
Submitted:
27 April 2024
Posted:
28 April 2024
You are already at the latest version
Abstract
Low dietary intake of calcium, vitamin D, vitamin C and magnesium has been associated with increased risk of osteoporosis. The purpose of the study was to evaluate changes in several bone health indicators and metabolic biomarkers in postmenopausal women, with high osteopenia or osteoporosis, followed by a nutritional intervention program. 115 apparently healthy postmenopausal women (52±8 years old) were randomized into four groups: group I (n=40) received daily 1000 mg vitamin C, 100 mcg vitamin D3, 500 mg calcium(Ca) and 300 mg magnesium (Mg); group II (n=42) received daily 100 mcg vitamin D3, 500 mg Ca and 300 mg Mg; group III (n=18) received daily 5 mg bisphosphonates, 100 mcg vitamin D3, 500 mg Ca and 300 mg Mg; and group IV (n=15) received daily about 364 mg polyphenols via an innovative functional food (50 g olive paste enriched with mountain tea extract) along with 100 mcg vitamin D3, 500 mg Ca and 300 mg Mg. Groups I -III received supplementation for a year whereas group IV for 5 months. Changes in bone health indicators and metabolic biomarkers were assessed at the beginning and at the end of the study. Anthropometric indices and whole-body bone mineral density (BMD) were also evaluated at the beginning and at the end of the intervention period. The results revealed improved elevated levels of 25(OH)D3, in groups II, III and IV (+3,71% and +1.45% and +5.62% respectively). Significant positive changes were recorded, for whole-body BMD, in all four study groups. Significant beneficial changes for total cholesterol were observed in group IV (-2.07%, P<0.05) and positive changes in group I for HDL biomarker (+61.62%, P<0.05). Additional larger-scale clinical trials and intervention studies are considered essential, to fully investigate and elucidate associations between dietary components and biochemical indices of bone health.
Keywords:
micronutrients
; functional foods
; olive paste
; bone mineral density
; bone health indicators
; postmenopausal women
1. Introduction
Osteoporosis is an extremely debilitating ailment characterized by reduced bone density and progressive weakening of bones, associated with an increased risk of bone fractures. Osteopenia is considered the precursor of osteoporosis and as defined by World Health Organization (WHO) is characterized by decreased bone mineral density (BMD) with a T-score between 1 up to 2.5 while a T-score below 2.5 indicates osteoporosis [1,2].
Aging has been associated with numerous chronic diseases including sleep disorders, malnutrition, osteoporosis as well as increased risk of falls [3,4,5]. Osteoporosis is the most prevalent metabolic disease among the elderly, leading to fractures, chronic pain, and higher mortality rates [6,7]. In the United States, over forty million people are diagnosed with osteoporosis due to progressive bone loss [8], while globally, more than 200 million are affected [2], with higher rates among postmenopausal women due to hormonal changes [8,9,10].
In Greece, the proportion of osteoporotic patients aged 50 and above receiving treatment rose from 1.67% in 2001 to 8.2% in 2011 [1]. Osteoporosis involves an imbalance between bone formation and resorption regulated by hormones like parathyroid hormones, calcitonin, and vitamin D. Various factors such as menopause, nutritional deficiencies, inflammation, aging, endocrine disorders, and cancer contribute to abnormal bone metabolism [11].
Research has predominantly focused on calcium and vitamin D for osteoporosis prevention and bone health. However, recent studies highlight additional nutrients like magnesium, potassium, vitamin C, vitamin K, B vitamins, carotenoids, and polyphenols in maintaining healthy BMD and preventing bone loss. More specifically, population studies suggest that magnesium and potassium promote bone strength by enhancing mineralization [12], while carotenoids and vitamin C potentially protects BMD by reducing oxidative stress [13]. Furthermore, intake of vitamin K is associated with a 65% decrease in the risk of hip fracture [14]. Recent research also highlights the potential benefits of ascorbic acid, with positive correlations observed between vitamin C supplementation and BMD [15]. Additionally, B vitamins have been found to indirectly influence bone turnover by acting as cofactors in metabolic reactions that stimulate osteoblast activity and bone formation [16].
It is well documented that dietary calcium deficiency is linked to low BMD, leading to osteopenia and osteoporosis over time [22]. Calcium supplementation is widely recognized for osteoporosis prevention in postmenopausal women [23,24]. Combining calcium with vitamin D supplements may reduce fracture risk, particularly in populations with low dietary intakes [25,26,27]. Albani & Petrou's study suggests that this combination prevents osteoporotic fractures by enhancing bone formation [27].
It has been also shown that functional foods and bioactive ingredients, including polyphenols, can influence bone metabolism [17,18,19,20,21]. These findings suggest that functional foods may enhance bone and joint health in aging individuals by optimizing bone metabolism and calcium balance. For example, fortified functional foods containing calcium, vitamin D, magnesium, and vitamin K play a crucial role in promoting bone health. Additionally, some functional foods containing polyphenols may decrease urinary calcium loss or inhibit bone resorption [20]. Chicken eggshells are also identified as a promising natural calcium source for functional foods [21].
Although there is no universal definition for the “functional foods”, foods are considered functional when they provide specific health-promoting effects beyond their nutritional value, containing bioactive compounds such as vitamins, minerals, antioxidants, probiotics, and phytochemicals. [27,28]. Studies have demonstrated that adopting a diet rich in conventional functional foods, such as fruits, vegetables, raw cereals, and fish, significantly reduces the risk of chronic diseases, including osteoporosis. [29,30]. Among traditional Mediterranean foods, olive paste and olive oil are considered functional due to the presence of bioactive compounds like oleic acid and polyphenols, offering various health benefits such as cardioprotection, inflammation reduction, gut health support, and osteoporosis risk reduction [31]. Similarly, mountain tea (Sideritis sp.) and orange juice, rich in antioxidants, help mitigate oxidative stress and inflammation [32,33]. Mountain tea, recognized for its antioxidant potential, has shown promise in protecting against osteoporosis. Studies on Sideritis euboea extract suggest significant protection against bone loss and improved bone strength in osteoporotic rat models [34]. Despite promising results, further research is needed to confirm the efficacy of Greek mountain tea in treating osteoporosis.
The purpose of the present study was to assess the impact of micronutrient supplementation, encompassing calcium, magnesium, vitamin C, and vitamin D, along with an innovative functional food fortified with polyphenols, on several bone health indicators, metabolic biomarkers, and BMD in postmenopausal women at heightened risk of osteopenia or osteoporosis. Limited research exists on the influence of vitamin C and polyphenol supplementation on bone metabolism, thus emphasizing the novelty of incorporating the innovative functional food supplement in this investigation.
2. Materials and Methods
2.1. Recruitment Process
The prospective randomized controlled trial was carried out at the Human Nutrition Unit (HNU), a research facility based within the University of the Aegean, Department of Food Science. Ethics approval was granted by the University of the Aegean Ethics Committee (No. 7505, 20 October 2019), provided that all procedures and protocols were followed in accordance with the ethical standards of the Declaration of Helsinki. The study is registered on ClinicalTrials.gov with unique protocol ID: Osteo21 and Identifier: NCT06135831. Phase I recruitment took place from March 2019 to June 2021 and women between 45 to 75 years of age, from Lemnos, Attica area and Tripoli city in Peloponnese, were invited to participate in the study, via private clinics. A total number of subjects n=130 was recruited and all participants were thoroughly informed with printed forms about the study objectives, methods, anticipated benefits confidentiality of the data and the voluntary nature of participation. The subjects were assured that their contribution to the study would be completely anonymous and signed a consent form. Medical history, recent biochemical blood tests (<15 days old) and data regarding their whole-body BMD were recorded. Inclusion criteria were age 45 to 75 years old (y.o.) and screening for osteoporosis (T-score ≤ -2.5) and osteopenia of the femur strength or spine (-2.5 ≤ T-score ≤ -1.0) took place. Subjects who were age > 75 y.o. and <45 years old and have been diagnosed with chronic diseases including cancer, diabetes, coronary heart disease and stroke were excluded from the study. All volunteers (n=130) were offered with a free of charge service to be able to provide their biochemical tests and their T-scores as part of the research protocol. The HNU research group provided the participants with the contact details of certain diagnostic clinics and private doctors, they were collaborating with, depending on the city and place of residence of the volunteers, so they were able to undertake their blood tests and DXA scan. Figure 1 present the flow diagram of the study according to CONSORT reporting guidelines for clinical trials. https://www.equator-network.org/reporting-guidelines/consort/.
