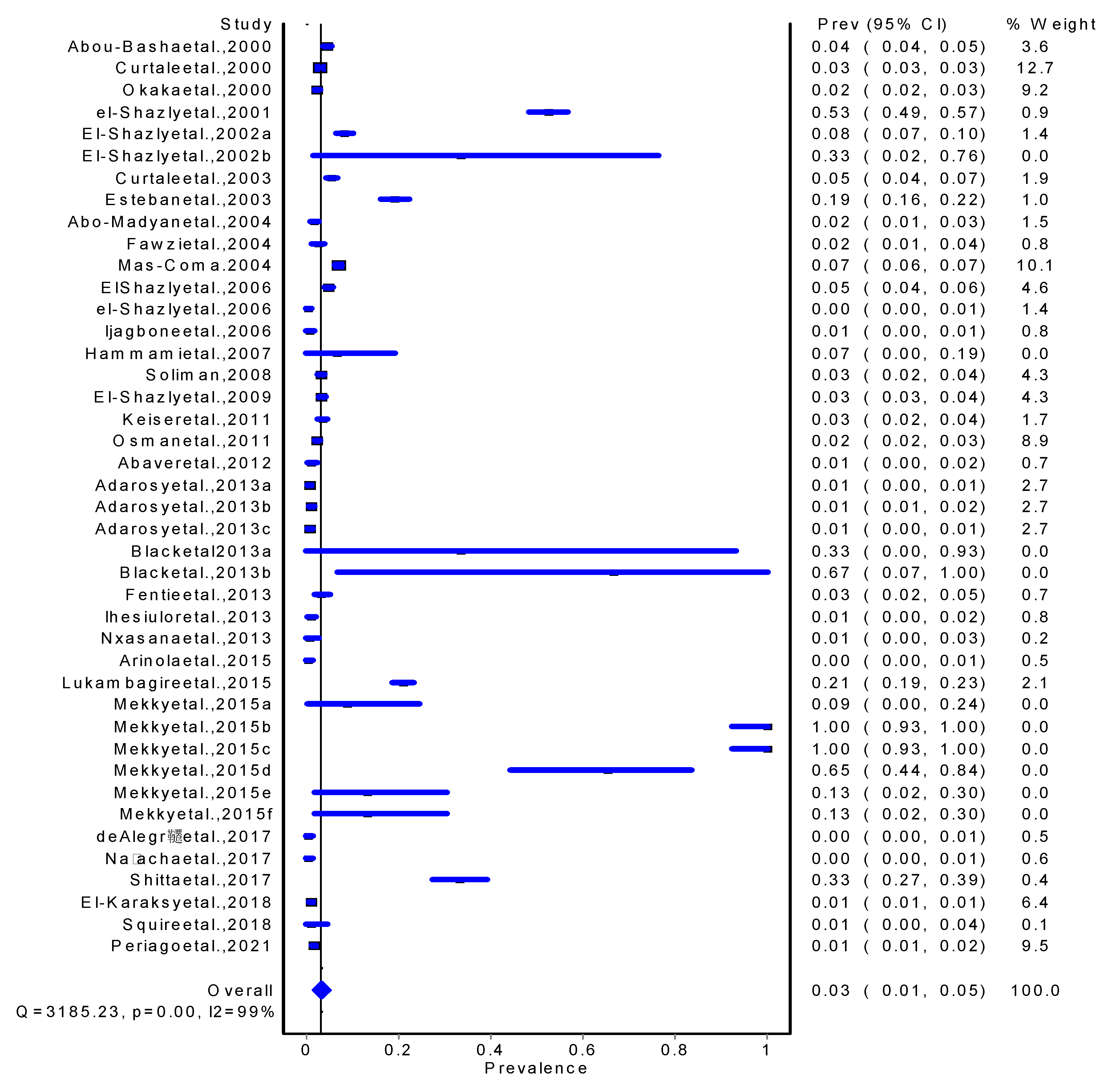
Figure 3.
