
Submitted:
23 April 2024
Posted:
24 April 2024
You are already at the latest version
Abstract
Intrinsic subtype of triple-negative breast cancer (TNBC) is based on genomic evaluation. In this study, we report the survival and pathological complete response (pCR) rates of TNBC patients subtyped by IHC and treated with neoadjuvant chemotherapy (NACT). A retrospective cohort of 187 TNBC patients who received NACT between 2008 and 2017 was used, and IHC subtyping was performed on biopsy specimens before chemotherapy. The subtyping revealed predominant basal-like tumors (IHC-BL, 61%), followed by basal-like immune-suppressed (IHC-BLIS, 31%), mesenchymal tumors (12.5%), luminal androgen receptor tumors (IHC-LAR, 12%) and basal-like immune-activated (IHC-BLIA, 10.9%). The pathological complete response (pCR) rate varied among subtypes, with IHC-BLIA showing the highest (30.0%) and IHC-LAR showing the lowest (4.5%). IHC-BLIS led in recurrence sites. Overall and disease-free survival analyses did not show significant differences among subtypes. Although, IHC-BLIA demonstrated a trend toward better survival and IHC-mesenchymal worse. Patients who achieved pCR exhibited significantly better disease-free survival and overall survival than non-responders. This study underscores the potential of IHC-based subtyping in TNBC management, highlighting distinct response patterns to neoadjuvant chemotherapy and potential implications for treatment strategies. Further research is warranted to validate these findings and explore tailored therapeutic approaches for specific TNBC subtypes.
Keywords:
triple negative breast cancer
; immunohistochemistry
; neoadjuvant chemotherapy
1. Introduction
According to Cancer Research UK, triple-negative breast cancer (TNBC) accounts for approximately 15% of malignancies affecting the breast. Characterized by the absence of estrogen, progesterone and Her2 receptor positivity, it is usually associated with a poor prognosis, and chemotherapy remains the main basis of systemic treatment.[1] In the last decade, the relevant benefits of chemotherapy combined with immunotherapy and targeted therapy for patients with pathogenic germline BRCA mutations have positively impacted outcomes in both curative and palliative settings.[2]
However, TNBC represents a heterogeneous group of several subtypes with distinct drivers, survival outcomes and responses to systemic therapy.[3] Several classifications have been proposed and validated, largely based on genomic evaluation of the tumors.[4] In 2011, Lehmann et al characterized 7 subtypes by gene expression, including one unstable. Basal-like 1 (BL1) is associated with genomic repair pathway deficiencies; basal-like 2 (BL2) is enriched in growth factor signaling-related genes; immunomodulatory (IM) is enriched in immunological signaling; and mesenchymal (M) and mesenchymal stem–like (MSL) are enriched in components and pathways related to cell motility and the luminal androgen receptor (LAR), and androgen and metabolism genes are enriched.[5] Later, in 2015, Burstein described four subtypes, namely, luminal androgen receptor (LAR), mesenchymal (MES), basal-like immune-suppressed (BLIS) and immune-activated (BLIA) subtypes.[6] One year later, the FUSCC classification introduced the immune-modulatory (IM) subtype, along with the known MES, BLIS and LAR subtypes.[7]
All the above classifications are based on molecular profiling, which could be valuable at the patient level for precision medicine approaches once some mutations predict the benefit of targeted therapy. However, for most patients, the treatment options will remain limited. Moreover, technical challenges, such as the need for fresh tissue, the length of time needed to perform the analysis, and the significantly high costs, impact its wide use in standard practice.[8,9]
Immunohistochemistry (IHC) is an established laboratory method for evaluating the presence of antigens that is widely used in breast cancer and is pivotal for tailoring systemic treatments (e.g., the human epidermal growth factor receptor 2 - HER2).[10] Moreover, IHC is significantly less expensive and laborious than gene expression and has been evaluated in several studies as a surrogate marker of established intrinsic genomic-based subtyping assays, as summarized in Table 1. [11,12,13,14,15,16,17,18]Although some studies have provided survival data amongst the subtypes, the effect of chemotherapy on the pathological complete response, if it also serves as surrogate biomarker of survival has not been reported.
In this study, we report the survival and pCR rates of patients who underwent IHC subtyping using our panel and who received neoadjuvant chemotherapy.
2. Results
One hundred eighty-seven patients were included in this analysis; the mean age was 52.43 (SD = 12.79) years, the mean tumor size was 47.64 (SD = 53.61) millimeters, and other demographic characteristics are summarized in Table 4.
For immunohistochemistry, staining for all 4 markers was possible in 98.4% (184) of the patients and partially in 3 patients due to tissue exhaustion. We successfully identified the characteristics of 4 subtypes in 96.3% (183) of patients. Overall, the frequency of the IHC-basal subtype was 61% (114). The percentages of basal subtypes identified by IHC-BLIS and IHC-BLIA were 31% (57) and 10.9% (20), respectively. The second most common subtype was IHC-MES 12.5% (23), followed by IHC-LAR 12.0% (22) and IHC-mixed 11.4% (21). (Table 2)
Among the 28 (15%) patients who achieved pCR, 75% exhibited an IHC-basal feature, 14.28% exhibited an IHC-mesenchymal feature, and 7.4% exhibited an IHC-LAR feature. The pCR rate in the IHC-BLIA group was the highest (30%), and that in the IHC-LAR group was the lowest (4.5%). (Table 3)
Patients who achieved pCR had a significantly better median disease-free (mDFS) survival NR (not reached) (CI: >50%) vs. no-PCR 30 m (months) (CI: 18-NR) (p=0.00022). Overall, it was also significantly greater in patients who achieved pCR according to the NR (CI: >50%) than in those who did not achieve pCR according to the 58-m (CI: 40-NR) no-PCR (p=0.00018). (Supplementary Figures S1 and S2).
Most of the recurrences occurred in the first 20 months following surgery. mDFS did not significantly differ among subtypes (p=0.52). (Figure 1A) IHC-BLIA demonstrated a greater mDFS for patients with NR (CI: 34-NR) than for patients with all other subtypes (CI: 23-NR) (p=0.14). The meDFS was also NR for the IHC-LAR, IHC-mixed and IHC-basal-like groups. ICH-BLIS patients had the second worst mDFS, 50 m (CI: 11-NR), and IHC-MES patients had a markedly short mDFS, 16 m (CI: 6-NR). Interestingly, the mDFS curves for patients who did not achieve pCR were less distinct among subtypes, suggesting that pCR has a crucial role regardless of intrinsic subtype. IHC-MES followed by IHC-Basal-like showed worse survival, respectively 17 m (CI: 6-NR) and 15m (CI: 6-NR). (Figure 1B).