2.2. Intervention Study Design
Eligible participants were 115 postmenopausal women, with an increased risk of osteoporosis and osteopenia, while 15 individuals were excluded because they did not meet the inclusion criteria. The subjects were randomized, with random series of numbers 1 to 4, into 4 groups: group I (n=40) received daily vitamin C (1000 mg), vitamin D3 (100 mcg), calcium (Ca) (500 mg) and magnesium (Mg) (300 mg); group II (n=42) received daily vitamin D3 (100 mcg), Ca (500 mg) and Mg (300 mg); group III (n=18) received bisphosphonates (alendronate and risedronate) (150 mg monthly-5 mg daily), vitamin D3 (100 mcg), Ca (500 mg ) and Mg (300 mg); and group IV (n=15) received daily 364 mg polyphenols via 50 g of an innovative functional food (Kalamata olive paste with mountain tea rich in polyphenols, (total phenolic 7,28±3.11 gallic acid/g) along with vitamin D3 (100 mcg), Ca (500 mg) and Mg (300 mg). Groups I -III received supplementation for a year (October 2020 to September 2021) whereas group IV received supplementation for 5 months (October 2020 to February 2021). The supplements and the functional food were delivered to the participants, by post, every 3 months. The supplements of vitamin C, vitamin D3, calcium, magnesium as well as bisphosphonates where be supplied by local pharmacy.
2.2.1. Questionnaires
Nutritional assessment was evaluated using a semi-quantitative food frequency questionnaire (FFQ) [35], modified to include additional natural functional foods, without alterations to the type of questions [36]. Modified categories included dairy products (low-fat, enriched-fortified etc.), meat (semi-dough etc.), superfoods, sweet (low-fat, sugar free), fruit juices, fruit and vegetables, cereals (vegetable fiber etc.) beverages (stew, without alcohol, with sweeteners), oil (olive oil, dried fruits, fish oil). Participants were informed on the suggested portion sizes for each food included on the list and were asked to record their frequency of consumption. Frequency of consumption was recorded as “everyday”, “3–6 times per week”, ‘2 times per week”, “once a week”, “1–2 times per month” and” seldom/never”. Moreover, participants were asked to complete a questionnaire assessing the adherence to Mediterranean-style diet (MedDietScore) [31,32,33]. The final score provides three levels of compliance categorizing as: low 0-20, moderate 21-35 and high 36-55 adherence. Higher values of this diet score indicate greater adherence to the Mediterranean diet.
Self-reported questionnaires were used, as a reaction to covid-19 restrictions and changes. More specifically, a general self-reported sociodemographic questionnaire was used to obtain data on age, gender, occupation, years of education, income etc. Participants also self-reported their medical history answering a standard questionnaire on several diseases in the form of Yes-or-No questions. In addition, self-reported data were collected for their weight and height [37,38,39].
Physical activity levels were evaluated using a 3-day questionnaire via online personal interview. Women were asked to report the time spent, alone or with a companion, in various physical activities on two weekdays and one weekend day. The questionnaire used classifies all activities during work, at the gym, and during leisure time into four categories related to the average intensity of each activity and its effects on the cardiovascular and musculoskeletal systems [40]. Questionnaires were designed to assess frequency of physical activity (months/year, weeks/month, days/week), duration (hours) and intensity (moderate to high). Based on these data, the total time spent in organized (including all activities regularly performed each week, usually in the gym under the guidance of a trainer) and unorganized activities that promote bone mass was calculated. The total weekly hours found to be spent in such activities were defined as moderate-intensity and intense physical activity. Physical activity was assessed only at the beginning of the study.
2.2.2. Anthropometric measurements
Body mass index (BMI) was calculated by dividing weight (kg) with standing height squared (m2). Participants were classified as underweight, normal weight, overweight and obese according to the BMI criteria for adult population (WHO, 2021) (41). More specifically, participants with a BMI < 18.5 were classified as underweight, normal weight with BMI between 18.5-24.9, overweight ranged between 25.0-29.9, and obese classified with BMI >30. Body composition analysis was performed assessing body fat (kg), muscle mass (kg), body water (kg) and bone mass (kg) with a segmental body composition analyzer (TANITA SC300), according to the body composition procedures manual. Height was measured with a stadiometer (seca 222) and accuracy ±0.5 cm. Waist and hip ratio were measured with a measuring tape (seca). Waist to hip ratio (WHR) was estimated by dividing the waist circumference to hip circumference (WHR = Waist Circumference/Hip Circumference). It is generally used as an indicator of body fat distribution and as a predictor of metabolic health risks including insulin resistance and impaired lipid profile [42].
Bone density was assessed by Dual Energy X-ray Absorption (DXA) (HOLOGIC EXPLORER Dexa scanner / HOLOGIC Discovery Dexa scanner, Hologic Inc.). DXA scan included whole-body BMD T-scores andwere performed at baseline and at the end of the study. The precision of DXA measurements can vary depending on factors such as the specific body region being measured, the DXA device used, and the population being studied. It is therefore certain that DXA measurements can be affected when data are collected from different sites, as here. Not having cross-calibration, due to challenges posed by covid-19 restrictions, is considered a limitation. However, taking proactive steps to address and mitigate the impact on the present study's validity enhances the credibility of our findings. Strategies to ensure quality control across the different sites included the development of standard operating procedures (SOPs), and the confirmation that all operators were adequately trained and certified in DXA measurements. In addition, harmonization techniques including standardized questionnaires and measurement procedures were applied.
2.3. Biomarkers
The procedure for testing volunteers' blood for biomarkers was performed after a 12-hour overnight fast, and blood samples were collected early in the morning (8:30-10:00 AM). The volunteers visited the clinics after a scheduled appointment and performed the corresponding biochemical tests. Biochemical analyses were carried out with an automated biochemical analyzer (COBAS c111, Roche, Basel, Switzerland). The participants provided the test results, to the research team, no later than 15 days after the scheduled appointment. Circulating levels of 25-OH vitamin D3, vitamin C, calcium (Ca), magnesium (Mg), parathyroid hormone (PTH), triglycerides, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, glucose, glycated hemoglobin HbA1c were recorded. The biomarkers assays were provided byRoche Diagnostics, F. Hoffmann-La Roche Ltd.
2.4. Olive paste enriched with mountain tea
Homogenized olive pastes, enriched with mountain tea, were supplied by two accredited Greek olive oil and olive products companies, Arcadian Taste and GAEA. The fortified olive pastes contained 7.5 g of extra virgin olive oil, 3.75 g of salt, 3.75 g of grated oregano, 3.75 g of grated pepper, 7.5 g of grated garlic, 6.25 g of orange juice, 65 g of Kalamon olives without seeds and 3 g of mountain tea and weighted 100 gr per portion size, as well. The nutritional composition (per 100 g), of the fortified homogenates of olive pastes mix, are described in the table below.

Table 1.
Nutritional composition of fortified homogenates of olive paste mix, per portion size.
| Nutritional Composition (per 100 g) | |
|---|---|
| Energy (kcal) | 157 |
| Carbohydrates (g) | 6.6 |
| Fat, total (g) | 12.4 |
| Protein (g/kg) | 2.7 |
| Saturated fat (g) | 1.1 |
| Sugar , total (g) | 2.7 |
| Total phenolic ingredients (μg Gallic Acid) | 728±311 |
| Total Antioxidant activity (μmol FeSO4) | 956±33 |
In vitro studies were performed at the HNU laboratory aiming to test the phenolic components and the antioxidant activity of the fortified olive pastes mix with Folin-Ciocalteau and FRAP (ferric reducing/antioxidant power assay) assays, according to relevant studies (36-43). The results showed that the novel olive paste with mountain tea had total phenolic content 7,28±3,11 μg gallic acid/g and total antioxidant activity 9,56±0,33 μmol FeSO4/g.