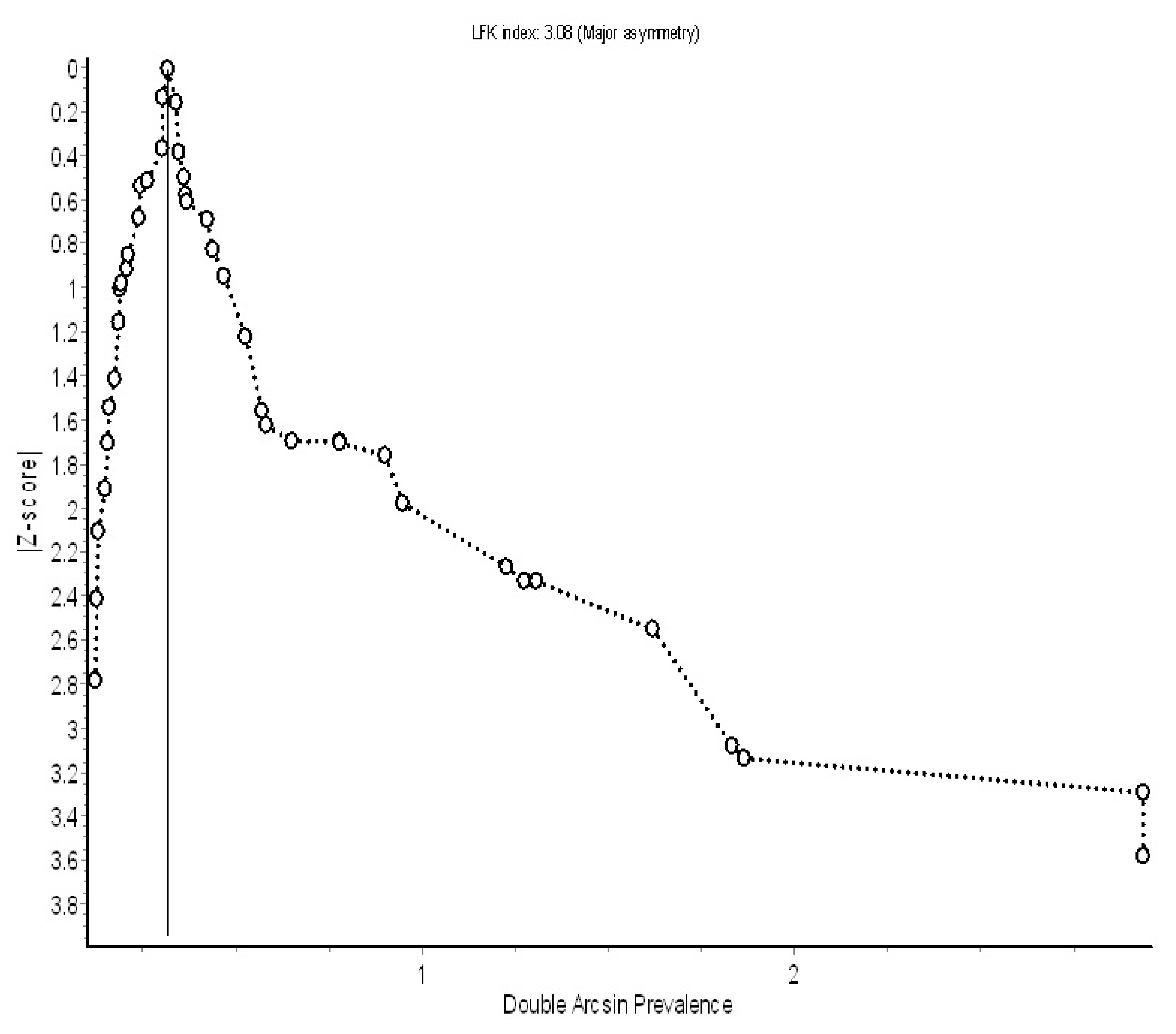
Showing Funnel plot of the double arcsine transformed prevalence estimates of for Human Fascioliasis in Africa for period 2000-2022.
Figure 3.
Showing Funnel plot of the double arcsine transformed prevalence estimates of for Human Fascioliasis in Africa for period 2000-2022.
Discussions
Human fascioliasis is a parasitic disease caused by the liver fluke Fasciola hepatica or Fasciola gigantica. The disease affects people in over 70 countries worldwide, with an estimated 2.4 million people infected worldwide. In Africa, fascioliasis occurs primarily in areas where livestock grazing is common, such as the Nile Valley, the Ethiopian Highlands, and South Africa. The epidemiology of human fascioliasis in Africa is influenced by several environmental, ecological and climatic factors that influence the growth, development and survival of the parasite and its intermediate host. The disease has been shown to be a major plant-borne zoonosis in the high-altitude Andean rural regions of Bolivia and Peru [72], in the northern provinces of Iran bordering the Caspian Sea [73,74], Nile Delta region of Egypt [75] and Central provinces of Vietnam [76].
The results of our analysis and review suggest that several epidemiological studies on the transmission of human fascioliasis have been conducted in Africa [7,77]. This adds to the growing evidence that human fascioliasis infections are becoming a problem Across Africa as described in Egypt [70,72,78], Ethiopia [79,80,81], South Africa [47], Tanzania [82], Angola [83], Nigeria [7,84], Senegal [7], Ghana [7,85], Morocco [7,8], Algeria [7,86] and Tunisia [7,79,87]. This increase trend of infections and spread across African region could be due to a shift in consumption of raw vegetables and raw or partially cooked liver [88] and also the presence of available intermediate hosts of snails. The analysis further indicates that the trend of human fascioliasis in Africa varies depending on local conditions and transmission patterns; this has been observed to spread across the African region with significant adaptations by the intermediate Vector snails as previously described [89,90]. The transmission of the disease is primarily zoonotic, with people becoming infected through consumption of contaminated watercress or other vegetables [79].