The pattern of recurrence was graphically distinct among subtypes. IHC-BLIS led recurrence in each category, and interestingly, no local or cerebral relapse occurred in patients with the IHC-LAR subtype. (Figure 2)
Overall survival analysis also revealed no significant differences among subtypes (p=0.61).(Figure 1C) IHC-BLIA had a greater mOS, NR (95% CI: NR>50%), than did the other subtypes at 60 m (95% CI: 48-NR) (p=0.081). IHC-BLIA exhibit the graphically highest mOS, with an NR (95% CI: 39-NR) mOS for patients who did not achieve pCR and IHC-MES was associated with a worse survival with 37m (95% CI: 27-NR). (Figure 1D)
3. Discussion
This study is pioneering in demonstrating pCR rates among TBNC subtypes using IHC. We found numerically higher pCR rates in the IHC-BLIA (30%) subgroup and a trend toward longer DFS and OS, while in the IHC-MES subgroup, survival was worse despite the pCR rate (17.4%) being closer to that of the whole population analyzed (15.0%).
The basal-like subtype was predominant in our sample, with 61.5% of the tumors harboring a basal component. In 2010, Oakman C et al reported higher rates of the BL phenotype in TNBC patients (71-91%).[19] Interestingly, Lehmann et all in 2011 reported that 49% of BL cases were characterized by intrinsic subtyping, but IHC seems to indicate a higher percentage (88%), and very likely, only half of these cases would correlate with the intrinsic BL subtype.[5] We observed rates somewhat closer to those reported by Zhao et al. and Jing Liang et al.[14,16] Identifying basal-like TNBC is clinically relevant, as data showed a benefit from adjuvant chemotherapy for patients with non-basal-like tumors and residual disease following surgery, despite the use of neoadjuvant chemotherapy. [20,21]
We identified a predominance of IHC-BLIS (31.0%) over IHC-BLIA (10.9%) in our population, which likely contributed to the overall modest pathological response rate of (15.0%). Although our IHC-BLIS rates are somewhat comparable to the values found by the authors performing IHC subtyping, the overall percentage of patients with the IHC-BLIA subtype is markedly lower.(Table 1) On the other hand, we found a markedly higher pCR rate in IHC-BLIA (30.0%) than the pCR rate in IHC-BLIS (14.0%). Based on recent publications, the new standard of care for early and high-risk TNBC patients includes immunotherapy alongside a taxane-platinum-based dose-dense chemotherapy, regardless of the presence of immune receptors/markers.[22] However, data are still needed to understand the efficacy of these regimens in TNBC patient subpopulations.
Immuno-inflamed occurred solely at the IHC-IM subtype according to Jing Lian et al. (2022), but a significant proportion of the other subtypes are immune-excluded, which raises the question of whether those subjects would benefit from immunotherapy in clinic.[16]
IHC-MES was the second most common subtype, and numerically, it was associated with worse mDFS and mOS, which is consistent with the findings in the literature. [13,14,15] Unfortunately, the benefit of conventional adjuvant systemic treatment for this subtype is often poor, if any, given its specific molecular characteristics, which has motivated researchers to consider regimens mimicking sarcomatous disease. [23] Moreover, given the preclinical and clinical activity of mTOR, PI3K, SRC/ABL and angiogenesis inhibitors, we believe that tailored treatment for this subtype could be warranted.[2]
The IHC-LAR subtype had the lowest pCR rate (4.5%) and was the third most common subtype in our sample. A long-standing effort has been made to offer anti-androgen targeting for this subtype, with no translation in registrational approvals. The main challenges might include the unreliable behavior of AR as a driver in TNBC, compared to that of ER in HR+ disease, as well as the cutoff of AR-receptor intensity to trigger intervention and the high-bar endpoints chosen in clinical trials to evaluate the AR-targeting effect.[24] As mentioned above, the current best adjuvant treatment for patients with residual disease is capecitabine; however, for specific subtypes, such as LAR, the benefit is unclear. Therefore, to answer this question and by leveraging our knowledge of prostate cancer, where androgen deprivation therapy plus androgen receptor pathway inhibitors can be combined with docetaxel, we believe that a cohort of patients with IHC-LAR in a potential umbrella trial for intrinsic subtypes of TNBC should considered to receive adjuvant capecitabine plus ARPI.[25]
The pattern of recurrence we observed in our IHC-based subtyping cohort aligned with that expected in the literature.(Table 1) Notably, brain relapse, a known independent factor of poor prognosis, occurred in 8% of the patients with IHC-MES, 14% in IHC-BLIS, and approximately 10% of those with the other IHC subtypes, but interestingly no patients with IHC-LAR experienced brain relapse. There is a longstanding discussion on how to optimize relapse monitoring in high-risk breast tumors, but no clear consensus has been reached. Our data could assist in identifying patients with a greater risk of recurrence, which could deserve more individualized monitoring given specific patterns of disease relapse and therefore might benefit from brain and visceral imaging, as well as promising emerging techniques, such as circulating tumor DNA, in addition to the current recommended approaches.[26]
Our study demonstrated a low percentage of unclassifiable 2.2%, and IHC-mixed 11.4% compared to the other studies mentioned in Table 1. In a study conducted by Yoo in 2022, the majority of patients with IHC-unclassifiable had presented with mesenchymal subtype on genomic classification.[15] Interestingly, both Zhao et al., Leeha et al. and Hu et al, did not reported mixed subtypes by using their IHC panels.[14,17,18] We believe IHC-unclassifiable and IHC-mixed should be expected given the IHC assay limitations and support the heterogeneous features of a significant proportion of TNBCs. [27]
Although the results of this study are promising, they should be interpreted in light of these limitations. Our retrospective design imposes challenges in survival analysis. There is no consensus about the use of an IHC subtyping panel, and IHC staining was performed utilizing archival tumor tissue from 2008 onward, which could have impacted the performance of the assay and requires validation using an established method for intrinsic genomic subtyping.