2.5. Statistical Analysis
2.5.1. Sample size calculation
Sample size calculation was performed using G*Power software version 3.1.9.2. Considering a probability of 95% that the study will detect a treatment difference at a two-sided 0.01 significance level, the sample of 120 individuals, 30 per group, allows the detection of a difference of 10% on Vitamin D levels within groups, calculated from the expected SD=0.2 between the differences of the treatment groups.
2.5.2. Data analysis
All data are presented as means±SD and as percentages (%) for differences observed at baseline and at the end of the study. The normal distribution of continuous variables was tested via Kolmogorov-Smirnov test. Changes in subjects` characteristics at baseline were estimated with one-wat ANOVA. Repeated measures ANOVA was used to define significant differences in all variables tested for each study groups, at baseline and at the end of the study. Repeated measures ANOVA was used to estimate significant differences amongst the four study groups, at baseline and at the end of the study. Statistical analysis was performed with the IBM-SPSS Statistics (version 21.0 IBM Corp, Armonk, NY). Correlations were performed by using x2 test. Level of statistical significance was at P<0.05.
3. Results
Descriptive data, at baseline, are shown in Table 2 for each study group. There were no differences that were statistically significant across groups, indicating homogeneity of the subjects within all groups at the beginning of the study.
The results did not indicate statistically significant differences between the four groups in all tested biomarkers (p<0,05). Table 3 shows the differences observed in bone health indicators tested, at the beginning and at the end of the study, including vitamin D (25(OH)D3) and parathyroid hormone (PTH). There were no statistically significant differences in either vitamin D (25(OH)D3) or PTH between the first and the second measurement.
Statistically significant differences were recorded, between the two measurements, for total cholesterol (Table 4), triglycerides, and HDL (Table 1 in Supplementary material). More specifically, a significant increase of serum cholesterol was noted for group III, in addition to a significant decrease observed in total cholesterol (-2.07%, P=0.034) for group IV. Difference in triglyceride levels, that were statistically significant, were also recorded between baseline and the end of the study, for both groups II and IV at +17.02%, (P= 0.034) and +16.32% (P=0.025) respectively. Moreover, an increase in HDL that was statistically significant was recorded for group I (+61.62%, P=0.047). This generated an additional significant difference in HDL, across groups, at the end of the study period (P=0.032) (data are shown in supplementary material). There were no other differences that were statistically significant.
Additional blood biomarkers were tested and differences that were statistically significant were noted for glucose, glycosylated hemoglobin (HbA1c) (Table 4) and magnesium (Mg) for group IV, only (Table 2 in Supplementary material). More specifically, significantly increased values were recorded for glucose (+2.33%, P=0.048) and HbA1c (+1.56%, P=0.0027), whereas decreased value with statistical significance was observed for Mg (-20.19%, P=0.01).
Differences that were statistically significant were recorded for whole-body BMD, at the end of the intervention period for all four groups (Table 5). More specifically the highest increase in whole-body BMD (+12.23%, P=0.043) was observed for group III, whereas the lowest increase was noted for group II (+1.55%, P=0.036%). In addition, for both groups I and IV a positive increase in whole-body BMD was recorded at +3.46 (P=0.027) and +11.98% (P=0.003) respectively.
A positive correlation was observed between intense physical activity and bone density for groups I, II and III at the end of the intervention period. The mean whole-body BMD was slightly higher for group II (2.83 ± 0.38) compared to groups I (2.65 ± 0.48) and III (2.61 ± 0.50).
Table 6.
Correlation of physical activity with whole-body BMD.
| Physical activity levels | Total bone density (rho) | P-value |
|---|---|---|
| moderate | ||
| Group I | - | - |
| Group II | - | - |
| Group III | - | - |
| Group IV | 3.20 ± 0.28 | 0.726 |
| P-value | - | - |
| intense | ||
| Group I | 2.65 ± 0.48 | 0.032 |
| Group II | 2.83 ± 0.38 | 0.032 |
| Group III | 2.61 ± 0.50 | 0.032 |
| Group IV | - | - |
| P-value | - | - |
*Correlation is significant at the 0.05 level with ANOVA test.
The results on Mediterranean diet showed moderate adherence in all 4 groups, without statistically significant differences (data not shown).
4. Discussion
The present study was designed to examine the effects of micronutrient supplementation in bone health indicators and other health biomarkers as well as in whole-body BMD, in postmenopausal women, with high risk of osteopenia or osteoporosis, after one-year (groups I, II and III) and five months (group IV) intervention. Various bone health indicators and other not traditional bone metabolism biomarkers, which can provide valuable information about the participants' bone health and metabolism, measured in the present study.
Reductions in parathyroid hormone (PTH) levels were observed in groups II and III, indicating an inverse correlation with 25-hydroxyvitamin D3 (25(OH)D3) levels. This documented inverse relationship between decreased serum 25(OH)D3 levels and PTH, crucial for calcium homeostasis and bone health, is well recognized [43]. However, the precise threshold at which 25(OH)D3 affects PTH levels remains uncertain [44]. Moreover, the optimal dose of calcium supplementation needed to inhibit PTH secretion is undefined, suggesting that inadequate supplementation may have contributed to elevated PTH levels in groups I and IV [45]. It is proposed that decreased PTH levels may result from increased 25(OH)D3 levels, especially with high calcium intake (>800mg) [45], potentially explaining the decrease in PTH levels in groups II and III. Further investigation is warranted to elucidate the metabolic response of PTH in postmenopausal women during calcium and vitamin D supplementation.
Overall, although beneficial changes in 25(OH)D3 levels were observed in groups II, III, and IV, no significant differences were detected across the study groups. This suggests that the administered amount of 25(OH)D3 may have been insufficient to adequately elevate serum levels, and/or the study duration may have been too short. Additionally, for group IV, low 25(OH)D3 levels may have been influenced by seasonal variations, as the intervention period extended from October to February. This finding aligns with prior research indicating decreased 25(OH)D3 levels during winter months, potentially outweighing the impact of vitamin D supplementation [46]. Interestingly, vitamin D deficiency appears more prevalent in elderly populations in Mediterranean countries, such as Greece, Italy, and Spain, compared to regions with less sunlight exposure. This disparity may be attributed to various factors, including dietary habits, food fortification practices, and vitamin D supplement usage in different regions.
Intervention programs typically evaluate the effectiveness of calcium and/or vitamin D supplementation on bone metabolism by assessing changes in whole-body bone mineral density (BMD), rather than specific bone health indicators [47]. During the present study, significant increases in whole-body BMD were observed in all four study groups, with the highest increase noted in group III, followed by group IV, I, and II, in descending order. Similar findings have been reported in previous research, particularly in postmenopausal Caucasian women receiving calcium supplementation (1600 mg/d) for a year [48]. While dietary interventions aim to mitigate age-related declines in BMD, significant increases are not typically expected. Some nutritional interventions have shown no effect on whole-body BMD [50], while others have reported moderate declines in bone loss following calcium and vitamin D supplementation [51].
The highest increase in whole-body BMD observed in group I may be attributed to vitamin C supplementation, as vitamin C plays a significant role in bone health. Research indicates that dietary vitamin C intake is associated with higher whole-body BMD in postmenopausal women [53] and affects bone turnover by enhancing collagen synthesis and osteoblast genesis [54]. Additionally, studies have shown an inverse relationship between vitamin C intake and the risk of fracture or osteoporosis [55].
Experimental pre-clinical data also suggest that a polyphenol-rich olive extract may help maintain whole-body bone mineral density (BMD) in postmenopausal women at high risk of osteoporosis [52]. Continuous monitoring of diet and supplementation is crucial for assessing long-term impacts on BMD response, and larger sample sizes are needed for comprehensive evaluation.
Previous studies [56,57,58] have linked serum parameters like triglycerides (TG) and cholesterol with bone health and metabolism. In our study, normal TG levels (<150 mg/dl) were seen in groups I, II, and IV, while group III showed borderline high levels (150-199 mg/dl) both at baseline and study end. Total cholesterol remained within normal ranges (<200 mg/dl) for groups II, III, IV, with group I showing borderline high levels (200-239 mg/dl). LDL (100-129 mg/dl) and HDL (>60 mg/dl) levels were normal in all groups at both time points. These findings are consistent with prior research on calcium and vitamin D co-supplementation, indicating no association with serum LDL levels [51]. Additionally, group IV showed significant improvements in total cholesterol, and group I exhibited positive changes in HDL, aligning with previous studies suggesting a beneficial effect of vitamin D and calcium supplementation on these parameters.