Our analysis and reviews have further pointed that transmission is predominantly described as zoonotic and anthroponotic [79,91]. The overall trend analysis across Africa indicateda generally low and stable transition between 2-5 publication reported on Human Fascioliasis from 2000-2012 and a significant swift upto 10 publications from 2012-2015 and steady drop to 2 publications in 2021. For example, in Egypt over twenty six publications on human fascioliasis reported and Nigeria with seven on human fascioliasis reportedpublications which correspond to the Fascioliasis outbreaks.The epidemiology is also influenced by socioeconomic factors and public health interventions. Indeed our analysis revealed that Poverty, poor sanitation and lack of access to clean water is major driver to increased risk of infection with the parasite across all observed countries with reported cases [7,39].
One Health epidemiological underpinning for this scoping review in Africa: This study has highlighted epidemiological setting categorization into rural, urban, or rural-urban that drives the emergent zoonosis [92]. The people from the low- to middle-income countries are more likely to suffer from fascioliasis whereas those residents from developed countries are likely to become infected if they feed on imported infested vegetable plants that evade quarantine measures [92,93]. Similar observation have been reported in this scoping review especially during field trips to endemic countries, city dwellers were at high risk of infection due to fascioliasis [93,94]. The human feeding and dietary habits are also another cause to weary especially when the source of food and water consumed are linked to marsh vegetations with open and free range animal husbandry practices [94], this scoping review has highlighted this an important epidemiological factor of human fascioliasis. The unregulated and uncontrolled supplies of vegetable products (such as carrots, cucumbers, cabbage, onions, tomatoes, spinach, etc.) to markets coupled with drinking contaminated water and fruit drinks/juices made from local plants make humans vulnerable to infection as previously documented [94].
One Health Concept of the Fascioliasis Prevention and Control in Africa: One Health approach recognizes the interconnections between human health, animal health, and the environment, emphasizing the need for collaborative efforts across disciplines to address complex health issues like fascioliasis [95,96].The diagnosis relies on a number of techniques; with the standard sedimentation method of faecal samples for eggs concentration followed by microscopy [15], coproantigen tests using feacal samples [16] and antibody detections in blood serum by ELISA [17,18], Meat inspections [19] by morphological identifications of the adult Fasciola parasites with Fasciola hepatica with a typical leafy shaped dorso-ventrally flattened longer-narrower body measuring 28-52mm whilst Fasciola hepatica shorter measuring 12-29mm [20,21]. PCR based tools provide the best molecular markers for diagnosing and differentiating the two species of Fasciola infections [22,23,24] in Lymnaeid snails [25]. The prevention and control of Fascioliasis in both animal and human populations relies heavily on the use of antiheminthic drugs with the following approved for regular deworming of animals: triclabendazole, closantel or nitroxynil and use of triclabendazole in both chronic and acute forms of human infections [26,27]. Additionally, health education campaigns geared at equipping farmers to practice animal hygiene and ensure regular deworming alongside established surveillance systems to detect, monitor and report outbreaks are key and vital.
Observed theoretical Gap: Fascioliasis is an emerging neglected zoonotic disease [13,97] affecting the health and wellbeing of humans and animals [97,98]. The burden of the infection is not well defined with studies showing geographical expansion of the disease in human-animal population due to climate change [99,100,101,102]. This is likely to be uncovered through increase awareness and continued surveillance systems [103]. There is need for research in new adjuvants/therapeutic agents to tackle the challenges of emerging resistance to triclabendazole treatment. Future research into genomics and molecular biology could be a fruitful area of investigations to bridge the theoretical gap in treatments.
Observed methodological Gap: There are studies that have assessed the global linkage of climate change [97] and annual prevalence of Fasciolasis at 0.45% (95%CL: 0.35-0.56) [104]. Other studies by [105] were able to highlight the significant role played by bibliometric document visualization and analysis where reporting steady increases in publications which corresponds to the Fascioliasis outbreaks between 1913 to 2021 although there was a sharp increase reported between 1965 to 1985 that explains the deadly outbreak in Britain and Europe at the time [105].These findings are similar to trends observed in our analysis reported here. There is lack of a standardized diagnostic tool as many diagnostics are reportedly used in different scenarios ranging from microscopy, serological tests and ELISA each with varying degrees of sensitivities and specificities. There are challenges in the differential assessments of acute versus chronic infections as well as differentiating a symptomatic and subclinical form of the disease which are missed during the surveys [106]. There are gaps in the reliability of data collection systems that incorrectly capture and report data often siloed to veterinary level reporting.
Conclusion
In summary, the epidemiology of human fascioliasis in Africa is complex and influenced by various factors. A better understanding of the epidemiology of the disease is critical to developing effective control strategies and reducing the burden of disease in affected communities. Mass administrations of drugs, improved sanitation, and health education programs have been effective in reducing the prevalence of human fascioliasis in some countries. However, sustained efforts are needed to control the disease in areas where it remains a public health problem. The results suggest that the burden of disease is underestimated due to a number of factors; Lack of reliable diagnostic tools, adequate surveillance systems, lack of denominator for cases tracked, low awareness and recognition among health professionals and the general public. This requires increased multispectral collaboration using a One Health approach.