4. Materials and Methods
4.1. Sample Selection and Outcome Definitions
Patients with localized or locally advanced TNBC who were treated with neoadjuvant chemotherapy followed by curative surgery at the same institution between January 2008 and December 2017 and who had available biopsy and surgical specimens met the inclusion criteria for this retrospective cohort.
From medical files, clinical and pathological data were collected to construct a database using an electronic case report form (supplementary file S1).
For this study, TNBC was defined as estrogen and progesterone receptor < 1% and HER2-negative +1 or +2 without fish amplification. Pathological complete response (pCR) was defined as the absence of invasive cancer on surgical specimens from the breast and axilla (ypT0/Tis pN0). Disease-free survival (DFS) was defined as the time between the day of the cycle of one day of chemotherapy regimen administration until cancer recurrence or cancer-related death. Overall survival (OS) was defined as the time between the day of the cycle one day after chemotherapy regimen administration until death related to any cause. In the case of loss to follow-up, the appointment date at the NCI, which contains information about disease and survival, will be used to censor the patient for the analysis.
2.2. IHC Analysis and Interpretation
Tissue samples were converted into histological sections on previously salinized slides. Evaluation of the cellular atypia pattern was performed by hematoxylin-eosin (HE) staining. The evaluated tumor area was selected by a pathologist, and the in situ regions within the invasive tumors were also delineated to allow a better evaluation of the stains. Tissue sections were immunoassayed with a Polymer Detection System (RE7150-K, Leica Biosystems Newcastle Ltd., Balliol Business Park West, Benton Lane, Newcastle Upon Tyne NE12 8EW, United Kingdom) according to the protocol established by the manufacturer. Primary antibodies were incubated with the tissues for 18 h at 4˚C at different dilutions determined by titration, as shown in Table 4.
The antibody panel was adapted from studies reported in the Table 1 and interpretation of the IHC results was performed by the author F.R., as shown in Table 3. The scoring was reviewed by the senior authors E.A., and the final scores agreed between F.R. and E.A..

Table 5.
Immunohistochemistry analysis and interpretation.
| IHC-subtype | Antibody results | |||||
|---|---|---|---|---|---|---|
| IDO-1 | FOX-C1 | AR | Claudin-3 | |||
| Basal-like unspecific (BL) | IDO-1 ≤ 10% and FOX-C1 < 4or IDO > 10% and FOX-C1 ≥ 4 | < 10% | Weak (W), M or I | |||
| Basal like immune-suppressed (BLIS) | ≤ 10% | ≥ 4 | < 10% | |||
| Basal like immune-activated (BLIA) | > 10% | < 4 | < 10% | |||
| Luminal androgen receptor (LAR) | ≤ 10% | < 4 | ≥ 10% | |||
| Mesenchymal (MES) | any | any | any | 0 | ||
| Mixed (criteria for ≥ 2 subtypes) | BLIS | LAR | ≤ 10% | ≥ 4 | ≥ 10% | W, M or I |
| BLIA | LAR | > 10% | < 4 | ≥ 10% | ||
| BL | LAR | IDO-1 ≤ 10% and FOX-C1 < 4or IDO > 10% and FOX-C1 ≥ 4 | ≥ 10% | |||
| MES | LAR | any | any | ≥ 10% | 0 | |
| Unclassifiable | ≤ 10% | ≤ 2 | < 5% | W, M or I | ||
For positive controls, tissues suggested by the antibody manufacturer’s datasheets were used. The reaction was visualized using diaminobenzidine (DAB), followed by hematoxylin counterstaining. Negative controls were prepared without the primary antibody. The positivity of the staining was analyzed in ten random fields and determined by manual counting using ImageJ® software according to the preestablished equation below.
Sc represents the number of stained cells in each field, where s = [1, 2, ∙∙∙, 10]; Tc represents the total number of cells in each field, where t = [1, 2, ∙∙∙, 10]; and p represents the mean percentage of positivity.
2.3. Statistical Analysis
Continuous variables are shown as the mean and standard deviation, and categorical variables are shown as the total value and percentage of the total value.
The time to overall survival was computed as the time of diagnosis until death or the last patient contact, and the disease-free survival time was computed as the time of surgery until recurrence or last patient contact.
The Kaplan‒Meier method was used to estimate survival curves, and the log rank test was performed to evaluate whether there were differences in covariate levels via univariate analysis. The significance level adopted to reject the null hypothesis was alfa equal to 0.05. A bar plot was used to demonstrate the frequency of subtypes at each site.
5. Conclusions
We successfully demonstrated that an affordable and widely reproducible panel of IHC assays can be used to subtype TNBC. Moreover, we were the first to demonstrate the pCR rate among IHC subtypes.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplementary S1.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, B.P., S.C. and E.A; methodology, B.P., S.C., P.V., F.R., C.S., and E.A; software, B.P., C.S., and E.A; validation, P.V. and E.A; formal analysis, B.P., S.C., C.S., and E.A; investigation, B.P., S.C., P.V., F.R., C.S., and E.A resources, B.P., S.C., P.V., F.R., C.S., and E.A; data curation, B.P., S.C., C.S., and E.A; writing—original draft preparation, B.P., S.C., C.S., and E.A; writing—review and editing, B.P., S.C., P.V., F.R., C.S., and E.A; visualization, B.P., S.C., C.S., and E.A; supervision, S.C. and E.A; project administration, B.P.,S.C., C.S., and E.A; funding acquisition, E.A.. All authors have read and agreed to the published version of the manuscript.”
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of the National Cancer Institute (NCI) in Rio de Janeiro Brazil Ethics Committee, under the number CAAE: 22893219.1.0000.5274.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of this research and no impact in the clinical decision which was already taken before the study.
Data Availability Statement
Authors are open to discuss data sharing in the terms of the National Cancer Institute.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Cancer Research UK, https://www.cancerresearchuk.org/about-cancer/breast-cancer/types/triple-negative-breast-cancer, Accessed [March [2023]. Publications: Cancer Research UK ([y2023]), Triple Negative Breast Cancer, Cancer Research UK. [Internet]. Cancer Research UK. 2023 [cited 2024 Mar 3]. Available from: https://www.cancerresearchuk.org/about-cancer/breast-cancer/types/triple-negative-breast-cancer.