The variability in the above results underscores the necessity for larger-scale, well-designed intervention trials to elucidate the effects of micronutrient supplementation on lipid biomarkers. Nonetheless, the significant reduction in total cholesterol observed in group IV, coupled with the statistical increase in BMD, indicates a positive impact. This aligns with previous research suggesting a negative correlation between total cholesterol and BMD [56,57].
Consistent with our findings, Filip et al. documented physiological ranges in serum lipid profiles for total cholesterol, TG, LDL, and HDL-cholesterol after administering a combination of polyphenol-rich olive extract (250 mg/day) and calcium (1000 mg/day) [58]. Both our study and that of Filip et al. suggest a novel positive influence on blood lipid profiles, potentially offering additional health benefits associated with olive polyphenol intake.
However, conclusive statements regarding the effect of micronutrient supplementation on lipid profile biomarkers in postmenopausal women cannot be drawn from our study alone, necessitating further investigation.
No statistically significant differences were found in circulating calcium levels among all study groups at the intervention's end. Improved serum calcium levels were observed in Groups I and III, likely due to calcium supplementation. However, there were no other statistically significant positive changes in serum calcium or magnesium levels, possibly due to low supplementation adherence.
While calcium plays a significant role, recent interest in natural components like polyphenols has grown. In the study by Filip et al., the polyphenol-rich olive extract administered to postmenopausal women with osteopenia for 12 months provided 100 mg of oleuropein daily. Despite not reaching the intended sample size (32 subjects), the treatment group showed a significant increase in osteocalcin levels compared to the placebo group [52].
In recent years, there has been significant interest in functional foods, with studies often assessing their total antioxidant capacity (TAC) and total phenolic content (TPC) using in vitro models. In the present study, the total antioxidant and phenolic content of olive paste enriched with mountain tea, was evaluated. Variations in antioxidant capacity and phenolic content among similar products may result from differences in sample preparation, extraction methods, and environmental conditions [59,60] Similar TPC values (6.4–180.5 mg GA/g) were determined for Thai plants (extracts with 95% ethanol), traditional Chinese medicinal plants (1.1–52.3 mg GA/g in extracts), culinary herbs and spices from Finland (18.5–147.0 mg GA/g) indicating a correlation between TAC and TPC. Medicinal herbs with high TAC tend to have elevated TPC levels, unaffected by changes in extraction solvents. Mountain tea is suggested as a potential antioxidant source with potential health benefits, including reducing the risk of osteoporosis [61].
Previous studies have linked similar functional foods, part of the Mediterranean diet, to positive associations with BMI and reducing osteoporosis risk [61]. Our findings also indicate a positive association between consumption of polyphenol-rich olive samples in group IV and healthy BMI within physiological ranges (18.5 – 24.9) at the end of the intervention period. These results highlight the scientific advancement of our study and the potential benefits of innovative functional foods in postmenopausal women at high risk of osteoporosis. However, consumer awareness regarding the health benefits of foods remains low [62].
Intense exercise was positively associated with increased whole-body BMD in groups I, II, and III, consistent with previous studies in postmenopausal women [49]. Weight-bearing and resistance exercises, particularly those involving high-impact and intensity, benefit bone health. Multicomponent exercise programs for osteoporosis aim to prevent bone loss, enhance muscle strength, balance, and reduce fear of falling [64]. While individual trials show varied outcomes regarding balance, muscle strength, and fear of falling, supervised exercise programs have demonstrated significant improvements in these areas for women with osteoporosis and vertebral fracture [64,65]. Regular monitoring and adjustments to exercise programs may be necessary for safe and effective implementation.
The present study is subject to several limitations. Firstly, challenges in obtaining consent for health record access and blood tests resulted in a reduced sample size despite efforts to ensure diverse representation. Furthermore, logistical constraints affected the provision of the novel food product to Group IV and additional supplements to Group II, leading to smaller participant numbers and a shorter intervention period for Group IV (five months) compared to the other groups (one year). Additionally, Group III had fewer participants due to difficulties in drug therapy supply. Delays in novel food production, beyond our control, further impacted the planned study timeline for Group IV, necessitating a shortened intervention and data collection period. This limitation holds significant importance, emphasizing the necessity for conducting a new interventional study of extended duration. Such a study is imperative to ensure the validity and robustness of the findings concerning the impact of the novel food product on the tested biomarkers.
Another limitation of the study was the absence of a control group. However, Group III, which received conventional therapy alongside supplements, could serve as a positive control group for comparisons with additional supplements or novel food.
Expanding the recruitment of volunteers to encompass diverse regions within the country, including urban, rural, and island locales, would enhance the robustness of conclusions drawn for the Greek population. Nevertheless, the incorporation of data from multiple locations, including Lemnos, the Attica region, and Tripoli city in Peloponnese, may have introduced potential confounding variables linked to data collection practices, especially given the disruptions posed by the COVID-19 pandemic. Therefore, it is imperative for future studies to establish standardized protocols and procedures for data collection across all study sites. Moreover, the inclusion of self-reported questionnaires, necessitated by contingency planning for Covid-19, introduces further potential confounding factors such as response bias, recall bias, temporal changes, perception of health, inconsistency in reporting, variability in interpretation, and lack of specificity. Despite proactive measures to support participant adherence to interventions, including virtual check-ins and electronic reminders, challenges stemming from the Covid-19 pandemic, such as disruptions in daily routines, heightened stress levels, and limited access to resources, may have impacted adherence.
Another limitation concerns the scope of the study, which focused solely on evaluating whole-body BMD. This decision was influenced by the challenges presented by the Covid-19 pandemic, resulting in the omission of DXA examination at anatomical sites such as the femoral neck and lumbar spine, which also serve as reference points for osteoporosis diagnosis. Furthermore, the study's analysis was restricted to BMD, overlooking other key biochemical markers of bone tissue remodeling, including NTX, CTX, b-ALP, and OC. Consequently, the investigation primarily examined general health biomarkers rather than specific bone health indicators in postmenopausal women with osteopenia or osteoporosis. Moreover, future studies could explore the potential benefits of including an additional group receiving bisphosphonates and functional foods, thus providing an avenue for further investigation. The study also encountered limitations related to differences in mean age between groups, as well as the failure to consider postmenopausal duration as a key determinant of bone density. Additionally, bisphosphonates were not analyzed in plasma, and regression analysis was not conducted to elucidate the effects of individual supplements, postmenopausal status, bisphosphonates, and physical activity on BMD. These limitations collectively contribute to potential sources of variability and complexity in observed patterns.
While we acknowledge these limitations, the insights gained from the available data still provide valuable information on the effects of polyphenol-rich novel-food supplementation on whole-body BMD and bone health indicators. Combining larger sample sizes and longer-term intervention studies increases precision and is more likely to detect true effects or differences, thereby reducing sampling bias in future studies.
5. Conclusions
The observed positive and significant changes in BMD across all study groups may be attributed to both micronutrient supplementation (groups I, II, III, and IV) and innovative functional food supplementation (group IV). Intense physical activity is positively associated with a significant increase in BMD. Supplementation, even after a 5-month intervention, led to increased BMD and maintenance of higher physiological levels of serum calcium, 25(OH)D3, vitamin C, and magnesium in postmenopausal women at high risk of osteoporosis. However, conclusions for group IV remain inconclusive due to the short-term nature of the study, which may not adequately assess the durability of interventions. Larger-scale clinical trials and intervention studies are needed to fully investigate associations between dietary components and biochemical indices of bone health. Collaboration with food companies producing olive oil and olive products, such as olive paste, could facilitate the implementation and promotion of novel food products in the market. Further studies are warranted to validate the results of the present study and explore the role of bioactive compounds in bone health parameters.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, Melina Konstantinidi and Antonios Koutelidakis; Data curation, Stavroula Stoupi; Formal analysis, Melina Konstantinidi and Stavroula Stoupi; Investigation, Melina Konstantinidi , Ioannis Anastasiou, Vlachos Nikolaos and George Tsakotos ; Methodology, Melina Konstantinidi , Ioannis Anastasiou, Vlachos Nikolaos, George Tsakotos and Antonios Koutelidakis; Project administration, Antonios Koutelidakis; Resources, Melina Konstantinidi , Ioannis Anastasiou, Vlachos Nikolaos and George Tsakotos ; Software, Melina Konstantinidi and Stavroula Stoupi; Supervision, Antonios Koutelidakis; Validation, Stavroula Stoupi, Ioannis Anastasiou, Vlachos Nikolaos, George Tsakotos and Antonios Koutelidakis; Visualization, Stavroula Stoupi and Antonios Koutelidakis; Writing – original draft, Melina Konstantinidi and Stavroula Stoupi; Writing – review & editing, Antonios Koutelidakis.