Fascioliasis has emerged as an important foodborne disease with human and zoonotic importance. Climate change together with emerging drug resistance and development of new parasite strains through hybridization are becoming serious threats and challenges likely to impact and potentially change the climate driven epidemiology of Fascioliasis disease in years to come. Therefore, its prudent that researchers must double the synergies towards research and innovations to develop promising vaccines that will be the margin bullet to provide the maximum required protection to livestock and humans.
Author Contributions
MA: EMT,MBM, DM,SN,PV,LM, MP, TM, KC, Conceptualized and designed the study, MA, EMT,MBM, DM, SN,PV,LM, MP, TM, KC, SM, MJC, ASS and BV, MA, EMT,MBM, DM, SN,PV,LM, MP, TM, collected the data, prepared it and proposed an analysis plan and interpreted the results. MA, EMT,MBM, DM, SN, PV and LM wrote the first drafted the manuscript. All the authors read, revised and approved the final manuscript.
Funding
This manuscript is part of PhD write up and the PhD study received financial support from the European Union’s Horizon 2020 research and innovation program under grant agreement No. 101000365.
Institutional Review Board Statement
Data used in the current study were generated from already published articles and followed the guidelines for systematic review and meta-analysis guideline and appropriate acknowledgements to authorship cited.
Informed Consent Statement
Not applicable
Data Availability Statement
The datasets generated and analyzed during the review are available and attached. Further details are on satisfactory request.
Acknowledgments
The authors thank for their contribution to this manuscript. We also acknowledge the contribution of all authors whose work citations provided us with a solid basis for these systematic reviews and analyzes of the manuscript. This scholarship received financial support from the European Union’s Horizon 2020 research and innovation program under grant agreement No. 101000365.
Conflicts of Interest
The authors declare that there are no conflicts of interest in the authorship of this publication.
References
- Mehmood, K., et al., A review on epidemiology, global prevalence and economical losses of fasciolosis in ruminants. Microbial pathogenesis, 2017. 109: p. 253-262. [CrossRef]
- Cwiklinski, K., et al., A prospective view of animal and human Fasciolosis. Parasite immunology, 2016. 38(9): p. 558-568. [CrossRef]
- Saleha, A., Liver fluke disease (fascioliasis): epidemiology, economic impact and public health significance. Southeast Asian J Trop Med Public Health, 1991. 22(361): p. 4.
- Newell, D.G., et al., Food-borne diseases—the challenges of 20 years ago still persist while new ones continue to emerge. International journal of food microbiology, 2010. 139: p. S3-S15. [CrossRef]
- Nyindo, M. and A.H. Lukambagire, Fascioliasis: An Ongoing Zoonotic Trematode Infection. Biomed Res Int, 2015. 2015: p. 786195. [CrossRef]
- Johansen, M.V., et al., Towards improved diagnosis of zoonotic trematode infections in Southeast Asia. Advances in Parasitology, 2010. 73: p. 171-195. [CrossRef]
- Dermauw, V., et al., Human fascioliasis in Africa: A systematic review. PLoS One, 2021. 16(12): p. e0261166. [CrossRef]
- Farag, H.F., Human fascioliasis in some countries of the Eastern Mediterranean Region. EMHJ-Eastern Mediterranean Health Journal, 4 (1), 156-160, 1998, 1998. [CrossRef]
- Ashrafi, K. and S. Mas-Coma, Fasciola gigantica transmission in the zoonotic fascioliasis endemic lowlands of Guilan, Iran: experimental assessment. Vet Parasitol, 2014. 205(1-2): p. 96-106. [CrossRef]
- Malatji, M., D. Pfukenyi, and S. Mukaratirwa, Fasciola species and their vertebrate and snail intermediate hosts in East and Southern Africa: a review. Journal of helminthology, 2020. 94. [CrossRef]
- Ashrafi, K., et al., Fascioliasis: a worldwide parasitic disease of importance in travel medicine. Travel Med Infect Dis, 2014. 12(6 Pt A): p. 636-49. [CrossRef]
- Lukambagire, A.H., D.N. McHaile, and M. Nyindo, Diagnosis of human fascioliasis in Arusha region, northern Tanzania by microscopy and clinical manifestations in patients. BMC Infect Dis, 2015. 15: p. 578. [CrossRef]
- Nyindo, M. and A.-H. Lukambagire, Fascioliasis: an ongoing zoonotic trematode infection. BioMed research international, 2015. 2015. [CrossRef]
- Addy, F., T. Romig, and M. Wassermann, Genetic characterisation of Fasciola gigantica from Ghana. Veterinary Parasitology: Regional Studies and Reports, 2018. 14: p. 106-110. [CrossRef]
- Calvani, N.E.D., et al., Scrambled eggs: A highly sensitive molecular diagnostic workflow for Fasciola species specific detection from faecal samples. Plos Neglected Tropical Diseases, 2017. 11(9): p. e0005931. [CrossRef]
- Kajugu, P.-E., et al., Fasciola hepatica: Specificity of a coproantigen ELISA test for diagnosis of fasciolosis in faecal samples from cattle and sheep concurrently infected with gastrointestinal nematodes, coccidians and/or rumen flukes (paramphistomes), under field conditions. Veterinary parasitology, 2015. 212(3-4): p. 181-187. [CrossRef]
- Salimi-Bejestani, M., et al., Development of an antibody-detection ELISA for Fasciola hepatica and its evaluation against a commercially available test. Research in veterinary science, 2005. 78(2): p. 177-181. [CrossRef]
- Cabán-Hernández, K., et al., Development of two antibody detection enzyme-linked immunosorbent assays for serodiagnosis of human chronic fascioliasis. Journal of Clinical Microbiology, 2014. 52(3): p. 766-772. [CrossRef]
- Khaitsa, M.L., J. Hammond, and J. Opuda-Asibo, Use of meat inspection records in veterinary planning. Bulletin of animal health and production in Africa, 1994.