- de Paula B, Kieran R, Koh SSY, Crocamo S, Abdelhay E, Muñoz-Espín D. Targeting Senescence as a Therapeutic Opportunity for Triple-Negative Breast Cancer. Mol Cancer Ther [Internet]. 2023, 22, 583–598. [CrossRef] [PubMed]
- Rala de Paula, B.H.; Kumar, S.; Morosini, F.M.; Calábria Cardoso, D.E.M.; Moreira de Sousa, C.A.; Crocamo, S. Real-world assessment of the effect of impact of tumor size on pathological complete response rates in triple negative breast cancer after neoadjuvant chemotherapy. Chinese Clin Oncol. 2020, 9, 1–9. [Google Scholar] [CrossRef]
- Marra, A.; Trapani, D.; Viale, G.; Criscitiello, C.; Curigliano, G. Practical classification of triple-negative breast cancer: intratumoral heterogeneity, mechanisms of drug resistance, and novel therapies. npj Breast Cancer [Internet]. 2020, 6, 54. [Google Scholar] [CrossRef] [PubMed]
- Lehmann BD, Bauer JA, Chen X, Sanders ME, Chakravarthy AB, Shyr Y, et al. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J Clin Invest [Internet]. 2011, 121, 2750–2767. [CrossRef]
- Burstein MD, Tsimelzon A, Poage GM, Covington KR, Contreras A, Fuqua SAW, et al. Comprehensive Genomic Analysis Identifies Novel Subtypes and Targets of Triple-Negative Breast Cancer. Clin Cancer Res [Internet]. 2015, 21, 1688–1698. [CrossRef] [PubMed]
- Liu Y-R, Jiang Y-Z, Xu X-E, Yu K-D, Jin X, Hu X, et al. Comprehensive transcriptome analysis identifies novel molecular subtypes and subtype-specific RNAs of triple-negative breast cancer. Breast Cancer Res [Internet]. 2016, 18, 33. [CrossRef]
- Bianchini, G.; De Angelis, C.; Licata, L.; Gianni, L. Treatment landscape of triple-negative breast cancer — expanded options, evolving needs. Nat Rev Clin Oncol [Internet]. 2022, 19, 91–113. [Google Scholar] [CrossRef]
- Yang, R.; Li, Y.; Wang, H.; Qin, T.; Yin, X.; Ma, X. Therapeutic progress and challenges for triple negative breast cancer: targeted therapy and immunotherapy. Mol Biomed [Internet]. 2022, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Rossi C, Fraticelli S, Fanizza M, Ferrari A, Ferraris E, Messina A, et al. Concordance of immunohistochemistry for predictive and prognostic factors in breast cancer between biopsy and surgical excision: a single-centre experience and review of the literature. Breast Cancer Res Treat [Internet]. 2023, 198, 573–582. [CrossRef]
- Choi, J.; Jung, W.-H.; Koo, J.S. Clinicopathologic features of molecular subtypes of triple negative breast cancer based on immunohistochemical markers. Histol Histopathol. 2012, 27, 1481–1493. [Google Scholar]
- Kim, S.; Moon, B.I.; Lim, W.; Park, S.; Cho, M.S.; Sung, S.H. Feasibility of Classification of Triple Negative Breast Cancer by Immunohistochemical Surrogate Markers. Clin Breast Cancer. 2018, 18, e1123–32. [Google Scholar] [CrossRef] [PubMed]
- Kumar S, Bal A, Das A, Bhattacharyya S, Laroiya I, Khare S, et al. Molecular Subtyping of Triple Negative Breast Cancer by Surrogate Immunohistochemistry Markers [Internet]. 2020. Available from: www.appliedimmunohist.com.
- Zhao S, Ma D, Xiao Y, Li X-M, Ma J-L, Zhang H, et al. Molecular Subtyping of Triple-Negative Breast Cancers by Immunohistochemistry: Molecular Basis and Clinical Relevance. Oncologist. 2020, 25, e1481–91. [CrossRef] [PubMed]
- Yoo, T.-K.; Kang, J.; Lee, A.; Chae, B.J. A triple-negative breast cancer surrogate subtype classification that correlates with gene expression subtypes. Breast Cancer Res Treat [Internet]. 2022, 191, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Lian J, Ma H xia, Xu EW, Bu P, Yun KM, Xi YF. Subclassifying triple-negative breast cancers and its potential clinical utility. Virchows Arch. 2022, 481, 13–21. [CrossRef]
- Leeha, M.; Kanokwiroon, K.; Laohawiriyakamol, S.; Thongsuksai, P. Immunohistochemistry-based molecular subtyping of triple-negative breast cancer and its prognostic significance. Pathol Oncol Res [Internet]. 2023, 29. Available from: https://www.por-journal.com/articles/10.3389/pore.2023.1611162.
- Hu H, Tong K, Tsang JY, Ko CW, Tam F, Loong TC, et al. Subtyping of triple-negative breast cancers: its prognostication and implications in diagnosis of breast origin. ESMO Open [Internet] 2024, 9. [CrossRef]
- Oakman, C.; Viale, G.; Di Leo, A. Management of triple negative breast cancer. The Breast [Internet]. 2010, 19, 312–321. [Google Scholar] [CrossRef]
- Lluch A, Barrios CH, Torrecillas L, Ruiz-Borrego M, Bines J, Segalla J, et al. Phase III Trial of Adjuvant Capecitabine After Standard Neo-/Adjuvant Chemotherapy in Patients With Early Triple-Negative Breast Cancer (GEICAM/2003-11\_CIBOMA/2004-01). J Clin Oncol [Internet]. 2020, 38, 203–213. [CrossRef]
- Mayer IA, Zhao F, Arteaga CL, Symmans WF, Park BH, Burnette BL, et al. Randomized Phase III Postoperative Trial of Platinum-Based Chemotherapy Versus Capecitabine in Patients With Residual Triple-Negative Breast Cancer Following Neoadjuvant Chemotherapy: ECOG-ACRIN EA1131. J Clin Oncol [Internet]. 2021, 39, 2539–2551. [CrossRef]
- Han, H.S.; Vikas, P.; Costa, R.L.B.; Jahan, N.; Taye, A.; Stringer-Reasor, E.M. Early-Stage Triple-Negative Breast Cancer Journey: Beginning, End, and Everything in Between. Am Soc Clin Oncol Educ B [Internet], 2023; e390464. [Google Scholar] [CrossRef]
- Yin, L.; Duan, J.-J.; Bian, X.-W.; Yu, S. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res [Internet]. 2020, 22, 61. [Google Scholar] [CrossRef]
- Xu M, Yuan Y, Yan P, Jiang J, Ma P, Niu X, et al. Prognostic Significance of Androgen Receptor Expression in Triple Negative Breast Cancer: A Systematic Review and Meta-Analysis. Clin Breast Cancer [Internet]. 2020, 20, e385–96. [CrossRef]
- Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, et al. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 , × , 2 factorial design. Lancet [Internet]. 2022, 399, 1695–1707. [CrossRef] [PubMed]
- Aldrich, J.; Canning, M.; Bhave, M. Monitoring of Triple Negative Breast Cancer After Neoadjuvant Chemotherapy. Clin Breast Cancer [Internet]. 2023, 23, 832–834. [Google Scholar] [CrossRef] [PubMed]
- Asleh, K.; Riaz, N.; Nielsen, T.O. Heterogeneity of triple negative breast cancer: Current advances in subtyping and treatment implications. J Exp Clin Cancer Res [Internet]. 2022, 41, 265. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A) Disease-free survival according to IHC subtypes. (B) Disease-free survival in patients with no PCR according to IHC subtype. (C) OS according to IHC subtypes. (D) OS in patients with no PCR according to IHC subtype.