Funding
This research was partially funded by AGRICA II, network of excellence in agri-food research and innovation of the northern Aegean, project 80462, ESPA 2020.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the ethics and deontology committee of the University of the Aegean (protocol no. No. 7505, 20 October 2019).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
New data is not available.
Acknowledgments
Authors would like to thank every individual, postmenopausal women, who participated to the study for her cooperation. The authors also thank a lot the companies Arcadian Taste and GEAE for the production of the innovative food.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Makras, P.; Athanasakis, K.; Boubouchairopoulou N.; Rizou, S.; Anastasilakis, A. D.; Kyriopoulos, J.; Lyritis, G. P.; Cost-effective osteoporosis treatment thresholds in Greece. Intern Osteoporosis Found, 2015 7, 1949-57. [CrossRef]
- Kanis, J.A. et al.; A reference standard for the description of osteoporosis. Bone 2008, 42, 467-75. [CrossRef]
- World Health Organization. (2019). Decade of Healthy Ageing 2020-2030 Proposal [PDF]. Retrieved from https://www.who.int/docs/default-source/documents/decade-of-health-ageing/decade-ageing-proposal-en.pdf?Status=Temp&sfvrsn=b0a7b5b1_12.
- Vaisi-Raygani, A.; Mohammadi, M.; Jalali, R.; Ghobadi, A.; Salari, N.; The prevalence of obesity in older adults in Iran: a systematic review and metaanalysis. BMC Geriatr 2019, 19(1), 1–9. [CrossRef]
- Khoddam, H.; Eshkevarlaji, S.; Nomali, M.; Modanloo, M.; Keshtkar, A.A.; Prevalence of malnutrition among elderly people in Iran: protocol for a systematic review and meta-analysis. JMIR Res Protoc 2019, 8(11), e15334. [CrossRef]
- Cheraghi P.; Cheraghi, Z.; Bozorgmehr, S.; The Prevalence and risk factors of osteoporosis among the elderly in Hamadan province: a cross sectional study. Med J Islam Repub Iran 2018, 32, 111. [CrossRef]
- Cauley, J.A.; Public health impact of osteoporosis. J Gerontol Ser A Biomed Sci Med Sci 2013, 68(10), 1243–51.
- Bryant, L.; Osteoporosis and Osteopenia – Vitamin Therapy for stronger bones. e-book, 1st Edition; Chicago, 2019; pp.16.
- Liu, H.F.; Yang, L.; He, H.C.; Zhou, J.; Liu, Y; Wang, C.Y.; Wu, Y. C.; and He, C.Q. Pulsed electromagnetic fields on postmenopausal osteoporosis in southwest China: a randomized, active-controlled clinical trial. Bioelectromagnetics, 2013, 34, 323–332. [CrossRef]
- Yi-Chou, H.; Wu, C.C.; Liao, M. T.; Shyu, J.F.; Hung, C.F.; Yen, T.H.; Lu, C.L.; Lu, K.C.; Role of Nutritional Vitamin D in Osteoporosis Treatment. ClinicaChimicaActa, 2018, 84, 179-191. [CrossRef]
- Garnero, P.; and Cremers, S. Bone turnover markers. Principles of Bone Biology, 2020; pp. 1801-1832.
- Tucker, K.L.; Hannan, M.T.; Chen, H.; Potassium, magnesium, and fruit and vegetable intakes are associated with greater bone mineral density in elderly men and women. Am J Clin Nutr 1999, 69, 727–736. [CrossRef]
- Sahni, S.; Hannan, M.T.; Blumberg, J.; Inverse association of carotenoid intakes with 4-y change in bone mineral density in elderly men and women: the Framingham Osteoporosis Study. Am J Clin Nutr 2009, 89, 416–424. [CrossRef]
- Booth, S.L.; Tucker, K.L; Chen, H.; Dietary vitamin K intakes are associated with hip fracture but not with bone mineral density in elderly men and women. Am J Clin Nutr 2000, 71,1201–1208. [CrossRef]
- Rondanelli, M.; Peroni, G.; Fossari F.; Vecchio; Faliva, M.A.; Naso, M.; Perna, S.; Di Paolo, E.; Riva, A.; Petrangolini G, Nichetti, M.; Tartara A.; Evidence of a Positive Link between Consumption and Supplementation of Ascorbic Acid and Bone Mineral Density. Nutrients 2021, 13 (3), 1012. [CrossRef] [PubMed]
- Clarke, M.; Ward, M.; Strain, JJ.; Hoey, L.; Dickey, W.; McNulty H.; B-vitamins and bone in health and disease: the current evidence. Proc Nutr Soc 2014, 73(2), 330-9. Epub 2014 Feb 26. [CrossRef] [PubMed]
- Position Statement Management of osteoporosis in postmenopausal women: 2010 position statement of The North American Menopause Society. Menopause: The Journal of The North American Menopause Society, 2010, 17(1), 25-54.
- Smith, J. (2021). The effects of polyphenols on bone metabolism. In Johnson, A. (Ed.), Advances in Nutrition Research (pp. 45-62). Elsevier. [CrossRef]
- Konstantinidi M, Lydatakis A, Olympiou A, et al. Study of the relationship among the consumption of bio-functional foods ingredients with bone metabolism indices in middle-aged and elderly people with osteoporosis risk. Public Health and Toxicology. 2022;2(Supplement 1):A127. [CrossRef]
- Weaver CM, Liebman M. Biomarkers of bone health appropriate for evaluating functional foods designed to reduce risk of osteoporosis. Br J Nutr. 2002 Nov;88 Suppl 2:S225-32. [CrossRef] [PubMed]
- . Arnold M, Rajagukguk YV, Gramza-Michałowska A. Functional Food for Elderly High in Antioxidant and Chicken Eggshell Calcium to Reduce the Risk of Osteoporosis-A Narrative Review. Foods. 2021 Mar 19;10(3):656. [CrossRef] [PubMed]
- Dimakopoulos, I.; Magriplis, E.; Mitsopoulou, A.V.; Karageorgou, D.; Bakogianni, I.; Micha, R.; Michas, G.; Chourdakis, M.; Ntouroupi, T.; Tsaniklidou, S.M.; Argyri, K.; Panagiotakos, D.B.; Zampelas, A. Association of serum vitamin D status with dietary intake and sun exposure in adults. Clin Nutr ESPEN, 2019, 34:23-31. [CrossRef]
- Sun, L.L.; Li, B.L.; Xie, H.L. Associations between the dietary intake of antioxidant nutrients and the risk of hip fracture in elderly Chinese: a case-control study. Br J Nutr 2014, 112, 1706–1714. [CrossRef]
- Dermience, M.; Lognay, G.; Mathieu, F.; Goyens, P. Effects of thirty elements on bone metabolism. J Trace Elem Med Biol; 2015; 32:86-106. 8: 32. [CrossRef]
- . Caroli, A.; Poli, A.; Ricotta, D.; Banfi, G.; Cocchi, D. Invited review: dairy intake and bone health. A viewpoint from the state of the art. J Dairy Sci 2011, 94:5249-62. [CrossRef]
- Tabatabaei-Malazy, O.; Salari, P.; Khashayar, P.; Larijani, B. New horizons in treatment of osteoporosis Daru 2017 25(1):2.
- Albani, E.; Petrou, P. A systematic review and meta-analysis of vitamin D and calcium in preventing osteoporotic fractures. Clinical Rheumatology, 2020, 3571-3579.