- Kendall, S., Relationships between the species of Fasciola and their molluscan hosts. Advances in parasitology, 1970. 8: p. 251-258. [CrossRef]
- Periago, M., et al., Phenotypic comparison of allopatric populations of Fasciola hepatica and Fasciola gigantica from European and African bovines using a computer image analysis system (CIAS). Parasitology research, 2006. 99(4): p. 368-378. [CrossRef]
- McGarry, J., et al., PCR-based differentiation of Fasciola species (Trematoda: Fasciolidae), using primers based on RAPD-derived sequences. Annals of Tropical Medicine & Parasitology, 2007. 101(5): p. 415-421. [CrossRef]
- Rokni, M.B., et al., Identification and differentiation of Fasciola hepatica and Fasciola gigantica using a simple PCR-restriction enzyme method. Experimental Parasitology, 2010. 124(2): p. 209-213. [CrossRef]
- Ai, L., et al., Specific PCR-based assays for the identification of Fasciola species: their development, evaluation and potential usefulness in prevalence surveys. Annals of Tropical Medicine & Parasitology, 2010. 104(1): p. 65-72. [CrossRef]
- Mas-Coma, S., M.A. Valero, and M.D. Bargues, Fasciola, lymnaeids and human fascioliasis, with a global overview on disease transmission, epidemiology, evolutionary genetics, molecular epidemiology and control. Advances in parasitology, 2009. 69: p. 41-146. [CrossRef]
- FAO, Foodborne parasitic infections: Fascioliasis Fact sheet. https://www.fao.org/3/cb1127en/cb1127en.pdf, accessed on 22/12/2021. 2021.
- WHO, A key role for veterinary authorities and animal health practitioners in preventing and controlling neglected parasitic zoonoses: a handbook with focus on Taenia solium, Trichinella, Echinococcus and Fasciola. 2021.
- Correa, A.C., et al., Bridging gaps in the molecular phylogeny of the Lymnaeidae (Gastropoda: Pulmonata), vectors of Fascioliasis. BMC evolutionary biology, 2010. 10(1): p. 1-12. [CrossRef]
- Arias-Pacheco, C., et al., Economic impact of the liver condemnation of cattle infected with Fasciola hepatica in the Peruvian Andes. Tropical animal health and production, 2020: p. 1-6. [CrossRef]
- Khan, M.K., et al., The global burden of fasciolosis in domestic animals with an outlook on the contribution of new approaches for diagnosis and control. Parasitology research, 2013. 112(7): p. 2421-2430. [CrossRef]
- Mas-Coma, S., M.A. Valero, and M.D. Bargues, Fascioliasis. Digenetic trematodes, 2014: p. 77-114. [CrossRef]
- Schols, R., et al., Invasive snails, parasite spillback, and potential parasite spillover drive parasitic diseases of Hippopotamus amphibius in artificial lakes of Zimbabwe. BMC biology, 2021. 19(1): p. 1-21. [CrossRef]
- Jean-Richard, V., et al., Estimating population and livestock density of mobile pastoralists and sedentary settlements in the south-eastern Lake Chad area. Geospatial health, 2015. 10(1). [CrossRef]
- Jaja, I.F., et al., Financial loss estimation of bovine fasciolosis in slaughtered cattle in South Africa. Parasite epidemiology and control, 2017. 2(4): p. 27-34. [CrossRef]
- Liba, J.W., N.N. Atsanda, and M.I. Francis, Economic loss from liver condemnation due to fasciolosis in slaughtered ruminants in Maiduguri abattoir, Borno State, Nigeria. Journal of Advanced Veterinary and Animal Research, 2017. 4(1): p. 65-70. [CrossRef]
- Schweizer, G., et al., Estimating the financial losses due to bovine fasciolosis in Switzerland. Veterinary Record, 2005. 157(7): p. 188-193. [CrossRef]
- Marcos, L., et al., Risk factors for Fasciola hepatica infection in children: a case–control study. Transactions of the Royal Society of Tropical Medicine and Hygiene, 2006. 100(2): p. 158-166. [CrossRef]
- LA, M.R., Clinical characteristics of chronic infection by Fasciola hepatica in children. Revista de gastroenterologia del Peru: organo oficial de la Sociedad de Gastroenterologia del Peru, 2002. 22(3): p. 228-233.