Figure 1.
(A) Disease-free survival according to IHC subtypes. (B) Disease-free survival in patients with no PCR according to IHC subtype. (C) OS according to IHC subtypes. (D) OS in patients with no PCR according to IHC subtype.

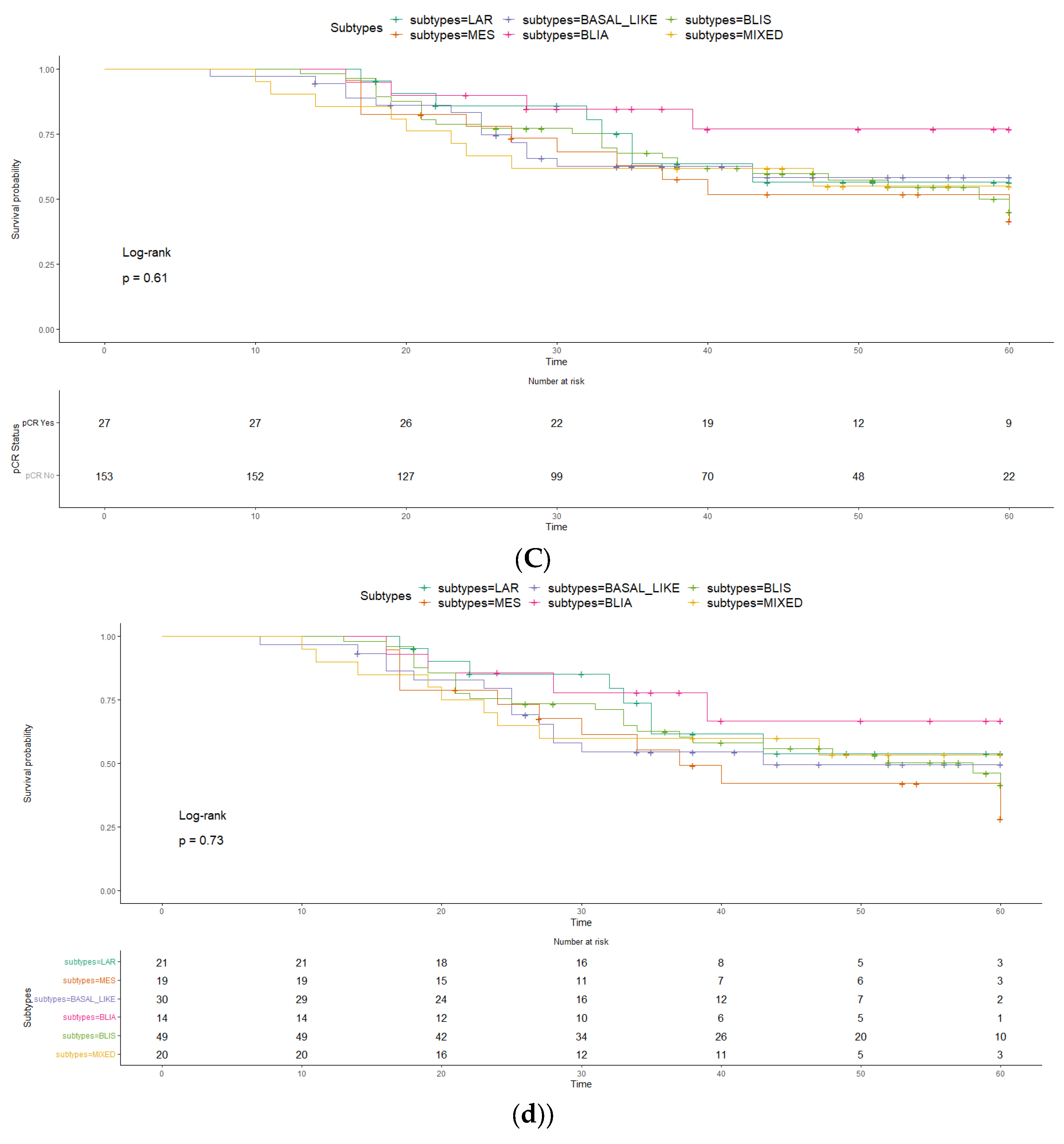
Figure 2.
Pattern of recurrence among IHC subtypes.Legend: A – Visceral recurrence; B – Non-Visceral/non-local/non-cerebral recurrence; C – Local recurrence; D – Cerebral recurrence.
Figure 2.
Pattern of recurrence among IHC subtypes.Legend: A – Visceral recurrence; B – Non-Visceral/non-local/non-cerebral recurrence; C – Local recurrence; D – Cerebral recurrence.
