
Submitted:
26 April 2024
Posted:
28 April 2024
You are already at the latest version
Abstract
Triple-negative breast cancer (TNBC), lacking specific receptors found in other breast cancer subtypes, poses significant treatment challenges due to limited therapeutic options. Therefore, it is necessary to develop novel treatment approaches for TNBC. In the last few decades, many attempts have been reported for alternative tools for TNBC treatment: immunotherapy, radiotherapy, targeted therapy, combination therapy, and nanotechnology-based therapy. Among them, combination therapy and nanotechnology-based therapy show the most promise for TNBC treatment. This review outlines recent advancements in these areas, highlighting the efficacy of combination therapy (immunotherapy paired with chemotherapy, targeted therapy, or radiotherapy) in both preclinical and clinical stages and nanotechnology-based therapies utilizing various nanoparticles loaded with anticancer agents, nucleic acids, immunotherapeutics, or CRISPRs in preclinical stages for TNBC treatment.
Keywords:
TNBC
; combinatorial therapy
; nanotechnology
; immunotherapy
; chemotherapy
1. Introduction
Based on the Global Cancer Observatory reported in 2018, two million cases of breast cancers have been diagnosed worldwide [1,2]. Several subtypes of breast cancers, including estrogen receptor (ER) positive, progesterone receptor (PR) positive, human epidermal growth factor 2 receptor positive (HER-2), and triple-negative breast cancer (TNBC) are known [3,4]. The TNBC is a heterogeneous group of tumors lacking ER, PR, and HER-2. The TNBC is found in 10-20% of all invasive breast cancers, and a majority of them are linked with African-Americans, younger age, higher grade and mitotic index, and more advanced stage at diagnosis [5]. Due to the absence of major targetable receptors, chemotherapy is the only preferred approach for systemic treatment of TNBC to enhance disease outcomes. The survival rate post-metastasis is shorter in comparison with other breast cancer subtypes. Due to these difficulties, the TNBC has limited treatment options and a poor response rate. Molecularly, there are seven subtypes of TNBC including basal-like subtypes (BL1 and BL2), mesenchymal (M), mesenchymal stem-like (MSL), immunomodulatory (IM), unstable (UNS), and luminal androgen receptor (LAR) [6].
Many methods exist for early diagnosis of TNBC: palpation, mammography, ultrasonography, ultrasound, magnetic resonance imaging (MRI), and immunohistochemistry (IHC) [7]. In daily medical practice, breast cancer diagnosis relies on three different types of analysis: (A) clinical examination; (B) radiological/image examination (that includes mammography, magnetic resonance imaging (MRI) ultrasonography, etc.), and (C) immunohistopathological examinations [4].
TNBC patients are treated with various therapies, depending on the type and stage of cancer. Some of these therapies include chemotherapy, immunotherapy, radiotherapy, stem cell therapy, laser treatment, hyperthermia, surgery, and photodynamic therapy [4,8]. Out of these, chemotherapy is the most common. Our group has recently published a review article that described TNBC and its treatment approaches in more detail [9]. Clinically available treatment options of TNBC are anthracyclines (e.g., doxorubicin) and taxanes (e.g., paclitaxel and docetaxel) in the neoadjuvant chemotherapy (NACT) or the adjuvant setting, immune checkpoint inhibitors (e.g. Aterolizumab and Pembrolizumab), vascular endothelial growth factor (VEGF–targeted therapy (Bevacizumab), mammalian target of rapamycin (mTOR) inhibitor (Ipatasertib and Everolimus), and antibody-drug conjugate (Sacituzumab- govitecan) [9]. However, these treatment options are insufficient to efficiently prolong patients’ lives since this disease is heterogeneous and associated with many variables. Therefore, alternative therapies are required to treat this aggressive disease. Advanced therapies such as combination therapy (immunotherapy with other therapies) and nanotechnology-based therapy could be potentially effective options in the future treatment of TNBC.
Combination therapy involves utilizing multiple treatment modalities to treat cancer effectively [10]. With the advancements in molecular biology, the combined use of therapeutic agents has become increasingly prevalent. The selection of these therapeutics varies depending on the type of cancer. Specifically, in the context of TNBC, extensive research has focused on combining immunotherapeutics with other agents due to the significant study of programmed death ligand-1 (PD-L1) expression on TNBC cells [11]. Recently, the FDA has granted approval for the use of pembrolizumab (an anti-PD-1 antibody) together with chemotherapy. This approval applies to patients dealing with locally recurrent unresectable or metastatic TNBC, specifically for those whose tumors exhibit PD-L1 expression, as well as for high-risk, early-stage TNBC [11,12]. Numerous preclinical and clinical stage investigations have been conducted, exploring the use of immunotherapeutics together with various other anticancer agents [13].
Over the past few decades, nanotechnology has garnered significant interest among experts in the fields of medical science and engineering due to its minuscule structure and distinctive characteristics, offering potential solutions to certain challenges encountered in medicine [14,15].
Within the realm of drug delivery, varied and diverse types of nanoparticles have been investigated for transporting therapeutics to specific areas in the body where diseased tissues, such as tumors, are located. Moreover, owing to the heterogeneity and distinct characteristics of tumor tissues and their microenvironments—such as leaky vasculature, expression of diverse receptors, and acidity—functionalized nanoparticles hold the potential to effectively target and deliver therapeutics to these locations [16]. Nanoparticles exhibit two distinct modes of targeting cancer: passive targeting, relying on the enhanced permeability and retention (EPR) effect, and active targeting, leveraging receptors that are overexpressed on cancer cell [17] and other features present inside cancer cells such as enzymes and acidic pH.
In this article, we will review recent research on the combination of immunotherapy with other therapies and nanotechnology-based therapies of TNBC in vitro and in vivo as well as clinical trials.
2. Combination of Immunotherapy with Other Therapies
As previously stated, due to the heterogeneous nature of TNBC and its deficiency in receptors, relying on a single treatment option is nearly impractical. Consequently, numerous studies have concentrated on combining existing therapies with novel approaches to address the challenges presented by TNBC (refer to Table 1). Notably, the most prevalent combinations involve immunotherapeutics paired with other anticancer agents (Figure 1).
2.1. Immunotherapy
Immunotherapy (IMT) represents a category of cancer treatment methods that utilize naturally occurring substances present in the human body or synthesized in the laboratory. These substances are employed to enhance the immune system, enabling the body to identify and destroy cancer cells. IMT has demonstrated encouraging outcomes in the treatment of TNB [11,18]. The most well-known immunotherapeutic agents are immune checkpoint inhibitors (ICIs), which block immunosuppressive receptors, for instance, cytotoxic T lymphocyte antigen-4 (CTLA-4) and programmed death-1 (PD-1), to improve the cytotoxicity and proliferative capacity of tumor-infiltrating lymphocytes (TILs). ICIs, including monoclonal antibodies against PD-1 (i.e., pembrolizumab, nivolumab), PD-L1 (i.e., atezolizumab, durvalumab, avelumab), and CTLA-4 (i.e., ipilimumab), have produced durable responses across many tumor types [18]. Numerous studies indicate that TNBC exhibits heightened sensitivity to immunotherapy as a result of its distinct characteristics in comparison to other subtypes of breast cancer [4,11]. First, TNBC exhibits an increased presence of TILs, serving as a crucial factor in responding to ICIs and correlating with improved prognosis in early-stage TNBC. Second, elevated PD-L1 expression on both tumor and immune cells in TNBC provides direct targets for ICIs, potentially influencing responses to anti-PD-1 therapies observed in other cancers. Third, TNBC is characterized by numerous nonsynonymous mutations (missense mutation: a mutation that changes an amino acid in a protein; it is also called a nonsynonymous mutation), generating tumor-specific neoantigens that activate neoantigen-specific T cells, potentially enhancing antitumor immune response, particularly when supported by ICIs [18]. Many comprehensive reviews have been reported for immunotherapy in TNBC [11,18,19].
2.2. Preclinical Stage Combination Immunotherapy
Cell therapy, especially chimeric antigen receptor (CAR)-T cell therapy, is one potential treatment option for various cancers including TNBC. Researchers have reported several studies using CAR-T cells with other therapeutic approaches against TNBC. For instance, Liu et al. carried out a study using monoclonal antibody (mAb) 2D2 and T cell receptor (TCR)-like (CAR)T cell therapy against TNBC. The generated mAb 2D2 specifically bound to New York Esophageal Squamous Cell Carcinoma-1 (NY-ESO- 1)157-165 in the context of human leukocyte antigen HLA-A* 02:01 but not to non-A2 or NY-ESO- 1 negative cells. NY-ESO-1 is one of the best immunogenic cancer antigens for immunotherapy in solid tumors [20,21]. The results showed that 2D2 CAR-T Cells were able to inhibit tumor growth in TNBC tumor-bearing mice [22]. Stuber et al. presented a combination study of receptor-tyrosine-kinase-like orphan receptor 1 (ROR1)-CAR T-cells with transforming growth factor β (TGF-β)-receptor signaling inhibitor SD-208 in TNBC. The study results showed that the presence of TGF- β in ROR1-CART cells with TNBC cell culture impaired the cytolytic activity, cytokine production, and proliferation of ROR1-CAR T-cells and its viability. When the specific kinase inhibitor SD-208 was used to protect CD8+ and CD4+ ROR1-CAR T-cells from the inhibitory effect of TGF-β, their antitumor function in vitro and in the microphysiologic 3D tumor model was found constant [23].
Combinations of radiolabeling or radiotherapy with other therapeutics in TNBC have been reported. McKnight et al. reported a combination therapy of radiolabeled antibody and cytotoxic inhibitor (dasatinib) in TNBC (MDA-MB-468) and patient-derived xenograft (PDX) tumors. The results of the combination treatment of cetuximab (epidermal growth factor receptor (EGFR) antibody) and dasatinib (tyrosine kinase inhibitor) showed better tumor regression compared to control and dasatinib-only-treated groups. No improvement was observed in MDA-MB-231 xenografts with the addition of cetuximab, likely due to its Kirsten rat sarcoma (KRAS)-mutated status. The authors concluded that cetuximab-PET can be used to examine the effects of dasatinib on EGFR cellular distribution and the expression of treatment response in wild-type KRAS TNBC [24]. Gregor et al. carried out a study using radiation therapy (RT) and ad libitum (AL) diet, and caloric restriction (CR) using in vivo TNBC model. The results demonstrated an immune suppressive environment with a significant increase in CD4+CD25+Foxp3+ Tregs after RT but not in CR mice. CD8:Treg ratio in CR+RT tumor infiltrating lymphocytes (TIL) was enhanced 4-fold compared with AL+RT mice. The results revealed that combining CR with RT decreases intratumoral Tregs, increases CD8:Treg and increases PD-1 expression via a process dependent on CD8 T-cells in a TNBC model [25].
Combination studies of chemotherapeutics with immunotherapeutics (ICIs, TKIs, and cellular therapeutics) in TNBC have been widely reported. For example, Singh S et al., reported immunostimulatory effect using low-dose cyclophosphamide coupled with the pharmacologic inhibition of tumor associated macrophages (TAMs) using either a small molecule colony stimulating factor 1 receptor (CSF1R) inhibitor or an anti-CSF1R antibody in preclinical syngeneic p53 null mouse models of TNBC. The TILs including helper T cells and antigen-presenting B cells that were enhanced in responders to combination therapy were analyzed by single cell RNA sequencing. The results revealed that the therapeutic combination was effective in treating several highly aggressive TNBC murine mammary tumor and lung metastasis models.[26] Lee et al. reported a combination therapy of Macitentan and anti-PD-L1 antibody against TNBC, colon and lung metastatic cancers. The results of the combination therapy revealed significant improvement for antitumor efficacy that was the result of increasing CD8+ T cell number and activity with decreasing Treg number in the tumors and draining lymph nodes in TNBC, colon, and lung syngeneic tumor models [27]. Zanker et al. evaluated the local and systemic impact of the intratumoral Toll-like receptor (TLR) 7/8 agonist 3M-052 alone or in combination with anti-PD-1 in metastatic TNBC models. The results showed that single intratumoral administration of 3M-052 reduced mammary tumor growth, induced a T-cell-inflamed tumor microenvironment (TME) and reduced metastatic spread to lung. Metastasis suppression was dependent on Interferon (IFN) signaling and an antitumor immune response, in contrast to primary tumor growth inhibition, which was retained in NOD scid gamma (NSG) and CD8+ T-cell-depleted mice. 3M-052 action was demonstrated via dendritic cell activation and production of type I IFN and other pro-inflammatory cytokines to initiate a T-cell inflamed TME and promote tumor cell antigen presentation [28]. Tentler JJ et al. reported the combination treatment of novel anticancer agent RX-5902 and CTLA-4 or PD-1 inhibitor antibodies in TNBC. The data revealed that the combination of RX-5902 and CTLA-4 or PD-1 inhibitors resulted in reduced tumor growth in the 4 T1 and human immune system and MDA-MB-231 xenograft models. RX-5902 treatment increased the number of activated T cells in tumor infiltrating lymphocytes (TILs) in comparison to vehicle. Also, RX-5902/nivolumab combination significantly enhanced CD4+ T cells in TILs and systemic granzyme B production. The authors concluded that RX-5902 improved the efficacy of nivolumab in a humanized, preclinical model of TNBC [29]. Tiara et al. carried out a combination treatment of immunotherapy and chemotherapy (Paclitaxel (PTX)) with positron emission tomography (PET) in TNBC to monitor therapeutic potential of the combinatorial therapy. The authors used anticancer drug PTX and anti-PD-1 or anti CTL4 antibody as immunotherapeutic agent against TNBC model. PET imaging during the combination therapy revealed that PTX improved immune response making it a better environment for IMT [30].