- Brown, L.; Caligiuri, S.; Brown, D.; Pierce, G. Clinical trials using functional foods provide unique challenges. J. Funct. Foods 2018, 45, 233–238. [CrossRef]
- Martirosyan, D.; Singh, J. A new definition of functional food by FFC: What makes a new definition unique? Functional Foods in Health and Disease. FFHD 2015, 5, 209–223.
- Sirtori, C.R.; Galli, C.; Anderson, J.W.; Sirtori, E.; Arnoldi, A. Functional Foods for Dyslipidaemia and Cardiovascular Risk Prevention. Nutr. Res. Rev 2009, 22, 244–261. [CrossRef]
- Koutelidakis, A.; Dimou, C. The effects of functional food and bioactive compounds on biomarkers of cardiovascular diseases. In Functional Foods Text Book, 1st ed.; Martirosyan, D., Ed.; Functional Food Center: Dallas, TX, USA, 2016; pp. 89–117. Functional Food Center: Dallas, TX, USA.
- Kyritsakis, A. Olive Oil – Conventionla and Organic, Edible Olive – Olive Paste, 4th edition, Thessaloniki, 2007; p.328-336.
- Franke, A.A.; Cooney, R.V.; Henning, S.M.; & Custer, L. J. Bioavailability and antioxidant effects of orange juice components in humans. Journal of Agricultural and Food Chemistry 2005, 53(13), 5170–5178. [CrossRef]
- Dontas IA, Lelovas PP, Kourkoulis SK, Aligiannis N, Paliogianni A, Mitakou S, Galanos A, Kassi E, Mitousoudis A, Xanthos TT, Papaioannou N, Lyritis GP. Protective effect of Sideritis euboea extract on bone mineral density and strength of ovariectomized rats. Menopause. 2011 Aug;18(8):915-22. [CrossRef] [PubMed]
- NHANES. NHANES Food Questionnaire. Atlanta, 2019; Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_03_04/tq_fpq_c.pdf (accessed on 10 December 2019).
- Ntrigios, I.; Ntrigiou, V.; Dimou, C.; Rigopoulos, N.; Koutelidakis, A. Correlation of specific functional foods consumption with anthropometric characteristics and body composition on a sample of 18–65 years old aged adults from Greece. In Proceedings of the 22nd International Conference Functional Foods and Chronic Diseases: Science and Practice, Boston, MA, USA, 22 September 2017.
- Alissa, E.M.; and Gordon, A.F. “Functional Foods and Nutraceuticals in the Primary Prevention of Cardiovascular Diseases”. Journal of Nutrition and Metabolism 2012, Volume 2012, p.p. 16.
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary patterns: a Mediterranean diet score and its relation to clinical and biological markers of cardiovascular disease risk. Nutr Metab Cardiovasc Dis 2006, 16(8), 559-568.
- Papagianni, O.; Moulas, I.; Loukas, T.; Magkoutis, A.; Skalkos, D.; Kafetzopoulos, D.; Dimou, C.Μ.; Karantonis, H. C.; Koutelidakis, A. E. Trends in Food Innovation: An Interventional Study on the Benefits of Consuming Novel Functional Cookies Enriched with Olive Paste. Sustainability, 2021 13(20).
- Shedd, K.M.; Hanson, K.B.; Alekel, D.L.; Schiferl, D.J.; Hanson, LN.; Van Loan MD.; Quantifying leisure physical activity and its relation to bone density and strength. Med Sci Sports Exerc 2007 39(12), 2189-98. [CrossRef] [PubMed]
- WHO. Obesity and Overweight Fact Sheet. 2021; Available online: https://www.who.int/news-room/fact-sheets/obesity-andoverweight (accessed on 10 June 2021).
- Myint, PK.;Kwok, CS.; Luben,; RN.; Wareham, NJ.; Khaw KT.; Body fat percentage, body mass index and waist-to-hip ratio as predictors of mortality and cardiovascular disease. Heart 2014 100(20), 1613-9. [CrossRef] [PubMed]
- Mukhopadhyay P, Ghosh S, Bhattacharjee K, Chowdhury S. Inverse Relationship Between 25 Hydroxy Vitamin D and Parathormone: Are there Two Inflection Points? Indian J Endocrinol Metab. 2019 Jul-Aug;23(4):422-427. [CrossRef] [PubMed]
- Rosen CJ. Clinical practice. Vitamin D insufficiency. N Engl J Med. 2011 Jan 20;364(3):248-54. PMID: 21247315. [CrossRef] [PubMed]
- Aloia J, Bojadzievski T, Yusupov E, Shahzad G, Pollack S, Mikhail M, Yeh J. The relative influence of calcium intake and vitamin D status on serum parathyroid hormone and bone turnover biomarkers in a double-blind, placebo-controlled parallel group, longitudinal factorial design. J Clin Endocrinol Metab. 2010 Jul;95(7):3216-24. Epub 2010 May 12. [CrossRef] [PubMed]
- Meier C, Woitge HW, Witte K, Lemmer B, Seibel MJ. Supplementation with oral vitamin D3 and calcium during winter prevents seasonal bone loss: a randomized controlled open-label prospective trial. J Bone Miner Res. 2004 Aug;19(8):1221-30. Epub 2004 May 24. [CrossRef] [PubMed]
- Weisman SM, Matkovic V. Potential use of biochemical markers of bone turnover for assessing the effect of calcium supplementation and predicting fracture risk. Clin Ther. 2005 Mar;27(3):299-308. [CrossRef] [PubMed]
- Méndez-Sánchez L, Clark P, Winzenberg TM, Tugwell P, Correa-Burrows P, Costello R. Calcium and vitamin D for increasing bone mineral density in premenopausal women. Cochrane Database Syst Rev. 2023 Jan 27;1(1):CD012664. [CrossRef] [PubMed]
- Kemmler W, Engelke K, Lauber D, Weineck J, Hensen J, Kalender WA. Exercise effects on fitness and bone mineral density in early postmenopausal women: 1-year EFOPS results. Med Sci Sports Exerc. 2002 Dec;34(12):2115-23. [CrossRef] [PubMed]
- Sahni S, Tucker KL, Kiel DP, Quach L, Casey VA, Hannan MT. Milk and yogurt consumption are linked with higher bone mineral density but not with hip fracture: the Framingham Offspring Study. Arch Osteoporos. 2013;8(0):119. Epub 2013 Feb 1. Erratum in: Arch Osteoporos. 2013 Dec;8(1-2):132. [CrossRef] [PubMed]
- Jackson RD, LaCroix AZ, Gass M, Wallace RB, Robbins J, Lewis CE, Bassford T, Beresford SA, Black HR, Blanchette P, Bonds DE, Brunner RL, Brzyski RG, Caan B, Cauley JA, Chlebowski RT, Cummings SR, Granek I, Hays J, Heiss G, Hendrix SL, Howard BV, Hsia J, Hubbell FA, Johnson KC, Judd H, Kotchen JM, Kuller LH, Langer RD, Lasser NL, Limacher MC, Ludlam S, Manson JE, Margolis KL, McGowan J, Ockene JK, O'Sullivan MJ, Phillips L, Prentice RL, Sarto GE, Stefanick ML, Van Horn L, Wactawski-Wende J, Whitlock E, Anderson GL, Assaf AR, Barad D; Women's Health Initiative Investigators. Calcium plus vitamin D supplementation and the risk of fractures. N Engl J Med. 2006 Feb 16;354(7):669-83. Erratum in: N Engl J Med. 2006 Mar 9;354(10):1102. [CrossRef] [PubMed]
- Filip, R.; Possemiers, S.; Heyerick, A.; Pinheiro, I.; Raszewski, G.; Davicco, M.J.; Coxam, V. Twelve-Month consumption of a polyphenol extract from olive (OLEA EUROPAEA) in a double blind, randomized trial increases serum total osteocalcin levels and improves serum lipid profiles in postmenopausal women with osteopenia. J Nutr Health Aging, 2015; Volume 19, Number 1, (1):77-86.