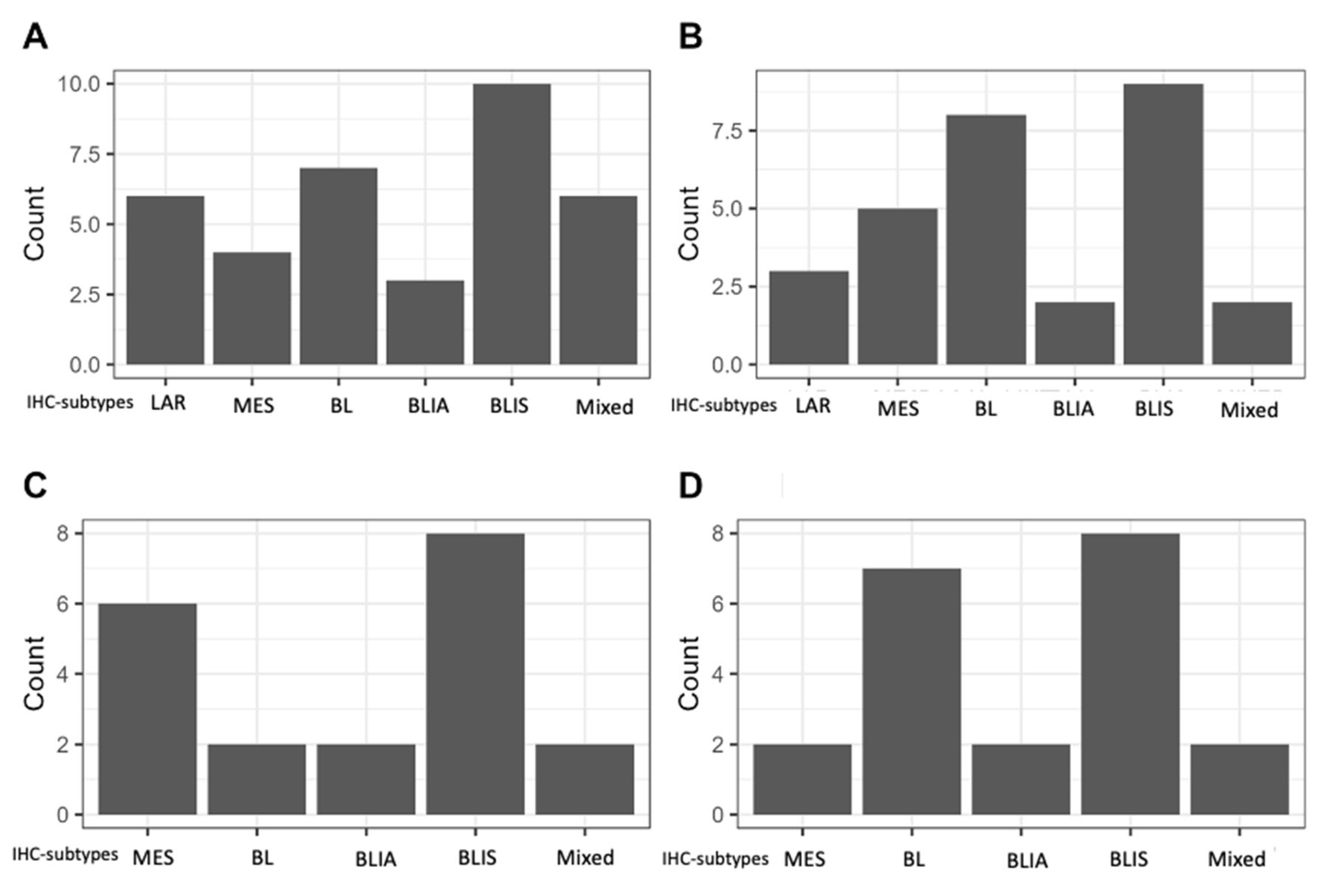
Table 1.
Retrospective studies evaluating IHC as a surrogate for TNBC subtyping.
| Choi J et al, 201211 | Kim S et al, 201812 | Kumar S et al, 202013 | Zhao S et al, 202014 | Yoo T-K et al, 202115 | Lian J et al, 202216 | Leeha M et al, 202317 | Hu H. et al18 | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Total subjects | 122 | 200 | 245 | 210 | 183 | 214 | 145 | 93 | 195 | 123 |
| Methods used for subtyping | IHC | IHC | IHC | RNA and Gene expression and IHC staining | RNA and Gene expression and IHC staining | IHC | RNA and Gene expression and IHC staining | IHC | ||
| Adjuvant treatment | Chemo or radiation based on staging | Not reported | Not reported | ~93% (taxane 75.7% and non-taxane 17.6%) | ~90% (62.8% and 26.8%) | ~91% (84.1% and 7.0%) | Not reported | Not reported | ~ 90% (regimen not disclosed) | Not reported |
| IHC-Apocrine/LAR definition | AR and/or GGT1> 10% | AR > 1% | AR ≥1% | AR ≥ 10% | AR Allred score 8 (5 + 3) | AR ≥ 10% | AR Allred score 8 (5 + 3) | AR≥10%, regardless of the expressionof other markers) | ||
| IHC-BLIS definition | - | FOXC1 ≥ 4 and IDO-1 ≤ 10% | - | AR –, CD8 -, FOXC1> 10% | TIL low; AR <10% ; CD8 <20% ; FOXC1 >= 10% | AR < 10%, CD8 TIL < 20%, FOX-C1 <10%, and regardless of DCLK1 values | ||||
| IHC-BLIA or IM definition | - | IDO-1 > 10% and FOX-C1 < 4 | - | AR – and CD8 activated ³20% | LAR-negative and TIL score > 70% | AR <10% ; TIL high ; CD8 ³ 20% | LAR-negative and TIL score > 70% | AR < 10%, CD8 TIL ≥ 20%, and regardless of FOX-C1 and DCLK1 values | ||
| IHC-Basal definition | CK 5/6 > 10% and/or EGFR moderate or intense | CK 5/6 and/or EGFR > 1% | BL1: EGFR <4, CK5/6 ≥ 4 and/or CK4/14 ≥4 | - | LAR -, IM -, M -, and with diffuse and strong p16 staining | - | - | CK 5/6 and or EGFR + | ||
| BL2: EGFR ≥ 4, irrespective of CK5/6 and/or CK 4/14 result | ||||||||||
| IHC-Claudin-low / Mesenchymal definition | Claudin 3, 4, 7 negative and/or e-cadherin negative | Claudin-3 negative and or e-Cadherin negative | E-cadherin, Claudin 3 and 7 ≥4, Vimentin ≥ 4 | AR – CD8- FOXC1- DCLK1≥10% | LAR negative and TIL score < 20% | Metaplastic features; AR <10% ; CD8 <20% ; FOXC1 <10% | LAR negative and TIL score < 20% | AR < 10%, CD8 TIL < 20%, FOX-C1 <10% and DCLK1 ≥10%, | ||
| IHC-Mixed definition | 2 characteristics of 2 different subtypes | 2 or 3 different tumours | ≥ 2 of other categories | Not reported | Not reported | |||||
| IHC-Unclassifiable definition | Not belonging to any subtype | None of the above features | Did not fit in any category | AR – CD8- FOXC1- DCLK1- | All other manifestations | Not reported | All other manifestations | AR < 10%, CD8 TIL < 20%, FOX-C1 <10% and DCLK1 <10% | ||
| IHC-LAR rate | 12 (9.8%) | 22 (11%) | 41 (16.7%) | 60 (28.6%) | 42 (23%) | 53 (24.8%) | 26 (17.9%) | 23 (24.7%) | 37 (18.9%) | 28 (28.6%) |
| IHC-BLIS rate | 11 (5.5%) | - | 80 (38.1%) | 71 (38.8%) | 90 (42.1%) | 39 (41.9%) | 103 (52.8%) | 20 (20.4%) | ||
| IHC-BLIA or IM rate | 27 (13.5%) | - | 40 (19.4%) | 34 (18.6%) | 39 (18.2%) | 21 (14.5%) | 24 (25.8%) | 34 (17.4%) | 39 (39.8%) | |
| IHC-Basal rate | 27 (22.1%) | 85 (42.5%) | BL 36 (14.6%) ; BL1 32 (13.1%) ; BL2 4 (1.6%) | 120 (57.1%) | 105 (57.4%) | 129 (60.3%) | BL1 27 (18.6%) | 63 (67.7%) | 137 (70.2%) | |
| IHC-Mesenchymal rate | 28 (23%) | 23 (11.5%) | 70 (28.6%) | 16 (7.6%) | 18 (9.8%) | 17 (7.9%) | 44 (30.3%) | 7 (7.5%) | 1 (0.5%) | 11 (11.2%) |
| IHC-Mixed rate | 23 (18.9%) | 60 (30%)LAR+MES 8 (4%) ; LAR+BL 27 (13.5%) ; MES+BL 19 (9.5%) ; LAR+MES+BL 6 (3%) | 37 (15.1%) | 0 | 0 | 0 | NR | 0 | NR | NR |
| IHC-Unclassifiable rate | 32 (26.2%) | 10 (5%) | 61 (24.9%) | 14(6.7%) | 18 (9.8%) | 15 (7%) | 18 (12.4%) | 0 | 20 (10.2%) | 25 (20.3%) |
| Confirmation method | no | no | mRNA | mRNA | no | mRNA | No | |||
| follow-up median | 59.5 months | 41 m (0-64) | 40 m (12-58) | 40.95 m (IQR 23.48-89.22) | 62 m (IQR 43-105) | |||||