He et al., reported the combination treatment of AEE788 (receptor tyrosine kinases inhibitor) and rapalog (mTOR inhibitors) in TNBC. The results showed that the combination treatment effectively inhibits phosphorylation of mTOR and 4EBP1, relieves mTOR inhibition-mediated upregulation of cyclin D1, and maintains suppression of AKT and ERK signaling, thereby sensitizing TNBC cells to the rapalogs. siRNA validation of cheminformatics-based predicted AEE788 targets has further revealed the mTOR interactive RPS6K members (RPS6KA3, RPS6KA6, RPS6KB1, and RPS6KL1) as synthetic lethal targets for rapalog combination treatment. The authors concluded that their results provided a potential multi-kinase inhibitor combinatorial strategy to overcome mTOR-targeted therapy resistance in TNBC cells since mTOR signaling is highly activated in TNBC tumors.[31]
2.3. Clinical Stage Combination Immunotherapy
Several combinatorial studies using various antibodies (ICIs) along with other therapeutics (mostly chemotherapeutics) have been under clinical trials. For instance, Pembrolizumab (anti PD-1 antibody), Atezolizumab (anti PD-L1 antibody), Camrelizumab (anti-PD-1 antibody), and Durvalumab (PD-L1 antibody) have been applied in clinical trials as a combination with anticancer agents.
2.3.1. Pembrolizumab (Anti PD-1 Antibody) Combination
Ho et al. reported a phase II clinical trial combination of pembrolizumab (anti PD-1 antibody) with radiotherapy in seventeen patients with median age of 52 years old with TNBC. The results showed that the combination therapy had a similar response with pembrolizumab monotherapy in patients with PD-L1 positive mTNBC. In some cases, this combination therapy could be more effective than pembrolizumab alone in the treatment of patients with mTNB [32]. Schneeweiss et al. performed phase Ib clinical trial of pembrolizumab with capecitabine (a chemotherapy agent) or PTX (a chemotherapy agent) in 29 patients with TNBC. The trial resulted in longitudinal immunological profiling of the effect of the combination therapy. The patients with mTNBC showed depletion of T-cells subsets and reduced T-cell clonal richness compared with untreated early-stage breast cancer (ESBC) patient [33]. Anders et al. ran a Phase II clinical study in forty patients with pretreated mTNBC using combination of pembrolizumab and cyclophosphamide (Cy, anti-neoplastic agent). The authors first administered Cy intravenously (300 mg/ml) and after one day pembolizumab (200 mg) was given intravenously. The data showed that low-dose Cy was not effective in depleting Tregs prior to anti-PD1 therapy. They found that Clinical Benefit Rate (CBR) was most associated with the expression of B cell signatures in pretreatment tumor specimens. Similar with previous preclinical studies, the results revealed that the B cell response could play important role in the immune response to ICI therapy in patients with mTNBC [34]. Criscitiello et al. performed a phase I clinical trial using a combination of targeted chemotherapy (PI3K/AKT/ mTOR inhibitor) and immunotherapy (PD1/PD-L1 inhibitor) in one hundred fifty one patients with metastatic breast cancer including seventy of hormone receptor positive (HR+), eighteen of HER2 and sixty three of TNBC. The authors found that the patients with TNBC have low outcomes [35].
2.3.2. Atezolizumab (Anti PD-L1 Antibody) Combination
Iwata et al. carried out Phase III IM passion 130 clinical trial in 902 patients with TNBC using atezolizumab (anti PD-L1 antibody) combined with nab-paclitaxel (chemotherapy agent). The trial results showed prolonged progression-free survival (PFS) in both the intention-to- treat (ITT) population and programmed death –ligand 1 (PD-L1)-positive subgroup compared to placebo plus nab-Paclitaxel. The efficacy of combination of immunotherapy and chemotherapy agents in Japanese patients with TNBC was consistent with the overall IM passion 130 population [36]. Hecht et al. presented results of Phase Ib study of combination talimogene laherparevec with atezolizumab in eleven patients with mTNBC and twenty five patients with metastatic colorectal cancer (mCRC). The trial’s results confirmed that the safety profile for intralesional T-VEC and atezolizumab fits with the expected safety profile, including the risks of intrahepatic injection, with very limited evidence of antitumor activity in patients with liver metastases associated with TNBC or CRC [37].
2.3.3. Camrelizumab (Anti-PD-1 Antibody) Combination
Liu et al. conducted an open label Phase II clinical trial of combinational treatment of check point blockade (camrelizumab) and antiagiogenesis (apatinib) for forty patients with TNBC. The objective response rate (ORR) of this combinational therapy was much higher than previously reported ORR by anti-PD-1/ PD-L1 antibody or apatinib monotherapy. Also, the combination of two agents exhibited favorable therapeutic effects and a manageable safety profile in patients with advanced TNBC [38]. In another study, Liu et al. carried out a multicenter Phase II clinical trial of camrelizumab (anti-PD-1 antibody) combined with Apatinib and Eribulin (antineoplastic) in forty six pretreated patients with advanced TNBC. The combinatorial therapy trial showed promising efficacy with a measurable safety profile in patients with heavily pretreated advanced TNBC. The ORR of the trial was 37% (17/46, 95% CI 23.2-52.5). The authors mentioned that the favorable ORR and progression-free survival (PFS) were associated with lower tumor PML or PLOD3 expression in the patients [39]. Zhang et al. performed a phase Ib clinical trial of camrelizumab in combination with apatinib and furuloparib in 32 patients with recurrent or metastatic TNBC. The result revealed no dose-limiting toxicity, 62.1% (95% CI, 42.3-79.3) of the disease control rate (DCR), 52 months (95% CI, 3.6- 7.3) of the median PSF, and 64.2% (95% CI, 19-88.8) of 12-month overall survival rate, respectively. Overall results demonstrated that the combination of camrelizumab with apatinib and furuloparib inhibitors showed manageable safety profile in patients with recurrent or metastatic TNBC. Also, the data exhibited low ORR and promising DCR and PFS [40].
Wu et al. performed Future –C Plus Phase 2 clinical trial of camrelizumab (anti PD-1 mAb) with famitinib (an angiogenesis inhibitor) and chemotherapy in forty eight advanced immunomodulatory TNBC patients. The results showed 81.3% (95% CI, 70.2- 92.2) of the ORR and 13.6 months (95% CI, 8.4-18.8) of the median PFS. Also, data revealed that patients with CD8- or PD-L1 positive tumors benefit more from this regimen [41].
2.3.4. Durvalumab (PD-L1 Antibody) Combination
Foldi et al. performed a Phase I/II clinical trial of durvalumab (PD-L1 antibody) concomitant with neoajuvant chemotherapy in sixty-seven patients with an early stage TNBC. The authors used nab-paclitaxel, doxorubicin, and cyclophosphamide as neoadjuvant chemotherapy agents. The results showed that 3-year event free survival were 78.3% and 71.4% in non- African American (AA) and AA patients and 3 year overall survival was 87% and 81%, respectively. The authors concluded that this combination therapy has similar improved efficacy in early stage TNBC both in AA and non-AA patients [42]. Pusztai et al. carried out I-SPY2 trial (clinical) in seventy-three patients with stage II/III HER-2 negative BC. The results of I-SPY2 trial showed that combination of durvalumab and olaparib with paclitaxel enhanced pathologic complete response (pCR) rate in HER-2 negative BC, including TNBC and ER-positive cancers. Among the ER positive/ HER2-negative cancers, only the highly proliferative, estrogen receptor low, Mamma Print MP2 subset benefited from the combination therapy [43]. Loibl et al. executed a randomized phase II clinical trial of durvalumab (anti PD-L1 antibody) and an anthracycline taxane-based combination in 174 patients with early TNBC. The research results showed that pathological complete response (pCR) rate with durvalumab was 53.4% (95% CI 42.5% to 61.4%) versus placebo 44.2% (95% CI 33.5% to 55.3%). The significant increase of the pCR rate was observed only in the subgroup of patients who received durvalumab alone 2 weeks before start of chemotherapy [44].
2.3.5. Other Immunotherapeutic Combinations
Li et al. studied Phase II, open-label trial of anti-PD-1 antibody (SHR-1210) in combination with apatinib (VEGFR2 inhibitor) for twelve advanced TNBC patients. The results showed the dose-dependent synergy of anti-angiogenic therapy and anti-PD-1 antibody in preclinical breast cancer models and in patients with advanced TNBC [45]. Chick et al. a multicenter, randomized, single-blind, phase IIb clinical trial in 587 patients using a combination of the HER2-derived peptide vaccine NPs + trastuzumab (anti HER2 antibody) vs granulocyte macrophage colony-stimulating factor (GM-CSF) + trastuzumab. The results showed that the combinatorial treatment has a significant benefit in 36-month disease free survival among patients with TNBC, which was not observed in trastuzumab monotherapy [46]. Mohamed et al. studied Phase II clinical trial in fifty-four patients with TNBC using a combination of bevacizumab (anti VEGF-A antibody) with carboplatin and paclitaxel. The trial’s results exhibited 27 months of median PFS (85% confidence interval (CI), 17.019- 36.981), and median overall survival (95% CI, 38.973 – 71.027) [47].
Goal et al. carried out phase III PRESERVE 2 clinical trial of a combination therapy of trilaciclib (intravenous CDK4/6 inhibitor) with gemcitabine (GCb) and carboplatin for 250 patients with mTNBC. Previous phase II study’s data in patients with TNBC demonstrated that administrating trilaciclib prior to GCb resulted in clinically meaningful improvements in overall survival (OS) compared with GCb alone [48]. Wang et al. ran a phase-I clinical trial of DC-CIKs immunotherapy with specific chemotherapy (Cy, thiotepa, and carboplatin) in twenty- three metastatic anthracyclines and taxanes pretreated TNBC patients. The authors found that the partial response rate was 13%, stable and progressive disease rates were 56.5 and 30.4%, respectively. Also, they explored that the median PFS was 13.5 months (95% CI 10.1 – 16.9 months) and OS was 15.2 months (95% CI, 12.5- 18.1 months). Overall data suggested that the combination therapy was effective and safe for younger mTNBC who were pretreated with anthracyclines and taxanes based adjuvant chemotherapy [49]. Jiang et al. carried out phase bI/II FUTURE clinical trial of combination of immunotherapeutic agents and chemotherapy in seven groups (pyrotinib with capecitabine, androgen receptor inhibitor with CDK4/6 inhibitor, anti PD-1 with nab-paclitaxel, PARP inhibitor included, and anti-VEGFR included, or mTOR inhibitor with nab-paclitaxel) in sixty-nine refractory metastatic TNBC patients. The results exhibited that the ORR was 20 (29.0%, 95% CI 18.7-41.2%) in the patients. Overall, the clinical trial, the FUTURE, revealed that combinatorial therapy of molecular subtyping with targeted sequencing was a promising treatment option for refractory mTNBCs [50].
3. Nanotechnology-Based Therapies for TNBC
Nanotechnology represents an innovative technology centered around nanoparticles (NPs) characterized by surface charge, small particle size, and structure tailored for precise targeted drug delivery, utilizing a receptor-specific target within cancerous cells.[51] The NPs are crafted from diverse materials like polymers, lipids, proteins, silicon, gold, silver, graphene, and copper. [52] Their fabrication allows for tailoring specific properties based on materials, facilitating ease of targeting sites expressing particular receptors or other stimulants. One of the key advantages of nanoparticles is their ability to carry substantial payloads through encapsulation or incorporation compared to antibody-drug conjugates or polymer-drug conjugates. Table 2 provides an overview of the nanoparticles examined in the treatment of TNBC. Meanwhile, Figure 2 offers a summary visualizing the landscape of nanoparticles in TNBC.
3.1. Polymer-Based Nanoparticles
Polymer-derived nanoparticles have garnered extensive exploration as carrier systems in biomedical applications due to their biocompatibility and lack of toxicity [53]. Moreover, polymers are more cost-efficient when compared to lipids and other materials. Numerous polymer-based nanoparticles, derived from either natural or synthetic polymers, have been documented as carriers for delivering anticancer drugs in the treatment of various cancers, including TNBC [53,54].