- Mas-Coma, S., Human fascioliasis: epidemiological patterns in human endemic areas of South America, Africa and Asia. Southeast Asian J Trop Med Public Health, 2004. 35(Suppl 1): p. 1-11.
- Moher, D., et al., Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol, 2009. 62(10): p. 1006-12. [CrossRef]
- Munn, Z., et al., The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int J Health Policy Manag, 2014. 3(3): p. 123-8. [CrossRef]
- Abaver, D.T., et al., Enteric parasitic infections in HIV-infected patients with low CD4 counts in Toto, Nigeria. 2012.
- Abo-Madyan, A.A., et al., Clinical trial of Mirazid in treatment of human fascioliasis, Ezbet El-Bakly (Tamyia Center) Al-Fayoum Governorate. J Egypt Soc Parasitol, 2004. 34(3): p. 807-818.
- Abou-Basha, L., et al., Hepatic fibrosis due to fascioliasis and/or schistosomiasis in Abis 1 village, Egypt. Eastern Mediterranean Health Journal= La Revue de Sante de la Mediterranee Orientale= Al-majallah Al-sihhiyah Li-sharq Al-mutawassit, 2000. 6(5-6): p. 870-878.
- Adarosy, H.A., et al., Changing pattern of fascioliasis prevalence early in the 3rd millennium in Dakahlia Governorate, Egypt: an update. J Egypt Soc Parasitol, 2013. 43(1): p. 275-86. [CrossRef]
- Arinola, G.O., et al., Serum Micronutrients in Helminth-infected Pregnant Women and Children: Suggestions for Differential Supplementation During Anti-helminthic Treatment. Ann Glob Health, 2015. 81(5): p. 705-10. [CrossRef]
- Black, J., et al., Human fascioliasis in South Africa. South African Medical Journal, 2013. 103(9): p. 658-659. [CrossRef]
- Curtale, F., Anaemia among young male workers in Alexandria, Egypt. EMHJ-Eastern Mediterranean Health Journal, 6 (5-6), 1005-1016, 2000, 2000. [CrossRef]
- Curtale, F., et al., Clinical signs and household characteristics associated with human fascioliasis among rural population in Egypt: a case-control study. Parassitologia, 2003. 45(1): p. 5-11.
- de Alegría, M.L.A.R., et al., Prevalence of Strongyloides stercoralis and other intestinal parasite infections in school children in a rural area of Angola: a cross-sectional study. The American journal of tropical medicine and hygiene, 2017. 97(4): p. 1226. [CrossRef]
- El Shazly, A.M., et al., Intestinal parasites in Dakahlia governorate, with different techniques in diagnosing protozoa. J Egypt Soc Parasitol, 2006. 36(3): p. 1023-34.
- el-Shazly, A.M., et al., Clinico-epidemiological study of human fascioliasis in an endemic focus in Dakahlia Governorate, Egypt. J Egypt Soc Parasitol, 2001. 31(3): p. 725-36.
- El-Shazly, A.M., et al., Past and present situation of human fascioliasis in Dakahlia Governorate, Egypt. J Egypt Soc Parasitol, 2009. 39(1): p. 247-62.
- el-Shazly, A.M., et al., The reflection of control programs of parasitic diseases upon gastrointestinal helminthiasis in Dakahlia Governorate, Egypt. Journal of the Egyptian Society of Parasitology, 2006. 36(2): p. 467-480.
- el-Shazly, A.M., et al., Evaluation of two serological tests in diagnosis of human cases of biliary and ectopic fascioliasis. J Egypt Soc Parasitol, 2002. 32(1): p. 79-90.
- Esteban, J.G., et al., Hyperendemic fascioliasis associated with schistosomiasis in villages in the Nile Delta of Egypt. Am J Trop Med Hyg, 2003. 69(4): p. 429-37. [CrossRef]
- Fawzi, M., et al., Vegetable-transmitted parasites among inhabitants of El-Prince, Alexandria and its relation to housewives’ knowledge and practices. J Egypt Public Health Assoc, 2004. 79(1-2): p. 13-29.
- Fentie, T., et al., Epidemiology of human fascioliasis and intestinal parasitosis among schoolchildren in Lake Tana Basin, northwest Ethiopia. Trans R Soc Trop Med Hyg, 2013. 107(8): p. 480-6. [CrossRef]
- Hammami, H., N. Hamed, and A. Ayadi, Epidemiological studies on Fasciola hepatica in Gafsa Oases (south west of Tunisia). Parasite, 2007. 14(3): p. 261-4. [CrossRef]
- Ihesiulor, G.U., et al., Helminths of the gastrointestinal tract among children in Kano, Northern Nigeria. Asian Journal of Biological and Life Science, 2013. 2(2).