- Kim YA, Kim KM, Lim S, Choi SH, Moon JH, Kim JH, Kim SW, Jang HC, Shin CS. Favorable effect of dietary vitamin C on bone mineral density in postmenopausal women (KNHANES IV, 2009): discrepancies regarding skeletal sites, age, and vitamin D status. Osteoporos Int. 2015 Sep;26(9):2329-37. Epub 2015 Apr 24. [CrossRef] [PubMed]
- . Bolland M, Barber P, Doughty R, Mason B, Horne A, Ames R, et al. Vascular events in healthy older women receiving calcium supplementation: randomised controlled trial. BMJ (Clin Res Ed) 2008;336(7638):262e6. [CrossRef]
- Kim, M.H.; Lee, H.J.; Osteoporosis, vitamin C intake, and physical activity in Korean adults aged 50 years and over. J Phys Ther Sci 2016, 28, 725–730. [CrossRef]
- Yahagi K, Davis HR, Arbustini E, Virmani R. Sex differences in coronary artery disease: pathological observations. Atherosclerosis. 2015 Mar;239(1):260-7. Epub 2015 Jan 20. [CrossRef] [PubMed]
- Morvaridzadeh, M.; Agah S, Alibakhshi P, Heydari H, Hoseini AS, Palmowski A, Toupchian O, Abdollahi S, Rezamand G, Heshmati J.; Effects of Calcium and Vitamin D Co-supplementation on the Lipid Profile: A Systematic Review and Meta-analysis. Clin Ther. 2021, 43(9), 274-296. Epub 2021 Aug 27. [CrossRef] [PubMed]
- Kim, K. C., Shin, D. H., Lee, S. Y., Im, J. A., Lee, D. C., & Lee, H. R. (2012). Relationship between serum total cholesterol level and osteoporotic status in elderly Korean men and women. The Korean Journal of Internal Medicine, 27(2), 176-182.
- Skenderidis, P.; Kerasioti, E.; Karkanta, E.; Stagos, D.; Kouretas, D.; Petrotos, K.; Hadjichristodoulou, C.; Tsakalof, A. Assessmentof the antioxidant and antimutagenic activity of extracts from goji berry of Greek cultivation. Toxicol. Rep., 2018; 5, 251–257.
- Ulewicz-Magulska, B.; Wesolowski, M. Total Phenolic Contents and Antioxidant Potential of Herbs Used for Medical and Culinary Purposes. Plant Foods Hum. Nutr., 2018; 74, 61–67.
- Konstantinidi, M.; Koutelidakis, A.E. Functional foods and bioactive compounds: A review of its possible role on weight management and obesity’s metabolic consequences. Medicines, 2019; 6, 94. [CrossRef]
- Annunziata, A.; Mariani, A. Do consumers care about nutrition and health claims? Some evidence from Italy. Nutrients, 2019; 11, 2735. [CrossRef]
- Stanghelle B, Bentzen H, Giangregorio L, Pripp AH, Skelton DA, Bergland A. Effects of a resistance and balance exercise programme on physical fitness, health-related quality of life and fear of falling in older women with osteoporosis and vertebral fracture: a randomized controlled trial. Osteoporos Int. 2020 Jun;31(6):1069-1078. Epub 2020 Jan 10. Erratum in: Osteoporos Int. 2020 Apr 27. [CrossRef] [PubMed]
- Gibbs JC, MacIntyre NJ, Ponzano M, Templeton JA, Thabane L, Papaioannou A, Giangregorio LM (2019) Exercise for improving outcomes after osteoporotic vertebral fracture. Cochrane Database Syst Rev 7:Cd008618.
- Filipović TN, Lazović MP, Backović AN, Filipović AN, Ignjatović AM, Dimitrijević SS, et al. A 12-week exercise program improves functional status in postmenopausal osteoporotic women: randomized controlled study. Eur J Phys Rehabil Med 2021;57:120-30. [CrossRef]
Figure 1.
Flow diagram of the study.
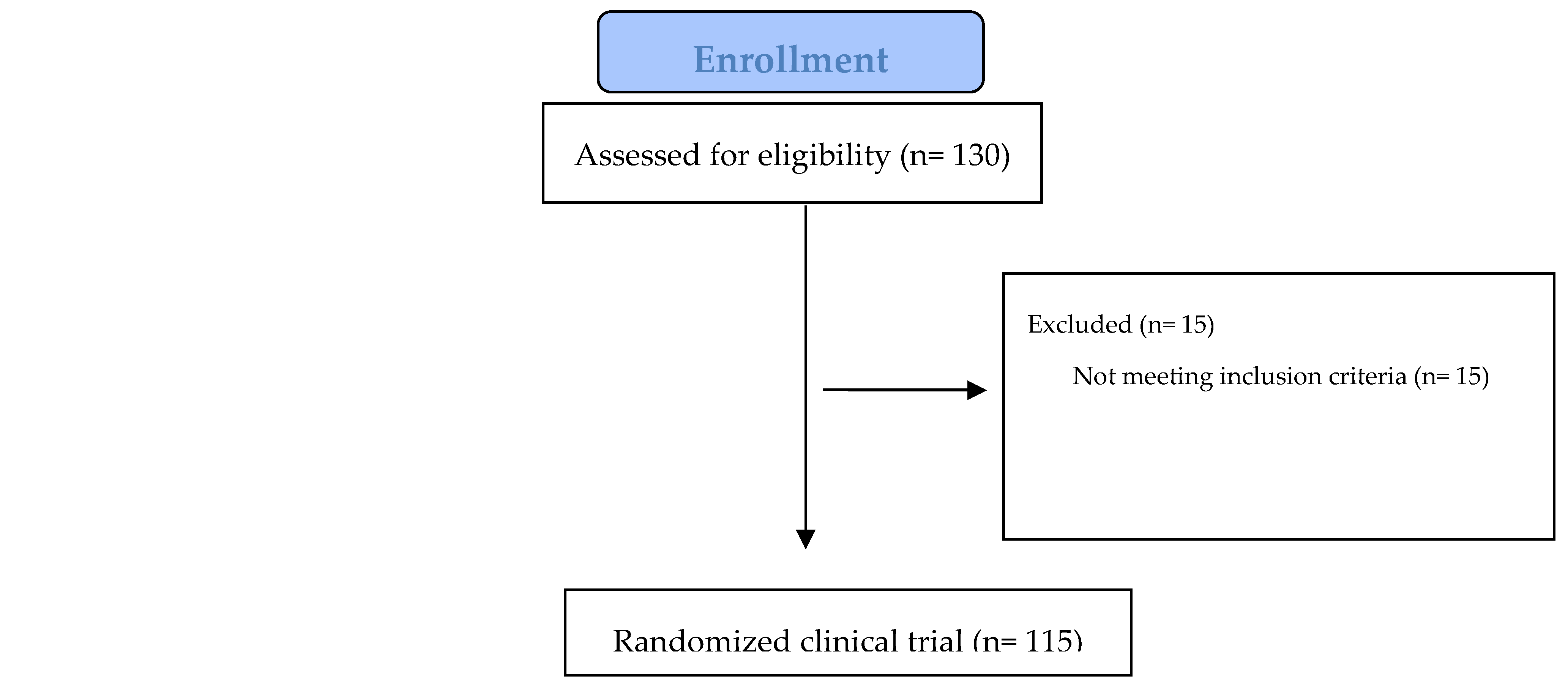
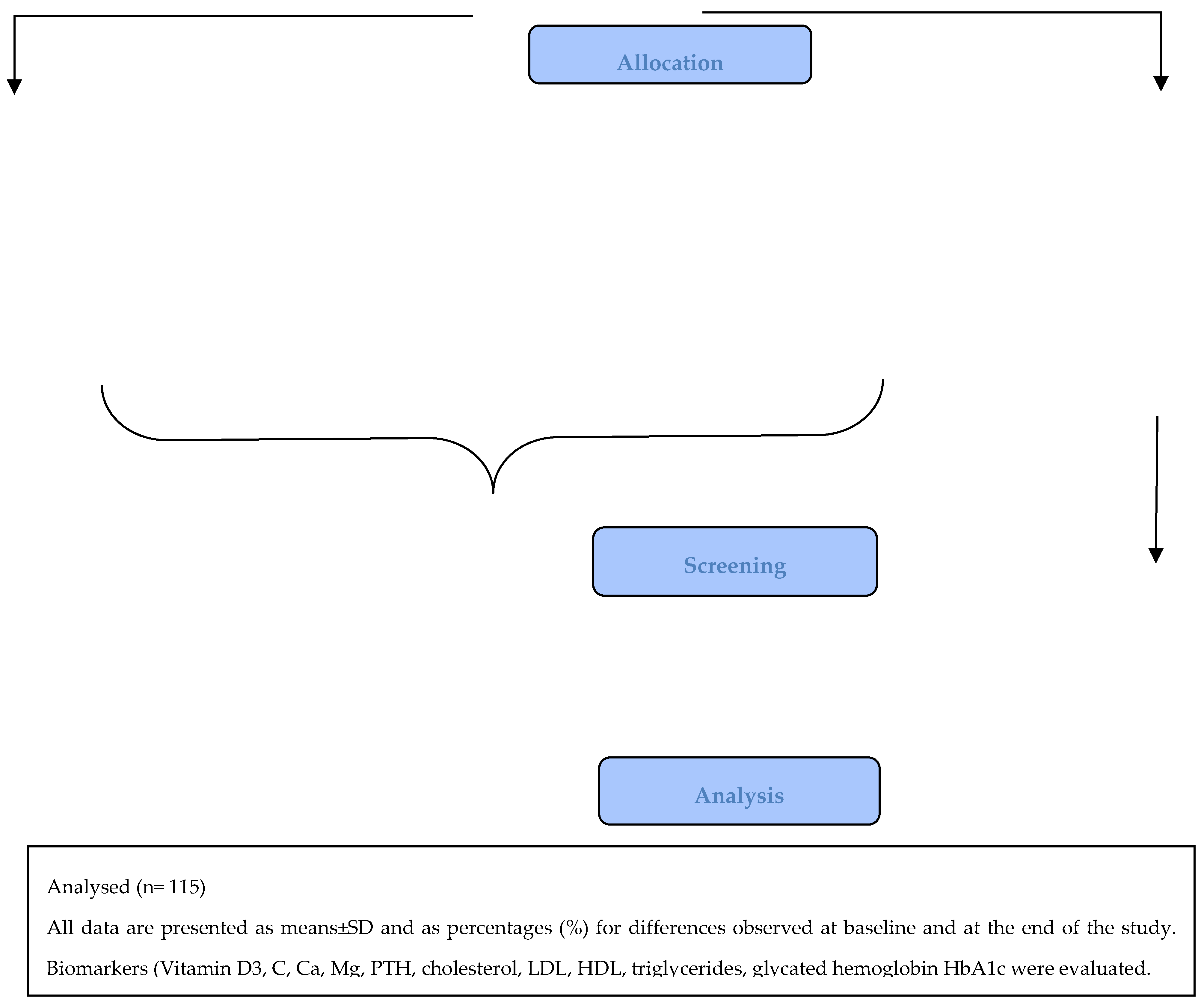
Table 2.
Participants characteristics at baseline.
| Characteristics | Group I (n=40) | Group II (n=42) | Group III (n=18) | Group IV (n=15) | P-value |