Krausz et al. developed doxorubicin (DOX) containing sol-gel polymer nanoparticle formulation and tested against DOX-resistant TNBC cell lines. The sol-gel NP formulation is composed of chitosan, polyethylene glycol (PEG), DOX, and tetramethyl orthosilicate HCl. A cytotoxicity study of the DOX-nano hydrogel was performed in DOX-resistant TNBC cell lines, including SUM149 PT, Hs578T and MDA-MB-157 cell lines. The data showed that the high concentration of DOX-NPs (800 nM) killed more chemoresistant TNBC cells compared with free DOX. However, both groups at a low dose (100 nM) had similar cell-killing activity [55]. Wu et al. developed an indocyanine green (ICG)-loaded glycated chitosan (GC)-based self-assembled nanoparticle (GC@ICG NPs). The authors used GC as a polysaccharide macromolecular immunoadjuvant and ICG as a photoactive agent for combination therapy of phototherapy and immunotherapy. An in vivo study of the GC@ICG NPs showed a strong reduction in tumor growth in the 4T1 tumor-bearing mouse model as well as suppression for lung metastasis, enhancing infiltration of CD8+T cells in distant tumors [56]. Li et al. developed hyaluronic acid (HA)-targeted chitosan nanoparticle loaded with curcumin (CUR). The authors synthesized chitosan (CS)- poly (N-isopropyl acrylamide) that self-assembled to form a nanoparticle due to its amphiphilicity. The CS-NPs were incorporated with CUR and attached HA as a targeting ligand for the CD44 receptor, expressed on the surface of TNBC. The NPs showed better cell-killing effect and high tumor growth suppression activity in the TNBC tumor-bearing mouse model compared with free drug and non-targeted NPs [57].
Sulaiman et al. presented the results of a lipid and poly (lactic-co-glycolic acid) (PLGA) polymer hybrid nanoparticle-based delivery platform co-loading paclitaxel and verteporfin (PV-NP) that was tested against TNBC patient-derived xenograft (PDX) tumor and cancer stem cells (CSCs). The data showed that the dual drug-loaded NPs (lipid- polymer hybrid NPs) significantly inhibited NF-kB, Wnt, and YAP pathways, known to be involved with the growth of TNBC cells, and revealed synergistic effects on killing TNBC bulk tumors and CSCs. The authors performed efficacy studies of NPs in MDA-MB- 231 TNBC cells and HCl- 002 PDX TNBC tumor model in athymic mice [58]. Chen et al. developed PD-L1- targeted CD155 siRNA (siCD155) – loaded mPEG-PLGA-PLL (PEAL) nanoparticles (NPs) to block PD-L1 and CD155 in a spatiotemporal manner based on their finding of PD-L1 and CD155 receptor co-expression in TNBC. The results showed the combinatorial NPs enhanced early-stage CD8+Tcell immune surveillance against 4T1 tumors, but reversed inhibition status of the late-stage CD8+Tcells to prevent 4T1 tumor immune escape [59]. Valcourt et al. carried out research using Notch1- targeted miRNA (miR-34a)-encapsulated PLGA NPs for TNBC treatment. In vitro study exhibited that the targeted miRNA-polymer NPs had the potential to regulate Notch signaling and downstream miR-34a targets in TNBC, resulting in induced senescence, and reduced cell proliferation and cell migration. The authors used the Notch antibody for two purposes: i) targeting to Notch receptor expressed on TNBC and ii) suppressing Notch signaling through signal cascade interference [60]. Valcourt et al. also studied photothermal agent (IR820 dye) -loaded PLGA NPs against TNBC at in vitro and in vivo levels. The results demonstrated that the IR820-PLGA NPs have higher cell-killing activity in the presence of irradiation with 808 nm light against the MDA-MB-231 TNBC cell line, whereas almost no cell killing was observed with treatment without light exposure. In vivo photothermal study revealed that the IR820-PLGA NPs significantly reduced tumor growth in tumor-bearing mice [61]. Further, Valcourt et al. carried out a study using Notch1 antibody-targeted small molecule drug ABT-737 (Bcl2 inhibitor) - loaded PLGA NPs for TNBC treatment. As shown in the previous report, Notch antibody has dual advantages, including TNBC cell-specific binding and suppression of Notch signaling. Overall results showed that Notch1 antibody-targeted ABT-737-loaded PLGA NPs had a strong targeting ability to TNBC, and efficiently regulated Bcl-2 and Notch signaling to induce cell death in vitro, as well as greatly accumulated in tumor tissue and reduced tumor growth, resulting in high survival of murine [62]. Agnello et al. developed EGFR-targeted cisplatin-loaded PLGA polymer NPs and evaluated against an MDA-MB-231 (TNBC) - bearing tumor nude mouse model. The results indicated that cisplatin-loaded aptamer-targeted NPs held much higher cytotoxicity in tumor cells as compared with free drugs, and significantly reduced tumor growth with higher targeting efficiency and without any signs of systemic toxicity in comparison with free drug and untargeted NPs [63].
Bahman et al. studied dasatinib (tyrosine kinases inhibitor)- loaded poly (styrene-co-maleic acid) (SMA) nanoparticles against both the TNBC cell line and tumor model. Their purpose was to protect dasatinib from fast pharmacokinetic degradation and to prolong its activity by encapsulation in the NPs. The in vitro results exhibited similar cytotoxicity for both NPs and free drug against three cell lines, whereas the tumor suppression efficacy of the NPs in 4T1 tumor-bearing Balb/c mice was 7-fold higher than the same concentration of free drug. The authors claimed that the strong in vivo activity rose by the protection of a SMA micelle system of TKI from the enzymatic degradation [64]. Nabil et al. developed CD44-targeted hydrophobic drug (CFM-4.16)-loaded polymeric NPs to improve drug solubility, tumor accumulation, and anticancer efficacy against TNBC at in vitro and in vivo levels. The authors used hyaluronic acid as a targeting ligand, tocopheryl polyethylene glycol succinate (TPGS) and SMA as the main components of NPs, and momelotinib (MMB; a JAK/STAT inhibitor) as a co-payload. The results showed that CD44-targeted dual drug-loaded polymer NPs selectively delivered the payload to CD44 overexpressing TNBC, resulting in reduced cell viability. In vivo imaging study revealed higher tumor accumulation of CD44- T-PNPs in TNBC tumor-bearing mice [65]. El- Deeb et al. developed Taluramycin A-loaded SMA nano micelle (TFA-SMA) with the purpose of reducing side effects of the drug and increasing tumor accumulation. The results revealed that the nanomedicine holds high anticancer efficacy against TNBC. More importantly, the tumor accumulation of TFA increased four times in the case of TFA-SMA nano micelle in comparison with the free drug in 4T1 tumor-bearing mice [66]. Greish et al. reported cannabinoid (WIN55,212-2) and DOX–co–loaded polymeric NPs (SMA-WIN) and analyzed them in the 4T1 tumor-bearing mouse model. The in vitro cytotoxicity of SMA-WIN and free WIN in three cell lines was similar. However, an in vivo antitumor study against tumor-bearing mice revealed that the combination of DOX and SMA-WIN NPs reduced 60% of tumor growth in comparison with the control group, whereas free DOX and SMA- WIN were able to reduce 34% and 42% tumor growth, respectively [67].
Jiao et al studied photo-sensitive prodrug polymer nanoparticles (AIP/CPT-NPs) against TNBC. The results showed that combined drug (photosensitizer Al and camptothecin)-loaded NPs induced potent in vivo phototherapeutic damage by 660 nm light exposure, resulting in metastatic tumor suppression in the TNBC model [68]. Xu et al. reported pH- pH-activated nanoparticles encapsulating POLR2A siRNA (siPOL2) for suppression of POLR2A expression in TNBC. The data showed that siPOL2 polymer NPs inhibit the expression of the POLR2A gene (essential neighboring gene of TP53), reducing tumor models as compared to control groups [69]. Zou et al. developed reactive oxygen species (ROS)- responsive galactosylated NPs (DOX@NPs) to inhibit TNBC. The results revealed that DOX@NPs increased tumor cell apoptosis, accumulated efficiently in tumors and suppressed tumor growth in the 4T1 tumor – bearing mouse model by increasing tumor accumulation due to galactose receptor targeting as compared with the control group [70].
Cui et al. developed mitochondria-targeted copper-depleting nanoparticle (CDN) and evaluated them against TNBC. The CDN consists of a copper-depleting moiety (CDM) and a semiconducting polymer NP (SPN). In vitro study of CDN in TNBC cells presented a reduction in oxygen consumption and oxidative phosphorylation, and a decrease in ATP production, resulting in cell apoptosis. An in vivo study in three tumor models showed that CDN inhibited tumor growth, and substantially improved survival, indicating low systemic toxicity [71].
Babu et al. produced hyaluronic acid-coupled cerum oxide – poly(ethyleneimine nanoparticle (CePEI-NPs) with the purpose of using it as a therapeutic agent in TNBC. In vitro study showed that the HA-CePEI-NPs induced a reduced mitochondrial membrane potential (MMP), which often occurs by generation of reactive oxygen species (ROS) during the treatment process. They confirmed that the NPs killed the TNBC cells by mitochondria-mediated apoptosis mechanism due to the release of cytochrome c [72].
3.2. Lipid-Based Nanoparticles
Lipid-based nanoparticles have undergone extensive research as carriers for delivering therapeutic agents. The initial FDA-approved nanoparticle, Doxil, encapsulates Doxorubicin (DOX) within lipid bilayers [16]. A recent milestone in mRNA (messenger RNA) vaccine advancement is closely associated with lipid nanoparticles (LNPs), as they facilitate mRNA delivery to the intended site without degradation [73]. Eskiller et al. developed talazoparib (PARP inhibitor) - loaded solid lipid nanoparticle (SLN) to avoid talazoparib-resistance in TNBC cells. The in vitro study showed that talaroparib-SLN has a strong suppression effect of MDR1, BCRP, and MRP1 gene and holds a high protein expression level in comparison with free talazoparib, indicating a promising therapeutic carrier to reverse MDR-mediated resistance in TNBC [74]. Moknlis et al. prepared micro RNA (miR-873)-loaded lipid nanoparticle. The authors demonstrated that the miR-873-NPs suppressed KRAS mRNA which is a mutated proto-oncogene in TNBC. Also, an in vivo study showed that delivery of miR-873 NPs reduced tumor growth by inhibiting KRAS expression in PDAC and TNBC xenograft–tumor models [75]. Zhao et al. developed siRNA and albumin-encapsulated exosome nanoparticles (CBSA/siS100A4@Exosome) with the purpose of treating TNBC. The research data revealed that CBSA/siS100A4@Exosome accumulated in the lung as compared with the same drug-loaded liposome and showed a significant inhibition for the growth of tumor cells owing to excellent gene-silencing effect [76]. Guo et al. developed a noncationic, deformable, and tumor-targeted nanolipogel system (tNLG) for CRISPR genome editing in TNBC tumors. The lipogel tNLGs comprise a shell consisting of two types of noncationic lipids and an alginate core containing 3CR1SPR plasmids. The authors demonstrated that tNLGs are a potent CRISPR knockout of lipocalin 2 (Lcn2), which is a breast cancer oncogene, in human TNBC cells in vitro and in vivo. An in vivo study in an orthotopic TNBC tumor model showed that CRISPR knockout of Lcn2 reached > 81% by tNLGs, resulting in significant tumor growth suppression (>77%) [77].
3.3. Inorganic Material-Based Nanoparticle
For the past decade, inorganic nanoparticles have been under scrutiny as a drug carrier system and for their potential as theranostic agents, owing to their minimal toxicity and straightforward preparation [78]. Gold nanoparticles, in particular, have received extensive investigation as both a diagnostic agent and a carrier for drug delivery [51]. Additionally, iron oxide nanoparticles represent one of the FDA-approved nanoparticle varieties [79].
Ramchandani et al. developed microRNA (miR-708) – loaded multi-layered gold nanoparticle for the treatment of mTNBC. The data showed that the miR708-NP directly targeted the SOX2/OCT4-mCherry + miR-708low tumor cells to repair metastasis in vivo and had minimal host toxicity, demonstrating a great potential for reducing TNBC progression in 4T1 breast tumor-bearing Balb/cJ mice [80]. Oli et al. ran a combinatorial treatment using an immune check point inhibitor with magnetic iron oxide (MIO) nanoparticle hyperthermia against a metastatic TNBC tumor model. Research results showed that although the combination of MIO and immune ICIs (anti PD-1 and anti CTLA-4 antibodies) reduced tumor volume in 4T1- luciferase cell-implanted BALB/c mice as compared to the control group, there was no improvement in the overall survival of mice with the treatment. In addition, the data revealed single - fraction application of MION/ hyperthermia (HT) combined with immune checkpoint inhibition has the potential to improve metastatic dissemination to the lungs [81]. Zhang et al. developed a hollow mesoporous iron nanoparticle (HFON) encapsulating DOX that can be used as both a therapeutic agent and Magnetic Resonance Imaging (MIR) diagnostic agent for TNBC. In vitro apoptosis study demonstrated that DOX@HFON induced apoptosis, autophagy, and ferroptosis, resulting in apoptotic cell death in the TNBC cell line. In vivo antitumor study exhibited that MAGNET@DOX@HFON group significantly inhibited tumor growth as well as had a great MIR imaging ability in TNBC tumor tissue. The authors concluded that the combinatorial NPs could be potential theranostic agents in TNBC [82].