- Ijagbone, I.F. and T.F. Olagunju, Intestinal helminth parasites in school children in Iragbiji, boripe local government, Osun state, Nigeria. African Journal of Biomedical Research, 2006. 9(1). [CrossRef]
- Keiser, J., et al., Efficacy and safety of artemether in the treatment of chronic fascioliasis in Egypt: exploratory phase-2 trials. PLoS Negl Trop Dis, 2011. 5(9): p. e1285. [CrossRef]
- Mekky, M.A., et al., Human fascioliasis: a re-emerging disease in upper Egypt. Am J Trop Med Hyg, 2015. 93(1): p. 76-9. [CrossRef]
- Na’acha, E., P. Vandi, and G. Chessed, Species and prevalence determination of Human Intestinal Parasites among Patients attending two Medical Centers in Yola, Adamawa State, Nigeria. Journal of Applied Sciences and Environmental Management, 2017. 21(3): p. 431-437. [CrossRef]
- Nxasana, N., et al., Prevalence of intestinal parasites in primary school children of Mthatha, Eastern Cape Province, South Africa. Annals of medical and health sciences Research, 2013. 3(4): p. 511-516. [CrossRef]
- Okaka, C., A. Awharitoma, and J. Okonji, Gastrointestinal parasites of school children in Benin city, Nigeria. Iranian Journal of Public Health, 2000. 29(1-4): p. 1-12.
- Osman, M., et al., Evaluation of two doses of triclabendazole in treatment of patients with combined schistosomiasis and fascioliasis. EMHJ-Eastern Mediterranean Health Journal, 17 (4), 266-270, 2011, 2011. [CrossRef]
- Periago, M.V., et al., Very high fascioliasis intensities in schoolchildren from Nile Delta Governorates, Egypt: The Old World highest burdens found in lowlands. Pathogens, 2021. 10(9): p. 1210. [CrossRef]
- Shitta, K., H. Audu, and A. Usman, Prevalence of geohelminthes in school children in some parts of Lokoja, Kogi State, North-Central Nigeria. Bayero Journal of Pure and Applied Sciences, 2017. 10(1): p. 151-154. [CrossRef]
- Soliman, M.F., Epidemiological review of human and animal fascioliasis in Egypt. The Journal of Infection in Developing Countries, 2008. 2(03): p. 182-189. [CrossRef]
- Squire, S.A., et al., Gastrointestinal helminths in farmers and their ruminant livestock from the Coastal Savannah zone of Ghana. Parasitology research, 2018. 117: p. 3183-3194. [CrossRef]
- Mas-Coma, M., J. Esteban, and M. Bargues, Epidemiology of human fascioliasis: a review and proposed new classification. Bulletin of the World Health Organization, 1999. 77(4): p. 340.
- Rokni, M.B., et al., Diagnosis of human fasciolosis in the Gilan province of Northern Iran: application of cathepsin L-ELISA. Diagnostic microbiology and infectious disease, 2002. 44(2): p. 175-179. [CrossRef]
- Moghaddam, A., et al., Human and animal fascioliasis in Mazandaran province, northern Iran. Parasitology Research, 2004. 94: p. 61-69. [CrossRef]
- Esteban, J.-G., et al., Hyperendemic fascioliasis associated with schistosomiasis in villages in the Nile Delta of Egypt. The American journal of tropical medicine and hygiene, 2003. 69(4): p. 429-437. [CrossRef]
- De, N.V., et al., The food-borne trematode zoonoses of Vietnam. The Southeast Asian Journal of Tropical Medicine and Public Health, 2003. 34: p. 12-34.
- Mas-Coma, S., Epidemiology of fascioliasis in human endemic areas. Journal of helminthology, 2005. 79(3): p. 207-216. [CrossRef]
- El-Shazly, A., et al., Clinico-epidemiological study of human fascioliasis in an endemic focus in Dakahlia Governorate, Egypt. Journal of the Egyptian Society of Parasitology, 2001. 31(3): p. 725-736.
- Ashrafi, K., et al., Fascioliasis: a worldwide parasitic disease of importance in travel medicine. Travel medicine and infectious disease, 2014. 12(6): p. 636-649. [CrossRef]
- Fentie, T., et al., Epidemiology of human fascioliasis and intestinal parasitosis among schoolchildren in Lake Tana Basin, northwest Ethiopia. Transactions of The Royal Society of Tropical Medicine and Hygiene, 2013. 107(8): p. 480-486. [CrossRef]
- Bayu, B., et al., Cases of human fascioliasis in North-West Ethiopia. Ethiopian Journal of Health Development, 2005. 19(3): p. 237-240. [CrossRef]
- Lukambagire, A.-H.S., D.N. Mchaile, and M. Nyindo, Diagnosis of human fascioliasis in Arusha region, northern Tanzania by microscopy and clinical manifestations in patients. BMC infectious diseases, 2015. 15: p. 1-8. [CrossRef]
- Noel, K., et al., Fasciolosis risk factors for public health in Huambo, Angola. Revista de Salud Animal, 2013. 35(3): p. 164-173.