|---|---|---|---|---|---|
| Age (years) | 45 ± 8 | 56 ± 8 | 56 ± 8 | 45 ± 7 | 0.839 |
| Height (cm) | 154 ± 36 | 162 ± 9 | 159 ± 6.5 | 162 ± 8.4 | 0.39 |
| Weight (kg) | 74 ± 15.4 | 76 ± 17.4 | 73 ± 13 | 69 ± 10 | 0.628 |
| BMI (kg/m2) | 28.34 ± 5.95 | 29.11 ± 6.45 | 28.79 ± 3.86 | 26.7 ± 0.82 | 0.385 |
| BMI overweight category (kg/m2) | 28.34 ± 5.95 | 29.11 ± 6.45 | 28.79 ± 3.86 | 26.7 ± 0.82 | 0.385 |
| Body fat (Kg) | 36.23 ± 10.87 | 35.91 ± 8.2 | 39.17 ± 13.32 | 35.0 ± 10.74 | 0.61 |
| Muscle mass (Kg) | 44.88 ± 7.22 | 44.21 ± 8.05 | 43.16 ± 6.40 | 43.17 ± 7.01 | 0.4 |
| Total body water (Kg) | 47.01 ± 5.48 | 44 ± 6.13 | 44.86 ± 5 | 44.84 ± 5.20 | 0.25 |
Values presented at baseline and at the end of the study are presented as means±SD. *Level of significance for differences observed within the same group, between the two measurements.
Table 3.
Changes in the levels of bone health indicators.
| Beginning of study | End of study | % change | P-value* | |
|---|---|---|---|---|
| 25(OH)D3 (ng/ml) | ||||
| Group I | 27.42 ± 12.12 | 26.48 ± 7.96 | - 3.43 % | 0.2 |
| Group II | 23.15 ± 8.37 | 24.01 ± 8.68 | 3.71 % | 0.2 |
| Group III | 28.21 ± 8.84 | 28.62 ± 7.78 | 1.45 % | 0.2 |
| Group IV | 26.69 ± 6.83 | 28.19 ± 6.44 | 5.62 % | 0.81 |
| PTH (pg/ml) | ||||
| Group I | 62.63 ± 27.00 | 76.44 ± 36.45 | 22.05 % | 0.77 |
| Group II | 58.95 ± 23.96 | 56.71 ± 23.85 | - 3.80 % | 0.77 |
| Group III | 69.01 ± 17.82 | 52.21 ± 17.87 | - 24.34 % | 0.77 |
| Group IV | 48.84 ± 19.49 | 55.6 ± 19.63 | 13.84 % | 0.11 |
Table 4.
Changes in Total Cholesterol, Glucose and HbA1c.
| Beginning of study | End of study | % change | P-value* | |
|---|---|---|---|---|
| Total cholesterol (mg/dl) | ||||
| Group I | 210.82 ± 30.17 | 207 ± 29.32 | - 1.81 % | 0.54 |
| Group II | 200.1 ± 33.14 | 197.85 ± 36.96 | - 1.12 % | 0.54 |
| Group III | 192.89 ± 29.46 | 197.17 ± 13.72 | 2.22 % | 0.034 |
| Group IV | 185.14 ± 34.17 | 181.31 ± 32.21 | - 2.07 % | 0.034 |
| P-value† | 0 | 0 | -0.70% | 0.39 |
| Glucose (mg/dl) | ||||
| Group I | 91.82 ± 8.93 | 93.33 ± 4.62 | 1.64 % | 0.37 |
| Group II | 96.15 ± 15.27 | 99.56 ± 17.68 | 3.55 % | 0.37 |
| Group III | 108 ± 16.97 | 109.5 ± 14.85 | 1.40 % | 0.37 |
| Group IV | 93.81 ± 8.98 | 96 ± 11.74 | 2.33 % | 0.048 |
| P-value† | 0.136 | 0.29 | 2.23 % | 0.29 |
| HbA1c (%) | ||||
| Group I | 5.64 ± 0.39 | 5.77 ± 0.42 | 2.30 % | 0.27 |
| Group II | 5.74 ± 0.53 | 5.72 ± 0.55 | - 0.35 % | 0.27 |
| Group III | 5.71 ± 0.67 | 5.76 ± 0.8 | 0.88 % | 0.27 |
| Group IV | 5.76 ± 0.81 | 5.85 ± 0.83 | 1.56 % | 0.027 |
Values presented at baseline and at the end of the study are presented as means±SD. *Level of significance for differences observed within the same group, between the two measurements.
Table 5.
Changes in whole-body BMD.
| Beginning of study | End of study | % change | P-value* | |
|---|---|---|---|---|
| Whole-body BMD (g/cm2) | ||||
| Group I | 1.38 ± 0.49 | 1.85 ± 0.5 | 3.46 % | 0.027 |
| Group II | 1.29 ± 0.45 | 1.31 ± 0.47 | 1.55 % | 0.036 |
| Group III | 1.39 ± 0.5 | 1.56 ± 0.51 | 12.23 % | 0.043 |
| Group IV | 1.67 ± 0.48 | 1.87 ± 0.35 | 11.98 % | 0.003 |
| P-value | 0.298 | 0.187 | 14.96 % | 0.027 |
Values presented at baseline and at the end of the study are presented as means±SD. *Level of significance for differences observed within the same group, between the two measurements.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