Fan et al. developed gamabufotalin and doxorubicin (DOX)-coloaded graphene oxide quantum dots nanoparticles (GTDC NPs). The authors used TAT and RGD peptides as targeting ligand to tumor tissue. Flow cytometer analysis demonstrated that dual drug-loaded NPs induced more than 89% apoptosis in TNBC cells. In vivo study showed that the tumor accumulation of targeted dual drug-loaded GTDC NPs increased 2 times in comparison with naked GTDC NPs, resulting in enhanced antitumor efficacy. Also, the data presented 84% reduction in lung metastasis through the treatment of NPs against TNBC tumor-bearing mice [83].
Zhang et al. developed a biomimetic nanoparticle from leukocyte/ platelet hybrid membrane (LPHM) and dendritic large pore mesoporous silicon nanoparticles (DLMSNs). The NPs were co-loaded with near-infra-red (NIR) fluorescence dye IR780 and a chemotherapeutic agent DOX to use combinatorial therapeutics. An in vitro cytotoxicity study in the presence of laser irradiation exhibited the LPHM@DDI NPs had a synergistic cell-killing efficacy in TNBC cells, which was raised by apoptosis-inducing. The NPs also showed high tumor growth suppression in 4T1 tumor-bearing mice in comparison with control groups [84].
Jiang et al. developed ZrC nanoparticle in conjunction with radiotherapy (RT) and phototherapy (PT) to enhance antitumor and antimetastatic effects in TNBC. To enhance biocompatibility and targeting ability, the authors coated the nanoparticles with a bovine serum albumin (BSA) and attached folic acid to the NPs. The size of NPs was approximately 100 nm. An in vitro immunofluorescence study revealed more DNA damage and more ROS generation in TNBC cells through ZrC NP treatment. Further, in vitro and in vivo studies showed that ZrC NPs with a combination of RT and PT had a strong cell-killing effect and tumor-suppressing activity in the TNBC tumor-bearing mouse model [85].
3.4. Peptide and Protein-Based Nanoparticle
Nanoparticles derived from peptides and proteins have been studied as drug delivery systems of varied and diverse therapeutics due to their biocompatibility and minimal toxicity. An instance of this is Abraxane, an FDA-approved nano-complex composed of albumin and Paclitaxel, applied for the treatment of several cancer types [86].
Egorova et al. developed chemokine receptor 4- targeted peptide–based NPs for combinatorial delivery of siRNAs suppressing major transduction pathways. The results showed that the combinatorial transfection of anti COL4A2 and anti–CDC20 siRNAs NPs revealed 1.5-2 fold inhibition of proliferation and migration of TNBC cells. The authors concluded that CXCR4 ligand-modified L1- polyplexes containing AQP3, CDC20, and COL4A2 siRNAs have a huge combinatorial effect on inhibiting the proliferation of TNBC cells [87].
Yuan et al. carried out a study using Abraxane (paclitaxel-loaded albumin NPs) along with Taxol as a control against TNBC. The in vitro study results showed that both Abraxane and free Taxol had similar cytotoxicity in TNBC cell lines. In the case of the in vivo study, although Abraxane held 3 - 5–fold lower blood drug concentration in comparison with Taxol, they exhibited similar tumor suppression effects in orthotopic breast cancer NOD/SCID mouse model. In contrast, Abraxane reduced breast cancer stem-like cells (CSCs) frequency by 3 to 9 folds, while Taxol enhanced breast CSCs frequency in the tumor model. In addition, the data showed that Abraxane improved 3 to 15 times intracellular uptake in cancer cells as compared to Taxol, indicating Abraxane’s superior efficacy against CSCs to Taxol [88].
Wang et al. developed peptide-drug conjugate (PTX-SM-TAR) comprising PTX and a fused peptide TAR consisting of a tumor-targeting peptide, A7R, and a cell-penetrating peptide, TAT. The PTX-MS-TAR conjugate self-assembled into nanoparticles. The in vitro study of PTX-SM-TAR NPs exhibited higher binding affinity to NRP1 (Neuropilin 1, tumor angiogenesis receptor), great transvascular transport, and tumor penetration ability. In vivo antitumor efficacy study showed that PTX-SM-TAR NPs had a 43.24% of tumor inhibition rate, whereas PTX and TAR groups reveal 28.47% and 7.81% of tumor inhibition rates, respectively, against 4T1 cell-based TNBC tumor model [89].
Liu et al. described cyclic arginyl-glycyl-aspartic acid (cRGD) peptide–targeted human serum albumin (HSA) nanosystem with the purpose to co-deliver albendazole (ABZ) and iodine -131 (131I) for chemoradiotherapy of TNBC. The NPs were prepared by self-assembling HSA in the presence of ABZ and by attaching cRGD and 131I to the surface of the NPs. An in vitro cytotoxicity study exhibited that the NPs had high cell-killing activity and reduced cell migration in MDA-MB-231 and 4T1 cells compared with free drug and non-targeted NPs. In vivo, the targeted and radiolabeled NPs suppressed tumor growth in 4T1 tumor-bearing mice and were able to accumulate in tumor tissue [90].
4. Conclusion
Numerous studies conducted over the past few decades have explored various treatment approaches for Triple-Negative Breast Cancer (TNBC), including chemotherapy, immunotherapy, phototherapy, radiotherapy, and targeted therapy. However, the heterogeneous nature and limited receptor expression of TNBC have rendered monotherapies ineffective. Recent successful clinical trials have focused on combination therapies, such as the combination of immunotherapy (ICIs) with chemotherapy or targeted therapy. Some of these combination therapies have received approval from the US FDA. This review article provides a comprehensive summary of recent efforts in research both in preclinical and clinical stages of combination therapies, encompassing immunotherapy with chemotherapy, immunotherapy with other therapies, chemotherapy with targeted therapy, as well as preclinical nanotechnology-based therapy for TNBC.
Combination therapy encompasses the pairing of immune checkpoint inhibitors (ICIs) with chemotherapeutics, cyclin-dependent kinase inhibitors (CKIs) with chemotherapeutics, targeted therapeutics with chemotherapeutics, and radiotherapeutics with chemotherapeutics. Nanotechnology-based therapy involves the utilization of diverse materials of formulation, including those made of polymers, lipids, inorganic materials, and proteins. These nanoparticles have the capability to transport a range of therapeutic agents, such as anticancer drugs, nucleic acids, small molecule inhibitors, and other biologics. Moving forward, a substantial percentage of cancer treatment options, including TNBC, are anticipated to involve combination therapies. Furthermore, nanotechnology-based therapies are poised to progress into clinical trials and gain approval for applications.
While combination immunotherapies with other therapies have demonstrated promising outcomes, further research is required to explore additional combinations that can extend patients' lives. The integration of AI and drug delivery systems holds promise for developing more potent therapeutic combinations in the future. Specifically, in the context of nanoparticle-based therapies for cancer treatment, increasing the number of clinical stage studies is imperative to enhance the likelihood of reaching the approval stage. This necessitates conducting optimization studies in both academic and industrial settings to refine these therapies and maximize their efficacy.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021, 71, 209. [Google Scholar] [CrossRef] [PubMed]
- Schick, J.; Ritchie, R.P.; Restini, C. Breast Cancer Therapeutics and Biomarkers: Past, Present, and Future Approaches. Breast Cancer (Auckl). 2021, 15, 1178223421995854. [Google Scholar] [CrossRef]
- Kumar, P.; Aggarwal, R. An overview of triple-negative breast cancer. Arch Gynecol Obstet. 2016, 293, 247. [Google Scholar] [CrossRef] [PubMed]
- Medina, M.A.; Oza, G.; Sharma, A.; Arriaga, L.G.; Hernandez Hernandez, J.M.; Rotello, V.M.; Ramirez, J.T. Triple-Negative Breast Cancer: A Review of Conventional and Advanced Therapeutic Strategies. Int J Environ Res Public Health. 2020, 17, 2078. [Google Scholar] [CrossRef]
- Yin, L.; Duan, J.J.; Bian, X.W.; Yu, S.C. Triple-negative breast cancer molecular subtyping and treatment progress. Breast Cancer Res. 2020, 22, 61. [Google Scholar] [CrossRef]
- Berger, E.R.; Park, T.; Saridakis, A.; Golshan, M.; Greenup, R.A.; Ahuja, N. Immunotherapy Treatment for Triple Negative Breast Cancer. Pharmaceuticals (Basel). 2021, 14, 763. [Google Scholar] [CrossRef] [PubMed]
- Thakur, V.; Kutty, R.V. Recent advances in nanotheranostics for triple negative breast cancer treatment. J Exp Clin Cancer Res. 2019, 38, 430. [Google Scholar] [CrossRef]
- Al-Mahmood, S.; Sapiezynski, J.; Garbuzenko, O.B.; Minko, T. Metastatic and triple-negative breast cancer: challenges and treatment options. Drug Deliv Transl Res. 2018, 8, 1483. [Google Scholar] [CrossRef]