- Isah, U.M. and A. Dalhatu, Epidemiological studies of human fascioliasis among selected individuals in northern Bauchi state, Nigeria.
- Futagbi, G., et al., Assessment of Helminth Infections in Goats Slaughtered in an Abattoir in a suburb of Accra, Ghana. West African Journal of Applied Ecology, 2015. 23(2): p. 35-42.
- Chougar, L., et al., Genetically ‘pure’Fasciola gigantica discovered in Algeria: DNA multimarker characterization, trans-Saharan introduction from a Sahel origin and spreading risk into north-western Maghreb countries. Transboundary and Emerging Diseases, 2020. 67(5): p. 2190-2205. [CrossRef]
- Zaimi, I., et al., Hepatic fascioliasis in Tunisia. Tunisie Medicale, 1971. 49(1): p. 39-49.
- Slifko, T.R., H.V. Smith, and J.B. Rose, Emerging parasite zoonoses associated with water and food. International journal for parasitology, 2000. 30(12-13): p. 1379-1393. [CrossRef]
- Malatji, M.P., J. Lamb, and S. Mukaratirwa, Molecular characterization of liver fluke intermediate host lymnaeids (Gastropoda: Pulmonata) snails from selected regions of Okavango Delta of Botswana, KwaZulu-Natal and Mpumalanga provinces of South Africa. Veterinary Parasitology: Regional Studies and Reports, 2019. 17: p. 100318. [CrossRef]
- Malatji, M.P., D.M. Pfukenyi, and S. Mukaratirwa, Fasciola species and their vertebrate and snail intermediate hosts in East and Southern Africa: a review. J Helminthol, 2019. 94: p. e63. [CrossRef]
- Singh, K., et al., Special Issues. Statistics, 2022. 3(3).
- Keiser, J. and J. Utzinger, Emerging foodborne trematodiasis. Emerging infectious diseases, 2005. 11(10): p. 1507. [CrossRef]
- WHO, Control of foodborne trematode infections: report of a WHO study group. 1995: World Health Organization.
- Mas-Coma, S., M. Bargues, and M. Valero, Human fascioliasis infection sources, their diversity, incidence factors, analytical methods and prevention measures–CORRIGENDUM. Parasitology, 2020. 147(5): p. 601-601. [CrossRef]
- Webb, C.M. and M.M. Cabada, Recent developments in the epidemiology, diagnosis, and treatment of Fasciola infection. Curr Opin Infect Dis, 2018. 31(5): p. 409-414. [CrossRef]
- Fitzpatrick, J., Global food security: the impact of veterinary parasites and parasitologists. Veterinary Parasitology, 2013. 195(3-4): p. 233-248. [CrossRef]
- Caravedo, M.A. and M.M. Cabada, Human fascioliasis: current epidemiological status and strategies for diagnosis, treatment, and control. Research and reports in tropical medicine, 2020: p. 149-158. [CrossRef]
- WHO, A key role for veterinary authorities and animal health practitioners in preventing and controlling neglected parasitic zoonoses: A handbook with focus on Taenia solium, Trichinella, Echinococcus and Fasciola. 2021: Food & Agriculture Org.
- Mas-Coma, S., M. Valero, and M. Bargues, Effects of climate change on animal and zoonotic helminthiases. Rev Sci Tech, 2008. 27(2): p. 443-57.
- Mas-Coma, S., M.A. Valero, and M.D. Bargues, Climate change effects on trematodiases, with emphasis on zoonotic fascioliasis and schistosomiasis. Veterinary parasitology, 2009. 163(4): p. 264-280. [CrossRef]
- Fox, N.J., et al., Predicting impacts of climate change on Fasciola hepatica risk. PLoS One, 2011. 6(1): p. e16126. [CrossRef]
- Afshan, K., et al., Impact of climate change and man-made irrigation systems on the transmission risk, long-term trend and seasonality of human and animal fascioliasis in Pakistan. Geospatial Health, 2014. 8(2): p. 317-334. [CrossRef]
- Webb, C.M. and M.M. Cabada, Recent developments in the epidemiology, diagnosis, and treatment of Fasciola infection. Current opinion in infectious diseases, 2018. 31(5): p. 409-414. [CrossRef]
- Infantes, L.R.R.-H., et al., The Global Prevalence of Human Fascioliasis: A Systematic Review and Meta-Analysis. 2023. [CrossRef]
- Ahmad, T., et al., A bibliometric analysis and global trends in fascioliasis research: A neglected tropical disease. Animals, 2021. 11(12): p. 3385. [CrossRef]
- Momčilović, S., et al., Rapid diagnosis of parasitic diseases: current scenario and future needs. Clinical Microbiology and Infection, 2019. 25(3): p. 290-309. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