| Disease free survival (DFS) | Basal like and unclassifiable show less favourable prognosis, mesenchymal and mixed intermediate and AR showed a better prognosisCk 5/6 and Claudin positivity worse DFS | BLIS worse prognosis.LAR, BLIA, BL and NOS favourableThis was also true for Burstein (4 subtypes)FOXC1 – worse prognosis | - | IM (HR=0.07), LAR (HR=0.18), BLIS (HR=0.26) better RFS than MES | MES worse RFS | Significantly worse DFS for M subtype according to surrogate subtypes and although not clinically significant IM tends to be better survival | No significant differenceLow recurrence 11 cases (11.83%) | 5 y 64.7% and no subtypes difference | IM-inflamed better DFS compared to others and BLIS the worse survival | |
| Overall Survival (OS) | Discohesiviness worse survival | Mesenchymal and unclassified shorted OS (68.2 and 69.2m) | T+N+IHC was superior to T+N categories in time dependent AUC | - | - | 5 y OS = 65.0%IM significantly better OS but other did not differentiate between each other | IM-inflamed better breast specific survival and BLIS the worse compared to others | |||
Legend: IHC – immunohistochemistry; LAR – luminal androgen receptor; AR – androgen receptor; RNA – ribonucleic acid; GGT1 – gamma-glutamyl transferase 1; FOXC1 – Forkhead Box C1; IDO-1 - indoleamine 2,3 dioxygenase-1; CD8 – cluster of diferential 8; TIL – tumour infiltrating lymphocites; CK – cytokeratine; EGFR – endothelial growth factor receptor; IM – immunomodulatory; M – mesenchymal; DCLK1 – doublecortin like kinase 1; MES – mesenchymal stem-cell like; T – tumour; N – lymph node; AUC – area under the curve; IQR – Interquartile range .
Table 2.
Clinical and pathological summary.
| Variables | |||||
|---|---|---|---|---|---|
| Age (Mean (SD) | 52.42 | (12.79) | |||
| Tumor size (Mean (SD) | 47.64 | (53.61) | |||
| Number of positive lymph nodes (Mean (SD) | 2.14 | (4.01) | |||
| T1-T2 | 58 | (31.0%) | |||
| Clinical Tumor(T) stage (N (%) | T3 | 57 | (30.5%) | ||
| T4 | 72 | (38.5%) | |||
| Clinical Lymph node(N) stage (N (%) | N0 | 79 | (42.2%) | ||
| N1 | 78 | (41.7%) | |||
| N2 | 28 | (15.0%) | |||
| N3 | 2 | (1.1%) | |||
| Histologic subtype (N (%) | Invasive ductal carcinoma | 176 | (94.2%) | ||
| other | 10 | (5.3%) | |||
| NA | 1 | (0.5%) | |||
| Tumor Grade (N (%) | 1 | 2 | (1.1%) | ||
| 2 | 59 | (31.6%) | |||
| 3 | 118 | (63.1%) | |||
| NA | 8 | 4.8% | |||
| ki67 (Mean (SD) | 65.47 | (24.49) | |||
| Angiolymphatic invasion (N (%) | Yes | 98 | (52.4%) | ||
| no | 39 | (20.9%) | |||
| Not-assessed | 50 | 26.7% | |||
| Lymphatic infiltrate (N (%) | Yes | 32 | (17.1%) | ||
| No | 100 | (53.5%) | |||
| Not-assessed | 55 | 29.4% | |||
| IHC-subtype (N (%) | Basal-like (BL) | unspecified | 36 | 19.6% | |
| Immunosuppressed (IS) | 57 | 31.0% | |||
| Imunoactivated (IA) | 20 | 10.9% | |||
| Luminal Androgen Receptor | 22 | 12.0% | |||
| Mesenchymal | 23 | 12.5% | |||
| Mixed | 21 | 11.4% | |||
| Unclassifiable | 4 | 2.2% | |||
| Not amendable of subtyping | 3 | (1.6%) | |||
| Neoadjuvant chemotherapy (N (%) | ACx4 + TXTx4 | 144 | 77% | ||
| ACx4 + wPacx12 | 19 | 10.2% | |||
| TCx4 | 5 | 2.7% | |||
| Other regimens | 19 | 10.2% | |||
| Surgery modality (N (%) | Modified radical mastectomy | 120 | (64.2%) | ||
| Conventional mastectomy | 17 | (9.1%) | |||
| Conservative surgery | 50 | (26.7%) | |||
| Pathologic response (N (%) | Complete | 28 | (15.0%) | ||
| Noncomplete | 159 | (85.0%) | |||
| Pathologic complete response according to IHC-subtype (N (%) | Basal-like (BL) | unspecified | 7 | 19.4% | |
| Immunosuppressed (IS) | 8 | 14.0% | |||
| Imunoactivated (IA) | 6 | 30.0% | |||
| Luminal Androgen Receptor | 1 | 4.5% | |||
| Mesenchymal | 4 | 17.4% | |||
| Mixed | 1 | 4.8% | |||
| Unclassifiable | 1 | 25.0% | |||
Legend: SD – standard deviation; N – number of patients; AC – anthracycline + cyclophosphamide; TXT – docetaxel; wPac – weekly paclitaxel; TC – docetaxel + platinum.