- Obidiro, O.; Battogtokh, G.; Akala, E.O. Triple Negative Breast Cancer Treatment Options and Limitations: Future Outlook. Pharmaceutics. 2023, 15, 1796. [Google Scholar] [CrossRef]
- Bhatia, K.; Bhumika, *!!! REPLACE !!!*; Das, A. Combinatorial drug therapy in cancer - New insights. Life Sci. 2020, 258, 118134. [Google Scholar] [CrossRef]
- Emens, L.A. Immunotherapy in Triple-Negative Breast Cancer. Cancer J. 2021, 27, 59. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Kim, K. Theranostics for Triple-Negative Breast Cancer. Diagnostics (Basel). 2023, 13, 272. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Gao, F.; Ahmed, A.; Rafiq, M.; Yu, B.; Cong, H.; Shen, Y. Immunotherapy: cancer immunotherapy and its combination with nanomaterials and other therapies. J Mater Chem B. 2023, 11, 8586. [Google Scholar] [CrossRef] [PubMed]
- Mishra, S. Nanotechnology in medicine. Indian Heart J. 2016, 68, 437. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, M.A.; Fallica, A.N.; Virzi, N.; Kesharwani, P.; Pittala, V.; Greish, K. The Promise of Nanotechnology in Personalized Medicine. J Pers Med. 2022, 12, 673. [Google Scholar] [CrossRef] [PubMed]
- Mosleh-Shirazi, S.; Abbasi, M.; Moaddeli, M.R.; Vaez, A.; Shafiee, M.; Kasaee, S.R.; Amani, A.M.; Hatam, S. Nanotechnology Advances in the Detection and Treatment of Cancer: An Overview. Nanotheranostics. 2022, 6, 400. [Google Scholar] [CrossRef] [PubMed]
- Attia, M.F.; Anton, N.; Wallyn, J.; Omran, Z.; Vandamme, T.F. An overview of active and passive targeting strategies to improve the nanocarriers efficiency to tumour sites. J Pharm Pharmacol. 2019, 71, 1185. [Google Scholar] [CrossRef] [PubMed]
- Keenan, T.E.; Tolaney, S.M. Role of Immunotherapy in Triple-Negative Breast Cancer. J Natl Compr Canc Netw. 2020, 18, 479. [Google Scholar] [CrossRef] [PubMed]
- Emens, L.A. Breast Cancer Immunotherapy: Facts and Hopes. Clin Cancer Res. 2018, 24, 511. [Google Scholar] [CrossRef]
- Zeng, G.; Li, Y.; El-Gamil, M.; Sidney, J.; Sette, A.; Wang, R.F.; Rosenberg, S.A.; Robbins, P.F. Generation of NY-ESO-1-specific CD4+ and CD8+ T cells by a single peptide with dual MHC class I and class II specificities: a new strategy for vaccine design. Cancer Res. 2002, 62, 3630. [Google Scholar]
- Zeng, G.; Touloukian, C.E.; Wang, X.; Restifo, N.P.; Rosenberg, S.A.; Wang, R.F. Identification of CD4+ T cell epitopes from NY-ESO-1 presented by HLA-DR molecules. J Immunol. 2000, 165, 1153. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Xu, Y.; Xiong, W.; Yin, B.; Huang, Y.; Chu, J.; Xing, C.; Qian, C.; Du, Y.; Duan, T.; Wang, H.Y.; Zhang, N.; Yu, J.S.; An, Z.; Wang, R. Development of a TCR-like antibody and chimeric antigen receptor against NY-ESO-1/HLA-A2 for cancer immunotherapy. J Immunother Cancer. 2022, 10, e004035. [Google Scholar] [CrossRef] [PubMed]
- Stuber, T.; Monjezi, R.; Wallstabe, L.; Kuhnemundt, J.; Nietzer, S.L.; Dandekar, G.; Wockel, A.; Einsele, H.; Wischhusen, J.; Hudecek, M. Inhibition of TGF-beta-receptor signaling augments the antitumor function of ROR1-specific CAR T-cells against triple-negative breast cancer. J Immunother Cancer. 2020, 8, e000676. [Google Scholar] [CrossRef] [PubMed]
- McKnight, B.N.; Kim, S.; Boerner, J.L.; Viola, N.T. Cetuximab PET delineated changes in cellular distribution of EGFR upon dasatinib treatment in triple negative breast cancer. Breast Cancer Res. 2020, 22, 37. [Google Scholar] [CrossRef] [PubMed]
- Manukian, G.; Kivolowitz, C.; DeAngelis, T.; Shastri, A.A.; Savage, J.E.; Camphausen, K.; Rodeck, U.; Zarif, J.C.; Simone, N.L. Caloric Restriction Impairs Regulatory T cells Within the Tumor Microenvironment After Radiation and Primes Effector T cells. Int J Radiat Oncol Biol Phys. 2021, 110, 1341. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Lee, N.; Pedroza, D.A.; Bado, I.L.; Hamor, C.; Zhang, L.; Aguirre, S.; Hu, J.; Shen, Y.; Xu, Y.; Gao, Y.; Zhao, N.; Chen, S.H.; Wan, Y.W.; Liu, Z.; Chang, J.T.; Hollern, D.; Perou, C.M.; Zhang, X.H.F.; Rosen, J.M. Chemotherapy Coupled to Macrophage Inhibition Induces T-cell and B-cell Infiltration and Durable Regression in Triple-Negative Breast Cancer. Cancer Res. 2022, 82, 2281. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.H.; Bae, J.H.; Choe, E.J.; Park, J.M.; Park, S.S.; Cho, H.J.; Song, B.J.; Baek, M.C. Macitentan improves antitumor immune responses by inhibiting the secretion of tumor-derived extracellular vesicle PD-L1. Theranostics. 2022, 12, 1971. [Google Scholar] [CrossRef] [PubMed]
- Zanker, D.J.; Spurling, A.J.; Brockwell, N.K.; Owen, K.L.; Zakhour, J.M.; Robinson, T.; Duivenvoorden, H.M.; Hertzog, P.J.; Mullins, S.R.; Wilkinson, R.W.; Parker, B.S. Intratumoral administration of the Toll-like receptor 7/8 agonist 3M-052 enhances interferon-driven tumor immunogenicity and suppresses metastatic spread in preclinical triple-negative breast cancer. Clin Transl Immunology. 2020, 9, e1177. [Google Scholar] [CrossRef] [PubMed]
- Tentler, J.J.; Lang, J.; Capasso, A.; Kim, D.J.; Benaim, E.; Lee, Y.B.; Eisen, A.; Bagby, S.M.; Hartman, S.J.; Yacob, B.W.; Gittleman, B.; Pitts, T.M.; Pelanda, R.; Eckhardt, S.G.; Diamond, J.R. RX-5902, a novel beta-catenin modulator, potentiates the efficacy of immune checkpoint inhibitors in preclinical models of triple-negative breast Cancer. BMC Cancer. 2020, 20, 1063. [Google Scholar] [CrossRef]
- Napier, T.S.; Lynch, S.E.; Lu, Y.; Song, P.N.; Burns, A.C.; Sorace, A.G. Molecular Imaging of Oxygenation Changes during Immunotherapy in Combination with Paclitaxel in Triple Negative Breast Cancer. Biomedicines. 2023, 11, 125. [Google Scholar] [CrossRef]
- He, J.; McLaughlin, R.P.; van der Noord, V.; Foekens, J.A.; Martens, J.W.M.; van Westen, G.; Zhang, Y.; van de Water, B. Multi-targeted kinase inhibition alleviates mTOR inhibitor resistance in triple-negative breast cancer. Breast Cancer Res Treat. 2019, 178, 263. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.Y.; Barker, C.A.; Arnold, B.B.; Powell, S.N.; Hu, Z.I.; Gucalp, A.; Lebron-Zapata, L.; Wen, H.Y.; Kallman, C.; D'Agnolo, A.; Zhang, Z.; Flynn, J.; Dunn, S.A.; McArthur, H.L. A phase 2 clinical trial assessing the efficacy and safety of pembrolizumab and radiotherapy in patients with metastatic triple-negative breast cancer. Cancer. 2020, 126, 850. [Google Scholar] [CrossRef] [PubMed]
- Schneeweiss, A.; Michel, L.L.; Mobus, V.; Tesch, H.; Klare, P.; Hahnen, E.; Denkert, C.; Kast, K.; Pohl-Rescigno, E.; Hanusch, C.; Link, T.; Untch, M.; Jackisch, C.; Blohmer, J.U.; Fasching, P.A.; Solbach, C.; Schmutzler, R.K.; Huober, J.; Rhiem, K.; Nekljudova, V.; Lubbe, K.; Loibl, S.; Gbg, *!!! REPLACE !!!*; Ago, B. Survival analysis of the randomised phase III GeparOcto trial comparing neoadjuvant chemotherapy of intense dose-dense epirubicin, paclitaxel, cyclophosphamide versus weekly paclitaxel, liposomal doxorubicin (plus carboplatin in triple-negative breast cancer) for patients with high-risk early breast cancer. Eur J Cancer. 2022, 160, 100. [Google Scholar] [PubMed]
- Anders, C.K.; Woodcock, M.G.; Van Swearingen, A.E.D.; Moore, D.T.; Sambade, M.J.; Laurie, S.; Robeson, A.; Kolupaev, O.; Cuaboy, L.A.; Garrett, A.L.; McKinnon, K.; Cowens, K.; Bortone, D.; Calhoun, B.C.; Wilkinson, A.D.; Carey, L.; Jolly, T.; Muss, H.; Reeder-Hayes, K.; Kaltman, R.; Jankowitz, R.; Gudena, V.; Olajide, O.; Perou, C.; Dees, E.C.; Vincent, B.G.; Serody, J.S. Evaluating the efficacy of a priming dose of cyclophosphamide prior to pembrolizumab to treat metastatic triple negative breast cancer. J Immunother Cancer. 2022, 10, e003427. [Google Scholar] [CrossRef] [PubMed]
- Criscitiello, C.; Marra, A.; Morganti, S.; Zagami, P.; Gandini, S.; Esposito, A.; Curigliano, G. Clinical outcomes of patients with metastatic breast cancer enrolled in phase I clinical trials. Eur J Cancer. 2021, 157, 40. [Google Scholar] [CrossRef] [PubMed]
- Iwata, H.; Inoue, K.; Kaneko, K.; Ito, Y.; Tsugawa, K.; Hasegawa, A.; Nakagawa, S.; Kuratomi, H.; Tamura, K. Subgroup analysis of Japanese patients in a Phase 3 study of atezolizumab in advanced triple-negative breast cancer (IMpassion130). Jpn J Clin Oncol. 2019, 49, 1083. [Google Scholar] [CrossRef]
- Hecht, J.R.; Raman, S.S.; Chan, A.; Kalinsky, K.; Baurain, J.F.; Jimenez, M.M.; Garcia, M.M.; Berger, M.D.; Lauer, U.M.; Khattak, A.; Carrato, A.; Zhang, Y.; Liu, K.; Cha, E.; Keegan, A.; Bhatta, S.; Strassburg, C.P.; Roohullah, A. Phase Ib study of talimogene laherparepvec in combination with atezolizumab in patients with triple negative breast cancer and colorectal cancer with liver metastases. ESMO Open. 2023, 8, 100884. [Google Scholar] [CrossRef]
- Liu, J.; Liu, Q.; Li, Y.; Li, Q.; Su, F.; Yao, H.; Su, S.; Wang, Q.; Jin, L.; Wang, Y.; Lau, W.Y.; Jiang, Z.; Song, E. Efficacy and safety of camrelizumab combined with apatinib in advanced triple-negative breast cancer: an open-label phase II trial. J Immunother Cancer. 2020, 8, e000696. [Google Scholar] [CrossRef]