Table 3.
Summary of the characteristics of patients who achieved a pathological complete response.
| Subject number | Age | Clinical stage (TNM) | histological subtype | Grade | Ki67(%) | Neoadjuvant regimen (x number of cycles) | IHC-subtype |
|---|---|---|---|---|---|---|---|
| Patient 1 | 66 | T4N1M0 | IDC | 2 | 90 | Other – Acx3 + wPacx3 | BLIS |
| Patient 2 | 63 | T3N0M0 | IDC | 3 | 5 | ACx4 + TXTx4 | unclassifiable |
| Patient 3 | 54 | T3N1M0 | IDC | 3 | 70 | ACx4 + TXTx4 | MES |
| Patient 4 | 67 | TxN2M0 | IDC | NR | 70 | ACx4 + TXTx4 | LAR |
| Patient 5 | 47 | T3N0M0 | IDC | 3 | 95 | ACx4 + TXTx4 | BLIS |
| Patient 6 | 60 | T4N2M0 | IDC | 3 | 80 | ACx4 + TXTx4 | BL-unspecific |
| Patient 7 | 47 | T4N1M0 | IDC | 3 | 80 | ACx4 + TXTx4 | BL-unspecific |
| Patient 8 | 52 | T4N1M0 | IDC | 3 | 90 | ACx4 + TXTx4 | LAR/BLIS |
| Patient 9 | 56 | T3N0M0 | IDC | 2 | 50 | ACx4 + TXTx4 | MES |
| Patient 10 | 44 | T3N1M0 | IDC | 3 | 95 | ACx4 + TXTx4 | BL-unspecific |
| Patient 11 | 61 | T4N2M0 | IDC | 2 | 70 | ACx4 + TXTx4 | BLIA |
| Patient 12 | 39 | T3N0M0 | Other | NR | 95 | ACx4 + TXTx4 | BLIS |
| Patient 13 | 47 | T2N0M0 | IDC | 2 | 95 | ACx4 + TXTx4 | BLIA |
| Patient 14 | 46 | T4N3M0 | IDC | 2 | 60 | ACx4 + TXTx4 | BL-unspecific |
| Patient 15 | 44 | T3N0M0 | IDC | 3 | 90 | ACx4 + TXTx4 | BLIS |
| Patient 16 | 68 | T4N0M0 | IDC | 2 | 75 | ACx4 + TXTx4 | BLIA |
| Patient 17 | 64 | T4N2M0 | IDC | 3 | 70 | Other - TCx4 + ACx6 | BL-unspecific |
| Patient 18 | 41 | T3N0M0 | IDC | 3 | 70 | ACx4 + TXTx4 | BLIA |
| Patient 19 | 63 | T4N0M0 | IDC | 2 | 15 | ACx4 + TXTx4 | BLIA |
| Patient 20 | 34 | T4N0M0 | IDC | 3 | 100 | ACx4 + TXTx4 | BLIS |
| Patient 21 | 37 | T3N0M0 | IDC | 3 | 50 | ACx4 + TXTx4 | BLIS |
| Patient 22 | 71 | T2N1M0 | IDC | 2 | 50 | ACx4 + wPacx4 | BLIA |
| Patient 23 | 43 | T3N0M0 | IDC | 3 | 70 | ACx4 + TXTx4 | BLIS |
| Patient 24 | 47 | T2N0M0 | IDC | 2 | 5 | ACx4 + TXTx4 | MES |
| Patient 25 | 62 | T1N0M0 | IDC | 3 | 80 | ACx4 + TXTx4 | BL-unspecific |
| Patient 26 | 51 | T2N1M0 | IDC | 3 | 80 | ACx4 + TXTx4 | MES |
| Patient 27 | 27 | T2N0M0 | IDC | 3 | 95 | ACx4 + TXTx4 | BLIS |
| Patient 28 | 59 | T4N0M0 | IDC | 3 | 60 | ACx4 + wPacx4 | BL-unspecific |
Legend: T – tumor; N – lymph nodes; M – metastasis; IDC – invasive ductal carcinoma; NR – not reported; AC – anthracycline + cyclophosphamide; TXT – docetaxel; wPac – weekly paclitaxel; TC – docetaxel + platinum; W – weak; I – intense.
Table 4.
Antibodies used in the analysis.
| Antibody | Definition of positivity expression | Brand | Dilution | Control |
|---|---|---|---|---|
| IDO-1 | > 10% of tumor cells | Abcam | 1:1000 | Breast |
| Claudin-3 | Allred score ≥ 4 | Abcam | 1:200 | Breast |
| Androgen Receptor | ≥ 20% of tumor cells | Cell Marque | 1:400 | Gallbladder |
| FOX-C1 | Moderate (M) or intense (I) | Abcam | 1:300 | Breast |
| Ki-67 | ≥1% of tumor cells | Ventana-Roche | Ready to use | Breast |
Legend: IDO-1 – Indoleamine 2,3-dioxygenase, FOX-C1 – Forkhead Box C1.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