- Liu, J.; Wang, Y.; Tian, Z.; Lin, Y.; Li, H.; Zhu, Z.; Liu, Q.; Su, S.; Zeng, Y.; Jia, W.; Yang, Y.; Xu, S.; Yao, H.; Jiang, W.; Song, E. Multicenter phase II trial of Camrelizumab combined with Apatinib and Eribulin in heavily pretreated patients with advanced triple-negative breast cancer. Nat Commun. 2022, 13, 3011. [Google Scholar] [CrossRef]
- Zhang, Q.; Shao, B.; Tong, Z.; Ouyang, Q.; Wang, Y.; Xu, G.; Li, S.; Li, H. A phase Ib study of camrelizumab in combination with apatinib and fuzuloparib in patients with recurrent or metastatic triple-negative breast cancer. BMC Med. 2022, 20, 321. [Google Scholar] [CrossRef]
- Wu, S.Y.; Xu, Y.; Chen, L.; Fan, L.; Ma, X.Y.; Zhao, S.; Song, X.Q.; Hu, X.; Yang, W.T.; Chai, W.J.; Guo, X.M.; Chen, X.Z.; Xu, Y.H.; Zhu, X.Y.; Zou, J.J.; Wang, Z.H.; Jiang, Y.Z.; Shao, Z.M. Combined angiogenesis and PD-1 inhibition for immunomodulatory TNBC: concept exploration and biomarker analysis in the FUTURE-C-Plus trial. Mol Cancer. 2022, 21, 84. [Google Scholar] [CrossRef]
- Foldi, J.; Kahn, A.; Silber, A.; Qing, T.; Reisenbichler, E.; Fischbach, N.; Persico, J.; Adelson, K.; Katoch, A.; Chagpar, A.; Park, T.; Blanchard, A.; Blenman, K.; Rimm, D.L.; Pusztai, L. Clinical Outcomes and Immune Markers by Race in a Phase I/II Clinical Trial of Durvalumab Concomitant with Neoadjuvant Chemotherapy in Early-Stage TNBC. Clin Cancer Res. 2022, 28, 3720. [Google Scholar] [CrossRef]
- Pusztai, L.; Yau, C.; Wolf, D.M.; Han, H.S.; Du, L.; Wallace, A.M.; String-Reasor, E.; Boughey, J.C.; Chien, A.J.; Elias, A.D.; Beckwith, H.; Nanda, R.; Albain, K.S.; Clark, A.S.; Kemmer, K.; Kalinsky, K.; Isaacs, C.; Thomas, A.; Shatsky, R.; Helsten, T.L.; Forero-Torres, A.; Liu, M.C.; Brown-Swigart, L.; Petricoin, E.F.; Wulfkuhle, J.D.; Asare, S.M.; Wilson, A.; Singhrao, R.; Sit, L.; Hirst, G.L.; Berry, S.; Sanil, A.; Asare, A.L.; Matthews, J.B.; Perlmutter, J.; Melisko, M.; Rugo, H.S.; Schwab, R.B.; Symmans, W.F.; Yee, D.; Van't Veer, L.J.; Hylton, N.M.; DeMichele, A.M.; Berry, D.A.; Esserman, L.J. Durvalumab with olaparib and paclitaxel for high-risk HER2-negative stage II/III breast cancer: Results from the adaptively randomized I-SPY2 trial. Cancer Cell. 2021, 39, 989. [Google Scholar] [CrossRef]
- Loibl, S.; Untch, M.; Burchardi, N.; Huober, J.; Sinn, B.V.; Blohmer, J.U.; Grischke, E.M.; Furlanetto, J.; Tesch, H.; Hanusch, C.; Engels, K.; Rezai, M.; Jackisch, C.; Schmitt, W.D.; von Minckwitz, G.; Thomalla, J.; Kummel, S.; Rautenberg, B.; Fasching, P.A.; Weber, K.; Rhiem, K.; Denkert, C.; Schneeweiss, A. A randomised phase II study investigating durvalumab in addition to an anthracycline taxane-based neoadjuvant therapy in early triple-negative breast cancer: clinical results and biomarker analysis of GeparNuevo study. Ann Oncol. 2019, 30, 1279. [Google Scholar] [CrossRef]
- Li, Q.; Wang, Y.; Jia, W.; Deng, H.; Li, G.; Deng, W.; Chen, J.; Kim, B.Y.S.; Jiang, W.; Liu, Q.; Liu, J. Low-Dose Anti-Angiogenic Therapy Sensitizes Breast Cancer to PD-1 Blockade. Clin Cancer Res. 2020, 26, 1712. [Google Scholar] [CrossRef] [PubMed]
- Chick, R.C.; Clifton, G.T.; Hale, D.F.; Vreeland, T.J.; Hickerson, A.T.; Kemp Bohan, P.M.; McCarthy, P.M.; Litton, J.K.; Alatrash, G.; Murthy, R.K.; Qiao, N.; Philips, A.; Lukas, J.; Holmes, J.P.; Mittendorf, E.A.; Peoples, G.E. Subgroup analysis of nelipepimut-S plus GM-CSF combined with trastuzumab versus trastuzumab alone to prevent recurrences in patients with high-risk, HER2 low-expressing breast cancer. Clin Immunol. 2021, 225, 108679. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, R.F.; Bakri, H.M.; Abdelfattah, O.N.; Eid, S. Does bevacizumab carry a hope for metastatic triple-negative breast cancer in the era of immunotherapy? Anti-Cancer Drug. 2022, 33, E604. [Google Scholar] [CrossRef] [PubMed]
- Goel, S.; Tan, A.R.; Rugo, H.S.; Aftimos, P.; Andric, Z.; Beelen, A.; Zhang, J.; Yi, J.S.; Malik, R.; O'Shaughnessy, J. Trilaciclib prior to gemcitabine plus carboplatin for metastatic triple-negative breast cancer: phase III PRESERVE 2. Future Oncol. 2022, 18, 3701. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Ren, J.; Zhang, J.; Yan, Y.; Jiang, N.; Yu, J.; Di, L.; Song, G.; Che, L.; Jia, J.; Zhou, X.; Yang, H.; Lyerly, H.K. Prospective study of cyclophosphamide, thiotepa, carboplatin combined with adoptive DC-CIK followed by metronomic cyclophosphamide therapy as salvage treatment for triple negative metastatic breast cancers patients (aged <45). Clin Transl Oncol. 2016, 18, 82. [Google Scholar]
- Jiang, Y.Z.; Liu, Y.; Xiao, Y.; Hu, X.; Jiang, L.; Zuo, W.J.; Ma, D.; Ding, J.; Zhu, X.; Zou, J.; Verschraegen, C.; Stover, D.G.; Kaklamani, V.; Wang, Z.H.; Shao, Z.M. Molecular subtyping and genomic profiling expand precision medicine in refractory metastatic triple-negative breast cancer: the FUTURE trial. Cell Res. 2021, 31, 178. [Google Scholar] [CrossRef]
- Mitchell, M.J.; Billingsley, M.M.; Haley, R.M.; Wechsler, M.E.; Peppas, N.A.; Langer, R. Engineering precision nanoparticles for drug delivery. Nat Rev Drug Discov. 2021, 20, 101. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Zhou, Y.; Liu, L.; Xu, Y.; Chen, Q.; Wang, Y.; Wu, S.; Deng, Y.; Zhang, J.; Shao, A. Nanoparticle-Based Drug Delivery in Cancer Therapy and Its Role in Overcoming Drug Resistance. Front Mol Biosci. 2020, 7, 193. [Google Scholar] [CrossRef]
- Zielinska, A.; Carreiro, F.; Oliveira, A.M.; Neves, A.; Pires, B.; Venkatesh, D.N.; Durazzo, A.; Lucarini, M.; Eder, P.; Silva, A.M.; Santini, A.; Souto, E.B. Polymeric Nanoparticles: Production, Characterization, Toxicology and Ecotoxicology. Molecules. 2020, 25, 3731. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Li, J.; Gu, L.; Wu, K.; Xing, H. Nanoparticles for Chemoimmunotherapy Against Triple-Negative Breast Cancer. Int J Nanomedicine. 2022, 17, 5209. [Google Scholar] [CrossRef] [PubMed]
- Krausz, A.E.; Adler, B.L.; Makdisi, J.; Schairer, D.; Rosen, J.; Landriscina, A.; Navati, M.; Alfieri, A.; Friedman, J.M.; Nosanchuk, J.D.; Rodriguez-Gabin, A.; Ye, K.Q.; McDaid, H.M.; Friedman, A.J. Nanoparticle-Encapsulated Doxorubicin Demonstrates Superior Tumor Cell Kill in Triple Negative Breast Cancer Subtypes Intrinsically Resistant to Doxorubicin. Precis Nanomed. 2018, 1, 173. [Google Scholar] [PubMed]
- Wu, J.; Wang, S.; Liu, S.; Liu, F.; Zhou, F. Immunoadjuvant Nanoparticles as Trojan Horses for Enhanced Photo-Immunotherapy in the Treatment of Triple-Negative Breast Cancer. Front Pharmacol. 2022, 13, 883428. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Liu, L.; Shang, H.; Feng, X.; Fan, N.; Wang, J.; Wu, Y.; Chen, Y.; Chu, X.; Zhong, M.; Sun, Y.; Fu, H.; Huang, W.; Li, Y. Self-Assembling Anchorage of Hyaluronic Acid on the Nanoparticle Surface Confers Superiority of Triple Negative Breast Cancer Treatment. Pharmaceutics. 2022, 14, 2461. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, A.; McGarry, S.; El-Sahli, S.; Li, L.; Chambers, J.; Phan, A.; Cote, M.; Cron, G.O.; Alain, T.; Le, Y.; Lee, S.H.; Liu, S.; Figeys, D.; Gadde, S.; Wang, L. Co-targeting Bulk Tumor and CSCs in Clinically Translatable TNBC Patient-Derived Xenografts via Combination Nanotherapy. Mol Cancer Ther. 2019, 18, 1755. [Google Scholar] [CrossRef]
- Chen, C.; Guo, Q.; Fu, H.; Yu, J.; Wang, L.; Sun, Y.; Zhang, J.; Duan, Y. Asynchronous blockade of PD-L1 and CD155 by polymeric nanoparticles inhibits triple-negative breast cancer progression and metastasis. Biomaterials. 2021, 275, 120988. [Google Scholar] [CrossRef]
- Valcourt, D.M.; Day, E.S. Dual Regulation of miR-34a and Notch Signaling in Triple-Negative Breast Cancer by Antibody/miRNA Nanocarriers. Mol Ther Nucleic Acids. 2020, 21, 290. [Google Scholar] [CrossRef]
- Valcourt, D.M.; Dang, M.N.; Day, E.S. IR820-loaded PLGA nanoparticles for photothermal therapy of triple-negative breast cancer. J Biomed Mater Res A. 2019, 107, 1702. [Google Scholar] [CrossRef] [PubMed]
- Valcourt, D.M.; Dang, M.N.; Scully, M.A.; Day, E.S. Nanoparticle-Mediated Co-Delivery of Notch-1 Antibodies and ABT-737 as a Potent Treatment Strategy for Triple-Negative Breast Cancer. ACS Nano. 2020, 14, 3378. [Google Scholar] [CrossRef] [PubMed]
- Agnello, L.; Tortorella, S.; d'Argenio, A.; Carbone, C.; Camorani, S.; Locatelli, E.; Auletta, L.; Sorrentino, D.; Fedele, M.; Zannetti, A.; Franchini, M.C.; Cerchia, L. Optimizing cisplatin delivery to triple-negative breast cancer through novel EGFR aptamer-conjugated polymeric nanovectors. J Exp Clin Cancer Res. 2021, 40, 239. [Google Scholar] [CrossRef] [PubMed]
- Bahman, F.; Pittala, V.; Haider, M.; Greish, K. Enhanced Anticancer Activity of Nanoformulation of Dasatinib against Triple-Negative Breast Cancer. J Pers Med. 2021, 11, 559. [Google Scholar] [CrossRef] [PubMed]
- Nabil, G.; Alzhrani, R.; Alsaab, H.O.; Atef, M.; Sau, S.; Iyer, A.K.; Banna, H.E. CD44 Targeted Nanomaterials for Treatment of Triple-Negative Breast Cancer. Cancers (Basel). 2021, 13, 898. [Google Scholar] [CrossRef] [PubMed]
- El-Deeb, I.M.; Pittala, V.; Eltayeb, D.; Greish, K. Selective Targeting of Breast Cancer by Tafuramycin A Using SMA-Nanoassemblies. Molecules. 2021, 26, 3532. [Google Scholar] [CrossRef] [PubMed]
- Greish, K.; Mathur, A.; Al Zahrani, R.; Elkaissi, S.; Al Jishi, M.; Nazzal, O.; Taha, S.; Pittala, V.; Taurin, S. Synthetic cannabinoids nano-micelles for the management of triple negative breast cancer. J Control Release. 2018, 291, 184. [Google Scholar] [CrossRef] [PubMed]
- Jiao, J.; Lu, H.; Wang, S. Photo-responsive prodrug nanoparticles for efficient cytoplasmic delivery and synergistic photodynamic-chemotherapy of metastatic triple-negative breast cancer. Acta Biomater. 2021, 126, 421. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Liu, Y.; Li, Y.; Wang, H.; Stewart, S.; Van der Jeught, K.; Agarwal, P.; Zhang, Y.; Liu, S.; Zhao, G.; Wan, J.; Lu, X.; He, X. Precise targeting of POLR2A as a therapeutic strategy for human triple negative breast cancer. Nat Nanotechnol. 2019, 14, 388. [Google Scholar] [CrossRef]
- Zhou, J.Y.; Li, K.K.; Zang, X.L.; Xie, Y.; Song, J.X.; Chen, X.H. ROS-responsive Galactosylated-nanoparticles with Doxorubicin Entrapment for Triple Negative Breast Cancer Therapy. Int J Nanomed. 2023, 18, 1381. [Google Scholar] [CrossRef]
- Cui, L.; Gouw, A.M.; LaGory, E.L.; Guo, S.; Attarwala, N.; Tang, Y.; Qi, J.; Chen, Y.S.; Gao, Z.; Casey, K.M.; Bazhin, A.A.; Chen, M.; Hu, L.; Xie, J.; Fang, M.; Zhang, C.; Zhu, Q.; Wang, Z.; Giaccia, A.J.; Gambhir, S.S.; Zhu, W.; Felsher, D.W.; Pegram, M.D.; Goun, E.A.; Le, A.; Rao, J. Mitochondrial copper depletion suppresses triple-negative breast cancer in mice. Nat Biotechnol. 2021, 39, 357. [Google Scholar] [CrossRef] [PubMed]
- Babu Varukattu, N.; Lin, W.; Vivek, R.; Rejeeth, C.; Sabarathinam, S.; Yao, Z.; Zhang, H. Targeted and Intrinsic Activity of HA-Functionalized PEI-Nanoceria as a Nano Reactor in Potential Triple-Negative Breast Cancer Treatment. ACS Appl Bio Mater. 2020, 3, 186. [Google Scholar] [CrossRef]
- Zong, Y.; Lin, Y.; Wei, T.; Cheng, Q. Lipid Nanoparticle (LNP) Enables mRNA Delivery for Cancer Therapy. Adv Mater. 2023, 35, e2303261. [Google Scholar] [CrossRef]
- Eskiler, G.G.; Cecener, G.; Egeli, U.; Tunca, B. Talazoparib nanoparticles for overcoming multidrug resistance in triple-negative breast cancer. J Cell Physiol. 2020, 235, 6230. [Google Scholar] [CrossRef] [PubMed]
- Mokhlis, H.A.; Bayraktar, R.; Kabil, N.N.; Caner, A.; Kahraman, N.; Rodriguez-Aguayo, C.; Zambalde, E.P.; Sheng, J.; Karagoz, K.; Kanlikilicer, P.; Abdel Aziz, A.A.H.; Abdelghany, T.M.; Ashour, A.A.; Wong, S.; Gatza, M.L.; Calin, G.A.; Lopez-Berestein, G.; Ozpolat, B. The Modulatory Role of MicroRNA-873 in the Progression of KRAS-Driven Cancers. Mol Ther Nucleic Acids. 2019, 14, 301. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Gu, C.; Gan, Y.; Shao, L.; Chen, H.; Zhu, H. Exosome-mediated siRNA delivery to suppress postoperative breast cancer metastasis. J Control Release. 2020, 318, 1. [Google Scholar] [CrossRef]
- Guo, P.; Yang, J.; Huang, J.; Auguste, D.T.; Moses, M.A. Therapeutic genome editing of triple-negative breast tumors using a noncationic and deformable nanolipogel. Proc Natl Acad Sci U S A. 2019, 116, 18295. [Google Scholar] [CrossRef]
- Bayda, S.; Hadla, M.; Palazzolo, S.; Riello, P.; Corona, G.; Toffoli, G.; Rizzolio, F. Inorganic Nanoparticles for Cancer Therapy: A Transition from Lab to Clinic. Curr Med Chem. 2018, 25, 4269. [Google Scholar] [CrossRef]
- Wu, L.; Wen, W.; Wang, X.; Huang, D.; Cao, J.; Qi, X.; Shen, S. Ultrasmall iron oxide nanoparticles cause significant toxicity by specifically inducing acute oxidative stress to multiple organs. Part Fibre Toxicol. 2022, 19, 24. [Google Scholar] [CrossRef]
- Ramchandani, D.; Lee, S.K.; Yomtoubian, S.; Han, M.S.; Tung, C.H.; Mittal, V. Nanoparticle Delivery of miR-708 Mimetic Impairs Breast Cancer Metastasis. Mol Cancer Ther. 2019, 18, 579. [Google Scholar] [CrossRef]
- Oei, A.L.; Korangath, P.; Mulka, K.; Helenius, M.; Coulter, J.B.; Stewart, J.; Velarde, E.; Crezee, J.; Simons, B.; Stalpers, L.J.A.; Kok, H.P.; Gabrielson, K.; Franken, N.A.P.; Ivkov, R. Enhancing the abscopal effect of radiation and immune checkpoint inhibitor therapies with magnetic nanoparticle hyperthermia in a model of metastatic breast cancer. Int J Hyperthermia. 2019, 36, 47. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Bao, S.; Qiu, G.; Liang, J.; Wang, Q.; Zhu, X.; Qin, G.; Liu, J.; Zhao, C. An Magnetic-Targeting Nano-Diagnosis and Treatment Platform for TNBC. Breast Cancer (Dove Med Press). 2023, 15, 101. [Google Scholar] [CrossRef] [PubMed]
- Fan, J.; Liu, B.; Long, Y.; Wang, Z.; Tong, C.; Wang, W.; You, P.; Liu, X. Sequentially-targeted biomimetic nano drug system for triple-negative breast cancer ablation and lung metastasis inhibition. Acta Biomater. 2020, 113, 554. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Liu, H.; Li, L.; Guo, Z.; Song, J.; Yang, X.; Wan, G.; Li, R.; Wang, Y. Leukocyte/platelet hybrid membrane-camouflaged dendritic large pore mesoporous silica nanoparticles co-loaded with photo/chemotherapeutic agents for triple negative breast cancer combination treatment. Bioact Mater. 2021, 6, 3865. [Google Scholar] [CrossRef] [PubMed]
- Jiang, S.; Liu, Z.; Tian, Y.; Zhuang, M.; Piao, S.; Gao, Y.; Tam, A.; Hu, H.; Cheng, W. A Comprehensive Evaluation of ZrC Nanoparticle in Combined Photothermal and Radiation Therapy for Treatment of Triple-Negative Breast Cancer. Front Oncol. 2021, 11, 801352. [Google Scholar] [CrossRef] [PubMed]
- Yardley, D.A. nab-Paclitaxel mechanisms of action and delivery. J Control Release. 2013, 170, 365. [Google Scholar] [CrossRef]
- Egorova, A.; Pyankov, I.; Maretina, M.; Baranov, V.; Kiselev, A. Peptide Nanoparticle-Mediated Combinatorial Delivery of Cancer-Related siRNAs for Synergistic Anti-Proliferative Activity in Triple Negative Breast Cancer Cells. Pharmaceuticals (Basel). 2021, 14, 957. [Google Scholar] [CrossRef]
- Yuan, H.; Guo, H.; Luan, X.; He, M.; Li, F.; Burnett, J.; Truchan, N.; Sun, D. Albumin Nanoparticle of Paclitaxel (Abraxane) Decreases while Taxol Increases Breast Cancer Stem Cells in Treatment of Triple Negative Breast Cancer. Mol Pharm. 2020, 17, 2275. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhao, C.; Lu, L.; Jiang, H.; Wang, F.; Zhang, X. Transcytosable Peptide-Paclitaxel Prodrug Nanoparticle for Targeted Treatment of Triple-Negative Breast Cancer. Int J Mol Sci. 2023, 24, 4646. [Google Scholar] [CrossRef]
- Liu, S.; Liu, H.; Sun, H.; Deng, S.; Yue, L.; Weng, Z.; Yang, J.; Zuo, B.; He, Y.; Zhang, B. (cRGD)2 peptides modified nanoparticles increase tumor-targeting therapeutic effects by co-delivery of albendazole and iodine-131. Anticancer Drugs. 2022, 33, 19. [Google Scholar] [CrossRef]
- Wang, X.; Tokheim, C.; Gu, S.S.; Wang, B.; Tang, Q.; Li, Y.; Traugh, N.; Zeng, Z.; Zhang, Y.; Li, Z.; Zhang, B.; Fu, J.; Xiao, T.; Li, W.; Meyer, C.A.; Chu, J.; Jiang, P.; Cejas, P.; Lim, K.; Long, H.; Brown, M.; Liu, X.S. In vivo CRISPR screens identify the E3 ligase Cop1 as a modulator of macrophage infiltration and cancer immunotherapy target. Cell. 2021, 184, 5357. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.T.H.; Xu, P.; Chow, A.; Man, S.; Kruger, J.; Khan, K.A.; Paez-Ribes, M.; Pham, E.; Kerbel, R.S. Pre- and post-operative anti-PD-L1 plus anti-angiogenic therapies in mouse breast or renal cancer models of micro- or macro-metastatic disease. Br J Cancer. 2019, 120, 196. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic diagram of combination therapy against TNBC. (A) Illustrates a combination therapeutics; (B) presents TNBC cells that express various ligands; (C) metastatic cancer cells that is located in other area than primary tumor tissue; and (D) the remaining healthy tissue after combination treatment.
Figure 1.
Schematic diagram of combination therapy against TNBC. (A) Illustrates a combination therapeutics; (B) presents TNBC cells that express various ligands; (C) metastatic cancer cells that is located in other area than primary tumor tissue; and (D) the remaining healthy tissue after combination treatment.
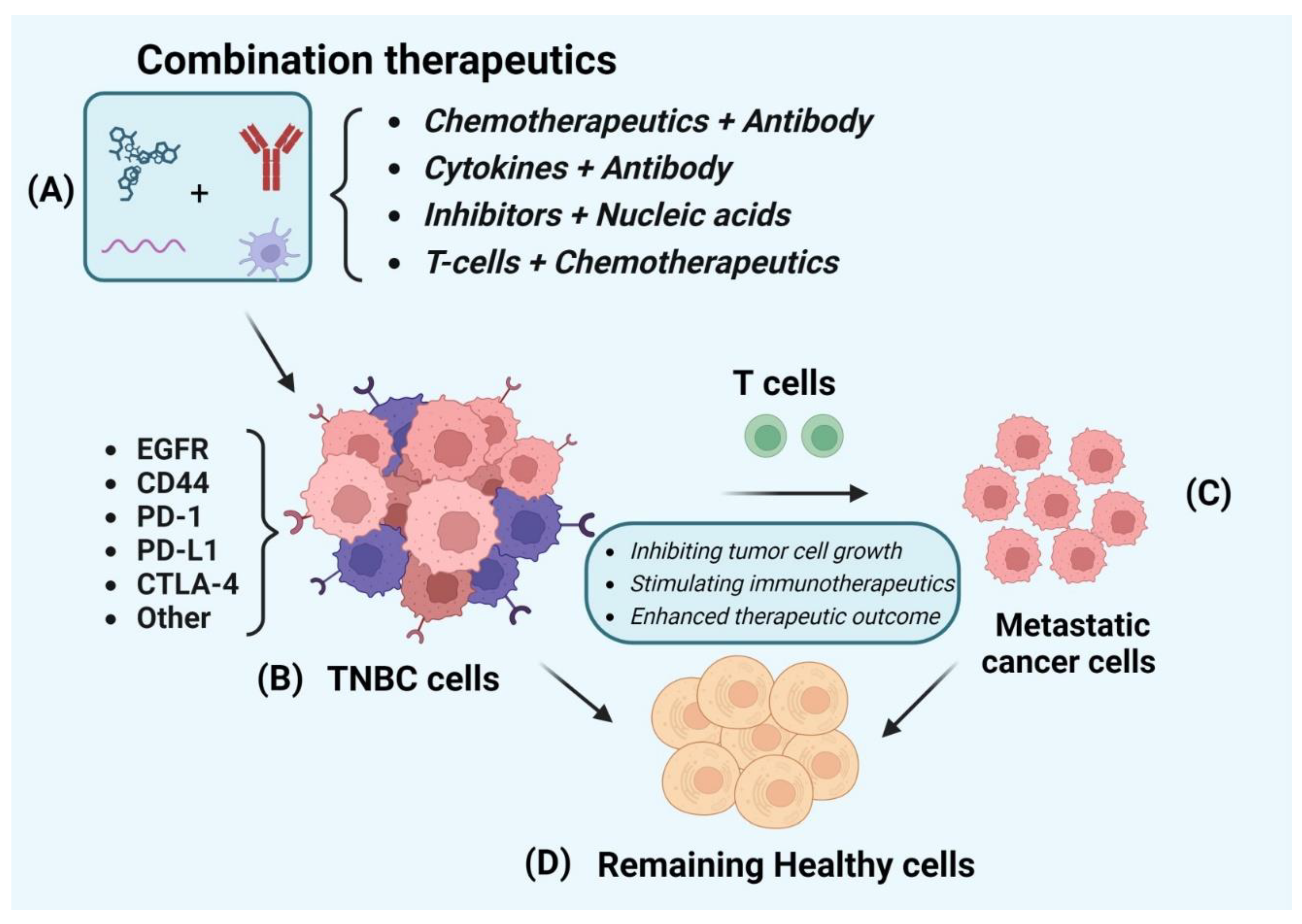
Figure 2.
The schematic diagram for nanoparticle-based therapy against TNBC. (A) Illustrates drug-loaded nanoparticles; (B) presents internalization of nanoparticles through TNBC cells; (C) metastatic cancer cells that are located in other areas than primary tumor tissue; and (D) the remaining healthy tissue after treatment of nanoparticle-based therapeutics.
Figure 2.
The schematic diagram for nanoparticle-based therapy against TNBC. (A) Illustrates drug-loaded nanoparticles; (B) presents internalization of nanoparticles through TNBC cells; (C) metastatic cancer cells that are located in other areas than primary tumor tissue; and (D) the remaining healthy tissue after treatment of nanoparticle-based therapeutics.
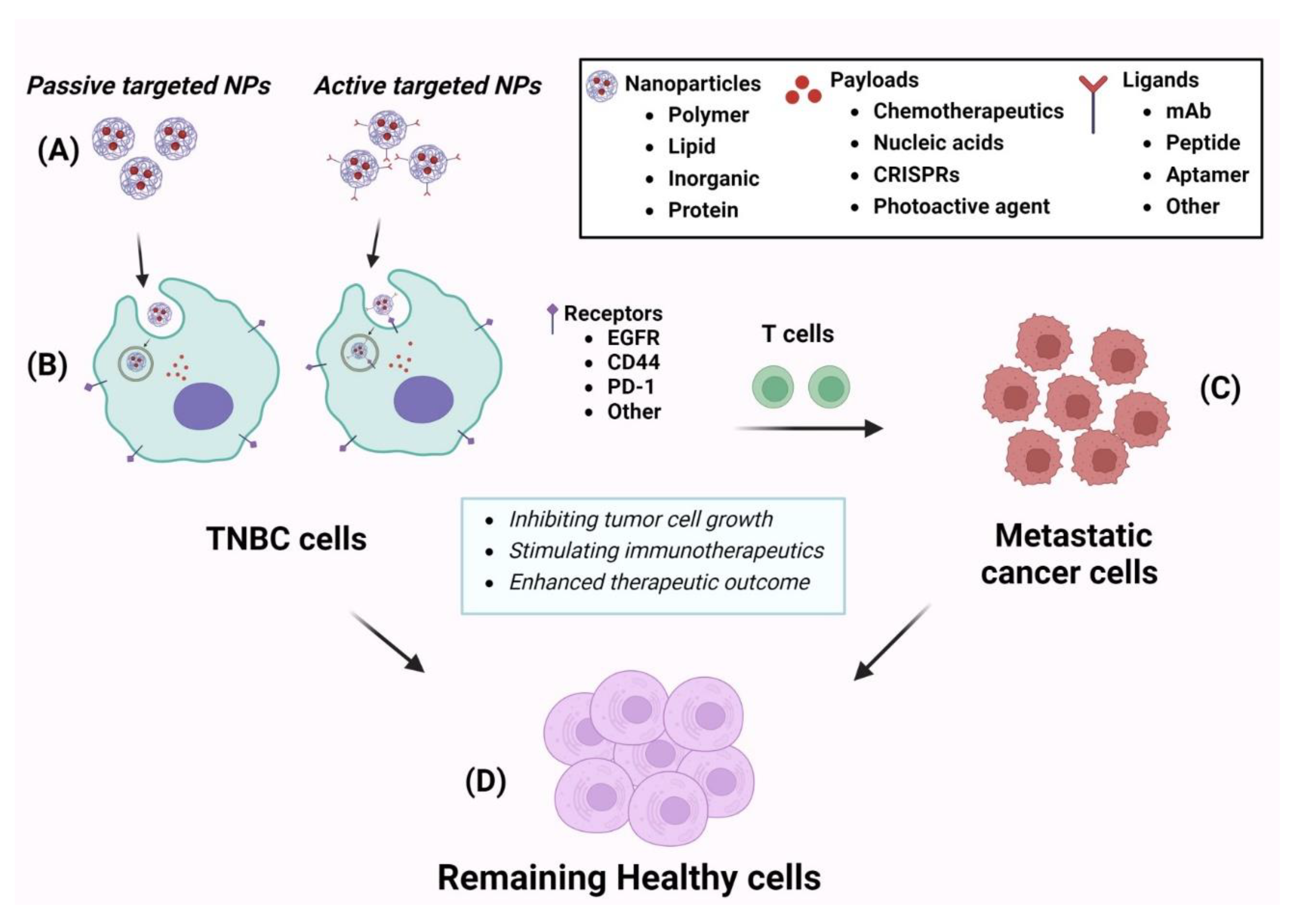

Table 1.
Summary of combination between immunotherapy and other therapies.
| Comb Therapeutics | Cell line and model | Stage | Results | Molecular target | Ref |
|---|---|---|---|---|---|
| Monoclonal antibody 2D2 and TCR-like CAR-T cell | HEK293T, MDA-MB231-ESO1, PC3-A2-ESO1T2, Mel586, Mel624, Mel1558 cells; MDA-MD231-N4-ESO-1 | In vitro and in vivo | TCR-like antibody derived CAR-T cells were able to inhibit tumor cell growth and overall survival of mouse. | HLA-A2, NY-ESO-1 | [22] |
| Anti-PD1 antibody and CRISPR knockout |
4T1-tumor bearing mice model |
In vitro and in vivo | In vivo CRISPR knockout enhanced antitumor immunity and strengthened immune checkpoint blockade | E3 ubiquitin ligase Cop1 | [91] |
| ICIs and PTX | 4T1, EO771; 4T1 and E0771 tumor-bearing mice model | In vitro and in vivo | The combination treatment reduced tumor growth . | PD-1 and CTLA-4 | [30] |
| Dasatinib/ radiotracer-attached cetuximab | MDA-MB231 cell and MDA-MB468 PDX tumor model | In vitro and in vivo | The results showed that combination of radiolabeled antibody and dasatinib was able to monitor drug distribution and treatment response in KRAS TNBC. | EGFR | [24] |
| Macitentan/ anti-PD-1 antibody | MDA-MB231, 4T1, CT26 and LL/2, EMT6; MDA-MB231, 4T1, and EMT6 tumor- bearing mice | In vitro and in vivo | The combination of MAC and anti-PD-1 antibody showed strong antitumor effect against TNBC, colon and lung cancer. | PD-1, CD8+T endothelin receptor | [27] |
| Radiotherapy/ caloric restriction ad libitum diet |
4T1-tumor bearing mice model |
In vitro and in vivo | The results revealed that the combination RT and CR enhanced immuno therapy effect against TNBC. | CD+8T cell, TME | [25] |
| 3M-O52 and anti PD1 antibody | E0771, CAL-120 and MDA-MB-231cells; 4T1.2 or E0771 bearing mice | In vitro and in vivo | The results showed the combination treatment reduced tumor growth and metastatic spread to lung | IFN, TME, PD1, Toll like receptor 7/8 | [28] |
| Cyclophosphamide (Cytoxan) and CSF1R inhibitor or an anti-CSF1R antibody | T11, T12 cell lines; T11, T12 and 215/R tumor -bearing mice model | In vitro and in vivo | The results illustrated the complexity of the tumor immune microenvironment and highlight different immune responses that result from rational immunotherapy combinations. | CSF1R | [26] |
| CAR-T cell and TGF-B inhibitor SA-208 | MDA-MB-231 | In vitro and in vivo | The results showed the combinatorial treatment of CAR-T cell and TGF-B receptor blockade was able to suppress tumor growth. | ROR1, TGF-B receptor | [23] |
| RX-5902 and PD-1 or CTLA-4 combination | 4T1 and MDA-MB231 TNBC tumor bearing mice model | In vitro and in vivo | The combination treatment decreased tumor growth and increased activated T cells | CTLA-4/ PD-1 | [29] |
| Anti-PD-L1 antibody and sunitinib/ Paclitaxel | EMT-6/P, EMT-6/CDDP, REN CA, | In vitro and in vivo | In the EMT-6/CDDP model, combination of anti-PD-L1 with paclitaxel chemotherapy (with or without anti-VEGF) was most effective as a neoadjuvant therapy in breast cancer. | PD-L1/ VEGF/VEGFR2 | [92] |
| Pembrolizumab and radiotherapy | 17 patients with TNBC | Phase II trial | Neutral efficacy but encocering? clinical activity | PD-L1 | [32] |
| Pembrolizumab and cyclophosphamide (antineoplastic agent) | 40 patients with TNBC | Phase II | Low outcome for TNBC patients | [34] | |
| Aterolizumab and nabpaclitaxel | 902 patients with TNBC | Phase III | Consistent with the overall IM passion 130 population | PD-L1 | [36] |
| Camrelizumab and Apatinib | 40 patients | Phase II | Objective response rate was much higher than monotherapy | PD-L1 | [38] |
| Durvalumab and nab-paclitaxel, DOX, and Cyclophosphamide | 67 patients with early stage TNBC | Phase I/II | The combination treatment improved survival rate of the patients. | PD-L1 | [42] |
Table 2.
Summary of nanotechnology-based therapy (therapeutic agent-loaded nanoparticles and their efficacy against TNBC.
Table 2.
Summary of nanotechnology-based therapy (therapeutic agent-loaded nanoparticles and their efficacy against TNBC.
| Nanoparticle | Drug | Cell line and model | Stage | Results | Targeting moiety and receptor | Ref |
|---|---|---|---|---|---|---|
| Sol-gel polymer nanoparticle | DOX | SUM149PT, HS578T, MDA-MB157 | In vitro and in vivo | DOX-NPs showed higher cell killing activity in comparison to free DOX. | EPR | [55] |
| HA-coated chitosan NPs | Curcumin | 4T1 cell line, 4T1 tumor-bearing mice |
In vitro and in vivo | It exhibited higher antitumor efficacy in TNBC- tumor model. | CD44 receptor | [57] |
| Lipid-polymer hybrid nanoparticle | PTX and verterporfin | MDA-MB231 cell line, HCl-002 PDX TNBC mice model |
In vitro and in vivo | As compared free drugs, the NPs showed significant suppression for tumor growth. | NFkB, Wnt and VAP pathways, cancer stem cells | [58] |
| mPEG-PLGA-PLL NPs | siRNA CD155 | 4T1 cell line, 4T1 –orthotopic tumor model |
In vitro and in vivo | The NPs improved early stage CD8+T cell immunosurveillance. | PD-L1 and CD155 receptor | [59] |
| PLGA Nps | miRNA | MDA-MB231 TNBC cell, MCF-10A normal cells | In vitro and in vivo | The NPs was able to impair TNBC cells | Notch-1 signal, miR-34a downstream | [60] |
| PLGA NPs | IR820 dye | MDA-MB231 cell, Tumor-bearing mice |
In vitro and in vivo | The NPs significantly reduced TNBC tumor growth. | EPR | [61] |
| PLGA NPs | ABT-737 (BcL2 inhibitor) | MDA-MB231 cell line, MCF-10A normal cell | In vitro and in vivo | The NPs exhibited high tumor accumulation and strong inhibition of tumor growth in TNBC tumor model. | Notch – 1 signal targeting | [62] |
| SMA polymer NPs | Dasatinib (TKI) | MDA-MB231, MCF7, and 4T1 cells; 4T1-bearing tumor model | In vitro and in vivo | The NPs showed 7-fold higher tumor suppression effect than free drug in tumor-bearing mice model. | EPR, ABL kinase Src (Kin2) receptor TKI | [64] |
| TPGS-SMA polymer NPs | CFM-4.16/ momelotinib | MDA-MB-231, MDA-MB468; MDA-MB231-bearing mice model | In vitro and in vivo | The NP revealed strong targeting ability to CD44 expressing cell | CD44 receptor | [65] |
| SMA polymer micelle | Taluzamycin-A | MDA-MB-231, MDA-MB468, MCF-7 cells; 4T1-tumor bearing mice | In vitro and in vivo | The NPs was uptaken by tumor tissue 4-times greater than free drug. | EPR | [66] |
| Polymer NPs | AL/ camptothecin | 4T1- cell line 4T1-tumor bearing mice model |
In vitro and in vivo | The combinatorial drug-loaded NPs showed tumor suppression effect against metastatic TNBC. | EPR, light sensitive delivery | [68] |
| PLGA polymer and lipid hybrid NPs | siRNA | MDA-MB453, MDA-MB231 cells; MDA-MB453 and MDA-MB231 –bearing mice model | In vitro and in vivo | The results showed that the NPs inhibited POLR2A and significantly reduced POLR2A positive tumor growth | POLR2A | [69] |
| P-glactose – polymethacrylate NPs | DOX | Human MDA-MB231, 4T1, HUVEC cells; 4T1 tumor-bearing mice | In vitro and in vivo | DOX-loaded NPs revealed higher cellular uptake and tumor accumulation as well as tumor suppression effect | Glactose, EPR | [70] |
| SMA-WIN polymer NPs | DOX and canabinoid | MDA-MB231, 4T1, MCF7; 4T1 –bearing mice | In vitro and in vivo | The dual drug-loaded NPs significantly reduced tumor growth as comparison in free drugs. | EPR | [67] |
| PLGA NPs | Cisplatin | MDA-MB231, BT-549, and MDA-231-EGFR-KO cells; MDA-M231 and MDA-MB231-KO- bearing mice | In vitro and in vivo | The cisplatin-PLGA Nps revealed strong tumor suppression efficacy in TNBC mice model | EGFR | [63] |
| HA-CePEI NPs | Cerium oxide (Ceria) | MDA-MB231, and HBL-100 cells | In vitro and in vivo | The NPs showed a strong apoptotic effect in TNBC cells due to its ROS generation and targeting ability | CD44 | [72] |
| SLNPs | PARP inhibitor talaroparib | HCC1937, MCF10A, and HCC1937-RC cells | In vitro and in vivo | The NPs were able to reduce MDR1, BCRP, and MRP1 gene expression, leading efficient therapeutic activity. | EPR | [74] |
| LNPs | microRNA (miR-878) | MCF10A, MDA-MB436, MDA-MB231, MDA-MB453, BT-20, HCC1937, SKBR3, T47D, HEK293 noraml HPDA, PANC1, BxPC3, MiaPaCa-2, Capan -2 | In vitro and in vivo | The NPs inhibited tumor growth in PDAC and TNBC tumor by suppressing cell proliferation and inducing apoptosis | EPR | [75] |
| Lipogel tNLGs | 3CRISPR plasmid | MDA-MB231, MDA-MB436, MCF10A; MDA-MB231-tumor-beairng mice | In vitro and in vivo | The NPs suppressed the expression of LCN2 oncogene and inhibited minimal host toxicity | ICAM1 | [77] |
| LbL- coated Gold NPs | miRNA (miR-708) | MDA-MB231, 293T, MDA-MB231-LM2 cells; 4T1-tumor-bearing mice | In vitro and in vivo | miRNA-gold NPs exhibited minimal host toxicity | EPR | [80] |
| Magnetic iron oxide NPs | Immune check point inhibitor | 4T1 cell line and 4T1 –tumor bearing mice | In vitro and in vivo | The MIO NPs reduced tumor growth in TNBC tumor model | EPR, PD-1, CTLA-4 | [81] |
| Graphene oxide Qdot NPs | Gamma bufotacin and DOX | MDA-MB231, BGC-823, Hela, NIH-3T3 RAW264.7 | In vitro and in vivo | The dual drug-loaded NPs were uptaken 2-fold higher by tumor cells in comparison with naked one and reduced lung metastasis. | TAT, RGD | [83] |
| Peptide-drug conjugate NPs | PTX | 4T1-mcherry-luc cell; 4T1-tumor bearing mice | In vitro and in vivo | The NPs strongly inhibited tumor growth | NRP1 (Neuropilin 1) | [89] |
| RGD-HAS NPs | Aldendarole/ iodine-131 | MDA-MB231; 4T1-cells | In vitro and in vivo | RGA-coupled NPs were able to penetrate into tumor and inhibit tumor growth | cRGD and integrin | [90] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



